an enzyme-immunoassay for antibodies against hepatitis b core antigen: characteristics and clinical...
TRANSCRIPT

Journal of Virological Methods, 17 (1987) 95-103
Elsevier
95
JVM 00625
An enzyme-immunoassay for antibodies against hepatitis B core antigen: characteristics and
clinical validation
L. Matthyssen ‘, A. Arndt-Hanser2, W. Lange3, G. Maass4, K. Schiitt2, A. van Loon’ and G. Walters’
‘Organon Scientific Development Group, Oss, The Netherlands: ‘Transfusionszentrale der Universitiitskliniken, Mainz, F. R. G. ; ‘Robert Koch-lnstitut des Bundesgesundheitsamtes, Berlin,
F. R. G. ; jlnstitut fur Virusdiagnostik (Landesuntersuchungsamt), Miinster, F. R. G. ; ‘Department of Medical Microbiology, University Hospital Nijmegen, The Netherlands
(Accepted 27 March 1987)
Summary
An enzyme-immunoassay (EIA) for antibodies to hepatitis B core antigen (anti- HBc) was developed.
The new test uses undiluted samples, incubated directly into an HBcAg coated well. Three alternative test procedures are possible. The stability of reagents was studied and a preclinical evaluation was performed intramurally. An assay correlation study was organised.
We report the results of the external evaluation performed at 4 centres. A mean analytical sensitivity of 1.1, 1.2 and 0.36 PEI units/ml anti-HBc was found for procedure I (1 h/l h/30 min), procedure II (30 min/30 min/30 min) and procedure III (16-20 h/l h/30 min), respectively. In total, 5288 determinations on serum or plasma from various patients and healthy individuals were performed: 10% with procedure I, 52% with procedure II and 38% with procedure III. The qualitative (positive or negative) results were compared with those found with tests used routinely at the centres - 47% with Corzyme (Abbott) and 53% with Corab (Abbott) - in a first screening. A final evaluation was made taking into account the repeatability of the results. Based on all results together, the agreement between the new EIA for anti-HBc and the routine tests was 97.6% at the first screening and increased to 99.0% after further evaluation.
Assay correlation; EIA; Anti-HBc
Correspondence to: L. Matthyssen, Organon Diagnostics Research Laboratories, P.O. Box 20. 5340 BH Oss, The Netherlands.
0166-09341871f103.50 0 1987 Elsevier Science Publishers B.V. (Biomedical Division)

96
Introduction
The involvement of HBcAg and antibodies to HBcAg (anti-HBc) in HBV was described (Almeida et al., 1971). The detection of anti-HBc soon became incorporated in the general serology for viral hepatitis and is still a useful marker (Gerety, 1985). Anti-HBc plays a unique role among HBV markers, because it is present at practically all stages of HBV infection. The occurrence of antibodies to HBcAg in serum or plasma indicates that the patient has contracted HBV sometime previously.
Further testing of anti-HBc positive specimens for HBsAg and anti-HBs distinguishes immunity from ongoing acute or chronic infections (Slade and Vroon, 1984). The clinical significance of an isolated anti-HBc positive result, either from a ‘core window’ (where HBsAg is no longer detectable and seroconversion did not yet occur) or long after infection with loss of anti-HBs, is not yet clear, nor the suitability of testing for anti-HBc in prevaccination screening (Kane et al., 1985). The value of anti-HBc as a surrogate marker for non-A, non-B post transfusion hepatitis in blood banks, is subject of discussions (Kolata, 1986).
An enzyme-immunoassay for anti-HBc in strips was developed. The characteristics and clinical validation of this test have been evaluated in an assay correlation study at 4 centres.
Materials and Methods
Study protocot
The aim of the validation study was to compare the results of the new test with the results obtained with commercially available and licensed tests. The four centres that participated and the performed test procedures are given in Table 1.
In brief, at centre 1 a general evaluation was done using procedure III of the new test and a RIA as the reference. Another general evaluation was performed at centre 3, using the three alternative procedures (I, II, III) of the new test and an EIA as the reference.
Centre 2 performed a comparative study on the shortest test procedure (II)
TABLE 1
Assay correlation: new EIA for anti-HBc.
Centre Study location Test procedure Reference
1 Miinster (F.R.G.) III Corab 2 Maim (F.R.G.) II Corab 3 Berlin (F.R.G.) IiIIiIII Corzyme 4 Nijmegen (The Netherlands) III Corzyme
I = 1 h 37”Ul h 37”C/30 min RT; II = 30 min 5OW30 min 5OW30 min RT; III = 16-20 h RT/l h 37W30 min RT.

97
against a RIA and evaluated the role of the various anticoagulants. With the reference test only sera were tested. At centre 4 the overnight test procedure (III) was compared with a reference EIA on samples of staff and members of institutions of mentally retarded people, considered to be at a higher risk for HBV.
When discrepant results between the new test and the reference test were found in the first screening, both tests were repeated unless otherwise stated. Not repeatable results were excluded from the final evaluation. During the evaluation period sensitivity panels were incorporated in several test runs of the new test. These sensitivity panels were calibrated in PEI units (U)/ml anti-HBc against the reference preparation for anti-HBc as issued by the Paul Ehrlich Institute (F.R.G.). The analytical sensitivity of the test procedures or the detection limit at the cut- off point of the test was determined using these sensitivity panels by interpolation on a dose-response curve of the panel.
Study population
The actual number of samples tested and the composition of the study population are given in Table 2. At centre 2, the serum from 556 blood donors as well as the corresponding various plasmas were tested with the new test. They were classified as different samples (n=2224). For the evaluation, only the result obtained with the serum in the reference test was available and this result was considered representing the true state of the donor sample, either serum or plasma.
At centre 3 a comparative study of the three available new test procedures was performed on 537 different samples. This resulted in 1611 determinations. The total number of determinations performed in the first screening at the 4 centres was 5288.
Assays
All specimens were tested for anti-HBc with commercially available assays: Corab or Corzyme from Abbott Laboratories. The tests were performed according to the prescriptions of the manufacturer.
All specimens were tested with the new EIA for anti-HBc. The test kit became recently available as Hepanostika anti-HBc (Organon Teknika) and Hepanostika Anticore (Organon Teknika Corporation).
In brief, the test is an enzyme-immunoassay based on an inhibition principle. The wells of polystyrene strips are coated with HBcAg produced by recombinant DNA-technology. The test sample (control) is incubated in such a well. There are three procedural options for incubations: Procedure I= 60 min 37”C/60 min 37”C/30 min RT; procedure II= 30 min 5o”C/30 min 5O”C/30 min RT; procedure III= overnight RT/60 min 37”C/30 min RT.
With an anti-HBc positive sample the HBcAg will be blocked partially or completely. After a wash step, human anti-HBc, labelled with the enzyme horseradish peroxidase is added. This labelled antibody binds to the unblocked solid-phase antigen After a wash step the enzyme substrate (peroxide and tetramethylbenzidine) is added.

98
TABLE 2
Distribution of the study population.
Samples Centre
1 2 3 4
Blood donors sera
plasma-citrate
-EDTA
-heparin
108 556 200 106 556
10 556
556
Routine patients
prevaccination
high-risk populations
Non-HBV diseases anti-HAV IgM +
anti-CMV IgM + anti-EBV IgM +
anti-Tox IgM + NANB
RF+
anti-Rub IgM +
HBV diseases acute
chronic
(acute/chronic)
remote
Total (samples)
Total (determinations)
Overall n = 5288 (first screening)
100 100
100 50
852
9 10
10 10 10
10
10 20
9
49
50 99 48 10 10
601 2224 537 852 601 2224 1611 852
A blue colour is produced, which turns yellow when the reaction is stopped with sulphuric acid. If the sample contains anti-HBc, only a reduced colour develops in comparison with negative control samples. Samples are evaluated on the basis of a cut-off value deduced from the positive and negative controls included in each test run (strip-holder). In fact, the cut-off value is fixed at 50% inhibition. Within limits, the amount of anti-HBc present in the sample is inversely proportional to colour development.
Analysis
Calculations of between test agreement, sensitivity and specificity were made by methods described (Galen and Gambino, 1975) using the results of the comparative tests (Corab or Corzyme) as reference.

99
Results
Analytical sensitivity
The mean result for each centre and the overall results are given in Table 3. The analytical sensitivity of procedures I and II are comparable (between 1.0 and 1.5 units/ml anti-HBc according to the PEI-reference preparation). The analytical sensitivity of procedure III is at least two times higher.
Assay correlation, diagnostic sensitivity, specificity and agreement
The qualitative results (positive or negative) obtained in a first test (screening) were all compared with the results of the routinely used tests (either Corzyme or Corab). No data were left out and for calculations it was assumed that the results of the reference (routine) tests were correct (100% sensitive, 100% specific) in view of the true clinical situation of each sample (from blood donors or patients). A final evaluation was made taking into account the repeatability of the initially discrepant results for both the new test and the reference test. Results that were not repeatable (irreproducible) were left out from the final evaluation. The total number of determinations (in the first screening) was 5288. After elimination of irreproducible results, the results of 5210 determinations remained available for final evaluation. The background for exclusion of 78 results was: 7 samples at centre 1 (3 x irreproducible new test; 4 x irreproducible reference); 38 samples at centre 3 (all irreproducible reference; new test was not repeated but with exception of one sample there was agreement on the same samples tested with the three procedures of the new test); 33 samples at centre 4 (2 x no material available for repeat testing; 12 x irreproducible new test; 19 x irreproducible reference).
At centre 2 no repeat testing of discrepant samples was performed and therefore the results of the first screening are also used in the final evaluation.
For the overall assay correlation the results of first screening and final evaluation have been used. Further comparative evaluation (reference tests, various
TABLE 3
Analytical sensitivity of new EIA for anti-HBc (expressed in PEI units/ml anti-HBc)
Centre Procedure
I II III
1 0.42 (6)* 0.40 (5)
2 1.2 (3) 3 1.1 (3) 1.2 (3) 0.35 (2)** 4 0.27 (5)
Overall 1.1 1.2
* Between parentheses = number of individual determinations. ** One result excluded (as outlier).
0.36

100
TABLE 4
Assay correlation: overall results.
Evaluation
First
Final
R N R N R N R N + + + - + _ _
1169 38 91 3990 1169 25 26 3990
Calculations First screening
% specificity 97.8
% sensitivity 96.9
% agreement 97.6
n samules comuared 5288
Final evaluation
99.4
97.9
99.0
5210
R = reference test (Corab or Corzyme); N = new test.
procedures of the new test, and various study populations) was done based on the results of the first screening, being more in line with the clinical routine where in general only one test for anti-HBc will be used.
Overall results
The results of all determinations (first screening, n=5288; final evaluation, n=5210), irrespective of the centre, the procedure or reference test used are given in Table 4, including also the calculations using the results of the routine tests as the reference. The agreement between the new test and the reference test increased from 97.6% at the first screening to 99.0% after final evaluation. One percent of the determinations remained discrepant. Half of the discrepant results were classified as false-positive, the other half as false-negative, based on the results of the reference test. Overall the specificity correlated better than the sensitivity in the final evaluation (99.4% versus 97.9%). An evaluation of the analytical sensitivity of the reference tests was not performed at the centres during this trial.
TABLE 5
Assay correlation. Overall results of first screening in relation to reference test.
R N R N R N R N + + + - + - -
Corab 257 20 5 2543 Corzvme 912 33 71 1447
Calculations Corab Corzyme
% specificity 99.2 95.3 % sensitivity 98.1 96.5 % agreement 99.1 95.8 n samples compared 2825 2463
R = reference test (Corab or Corzyme); N = new test.
101
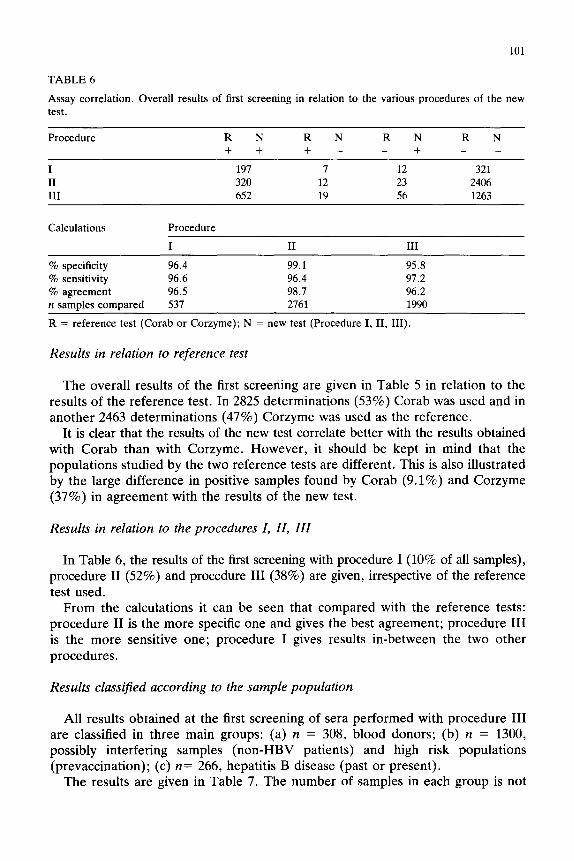
TABLE 6
Assay correlation. Overall results of first screening in relation to the various procedures of the new test.
Procedure R N R N R N R N + + + - +
I 197 7 12 321 II 320 12 23 2406 III 652 19 56 1263
Calculations Procedure
I II III
% specificity 96.4 99.1 95.8 % sensitivity 96.6 96.4 97.2 % agreement 96.5 98.7 96.2 n samples compared 537 2761 1990
R = reference test (Corab or Corzyme); N = new test (Procedure I, II, III).
Results in relation to reference test
The overall results of the first screening are given in Table 5 in relation to the results of the reference test. In 2825 determinations (53%) Corab was used and in another 2463 determinations (47%) Corzyme was used as the reference.
It is clear that the results of the new test correlate better with the results obtained with Corab than with Corzyme. However, it should be kept in mind that the populations studied by the two reference tests are different. This is also illustrated by the large difference in positive samples found by Corab (9.1%) and Corzyme (37%) in agreement with the results of the new test.
Results in relation to the procedures I, II, III
In Table 6, the results of the first screening with procedure I (10% of all samples), procedure II (52%) and procedure III (387 ) o are given, irrespective of the reference test used.
From the calculations it can be seen that compared with the reference tests: procedure II is the more specific one and gives the best agreement; procedure III is the more sensitive one; procedure I gives results in-between the two other procedures.
Results classified according to the sample population
All results obtained at the first screening of sera performed with procedure III are classified in three main groups: (a) n = 308, blood donors; (b) n = 1300, possibly interfering samples (non-HBV patients) and high risk populations (prevaccination); (c) n= 266, hepatitis B disease (past or present).
The results are given in Table 7. The number of samples in each group is not

102
TABLE 7
Assay correlation. Results (%) of first screening of different populations
Population
(a) Blood donors (n= 308) (b) Patients/non HBV (n= 298)
High risk populations (n= 1002) (cl HBV disease In=2661
R N R N R N R N + + + +
8.1 0 1.6 90.3 12.1 0.3 5.7 81.0 32.5 1.5 3.1 62.9 97.0 1.1 0.8 1.1
R = reference test (Corab or Corzyme): N = new test (Procedure III).
comparable. The percentage of discrepant results (of first screening) for a, b and c was 1.6, 4.9 and 1.9%, respectively and decreased to 1, 1.4 and 0.4% after final evaluation.
The percentage of positive results (in agreement with the reference tests) was 8.1, 27.8 and 97% for a, b and c, respectively.
The number of anti-HBc positive blood donors is rather high (8.1%). In case all data on sera of different blood donors (including the results on sera tested with procedures I and II) would have been used (n=864) a total of 57 samples (6.6%) was found positive.
The overall performance of this new EIA for anti-HBc was good. No invalid test runs were obtained. The three procedural options (from results within 2 h to results after an overnight incubation) worked well. Undiluted samples and ready- for-use controls and conjugate are used. The samples are incubated immediately in the coated wells. The reagents are stable, and due to the strip format also smaller series of samples can be tested economically.
Discussion
The results of the study show that the new EIA for total anti-HBc correlates well with the available approved tests (Corab and Corzyme) for anti-HBc. The overall agreement was 99.0% on 5210 determinations left after the exclusion of inconclusive results both for the reference tests and the new EIA. The occurrence of 1% discrepant results (0.5% false-positives and 0.5% false-negatives based on the results of the tests used as reference) cannot be explained without an additional in-depth study on these samples. The lack of a confirmatory test for anti-HBc is a drawback to prove the true state of the sample. More information has to be gathered by additional tests for HBV markers on the same sample and other samples from the same donor or patient. The overall final specificity was 99.4% against a sensitivity of 97.9%.
Procedure III of the new EIA resulted in the highest analytical sensitivity. In the correlation study this higher analytical sensitivity did not result in a much higher

103
diagnostic sensitivity than found with procedures I and II. It remains questionable whether more sensitive tests for anti-HBc are needed, unless also more specific. A more sensitive RIA was described (Wolff and Gerlich, 1984) but not yet proposed as a suitable alternative for the present tests.
In the comparative evaluation of sera and plasmas no significant differences were found. There are not sufficient data to prove that the correlation of the new test is better with Corab than with Corzyme, although this tendency was found.
From a clinical point of view, it is not surprising that the incidence of anti-HBc found was lowest in the donor population (overall 6.6%) and highest (97%) for samples from patients with current or remote HBV disease.
The usefulness of anti-HBc screening of blood donors to reduce post-transfusion hepatitis non-A, non-B has been discussed previously (Nath et al., 1983) and has regained interest. Recent publications argue both in favour and against introduction (Koziol et al., 1986; Roeckel and Watts, 1986; Aymard et al., 1986; Hoyos et al., 1986).
On the basis of this limited study it should be considered that overall 6.6% of the blood donations might become suspected.
References
Almeida, J.D., Rubinstein, D. and Stott, E.J. (1971) New antigen-antibody system in Australia-antigen- positive hepatitis. Lancet II, 1225-1227.
Aymard, J.P., Janot, C., Gayet, S., Guillemin, C., Canton. P., Gaucher, P. and Streiff, F. (1986) Post- transfusion non-A, non-B hepatitis after cardiac surgery. VOX Sang. 51, 236-238.
Galen, R.S. and Gambino. S.R. (1975) Sensitivity. specificity. prevalence and incidence. In: Beyond
Normality. pp. 9-14. John Wiley and Sons Inc. New York.
Gerety, R.J. (1985) Hepatitis B core antigen and antibody (HBcAg/Anti-HBc). In: Hepatitis B. pp.
27-45. Academic Press, U.S.A.
Hoyos, M., Sarrion, J.B.. Perez-Castellanos. T. Marty, M.L. and Berenguer. J. (1986) Markers for non-A. non-B hepatitis. Ann. Intern. Med. 105. 467.
Kane, M.A., Hadler, S.C. and Maynard. J.E. (1985) Antibody to. hepatitis B surface antigen and
screening before hepatitis B vaccination (Editorial). Ann. Intern. Med. 103, 791-793.
Kolata, G. (1986) News and comments: new blood test raises thorny issues. Science 233, 149-150.
Koziol. D.E., Holland, P.V., Alling, D.W.. Melpolder, J.C., Solomon, R.E., Purcell, R.U.. Hudson, L.M.. Shoup. F.J., Krakauer, H. and Alter, H.J. (1986) Antibody to hepatitis B core antigen as a
paradoxical marker for non-A, non-B hepatitis agents in donated blood. Ann. Intern. Med. 104,
488-495.
Nath, N., Pielech, M. and Dodd, R.Y. (1983) Hepatitis-associated markers in the American Red Cross
blood donor population. VOX Sang. 44, 312-318.
Roeckel, I.E. and Watts, W.T. (1986) Prevalence of post-transfusion non-A, non-B hepatitis. Pathologist, July 1986, 6-7.
Slade. B.A. and Vroon, D.M. (1984) Anti-HBc to screen for susceptibility to hepatitis B. Lancet I, 1246-1247.
Wolff, W. and Gerlich, W.H. (1984) Direct radioimmunoassay of antibody against hepatitis B core
antigen using 32P-labelled core particles. Eur. J. Clin. Microbial. 3, 25-29.