allergy arkwright ac anaphylaxis controversies finer points
TRANSCRIPT

Management of Anaphylaxis
Controversial dogmaControversial dogma
Dr Peter Arkwright
Senior Lecturer in Paediatric Allergy and Immunology
Royal Manchester Children’s Hospital

• Adrenaline
– Position
– Number
• Avoidance
Dogma in the dock
• Avoidance
– versus exposure
– gut versus skin

• first line treatment for anaphylaxis
• for food and venom associated
anaphylaxis, recommended route is
Adrenaline
anaphylaxis, recommended route is
intramuscular, not subcutaneous or
intravenous

Concernincrease obesity in society
with the increasing levels of obesity will auto-
injectors still deliver adrenaline into the
muscle?muscle?

2011 Overweight or obese Obese
>30 kg/m2
Men 65 24
Women 58 26
Children 30 16

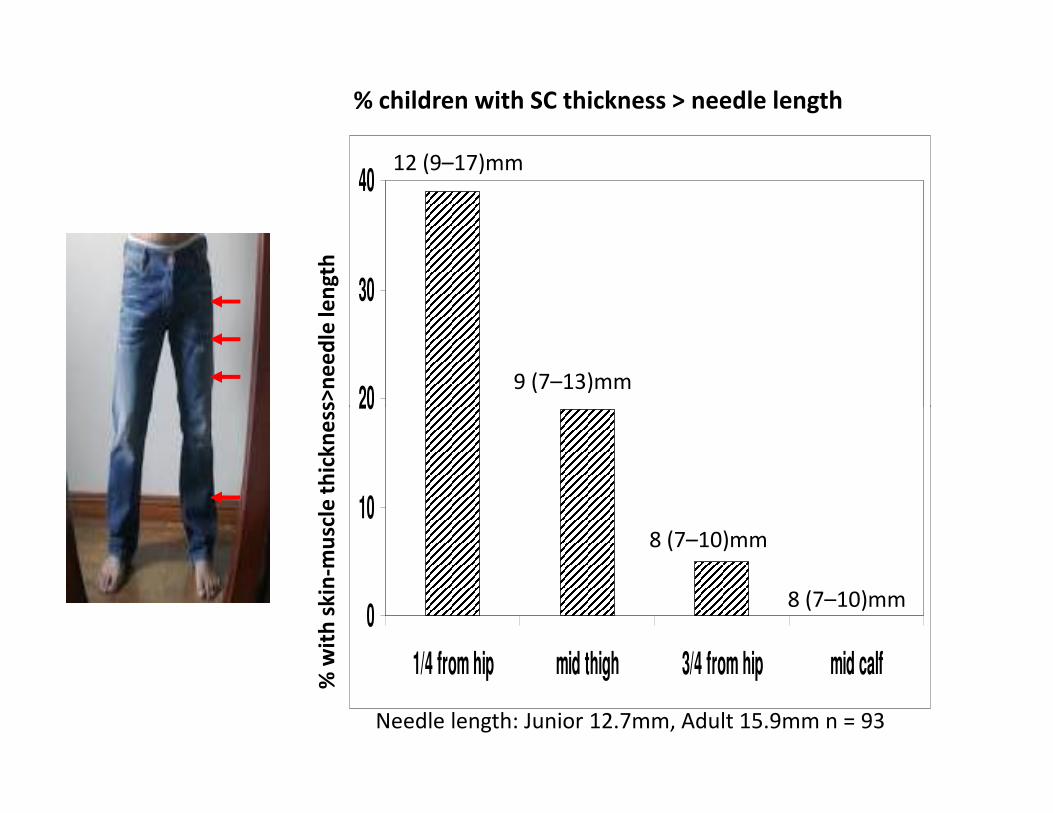
• skin to muscle depth was measured by ultrasound at set
distances down the thigh and leg in 93 children attending the
paediatric allergy clinic at RMCH
• weight, height and waist circumference were measured and
BMI calculated Bewick et al, JACI IP, 2013
• age 1 to 16 years old, median 6 years
• 56% male
• 64% White, 24% Asian
• overweight 9%, obese 17%
Results
• overweight 9%, obese 17%
20
30
40
mu
scle
th
ick
ne
ss>
ne
ed
le le
ng
th
12 (9–17)mm
9 (7–13)mm
% children with SC thickness > needle length
0
10
20
1/4 from hip mid thigh 3/4 from hip mid calf
% w
ith
sk
in-m
usc
le t
hic
kn
ess
>n
ee
dle
len
gth
8 (7–10)mm
8 (7–10)mm
Needle length: Junior 12.7mm, Adult 15.9mm n = 93

50
75
100
% of children with skin to muscle thickness > needle length
Green – healthy weight
Yellow – overweight (85-94th C)
Red – obese (>95th C)gender/age specific BMI
2000 CDC growth charts
% s
kin
to
mu
scle
th
ick
ne
ss >
ne
ed
le le
ng
th
0
25
50
n = 93
% s
kin
to
mu
scle
th
ick
ne
ss >
ne
ed
le le
ng
th
1/4 from hip mid calf3/4 from hipmid thigh
age and gender are not independent determinants

• 120 adults, aged 18 - 55 years old
• mid-thigh measurements only
• mean BMI 29.2 kg/m2
• 31% potential failure risk (women 55% vs men
Bhalla et al, Ohio study in adults
• 31% potential failure risk (women 55% vs men
5%)
Bhalla et al, Am J Emerg Med, 2013

• review of records 4 New England Hospitals 2001
– 2006 of ED patients presenting with allergic
reactions
• 18% overweight, 22% obese
Rudders et al, New England retrospective
review
• 18% overweight, 22% obese
• 321 (261 children and 60 adults) received
adrenaline: 267 1 dose; 54 2+ doses
• obese patients or women were no more likely to
receive 2 doses
• nor were those with respiratory symptomsRudders et al, JACI, 2012

• Obesity in both children and adults is
associated with an increased risk that
adrenaline will not be injected into the muscle
• Does it matter? If it did one might expect
Conclusions
• Does it matter? If it did one might expect
more second doses, hospital admissions and
deaths in obese and in women.
• In more obese children consider injector in
lower half of thigh

• AC is recommending TWO devices
• clinicians vary in the number of auto-injectors
they prescribe
Number of prescribed auto-injectors

Number of pens in
children with food allergyMt Sinai Hospital
New York
RMCH
Manchester
number of children 413, median 4.5 y
pea/tree nuts, milk
84% had auto-injectors
prescribed
298, median 10 y
pea/tree nuts, milk
100% had auto-injectors,
95% had 2+ devices
Jarvinen et al, JACI, 2008
Arkwright, JACI 2009
prescribed 95% had 2+ devices
Number requiring auto-injector
1 dose 71 (19%)
50% by non-meds
18 (6%)
2 doses 18 (4%) egg - restaurant
1 by non-med
0

• auto-injectors should never be prescribed
without concomitant training on how and
when to use the device
• decision on the number of auto-injectors
Discussion
• decision on the number of auto-injectors
should be based on evidence and need
• variables include: peer-reviewed published
evidence, family’s requirements, residential
location, travel


• Is strict avoidance of foods that children are
partly tolerant to making their food allergies
– more severe?
Controversy
– more severe?
– more prolonged?

Egg
NATURAL HISTORY OF CHILDREN WHO TOLERATE BAKED MILK AND EGG
0
Milk
Pro
ba
bil
ity
of
de
ve
lop
ing
to
lera
nce
Challenge: baked milk muffin
1.3g of dry milk powder
cooked 180C for 30 min
Challenge: baked egg muffin
2.2g of dry milk powder
cooked 180C for 30 min
Kim JS et al, JACI, 2011, n = 88
¾ of children tolerated baked milk challenge
8X more likely to develop tolerance to fresh milk
Leonard SA et al, JACI, 2012, n = 79
Time to mean scrambled egg tolerance
3½ versus 5 years
Pro
ba
bil
ity
of
de
ve
lop
ing
to
lera
nce
MMonths following first visit

Pro
ba
bil
ity
of
de
ve
lop
ing
to
lera
nce
Milk Egg
Baked food
Complete avoidance
CURING MILK AND EGG ALLERGY WITH BAKED FOODS
Baked milk muffin
1.3g of dry milk powder
cooked 180C for 30 min
Baked egg muffin
2.2g of egg protein
cooked 180C for 30 min
MMonths following first visit
Pro
ba
bil
ity
of
de
ve
lop
ing
to
lera
nce
Leonard SA et al, JACI, 2012, n = 79
Children eating baked egg were 15X more
likely to develop tolerance to scrambled egg
Kim JS et al, JACI, 2011, n = 88
Children eating baked milk were 4X more
likely to develop tolerance to fresh milk

Standard advice
• Children with immediate cow’s milk or egg
allergy should avoid these foods in all forms
unless otherwise advised by an allergy
specialistspecialist

• Addition of dietary baked milk and egg is safe,
convenient and well-accepted by many
patients with milk and egg allergy
• Recommending baked milk and egg products
Evidence-based advice
• Recommending baked milk and egg products
to milk and egg allergic children represents an
important shift in the treatment paradigm for
these allergies
JACI, 2011

Palmar hyperlinearity(excessive lines on palms)
filaggrin
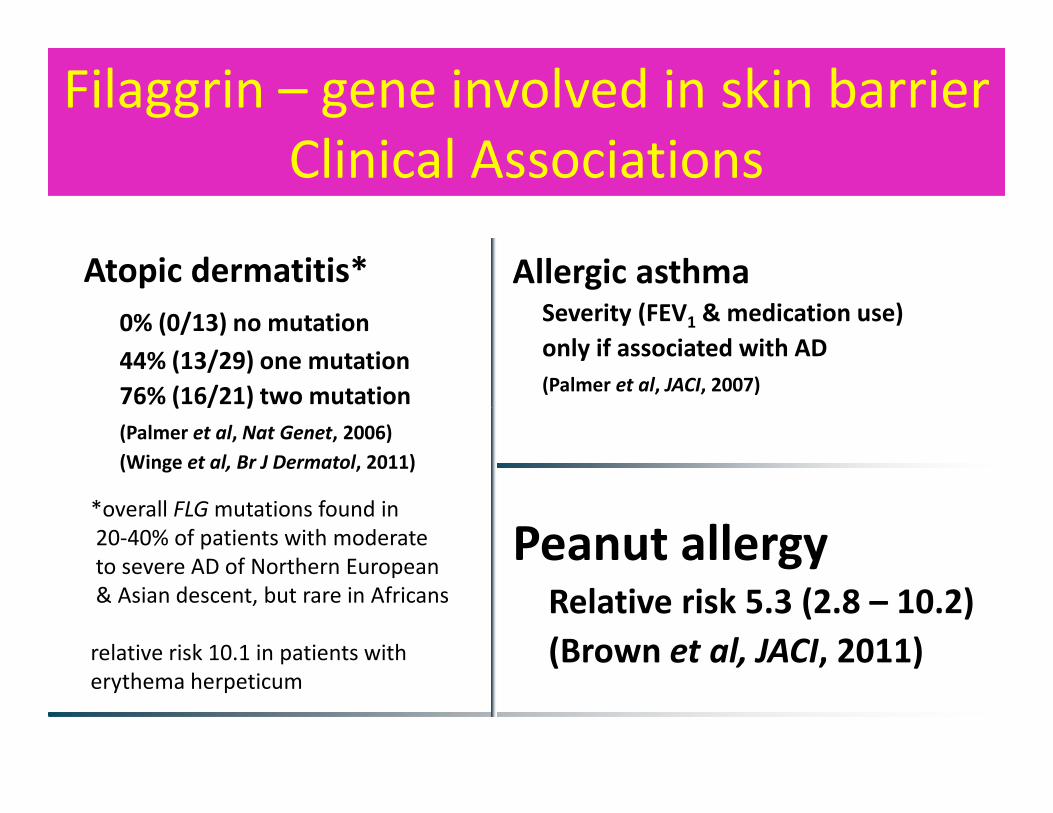
Filaggrin – gene involved in skin barrier
Clinical Associations
Atopic dermatitis*
0% (0/13) no mutation
44% (13/29) one mutation
76% (16/21) two mutation
Allergic asthmaSeverity (FEV1 & medication use)
only if associated with AD
(Palmer et al, JACI, 2007)76% (16/21) two mutation
(Palmer et al, Nat Genet, 2006)
(Winge et al, Br J Dermatol, 2011)
Peanut allergyRelative risk 5.3 (2.8 – 10.2)
(Brown et al, JACI, 2011)
*overall FLG mutations found in
20-40% of patients with moderate
to severe AD of Northern European
& Asian descent, but rare in Africans
relative risk 10.1 in patients with
erythema herpeticum

Tolerance
Allergy
GUT SKIN
• Age
• Severe asthma
• Genetic factors
Risk factors for severe and complex allergies
• Genetic factors
• Unnecessary food avoidance

• Adrenaline auto-injectors– increasing obesity in the community is increasing the
potential for more injections not being delivered into the muscle
– critical to ensure that auto-injectors are only prescribed to patients and carers that are adequately training in their use,
Points for discussion
patients and carers that are adequately training in their use, rather than prescribing additional pens in case of misfiring because of lack of training
• Avoidance– there is increasing evidence that complete avoidance of milk
and egg can prolong and exacerbate these allergies
– Ongoing studies e.g. LEAP will help to answer whether this is also the case for other foods e.g. peanut