an online journal of case reports edited by gi...
TRANSCRIPT

ACG Case Reports Journal | Volume 1 | Issue 3April 2014
acgcasereports.gi.orgEditor-in-Chief: Mohammad Yaghoobi, MD, MSc, AFS
An online journal of case reports edited by GI fellows

EISSN: 2326-3253 © American College of Gatstroenterology
EDITORIAL BOARD
Editor in ChiefMohammad Yaghoobi, MD, MSc, AFSMedical University of South Carolina, Charleston, SC
Executive EditorManish Singla, MDWalter Reed National Military Medical Center, Bethesda, MD
Associate EditorsDaniel E. Freedberg, MDColumbia University Medical Center, New York, NY
Nazia Hasan, MD, MPHNew York University School of Medicine, New York, NY
Ryan Law, DOMayo Clinic, Rochester, MN
Kalyan Ray Parashette, MDIndiana University School of Medicine, Indianapolis, IN
Andres J. Yarur, MDUniversity of Miami Miller School of Medicine, Miami, FL
EDITORIAL STAFF
Lindsey ToppEditorial Advisor
Jenny DunningtonEditorial Assistant
Theresa BongornoGraphic Designer
AIMS AND SCOPE
ACG Case Reports Journal, published by the American College of Gastroenterol-ogy and edited exclusively by GI fellows, provides a peer-reviewed publishing out-let for GI fellows, private practice clinicians, and other members of the healthcare team to share interesting case reports. This quarterly, open-access publication will make all content freely available online to all readers. ACG Case Reports Journal publishes case reports, images, and letters to the editor in all topics of gastroenterology and hepatology.
The ACG Case Reports Journal was created to help fulfill ACG’s commitment to providing growth and learning opportunities for GI fellows, and helps fellows meet core curriculum requirements for non-patient care activities. To this end, all case submissions must have a GI fellow or a resident interested in pursuing GI fellowship as the lead author. Cases authored by private practice clinicians and other members of the health care team who might traditionally face difficulty publishing with leading journals are also welcome.
PUBLISHER INFORMATION
Founded in 1932, the American College of Gastroenterology (ACG) is an organi-zation with an international membership of more than 12,000 individuals from 86 countries. The College is committed to serving the clinically oriented digestive disease specialist through its emphasis on scholarly practice, teaching and research. The mission of the College is to serve the evolving needs of physicians in the delivery of high quality, scientifically sound, humanistic, ethical, and cost-effective health care to gastroenterology patients.
American College of Gastroenterology6400 Goldsboro Road, Suite 200 Bethesda, MD 20817Phone: 301-263-9000 | Fax: [email protected]
PUBLICATION
ACG Case Reports Journal is published online each quarter, and issues feature images, video clips, and multimedia content in addition to case descriptions. As an open-access publication, full-text articles are freely accessible for all readers in both HTML and PDF format immediately upon online publication. There is no print version of the Journal, but issue articles will be collated into an easily down-loadable PDF for offline viewing and printing. ACG Case Reports Journal does not charge submission or publication fees for authors.
PREPARING FOR SUBMISSION
Manuscripts must be submitted online at mc.manuscriptcentral.com/acgcr. Questions regarding submission or site access should be sent to [email protected]. The ACG Case Reports Journal recommends that submitted manuscripts follow the general recommendations put forth by the ICMJE Uniform Requirements for Manuscripts.
PERMISSIONS
Authors are required to obtain permission to reproduce previously copyrighted materials from other sources in both print and electronic form. For questions regarding permissions for manuscripts published in ACG Case Reports Journal, please contact [email protected].
ETHICS AND JOURNAL CONFLICT OF INTEREST
Authors must disclose all conflicts of interest, financial and otherwise, upon manuscript submission. Each year, the Editors publicly disclose their conflicts of interest on the ACG Case Reports Journal website.
When reporting on human or animal subjects, authors must state whether the work was approved by a local IRB or ethics committee, or in accordance with the Helsinki Declaration of 1975, as revised in 2008. Efforts should always be made to guarantee protection of patient privacy in submitted cases.
OPEN ACCESS AND CREATIVE COMMONS LICENSING
ACG Case Reports Journal content is licensed according to the Creative Com-mons Attribution-Noncommercial-No Derivative Works 3.0 Unported license, under which users are free to share (copy, distribute and transmit) the contribu-tion under the following conditions:
• Attribution. Users must attribute the contribution in the manner specified by the author or licensor (but not in any way that suggests that they or their use of the contribution is endorsed by the author or licensor).
• Non-commercial. Users may not use this contribution for commercial purposes.
• No derivative works. Users may not alter, transform, or build upon this work.
For any reuse or distribution, users must make clear to others the license terms of this work. The best way to do this is with a link to the web URL of the pub-lished work. Any of the above conditions can be waived if users obtain permis-sion from the copyright holder. The full legal terms of this license can be found on the Creative Commons website.
DUPLICATE PUBLICATION
Manuscripts must not be submitted to or previously published in any other journal. Any case that has been presented as a poster or oral presentation at any scientific meeting should contain a disclosure statement of this fact on the title page of the submission. Further, any cases published as an abstract related to a scientific meeting should be considerably expanded and enriched from the abstract version, and should contain a full disclosure of this former publication, including a full citation.
MANUSCRIPT ARCHIVE DEPOSITION
If your funding bodies and/or institution requires authors to self-archive articles in publicly accessible archives, then authors are responsible for depositing the accepted version of their manuscript into such an archive. ACG Case Reports Journal will register for indexing on PubMed as soon as possible.
ACGCASE REPORTS JOURNALacgcasereports.gi.org
ABOUT THE JOURNAL

TABLE OF CONTENTSACG Case Reports Journal | Volume 1 | Issue 3
April 2014
acgcasereports.gi.org
Letter from the Editor____________________________________________________________
118 Tips for a Successful Case Report Mohammad Yaghoobi, MD, MSc, AFS
Images____________________________________________________________
119 Unusual Finding of an Intact Moth During Routine Colonoscopy Brijesh B. Patel, MD, Christian M. Andrade, MD, Marc J. Lajeunesse, PhD, and Reynaldo Geerken, MD
120 Emphysematous Gastritis: An Ominous Diagnosis Managed Conservatively Brent E. Murchie, MD, Andrew C. Berry, BS, Andrew Ukleja, MD, Ryan
McPherson, BA, Ariel Caplan, DO, and Warren L. Reuther III, MD
122 Endosonographic Findings in Colitis Cystica Profunda Mohamed Sultan, MD, Walid Chalhoub, MD, Klaus Gottlieb, MD, and Gustavo
Marino, MD
124 Hepatobiliary Fascioliasis: An Uncommon Cause of Biliary Obstruction in the United States
Jeff Basile, MD, M. Stanley Branch, MD, Svetang V. Desai, MD, Christopher Arnold, MD, Alastair Smith, MB, CHB, FRCP, and Tzu-Hao Lee, MD
Case Reports____________________________________________________________
126 A Novel Approach to Management of Esophageal Pill Impaction Brent W. Lacey, MD, Sean Caufield, MD, Eric Lavery, MD, and Brett Partridge, MD
128 Hepatic Portal Venous Gas: An Unusual Complication Following Upper Endoscopy and Dilation
Kristina Seeger, MD, and Sami R. Achem, MD
131 Acute Esophageal Necrosis: A Case of Black Esophagus Associated with Bismuth Subsalicylate Ingestion
Jean Abed, MD, Pavan Mankal, MD, Hani Judeh, MD, and Sang Kim, MD
134 A Treatment Option for Esophageal Intramural Pseudodiverticulosis Amy Tyberg, MD, and Daniela Jodorkovsky, MD
137 Glass Microparticulate Ingestion: An Unusual and Difficult-to-Diagnose Cause of Chronic Abdominal Pain
R. Brooks Vance, MD, Marcus Mühlbauer, MD, PhD, Elizabeth B. Dreesen, MD, C. Robert Bagnell, Jr., PhD, Georgette A. Dent, MD, Hans Herfarth, MD, PhD, Christian Jobin, PhD, and Evan S. Dellon, MD, MPH
Diffuse portal venous gas throughout the right he-patic lobe extending to the periphery of the liver. (Image from Seeger et al, page 128.)
Abdominal CT showing IVC filter struts penetrat-ing the duodenum and right psoas muscle.(Im-age from Oza et al, page 143.)

TABLE OF CONTENTS
acgcasereports.gi.org
Case Reports____________________________________________________________
140 Hemophagocytic Lymphohistiocytic Syndrome and Enteropathy-Associated T-cell Lymphoma in a Patient with Refractory Celiac Disease
Lucy Lu, MD, Shuoyan Ning, MD, Zain Kassam, MD, Richard Hunt, MB, MACG, and Marco Puglia, MD
143 Asymptomatic Duodenal Perforation from an Inferior Vena Cava Filter Jean R. Park, MD, Veeral M. Oza, MD, and Somashekar G. Krishna, MD, MPH
145 Hematochezia Associated with Sevalamer-Induced Mucosal Injury Preethi Chintamaneni, MD, Rohit Das, MD, Shih-Fan Kuan, MD, Taher R.
Kermanshahi, MD, and Jana G. Hashash, MD
148 Use of Serum Infliximab Level Prior to Cyclosporine Salvage Therapy in Severe Ulcerative Colitis
Christopher G. Chapman, MD, Ashley Bochenek, MSN, APN/FNP-BC, Adam C. Stein, MD, and David T. Rubin, MD
151 A Unique Case of Hematemesis in a 17-Year-Old Female Tobias Zuchelli, MD, Eva Alsheik, MD, Bhavik Bhandari, MD, and Daniel
Ringold, MD
154 Groove Pancreatitis: Four Cases from a Single Center and Brief Review of the Literature
Tyler P. Black, MD, Cynthia D. Guy, MD, Rebekah R. White, MD, Jorge Obando, MD, and Rebecca A. Burbridge, MD
158 Bouveret’s Syndrome with Severe Esophagitis and a Purulent Fistula Rami Bonam, MD, Zahid Vahora, MD, Glenn Harvin, MD, and William Leland, MD
161 A Case of an Ectopic Ampulla of Vater in the Pyloric Channel Sunil Dacha, MD, Xiao Jing Wang, MD, and Emad Qayed, MD
164 Sarcoidosis Presenting as Necrotizing Sarcoid Granulomatosis of the Liver, Sclerosing Cholangitis, and Gastric Ulcer
Njideka Momah, MD, Adetola Otesile, BSc, Rishi Pawa, MD, and Steve Shedlofsky, MD
167 Polymyositis Associated with Hepatitis B Virus Cirrhosis and Advanced Hepatocellular Carcinoma
Kessarin Thanapirom, MD, Satimai Aniwan, MD, and Sombat Treeprasertsuk, MD
170 Ceftriaxone-Induced Gallstones: Case Report and Literature Review Aditi Nayak, MD, and Adam Slivka, MD, PhD
A balloon occlusion cholangiogram showing a distal common bile duct diameter of 7 mm and a round filling defect consistent with a bile duct stone. (Image from Dacha et al, page 161.)
ACG Case Reports Journal | Volume 1 | Issue 3April 2014
Successful coil embolization of a 2.8-cm GDA pseudoaneurysm and outflow track of the right gastroepiploic artery.(Image from Zuchelli et al, page 151.)

acgcasereports.gi.org ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014118
ACG CASE REPORTS JOURNAL
Tips for a Successful Case Report After a year of serving as the Editor-in-Chief of the ACG Case Reports Journal, I have been privileged to read hundreds of submitted case reports. Every submitted report has had its merits, and I wanted to highlight the characteristics of successful and well-written case reports that we have seen. NoveltyNovelty is the single most important factor in writing an interesting case report. A comprehensive literature search can determine if the subject has been previously reported and can highlight novel aspects of your case to distinguish it from those in the literature. A specific and unique title to describe your case will grab the reader’s attention.
Use Medical LanguageMake yourself familiar with the language of current medical literature before writing your manuscript. This can help you translate your case from a vernacular
used in daily patient care to a more formal style of scientific writing. Manuscripts with simple text, active voice, and straightforward language attract readers, while unnecessary data and flowery language may be confusing and tedious.
Identify LimitationsGiven the limitations of a case report compared to other forms of evidence-based documents, it is necessary to place your case in context. It is difficult to prove association with certainty in a case report; therefore, the discussion should avoid making wide-reaching conclusions based on a single experience. Advice from a senior colleague can help contextualize the role your case plays in the academic sphere.
Remember the Author InstructionsPrior to submitting a case report, remember to review the author guidelines and instructions. These details differ based on the target journal, but following them carefully will shorten the review process. Take this time to also have a colleague review your manuscript for spelling or grammatical errors, and clarifications of scientific writing. Reviewers enjoy reading clear and well-written manuscripts, and are often turned off by simple spelling and grammatical mistakes. One final review before submitting your manuscript can help identify small, overlooked mistakes and give your writing more polish.
Confidentiality and Patients’ RightsEvery effort should be made to obtain an informed consent from the patient, parents of a minor patient, or the next of kin of deceased patients. Make sure no identifying patient information is included in the text or in images. If consent cannot be obtained, provide a thorough description of the situation with your submission. In the current era of evidence-based medicine, case reports are considered first-line evidence and might be the first academic contribution a young physician has in his or her career. I hope the above guidance and the opportunity provided by the ACG Case Reports Journal helps encourage our next generation of writers.
Mohammad Yaghoobi, MD, MSc, AFSEditor-in-ChiefACG Case Reports Journal
ACG Case Rep J 2014;1(3):118. doi:10.14309/crj.2014.20. Published online: April 4, 2014.
Copyright: © 2014 ACG Case Reports Journal. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
LETTER FROM THE EDITOR

ACG CASE REPORTS JOURNAL
acgcasereports.gi.org ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014119
IMAGE | ENDOSCOPY
Unusual Finding of an Intact Moth During Routine ColonoscopyBrijesh B. Patel, MD1,2, Christian M. Andrade, MD1,2, Marc J. Lajeunesse, PhD3, and Reynaldo Geerken, MD2
1Division of Digestive Diseases and Nutrition, University of South Florida, Tampa, FL2Department of Gastroenterology, James A. Haley Veterans Affairs, Tampa, FL3Department of Integrative Biology, University of South Florida, Tampa, FL
Case ReportThere is scant literature describing inadvertent ingestion of insects visualized during endoscopy.1,2 Previously de-scribed insects include ants, wasps, bees, yellow jackets, and cockroaches. We present a case of a 55-year-old male with a normal colonoscopy except for the discovery of a lifeless winged insect between folds of the trans-verse colon (Figure 1). In the image, the insect is ventral side up on the colon lining. Two compound eyes and abdomen are visible, but the thorax and portions of the wings are overexposed. Six legs can be discerned, and the insect had roughly a 6-mm craniocaudal length and a 12-mm wingspan. The image was later identified by an entomologist as a moth belonging to order Lepidoptera. Moths typically have scales covering the body and wings, but these scales are easily removed when exposed to an acidic environment. A loss of these scales explains the whitish coloration of the moth, as most of the pigmentation is found on the scales. Although these ingestions are of little consequence to the patient, they are quite rare and may even be startling to the endoscopist. To our knowledge, this is the first case of a moth described within the gastrointestinal tract.
ACG Case Rep J 2014;1(3):119. doi:10.14309/crj.2014.21. Published online: April 4, 2014.
Correspondence: Brijesh B. Patel, Division of Digestive Diseases and Nutrition, University of South Florida Morsani College of Medicine, 12901 Bruce B. Downs Blvd., MDC 82, Tampa, FL 33612 ([email protected]).
Copyright: © 2014 Patel et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Figure 1. Winged insect noted in the transverse colon during routine colonoscopy.
Disclosures
Author contributions: BB Patel, CM Andrade, and MJ Lajeunesse wrote and edited the manuscript. R. Geerken provided endoscop-ic images and reviewed and edited the final manuscript. BB Patel is the article guarantor.
Financial disclosure: None of the authors re-ceived financial support for the manuscript or express any personal or financial conflicts of interest.
Informed consent was obtained for this case report.
Received: December 20, 2013; Accepted: February 18, 2014
References1. Kumar AR, Perez JA, Miick R, Govil YK. An unusual finding during screening colonoscopy: A cockroach! Endoscopy. 2010;42
(suppl 2):E209–E210. 2. Malik TA, Luz LP, Peter S. Caught on camera: An unusual type of bug in the gut. Gastrointest Endosc. 2011;73(2):363–4.

ACG CASE REPORTS JOURNAL
acgcasereports.gi.org ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014120
IMAGE | STOMACH
Emphysematous Gastritis: An Ominous Diagnosis Managed ConservativelyBrent E. Murchie, MD1, Andrew C. Berry, BS2, Andrew Ukleja, MD1, Ryan McPherson, BA2, Ariel Caplan, DO3, and Warren L. Reuther III, MD4
1Digestive Diseases Institute, Cleveland Clinic Florida, Weston, FL2Kansas City University of Medicine and Biosciences, Kansas City, MO3Internal Medicine Department, Palm Beach Centre for Graduate Medical Education, West Palm Beach, FL4Department of Radiology, West Palm Hospital, West Palm Beach, FL
Case ReportA 54-year-old female with HIV, diabetes, and chronic obstructive pulmonary disease (COPD) presented with altered mental status, diabetic ketoacidosis, nonspecific gastrointestinal symptoms, and a buttock abscess. Initial abdominal and pelvic computed tomography (CT) without contrast demonstrated a small pericardial effusion, air in the gastric wall, and perianal abscess. Amid worsening leukocytosis (22.500/mm3), a wide excisional debridement of abscess was performed and later repeated. CT angiography of the chest demon-strated a markedly distended stomach with small amount of portal venous air (Figure 1). Abdominal X-ray of the kidney, ureters, and bladder (KUB) demonstrated a distended stomach with wall emphysema and gas col-lection within the gluteal region (Figure 2). Esophagogastroduodenoscopy (EGD) revealed black eschars and
ACG Case Rep J 2014;1(3):120–121. doi:10.14309/crj.2014.22. Published online: April 4, 2014.
Correspondence: Andrew C. Berry, Kansas City University of Medicine and Biosciences, 1750 E. Independence Ave. Kansas City, MO 64106 ([email protected]).
Copyright: © 2014 Murchie et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Figure 1. CT chest angiography demonstrating portal venous air and a mottled, non-linear air pattern in the gastric wall.
Figure 2. Abdominal X-ray of kidney, ureters, and bladder (KUB) showing gas/air within both the gastric lumen and the stomach wall.
exudates in the stomach body and fundus (Figure 3). When gastric wall air is present, emphysematous gastritis—with a mortality rate of 50–80%—must be properly distinguished from the more common and less devastating gastric emphysema.1,2 Air within the

Publish your work in ACG Case Reports JournalACG Case Reports Journal is a peer-reviewed, open-access publication that provides GI fellows, private practice clinicians, and other members of the health care team an opportunity to share interesting case reports with their peers and with leaders in the field. Visit http://acgcasereports.gi.org for submission guidelines. Submit your manuscript online at http://mc.manuscriptcentral.com/acgcr.
Murchie et al
acgcasereports.gi.org
Emphysematous Gastritis
121 ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014
gastric wall, together with portal venous air, leukocytosis, and a source of infection all support the diagnosis of emphy-sematous gastritis.3,4 Without evidence of sepsis or ischemia, surgical intervention was not indicated. Conservative man-agement with bowel rest, parenteral nutrition, and broad-spectrum antibiotics was successful.5 The role of endoscopy in cases like this is strictly to monitor severity, identify gastric necrosis, and exclude other pathology.
Disclosures
Author contributions: All authors contributed to evaluating and managing the case and to writing the manuscript. AC Berry is the article guarantor.
Financial disclosure: No financial support or conflicts ofinterest to report.
Informed consent was obtained for this case report.
Received: November 18, 2013; Accepted: March 16, 2014
References1. Iannuzzi J, Watson TJ, Litle VR. Emphysematous gastritis: A young
diabetic’s recovery. Int J Surg Case Rep. 2012;3(4):125–7.2. Yalamanchili M, Cady W. Emphysematous gastritis in a hemodialysis
patient. South Med J. 2003;96(1):84–8.3. Kussin SZ, Henry C, Navarro C, et al. Gas within the wall of the
stomach: Report of a case and review of the literature. Dig Dis Sci. 1982;27(10):949–54.
4. Loi TH, See JY, Diddapur RK, Issac JR. Emphysematous gastritis: A case report and a review of literature. Ann Acad Med Singapore. 2007;36(1):72–3.
5. Szuchmacher M, Bedford T, Sukharamwala P, et al. Is surgical inter-vention avoidable in cases of emphysematous gastritis? A case pre-sentation and literature review. Int J Surg Case Rep. 2013;4(5):456–9.
Figure 3. EGD demonstrating black eschars and exudates in the body and fundus of the stomach.

ACG CASE REPORTS JOURNAL
acgcasereports.gi.org ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014122
IMAGE | COLON
Endosonographic Findings in Colitis Cystica ProfundaMohamed Sultan, MD1, Walid Chalhoub, MD1, Klaus Gottlieb, MD2, and Gustavo Marino, MD2
1Division of Gastroenterology, MedStar Georgetown University Hospital, Washington, DC 2Division of Gastroenterology, Veteran Affairs Medical Center, Washington, DC
Case ReportA 27-year-old male was referred to our institution for further evaluation of persistent rectal bleeding. A prior colonoscopy showed a sigmoid soft tissue lesion, and pathology revealed chronic active colitis and granula-tion tissue with ulcers and focal adenomatous changes. We performed a flexible sigmoidoscopy that showed a 4.5-cm multilobulated polypoid lesion approximately 45 cm from the anal verge (Figure 1). A 20 MHz Olympus endoscopic ultrasound (EUS) miniprobe showed hypoechoic lesion with cystic/spongy features involving the mucosa and submucosa (Figure 2). These features were thought to suggest colitis cystica profunda (CCP). His-tologic examination of snare biopsies identified dilated glands with mucinous content, surrounded by variable degrees of fibrosis on a background of interspersed chronic inflammatory cells, with few colonic mucosal crypts and mild inflammatory cell infiltrate (Figure 3). The patient was instructed to follow up with gastroenterology if bleeding recurred.
CCP is a rare, benign disease of the colon and rectum often mimicking malignancy. It was first described in 1766 by Stark, who reported 2 cases associated with dysentery.1 Histologically, it is characterized by dilated mucous glands mostly limited to the submucosa, but there are reported cases of penetration to the muscularis mucosa.1 The etiology of CCP remains controversial; however, many consider solitary rectal ulcer syndrome (SRUS) and
ACG Case Rep J 2014;1(3):122–123. doi:10.14309/crj.2014.23. Published online: April 4, 2014.
Correspondence: Mohamed Sultan, Georgetown University Hospital, Gastroenterology, 3800 Reservoir Rd. NW, 5th Floor PHC Building, Department of Medicine, Washington, DC, 20007 ([email protected]).
Copyright: © 2014 Sultan et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Figure 1. Endoscopic image of CCP showing polypoid lesion with lobulated appearance and some hemorrhagic areas with normal surrounding mucosa.
Figure 2. EUS showing hypoechoic lesion with cystic/spongy features, with involvement of the mucosa and submucosal. The muscularis propria appears intact.

Publish your work in ACG Case Reports JournalACG Case Reports Journal is a peer-reviewed, open-access publication that provides GI fellows, private practice clinicians, and other members of the health care team an opportunity to share interesting case reports with their peers and with leaders in the field. Visit http://acgcasereports.gi.org for submission guidelines. Submit your manuscript online at http://mc.manuscriptcentral.com/acgcr.
Sultan et al
acgcasereports.gi.org
Colitis Cystica Profunda
123 ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014
CCP to be different manifestations of the same pathology due to overlapping features.2 Surface mucosal biopsies may rule out neoplasia, but only deep biopsies show character-istic histological features.1 There are few case reports of the endosonographic features of CCP,3 which include multiple hypoechoic or anechoic lesions affecting mucosa or sub-mucosa, with areas of echorefringent fibrosis between le-sions in the absence of lymph node enlargement. EUS was instrumental in making our diagnosis and providing proper counseling to the patient.
Disclosures
Author contributions: All authors contributed equally to this article. M. Sultan is the article guarantor.
Financial disclosure: The authors have no financial disclosure.
Informed consent was obtained for this case report.
Received: December 9, 2013; Accepted: March 4, 2014
References1. Guest CB, Reznick RK. Colitis cystica profunda: Review of the litera-
ture. Dis Colon Rectum. 1989;32(11):983–8. 2. Vora IM, Sharma J, Joshi AS. Solitary rectal ulcer syndrome and colitis
cystica profunda. A clinico-pathological review. Indian J Pathol Micro-biol. 1992;35(2):94–102.
3. Hulsmans FJ, Tio TL, Reeders JW, Tytgat GN. Transrectal US in the diagnosis of localized colitis cystica profunda. Radiology. 1991;181(1):201–3.
Figure 3. Hematoxylin and eosin stain section showing transmural dilated glands with mucinous content, surrounded by variable degrees of fibrosis on a background of interspersed chronic inflammatory cells and few colonic mucosal crypts, with mild inflammatory cells infiltrate.

ACG CASE REPORTS JOURNAL
acgcasereports.gi.org ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014124
IMAGE | BILIARY
Hepatobiliary Fascioliasis: An Uncommon Cause of Biliary Obstruction in the United StatesJeff Basile, MD1, M. Stanley Branch, MD1, Svetang V. Desai, MD1, Christopher Arnold, MD2, Alastair Smith, MB, CHB, FRCP1, and Tzu-Hao Lee, MD3
1Division of Gastroenterology, Department of Medicine, Duke University Medical Center, Durham, NC2Division of Infectious Diseases, Department of Medicine, Duke University Medical Center, Durham, NC3Department of Internal Medicine, Duke University Medical Center, Durham, NC
Case ReportA 43-year-old woman presented with recurring upper abdominal pain. She had a 5-year history of symptomatic cholelithiasis without improvement following cholecystectomy. She had no prior history of elevated liver tests or jaundice. Her travel history was pertinent for annual trips to the Bahamas. On admission, the patient had a bilirubin of 4.7 mg/dL and liver enzymes more than 5 times the upper limit of normal. Abdominal computed tomography (CT) scan demonstrated a wedge-shaped area of decreased attenuation in liver segment III (Fig-ure 1). Endoscopic retrograde cholangiopancreatography (ERCP) revealed a curvilinear filling defect within the distal common bile duct (Figure 2). Following papillary sphincterotomy, a living parasite was removed from the common bile duct (Video 1) and confirmed by pathology as Fasciola hepatica (Figure 3). Nitazoxanide was prescribed. Her liver enzymes normalized after 1 week of therapy, and symptoms resolved completely. Magnetic resonance imaging (MRI) 4 months later demonstrated resolution of all imaging abnormalities.
ACG Case Rep J 2014;1(3):124–125. doi:10.14309/crj.2014.24. Published online: April 4, 2014.
Correspondence: Jeffrey Basile, Durham University Medical Center, 3913 Durham, NC, 27710 ([email protected]).
Copyright: © 2014 Basile et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Figure 1. Abdominal CT scan showing a wedge-shaped area of de-creased attenuation in liver segment III.
Figure 2. Rotational fluoroscopic 3-D reconstruction image taken during ERCP showing a curvilinear filling defect in the distal com-mon bile duct (white arrows) secondary to obstruction from Fas-ciola hepatica.
We describe the case of a healthy patient with biliary obstruction caused by hepatobiliary fascioliasis, likely from eating raw vegetables or watercress in a devel-oping area of the Caribbean, where outbreaks of this

Publish your work in ACG Case Reports JournalACG Case Reports Journal is a peer-reviewed, open-access publication that provides GI fellows, private practice clinicians, and other members of the health care team an opportunity to share interesting case reports with their peers and with leaders in the field. Visit http://acgcasereports.gi.org for submission guidelines. Submit your manuscript online at http://mc.manuscriptcentral.com/acgcr.
Basile et al
acgcasereports.gi.org
Hepatobiliary Fascioliasis
125 ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014
trematode have been noted.1,2 Further awareness of fascio-liasis may help facilitate the diagnosis and management of this rare yet treatable cause of hepatobiliary disease in the United States.
References1. Mas-Coma S, Valero MA, Bargues MD. Chapter 2. Fasciola, lymnaeids
and human fascioliasis, with a global overview on disease transmis-sion, epidemiology, evolutionary genetics, molecular epidemiology and control. Adv Parasitol. 2009;69:41–146.
2. Fried B, Graczyk TK, Tamang L. Food-borne intestinal trematodiases in humans. Parasitol Res. 2004;93(2):159–170.
Figure 3. Image of the liver fluke, Fasciola hepatica, captured during ERCP.
Video 1. Video demonstrating removal of Fasciola hepatica from the com-mon bile duct after retrieval balloon sweep during ERCP. Please view the video at http://acgcasereports.gi.org/?p=1944.
Disclosures
Author contributions: All authors contributed equally to the preparation of this manuscript. J. Basile is the article guarantor.
Financial disclosure: The authors report no conflicts of inter-est or financial support for this article.
Informed consent was obtained for this case report.
Received: October 10, 2013; Accepted: January 16, 2014

ACG CASE REPORTS JOURNAL
acgcasereports.gi.org ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014126
CASE REPORT | ENDOSCOPY
A Novel Approach to Management of Esophageal Pill ImpactionBrent W. Lacey, MD, Sean Caufield, MD, Eric Lavery, MD, and Brett Partridge, MD
Naval Medical Center San Diego, San Diego, CA
AbstractA 26-year-old male presented with symptoms of acute esophageal obstruction immediately after swallowing an 800-mg ibuprofen tablet. Multiple attempts to extract the pill with a variety of traditional endoscopic retrieval devices were unsuccessful. We successfully destroyed the pill using a threaded-tip biliary stent retrieval device to drill a hole in the center of the pill, which allowed us to use a rat-tooth forceps to crush the pill. This case report demonstrates a novel use of this device in a challenging esophageal pill extraction.
IntroductionEsophageal foreign body impaction can be managed with a variety of standard endoscopic retrieval devices, but anatomic features and the nature of the foreign body can make successful extraction difficult or impos-sible with standard techniques. We present this case to demonstrate a novel approach to the management of a challenging esophageal pill impaction.
Case ReportA 26-year-old male presented with symptoms of acute esophageal obstruction immediately after swallowing an 800-mg ibuprofen tablet. He could not swallow oral secretions and complained of focal anterior neck pain. During an urgent upper endoscopy, we encountered a circular, hard pill tightly impacted at a mid-esophageal stricture. The esophagus had a narrow caliber and the diagnostic endoscope could only be advanced to a point just proximal to the pill (Figure 1A). Multiple attempts to extract the pill with a variety of traditional endoscopic retrieval devices, including rat-tooth forceps, polypectomy snare, retrieval net, biopsy forceps, and three-pronged grasper, were unsuccessful.
After consideration of management options for refractory esophageal impaction (including surgical referral), we chose to attempt to disrupt the pill with a 7 French threaded-tip Soehendra biliary stent retriever (Cook Medical, Winston-Salem, NC). The stent retriever was centered in the lumen and placed gently against the center of the pill (Figure 1B). Clockwise rotation of the threaded tip created a central defect within the pill matrix (Figure 1C), then we used the rat-tooth forceps to rapidly crush the remaining pill, working off the central defect (Figure 1D). After pulverizing the impacted pill, we observed an esophageal stricture 8 mm in diameter (Figure 2), which we traversed with a narrow caliber (5.5 mm) upper endoscope and completed the examination. The patient recovered unevent-fully. The endoscopic appearance and biopsies of the esophagus were consistent with eosinophilic esophagitis, which subsequently required esophageal dilation for treatment.
DiscussionThe biliary stent retrieval device (Figure 3) has a threaded tip designed to be advanced over a guidewire into a metal biliary stent to facilitate extraction.1 Since its introduction, the device has been used for other purposes, such as expanding a hole in a metallic mesh stent for multiple stenting of a hilar biliary obstruction,2 EUS-guided drainage of a pancreatic pseudocyst,3 dilating refractory pancreatic duct strictures,4 and dilating pancreaticojejunostomy
ACG Case Rep J 2014;1(3):126–127. doi:10.14309/crj.2014.25. Published online: April 4, 2014.
Correspondence: Brent W. Lacey, Naval Medical Center San Diego, 34800 Bob Wilson Dr., San Diego, CA, 92108 ([email protected]).
Copyright: © 2014 Lacey et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

Publish your work in ACG Case Reports JournalACG Case Reports Journal is a peer-reviewed, open-access publication that provides GI fellows, private practice clinicians, and other members of the health care team an opportunity to share interesting case reports with their peers and with leaders in the field. Visit http://acgcasereports.gi.org for submission guidelines. Submit your manuscript online at http://mc.manuscriptcentral.com/acgcr.
Lacey et al
acgcasereports.gi.org
Esophageal Pill Impaction
127 ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014
strictures.5 This is the first published case using the device for management of an esophageal pill impaction. The threaded tip may cut rapidly, so it is important to drill through the pill carefully, checking progress frequently lest the device dam-age the esophageal wall. This device does not use electrocau-tery. Once a hole is created in the center of the pill, standard devices such as the rat-tooth forceps used in this case have the necessary leverage to crush the pill easily.
When encountering an esophageal pill impaction refractory to extraction with standard endoscopic retrieval devices, en-doscopists may consider utilizing a threaded-tip biliary stent retriever. Further studies would be required to determine the efficacy and safety of the stent retriever in the removal of a variety of impacted foreign bodies within the gastrointestinal tract.
Disclosures
Author contributions: BW Lacey was the primary author of the final manuscript and the article guarantor. S. Caufield, E. Lavery, and B. Partridge contributed to and edited the final manuscript.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
Received: February 10, 2014; Accepted: March 16, 2014
References1. Diehl DL, Adler DG, Conway JD, et al; ASGE Technology Committee. En-
doscopic retrieval devices. Gastrointest Endosc. 2009;69(6):997–1003.2. Hara T, Yamaguchi T, Sudo K, et al. Expansion of a metallic mesh stent
hole using a Soehendra stent retriever in multiple stenting of biliary hilar obstruction. Endoscopy. 2008;(suppl 40):E147–8.
3. Yamaguchi T, Ishihara T, Tadenuma H, et al. Use of a Soehendra stent retriever to treat a pancreatic pseudocyst with EUS-guided cystogastros-tomy. Endoscopy. 2004;36(8):755.
4. Ziebert JJ, DiSario JA. Dilation of refractory pancreatic duct strictures: The turn of the screw. Gastrointest Endosc. 1999;49(5):632–5.
5. Partridge BJ, Tokar JL, Kennish J, et al. The endoscopic management of pancreaticojejunostomy strictures. [ASGE Video Forum 2010]. Gas-trointest Endosc. 2010;71(5):AB100–101.
Figure 1. (A) Impacted pill encountered at 25 cm from the incisors. (B) A Soehendra threaded-tip biliary stent retrieval device was used to drill through the pill, (C) yielding a central defect. (D) A rat-tooth forceps was subsequently able to gain sufficient leverage to destroy the pill.
Figure 2. Endoscopic view of the esophageal stricture after destruction of the pill.
Figure 3. Soehendra threaded-tip biliary stent retrieval device. Image cour-tesy of Cook Medical.
A
D
B
C

ACG CASE REPORTS JOURNAL
acgcasereports.gi.org ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014128
CASE REPORT | ENDOSCOPY
Hepatic Portal Venous Gas: An Unusual Complication Following Upper Endoscopy and DilationKristina Seeger, MD1, and Sami R. Achem, MD2
1Department of Internal Medicine, Mayo Clinic, Jacksonville, FL 2Division of Gastroenterology and Hepatology, Mayo Clinic, Jacksonville, FL
AbstractHepatic portal venous gas (HPVG), a rare condition in which gas accumulates in the portal venous circulation, is often associated with a significant underlying pathology, such as intestinal ischemia, sepsis, and trauma. HPVG after endoscopy or dilation is an unusual complication. We report a case of HPVG following upper endoscopy and dilation for an esophageal stricture in a 34-year-old patient with eosinophilic esophagitis (EoE). The patient was treated conservatively, and his symptoms resolved. Follow-up computed tomography (CT) scan showed resolution of HPVG. This case highlights a rare and potentially ominous complication of upper endoscopy and dilation and underscores the role of conservative management.
IntroductionHepatic portal venous gas (HPVG) is a rare condition in which intraluminal gas or gas produced by bacteria in the gut enters the portal venous circulation.1 Common precipitating factors favoring the development of portal venous gas include intestinal wall disruption, bowel distention, and sepsis, which typically suggest an ominous underlying pathology.2 We describe a previously unrecognized cause of HPVG following an upper endoscopy and dilation for a benign esophageal stricture in a young male patient with eosinophilic esophagitis (EoE).
Case ReportA healthy 34-year-old male with a past medical history significant for EoE and asthma presented with unex-plained dysphagia. He underwent esophagogastroduodenoscopy (EGD), which revealed esophageal mucosal changes that were suggestive of EoE, including loss of vascular pattern and white exudates, and a benign esophageal stricture at the gastroesophageal junction. The stricture was dilated with a balloon size of 18 mm. Esophageal biopsies confirmed the diagnosis of EoE.
Within an hour after the procedure, the patient experienced nausea and epigastric pain. His physical exam was remarkable for diffuse epigastric tenderness with no guarding or rigidity. Laboratory tests were normal (complete blood count, liver, and pancreatic enzymes). Abdominal computed tomography (CT) demonstrated diffuse portal venous gas throughout the right hepatic lobe extending to the periphery of the liver (Figure 1). The patient was hospitalized and treated conservatively with intravenous fluids and pain control. He was discharged the following day after his symptoms had resolved. A follow-up repeat CT scan revealed no residual portal vein air. He contin-ued to do well at a 6-month follow-up.
DiscussionHPVG has often been thought of as an ominous clinical finding; it is commonly the result of portomesenteric vein gas accumulation resulting from bowel ischemia.2 Other etiologies associated with HPVG are summarized
ACG Case Rep J 2014;1(3):128–130. doi:10.14309/crj.2014.26. Published online: April 4, 2014.
Correspondence: Sami R. Achem, Division of Gastroenterology, Mayo Clinic, 4500 San Pablo Road South, Jacksonville, FL, 32224 ([email protected]).
Copyright: © 2014 Seeger et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

Hepatic Portal Venous Gas
acgcasereports.gi.org ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014
Seeger et al
129
in Table 1. Only a small fraction of cases are attributed to radiologic and endoscopic procedures. Of these, HPVG has been reported following EGD in patients with a gastric ulcer3 and duodenal tumor,4 after corrosive acid ingestion,5 follow-ing esophageal variceal sclerotherapy and banding,6 after percutaneous endoscopic gastrostomy, and after ERCP.5
HPVG is best diagnosed with CT, where it appears as tubular areas of decreased attenuation in the liver. The low attenu-ation areas are caused by accumulation of gas in the intra-hepatic portal veins, where it is carried by centrifugal blood to the hepatic periphery.2 Due to the high carbon dioxide content of portal venous gas, it is expected to last briefly in the vascular system before it is absorbed or removed by bulk flow, unless gas production persists.7
The mechanism for the formation of HPVG is unclear, but it has been hypothesized that certain factors allow gas to enter the portal circulation through veins or lymphatics of the in-testinal wall and reach the hepatic veins through the hepatic sinusoids.7 These factors may include compromised bowel wall integrity, bowel distention, increased intraluminal pres-sure, and sepsis. Bacterial fermentation of carbohydrates in sepsis may also contribute to the development of HPVG.2
Endoscopic examination of our patient revealed esophageal inflammation with no gross ulcerations. It is possible this underlying esophageal inflammation contributed to com-promised mucosal integrity. The esophageal inflammation coupled with the endoscopic procedure (air insufflation) and esophageal dilation likely facilitated diffusion of intraluminal air across the gastrointestinal mucosa. It has been proposed that endoscopic procedures facilitate diffusion in several
ways. Specifically, shear pressure caused by dilation may compromise mucosal wall integrity, and gastric or lumen dis-tention caused by insufflation may lead to increased intralu-minal pressures, forcing air across the mucosal surface.5,7
The presence of HPVG may convey the notion of a life-threatening complication. However, HPVG is not necessarily an indication for surgical management and may require no treatment.7,8 The underlying etiology and clinical condition of the patient should dictate management. Surgical manage-ment is warranted in clinically unstable patients, or if there is evidence of peritonitis or bowel perforation. Conservative management may be used in clinically stable patients or those who have developed HPVG from an invasive proce-dure.2 Due to the likely iatrogenic-induced HPVG in our pa-tient, he was treated conservatively with fluids and analge-sics, which resolved his symptoms and CT findings.
We describe a case of HPVG following EGD and dilation in a young patient with EoE. Only a handful of cases have men-tioned HPVG following endoscopic procedures, and a large national database from the American Society for Gastroin-testinal Endoscopy does not mention it as a complication
Figure 1. Diffuse portal venous gas throughout the right hepatic lobe extend-ing to the periphery of the liver.
Table 1. Reported Causes of Hepatic Portal Venous Gas
Abdominal Conditions
Mesenteric ischemia4 Necrotizing entercolitisInflammatory bowel diseaseDiverticulitisIntra-abdominal sepsisPneumatosis intestinalisPancreatitisBowel obstructionSuppurative cholangitis5
Bowel necrosisIIleusPeptic ulcer diseaseC. difficle colitisInfectious enteritisGastric cancer1
Ileitis10
Volvulus2
Fecal impaction7
Iatrogenic Corticosteroid therapy11
Endoscopic retrograde cholangiopancreatographyEsophageal variceal bandingPercutaneous endoscopic gastrostomyEndoscopic balloon dilation5
Upper endoscopy3
Air contrast barium enemaEndoscopic ultrasound-guided fine needle biopsySclerotherapyColonoscopy9
Trauma Gastric dilationCaustic ingestion12
Other Liver transplant4
Gynecologic cancer2
Chronic obstructive pulmonary disease11

Publish your work in ACG Case Reports JournalACG Case Reports Journal is a peer-reviewed, open-access publication that provides GI fellows, private practice clinicians, and other members of the health care team an opportunity to share interesting case reports with their peers and with leaders in the field. Visit http://acgcasereports.gi.org for submission guidelines. Submit your manuscript online at http://mc.manuscriptcentral.com/acgcr.
Seeger et al
acgcasereports.gi.org
Hepatic Portal Venous Gas
130 ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014
after EGD or dilation.9 This case illustrates the need to rec-ognize a rare complication following EGD and dilation. In this setting, HPVG can be effectively managed conservatively.
Disclosures
Author contributions: K. Seeger completed the literature search and review, and wrote the manuscript. SR Achem evaluated the patient, designed the study, wrote and edited the manuscript, and is the article guarantor.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
Received: November 21, 2013; Accepted: January 27, 2014
References1. Alqahtani S, Coffin CS, Burak K, et al. Hepatic portal venous gas:
A report of two cases and a review of the epidemiology, pathogen-esis, diagnosis and approach to management. Can J Gastroenterol. 2007;21(5):309–13.
2. Sebastià C, Quiroga S, Espin E, et al. Portomesenteric vein gas: Pathologic mechanisms, CT findings, and prognosis. Radiographics. 2000;20(5):1213–24; discussion 1224–6.
3. Kuo SM, Chang WK, Yu CY, Hsieh CB. Silent hepatic portal venous gas following upper gastrointestinal endoscopy. Endoscopy. 2009;41(sup-pl 2):E121–2.
4. Lamparter S, Goecke W, Koehler HH. Hepatic portal venous gas after upper endoscopy in a patient with a gastrointestinal stromal tumor. J Clin Ultrasound. 2009;37(7):401–2.
5. Lee CG, Kang HW, Song MK, et al. A case of hepatic portal venous gas as a complication of endoscopic balloon dilatation. J Korean Med Sci. 2011;26(8):1108–10.
6. Ahmed K, Atiq M, Richer E, et al. Careful observation of hepatic portal venous gas following esophageal variceal band ligation. Endoscopy. 2008;40(suppl 2):E103.
7. Kesarwani V, Ghelani DR, Reece G. Hepatic portal venous gas: A case report and review of literature. Indian J Crit Care Med. 2009;13(2):99–102.
8. Franken JM, Veen EJ. Hepatic portal venous gas. J Gastrointestin Liver Dis. 2010;19(4):360.
9. Ben-Menachem T, Decker GA, Early DS, et al. ASGE Standards of Practice Committee. Adverse events of upper GI endoscopy. Gastroin-testinal Endosc. 2012;76(4):707–18.
10. Niki M, Shimizu I, Horie T, et al. Hepatic portal venous gas disappear-ing within 24 hours. Internal Med. 2002;41(11):950–2.
11. Abboud B, El Hachem J, Yazbeck T, Doumit C. Hepatic portal venous gas: Physiopathology, etiology, prognosis, and treatment. World J Gas-troenterol. 2009;15(29):3585–90.
12. Bani-Hani KE, Heis HA. Iatrogenic gastric dilatation: A rare and transient cause of hepatic-portal venous gas. Yonsei Med J. 2008;49(4):669–71.

ACG CASE REPORTS JOURNAL
acgcasereports.gi.org ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014131
CASE REPORT | ESOPHAGUS
Acute Esophageal Necrosis: A Case of Black Esophagus Associated with Bismuth Subsalicylate IngestionJean Abed, MD1, Pavan Mankal, MD1, Hani Judeh, MD1, and Sang Kim, MD2
1Department of Medicine, Icahn School of Medicine, Mount Sinai St. Luke’s and Roosevelt Hospitals, New York, NY2Department of Medicine, Division of Gastroenterology, Weill Cornell Medical College, New York, NY
AbstractWe present a case of acute esophageal necrosis (AEN) likely caused by chronic use of bismuth subsalicylate, an active ingredient in over-the-counter Pepto-Bismol®, which contains 220 g of salicylic acid in each 30 mL quan-tity. While aspirin is known to cause gastritis and gastric ulcers, this is the first case, to our knowledge, reporting AEN after chronic bismuth subsalicylate use.
IntroductionAcute esophageal necrosis (AEN), or black esophagus, is a rare entity caused by variety of factors. One theory is that the relatively low perfusion state in the distal areas of the esophagus make it susceptible to mucosal in-jury. We present the first case report of AEN after using large doses of over-the-counter Pepto-Bismol® (bismuth subsalicylate).
Case ReportAn woman in her early 80s with past medical history significant for ulcerative colitis and gastroesophageal reflux (GERD) with use of bismuth subsalicylate was admitted to the hospital for 2 days of constant, diffuse ab-dominal pain with melena. She denied any tobacco, alcohol, illicit drug, or any nonsteroidal anti-inflammatory drug (NSAID) use. On admission, the patient was hemodynamically stable; her physical exam was notable for a slightly distended abdomen with diffuse tenderness to palpation without any rebound or guarding. She had positive guaiac stool with negative stool cultures. Laboratory tests revealed leukocytosis and hemoglobin of 10.1 g/dL (baseline: 14 g/dL). The basic metabolic panel, hepatic function panel, coagulation studies, and urinalysis were all normal.
On the second day of admission, the patient underwent an esophagogastroduodenoscopy (EGD) that revealed an ulcerated and darkened necrotic esophageal mucosa extending continuously from 20 cm beyond the incisors to the gastroesophageal junction (Figure 1). A biopsy revealed extensive necrosis, marked inflammation, and absence of esophageal epithelium consistent with AEN (Figure 2).
The patient reported consuming 40–50 antacids per day for 8–10 years for her acid reflux disease. Total paren-teral nutrition was started and the patient was managed conservatively. A repeat EGD 10 days after admission demonstrated diffuse esophageal edema and pink granulation tissue consistent with healing esophageal mucosa (Figure 3). The patient’s diet was slowly advanced and she was discharged in stable condition 2 weeks after admission.
ACG Case Rep J 2014;1(3):131–133. doi:10.14309/crj.2014.27. Published online: April 4, 2014.
Correspondence: Jean Abed, Department of Medicine, Icahn School of Medicine, Mount Sinai St. Luke’s and Roosevelt Hospitals, 1000 10th Ave, New York, NY 10019 ([email protected]).
Copyright: © 2014 Abed et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

AEN Associated with Bismuth Subsalicylate Ingestion
acgcasereports.gi.org ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014
Abed et al
132
DiscussionAEN, or black esophagus, is a rare clinical entity with an incidence ranging from 0.01% to 0.2% in autopsy studies and clinical trials.1–3 Prior case studies have shown a pre-dilection for AEN in individuals who suffer from cardiovas-cular ischemic events, acute alcohol intoxication, and caustic injury from alkaline compounds, but AEN is thought to be a result of many factors.4–6 The most common presentation is hematemesis and melena, with endoscopy demonstrating friable or macerated mucosa involving the distal two-thirds of the esophagus with a very sharp demarcation at the gas-troesophageal junction.4 The reason for the location may be due to the relatively low perfusion state compared to more proximal areas of the esophagus that are often affected in patients with vasculopathy. Histopathology often shows mu-cosal and submucosal necrosis with heavy leukocyte infiltra-tion, as seen in our patient, though biopsy is not required for diagnosis.7 Management is conservative, but patients re-quire close monitoring due to the risk of complications such as superimposed infections, stenosis, strictures, and perfo-rations. Mortality can reach as high as 32% (often in cases presenting with other comorbidities), but mortality specific to AEN is around 6%.6
The exact etiology of AEN in this case is unclear in the ab-sence of vascular disease. AEN in this patient might be sec-ondary to the chronic ingestion of a large dose of antacids (i.e., bismuth subsalicylate) causing chemical injury and ne-crosis. Bismuth subsalicylate, an active ingredient in over-
Figure 1. Endoscopy performed at the time of admission shows an ulcerated and necrotic esophageal mucosa starting 20 cm beyond the incisors to the gastroesophageal junction with normal gastric mucosa.
Figure 2. Endoscopic biopsy demonstrates an ulcerated esophageal mu-cosa with complete absence of the epithelium and replacement by a fi-brinopurulent exudate characteristic of ulcerative lesions. The underlying mucosa shows increased inflammation and vascularity.
Figure 3. Repeat endoscopy 10 days after admission shows diffuse esopha-geal edema, mild friability, and pink granulation tissue consistent with re-solving esophagitis.
the-counter Pepto-Bismol®, is used widely to treat symptom-atic inflammation of gastric and intestinal epithelium. The reactivity of bismuth with sulfur molecules ingested from food can lead to linguinal hyperpigmentation (black tongue),

Publish your work in ACG Case Reports JournalACG Case Reports Journal is a peer-reviewed, open-access publication that provides GI fellows, private practice clinicians, and other members of the health care team an opportunity to share interesting case reports with their peers and with leaders in the field. Visit http://acgcasereports.gi.org for submission guidelines. Submit your manuscript online at http://mc.manuscriptcentral.com/acgcr.
Abed et al
acgcasereports.gi.org
AEN Associated with Bismuth Subsalicylate Ingestion
133 ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014
which is often benign and reversible with medication dis-continuation.8 The high doses of an alkalizing medication such as bismuth subsalicylate, which contains 220 g of sali-cylic acid per 30 mL quantity, may have caused chemical injury to the esophageal epithelium to develop even without the use of other NSAIDs. The chemical reaction between bismuth and sulfur may have created the dark pigmenta-tion of the esophagus classic to AEN.9 To our knowledge, no other case report has reported a black esophagus after pro-longed, heavy use of over-the-counter bismuth subsalicylate with rapid recovery after the discontinuation of the causative agent.
Disclosures
Author contributions: J. Abed and P. Mankal wrote the man-uscript. H. Judeh and S. Kim provided the case history and photographs. S. Kim is the article guarantor.
Financial disclosure: No conflicts of interest or financial dis-closures to report.
The patient consented in writing to all procedures. The au-thors made every effort to contact the patient and her next of kin, but due to the length of time between the case and this report, neither the patient nor the next of kin could be reached for consent to publish. However, the authors feel that the patient information is sufficiently anonymous and that the patient would not object to this publication.
Received: December 10, 2013; Accepted: February 20, 2014
References1. Postlethwait RW, Musser AW. Changes in the esophagus in 1,000 au-
topsy specimens. J Thorac Cardiovasc Surg. 1974;68(6):953–6.2. Ben Soussan E, Savoye G, Hochain P, et al. Acute esophageal necrosis:
A 1-year prospective study. Gastrointest Endosc. 2002;56(2):213–7.3. Lacy BE, Toor A, Bensen SP, et al. Acute esophageal necrosis: Report of
two cases and a review of the literature. Gastrointest Endosc. 1999;49(4 pt 1):527–32.
4. Neumann DA, 2nd, Francis DL, Baron TH. Proximal black esopha-gus: A case report and review of the literature. Gastrointest Endosc. 2009;70(1):180–1.
5. Cappell MS. Esophageal necrosis and perforation associated with the anti-cardiolipin antibody syndrome. Am J Gastroenterol. 1994;89(8):1241–5.
6. Gurvits GE. Black esophagus: Acute esophageal necrosis syndrome. World J Gastroenterol. 2010;16(26):3219–25.
7. Rejchrt S, Douda T, Kopacova M, et al. Acute esophageal necrosis (black esophagus): Endoscopic and histopathologic appearance. En-doscopy. 2004;36(12):1133.
8. Cohen PR. Black tongue secondary to bismuth subsalicylate: Case re-port and review of exogenous causes of macular lingual pigmentation. J Drugs Dermatol. 2009;8(12):1132–5.
9. Sugawa C, Takekuma Y, Lucas CE, Amamoto H. Bleeding esophageal ulcers caused by NSAIDs. Surg Endosc. 1997;11(2):143–6.

ACG CASE REPORTS JOURNAL
acgcasereports.gi.org ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014134
CASE REPORT | ESOPHAGUS
A Treatment Option for Esophageal Intramural PseudodiverticulosisAmy Tyberg, MD, and Daniela Jodorkovsky, MD
Division of Gastrointestinal and Hepatobiliary Diseases, New York Medical College, Westchester Medical Center, Valhalla, NY
AbstractEsophageal intramural pseudodiverticulosis (EIPD) is a rare condition often presenting with esophageal stric-tures. Treatment is often limited to endoscopic dilatation and treatment of the underlying esophageal pathology. We present a case of a patient with longstanding GERD on famotidine (she experienced anaphylaxis with proton pump inhibitors [PPIs]) who presented with dysphagia and weight loss. Work-up revealed a diagnosis of EIPD with a 5-mm mid-esophageal stricture. Therapy with dilatation was unsuccessful until the addition of sucralfate, after which dilatation was successful and symptoms resolved. In patients who are unable to take PPIs, the addi-tion of sucralfate may enhance the success of dilatations of esophageal strictures and EIPD.
IntroductionEsophageal intramural pseudodiverticulosis (EIPD) is a rare condition of unclear pathogenesis that was first described in 1960.1 Since then and through 2011, only about 200 cases have been reported worldwide.2 The true incidence of EIPD is unknown, though in a retrospective review of esophageal radiograms from 1986, EIPD was found to have a prevalence of approximately 0.15%.3 The primary symptom of this condition is dysphagia, usually due to the presence of an esophageal stricture that often accompanies diagnosis.4,5 Associated condi-tions reported in the literature include diabetes, alcoholism, gastroesophageal reflux disease (GERD), fungal in-fections, and esophageal neoplasms.4,5 Dysmotility disorders are occasionally associated with EIPD, including 2 reported cases of achalasia and 1 case of nutcracker esophagus,6,7 though no causal relationship has been elu-cidated.8 Treatment is often limited to endoscopic dilatation and treatment of the underlying esophageal condi-tion, such as acid suppression therapy or treatment of fungal infections.4,5,9–11 In rare cases, esophagectomy has been required.12 We present a case of a patient with EIPD managed successfully with dilatation and sucralfate.
Case ReportA 58-year-old female was admitted to the hospital with several months of progressive dysphagia and a 20-lb weight loss. Her medical history was significant for GERD, for which she was only prescribed famotidine due to a prior anaphylactic allergy to proton pump inhibitors (PPIs). A barium esophagram showed a smooth mid-esophageal stricture and several intramural diverticula and intramural tracts distal to the stricture (Figure 1).
An esophagogastroduodenoscopy (EGD) was done to examine the stricture. The luminal diameter was approxi-mately 5 mm, and length was 6 mm. There was no desquamation, ulceration, or furrowing of the mucosa. The stricture could only be traversed with an XP 180 endoscope. Distal to the stricture, the esophagus was found to have innumerable shallow depressions (Figure 2). Multiple biopsies were taken from within and adjacent to the stricture. Pathology showed histologic evidence of esophagitis with neutrophils and lymphocytes, and rare
ACG Case Rep J 2014;1(3):134–136. doi:10.14309/crj.2014.28. Published online: April 4, 2014.
Correspondence: Amy Tyberg, New York Medical College, Gastrointestinal and Hepatobiliary Diseases, Munger Pavilion Suite 206, Valhalla, NY, 10595 ([email protected]).
Copyright: © 2014 Tyberg et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

Esophageal Intramural Pseudodiverticulosis
acgcasereports.gi.org ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014
Tyberg et al
135
Figure 1. Barium swallow showing intramural diverticula and intramural tracts.
eosinophils without evidence of malignancy or an alternative diagnosis. The patient was diagnosed with EIPD.
A series of near-weekly balloon dilatations were performed with minimal success. The first dilatation session used a 6-mm, followed by a 7.5-mm, through-the-scope (TTS) bal-loon. Ten days later, bougie dilatation was performed using a 27 French dilator, and moderate force was required. A TTS balloon was then used to dilate from 9 mm to 10 mm. Two weeks later, the stricture was still unable to be traversed with a GIF-160, and the diameter was estimated to have re-turned back to 8 mm. A TTS balloon was used to dilate from 8 mm to 12 mm. The fourth dilatation session showed that the stricture still could not be traversed; the diameter had narrowed again. A TTS balloon was used to dilate from 12 mm to 14 mm.
The patient was then prescribed sucralfate suspension 4 times daily. The next dilatation started with a 12-mm bal-loon, and the stricture was dilated to 15 mm. Dysphagia symptoms largely resolved at this time, though the patient noted on follow-up that she had to be “very careful” eating solid food and chased all oral intake with liquid. One final
dilatation session was performed 1 month later. The stricture could be easily traversed with a GIF-160, and the luminal diameter was estimated to be 12 mm. The stricture was di-lated with a 15–18-mm controlled radial expansion (CRE) balloon. After these dilatations, the patient’s dysphagia com-pletely resolved, and she has since gained 21 lbs. She has not required further dilation at 1 year follow-up.
DiscussionEIPD is a rare disorder with an unclear pathogenesis. It is often associated with esophageal strictures, and therapy consists mainly of endoscopic dilatation. There have been no reports of the use of esophageal stents for the treatment of EIPD in the literature. EIPD can be associated with other conditions, the most common of which are GERD and fun-gal infections. Treatment of these other underlying condi-tions, such as acid suppression in the setting of GERD, is often required. In patients who are unable to tolerate stan-dard acid suppression therapy with proton-pump inhibitors (PPIs), the addition of sucralfate may enhance the success of dilatations of esophageal strictures, as our case illustrates. A recent Cochrane review showed sucralfate to be associ-ated with a trend towards esophagitis healing in the setting of GERD, though the effect was modest and not statistically significant.13 Sucralfate functions by forming a physical bar-rier between esophageal mucosa and harmful agents, pro-moting mucosal healing, and decreasing the inflammatory response.14 All of these mechanisms may explain its benefi-cial role in this case. Regardless of the mechanism, this case suggests that in patients with EIPD and stricture formation who are unable to tolerate PPI therapy, sucralfate may be a viable alternative.
Disclosures Author contributions: A. Tyberg collected data, wrote the manuscript, and is the article guarantor. D. Jodorkovsky ed-ited the manuscript.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
Received: November 20, 2013; Accepted: March 18, 2014
Figure 2. EGD showing esophagus with innumerable shallow depressions.

Publish your work in ACG Case Reports JournalACG Case Reports Journal is a peer-reviewed, open-access publication that provides GI fellows, private practice clinicians, and other members of the health care team an opportunity to share interesting case reports with their peers and with leaders in the field. Visit http://acgcasereports.gi.org for submission guidelines. Submit your manuscript online at http://mc.manuscriptcentral.com/acgcr.
Tyberg et al
acgcasereports.gi.org
Esophageal Intramural Pseudodiverticulosis
136 ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014
References1. Mendl K, McKay JM, Tanner CH. Intramural diverticulosis of the esoph-
agus and Rokitansky-Aschoff sinuses in the gallbladder. Br J Radiol. 1960;33(392):496–501.
2. Hahne M, Schilling D, Arnold JC, Riemann JF. Esophageal intramural pseudodiverticulosis: Review of symptoms including upper gastrointes-tinal bleeding. J Clin Gastroenterol. 2001;33(5):378–82.
3. Levine MS, Moolten DN, Herlinger H, Lauger I. Esopheal intra-mural pseudodiverticulosis: A reevaluation. Am J Roentgenol. 1986;147(6):1165–70.
4. Brühlmann WF, Zollikofer CL, Maranta E, et al. Intramural pseudodiver-ticulosis of the esophagus: Report of seven cases and literature review. Gastrointest Radiol. 1981;6(3):199–208.
5. Umlas J, Sakhuja R. The pathology of esophageal intramural pseudodi-verticulosis. Am J Clin Pathol. 1976;65(3):314–20.
6. Turan I, Ozen E, Bor S, Ozutemiz O. Esophageal intramural pseudodi-verticulosis associated with achalasia: An unusual endoscopic appear-ance. Endoscopy. 2009;41(suppl 2):E23–E24.
7. Walker S, Hippéli R, Goës R. Diffuse esophageal intramural pseudo-diverticulosis and nutcracker esophagus in a 54-year-old man. Klin Wochenschr. 1990;68(3):187–90.
8. Sabanathan S, Salama FD, Morgan WE. Oesophageal intramural pseu-dodiverticulosis. Thorax. 1985;40(11):849–57.
9. Chiba T, Iijima K, Koike T, et al. A case of severe esophageal intra-mural pseudodiverticulosis whose symptoms were ameliorated by oral administration of anti-fungal medicine. Case Rep in Gastroenterol. 2012;6:103–110.
10. Attila T, Marcon NE. Esopahgeal intramural pseudodiverticulosis with food impaction. Can J Gastroenterol. 2006;20(1):37–38.
11. Chon YE, Hwang S, Jung KS, et al. A case of esophageal intramural pseudodiverticulosis. Gut Liver. 2011;5(1):93–5.
12. Liu SM, Wu HH, Chang KK, et al. Esophageal intramural pseu-dodiverticulosis complicated with stricture. J Formos Med Assoc. 2010;109(3):241–4.
13. Khan M, Santana J, Donnellan C, et al. Medical treatments in the short term management of reflux oesophagitis. Cochrane Database Syst Rev. 2007;2:CD003244.
14. Gümürdülü Y, Karakoc E, Kara B, et al. The efficiency of sucralfate in corrosive esophagitis: A randomized, prospective study. Turk J Gastro-enterol. 2010;21(1):7–11.

ACG CASE REPORTS JOURNAL
acgcasereports.gi.org ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014137
CASE REPORT | STOMACH
Glass Microparticulate Ingestion: An Unusual and Difficult-to-Diagnose Cause of Chronic Abdominal PainR. Brooks Vance, MD1, Marcus Mühlbauer, MD, PhD1, Elizabeth B. Dreesen, MD2, C. Robert Bagnell, Jr., PhD3, Georgette A. Dent, MD3, Hans Herfarth, MD, PhD1, Christian Jobin, PhD1, and Evan S. Dellon, MD, MPH1
1Center for Gastrointestinal Biology and Disease, Division of Gastroenterology and Hepatology, Department of Medicine, University of North Carolina School of Medicine, Chapel Hill, NC2Department of Surgery, University of North Carolina School of Medicine, Chapel Hill, NC 3Department of Pathology and Laboratory Medicine, University of North Carolina School of Medicine, Chapel Hill, NC
AbstractIn the absence of overt structural abnormalities, the diagnostic approach to chronic abdominal pain can be challenging. Occupational particulate inhalation causing injury to an organ other than the lung is rare. We report a case of inadvertent glass microparticulate ingestion causing chronic abdominal pain with altered local and systemic inflammatory responses.
IntroductionOccupational particulate inhalation causing injury in an organ other than the lung is rare, and when present, can be difficult to diagnose.1,2 We report a case of inadvertent glass microparticulate ingestion causing chronic ab-dominal pain with altered local and systemic inflammatory responses. We also describe the specialized etiologic evaluation, including x-ray microanalysis, immunohistochemistry, and peripheral blood assays, that were used to confirm the diagnosis, and suggest that altered local and systemic inflammatory response might be responsible.
Case ReportThe patient is a previously healthy 38-year-old man who developed chronic recurrent abdominal pain after start-ing work as a manager at a glass-cutting factory. He was present on the factory floor while glass was being cut, ground, and smoothed, and did not routinely use protective gear. The abdominal pain was episodic, periumbili-cal, lasted several days, and would resolve spontaneously. He was asymptomatic between episodes.
Physical exam was unremarkable both during and between pain episodes. An extensive laboratory work-up revealed only a mildly elevated C-reactive protein. Blood counts, electrolytes, liver and kidney function, thyroid tests, and iron studies were normal. Blood cultures were negative. Testing for HIV, C1 esterase, complement levels, porphyrins, heavy metals, and paroxysmal nocturnal hemoglobinuria was unrevealing. Upper endoscopy, colonoscopy, and capsule endoscopy were non-diagnostic. Abdominal CT during a pain flare showed mild thickening in the appendix and mesenteric stranding with sub-centimeter lymph nodes. Diagnostic laparoscopy revealed vermiform-appearing adhesions on the abdominal wall (Figure 1). Mesenteric biopsy showed chronic inflammation with evidence of foreign body reaction (Figure 2).
ACG Case Rep J 2014;1(3):137–139. doi:10.14309/crj.2014.29. Published online: April 4, 2014.
Correspondence: Evan S. Dellon, CB# 7080, Bioinformatics Building, 130 Mason Farm Rd., UNC-CH, Chapel Hill, NC, 27599-7080 ([email protected]).
Copyright: © 2014 Vance et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

Glass Microparticulate Ingestion
acgcasereports.gi.org ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014
Vance et al
138
To investigate these histopathologic findings in more detail, specialized testing was performed. X-ray microanalysis re-vealed the presence of silicon (Figure 3), silver chloride, tung-sten, titanium, and vanadium, which are metals commonly used in glass manufacturing. On immunohistochemistry, there was scant staining for IL-1ß. Lipopolysaccharide (LPS)-induced IL-1ß protein secretion was also significantly lowered in this patient compared to healthy controls (Figure 4).
On clinical follow-up of 3 years, exposure avoidance with a respirator mask at work led to significant symptom improve-ment, and lapses in exposure avoidance led to recurrent symptoms.
DiscussionOccupational particulate ingestion causing inhalational lung injury is well reported. However, particulate involvement of other organ systems is rare, and the clinical significance of such exposures is not well understood.1,2 The inflammatory
response and cellular changes generated by foreign body reaction have been recently reported for inhalational expo-sures in coal miners, ship-builders, and glass manufactur-ers.3–6 Ferrira et al described a glass laminator with inflam-matory lung granulomas consisting of silica-predominant particulate.7 However, only 1 report has described similar exposures involving the GI tract in “glass dust esophagitis” in a glass grinder who presented with chest pain.8
Dysfunction of the intestinal inflammasome, particularly with altered levels of cytokines such as IL-1ß, may contribute to many gastrointestinal conditions, including inflammatory bowel disease, colon cancer, and functional bowel disor-ders.9 In our patient, we detected a number of mesenteric glass microparticulates suggestive of inadvertent ingestion and subsequent microperforation. We also found lower IL-1ß levels locally in mesenteric tissue and systemically with blunted IL-1ß secretion after LPS stimulation. There is evi-dence that silica can suppress murine macrophage produc-
Figure 1. Intraoperative laparoscopic image showing unusual-appearing vermiform lesions in the right lateral abdominal sidewall with thin adherent omentum.
Figure 2. Histopathologic findings on examination of mesenteric biopsy speci-mens (40x). (A) Hematoxylin and eosin stain showing papillary mesothelial hy-perplasia with the presence of a refractile foreign body (arrow). (B) The foreign body material is clearly illustrated when viewed under polarized light.
Figure 3. Results of specialized testing with x-ray microanalyses. (A) High levels of silicon are demonstrated in the x-ray microanalysis from the biopsy specimen. The energy applied, measured in keV, is on the x axis, and the resulting counts are on the y axis. (B) An electron microscopy image of the silicon foreign body.
A B
A
B

Publish your work in ACG Case Reports JournalACG Case Reports Journal is a peer-reviewed, open-access publication that provides GI fellows, private practice clinicians, and other members of the health care team an opportunity to share interesting case reports with their peers and with leaders in the field. Visit http://acgcasereports.gi.org for submission guidelines. Submit your manuscript online at http://mc.manuscriptcentral.com/acgcr.
Vance et al
acgcasereports.gi.org
Glass Microparticulate Ingestion
139 ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014
tion of the pro-inflammatory cytokines IL-1 and IL-6,3 and this mechanism provides a possible explanation for our find-ings. IL-1ß receptors are now therapeutic targets for novel immunomodulatory medications such as anakinra, an IL-1ß receptor antagonist.10,11 A side effect of this medication is chronic abdominal pain; in theory, excess inhibition resulting in reduced IL-1ß levels may contribute to abdominal pain.
We hypothesize that inadvertent glass microparticulate in-gestion and microperforation led to a silica-induced impair-ment of IL-1ß secretion and subsequent chronic inflamma-tion and pain. It is important to consider occupational expo-sures in patients with unexplained chronic gastrointestinal complaints that do not fit with symptom patterns in other established disorders.
Disclosures
Author contributions: RB Vance collected and interpreted data, and drafted, critically revised, and approved the manu-script. M. Mühlbauer collected, interpreted, and analyzed data, and critically revised and approved the manuscript. EB Dreesen provided patient care and critically revised and approved the manuscript. CR Bagnell and GA Dent pro-vided pathologic analysis and interpretation, and critically revised and approved the manuscript. H. Herfarth and C. Jobin designed the study, interpreted data, and critically re-
vised and approved the manuscript. ES Dellon designed the study, provided patient care, collected and interpreted data, drafted, critically revised, and approved the manuscript, and is the article guarantor.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
Previous Presentation: This paper was presented as a poster at the 2012 ACG Annual Meeting.
Received: January 20, 2014; Accepted: March 4, 2014
References1. Gerhardsson de Verdier M, Plato N, Steineck G, Peters JM. Occupa-
tional exposures and cancer of the colon and rectum. Am J Ind Med. 1992;22(3):291–303.
2. Bunderson-Schelvan M, Pfau JC, Crouch R, Holian A. Nonpulmonary outcomes of asbestos exposure. J of Toxicol Environ Health B Crit Rev. 2011;14(1–4):122–52.
3. Hwang M, Park KK, Chang YC, et al. Silica-ceramic suppresses the ex-pression of pro-inflammatory cytokines induced by lipopolysaccharide macrophages. J Biomed Mater Res A. 2007;80(3):513–9.
4. Castranova, V, Vallyathan V. Silicosis and coal workers’ pneumoconiosis. Environ Health Perspect. 2000;108(suppl 4):675–84.
5. Hedly-Whyte J, Milamed DR. Asbestos and ship-building: Fatal conse-quences. Ulster Med J. 2008;77(3):191–200.
6. Ji X, Hou Z, Wang T, et al. Polymorphisms in inflammasome genes and risk of workers’ pneumoconiosis in a Chinese population. PLoS One. 2012;7(10):e47949.
7. Ferriera AS, Moreira VB, Castro MC, et al. Case report: Analytical elec-tron microscopy of lung granulomas associated with exposure to coat-ing materials carried by glass wool fibers. Environ Health Perspect. 2010;118(2):249–52.
8. Park HS, Han DS, Bae JH. Glass dust esophagitis: An unusual cause of chest pain. Gastrointest Endosc. 2012;75(3):668.
9. Chen GY, Núñez G. Inflammasomes in intestinal inflammation and can-cer. Gastroenterology. 2011;141(6):1986–99.
10. Marchand F, Perreti M, McMahon SB. Role of the immune system in chronic pain. Nat Rev Neurosci. 2005;6(7):521–32.
11. McDermott MF. Rilonacept in the treatment of chronic inflammatory disorders. Drugs Today (Barc). 2009;45(6):423–30.
Figure 4. White blood cells from the patient display impaired LPS-induced IL-1ß protein secretion compared to healthy controls (n=3). Error bars rep-resent the standard deviation of the measurements (each experiment was performed in triplicate for each of the samples).

ACG CASE REPORTS JOURNAL
acgcasereports.gi.org ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014140
CASE REPORT | SMALL BOWEL
Hemophagocytic Lymphohistiocytic Syndrome and Enteropathy-Associated T-cell Lymphoma in a Patient with Refractory Celiac DiseaseLucy Lu, MD1, Shuoyan Ning, MD1, Zain Kassam, MD2, Richard Hunt, MB, MACG3, and Marco Puglia, MD3
1Department of Medicine, McMaster University, Hamilton, Ontario, Canada2Harvard School of Public Health, Harvard University, Boston, MA3Division of Gastroenterology, McMaster University, Hamilton, Ontario, Canada
AbstractA 70-year-old woman with celiac disease presented with weight loss and diarrhea unresponsive to gluten-free diet (GFD) and prednisone. Diagnosis of type 2 refractory celiac disease (RCD) was made by small intestinal biop-sies showing severe villous blunting and intraepithelial lymphocytosis. She was diagnosed with hemophagocytic lymphohistiocytic syndrome (HLH) after developing fever, pancytopenia, hypofibrinogenemia, elevated ferritin, and demonstration of hemophagocytosis on her bone marrow biopsy. An expert pathologist on lymphoma reviewed her biopsies and revised the final diagnosis to type 1 enteropathy-associated T-cell lymphoma (EATL) based on large T-cells infiltrating the lamina propria. We describe the first case of HLH associated with localized EATL and RCD.
IntroductionHemophagocytic lymphohistiocytic syndrome (HLH) is a rare, rapidly progressive and potentially fatal syndrome characterized by overactive histiocytes. HLH has been described in advanced enteropathy-associated T-cell lym-phoma (EATL), a type of non-Hodgkin’s T-cell lymphoma associated with celiac disease. We report the first case of HLH associated with localized EATL in the context of refractory celiac disease (RCD).
Case ReportA 70-year-old woman with a 4-year history of celiac disease was referred for RCD unresponsive to strict gluten-free diet (GFD) and 1 month of treatment with prednisone. She initially presented with a 25-lb weight loss over 4 months, non-bloody diarrhea, and abdominal bloating, and had been diagnosed via duodenal biopsies showing villous atro-phy. Since then, she had followed a strict GFD.
Prior to referral, she had negative evaluations for metabolic and infectious causes of diarrhea. Her blood work showed increased anti-tissue transglutaminase IgA, antigliadin antibody IgG, and antigliadin IgA, with normal total IgA levels. An abdominal computed tomography (CT) showed inflammation in the small bowel with loss of the nor-mal jejunal mucosa. Five days into her admission, she developed melena; esophagogastroduodenoscopie (EGD), colonoscopy, and push enteroscopy did not identify a source of bleeding. She was diagnosed with type 2 RCD based on duodenal and jejunal biopsies, which demonstrated severe villous blunting, intraepithelial lymphocytosis, and lymphoplasmacytic infiltration. Her diarrhea persisted despite a strict GFD and prednisone. Cyclosporine 60 mg IV was started but discontinued due to drug-related fever. She was treated empirically with piperacillin/tazobactam and transferred to our center.
ACG Case Rep J 2014;1(3):140–142. doi:10.14309/crj.2014.30. Published online: April 4, 2014.
Correspondence: Lucy Lu, McMaster University – Medicine, 1280 Main Street West Health Sciences Centre, 2F51, Hamilton, Ontario, L8N 3Z5, Canada ([email protected]).
Copyright: © 2014 Lu et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

Hemophagocytic Lymphohistiocytic Syndrome
acgcasereports.gi.org ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014
Lu et al
141
On referral, the patient was cachectic, tachycardic, and hy-potensive with evidence of ongoing gastrointestinal bleeding. A repeat abdominal CT showed no small bowel abnormality, hepatosplenomegaly, or lymphadenopathy. HLH was suspect-ed after the patient developed pancytopenia, hypofibrinogen-emia, elevated liver enzymes, and hyperferritinemia (19,574 ug/L; normal: 51–400 ug/L) in the context of ongoing fever. Bone marrow biopsy confirmed the diagnosis, revealing prom-inent hemophagocytosis (Figure 1). An HLH treatment pro-tocol was initiated with dexamethasone 10 mg IV twice daily, cyclosporine 100 mg IV twice daily, anakinra 100 mg subcu-taneously daily, 1 dose of etoposide 100 mg IV, and intrave-nous immunoglobulin (IVIG), along with transfusions of blood products. She was unresponsive to treatment and remained pancytopenic while her ferritin increased to 60,552 ug/L.
Persistent diarrhea and GI bleeding were suspicious for a small bowel EATL. A pathologist experienced in lymphoma reviewed her previous small intestinal biopsies and revised the final di-agnosis to include type 1 EATL based on the high proportion of
large T-cells with prominent nucleoli infiltrating the lamina pro-pria and the abnormal T-cell marker profile (Figure 2). Unfor-tunately, on the day of the diagnosis, the patient passed away from a small intestinal bleeding.
DiscussionWe describe a rare case of EATL-associated with RCD and subsequent development of HLH, of which there are very few reported cases.1,2 RCD is a diagnosis of exclusion defined by ongoing symptoms and persistent villous atrophy despite a strict GFD for 1 year.3 RCD is classified into type 1 (normal intraepithelial lymphocyte morphology) and type 2 (abnormal intraepithelial lymphocyte morphology).3 Type 2 RCD, often di-agnosed in elderly women, is more commonly associated with serious complications, with 60–80% of patients developing EATL within 5 years.3 It carries a 5-year survival rate of 40–58%.4 HLA-DQ2 haplotype is present in up to 98% of cases.5
EATL is a rare form of non-Hodgkin’s T-cell lymphoma that is associated with celiac disease in up to 70% of cases.6 EATL usually develops in the jejunum or ileum, but can arise in any part of the gastrointestinal tract. Two types of EATL exist. Type 1 EATL is strongly linked to celiac disease and RCD7 and is characterized by large cells or non-monomorphic cytology with negative CD56 and positive CD30 T-cell marker expression. Type 2 EATL has a monomorphic cytology with CD56 expres-sion. The prognosis of EATL is poor. Median progression-free survival ranges between 3 and 6 months, with 5-year progres-sion-free survival of 3.2–18%.8 Mortality typically results from perforation, bleeding, and malabsorption.
EATL may not be identified on standard imaging. CT enterocly-sis may detect tumors as small as 5 mm, with sensitivity and specificity of 95–100%.9 Positron emission tomography (PET) scans may be more sensitive than CT for detecting EATL, but experience with magnetic resonance imaging (MRI) for diag-nosing EATL is limited.10 Validated magnetic resonance (MR) enteroclysis scores have been developed for identification of type 2 RCD and CD-related small bowel non-Hodgkin’s lym-phoma (NHL). The presence of less than 10 folds per 5 cm of jejunum, mesenteric fat infiltration, and bowel wall thickening are associated with type 2 RCD.11,12 The diagnosis of EATL re-lies primarily on histology. Treatment options for EATL include surgical resection and anthracycline-based chemotherapy with modest survival benefits.8 Emerging therapies utilizing high-dose induction chemotherapy and autologous stem cell transplantation have demonstrated improved survival.8,11
HLH is characterized by the activation, proliferation, and ab-normal function of histocytes.12 It requires at least 5 of the fol-lowing 8 criteria: fever, splenomegaly, peripheral cytopenia of 2 lineages, hypertriglyceridemia and/or hypofibrinogenemia, hyperferritinemia, elevated soluble CD25, absent natural killer cell activity, and histological hemophagocytosis in the bone marrow, lymph nodes, or spleen.13 Primary HLH is an auto-somal recessive genetic disorder.12 Secondary HLH is associ-
Figure 1. Bone marrow biopsy showing digested red blood cell debris in cytoplasm of macrophages as indicated by the arrows (200x power).
Figure 2. Endoscopic small intestinal biospy showing prominent infiltration of epithelium and lamina propria by medium-to-large mononuclear cells (20x power).

Publish your work in ACG Case Reports JournalACG Case Reports Journal is a peer-reviewed, open-access publication that provides GI fellows, private practice clinicians, and other members of the health care team an opportunity to share interesting case reports with their peers and with leaders in the field. Visit http://acgcasereports.gi.org for submission guidelines. Submit your manuscript online at http://mc.manuscriptcentral.com/acgcr.
Lu et al
acgcasereports.gi.org
Hemophagocytic Lymphohistiocytic Syndrome
142 ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014
ated with disorders that induce immune overactivation, such as viral infections, autoimmune diseases, or malignancies. In acquired HLH, the course is rapidly progressive with multi-organ dysfunction within weeks. Treatment includes addressing the underlying cause and chemotherapy with etoposide, high-dose corticosteroids, and cyclosporine A.12,14 Early administration of etoposide (<4 weeks from onset) has demonstrated improved survival in Epstein-Barr virus–associ-ated HLH.14,15 IVIG has helped to decrease HLH inflammatory response.14 Anakinra has shown limited success as a salvage therapy.16 Malignancy-associated HLH is rare, and no specific recommendation has been made regarding its treatment. In case reports of EATL-associated HLH, none of the patients re-ceived HLH-specific therapy.
There is no published case report of RCD associated with HLH. Only 7 cases have been reported of EATL-associated HLH, of which all patients had metastatic EATL before development of HLH and died within 3 months.1 Our patient rapidly declined after developing HLH and died shortly after a confirmed diag-nosis of HLH. This is the first case of EATL-associated HLH treated with HLH-specific therapy. Since vinblastine resulted in temporary im-provement in a previous case report,1 perhaps these patients should be treated more aggressively for their underlying EATL as opposed to HLH-directed therapy. Our patient did not re-ceive EATL-specific therapy because the diagnosis of EATL was delayed. Our case demonstrates that HLH can develop with RCD and early-stage EATL. Gastroenterologists should con-sider screening patients with RCD and EATL for HLH. Prompt referral is crucial for early diagnosis and treatment of EATL and HLH. When suspicion is high and EATL is not apparent on standard imaging, clinicians should remember that EATL requires histological diagnosis by an experienced pathologist.
Disclosures
Author contributions: L. Lu and S. Ning drafted the man-uscript. Z. Kassam, R. Hunt, and M. Puglia reviewed and edited the manuscript. All authors approved the final manu-script. M. Puglia is the article guarantor.
Acknowledgements: Dr. Denis Bailey and Dr. Catherine Ross for providing the pathology slides and assisting in their inter-pretation.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
Received: July 21, 2013; Accepted: March 21, 2014
References1. Amiot A, Allez M, Treton X, et al. High frequency of fatal haemophago-
cytic lymphohistiocytosis syndrome in enteropathy-associated T cell lym-phoma. Dig Liver Dis. 2012;44(4):343–9.
2. Mainwaring CJ, James CM, Pidgeon S, Webb S. Reactive haemo-phagocytosis as a consequence of gluten enteropathy associated in-testinal non-Hodgkin’s lymphoma with fatal outcome. Br J Haematol. 2011;114(2):248.
3. Rubio-Tapia A, Murray JA. Classification and management of refractory coeliac disease. Gut. 2010;59(4):547–57.
4. Al-Toma A, Verbeek WH, Hadithi M, et al. Survival in refractory coeliac disease and enteropathy-associated T-cell lymphoma: Retrospective evaluation of single-centre experience. Gut. 2007;56(10):1373–8.
5. Malamut G, Afchain P, Verkarre V, et al. Presentation and long term follow-up of refractory celiac disease: Comparison of type I and type II. Gastroenterology. 2009;136(1):81–90.
6. Catassi C, Bearzi I, Holmes GK. Association of celiac disease and intes-tinal lymphomas and other cancers. Gastroenterology. 2005;128(suppl 1):S79–86.
7. Isaacson PG, Chott A, Ott G, Stein H. Enteropathy-associated T-cell lym-phoma. In: Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, Thiele J, Vardiman JW, eds. WHO Classification of Tumours of Hae-matopoietic and Lymphoid Tissues. 4th ed. Lyon, France: IARC Press; 2008:289–91.
8. Sieniawski MK, Lennard AL. Enteropathy-associated T cell lymphoma: Epidemiology, clinical features, and current treatment strategies. Curr Hematol Malig Rep. 2011;6:231–40.
9. Boudiaf M, Jaff A, Soyer P, et al. Small-bowel diseases: Prospective eval-uation of multi-detector row helical CT enteroclysis in 107 consecutive patients. Radiology. 2004;233(2):338–44.
10. Van Weyenberg SJ, Meijerink MR, Jacobs MA, eta l. MR enteroclysis in refractory celiac disease: Proposal and validation of a severity scoring system. Radiology. 2011;259(1):151–61.
11. Lohan DG, Alhajeri AN, Cronin CG, et al. MR enterography of small-bowel lymphoma: Potential for suggestion of histologic subtype and the presence of underlying celiac disease. Am J Roentgenol. 2008;190(2):287–93.
12. Di Sabatino A, Biagi F, Gobbi PG, Corazza GR. How I treat enteropathy-associated T-cell lymphoma. Blood. 2012;119(11):2458–2468.
13. Sieniawski M, Angamuthu N, Boyd K, et al. Evaluation of enteropa-thy-associated T cell lymphoma comparing standard therapies with a novel regimen including autologous stem cell transplantation. Blood. 2010;115(18):3664–70.
14. Henter JI, Horne AC, Aricó M, et al. HLH 2004: Diagnostic and thera-peutic guidelines for hemophagocytic lymphohistiocytosis. Pediatr Blood Cancer. 2007;48(2):124–31.
15. Henter JI, Tondini C, Pritchard J. Histiocyte disorders. Crit Rev Oncol Hematol. 2004;50(2):157–74.
16. Jordan MB, Allen CE, Weitzman S, et al. How we treat hemophagocytic lymphohistiocytosis. Blood. 2011;118(15):4041–52.
17. Imashuku S, Kuriyama K, Teramura T, et al. Requirement for etoposide in the treatment of Epstein-Barr virus associated hemophagocytic lym-phohistiocytosis. J Clin Oncol. 2001;19(10):2665–73.
18. Bruck N, Suttorp M, Kabus M, et al. Rapid and sustained remission of systemic juvenile idiopathic arthritis-associated macrophage activation syndrome through treatment with anakinra and corticosteroids. J Clin Rheumatol. 2011;17(1):23–7.

ACG CASE REPORTS JOURNAL
acgcasereports.gi.org ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014143
CASE REPORT | SMALL BOWEL
Asymptomatic Duodenal Perforation from an Inferior Vena Cava FilterJean R. Park, MD, Veeral M. Oza, MD, and Somashekar G. Krishna, MD, MPH
Division of Gastroenterology, Hepatology and Nutrition, Department of Medicine, The Ohio State University, Columbus, OH
AbstractRecent exponential increase in inferior vena cava (IVC) filter placements has led to a higher rate of filter compli-cations. A 46-year-old man with a past history of IVC filter placement for bilateral deep vein thrombosis presented with lower abdominal pain. Imaging studies demonstrated IVC filter strut penetrations into multiple structures. Upper endoscopy confirmed an uncomplicated single IVC filter strut penetration into the duodenal wall. The abdominal pain was determined to be unrelated to IVC filter strut penetration, and the patient was managed con-servatively. Although IVC filter strut penetrations can cause significant complications, current guidelines remain unclear for management of asymptomatic enteric IVC filter strut penetrations.
IntroductionOver the last decade, inferior vena cava (IVC) filter placement has increased dramatically. Complications due to IVC filter include perforation of the aorta, the psoas muscles, and the gastrointestinal (GI) tract.1,2 These perforations are exceedingly rare and usually symptomatic.3 Existing literature describes cases of symptomatic duodenal perforations from IVC filters managed by surgical procedures.2 However, there is a paucity of literature on the treatment of asymptomatic penetrations. We present a patient with an asymptomatic duodenal penetra-tion by an IVC filter.
Case ReportA 46-year-old man with a history of paraplegia from prior trauma, bilateral lower extremity thrombus, and place-ment of an IVC filter 6 years ago underwent a computed tomography (CT) for evaluation of lower abdominal pain. The patient also complained of daytime urinary frequency, incontinence, nocturia, urgency, and weak urinary stream, and had evidence of microscopic hematuria. The CT scan was remarkable for IVC filter strut penetra-tions into the right psoas muscle, L3 vertebral body, and possibly the duodenum (Figure 1). The patient denied symptoms of GI bleeding and a complete blood count was unremarkable. An esophagogastroduodenoscopy (EGD) confirmed a single IVC filter strut penetrating into the second part of the duodenal wall. The intraluminal strut measured 1.5 cm in length, and the end of the strut was hooked, providing a soft end (Figure 2). There was no ulceration or bleeding at the site of penetration. The vascular surgeons felt that the potential complications from IVC filter removal would outweigh the benefits in an otherwise asymptomatic patient. Meanwhile, laboratory evaluation revealed that the patient had a urinary tract infection, and urology service diagnosed benign hypertro-phy of prostate. His abdominal pain was attributed to this cause. He was started on tamsulosin with antibiotics and later reported resolution of lower abdominal pain and urological symptoms. After 1 year of follow-up, the patient remains asymptomatic and free of complications secondary to duodenal penetration by the IVC filter.
ACG Case Rep J 2014;1(3):143–144. doi:10.14309/crj.2014.31. Published online: April 4, 2014.
Correspondence: Somashekar Krishna, 395 W. 12th Avenue, 2nd floor, Division of Gastroenterology, Hepatology and Nutrition Columbus, OH, 43220 ([email protected]).
Copyright: © 2014 Park et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

Publish your work in ACG Case Reports JournalACG Case Reports Journal is a peer-reviewed, open-access publication that provides GI fellows, private practice clinicians, and other members of the health care team an opportunity to share interesting case reports with their peers and with leaders in the field. Visit http://acgcasereports.gi.org for submission guidelines. Submit your manuscript online at http://mc.manuscriptcentral.com/acgcr.
Park et al
acgcasereports.gi.org
Asymptomatic Duodenal Perforation from an IVC Filter
144 ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014
Figure 1. Abdominal CT showing IVC filter struts penetrating the duodenum and right psoas muscle.
DiscussionCaval filters are classified by their anatomical site: infrarenal or suprarenal. Further categories include permanent filters (indi-cated for patients with life-long risk of pulmonary embolism) or retrievable/optional filters (for perioperative use).4 The optional filters have a retrieval hook facilitating easy removal, and the majority of filters currently being used are the retrievable type.4 Interventional radiology guidelines list access site thromboses, IVC occlusions, and IVC penetration as the most frequently re-ported complications. Other complications include filter move-ment and tilt, fracture or embolization, deployment outside the target area, and recurrent pulmonary embolism.5 Filter tilt is the resultant angulation after insertion and is usually minimal after placement in the IVC. A tilt of >15° away from the long axis of the IVC reduces efficacy and predisposes to caval perforation. To reduce risk of filter tilt, manufacturers have implemented ‘hooks’ and ‘legs’ at the end of the filter.4 The overall incidence of filter perforation through the IVC wall is approximately 0.3%.6
Currently, there are no guidelines for the management of pa-tients with asymptomatic IVC filter penetrations into the duode-
num. As the risks of removing the filter overweigh the any likely benefits in such cases, asymptomatic patients require a mul-tidisciplinary approach involving interventional radiology, gas-troenterology, and vascular surgery, and a closely monitored non-operative follow-up. In symptomatic patients, removal of the filter is difficult due to exposure of the IVC bounded by inflammatory reaction, so surgical treatment is recommended only after definitive failure of conservative management and if symptom relief is certain.7 When removal is contemplated, CT and EGD should be used to evaluate filter strut penetrations, and an open procedure by exploratory laparotomy is the typi-cal removal technique. Venotomy is performed to remove the filter, and if the filter struts are not extractable, they should be trimmed with wire cutters.7 In our patient, a non-surgical ap-proach was successfully adopted for the management of IVC filter strut penetration through the duodenal wall.
Disclosures
Author contributions: JR Park and VM Oza completed the literature review and wrote the manuscript. SG Krishna par-ticipated in clinical management of the patient, reviewed the manuscript, and is the author guarantor.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
Received: January 23, 2014; Accepted: March 16, 2014
References1. DuraiRaj R, Fogarty S. A penetrating inferior vena caval filter. Eur J Vasc
Endovasc Surg. 2006;32(6):737–9.2. Vandy F, Rectenwald JE, Criado E. Late gastrointestinal complications
of inferior vena cava filter placement: Case report and literature review. Perspect Vasc Surg Endovasc Ther. 2011;23(4):261–4.
3. Malgor RD, Hines GL, Terrana L, Labropoulos N. Persistent abdominal pain caused by an inferior vena cava filter protruding into the duode-num and the aortic wall. Ann Vasc Surg. 2012;26(6):858.e3–6.
4. Harvey JJ, Hopkins J, McCafferty IJ, Jones RG. Inferior vena cava filters: What radiologists need to know. Clin Radiol. 2013;68(7):721–2.
5. Caplin DM, Nikolic B, Kalva SP, et al. Quality improvement guidelines for the performance of inferior vena cava filter placement for the prevention of pulmonary embolism. J Vasc Interv Radiol. 2011;22(11):1499–1506.
6. Bogue CO, John PR, Connolly BL, et al. Symptomatic caval penetration by a Celect inferior vena cava filter. Pediatr Radiol. 2009;39(10):1110–3.
7. Malgor RD, Hines, GL, Terrana L, Labropoulos N. A systematic review of symptomatic duodenal perforation by inferior vena cava filters. J Vasc Surg. 2012;55(6):856–61.e3.
Figure 2. EGD showing an IVC filter strut perforating through the wall of the duodenum.

ACG CASE REPORTS JOURNAL
acgcasereports.gi.org ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014145
CASE REPORT | COLON
Hematochezia Associated with Sevalamer-Induced Mucosal InjuryPreethi Chintamaneni, MD1, Rohit Das, MD2, Shih-Fan Kuan, MD3, Taher R. Kermanshahi, MD3, and Jana G. Hashash, MD2
1Department of Internal Medicine, University of Pittsburgh Medical Center, Pittsburgh, PA2Department of Gastroenterology, Hepatology, and Nutrition, University of Pittsburgh Medical Center, Pittsburgh, PA3Department of Pathology, University of Pittsburgh Medical Center, Pittsburgh, PA
AbstractWe present a case of a 61-year-old woman with end-stage renal disease (ESRD) who developed painless hema-tochezia following initiation of anticoagulation. Work-up revealed a large ulceration in the sigmoid colon, and his-tologic images revealed sevelamer crystals embedded in the colonic mucosa, consistent with sevelamer crystal-mediated injury. This is a novel cause of gastrointestinal hemorrhage that has not previously been described in the literature. Physicians should be aware of the potential for sevelamer-induced injury.
IntroductionNon-absorbable drugs such as sequestering agents exert their effect in the gastrointestinal lumen by binding a target molecule and forming an insoluble complex preventing absorption. This class of drugs includes many commonly used medications such as sodium polystyrene sulfonate, cholestyramine, and sevelamer. While the potential for mucosal injury of the gastrointestinal tract has been demonstrated in the literature with the use of cholestyramine and sodium polystyrene sulfate, there have been few reports of sevelamer-associated mucosal injury.
Case ReportA 61-year-old African-American woman with a history of end-stage renal disease (ESRD) requiring chronic hemodialysis presented to our hospital for management of a thrombosed arteriovenous graft. After mechanical thrombectomy, the patient was started on an IV heparin infusion with transition to warfarin. Two days post-oper-atively, she developed painless hematochezia. Her medications included calcium acetate, cinacalcet, diltiazem, glipizide, hydroxyzine, losartan, omeprazole, pravastatin, and sevelamer 2,400 mg by mouth 3 times daily. She denied any recent nonsteroidal anti-inflammatory drug use. She denied having problems with constipation. Prior to surgery, the patient received a brief course of high-dose steroids as premedication for a contrast allergy.
Physical examination revealed a hemodynamically stable obese woman in no acute distress. Her abdomen was soft, non-tender, and non-distended. Rectal exam revealed dark red blood with no hemorrhoids or anal fissures. Laboratory evaluation revealed hemoglobin 10.8 g/dL (baseline: 11.1 g/dL). Colonoscopy revealed a 5-cm semi-circumferential ulceration in the sigmoid colon 25 cm from the anal verge (Figure 1 and Figure 2). The ulcer was not actively bleeding, so no endoscopic intervention for hemostasis was performed. The ulcer border was biopsied, and histology revealed an ulcer bed with attached fibrin, hemorrhage, and entrapped pale yellow-to-or-
ACG Case Rep J 2014;1(3):145–147. doi:10.14309/crj.2014.32. Published online: April 4, 2014.
Correspondence: Preethi Chintamaneni, Department of Internal Medicine, University of Pittsburgh Medical Center, 200 Lothrop Street, PUH, M2, C Wing, Pittsburgh, PA 15213 ([email protected]).
Copyright: © 2014 Chintamaneni et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

Hematochezia Associated with Sevalamer Use
acgcasereports.gi.org ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014
Chintamaneni et al
146
ange crystals, which is a finding associated with sevelamer-induced mucosal injury (Figure 3). Sevelamer was discon-tinued with no recurrence of hematochezia, and a heparin drip was restarted 6 hours after the colonoscopy without any subsequent gastrointestinal bleeding. After discussion with the vascular surgery team, the patient was switched to clopi-drogel for long-term anticoagulation. Repeat endoscopy is planned 6 months after this bleeding episode to check for mucosal healing after discontinuation of sevelamer.
DiscussionSevelamer is an anion exchange resin that is approved for use in the United States and Europe to treat hyperphospha-
temia in patients with ESRD who are on hemodialysis. It is a nonabsorbable polymer that dissociates from its anion (ei-ther carbonate in Renvela® or hydrochloride in Renagel®) and binds to dietary phosphate within the gastrointestinal tract preventing reabsorption.1 The most common side ef-fects associated with sevelamer use are gastrointestinal, including vomiting (22%), nausea (20%), diarrhea (19%), dyspepsia (16%), and constipation (8%). The most concern-ing adverse effect is metabolic acidosis, which is seen with sevelamer hydrochloride (Renagel®) but not with sevelamer carbonate (Renvela®). Sevelamer use is contraindicated in the presence of bowel obstruction. Sevelamer crystals are non-polarizable and are characterized as having broad, curved, irregular fish scales. Sevelamer crystal deposition in the colon may contribute to mucosal inflammation and ulcer formation. On hematoxylin and eosin stain, the crystals are two-toned in appearance with bright pink accentuations on a rusty yellow background.2
There is little existing literature regarding sevelamer crystal-mediated mucosal injury. A prospective series identified 15 pathology specimens from throughout the gastrointestinal tract containing sevelamer crystals, of which 14 had abnor-mal background mucosal findings.2 While some of these cases were felt to include incidental sevelamer crystal depo-sition in the context of other comorbidities, there were also patients with findings suggestive of direct sevelamer crystal-mediated injury as evidenced by acute ulcerations in various parts of the gastrointestinal tract. They also found a dose-dependent relationship with an increased degree of mucosal injury in patients receiving higher doses of sevelamer.
Madan et al described an incident of sevelamer use caus-ing lower gastrointestinal bleeding through the formation of a stercoral ulcer. Stercoral ulceration is defined as an ul-cer caused by pressure necrosis from a fecaloma. In this
Figure 1. A 5-cm semi-circumferential ulceration in the sigmoid colon 25 cm from the anal verge revealed by colonoscopy.
Figure 2. Ulcer in the sigmoid colon.
Figure 3. Hematoxylin and eosin stain of ulcer bed with sevelamer crystals.

Publish your work in ACG Case Reports JournalACG Case Reports Journal is a peer-reviewed, open-access publication that provides GI fellows, private practice clinicians, and other members of the health care team an opportunity to share interesting case reports with their peers and with leaders in the field. Visit http://acgcasereports.gi.org for submission guidelines. Submit your manuscript online at http://mc.manuscriptcentral.com/acgcr.
Chintamaneni et al
acgcasereports.gi.org
Hematochezia Associated with Sevalamer Use
147 ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014
case, sevelamer caused severe constipation, which in turn resulted in formation of a fecaloma and subsequently a ster-coral ulceration in the rectum.3 In contrast to this report, our patient did not report constipation and her ulcer was in the sigmoid colon, thus stercoral ulceration unlikely to be the cause of her colonic mucosal injury.
With the growing use of sevelamer in patients with ESRD, it is important to recognize the potential clinical impact of mucosal injury associated with sevelamer crystal deposition. Unfortunately, at this time, there are no known strategies described in the literature to prevent sevelamer-associated mucosal injury. Our case suggests that there may be an as-sociation between sevelamer use and mucosal injury, but further evidence is necessary to indicate causation. Sodium polysyterene sulfonate is a cation-exchange resin used in the treatment of hyperkalemia that is believed to be directly toxic to the colonic mucosa, resulting in colonic ischemia and ulceration. We postulate that sevelamer potentially me-diates mucosal injury under a similar mechanism, and that sevelamer crystals deposit in the mucosa of the colon, where they are directly toxic and result in ischemic changes and subsequent ulcer formation.
Disclosures
Author contributions: P. Chintamaneni and R. Das acquired and interpreted the data, and drafted the manuscript. SF Kuan and TR Kermanshahi acquired and interpreted the data. JG Hashash interpreted the data, and drafted and criti-cally revised the manuscript for important intellectual con-tent. P. Chintamaneni is the article guarantor.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
Received: January 15, 2014; Accepted: March 16, 2014
References1. Grinfeld J, Inaba A, Hutchinson A. Update and critical appraisal of
sevelamer in the management of chronic renal failure. Open Access J Urol. 2010;2:161–70.
2. Swanson BJ, Limketkai BN, Liu TC, et al. Sevelamer crystals in the gas-trointestinal tract: A new entity associated with mucosal injury. Am J Surg Pathol. 2013;37(11):1686–93.
3. Madan P, Bhayana S, Chandra P, Hughes JI. Lower gastrointesti-nal bleeding: Association with sevelamer use. World J Gastroenterol. 2008;14(16):2615–6.

ACG CASE REPORTS JOURNAL
acgcasereports.gi.org ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014148
CASE REPORT | INFLAMMATORY BOWEL DISEASE
Use of Serum Infliximab Level Prior to Cyclosporine Salvage Therapy in Severe Ulcerative ColitisChristopher G. Chapman, MD, Ashley Bochenek, MSN, APN/FNP-BC, Adam C. Stein, MD, and David T. Rubin, MD
Inflammatory Bowel Disease Center, University of Chicago Medical Center, Chicago, IL
AbstractMedical treatment options for severe, steroid refractory ulcerative colitis (UC) include infliximab (IFX) or cyclo-sporine (CSA), but general consensus has been that both agents should not be used together or even succes-sively. We report a case of a 17-year-old male with severe UC refractory to IV steroids with successful sequential salvage therapy guided by serum IFX level. After primary lack of response to IFX, an undetectable serum IFX level and elevated IFX antibodies were followed by immediate transition to IV CSA. This case demonstrates the possibility of therapeutic drug monitoring of IFX levels when calculating the risk/benefit ratio for patients with steroid-refractory UC failing primary salvage therapy.
IntroductionBoth infliximab (IFX) and cyclosporine (CSA) are effective for the treatment of severe ulcerative colitis (UC) that is refractory to IV steroids,1,2 but general consensus has been that both agents should not be used together or even successively. A recent randomized trial of these agents in IV steroid-refractory patients found no difference in efficacy, but 40% of patients did not respond to the therapy in either arm.3 Case series have reported signifi-cant infectious events when the 2 agents are used for salvage therapy in close succession.4–7 We report a case of severe UC with successive salvage therapy guided by serum IFX level.
Case ReportA 17-year-old male with a 6-month history of pan-UC presented to our center. He had primary non-response to 8 weeks of mesalamine and continuous oral prednisone. He was started on combination therapy with azathioprine (AZA) 50 mg per day and IFX 5 mg/kg IV at 0 and 2 weeks, but due to lack of response, received 7.5 mg/kg IV at 6 weeks. Despite this approach, he was unable to wean from prednisone with persistent disease activity charac-terized by 6–8 bloody loose stools per day with associated severe urgency and nocturnal bowel movements. He received his next IFX at 7.5 mg/kg 6 weeks later. When this failed to control his colitis, he transferred care to our institution and was admitted. At that time (2 weeks after his last IFX dose) admission labs (Table 1) and serum IFX level and antibodies to IFX (ATI) were ordered (electrochemiluminescence immunoassay [ECLIA]; Esoterix Endocrinology, Calabasa Hills, CA).
He was found to have Clostridium difficile (C. difficile) infection and was treated with oral vancomycin 125 mg 4 times daily, metronidazole 500 mg IV every 8 hours, and IV methylprednisolone 20 mg every 12 hours. He was maintained on dual therapy for C. difficile for 12 days with continuation of oral vancomycin monotherapy for an additional 18 days. Despite clearance of C. difficile (by negative PCR 7 days after initiating therapy), he continued to have frequent bloody stools and urgency. Colonoscopy confirmed the presence of diffuse moderate-
ACG Case Rep J 2014;1(3):148–150. doi:10.14309/crj.2014.33. Published online: April 4, 2014.
Correspondence: Christopher G. Chapman, 5841 S. Maryland Avenue, Chicago, IL, 60647 ([email protected]).
Copyright: © 2014 Chapman et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

Cyclosporine Salvage Therapy in Severe UC
acgcasereports.gi.org ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014
Chapman et al
149
to-severe active colitis (Figure 1). Biopsies demonstrated no evidence of viral cytopathic change, and immunostains were negative for cytomegalovirus infection. Eight days after ad-mission, IFX and ATI results showed that serum infliximab was undetectable, and ATI was 265 ng/mL (reference: <22 ng/mL). After discussion with the patient, we decided to pursue further medical management. CSA 2 mg/kg IV con-tinuous infusion was started (goal serum level: 300–400 ng/mL)8 with standard antibiotic prophylaxis for Pneumocystis pneumonia with trimethoprim/sulfamethoxazole (TMP/SMZ) and continued IV steroids. After 4 days of CSA, the hemato-chezia had stopped and the diarrhea started to resolve. He was discharged from the hospital on oral CSA, prednisone, TMP/SMZ, and AZA (Figure 2). At the time of this report 9 months later, he remains in steroid-free remission only on AZA, and there were no adverse events.
DiscussionMedical options for hospitalized patients with severe, corti-costeroid-refractory UC include IFX or CSA. Initial response rates for both CSA and IFX in this challenging patient popu-lation are similar, ranging from 62% to 83%,2,9–11 respec-tively, and 71% of patients at 3 months.1 A recent parallel, open label, randomized control trial comparing the 2 thera-pies found IV CSA and IFX to be no different for achieving short-term remission and colectomy-free survival, with simi-lar rates of serious adverse events.3
In patients treated with either CSA or IFX who do not respond to therapy, options include colectomy or, in a selective co-hort, successive salvage therapy with the other agent. Pub-lished experience with successive salvage medical therapy has been limited to several small case series. Manosa et al6 reported that 6 of 16 patients receiving IFX salvage after CSA (38%) required colectomy after a median follow-up time of 195 days, while in a similar cohort, Chaparro et al7 reported that 29% progressed to colectomy at 1 year. Maser et al4 reported a retrospective study of 19 patients with steroid-re-fractory UC who were treated with CSA or IFX within 30 days as sequential rescue therapy. At 1 year, 8 (42%) patients required colectomy; steroid-free remission was achieved in 40% of the IFX-salvage cohort and 33% in the CSA-salvage cohort without statistical difference between them. In the largest cohort published to date, Leblanc et al5 published a retrospective study of 86 patients in which 48 (56%) pa-tients had a colectomy despite sequential salvage therapy
Figure 1. Moderate-to-severe active ulcerative colitis in the sigmoid colon confirmed via colonoscopy.
Table 1. Patient Laboratory Admission Values and Normal Values
Laboratory Parameter Admission Values Normal Values
Sodium, mEq/L 140 134–149
Potassium, mEq/L 4.0 3.5–5.0
Chloride, mEq/L 104 95–108
Bicarbonate, mEq/L 28 23–30
Urea nitrogen, mg/dL 12 7–20
Creatinine, mg/dL 0.9 0.5–1.4
Glucose, mg/dL 85 60–109
Calcium, mg/dL 8.9 8.4–10.2
Total protein, g/dL 6.6 6.0–8.3
Albumin, g/dL 3.7 3.5–5.0
Total bilirubin, mg/dL 0.1 0.1–1.0
Alkaline phosphatase, U/L 67 100–390
AST, U/L 17 8–37
ALT, U/L 34 8–35
White blood cells, K/uL 19.0 3.5–11
Hemoglobin, g/dL 11.2 13.5–17.5
Platelets, K/uL 391 150–450
C-Reactive protein, mg/L 27 <5
AST = aspartate aminotransferase; ALT = alanine transaminase
Figure 2. Clinical course, with Simple Clinical Colitis Activity Index (SSCAI) and cyclosporine levels.

Publish your work in ACG Case Reports JournalACG Case Reports Journal is a peer-reviewed, open-access publication that provides GI fellows, private practice clinicians, and other members of the health care team an opportunity to share interesting case reports with their peers and with leaders in the field. Visit http://acgcasereports.gi.org for submission guidelines. Submit your manuscript online at http://mc.manuscriptcentral.com/acgcr.
Chapman et al
acgcasereports.gi.org
Cyclosporine Salvage Therapy in Severe UC
150 ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014
at 1 year, while 22% of patients had steroid-free remission.
The decision to pursue sequential medical therapy must account for the risks of delaying surgical intervention and that dual immunosuppression raises the risk of infection. Maser et al reported 3 (16%) serious infectious adverse events, including 1 death from gram-negative sepsis in the IFX salvage group. Leblanc et al reported that their IFX sal-vage group suffered 9 (10.5%) serious infectious complica-tions as well as 1 death due to post-colectomy pulmonary embolism, possibly related to delayed surgical intervention. Chaparro et al also reported an infection adverse event rate of 8.4%, including 1 death due to post-colectomy nosoco-mial pneumonia.
The significantly longer half-life for IFX (8–10 days) versus CSA (6–8 hours) has led some to suggest the use of CSA as a first approach to steroid-refractory UC; if CSA fails, a shorter wash-out period may allow for safer IFX use. A lack of experience with CSA by gastroenterologists has made this option impractical. There is increasing evidence that the primary non-response to IFX in severe colitis may be par-tially attributed to rapid metabolism or rapid clearance of the drug, with emerging reports of fecal elimination of the drug as a potential explanation.12,13
This is the first report of the use of therapeutic drug monitor-ing to minimize toxicity and guide IFX/CSA salvage therapy. We believe that this patient’s lack of response to IFX was due to rapid clearance and anti-drug antibodies. We do not know if he was losing IFX through a protein-losing colopathy and this “pseudo-episodic” therapy resulted in immunogenicity against the drug, or if he already had ATI that neutralized the IFX. In either explanation, it was clear that the subtherapeu-tic drug level was contributing to his lack of response to this therapy. The undetectable IFX level provided reassurance for use of salvage CSA. We propose that therapeutic moni-toring may be used in the assessment of salvage therapies for selected patients.
A practical limitation to this approach is the time required to obtain IFX and ATI levels with currently available clinical assays, which delays clinical and therapeutic decisions for the patient. We believe that waiting for these results is worth-while, considering the risks of surgery that may be averted. In the future, we hope “point of service” assays and improved turnaround times—driven by volume and demand—will re-duce waiting time and make this approach more practical.
Disclosures
Author contributions: CG Chapman and AC Stein were in-volved with patient care and wrote the manuscript. A. Bo-chenek was involved with patient care. DT Rubin was in-volved with patient care, reviewed and revised the manu-script, and is the article guarantor.
Financial disclosure: No financial support was received, and the authors have no conflicts of interest to report.
Informed consent was obtained for this case report.
Received: November 3, 2013; Accepted: December 16, 2013
References1. Jarnerot G, Hertervig E, Friis-Liby I, et al. Infliximab as rescue therapy in
severe to moderately severe ulcerative colitis: A randomized, placebo-controlled study. Gastroenterology. 2005;128(7):1805-11.
2. Lichtiger S, Present DH, Kornbluth A, et al. Cyclosporine in se-vere ulcerative colitis refractory to steroid therapy. N Engl J Med. 1994;330(26)1841–5.
3. Laharie D, Bourreille A, Branche J, et al. Ciclosporin versus inflix-imab in patients with severe ulcerative colitis refractory to intravenous steroids: A parallel, open-label randomised controlled trial. Lancet. 2012;380(9857):1909–15.
4. Maser EA, Deconda D, Lichtiger S, et al. Cyclosporine and infliximab as rescue therapy for each other in patients with steroid-refractory ulcerative colitis. Clin Gastroenterol Hepatol. 2008;6(10):1112–6.
5. Leblanc S, Allez M, Seksik P, et al. Successive treatment with cyclospo-rine and infliximab in steroid-refractory ulcerative colitis. Am J Gastroen-terol. 2011;106(4):771–7.
6. Mañosa M, López San Román, A, Garcia-Planella E,et al. Infliximab res-cue therapy after cyclosporin failure in steroid-refractory ulcerative colitis. Digestion. 2009;80(1):30–5.
7. Chaparro M, Burgueño P, Iglesias E, et al. Infliximab salvage therapy after failure of ciclosporin in corticosteroid-refractory ulcerative colitis: A multi-centre study. Aliment Pharmacol Ther. 2012;35(2):275 –83.
8. Van Assche G, D’Haens G, Noman M, et al. Randomized, double-blind comparison of 4 mg/kg versus 2 mg/kg intravenous cyclosporine in se-vere ulcerative colitis. Gastroenterology. 2003;125(4):1025–31.
9. García-López S, Gomollón-García F, Pérez-Gisbert J. Cyclosporine in the treatment of severe attack of ulcerative colitis: A systematic review. Gas-troenterol Hepatol. 2005;28(10):607–14.
10. Campbell S, Travis S, Jewell D. Ciclosporin use in acute ulcerative colitis: A long-term experience. Eur J Gastroenterol Hepatol. 2005;17(1):79–84.
11. Arts J, D’Haens G, Zeegers M, et al. Long-term outcome of treatment with intravenous cyclosporin in patients with severe ulcerative colitis. Inflamm Bowel Dis. 2004;10(2):73–8.
12. Brandse J, Wildenberg ME, Bruyn JR, et al. Fecal loss of infliximab as a cause of lack of response in severe inflammatory bowel disease. Pre-sented at: Digestive Disease Week; May 18, 2013; Abstract 157.
13. Kevans D, Murthy S, Iacono A, et al. Accelerated clearance of serum in-fliximab during induction therapy for acute ulcerative colitis is associated with treatment failure. Gastroenterology. 2012;142(suppl 1):S384–S385.

ACG CASE REPORTS JOURNAL
acgcasereports.gi.org ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014151
CASE REPORT | PANCREAS
A Unique Case of Hematemesis in a 17-Year-Old FemaleTobias Zuchelli, MD, Eva Alsheik, MD, Bhavik Bhandari, MD, and Daniel Ringold, MD
Division of Gastroenterology and Hepatology, Drexel University College of Medicine, Philadelphia, PA
AbstractHemosuccus pancreaticus (HP) is a rare cause of gastrointestinal bleeding (GIB) that should be considered in a patient with a history of pancreatitis and GIB. A 17-year-old female presented with nausea followed by an epi-sode of hematemesis. Fourteen weeks prior to presentation, she had 3 episodes of vomiting within a week. Six weeks prior to presentation, she developed abdominal pain and was diagnosed with acute idiopathic pancreati-tis. Computed tomography (CT) revealed a cystic lesion arising in the gastroduodenal artery (GDA), and coil em-bolization was performed. There are no reported cases of HP in an adolescent with acute idiopathic pancreatitis.
IntroductionHemosuccus pancreaticus (HP) was defined by Sandblom in 1970 as gastrointestinal bleeding secondary to rupture of a pseudoaneurysm into the pancreatic duct.1 This condition is exceedingly rare in the adolescent population. We describe an unusual presentation of HP in a 17-year-old female with a history acute idiopathic pancreatitis.
Case ReportA 17-year old white female presented with a sudden feeling of nausea followed by a single episode of reddish-brown emesis. The patient felt the reddish color was related to her breakfast of red licorice and cherry-flavored breakfast tarts. She reluctantly presented to the emergency room of our tertiary care center for further evaluation.
Fourteen weeks prior, she had 3 episodes of vomiting and abdominal pain and was prescribed a proton pump inhibitor (PPI). Two weeks after stopping the PPI (6 weeks prior to presentation) she experienced recurrent vomiting and abdominal pain requiring admission. Lipase was elevated to 3 times the upper limit of normal, but right upper quadrant ultrasound and laboratory tests, including liver function tests, calcium, and lipid panel, did not reveal an etiology. She was discharged with a diagnosis of acute idiopathic pancreatitis, although endoscopic ultrasound (EUS) and magnetic resonance cholangiopancreatography (MRCP) were not performed.
On this presentation, she had no episodes of nausea or vomiting beyond her first episode and her review of sys-tems was unremarkable. She denied nonsteroidal medications, herbals, alcohol, illicit drug use, recent travels, trauma, and sick contacts. In the emergency room, her vital signs were normal and physical exam was unre-markable, including rectal exam, which revealed brown stool. Admission labs showed hemoglobin 9.0 mg/dL, mean cell volume (MCV) 89 FL, blood urea nitrogen (BUN) 12 mg/dL, and creatinine 0.7 mg/dL. Liver function tests, amylase, and lipase were normal. An esophagogastroduodenoscopy (EGD) performed for anemia and hematemesis showed a large deformity in the antrum and duodenal bulb thought to be secondary to extrinsic compression. There was a deep duodenal ulcer in the area of extrinsic compression without evidence of active bleeding (Figure 1). Given the presence of extrinsic compression, we were concerned that this ulcer was an extrinsic process that warranted further radiologic imaging.
ACG Case Rep J 2014;1(3):151–153. doi:10.14309/crj.2014.34. Published online: April 4, 2014.
Correspondence: Tobias Zuchelli, Division of Gastroenterology and Hepatology, Drexel University College of Medicine, 219 North Broad Street, The Arnold T. Berman, M.D. Building, 5th Floor, Philadelphia, PA 19107 ([email protected]).
Copyright: © 2014 Zuchelli et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

Hematemesis in a 17-Year-Old Female
acgcasereports.gi.org ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014
Zuchelli et al
152
A contrast computed tomography (CT) scan of the abdomen was subsequently performed that revealed a 4.6 x 4.4 x 6.8-cm mixed attenuated cystic lesion with a thin enhancing rim (likely a pancreatic pseudocyst with mass effect on the an-trum and duodenum) and an ovoid focus extending from the gastroduodenal artery (GDA) suggestive of pseudoaneurysm formation (Figure 2). The patient was immediately referred to interventional radiology and underwent angiogram, which revealed a 2.8-cm GDA pseudoaneurysm. Successful coil embolizations of the GDA and outflow track of the right gas-troepiploic artery were performed (Figure 3). Her remaining hospital stay was uneventful. A follow-up CT scan 10 weeks later showed resolution of the pseudocyst and pseudoaneu-rysm. Genetic testing for CFTR and PRSS-1 did not reveal an etiology for the pancreatitis, and she currently remains asymptomatic.
DiscussionHemosuccus pancreaticus (HP) was defined by Sandblom in 1970 as gastrointestinal bleeding secondary to rupture of a pseudoaneurysm into the pancreatic duct.1 The most common cause of HP is chronic pancreatitis with pseudo-cyst erosion into a peripancreatic artery and formation of a pseudoaneurysm. Although HP only accounts for 1/1,500 cases of gastrointestinal bleeding, it should be considered in a patient with a history of pancreatitis.2 Idiopathic pan-creatitis, which is diagnosed when no underlying cause is found on routine investigation, comprises an estimated 30% of cases of acute pancreatitis in the adult population. It is exceedingly rare in adolescents. Pseudocysts occur in ap-proximately 10% of all cases of acute pancreatitis, of which 10% can develop HP. The most common arteries implicated in HP are the splenic (45%), gastroduodenal (17%), and pancreaticoduodenal (16%) arteries.3 Due to the high con-centration of digestive enzymes within pseudocysts, pseu-doaneurysms can eventually rupture into the ductal system. Bleeding is intermittent due to clot formation in the main pancreatic duct, and active bleeding from the papilla is visu-alized on upper endoscopy in only 30% of patients.4 Howev-er, upper endoscopy should always be performed to exclude other sources of gastrointestinal bleed. Point ulcers in the gastric or duodenal wall due to aneurysm can also be seen, as was the case in our patient.
Because of the intermittent nature of bleeding and difficul-ties in determining the bleeding source endoscopically, diag-nosis of HP is frequently delayed. The diagnosis is generally made with abdominal CT and/or selective angiography of the celiac trunk and superior mesenteric artery; the latter is 96% sensitive in detecting pseudoaneurysms.1 Interventional ra-diology is the primary modality for confirming diagnosis and treatment with coil embolization.5 If bleeding persists or is life threatening, treatment with a Whipple procedure or pseudo-cyst resection and ligation of the culprit vessel is indicated.
This case is unique in that the patient presented with acute
Figure 1. Deep duodenal ulcer in the area of extrinsic compression shown on EGD.
Figure 2. Abdominal CT showing a 4.6 x 4.4 x 6.8-cm mixed attenuated cystic lesion with a thin enhancing rim (likely a pancreatic pseudocyst with mass effect on the antrum and duodenum) and an ovoid focus extending from the GDA.
Figure 3. Successful coil embolizations of a 2.8-cm GDA pseudoaneurysm and outflow track of the right gastroepiploic artery.

Publish your work in ACG Case Reports JournalACG Case Reports Journal is a peer-reviewed, open-access publication that provides GI fellows, private practice clinicians, and other members of the health care team an opportunity to share interesting case reports with their peers and with leaders in the field. Visit http://acgcasereports.gi.org for submission guidelines. Submit your manuscript online at http://mc.manuscriptcentral.com/acgcr.
Zuchelli et al
acgcasereports.gi.org
Hematemesis in a 17-Year-Old Female
153 ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014
idiopathic pancreatitis followed by a bleed from HP 6 weeks later. There are no similar reported cases of HP in an ado-lescent with acute idiopathic pancreatitis. In a patient with a history of pancreatitis and gastrointestinal bleed, HP must be considered in the differential to ensure timely diagnosis and treatment of a potentially lethal condition.
Disclosures
Author contributions: T. Zuchelli and E. Alsheik drafted and critically revised the manuscript for important intellectual content. B. Bhandari critically revised the manuscript for im-portant intellectual content. D. Ringold drafted and critically revised the manuscript for important intellectual content and provided endoscopic images. T. Zuchelli is the article guar-antor.
Financial disclosure: None to report.
The IRB of Drexel University College of Medicine reviewed and approved this case report for publication. This institu-tion deems IRB approval as sufficient consent.
Received: December 13, 2013; Accepted: March 16, 2014
References1. Sandblom P. Gastrointestinal hemorrhage through the pancreatic duct.
Ann Surg. 1970;171(1):61–6. 2. Mandel SR, Jaques PF, Sanofsky S, Mauro MA, et al. Nonoperative
management of peripancreatic arterial aneurysms. A 10-year experi-ence. Ann Surg. 1987;205(2):126–8.
3. Castillo-Sang M, Higgins JA, Tsang AW, et al. Hemosuccus pancreaticus. Am Surg. 2009;75(9):865–7.
4. Toyoki Y, Hakamada K, Narumi S, et al. Hemosuccus pancreaticus: Problems and pitfalls in diagnosis and treatment. World J Gastroenterol. 2008; 14(17):2776–9.
5. Etienne S, Pessaux P, Tuech JJ, et al. Hemosuccus pancreaticus: A rare cause of gastrointestinal bleeding. Gastroenterol Clin Biol. 2005;29(3):237–42.
ACG CASE REPORTS JOURNAL
acgcasereports.gi.org ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014154
CASE REPORT | PANCREAS
Groove Pancreatitis: Four Cases from a Single Center and Brief Review of the LiteratureTyler P. Black, MD1, Cynthia D. Guy, MD2, Rebekah R. White, MD3, Jorge Obando, MD4, and Rebecca A. Burbridge, MD4
1Department of Internal Medicine, Duke University Medical Center, Durham, NC2Department of Pathology, Duke University Medical Center, Durham, NC3Department of Surgery, Duke University Medical Center, Durham, NC4Department of Gastroenterology, Duke University Medical Center, Durham, NC
AbstractGroove pancreatitis is a rare form of chronic pancreatitis that affects the groove anatomical area between the head of the pancreas, duodenum, and common bile duct. We provide a summary of the clinical findings of 4 groove pancreatitis cases diagnosed at a tertiary academic medical center over a 5-year period. A detailed review of the current literature surrounding this clinical entity is also provided. Although rare, groove pancreatitis should be considered in the differential diagnosis of patients presenting with pancreatic head mass lesions, as appropri-ate diagnosis can help avoid unnecessary surgical procedures.
IntroductionGroove pancreatitis is a rare condition characterized by fibrotic inflammation affecting the anatomical area between the head of the pancreas, duodenum, and common bile duct.1 This condition can often be difficult to differentiate from adenocarcinoma of the pancreatic head, but certain clinical, radiological, and histological fea-tures can be useful in making a diagnosis. The prevalence of groove pancreatitis has been difficult to establish, but has been reported as high as 24.5% in pancreaticoduodenectomy specimens from patients with chronic pancreatitis.2 It often presents in middle-aged males (aged 40–50 years) with a history of alcohol consumption, recurrent or chronic pancreatitis, and pancreatic head mass lesions on imaging.3 Its presentation is similar to adenocarcinoma of the pancreatic head or, more rarely, autoimmune pancreatitis, but can often be cured by conservative management.4,5 We present a series of 4 cases of groove pancreatitis diagnosed at a tertiary medi-cal center over a 5-year period, with a detailed review of the current medical literature.
Case ReportFour cases of suspected groove pancreatitis were identified over a 5-year period. Two cases had histological confirmation of groove pancreatitis. The other 2 cases were considered to be likely diagnoses based on the clini-cal presentation and imaging findings. Table 1 shows a summary of the findings for each case. The average age was 56.5 years. Two patients were African American and 2 were female. All patients presented with abdominal pain and were given a diagnosis of pancreatitis based on an elevation of lipase and/or amylase. Two patients had both computed tomography (CT) and magnetic resonance imaging (MRI), while the other 2 patients had either CT or MRI. A representative CT image from patient 3 is shown in Figure 1. Patients 1 and 4 were given a diagnosis of groove pancreatitis based on their imaging findings, whereas patients 2 and 3 were diagnosed by
ACG Case Rep J 2014;1(3):154–157. doi:10.14309/crj.2014.35. Published online: April 4, 2014.
Correspondence: Tyler P. Black, Duke University Medical Center, 2301 Erwin Road, Durham, NC, 27710 ([email protected]).
Copyright: © 2014 Black et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
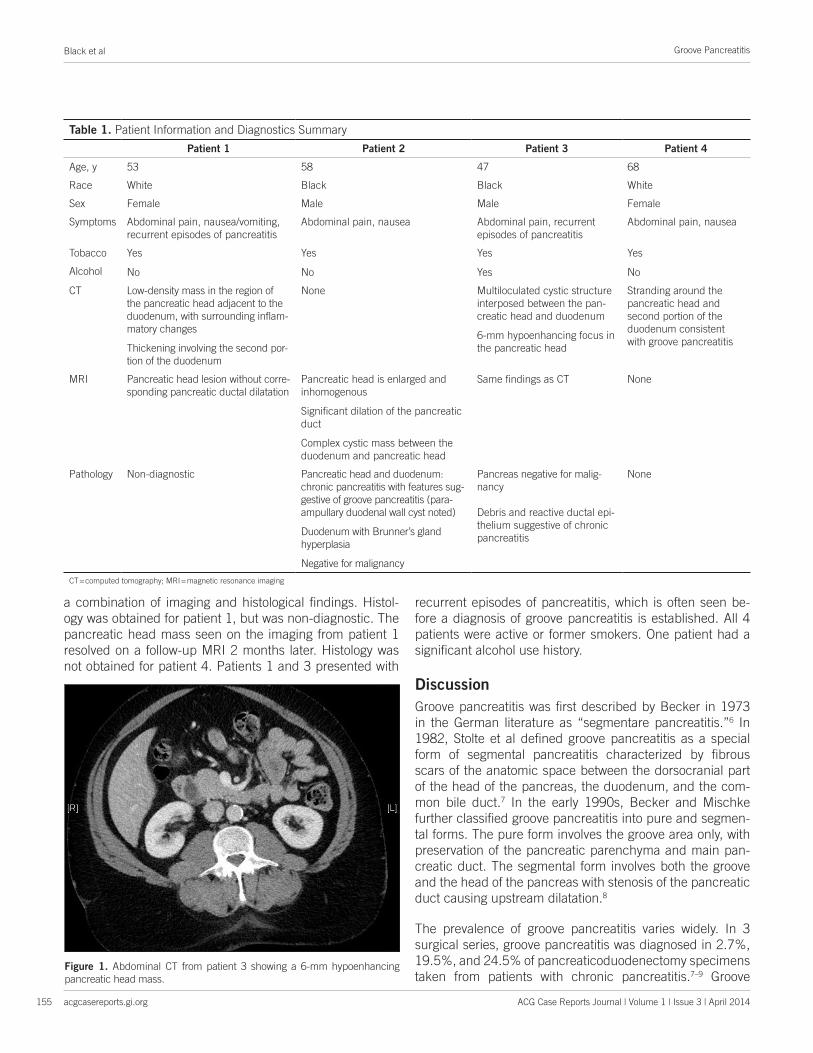
Groove Pancreatitis
acgcasereports.gi.org ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014
Black et al
155
a combination of imaging and histological findings. Histol-ogy was obtained for patient 1, but was non-diagnostic. The pancreatic head mass seen on the imaging from patient 1 resolved on a follow-up MRI 2 months later. Histology was not obtained for patient 4. Patients 1 and 3 presented with
recurrent episodes of pancreatitis, which is often seen be-fore a diagnosis of groove pancreatitis is established. All 4 patients were active or former smokers. One patient had a significant alcohol use history.
DiscussionGroove pancreatitis was first described by Becker in 1973 in the German literature as “segmentare pancreatitis.”6 In 1982, Stolte et al defined groove pancreatitis as a special form of segmental pancreatitis characterized by fibrous scars of the anatomic space between the dorsocranial part of the head of the pancreas, the duodenum, and the com-mon bile duct.7 In the early 1990s, Becker and Mischke further classified groove pancreatitis into pure and segmen-tal forms. The pure form involves the groove area only, with preservation of the pancreatic parenchyma and main pan-creatic duct. The segmental form involves both the groove and the head of the pancreas with stenosis of the pancreatic duct causing upstream dilatation.8
The prevalence of groove pancreatitis varies widely. In 3 surgical series, groove pancreatitis was diagnosed in 2.7%, 19.5%, and 24.5% of pancreaticoduodenectomy specimens taken from patients with chronic pancreatitis.7–9 Groove
Figure 1. Abdominal CT from patient 3 showing a 6-mm hypoenhancing pancreatic head mass.
Table 1. Patient Information and Diagnostics Summary
Patient 1 Patient 2 Patient 3 Patient 4
Age, y 53 58 47 68
Race White Black Black White
Sex Female Male Male Female
Symptoms Abdominal pain, nausea/vomiting, recurrent episodes of pancreatitis
Abdominal pain, nausea Abdominal pain, recurrent episodes of pancreatitis
Abdominal pain, nausea
Tobacco Yes Yes Yes Yes
Alcohol No No Yes No
CT Low-density mass in the region of the pancreatic head adjacent to the duodenum, with surrounding inflam-matory changes
Thickening involving the second por-tion of the duodenum
None Multiloculated cystic structure interposed between the pan-creatic head and duodenum
6-mm hypoenhancing focus in the pancreatic head
Stranding around the pancreatic head and second portion of the duodenum consistent with groove pancreatitis
MRI Pancreatic head lesion without corre-sponding pancreatic ductal dilatation
Pancreatic head is enlarged and inhomogenous
Significant dilation of the pancreatic duct
Complex cystic mass between the duodenum and pancreatic head
Same findings as CT None
Pathology Non-diagnostic Pancreatic head and duodenum: chronic pancreatitis with features sug-gestive of groove pancreatitis (para-ampullary duodenal wall cyst noted)
Duodenum with Brunner’s gland hyperplasia
Negative for malignancy
Pancreas negative for malig-nancy
Debris and reactive ductal epi-thelium suggestive of chronic pancreatitis
None
CT = computed tomography; MRI = magnetic resonance imaging

Groove Pancreatitis
acgcasereports.gi.org ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014
Black et al
156
pancreatitis often presents in alcoholic men aged 40–50 years.7,8 Presenting symptoms consist of abdominal pain, nausea, vomiting, and weight loss.7,8 Laboratory evaluation often reveals an elevation in pancreatic enzymes and rarely an elevation in hepatic enzymes.10 Carcinoembryonic anti-gen and carbohydrate antigen 19-9 can also be elevated.9
A diagnosis of groove pancreatitis is often difficult to es-tablish. The most important distinction to make is between groove pancreatitis and adenocarcinoma of the head of the pancreas. Ultrasound will typically show a hypoechoic mass, and CT will often reveal a hypodense, poorly enhanc-ing mass between the head of the pancreas and a thickened duodenal wall.11 The most characteristic MRI finding is a sheet-like mass between the head of the pancreas and the duodenum associated with duodenal wall cystic changes and thickening.5 Endoscopic retrograde cholangiopancrea-tography (ERCP) and endoscopic ultrasonography (EUS) are often useful in the differentiation of groove pancreati-tis from pancreatic adenocarcinoma, and should be used early in evaluation even when cross-sectional imaging is not suggestive of a mass.12 Table 2 lists characteristic imaging features differentiating groove pancreatitis from pancreatic adenocarcinoma.
The pathogenesis of groove pancreatitis remains unclear, and several mechanisms have been proposed. The most ac-cepted mechanism is a disturbance of pancreatic outflow in the duct of Santorini through the minor papilla.13,14 Chronic alcohol consumption is felt to contribute by increasing the viscosity of the pancreatic juice, leading to Brunner gland hyperplasia and causing occlusion or dysfunction of the mi-nor papilla.13,14 Another proposed mechanism is pancreatic heterotopia in the minor papilla causing dysfunction and oc-clusion of the papilla.13 Other factors, such as fibrous scar-ring secondary to peptic ulcers, gastric and duodenal resec-tions, or true duodenal wall cysts may also be related.5
The treatment of choice is conservative in the acute phase of groove pancreatitis and includes bowel rest, analgesia, and intravenous fluids.10 Patients may have a protracted course requiring supplemental nutrition with tube feeding or total parenteral nutrition. One report demonstrated success-ful treatment of groove pancreatitis by endoscopic drainage of the accessory pancreatic duct via the minor papilla in patients where obstruction of the minor papilla appears to play a role in the pathogenesis.15 Groove pancreatitis can be resistant to medical treatment and require surgical inter-vention. The surgical treatment of choice is a Whipple pro-cedure (pancreaticoduodenectomy) or a pylorus-preserving pancreaticoduodenectomy.2
In our series of 4 patients, a combination of clinical and ra-diological features was used to make the diagnosis of groove
pancreatitis. Although other case reports show common al-cohol use and a male predominance, 2 of our patients were female and only 1 patient had a history of significant alcohol use. Although rare, this condition should be considered in the differential diagnosis of pancreatic head masses with signs of duodenal wall infiltration. Alternatively, a careful and thorough evaluation to rule out adenocarcinoma should be performed before a definitive diagnosis of groove pancreati-tis is established.
Disclosures
Author contributions: All authors contributed equally to the preparation of this manuscript. RA Burbridge is the author guarantor.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
Received: December 20, 2013; Accepted: March 4, 2014
References1. Manzelli A, Petrou A, Lazzaro A, et al. Groove pancreatitis. A mini-series
report and review of the literature. JOP. 2011;12(3):230–3. 2. Balakrishnan V, Chatni S, Radhakrishnan L, et al. Groove pancreatitis: A
case report and review of literature. JOP 2007;8(5):592–7. 3. Levenick JM, Gordon SR, Sutton JE, et al. A comprehensive, case-based
review of groove pancreatitis. Pancreas. 2009;38(6):e169–e175. 4. Levenick JM, Sutton JE, Smith KD, et al. Pacreaticoduodenectomy for
the treatment of groove pancreatitis. Dig Dis Sci. 2012;57(7):1954–8. 5. Triantopoulou C, Dervenis C, Giannakou N, et al. Groove pancreatitis: A
diagnostic challenge. Eur Radiol. 2009;19(7):1736–43. 6. Becker V. Proceedings: Fundamental morphological aspects of
acute and chronic pancreatitis [in German]. Langenbecks Arch Chir. 1973;334:317–22.
7. Stolte M, Weiss W, Volkholz H, Rösch W. A special form of seg-mental pancreatitis: Groove pancreatitis. Hepatogastroenterology. 1982;29(5):198–208.
Table 2. Differentiation of Groove Pancreatitis and Pancreatic Adenocarcinoma Based on Imaging Features
Imaging Groove Pancreatitis Pancreatic Adenocarcinoma
CT Hypoechoic mass between pancreatic head and duodenum, duode-nal wall thickening, cystic changes, and stenosis, normal-to-mildly dilated common bile duct
Pancreatic head mass, with or without dilation of common bile duct and/or pancreatic duct
MRI Sheet-like mass in groove, duodenal thick-ening, common bile duct stenosis
Enlarged mass mostly in pan-creatic head, with widening of the space between the distal pancreatic duct and common bile duct and duodenal lumen
ERCP/EUS Smooth tubular common bile duct stenosis
Irregular common bile duct stenosis, vascular encasement
CT = computed tomography; ERCP = endoscopic retrograde cholangiopancreatography; EUS = endoscopic ultrasonography; MRI = magnetic resonance imagingAdapted from Levenick et al4 and Malde et al14

Publish your work in ACG Case Reports JournalACG Case Reports Journal is a peer-reviewed, open-access publication that provides GI fellows, private practice clinicians, and other members of the health care team an opportunity to share interesting case reports with their peers and with leaders in the field. Visit http://acgcasereports.gi.org for submission guidelines. Submit your manuscript online at http://mc.manuscriptcentral.com/acgcr.
Black et al
acgcasereports.gi.org
Groove Pancreatitis
157 ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014
8. Becker V, Mischke U. Groove pancreatitis. Int J Pancreatol. 1991;10(3–4):173–82.
9. Yamaguchi K, Tanaka M. Groove pancreatitis masquerading as pancre-atic carcinoma. Am J Surg. 1992;163(3):312–6.
10. Shudo R, Yazaki Y, Sakurai S, et al. Groove pancreatitis: Report of a case and review of the clinical and radiologic features of groove pancreatitis reported in Japan. Int Med. 2002;41(7):537–42.
11. Gabata T, Kadoya M, Terayama N, et al. Groove pancreatic carcinomas: Radiological and pathological findings. Eur Radiol. 2003;13:1679–84.
12. Newton B, Rittenbury M, Anderson M. Extrahepatic biliary obstruction associated with pancreatitis. Ann Surgery. 1983;197(6):645–53.
13. Chatelain, D, Vibert E, Yzet T, et al. Groove pancreatitis and pancreatic heterotopia in the minor duodenal papilla. Pancreas. 2005;30(4):e92–e95.
14. Malde DJ, Oliveira-Cunha M, Smith AM. Pancreatic carcinoma masquer-ading as groove pancreatitis: Case report and review of literature. JOP. 2011;12(6):598–602.
15. Isayama H, Kawabe T, Komatsu Y, et al. Successful treatment for groove pancreatitis by endoscopic drainage via the minor papilla. Gastroinest Endosc. 2005;61(1):175–8.

ACG CASE REPORTS JOURNAL
acgcasereports.gi.org ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014158
CASE REPORT | BILIARY
Bouveret’s Syndrome with Severe Esophagitis and a Purulent FistulaRami Bonam, MD1, Zahid Vahora, MD2, Glenn Harvin, MD2, and William Leland, MD2
1Mercer University School of Medicine, Macon, GA 2Internal Medicine, Brody School of Medicine at East Carolina University, Greenville, NC
AbstractBouveret’s syndrome is a rare variant of gallstone ileus with an overall incidence of 1–3%. It is a rare cause of gastric outlet obstruction resulting from the passage and impaction of a large gallstone through a cholecysto-duodenal fistula. A combination of diagnostic modalities is often required for a diagnosis. Management options include endoscopy and surgery. The most commonly performed procedures are enterolithotomy or gastrostomy, either alone or with cholecystectomy and fistula repair. We describe a unique variant of chronic Bouveret’s syn-drome with the unusual associations of severe esophagitis and a purulent fistula.
IntroductionBouveret’s syndrome is a cause of gastric outlet obstruction that results from the passage and impaction of a large gallstone through a cholecystoduodenal fistula. Bouveret first published 2 cases of this syndrome in 1896.1 It tends to occur more commonly in women, has a mean age of 74 years, and has an overall incidence of 1–3%.2 Various endoscopic and surgical techniques have been utilized in the management of Bouveret’s syndrome, and a number of variants of the syndrome have been reported. We describe a unique variant: chronic Bouveret’s syndrome characterized by the unusual associations of severe esophagitis and a purulent fistula.
Case ReportAn 81-year-old Caucasian female with a history of gastroesophageal reflux disease (GERD) and atrial fibrillation was admitted to hospital with a 1-week history of worsening emesis and 2 days of inability to tolerate oral intake. She denied any sick contacts, fever, chills, diarrhea, melena, or abdominal pain. The patient related a similar episode 4 months prior that resolved spontaneously. Work-up at that time included a negative abdominal x-ray. Since then, she had reduced her meal sizes to avoid symptoms and had lost 30 lbs.
Her abdominal exam was unremarkable. Laboratory examination showed normal hemoglobin, white blood cell 20,000/uL, normal liver enzymes, and hypokalemic hypochloremic metabolic alkalosis. An abdominal x-ray showed pneumobilia with no small bowel obstruction. An abdominal computed tomography (CT) confirmed the pneumobilia and revealed a 2.5-cm outpouching in the duodenal bulb suspicious for duodenal diverticula or duodenal ulcer (Figure 1). Esophagogastroduodenoscopy EGD showed severe esophagitis (Figure 2) and a large gallstone completely obstructing the proximal duodenum with surrounding purulent material (Figure 3).
The area of obstruction was impassable endoscopically. Endoscopic lithotripsy was performed by breaking the stone and removing debris via forceps, water pick, snares, balloon sweeps, and a variety of nets. The scope was then advanced, and multiple pieces of stones fell into the distal duodenum. We noted a fistula extending
ACG Case Rep J 2014;1(3):158–160. doi:10.14309/crj.2014.36. Published online: April 4, 2014.
Correspondence: Glenn Harvin, Brody School of Medicine at East Carolina University, Internal Medicine, 521 Moye Boulevard, Greenville, NC, 27834 ([email protected]; [email protected]).
Copyright: © 2014 Bonam et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
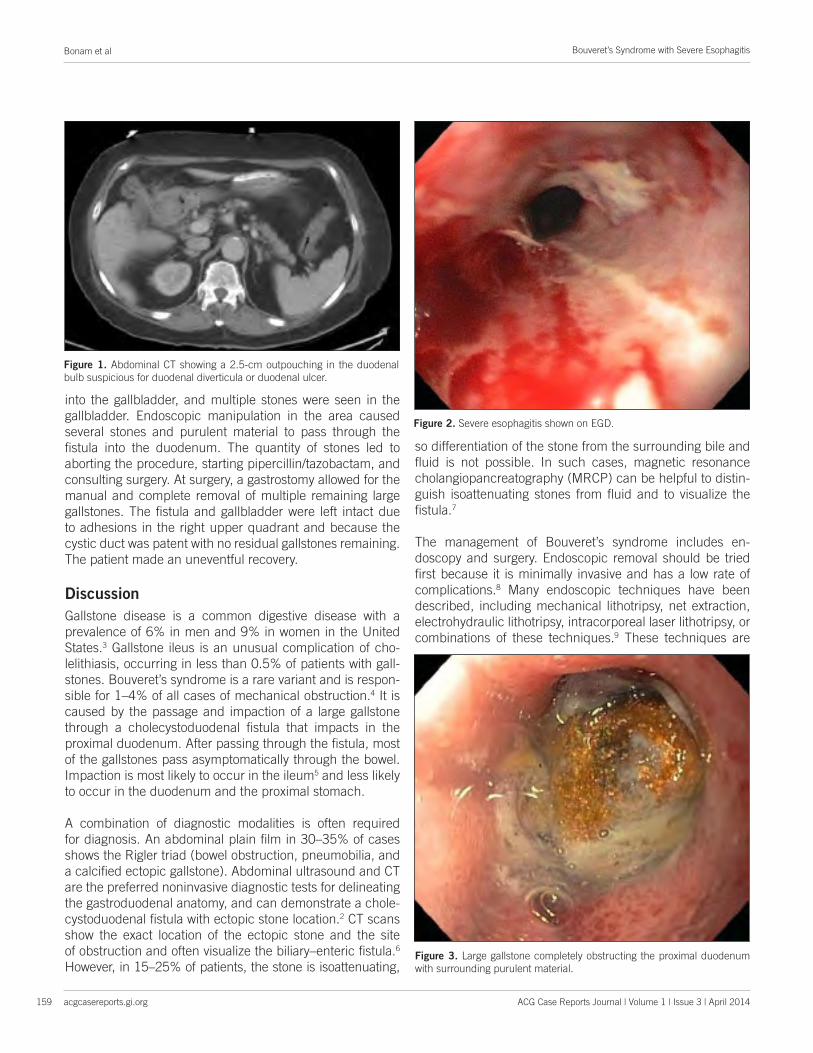
Bouveret’s Syndrome with Severe Esophagitis
acgcasereports.gi.org ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014
Bonam et al
159
into the gallbladder, and multiple stones were seen in the gallbladder. Endoscopic manipulation in the area caused several stones and purulent material to pass through the fistula into the duodenum. The quantity of stones led to aborting the procedure, starting pipercillin/tazobactam, and consulting surgery. At surgery, a gastrostomy allowed for the manual and complete removal of multiple remaining large gallstones. The fistula and gallbladder were left intact due to adhesions in the right upper quadrant and because the cystic duct was patent with no residual gallstones remaining. The patient made an uneventful recovery.
DiscussionGallstone disease is a common digestive disease with a prevalence of 6% in men and 9% in women in the United States.3 Gallstone ileus is an unusual complication of cho-lelithiasis, occurring in less than 0.5% of patients with gall-stones. Bouveret’s syndrome is a rare variant and is respon-sible for 1–4% of all cases of mechanical obstruction.4 It is caused by the passage and impaction of a large gallstone through a cholecystoduodenal fistula that impacts in the proximal duodenum. After passing through the fistula, most of the gallstones pass asymptomatically through the bowel. Impaction is most likely to occur in the ileum5 and less likely to occur in the duodenum and the proximal stomach.
A combination of diagnostic modalities is often required for diagnosis. An abdominal plain film in 30–35% of cases shows the Rigler triad (bowel obstruction, pneumobilia, and a calcified ectopic gallstone). Abdominal ultrasound and CT are the preferred noninvasive diagnostic tests for delineating the gastroduodenal anatomy, and can demonstrate a chole-cystoduodenal fistula with ectopic stone location.2 CT scans show the exact location of the ectopic stone and the site of obstruction and often visualize the biliary–enteric fistula.6
However, in 15–25% of patients, the stone is isoattenuating,
so differentiation of the stone from the surrounding bile and fluid is not possible. In such cases, magnetic resonance cholangiopancreatography (MRCP) can be helpful to distin-guish isoattenuating stones from fluid and to visualize the fistula.7
The management of Bouveret’s syndrome includes en-doscopy and surgery. Endoscopic removal should be tried first because it is minimally invasive and has a low rate of complications.8 Many endoscopic techniques have been described, including mechanical lithotripsy, net extraction, electrohydraulic lithotripsy, intracorporeal laser lithotripsy, or combinations of these techniques.9 These techniques are
Figure 2. Severe esophagitis shown on EGD.
Figure 3. Large gallstone completely obstructing the proximal duodenum with surrounding purulent material.
Figure 1. Abdominal CT showing a 2.5-cm outpouching in the duodenal bulb suspicious for duodenal diverticula or duodenal ulcer.

Publish your work in ACG Case Reports JournalACG Case Reports Journal is a peer-reviewed, open-access publication that provides GI fellows, private practice clinicians, and other members of the health care team an opportunity to share interesting case reports with their peers and with leaders in the field. Visit http://acgcasereports.gi.org for submission guidelines. Submit your manuscript online at http://mc.manuscriptcentral.com/acgcr.
Bonam et al
acgcasereports.gi.org
Bouveret’s Syndrome with Severe Esophagitis
160 ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014
more successful for proximal gallstone obstruction. The suc-cess rate of these time-consuming procedures is only 9%.10
Failed endoscopic attempts and distal migration of gall-stones after dislodgement are indications for surgery. The most commonly performed procedures are enterolithotomy or gastrostomy, either alone or with cholecystectomy and fis-tula repair. A fistula may spontaneously close, and repair may be unnecessary if the cystic duct is patent and no re-sidual gallstones are present.4
We suspect that this patient developed a partial obstruction approximately 4 months prior to our intervention. The pro-longed partial obstruction led to significant weight loss and the development of esophagitis. The chronic course of this patient’s illness is a unique presentation of Bouveret’s syn-drome. Perhaps the development of inflammation from the purulent fistula and elevated WBC count led to edema and complete obstruction. In published case reports of gallstone ileus and Bouveret’s syndrome, patients present with acute symptoms of small bowel obstruction typically within 1 week. Weight loss in Bouveret’s syndrome is reported in less than 20% of patients.2 A PubMed review of 20 published cases and a comprehensive review of 128 cases by Cappel and Da-vis2 revealed only 2% of Bouveret’s syndrome cases present-ed with esophagitis and none of them had a purulent fistula.
Gallstone-related obstruction of the small bowel is a rare oc-currence. Chronic Bouveret’s syndrome is possible when an elderly patient presents with upper gastrointestinal obstruc-tion symptoms, pneumobilia, significant weight loss, and esophagitis. In this patient, a purulent fistula and elevated WBC count was associated with the worsening of clinical symptoms. Antibiotics were instituted to prevent further complications associated with endoscopic instrumentation. Chronic Bouveret’s syndrome should be added to the grow-ing list of variants that have been reported in the literature.
Disclosures Author contributions: All authors contributed equally to the manuscript. R. Bonam is the article guarantor.
Financial disclosure: No conflicts of interest or funding to disclose. Informed consent was obtained for this case report.
Received: November 24, 2013; Accepted: February 18, 2014
References1. Bouveret L. Stenose du pylore adherent a la vesicule [in French]. Rev
Med (Paris). 1896;16:1–16.2. Cappell MS, Davis M. Characterization of Bouveret’s syndrome:
A comprehensive review of 128 cases. Am J Gastroenterol. 2006;101(9):2139–46.
3. Everhart JE, Khare M, Hill M, Maurer KR. Prevalence and ethnic dif-ferences in gallbladder disease in the United States. Gastroenterology. 1999;117(3):632–9.
4. Reisner RM, Cohen JR. Gallstone ileus: A review of 1001 reported cases. Am Surg. 1994;60(6):441–6.
5. Sánchez MR, Sánchez F, Bouzón Caamaño G, et al. Síndrome de Bouveret: A propósito de un caso [in Spanish]. Rev Clín Esp. 2003;203(8):399–400.
6. Lassandro R, Gagliardi N, Scuderi M, et al. Gallstone ileus analysis of radiological findings in 27 patients. Eur J Radiol. 2004;50:23–9.
7. Pickhardt PJ, Friedland JA, Hruza DS, Fisher AJ. CT, MR cholangio-pancreatography, and endoscopy findings in Bouveret’s syndrome. Am J Roentgenol. 2003;180(4):1033–5.
8. Bedogni G, Contini S, Meinero M, et al. Pyloroduodenal obstruction due to a biliary stone (Bouveret’s syndrome) managed by endoscopic extraction. Gastrointest Endosc. 1985;31(1):36–8.
9. Thompson RJ, Gidwani A, Caddy G, McKenna E, McCallion K. Endo-scopically assisted minimally invasive surgery for gallstones. Ir J Med Sci. 2009;178(1):85–7.
10. Lowe AS, Stephenson S, Kay CL, May J. Duodenal obstruction by gall-stones (Bouveret’s syndrome): A review of the literature. Endoscopy. 2005;37(1):82–7

ACG CASE REPORTS JOURNAL
acgcasereports.gi.org ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014161
CASE REPORT | BILIARY
A Case of an Ectopic Ampulla of Vater in the Pyloric ChannelSunil Dacha, MD1, Xiao Jing Wang, MD2, and Emad Qayed, MD1
1Division of Digestive Diseases, Department of Internal Medicine, Emory University School of Medicine, Atlanta, GA2Department of Internal Medicine, Emory University School of Medicine, Atlanta, GA
AbstractA 51-year-old male presented with abdominal pain and jaundice. He was subsequently diagnosed with choles-tatic jaundice and cholangitis. A side-viewing duodenoscope failed to identify the ampulla of Vater in the second portion of duodenum. A regular gastroscope was used, and an ectopic ampulla of Vater was identified in the pyloric channel.
IntroductionThe ampulla of Vater encompasses the openings of both the common bile duct and pancreatic duct. It is typi-cally located within the wall of the duodenum, surrounded by the small circular and longitudinal muscular seg-ments that comprise the sphincter of Oddi. We report the case of a man who presented with cholestatic jaundice and cholangitis, and was found to have an ectopic ampulla of Vater in the pyloric channel.
Case ReportA 51-year-old male presented with complaints of intermittent abdominal pain and chills for a few days prior to ad-mission. He was afebrile with normal vital signs. His physical examination was significant for scleral icterus and a benign abdominal exam. Laboratory data were significant for an aspartate transaminase (AST) of 153 IU/L, alanine transaminase (ALT) of 177 IU/L, alkaline phosphatase of 169 IU/L, total bilirubin of 5.5 mg/dL, and a direct bilirubin of 3.5 mg/dL.
Computed tomography (CT) suggested possible annular pancreas with pneumobilia. Right upper quadrant ultrasound revealed cholelithiasis, pneumobilia, and a common bile duct diameter of 8 mm. Magnetic resonance cholangiopancreatography (MRCP) showed a possible annular pancreas with hepatic and pancreatic duct dilation. On attempted endoscopic retrograde cholangiopancreatography (ERCP), the ampulla of Vater was not visualized in the second portion of the duodenum. A regular gastroscope was used for visualization and revealed a 2-cm gastric ulcer in the distal antrum with significant surrounding inflammation (Video 1). Distal to the ulcer in the pyloric chan-nel, two orifices were identified. One of them was draining bile and the other one was draining clear liquid. This was consistent with the biliary orifice and pancreatic orifice, respectively (Figure 1). A sphincterotome with a 0.035 wire was used to enter the orifice that was draining bile, which resulted in deep common bile duct cannulation.
A cholangiogram showed mild intrahepatic duct dilation, common bile duct dilation (to 1 cm), and a “hook–shaped” configuration of the distal common bile duct. These findings were consistent with an ectopic ampulla within the pylorus. A balloon occlusion cholangiogram showed a distal common bile duct diameter of 7 mm and a round filling defect consistent with a bile duct stone (Figure 2). A 3-mm limited sphincterotomy was performed at the ampullary orifice, followed by balloon dilation to 10 mm for 45 seconds under endoscopic and fluoroscopic guidance.
ACG Case Rep J 2014;1(3):161–163. doi:10.14309/crj.2014.37. Published online: April 4, 2014.
Correspondence: Sunil Dacha, 615 Michael Street Ste. 200, Atlanta, GA 30322 ([email protected]).
Copyright: © 2014 Dacha et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

Ectopic Ampulla of Vater in the Pyloric Channel
acgcasereports.gi.org ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014
Dacha et al
162
and cardia.1 Most of the reported cases suggest the pres-ence of the major papilla in the stomach. The minor papilla is reportedly found in the distal duodenum.2 Based on few published reports, there appears to be an increased risk for choledocholithiasis due to anomalous bile drainage and lack of sphincter control mechanisms. Pancreatobiliary secre-tions can lead to mucosal damage with ulcer formation. The anomalous location in the pylorus can facilitate reflux of gas-tric contents into the biliary tree, predisposing to biliary tree injury and cholangitis.2,3
Endoscopists who perform ERCP should be aware of this rare anomaly. In cases where the ampulla cannot be seen in a normal anatomical location, an ectopic ampulla should be suspected, and the endoscopist must carefully examine the stomach and the duodenum. As in our patient, a regular, forward-viewing gastroscope can be used to better visualize the stomach. A large sphincterotomy should be avoided due to increased risk of perforation. Ampullary balloon dilation is recommended to extract large bile duct stones.1,2,4
Disclosures
Author contributions: All authors contributed equally to the manuscript. S. Dacha is the article guarantor.
Financial disclosure: The authors disclose no conflict of in-terest or financial support.
Informed consent was obtained for this case report.
Figure 1. Two orifices in the pyloric channel distal to a 2-cm gastric ulcer iden-tified by regular gastroscope, consistent with the biliary and pancreatic orifices.
Video 1. Gastroscope visualization of the distal antrum and two orifices in the pyloric channel. Please view the video at acgcasereports.gi.org/?p=1997.
Figure 2. A balloon occlusion cholangiogram showing a distal common bile duct diameter of 7 mm and a round filling defect consistent with a bile duct stone.
Following balloon dilation, there was minor bleeding from the ampullary orifice. Hemostasis was achieved with injec-tion of 8 mL of epinephrine. The bile duct stone was suc-cessfully extracted using a balloon catheter. Biopsies ob-tained from the periampullary ulcer revealed acute fibrinous inflammation with no evidence of malignancy. The patient subsequently underwent laparoscopic cholecystectomy and continues to do well after 1 year of follow-up.
DiscussionEctopic location of ampulla in the stomach or first, third, or fourth part of the duodenum is a very rare congenital anom-aly. The reported incidence of anomalous termination of bile duct is 5.6–23%; the wide range is due to the limited number of cases, but this condition is being reported more frequently due the extensive availability of ERCP.1,2 The exact etiology of this congenital anomaly remains unclear, and is believed to be an abnormality during the embryonic developmental period. The liver and the biliary tract are formed from the hepatic diverticulum; the cranial part (pars hepatica) gives rise to the intrahepatic and common hepatic ducts. It has been proposed that an earlier subdivision of the hepatic di-verticulum during embryogenesis could cause the common bile duct to empty into ectopic locations.2
Ectopic biliary drainage into the stomach is most commonly reported in the body of the stomach, followed by the antrum

Publish your work in ACG Case Reports JournalACG Case Reports Journal is a peer-reviewed, open-access publication that provides GI fellows, private practice clinicians, and other members of the health care team an opportunity to share interesting case reports with their peers and with leaders in the field. Visit http://acgcasereports.gi.org for submission guidelines. Submit your manuscript online at http://mc.manuscriptcentral.com/acgcr.
Dacha et al
acgcasereports.gi.org
Ectopic Ampulla of Vater in the Pyloric Channel
163 ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014
Received: August 29, 2013; Accepted: January 16, 2014
References1. Saritas U, Senol A, Ustundag Y. The clinical presentations of ectopic
biliary drainage into duodenal bulbus and stomach with a thorough review of the current literature. BMC Gastroenterol. 2010;10:2.
2. Guerra I, Rábago LR, Bermejo F, et al. Ectopic papilla of Vater in the pylorus. World J Gastroenterol. 2009;15(41):5221–3.
3. Lee SS, Kim MH, Lee SK, et al. Ectopic opening of the common bile duct in the duodenal bulb: Clinical implications. Gastrointest Endosc. 2003;57(6):679–82.
4. Disibeyaz, Selcuk, et al. Anomalous opening of the common bile duct into the duodenal bulb: Endoscopic treatment. BMC Gastroenterol. 2007;7:26.

ACG CASE REPORTS JOURNAL
acgcasereports.gi.org ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014164
CASE REPORT | LIVER
Sarcoidosis Presenting as Necrotizing Sarcoid Granulomatosis of the Liver, Sclerosing Cholangitis, and Gastric UlcerNjideka Momah, MD1, Adetola Otesile, BSc2, Rishi Pawa, MD1, and Steve Shedlofsky, MD1
1University of Kentucky, Digestive Diseases and Nutrition, Lexington, KY2University of Kentucky, College of Medicine, Lexington, KY
AbstractSarcoidosis is a multisystem granulomatous disease. The liver is affected in up to 50–90% of cases. Sarcoidosis typically presents as non-necrotizing epithelioid granuloma. The occurrence of non-infective necrotizing sarcoid granuloma (NSG) is infrequent, and the finding of NSG in the liver is rare. We report a case of NSG of the liver and lymph nodes, granulomatous gastric ulcer, and secondary cholangitis coexisting in a patient. We discuss the clinical features of the case and briefly review NSG. There is only 1 previously reported case of NSG of the liver in literature.
IntroductionSarcoidosis is a multisystem granulomatous disease that has a prevalence of approximately 3–5 per 100,000. The incidence is highest among young adults aged 25–40 years old. The immunopathologic basis is complex and involves interplay between genetic predisposition, sarcoid antigen, and immune cells. The liver is affected in to 50–90% of cases. Sarcoidosis typically presents as non-necrotizing epithelioid granuloma, and presenta-tion as non-infective necrotizing sarcoid granuloma (NSG) is infrequent. The finding of NSG in the liver is rare.
Case ReportA 26-year-old African-American male was referred for epigastric and right upper quadrant (RUQ) abdominal pain and pruritus for 1 year, with associated nausea and intermittent vomiting. He denied nonsteroidal anti-inflam-matory use. Physical exam revealed scleral icterus, generalized lymphadenopathy, and tender hepatospleno-megaly. To evaluate his symptoms, an esophagogastroduodenoscopy (EGD) was done and showed esophageal varices and a gastric ulcer. Gastric ulcer biopsy showed chronic active gastritis and acute inflammation with focal granuloma, with stains negative for Helicobacter pylori. RUQ ultrasound showed gallbladder wall thickening and a cholecystectomy was planned; during the operation, the gallbladder was noted to be adherent to the liver and could not be dissected. The liver appeared nodular, so a wedge biopsy was performed, which demonstrated granulomatous inflammation with areas of necrotizing granulomata and portal triads that were difficult to locate.
Laboratory tests showed cholestatic liver pattern (Table 1). He had normal lipase, with negative tests for vi-ral hepatitis and HIV. Ferritin, cerruloplasmin, and alpha-1 antitrypsin serum levels were normal. Cytoplasmic anti-neutrophil cytoplasmic antibodies (C-ANCA), perinuclear anti-neutrophil cytoplasmic antibodies (P-ANCA), anti-nuclear, anti-mitochondrial, anti-smooth muscle, and anti-liver kidney antibodies were negative. Tests for Toxoplasma gondii, Bartonella, Brucella, Treponema pallidum, and Histoplasma were negative. Purified protein derivative (PPD) skin test was non-reactive. Chest computed tomography (CT) showed hilar and mediastinal lymphadenopathy. Abdominal CT showed hepatomegaly with asymmetric left lobe enlargement, splenomegaly,
ACG Case Rep J 2014;1(3):164–166. doi:10.14309/crj.2014.38. Published online: April 4, 2014.
Correspondence: Njideka Momah, Department of Digestive Diseases and Nutrition, University of Kentucky, 800 Rose St, Lexington, KY, 40536-0298 ([email protected]).
Copyright: © 2014 Momah et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

Sarcoidosis Presenting as NSG
acgcasereports.gi.org ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014
Momah et al
165
and retroperitoneal and periportal lymphadenopathy. A magnetic resonance cholangiogram showed sclerosing chol-angitis (Figure 1). An endoscopic retrograde cholangiogram (ERCP) was done to evaluate for extrahepatic biliary obstruc-tion and showed a normal common bile duct, though the left hepatic duct showed diffuse rarefaction and the right hepatic duct did not opacify. To confirm that the lymphade-nopathy was part of the same disease process, a right cervi-cal lymph node biopsy was done, which showed necrotizing and non-necrotizing granulomatous inflammation (Figure 2). Gram stains, acid fast bacilli (AFB), and Warthin-Starry stains were negative for microorganisms. Cultures for AFB, anaerobic, and fungal organisms were negative. Given these findings, the patient was diagnosed with sarcoidosis.
The patient was started on 40 mg of prednisone. He showed an improvement in abdominal pain and a decrease in total
Figure 1. Magnetic resonance cholangiogram of the liver showing hepato-megaly and sclerosing cholangitis.
Figure 2. Lymph node biopsy showing both necrotizing granulomas (red arrows) and non-necrotizing granulomas (black arrows).
Table 1. Patient Laboratory Values at Baseline and After 1 Year Of Prednisone
Baseline After 1 Year of Prednisone
WBC, k/uL 3.4 4.3
Hemoglobin, g/dL 10.6 12.8
Hematocrit, g/dL 31.1 38.6
AST, U/L 162 96
ALT, U/L 151 117
ALP, U/L 993 288
GGT, U/L 344 NA
T. bilirubin, mg/dL 8.6 1.4
T. protein, g/dL 8.8 7.4
Albumin, g/dL 2.1 2.9
INR 1.1 1.1
ACE 70 10
ACE = angiotensin-converting enzyme; AST = aspartate aminotransferase; ALT = alanine transami-nase; ALP = alkaline phosphatase; GGT = gamma glutamyl aminotransferase; INR = international normalized ratio; NA = not applicable; WBC = white blood cell
bilirubin. He was discharged with a plan for outpatient man-agement. His total bilirubin decreased (Table 1) and he con-tinued to require prednisone therapy.
DiscussionSarcoidosis is a multisystem disease. The liver is commonly affected, but hepatic presentations are usually mild.1 Up to 3% of patients develop severe hepatic involvement with por-tal hypertension and esophageal varices.2 Sarcoidosis rarely involves the luminal gastrointestinal tract and is usually as-ymptomatic. It is diagnosed on the basis of clinical presen-tation, biochemistry, radiology, and histopathology. The fea-tures depend on the affected organ. Hepatic sarcoidosis may present as fatigue, RUQ abdominal pain, pruritus, jaundice, weight loss, and fever.3 Features of esophageal sarcoidosis include dysphagia from impaired motility, esophagitis, stric-ture, or extrinsic compression from paraesophageal nodes.4 Gastric presentation includes epigastric pain, ulcers, gastric polyps/nodules, or linitis plastica-like lesions.4 Ten percent of individuals with sarcoidosis have gastric involvement with normal appearing mucosa.5 Involvement of the small bowel may clinically present with abdominal discomfort, malab-sorption, protein losing enteropathy, gastrointestinal bleed, or intestinal obstruction. Colonic manifestations include coli-tis, polyposis, or a mass.4
Our patient had compelling features of sarcoidosis, includ-ing including anergy to PPD, elevated serum angiotensin-converting enzyme (ACE) levels, a cholestatic liver biochem-istry, hilar and mediastinal lymphadenopathy, and histologic granulomas. The histology of sarcoidosis is typically described as non-necrotizing epithelioid granulomas, though necrotizing granuloma in the setting of sarcoidosis has been described.6

Publish your work in ACG Case Reports JournalACG Case Reports Journal is a peer-reviewed, open-access publication that provides GI fellows, private practice clinicians, and other members of the health care team an opportunity to share interesting case reports with their peers and with leaders in the field. Visit http://acgcasereports.gi.org for submission guidelines. Submit your manuscript online at http://mc.manuscriptcentral.com/acgcr.
Momah et al
acgcasereports.gi.org
Sarcoidosis Presenting as NSG
166 ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014
There are 3 histologic categories of hepatic sarcoidosis: cholestatic, necroinflammatory, and vascular patterns.7 Our patient falls in to the necroinflammatory pattern, which has chronic portal inflammation and spotty necrosis.
Liebow first described non-infective necrotizing granulomas and coined the term necrotizing sarcoid granuloma (NSG) in 1973.8 The majority of reported cases of NSG affect the lungs, but cases involving the skin, subcutaneous tissues, kidney, colon, and orbit have been reported. There is only 1 report of NSG involving the liver,7 but the clinical presenta-tion of the patient was not described. There is currently no consensus on whether NSG is a manifestation of sarcoid-osis or a distinct vasculitic entity. Saldana et al believed that NSG was a different entity. Their patients with NSG lacked extra-thoracic involvement, had normal serum ACE levels, and only a few had hilar adenopathy.9 Churg et al concluded that NSG was a histologic manifestation of nodular sarcoid.10
There is no confirmatory test for sarcoidosis. The diagno-sis is based on excluding other causes of granulomatosis, such as primary biliary cirrhosis, Crohn’s disease, tuberculo-sis, brucellosis, viral hepatitis, fungal infections, lymphoma, and drugs. The treatment of NSG is empiric. Oral predni-sone 40–60 mg daily for 8 weeks with a slow taper based on clinical response has been recommended.11 The unique features of this case are 2 rare manifestations of sarcoid-osis—NSG and a gastric ulcer—in the same patient, which has not been previously reported.
Disclosures
Author contributions: N. Momah designed the study and re-vised and critically reviewed the manuscript for content. A. Otesile obtained and edited the images. R. Pawa critically reviewed the manuscript. S. Shedlofsky revised and critically reviewed the manuscript for content, and is the article guar-antor.
Financial disclosure: The authors do not have any financial conflict of interest to disclose.
Informed consent was obtained for this case report.
Received: November 28, 2013; Accepted: March 18, 2014
References1. Flamm SL. Granulomatous liver disease. Clin Liver Dis. 2012;16(2):387–96.2. Judson MA. Hepatic, splenic, and gastrointestinal involvement with sar-
coidosis. Semin Respir Crit Care Med. 2002;23(6):529–41.3. Bakker GJ, Haan YC, Maillette de Buy Wenniger LJ, Beuers U. Sarcoid-
osis of the liver: To treat or not to treat? Neth J Med. 2012;70(8):349–56.4. Patel, A, et al. GI tract sarcoidosis: A Review. Prac Gastro. 2013;37(5):25–38.5. Palmer ED. Note on silent sarcoidosis of the gastric mucosa. J Lab Clin
Med. 1958;52(2):231–4.6. Strickland-Marmol LB, Fessler RG, Rojiani AM. Necrotizing sarcoid
granulomatosis mimicking an intracranial neoplasm: Clinicopathologic features and review of the literature. Mod Pathol. 2000;13(8):909–13.
7. Devaney K, Goodman ZD, Epstein MS, et al. Hepatic sarcoidosis. Clinicopath-ologic features in 100 patients. Am J Surg Pathol. 1993;17(12):1272–80.
8. Liebow AA. The J. Burns Amberson lecture: Pulmonary angiitis and gran-ulomatois. Am Rev Respir Dis. 1973;108(1):1–17.
9. Tomashefski JF, Cagle PT, Farver CF, Fraire AE. Dail and Hammar’s Pul-monary Pathology. New York, NY: Springer; 2008.
10. Churg A, Carrington CB, Gupta R. Necrotizing sarcoid granulomatosis. Chest. 1979;76(4):406–13.
11. Yeboah, J, Afkhami M, Lee C, Sharma OP. Necrotizing sarcoid granulo-matosis. Curr Opin Pulm Med. 2012;18(5):493–8.

ACG CASE REPORTS JOURNAL
acgcasereports.gi.org ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014167
CASE REPORT | LIVER
Polymyositis Associated with Hepatitis B Virus Cirrhosis and Advanced Hepatocellular CarcinomaKessarin Thanapirom, MD, Satimai Aniwan, MD, and Sombat Treeprasertsuk, MD
Department of Medicine, Chulalongkorn University, Bangkok, Thailand
AbstractPolymyositis (PM) is an inflammatory condition of skeletal muscle and is believed to be a paraneoplastic syn-drome associated with various types of cancer. PM associated with chronic hepatitis B virus (HBV)-related hepatocellular carcinoma (HCC) is very rare. We report a case of advanced HCC with chronic HBV cirrhosis that presented with proximal muscle weakness. Further investigation showed elevation of muscle enzymes, myopathic pattern of electromyography (EMG), and evidence of myositis compatible with PM. Lamivudine and 1 mg/kg of oral prednisolone were given. Two sessions of transcatheter arterial chemoembolization (TACE) were performed and sorafenib was started. Muscle enzymes normalized after 6 weeks of treatment. Unfortunately, 5 months after treatment, patient was readmitted and died of severe bacterial pneumonia.
IntroductionPolymyositis (PM) is an idiopathic inflammatory myopathy. It is a systemic disease that affects skeletal muscles and results in proximal muscle weakness. PM is associated with malignancy in 10–15% of patients.1–3 The 3 most commonly associated cancers are nasopharyngeal, lung, and breast cancer.4 Hepatocellular carcinoma (HCC)-associated PM is quite rare. We report a case of hepatitis B virus (HBV) cirrhosis with advanced HCC presenting with PM.
Case ReportA previously healthy 56-year-old male presented with a 6-week history of fever. Two weeks prior to admission, he developed progressive proximal muscle weakness. Through work-up, he was diagnosed with chronic HBV cir-rhosis (Child-Pugh B; MELD 7) with advanced HCC. On physical examination, body temperature was 38°C, blood pressure was 120/75, and pulse rate was 92 bpm. Examination of the limbs showed normal tone without muscle wasting or tenderness. There was bilateral proximal weakness in both upper and lower limbs, with grade 3 of 5 in strength of both flexion and extension based on the Medical Research Council scale (MRC), with normal strength in distal limbs. His neck muscles were also weak. Deep tendon reflexes and sensation were normal. He had hepa-tomegaly and signs of chronic liver stigmata, but no ascites and no signs of hepatic encephalopathy. His Eastern Cooperative Oncology Group (ECOG) performance status score was 2.
Laboratory revealed albumin 2.2 g/dL, total protein 4.4 g/dL, aspartate aminotransferase (AST) 724 IU/L, alanine aminotransferase (ALT) 236 IU/L, total bilirubin 1.0 mg/dL, alkaline phosphatase 148 U/L, prothrombin time (PT) 14.1 s, international normalized ratio (INR) 1.14, and creatinine 0.8 mg/dL. His creatinine phosphokinase was 17,963 IU/L. Serum electrolytes and thyroid function tests were normal. His viral profiles were positive for HBV with DNA polymerase chain reaction (PCR) of 17,460 IU/mL. Tests for hepatitis C virus and HIV were negative. Alpha-fetoprotein (AFP) was 56,310 ng/mL (normal: <25 ng/mL). Autoantibodies including anti-dsDNA, anti-Jo-1, anti-neutrophilic cytoplasmic antibody, anti-RNP, anti-SSA ,and anti-SSB were negative.
ACG Case Rep J 2014;1(3):167–169. doi:10.14309/crj.2014.39. Published online: April 4, 2014.
Correspondence: Sombat Treeprasertsuk, Department of Medicine, Faculty of Medicine, Chulalongkorn University, Rama4 Road, Pathumwan district, Bangkok 10330, Thailand ([email protected]).
Copyright: © 2014 Thanapirom et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.

Polymyositis Associated with HBV Cirrhosis and HCC
acgcasereports.gi.org ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014
Thanapirom et al
168
Abdominal computed tomography (CT) showed liver cirrhosis with an ill-defined 12 x 7-cm, arterial-enhancing, heteroge-neous, hypodense lesion in the left lobe of the liver with in-creased enhancement on venous and delay phase and cen-tral necrosis. The CT showed 2 additional arterial-enhancing lesions, size 6 x 7 cm and 3 x 3 cm, with contrast washout in the venous phase at hepatic segments V/VIII and VII and a left main portal vein thrombosis (Figure 1). Liver biopsy of the largest lesion was performed to exclude secondary liver neoplasm. Histology showed poorly differentiated carcinoma positive for glypican 3 (GPC3) and negative for CK7, CK20, and hepatocyte paraffin 1 (Figure 2), which was consistent with the diagnosis of HCC.
Electromyography (EMG) showed low-amplitude, short-dura-tion action potentials with an early recruitment pattern, nor-mal nerve conduction study, and repetitive nerve stimulation. These findings were highly suggestive of a myopathic pattern (Figure 3). Muscle biopsy showed increased endomysial con-nective tissue and lymphocyte infiltration with necrotic and re-generating myofibers (Figure 4). No vasculitis or perifascicular pattern was seen, and a diagnosis was polymyositis (PM) was confirmed. Prednisolone 1 mg/kg for PM treatment and lami-vudine for preventing hepatitis B reactivation were given. Two sessions of transcatheter arterial chemoembolization (TACE) were performed. His creatinine kinase level decreased to nor-mal after 6 weeks of treatment, but his muscle strength did not improve. Unfortunately, 5 months after treatment, he was readmitted with severe bacterial pneumonia and died after 16 days of hospitalization.
DiscussionHCC-associated PM is a rare condition. Only 4 cases of PM associated with HCC have been reported (Table 1).5–8 A previ-ous study showed that large tumor size and a high AFP level were commonly found in HCC patients who had paraneoplas-tic syndromes.9 Our patient had both a large tumor and a very high AFP level. The pathogenesis of PM has not been identi-fied. A possible mechanism is that an autoimmune process triggered by the tumor leads to clonally expanded CD8-pos-itive cytotoxic T-cells that invade muscle fibers and express major histocompatibility complex (MHC) class 1 antigen and release cytokines, causing muscle inflammation.10,11 HBV-associated PM has also been reported,12 so it is possible that HCC, HBV, or both may have caused PM in this patient.
The role of steroids for treating HCC-associated PM is con-troversial. Physicians should be aware of an increased risk of infection when using high-dose corticosteroids in patients with advanced HCC and cirrhosis. Our patient’s ability to maintain daily life was limited by his weakness; therefore, cor-
Figure 1. (A) Contrast-enhanced abdominal CT showing liver cirrhosis, an ill-defined, arterial-enhancing heterogeneous isodense to hypodense lesion (arrow), and (B) increased enhancement in the left lobe of the liver on venous phase with central necrosis (arrow) and left main portal vein throm-bosis (asterisk).
Figure 2. Histological examination of liver mass with haematoxylin and eo-sin (H&E) stain showing poorly differentiated carcinoma (arrows).
Figure 3. Needle electromyography showing low-amplitude, short-duration action potentials and early recruitment pattern.
Figure 4. Muscle biopsy showing increased endomysial connective tissue infiltrated by lymphocytes with necrotic and regenerating myofibers.
A B

Publish your work in ACG Case Reports JournalACG Case Reports Journal is a peer-reviewed, open-access publication that provides GI fellows, private practice clinicians, and other members of the health care team an opportunity to share interesting case reports with their peers and with leaders in the field. Visit http://acgcasereports.gi.org for submission guidelines. Submit your manuscript online at http://mc.manuscriptcentral.com/acgcr.
Thanapirom et al
acgcasereports.gi.org
Polymyositis Associated with HBV Cirrhosis and HCC
169 ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014
ticosteroids were given after discussion with him. As a result of corticosteroid therapy, lamivudine was needed for preven-tion HBV reactivation. Lamivudine has good efficacy for this indication, particularly when the HBV DNA is low, as in our patient.13,14 Most patients with HCC-associated PM have had poor prognosis and treatment outcomes. Despite high-dose corticosteroids and surgery/chemoembolization for HCC man-agement,5–8 few patients had improvement of muscle weak-ness and all died from HCC-related causes within 6 months after diagnosis.
Disclosures
Author contributions: K. Thanapirom wrote the first draft, collected the data, and conducted the literature research. S. Aniwan conducted the literature research and drafted the article. S. Treeprasertsuk reviewed the final draft and is the article guarantor.
Financial disclosure: No conflicts of interest or sources of funding to report.
Informed consent was obtained for this case report.
Received: January 4, 2014; Accepted: March 18, 2014
References1. Buchbinder R, Forbes A, Hall S, et al. Incidence of malignant disease
in biopsy-proven inflammatory myopathy. A population-based cohort study. Ann Intern Med. 2001;134(12):1087–95.
2. Hill CL, Zhang Y, Sigurgeirsson B, et al. Frequency of specific cancer
types in dermatomyositis and polymyositis: A population-based study. Lancet. 2001;357(9250):96–100.
3. Sigurgeirsson B, Lindelöf B, Edhag O, Allander E. Risk of cancer in pa-tients with dermatomyositis or polymyositis. A population-based study. N Engl J Med. 1992;326(6):363–7.
4. Ungprasert P, Leeaphorn N, Hosiriluck N, et al. Clinical features of in-flammatory myopathies and their association with malignancy: A system-atic review in Asian population. ISRN Rheumatol. 2013;2013:509354.
5. Tekaya R, Abdelghni K, Abdelmoula L, et al. Hepatocellular carcinoma with polymyositis as an initial symptom: A case report. Acta Clin Belg. 2011;66(1):53–4.
6. Kishore D, Khurana V, Raj A, et al. Hepatocellular carcinoma pre-senting as polymyositis: A paraneoplastic syndrome. Ann Saudi Med. 2011;31:533–5.
7. Iba-Ba J, Assengone Zeh Y, Bignoumba Ibouili R, et al. Polymyositis and hepatocarcinoma: A case report from Gabon. Med Trop. (Mars). 2009;69(6):548.
8. Kim MJ, Kim JA, Sung MS, Min JK. Hepatocellular carcinoma, poly-myositis, rhabdomyolysis, and acute renal failure. J Korean Med Sci. 2004;19(6):891–4.
9. Luo JC, Hwang SJ, Wu JC, Li CP, Hsiao LT, Lai CR, Chiang JH, et al. Paraneoplastic syndromes in patients with hepatocellular carcinoma in Taiwan. Cancer. 1999;86:799–804.
10. Greenberg SA. Proposed immunologic models of the inflamma-tory myopathies and potential therapeutic implications. Neurology. 2007;69(21):2008–19.
11. András C, Ponyi A, Constantin T, et al. Dermatomyositis and polymyosi-tis associated with malignancy: A 21-year retrospective study. J Rheu-matol. 2008;35(3):438–44.
12. Wong MH, Sockalingam S, Zain A. Polymyositis associated with hepa-titis B: Management with entacavir and prednisolone. Int J Rheum Dis. 2011;14(3):e38–41.
13. Loomba R, Rowley A, Wesley R, et al. Systematic review: The effect of preventive lamivudine on hepatitis B reactivation during chemotherapy. Ann Intern Med. 2008;148:519–28.
14. Hsu C, Hsiung CA, Su IJ, et al. A revisit of prophylactic lamivudine for chemotherapy-associated hepatitis B reactivation in non-Hodgkin’s lymphoma: A randomized trial. Hepatology. 2008;47(3):844–53.
Table 1. Summary of Baseline Characteristics, Treatment, and Outcome of Patients with HCC-Associated Polymyositis
Case 15 Case 26 Case 37 Case 48
Sex M F M M
Age, y 72 50 37 55
Largest tumor size, cm 12 4.8 7 6
AFP, ng/mL Elevated Elevated N/A Normal
PM therapy Corticosteroid Corticosteroid Corticosteroid, methotrexate
Corticosteroid
HCC therapy Chemoembolization Surgery Bed supportive care Chemotherapy
Outcomes after therapy
Clinical weakness Not improved Improved Improved Not improved
Serum CPK N/A Decreased Decreased N/A
HCC-related death Yes Yes Yes Yes
Follow-up, mo 2 2 3 2
AFP = alpha-fetoprotein; CPK = creatinine phosphokinase; HCC = hepatocellular carcinoma; N/A = not applicable

ACG CASE REPORTS JOURNAL
acgcasereports.gi.org ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014170
CASE REPORT | PEDIATRICS
Ceftriaxone-Induced Gallstones: Case Report and Literature ReviewAditi Nayak, MD, and Adam Slivka, MD, PhD
Division of Gastroenterology, Hepatology and Nutrition, University of Pittsburgh Medical Center, Pittsburgh, PA
AbstractWe report a case of gallbladder and common bile duct stones occurring in a 14-year-old male who was exposed to ceftriaxone for 6 weeks. Ceftriaxone-induced gallstones are under-reported and remain an important cause of gallstones in patients exposed to this antibiotic. Gallstone development should be considered in the appropriate clinical context.
IntroductionGallstones are most commonly seen in middle-aged multiparous women who are obese. Cholesterol-containing stones are most common. Liver disease and hemolysis are risk factors for black pigment stones, and biliary in-fections can cause mixed pigment stones. Gallstones in children are relatively uncommon. We report a case of a young male with antibiotic-induced gallstones after exposure to ceftriaxone for 6 weeks.
Case ReportA 14-year-old male sustained a right anterior cruciate ligament (ACL) tear during a soccer match and underwent a partial physeal-sparing anatomic ACL reconstruction using his own hamstrings. Two weeks later, he presented with an infected joint and underwent incision and drainage with hardware removal. Cultures grew Serratia marc-essens; the patient had a peripherally inserted central catheter (PICC) line placed and was discharged on 6 weeks of ceftriaxone 2 gm IV daily.
During the last week of his ceftriaxone therapy, he developed intermittent right upper quadrant (RUQ) pain with-out nausea. His third attack in 72 hours prompted an emergency room visit. On exam, he was fit and thin with a non-toxic appearance, without fever, tachycardia, or hypotension. He was anicteric and had RUQ tenderness. The remainder of his exam was normal. He had no history of liver disease or hemolysis. There was no family or personal history of gallstones.
His laboratory tests showed a normal hemogram without leukocytosis. His electrolytes, blood urea nitrogen (BUN), and creatinine were normal. His total bilirubin was 1.2 mg/dL, alanine transaminase (ALT) 270 IU/L, and aspartate transaminase (AST) 463 IU/L. His amylase and lipase were normal. CT scan showed several densely calcified gallstones in the gallbladder (Figure 1) and 1 stone in the distal common bile duct (Figure 2) without evidence of acute cholecystitis. He was admitted to the hospital and underwent an ERCP with biliary sphinc-terotomy and extraction of yellow-green stone material (Figure 3), which did not appear like typical cholesterol, mixed pigment, or black pigment stones. He had no anatomic biliary abnormalities. He did well and underwent uneventful laparoscopic cholecystectomy the next day.
ACG Case Rep J 2014;1(3):170–172. doi:10.14309/crj.2014.40. Published online: April 4, 2014.
Correspondence: Adam Slivka, University of Pittsburgh School of Medicine, Gastroenterology, F 392 PUH 200 Lothrop Street, Pittsburgh, Pennsylvania 15213 ([email protected]).
Copyright: © 2014 Nayak et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
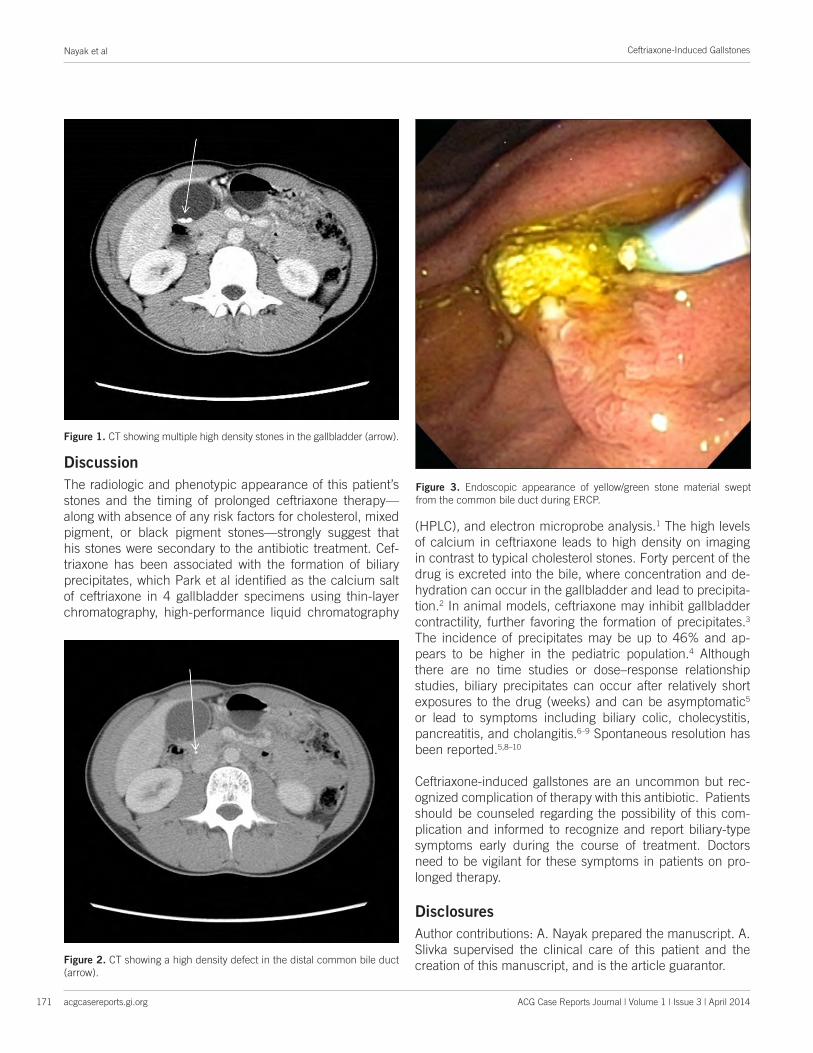
Ceftriaxone-Induced Gallstones
acgcasereports.gi.org ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014
Nayak et al
171
DiscussionThe radiologic and phenotypic appearance of this patient’s stones and the timing of prolonged ceftriaxone therapy—along with absence of any risk factors for cholesterol, mixed pigment, or black pigment stones—strongly suggest that his stones were secondary to the antibiotic treatment. Cef-triaxone has been associated with the formation of biliary precipitates, which Park et al identified as the calcium salt of ceftriaxone in 4 gallbladder specimens using thin-layer chromatography, high-performance liquid chromatography
(HPLC), and electron microprobe analysis.1 The high levels of calcium in ceftriaxone leads to high density on imaging in contrast to typical cholesterol stones. Forty percent of the drug is excreted into the bile, where concentration and de-hydration can occur in the gallbladder and lead to precipita-tion.2 In animal models, ceftriaxone may inhibit gallbladder contractility, further favoring the formation of precipitates.3 The incidence of precipitates may be up to 46% and ap-pears to be higher in the pediatric population.4 Although there are no time studies or dose–response relationship studies, biliary precipitates can occur after relatively short exposures to the drug (weeks) and can be asymptomatic5 or lead to symptoms including biliary colic, cholecystitis, pancreatitis, and cholangitis.6–9 Spontaneous resolution has been reported.5,8–10
Ceftriaxone-induced gallstones are an uncommon but rec-ognized complication of therapy with this antibiotic. Patients should be counseled regarding the possibility of this com-plication and informed to recognize and report biliary-type symptoms early during the course of treatment. Doctors need to be vigilant for these symptoms in patients on pro-longed therapy.
Disclosures
Author contributions: A. Nayak prepared the manuscript. A. Slivka supervised the clinical care of this patient and the creation of this manuscript, and is the article guarantor.
Figure 1. CT showing multiple high density stones in the gallbladder (arrow).
Figure 2. CT showing a high density defect in the distal common bile duct (arrow).
Figure 3. Endoscopic appearance of yellow/green stone material swept from the common bile duct during ERCP.

Publish your work in ACG Case Reports JournalACG Case Reports Journal is a peer-reviewed, open-access publication that provides GI fellows, private practice clinicians, and other members of the health care team an opportunity to share interesting case reports with their peers and with leaders in the field. Visit http://acgcasereports.gi.org for submission guidelines. Submit your manuscript online at http://mc.manuscriptcentral.com/acgcr.
Nayak et al
acgcasereports.gi.org
Ceftriaxone-Induced Gallstones
172 ACG Case Reports Journal | Volume 1 | Issue 3 | April 2014
Financial disclosure: Neither author has a conflict of interest related to this report.
Informed consent was obtained for this case report.
Received: January 16, 2014; Accepted: March 4, 2014
References1. Park HZ, Lee SP, Schy AL. Ceftriaxone-associated gallbladder sludge.
Identification of calcium-ceftriaxone salt as a major component of gall-bladder precipitate. Gastroenterology. 1991;100(6):1665–70.
2. Richards DM, Heel RC, Brogden RN, et al. Ceftriaxone. A review of its antibacterial activity, pharmacological properties and therapeutic use. Drugs. 1984;27(6):469–527.
3. Arpacik M, Ceran C, Kaya T, et al. Effects of ceftriaxone sodium on in vitro gallbladder contractility in guinea pigs. J Surg Res. 2004;122(2):157–61.
4. Choi YY, Jung HY, Choi SM, et al. Gallbladder pseudolithiasis by ceftriax-one in young adult. J Korean Surg Soc. 2011;81:423–6.
5. Bonnet JP, Abid L, Dabhar A, et al. Early biliary pseudolithiasis during ceftriaxone therapy for acute pyelonephritis in children: A prospective study in 34 children. Eur J Pediatr Surg. 2000;10(6):368–71.
6. Famularo G, Polchi S, De Simone C. Acute cholecystitis and pancre-atitis in a patient with biliary sludge associated with the use of ceftri-axone: A rare but potentially severe complication. Ann Ital Med Int. 1999;14(3):202–4.
7. Neff LP, Mishra G, Fortunato JE, et al. Microlithiasis, endoscopic ultra-sound, and children: Not just little gallstones in little adults. J Pediatr Surg. 2011;46(3):462–6.
8. Rodríguez Rangel DA, Pinilla Orejarena AP, Bustacara Diaz M, et al. Gallstones in association with the use of ceftriaxone in children. Ann Pediatr (Barc). 2014;80(2):77–80.
9. Meng D, Cao Y, Fu J, et al. Sonographic assessment of ceftriaxone-associated biliary pseudolithiasis in Chinese children. J Int Med Res. 2010;38(6):2004–10.
10. Schaad UB, Wedgwood-Krucko J, Tschaeppeler H. Reversible ceftriaxone-associated biliary pseudolithiasis in children. Lancet. 1988;2(8625):1411–3.