aggressive, long-termcyclosporine therapy for …jasn.asnjournals.org/content/5/10/1820.full.pdf ·...
TRANSCRIPT

1820 Volume 5 . Number 10 ‘ 1995
Aggressive, Long-Term Cyclosporine Therapy forSteroid-Resistant Focal Segmental �2
Elizabeth Ingulli, Anup Singh, Noosha Baqi, Hadi Ahmad, Shohreh Moazami, and Amir Tejani3
E. Ingulli. University of Minnesota. Minneapolis. MN
A. Singh. N. Baqi. H. Ahmad. S. Moazami. A. Tejani.SUNY Health Science Center. Brooklyn. NY
(J. Am. Soc. Nephrol. 1995; 5:1820-1825)
ABSTRACTShort-term cyclosporine (CsA) has been shown toreduce the proteinuria in refractory nephrotic syn-drome, but the effect on disease progression has not
been evaluated. This study was undertaken to evalu-ate whether maintenance C5A therapy in steroid-resistant focal segmental glomerulosclerosis (FSGS)will prevent progression to ESRD. Twenty-one blackand Hispanic children (mean age, 8.4 ± 4.5 yr) withbiopsy-proven, steroid/cyclophosphamide-resistantFSGS were treated with CsA (initiated at 6 mg/kg perday and titrated to the serum cholesterol level toachieve a response). The mean CsA dose was 7 (4 to20) mg/kg per day, the duration of CsA therapy was27.5 (3 to 97) months, and the duration of follow-upwas 8.5 ± 4.7 yr. At the end of CsA therapy, the mean(± SE) proteinuria fell from 6.2 ± 0.2 to 2.0 ± 0.1 g/24
h (P < 0.001), the mean albumin rose from 1.95 ± 0.04
to 3.41 ± 0.04 g/dL (P < 0.001), the mean cholesteroldecreased from 472 ± 12.7 to 257 ± 5.3 mg/dL (P <
0.005), and the mean creatinine rose from 0.79 ± 0.02to 1.16 ± 0.03 mg/dL (P < 0.005). Seven childrencontinue to receive maintenance CsA therapy, and14 patients have had CsA stopped: 6 for an increase
in serum creatinine and/or continued proteinuria, 5
for sustained remission, 2 for noncompliance, and 1
for pregnancy. Five (24%) of the 21 patients pro-gressed to ESRD. This ESRD rate was compared with ahistorical population with a similar age and follow-up,
and fewer patients were found to have progressed toESRD using long-term CsA therapy (5 of 21 (24%)versus 42 of 54 (78%); P < 0.05). Long-term CsA ther-apy reduces the proteinuria and blunts the progres-sion of FSGS to ESRD in black and Hispanic children.
Key Words: Cyclosporine. nephrotic syndrome. focal sclerosis
1 Received August 4. 1994. Accepted December 20, 1994.
2 Presented in part at the APS-5PR Meeting, seattle, May 1994.
3 correspondence to Dr. A. Tejani, Renal Division, SUNY Health Science center,Pediatrics, Box 49, 450 clarkson Ave., Brooklyn. NY 11203-2098.
104&6673/051 0-1 820$03.00/0Journal of the American Society of Nephroiogycopyright c 1995 by the American Society of Nephrology
F ocal segmental gbomemubosclerosis (FSGS) is the
most common acquired renal disease leading to
either dialysis or transplantation among North Amer-
ican children ( 1 ). We have previously reported thatblack and Hispanic children demonstrate a more vir-
ulent form of FSGS, resulting in a more rapid progres-sion to ESRD compared with white children (2). It has
been suggested that the protelnuria contributes to the
progression of disease and, when massive, can accel-erate the disease process (3). The treatment of protein-uria in patients with FSGS Is difficult because many
are resistant to corticosteroid and alkylating therapy
(4,5). Short-term cycbosporine (CsA), a potent immu-
nosuppressive, has been shown to reduce the massive
protelnuria in instances where corticosteroids and
alkylating agents have failed; however, dlscontinua-
tion of the drug often leads to a relapse of proteinuria(6-1 1 ). We have shown improved remission rates in
resistant patients using an alternative dosing regimenof CsA ( 1 2). To date, there are no studies addressingwhether a reduction in the proteinuria induced withCsA in this lesion affects the devolution of renal
function. In this study, we test the hypothesis that
maintenance CsA therapy will reduce the proteinuria
and blunt the progression to ESRD among black and
Hispanic patients with FSGS.
MATERIALS AND METHODS
Patients were included in this study if they (1 ) had biopsy-proven FSGS and proteinurla �40 mg/m2 per hour or 3g/day; (2) were younger than 18 yr of age; (3) were black orHispanic; (4 ) were corticosteroid resistant, which was de-fined as a failure to respond to the International Study ofKidney Disease in Children protocol of prednisone. 60mg/rn2 per day, for the first 4 wk, followed by 40 mg/m2every other day for 4 wk; and (5) received at least one courseof cyclophosphamide (2.5 to 3 mg/kg per day for 60 days).Additionally, parents and patients were required to consentto percutaneous renal biopsies at 12- to 18-month intervalsafter the initiation of CsA therapy.
The protocol for treating patients with CsA has variedthrough the years. Previously, patients received CsA at aninitial daily dose of 7 mg/kg. The dose was titrated tomaintain a whole blood trough level measured by high-pressure liquid chromatography between 100 and 200 ng/mL. The dose was reduced if the bevel was more than 200ng/mL. but the dose was not increased above 7 mg/kg perday if the level was below 100 ng/mL (1 1). More recently, Inthe setting of severe hypercholesterolemla, the dose of CsA istitrated to the serum cholesterol level to achieve a response,regardless of blood level. Patients are started with 10 mg/kgof CsA, and the dose is gradually increased in a stepwisemanner every 2 wk. In the presence of severe hypercholes-terolemia, this stepwise Increase In CsA dose is carried on upto a maximum of32 mg/kg unless signs ofnephrotoxicity areseen. Nephrotoxicity was defined as a rise of serum creati-

Ingulli et al
Journal of the American Society of Nephrology 1821
TABLE 1 . The mean (± SD) proteinuria, serumalbumin, serum cholesterol, and serum creatinine inthe 21 patients before the initiation of CsA (PRE) andat the end of CsA therapy (POST)
Parameter PRE CSA POST CSA P Value
Proteinuria (g/24 h) 6.2 ± 4.6 2.0 ± 2.5 <0.001Albumin (g/dL) 1 .95 ± 0.73 3.41 ± 0.75 <0.001Cholesterol (mg/dL) 472 ± 241 257 ± 107 <0.005
Creatinine (mg/dL) 0.79 ± 0.34 1.16 ± 0.63 <0.005
nine equal to or greater than 0.5 mg on two consecutive days.When clinical evidence of nephrotoxlclty was present, thedose of CsA was reduced by one-third and then graduallyincreased If the clinical signs of nephrotoxicity disappeared.Because CsA dosing Is titrated to cholesterol level, whenserum cholesterol is below 400 mg/dL, a stepwise reductionin CsA dose Is carried out so that patients with cholesterollevels of 200 or less are generally maintained on 10 mg/kg orless of CsA.
After a reduction in the proteinurla below 500 mg/day, thedose of CsA is gradually tapered and withdrawn over a 2- to3-month period. Recurrence of the proteinuria during thetaper or after the withdrawal of the drug resulted in reinsti-tution of the drug according to the protocol previously dis-cussed. In patients in whom a reduction of proteinurla doesnot occur within 3 months, the drug is discontinued. In anypatient exhibiting two consecutive rises in serum creatinineof 0.5 mg or more, despite CsA dose reduction, the drug waswithdrawn.
All patients received low-dose prednisone at the InitiationofCsA therapy. Children younger than 6 yr ofage were begunon 5 mg daily. those 6 to 12 years ofage were begun on 10 mgdaily, and those 12 to 18 yr ofage were begun on 15 mg daily.Two obese children received 20 mg of prednisone daily. Instable patients, prednisone was eventually discontinued. Inedematous patients, furosemide was administered. No pa-tients were given an angiotensin-converting enzyme inhibitorto treat their hypertension.
Patients were monitored In the clinic weekly where serumelectrolytes, BUN, creatinine, albumin, cholesterol, liverfunction tests, and 24-h urine protein excretion were mea-sured. Percutaneous renal biopsies were performed at 1 2- to18-month intervals to look for evidence of CsA-inducednephrotoxIclty. CsA nephrotoxlclty was diagnosed with the
presence of vacuolization of tubules, arteriolopathy, disrup-tion of tubular architecture, and stripe interstitial fibrosis.
Statistical analysis was carried out by the use of a pairedtest to compare individual values between groups. A f testwas used to compare groups. Actuarial renal survival rateswere calculated with product-limit estimates of survival cbs-tributions (13). A P value <0.05 was considered significant.Values are reported as means ± standard deviations unlessindicated.
RESULTS
Twenty-one children ( 1 3 boys) met inclusion criteriaand formed the study population. Thirteen patients
were black, and eight were Hispanic. All patients hadbiopsy-proven FSGS, and their proteinuria was resis-tant to both corticosteroid and cycbophospha.midetherapy. The mean age of the patients at the time ofdiagnosis was 8.4 ± 4.5 yr. The mean duration offollow-up was 8.5 ± 4.7 yr.
The mean duration of CsA therapy was 27.5 ± 22
months, and it ranged from 3 to 97 months. Table 1shows the mean pretherapy and posttherapy labora-tory values for all patients at the end of CsA therapy.There was a significant reduction in the mean 24-hproteinuria, serum albumin, and serum cholesterol atthe end of the study period. There was also a signifi-cant elevation in the serum creatinine bevel at the endof the study period.
At the most recent follow-up (April 1 994), 7 of the 21patients continue on maintenance CsA therapy. The
current status of these patients is shown in Table 2.CsA was discontinued in the remaining 14 patients, in5 because of sustained remission, in 5 because ofrising creatinine, and in 2 because of noncompliance.Persistent proteinuria (N = 1) and pregnancy (N = 1)necessitated withdrawal in two cases. Table 3 depictsthe current status of the five patients who continue tobe in remission without CsA or prednisone therapy. Intwo patients, the drug was discontinued because thepatients did not comply with the frequent clinic visitsand blood tests required. Both patients were in apartial remission of their nephrotlc syndrome (normal
serum albumin, no edema, and proteinuria of 1 . 1 and
TABLE 2. The proteinuria, serum albumin, and serum creatinine before CsA treatment (PRE) and at most recentfollow-up (POST), the serum cholesterol at the most recent follow-up, the duration of CSA therapy in months,and the most recent dose for the patients continuing on CSA
PatientNo.
Proteinuria(g/24 h)
PRE POST
Albumin
(g/dL)
PRE POST
Creatinine (mg/dL)Cholesterol
(mg/dL)
Durati on of CsA Dose
PRE POST CsA (months) Dose (mg/kg per day)
1 7.2 0.2 2.0 4.3 0.5 0.7 191 101 112 2.5 0.2 4.2 4.3 1.0 1.6 196 15 103 3.0 0 1.4 4.0 1.0 1.7 150 56 44 3.0 0.4 2.4 4.4 0.9 0.7 200 44 105 3.0 0 1.3 4.0 1.0 1.0 140 43 36 5.1 1.0 2.5 3.9 0.9 1.2 240 10 127 8.0 0.1 1.9 3.3 0.5 0.5 290 15 20
a,E
C.)
U)
2
0
START CSA
D/C CSA
CsA Therapy for FSGS
1822 Volume 5 . Number 10 . 1995
TABLE 3. The proteinuria, serum albumin, and serum creatinine before CSA treatment (PRE) and at most recentfollow-up (POST), the duration of CSA therapy in months, and the duration since the discontinuation of CSA inmonths in the patients with sustained remission
PatientNo.
Prote
(gI
PRE
inuria24 h)
POST
Albumi
PRE
n (g/dL)
POST
Creatinine(mg/dL)
PRE POST
Duration (months)
On CSA Off CSA
1 5.4 0.1 1.2 4.0 0.7 1.0 65 362 1.5 0.4 3.4 3.6 1.5 1.7 8 83 4.5 0.3 2.0 3.9 0.4 0.6 14 1054 3.4 0.5 1.9 3.1 0.4 0.9 25 855 12.0 0.1 1.8 4.3 0.4 0.5 21 18
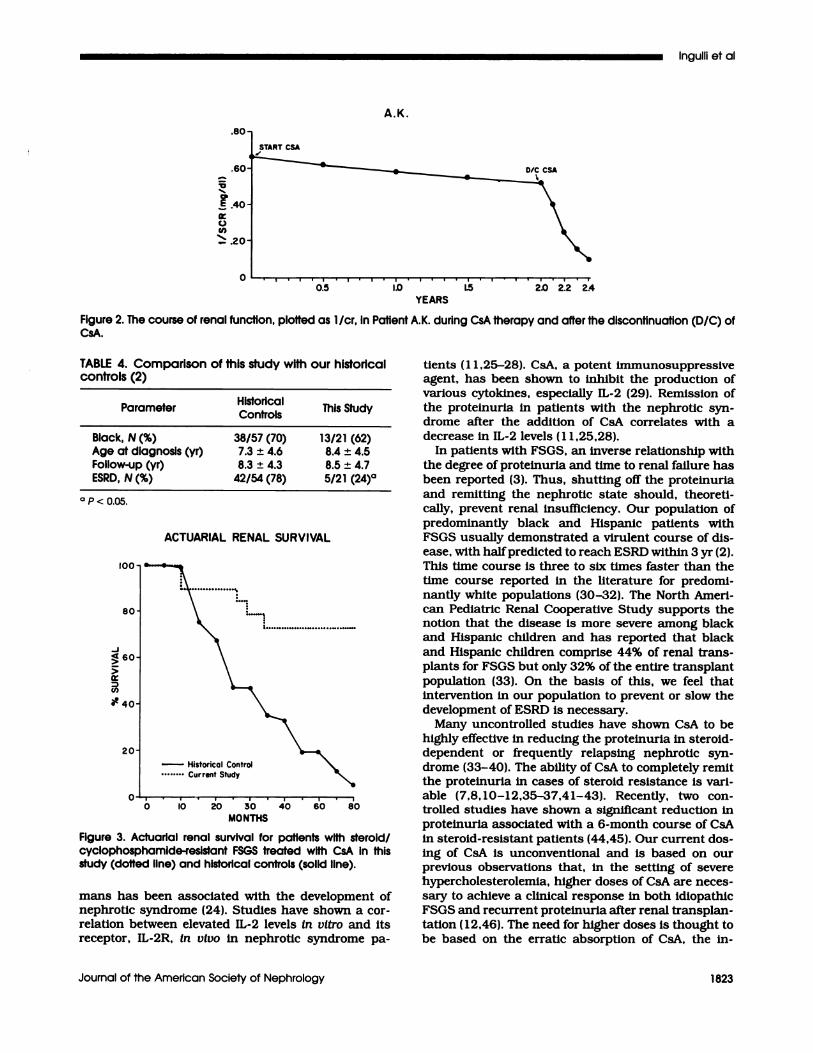
1 .0 g/ 24 h) at the time CsA was stopped. The patientswere treated with CsA for 28 and 30 months, respec-tively. In one of the patients, CsA was discontinued at
6.5 yr of age (serum creatinine, 0.8 mg/dL). After CsAwas stopped, a relapse of the nephrotic syndromeresulted In massive proteinuria, and in 8 months, thepatient progressed to ESRD. The course of this pa-
tient, plotted as 1 /cr, is shown in Figure 1 . For theother patient, no follow-up was available. CsA wasdiscontinued in one patient because of pregnancy. Atthe time CsA was stopped, she was in a partial remis-sion of her nephrotic syndrome.
In six patients, CsA was discontinued because ofcontinued proteinuria and/or a rise In serum creati-nine. Three of the six patients had a significant reduc-
tion (�50%) in their proteinuria, and one patient was
in complete remission of the proteinurla ( 100 mg/24h) at the time CsA was stopped. After the discontinu-ation ofCsA, massive proteinuria and edema resulted.
Four of the six patients progressed to ESRD within 2,
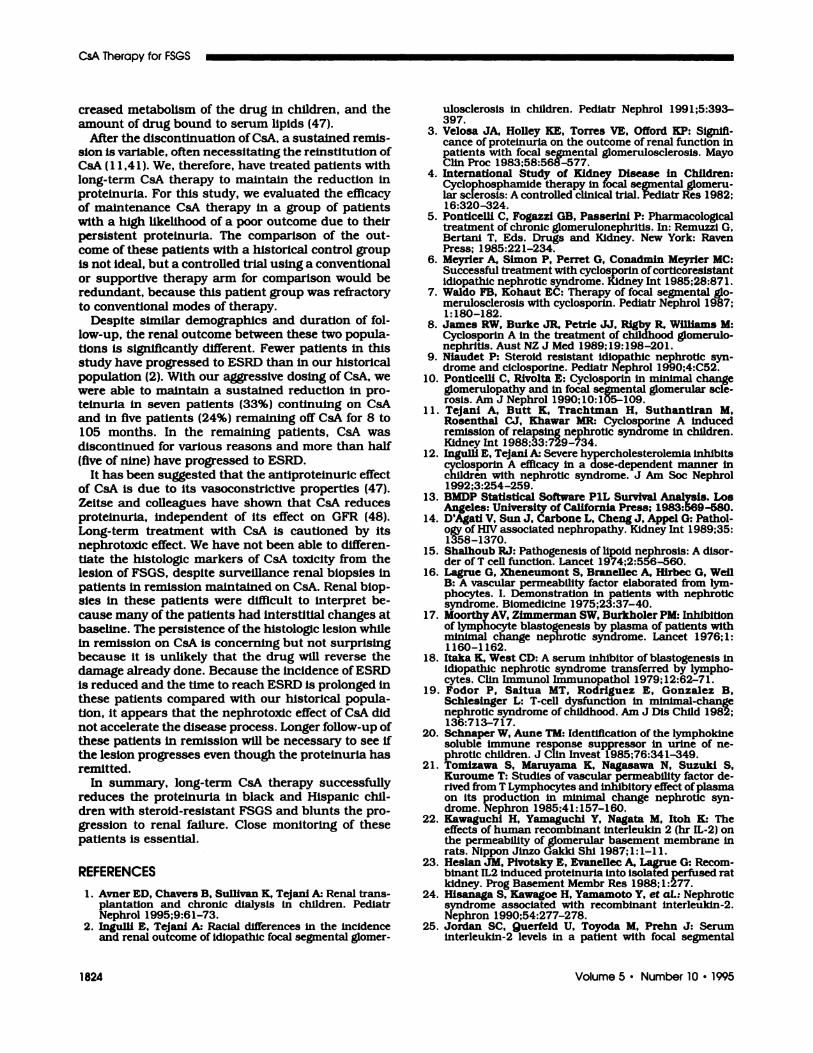
4, 6, and 24 months after CsA was discontinued. Arepresentative course of one of the patients, plotted as1 /cr, Is shown in Figure 2. This patient was begun onCsA at 1 2 yr of age with a serum creatinine of 1.5mg/dL. She was treated with CsA for 25 months witha significant reduction but continued proteinuria.Over that period of time, her serum creatinine had
J.M.
4 8 2 6 20 24 28 32 36 40
MONTHS
Figure 1 . The course of renal function, plotted as 1/cr, inPatientJ.M. during CsA therapy and after the discontinuatIon(D/C) of CsA.
risen to 2.0 mg/dL and the drug was stopped. Massiveproteinuria resulted, and the patient reached ESRD in4 months.
Five (24%) of the 21 patients have reached ESRD
over the study period. The time to reach ESRD fromthe time of the diagnosis of FSGS in the 5 patients was30, 43, 44, 47, and 63 months. We reviewed histologyto determine if globally prominent collapse of the
glomerula tuft ( 14) could identify progression toESRD. Of our 2 1 patients, only 4 had the collapsingvariant ofFSGS. One ofthese patients has a sustainedremission, one went into ESRD, one dropped out
because of noncompliance, and one continues to re-celve maintenance CsA. In order to determine whetherprolonged maintenance CsA therapy prevents the pro-gression to ESRD, we compared the renal outcome of
this study group with our historical controls prey-
ousby reported (2). Despite similar racial distributionsof patients In the two groups, the mean age at diagno-515, and the duration of follow-up, the renal outcomewas significantly better in CsA-treated patients (5 of2 1 124%] versus 42 of 54 [78%]; P < 0.05; Table 4). An
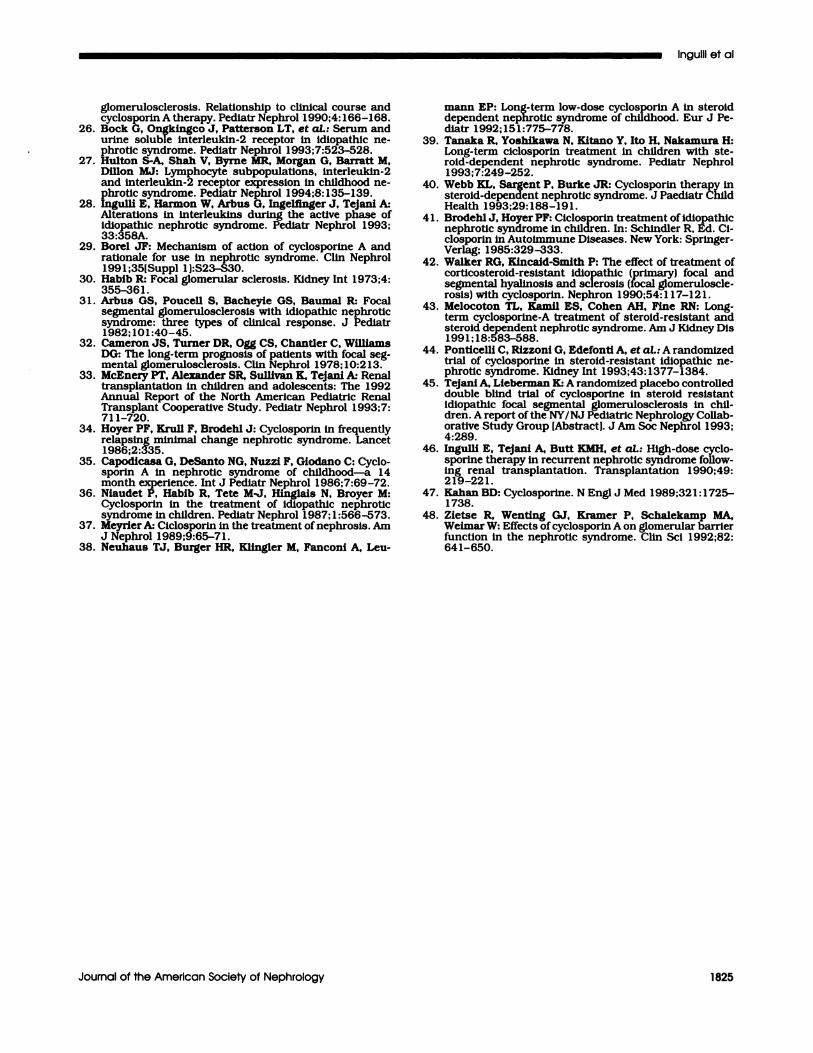
actuarial renal survival comparing this CsA-treatedpopulation with our historical controls Is depicted inFigure 3.
There was no clear histologic evidence for CsA neph-rotoxicity in any of the biopsy specimens; however, in
all of the biopsy specimens, the lesion of FSGS per-
sisted. Side effects Included gingival hyperplasia (N =
6), hypertrlchosis (N = 8), coarse facies (N = 4), andhypertension (N = 2 1 ); however, they did not necessi-tate the discontinuation of CsA.
DISCUSSION
On the basis of clinical correlations and in vitro
studies, it has been suggested that the proteinuria of
the nephrotic syndrome Is the result of a circulatingsubstance produced from an abnormal cellular im-mune response ( 15-20). With the Improved under-standing of the mechanisms of the immune response,
it is now believed that the circulating substance is a
cytokine, produced by T lymphocytes, that injures theglomerular basement membrane and/or the epithelialcell, resulting in the leakage of protein in the urine(2 1-23). Administration of interleukln-2 (IL-2) to hu-
.80
.60
csA
D/C CSA
0
YEARS
Historical ControlCurrent Study
10 20 30 40 60 80
MONTHS
Ingulli et al
Journal of the American Society of Nephrology 1823
�0
a,
E
C)Cl)
AK.
Figure 2. The course of renal function, plotted as 1/cr, in Patient AK. during CsA therapy and after the discontinuation (D/C) ofCsA.
TABLE 4. Comparison of this study with our historicalcontrols (2)
ParameterHistoricalControls
This Study
Black, N (%) 38/57 (70) 13/21 (62)Age at diagnosis (yr) 7.3 ± 4.6 8.4 ± 4.5Follow-up (yr) 8.3 ± 4.3 8.5 ± 4.7ESRD, N (%) 42/54 (78) 5/21 (24)�
a p < 0.05.
100
80
-J�60
>
U)
�40
20
ACTUARIAL RENAL SURVIVAL
Figure 3. ActuarIal renal survival for patients with steroid/cyclophosphamide-reslstant FSGS treated with CsA in thisstudy (doffed line) and historical controls (solid line).
mans has been associated with the development of
nephrotic syndrome (24). StudIes have shown a cor-relation between elevated IL-2 levels in vitro and its
receptor, IL-2R, in vivo in nephrotic syndrome pa-
tients ( 1 1 ,25-28). CsA, a potent immunosuppressive
agent, has been shown to inhibit the production of
various cytokines, especially IL-2 (29). Remission of
the proteinuria in patients with the nephrotic syn-drome after the addition of CsA correlates with a
decrease in IL-2 levels (11,25,28).In patients with FSGS, an inverse relationship with
the degree of proteinurla and time to renal failure has
been reported (3). Thus, shutting off the protelnurla
and remitting the nephrotic state should, theoreti-
cally, prevent renal insufficiency. Our population ofpredominantly black and Hispanic patients with
FSGS usually demonstrated a virulent course of dis-
ease, with halfpredlcted to reach ESRD within 3 yr (2).
This time course is three to six times faster than the
time course reported in the literature for predomi-
nantly white populations (30-32). The North Amen-
can Pediatric Renal Cooperative Study supports the
notion that the disease is more severe among black
and Hispanic children and has reported that black
and Hispanic children comprise 44% of renal trans-
plants for FSGS but only 32% of the entire transplant
population (33). On the basis of this, we feel that
intervention in our population to prevent or slow the
development of ESRD is necessary.Many uncontrolled studies have shown CsA to be
highly effective in reducing the proteinuria in steroid-
dependent or frequently relapsing nephrotic syn-
drome (33-40). The ability of CsA to completely remit
the protelnuria in cases of steroid resistance is van-
able (7,8,10-12,35-37,41-43). Recently, two con-
trolbed studies have shown a significant reduction inproteinuria associated with a 6-month course of CsA
in steroid-resistant patients (44,45). Our current dos-ing of CsA is unconventional and is based on our
previous observations that, in the setting of severe
hypercholestenolemia, higher doses of CsA are neces-
sary to achieve a clinical response in both idiopathic
FSGS and recurrent proteinunia after renal transplan-
tation ( 1 2,46). The need for higher doses is thought tobe based on the erratic absorption of CsA, the in-
CsA Therapy for FSGS
1824 Volume 5 . Number 10 ‘ 1995
creased metabolism of the drug in children, and theamount of drug bound to serum lipids (47).
Alter the discontinuation of CsA, a sustained remis-sion is variable, often necessitating the reinstitution of
CsA ( 1 1 ,4 1 ). We, therefore, have treated patients withlong-term CsA therapy to maintain the reduction inproteinuria. For this study, we evaluated the efficacyof maintenance CsA therapy in a group of patientswith a high likelihood of a poor outcome due to theirpersistent proteinuria. The comparison of the out-come of these patients with a historical control groupis not ideal, but a controlled trial using a conventionalor supportive therapy am for comparison would beredundant, because this patient group was refractoryto conventional modes of therapy.
Despite similar demographics and duration of fob-low-up, the renal outcome between these two popula-tions Is significantly different. Fewer patients In thisstudy have progressed to ESRD than in our historical
population (2). With our aggressive dosing of CsA, wewere abbe to maintain a sustained reduction in pro-teinuria in seven patients (33%) continuIng on CsAand in five patients (24%) remaining off CsA for 8 to105 months. In the remaining patients, CsA wasdiscontinued for various reasons and more than half
(five of nine) have progressed to ESRD.
It has been suggested that the antiproteinunic effect
of CsA is due to its vasoconstrictive properties (47).
Zeitse and colleagues have shown that CsA reduces
proteinuria, independent of its effect on GFR (48).
Long-term treatment with CsA is cautioned by its
nephrotoxic effect. We have not been abbe to differen-
tiate the histologic makers of CsA toxicity from the
lesion of FSGS, despite surveillance renal biopsies in
patients in remission maintained on CsA. Renal biop-
sles in these patients were difficult to interpret be-cause many of the patients had interstitial changes at
baseline. The persistence of the histologic lesion while
in remission on CsA Is concerning but not surprising
because it is unlikely that the drug will reverse the
damage already done. Because the incidence of ESRD
is reduced and the time to reach ESRD is prolonged in
these patients compared with our historical popula-
tion, It appears that the nephrotoxic effect of CsA did
not accelerate the disease process. Longer follow-up ofthese patients in remission will be necessary to see if
the lesion progresses even though the proteinuria has
remitted.
In summary, long-term CsA therapy successfully
reduces the proteinuria in black and Hispanic chib-
dren with steroid-resistant FSGS and blunts the pro-
gression to renal failure. Close monitoring of thesepatients is essential.
REFERENCES
1 . Avner ED, Chavers B, Sullivan K, Tejani A: Renal trans-plantation and chronic dialysis in children. PediatrNephrol 1995;9:61-73.
2. Inguui E, Tejani A: Racial differences In the incidenceand renal outcome of Idiopathic focal segmental glomer-
ulosclerosis in children. Pediatr Nephrol 199 1;5:393-397.
3. Vebosa JA, Holley KE, Torres VE, Offord KP: Signifi-cance of proteinuria on the outcome of renal function inpatients with focal segmental glomerulosclerosls. MayoChin Proc 1983;58:568-577.
4. International Study of Kidney Disease in Children:Cyclophosphamide therapy in focal segmental glomeru-lar sclerosis: A controlled clinical trial. Pediatr Res 1982;16:320-324.
5. Ponticelli C, Fogazzi GB, Passerini P: Pharmacologicaltreatment of chronic gbomerulonephritls. In: Remuzzi G,Bertani T, Eds. Drugs and Kidney. New York: RavenPress; 1985:221-234.
6. Meyrier A, Simon P, Perret G, Conadmin Meyrier MC:Successful treatment with cyclosporin of corticoreslstantidiopathic nephrotic syndrome. Kidney Int 1985;28:87 1.
7. Waldo FB, Kohaut EC: Therapy of focal segmental gb-merulosclerosis with cyclosporin. Pediatr Nephrol 1987;1:180-182.
8. James RW, Burke JR. Petrie JJ, Rigby R, Williams M:Cyclosporin A in the treatment of childhood glomerulo-nephritis. Aust NZ J Med 1989; 19:198-201.
9. Niaudet P: Steroid resistant Idiopathic nephrotlc syn-drome and cicbosporine. Pediatr Nephrol 1990;4:C52.
10. Pontlcelli C, Rivolta E: Cycbosporin in minimal changeglomerubopathy and in focal segmental gbomerular scle-rosis. Am J Nephrol 1990; 10:105-109.
1 1 . Tejani A, Butt K, Trachtman H, Suthantiran M,Rosenthal CJ, Khawar MR: Cyclosporine A inducedremission of relapsing nephrotic syndrome in children.Kidney Int l988;33:729-734.
12. Ingulll E, Tejani A: Severe hypercholesterolemia inhibitscyclosporin A efficacy in a dose-dependent manner inchildren with nephrotic syndrome. J Am Soc Nephrol1992;3:254-259.
13. BMDP Statistical Software P1L Survival Analysis. LosAngeles: University of California Press; 1983:569-580.
14. D’Agati V, Sun J, Carbone L, Cheng J, Appel G: Pathol-ogy of HIV associated nephropathy. Kidney Int l989;35:1358-1370.
15. Shaihoub RJ: Pathogenesis of lipold nephrosls: A disor-der ofT cell function. Lancet 1974;2:556-560.
16. Lagrue G, Xheneumont 5, Branellec A, Hirbec G, WellB: A vascular permeability factor elaborated from lym-phocytes. I. Demonstration in patients with nephroticsyndrome. Biomedicine 1975;23:37-40.
1 7. Moorthy AV, Zimmerman SW, Burkholer PM: Inhibitionof lymphocyte blastogenesis by plasma of patients withminimal change nephrotic syndrome. Lancet 1976;!:1160-1 162.
18. Itaka K, West CD: A serum Inhibitor of blastogenesis inidiopathic nephrotic syndrome transferred by lympho-cytes. Clin Immunol Immunopathol 1979; 12:62-71.
19. Fodor P. Saitua MT, Rodriguez E, Gonzalez B,Schlesinger L: T-cell dysfunction in minimal-changenephrotic syndrome of childhood. Am J Dis Child 1982;136:713-717.
20. Schnaper W, Aune TM: Identification of the lymphokinesoluble immune response suppressor in urine of ne-phrotic children. J Chin Invest l985;76:341-349.
2 1 . Tomizawa 5, Maruya.ma K, Nagasawa N, Suzuki S,Kuroume T: Studies of vascular permeability factor de-rived from T Lymphocytes and inhibitory effect of plasmaon its production in minimal change nephrotic syn-drome. Nephron 1985;4l:157-160.
22. Kawaguchi H, Yamaguchi Y, Nagata M, Itoh K: Theeffects of human recombinant interleukin 2 (hr IL-2) onthe permeability of gbomerubar basement membrane inrats. Nippon Jinzo Gakki Shi 1987; 1 : 1-1 1.
23. Heslan JM, Pivotsky E, Evanellec A, Lagrue G: Recom-binant IL2 induced proteinuria into isolated perfused ratkidney. Prog Basement Membr Res 1988; 1:277.
24. Hisanaga 5, Kawagoe H, Yamamoto Y, et at.: Nephroticsyndrome associated with recombinant interleukin-2.Nephron 1990;54:277-278.
25. Jordan SC, Querfe!d U, Toyoda M, Prehn J: Seruminterleukln-2 levels In a patient with focal segmental
lngulli et al
Journal of the American Society of Nephrology 1825
gbomerulosclerosis. Relationship to clinical course andcyclosporin A therapy. Pediatr Nephrol 1990;4: 166-168.
26. Bock G, Ongkingco J, Patterson LT, et at.: Serum andurine soluble lnterleukin-2 receptor in idiopathic ne-phrotic syndrome. Pediatr Nephrol 1993;7:523-528.
27. Hulton S-A, Shah V, Byrne MR, Morgan G, Barratt M,Dillon MJ: Lymphocyte subpopulations, interleukin-2and interleukin-2 receptor expression In childhood ne-phrotic syndrome. Pediatr Nephrol 1994;8: 135-139.
28. Ingulli E, Harmon W, Arbus G, Ingelfinger J, Tejani A:Alterations in interleukins during the active phase ofIdiopathic nephrotlc syndrome. Pediatr Nephrol 1993;33:358A.
29. Borel JF: Mechanism of action of cycbosporine A andrationale for use in nephrotic syndrome. Chin Nephrol1991;35lSuppl 1J:S23-S30.
30. Habib R: Focal glomerular sclerosis. Kidney Int l973;4:355-361.
3 1 . Arbus GS, Poucell 5, Bacheyie GS, Baumal R: Focalsegmental gbomerulosclerosis with Idiopathic nephrotlcsyndrome: three types of clinical response. J Pediatr1982; 101:40-45.
32. Cameron JS, Turner DR, Ogg CS, Chantler C, WifilamsDG: The long-term prognosis of patients with focal seg-mental glomerulosclerosls. Clin Nephrol 1978; 10:2 13.
33. McEnery PT, Alexander SR, Sullivan K, Tejani A: Renaltransplantation in children and adolescents: The 1992Annual Report of the North American Pediatric RenalTransplant Cooperative Study. Pediatr Nephrol l993;7:711-720.
34. Hoyer PF, Krull F, Brodehl J: Cyclosporin in frequentlyrelapsing minimal change nephrotlc syndrome. Lancet1986;2:335.
35. Capodicasa G, DeSanto NG, Nuzzi F, Giodano C: Cyclo-sporin A In nephrotlc syndrome of childhood-a 14month experience. Int J PedIatr Nephrol 1986;7:69-72.
36. Niaudet P, Habib R, Tete M-J, Hinglals N, Broyer M:Cyclosporin in the treatment of Idiopathic nephroticsyndrome in children. Pediatr Nephrol 1987; 1:566-573.
37. MeyrierA: Cicbosporin in the treatment ofnephrosls. AmJ Nephrol l989;9:65-71.
38. Neuhaus TJ, Burger HR. Klingler M, Fanconi A, Leu-
mann EP: Long-term low-dose cycbosponin A in steroiddependent nephrotic syndrome of childhood. Eur J Pe-diatr 1992;151:775-778.
39. Tanaka R, Yoshikawa N, Kitano Y, Ito H, Nakamura H:Long-term ciclosporin treatment in children with ste-rold-dependent nephrotlc syndrome. Pedlatr Nephrol1993;7:249-252.
40. Webb KL, Sargent P, Burke JR: Cycbosporin therapy insteroid-dependent nephrotic syndrome. J Paedlatr ChildHealth 1993;29:188-191.
4 1 . Brodehi J, Hoyer PF: Ciclosporin treatment of idiopathicnephrotic syndrome in children. In: Schindler R, Ed. Ci-closporin in Autoimmune Diseases. New York: Springer-Verlag; 1985:329-333.
42. Walker RG, Kincaid-Smith P: The effect of treatment ofcorticosteroid-resistant Idiopathic (primary) focal andsegmental hyalinosis and sclerosis (focal glomeruboscle-rosis) with cycbosporin. Nephron 1990;54: 1 17-121.
43. Melocoton TL, Ka.mll ES, Cohen AH, Fine RN: Long-term cyclosporine-A treatment of steroid-resistant andsteroid dependent nephrotic syndrome. Am J Kidney Dis1991; 18:583-588.
44. Ponticelli C, Rizzoni G, Edefonti A, et at.: A randomizedtrial of cyclosporine in steroid-resistant Idiopathic ne-phrotlc syndrome. Kidney mt 1993;43: 1377-1384.
45. Tejani A, Lieberman K: A randomized placebo controlleddouble blind trial of cyclosporine in steroid resistantIdiopathic focal segmental glomerubosclerosls in chil-then. A report ofthe NY/NJ Pediatric Nephrology Collab-orative Study Group lAbstracti. J Am Soc Nephrol 1993;4:289.
46. Ingulli E, Tejani A, Butt KMH, et at.: High-dose cyclo-sporine therapy in recurrent nephrotic syndrome follow-ing renal transplantation. Transplantation 1990;49:2 19-22 1.
47. Kahan BD: Cyclosporine. N Engl J Med 1989;32 1:1725-1738.
48. Zietse R, Wenting GJ, Kramer P, Schalekamp MA,Weimar W: Effects of cyclosporin A on gbomerular barrierfunction In the nephrotlc syndrome. Clin Sci 1992;82:641-650.