agenda solent nhs trust in-public board meeting · agenda solent nhs trust in-public board meeting...
TRANSCRIPT

Agenda Solent NHS Trust In-Public Board Meeting 27th March 2017 10.30-13:05pm Kestrel 1 & 2, Highpoint Venue, Bursledon Road, Southampton, SO19 8BR *Timings are tentative Item Time Dur. Title & Recommendation Exec Lead /
Presenter 1 10:30 5mins Chairman’s Welcome & Update
• Apologies to receive To receive
Chair
2 Register of Interests & Declaration of Interests To receive
Chair
3 Confirmation that meeting is Quorate No business shall be transacted at meetings of the Board unless the following are present; • a minimum of two Executive Directors • at least two Non-Executive Directors including the Chair
or a designated Non-Executive deputy Chair
Chair
4 *Minutes of Last Meeting and action tracker To agree
Chair
5 10:35 5mins
Matters Arising
Chair
6 10:40 5mins Any Other Business (not on the agenda but advised and agreed with the Chair for inclusion at this meeting)
Chair
7 10:45 15mins Safety and Quality First – including feedback from recent Board to Floor Visits To receive
Chief Executive / Chief Nurse
Strategy & Vision 8 11:00 10mins Chief Executive Report
To receive
Chief Executive
9 11:10 5mins Consideration of the Trust’s Foundation Trust application To agree
Chief Executive / Director of Finance & Performance
10 11:15am 15mins Annual Staff Survey Feedback To receive
Director of Finance & Performance
Solent NHS Trust Headquarters, Highpoint Venue, Bursledon Rd, Southampton, SO19 8BR Telephone: 023 8060 8900 Fax: 023 8053 8740 Website: www.solent.nhs.uk

Programme Delivery 11 11:30am 20mins Mental Health benchmarking
To receive (presentation included within papers) Clinical Director –MH Services
12 11:50am 20mins Performance Report • Operations • Quality and Risk • Finance • Workforce • ICT & Transformation • Infrastructure
To receive
Executive Leads
13 12:10pm 10mins Patient Experience Report To receive
Chief Nurse
External Relations 14 12:20pm 5mins Current and contemporary conversations with external
partners To receive verbal update
All executives
*Reporting Committees 15 12:25pm 5mins *Chairs report on Members Council
To receive
Chair
16 12:30pm 5mins *Complaints Review Panel To receive verbal update
Panel Chair
17 ------ ---- *Charitable Funds Committee Minutes & Chairs update No meeting held since last
Committee Chair
18 12:35pm 5mins *Assurance Committee Chair’s Update To receive exception report from February and March 2017 meetings – including:
- Clinical Audit Plan (see supplementary papers)
NED representative
19 12:40pm 5mins *Mental Health Act Scrutiny Committee Chairs update To receive exception report from February 2017 meeting
NED representative
20 ---- ----- *Governance and Nominations Committee No meeting held since last
Committee Chair
21 12:45pm 5mins Audit & Risk Committee To receive exception report from February 2017 meeting and to agree revised Terms of Reference
Committee Chair
Any other business 22 12:50pm 5mins Items for cascade to other committees
To discuss
Chair
Solent NHS Trust Headquarters, Highpoint Venue, Bursledon Rd, Southampton, SO19 8BR Telephone: 023 8060 8900 Fax: 023 8053 8740 Website: www.solent.nhs.uk

23 12:55pm 5mins Governor comments and questions
Chair
24 13:00pm 5mins Any other business & future agenda items
Chair
25 13:05pm ------ Close and move to Confidential meeting The public and representatives of the press may attend all meetings of the Trust, but shall be required to withdraw upon the Board of Directors resolving as follows: “that representatives of the press, and other members of the public, be excluded from the remainder of this meeting having regard to the confidential nature of the business to be transacted, publicity on which would be prejudicial to the public interest’” (Section 1 (2), Public Bodies (Admission to Meetings) Act 1960)
Chair
--------------------------- break ---------------------------------
Date of next meeting: 30th May 2017 Supplementary papers available on request from the Company Secretary.
Solent NHS Trust Headquarters, Highpoint Venue, Bursledon Rd, Southampton, SO19 8BR Telephone: 023 8060 8900 Fax: 023 8053 8740 Website: www.solent.nhs.uk

Minutes Solent NHS Trust In-Public Board Monday 30th January 2017 10:30-13:10 Kestrel 1 & 2, Solent NHS Trust Headquarters, Highpoint Venue, Bursledon Rd, Southampton, SO19 8BR
Chair: Alistair Stokes, Chairman (AMS)
Members: Sue Harriman, Chief Executive (SH) Andrew Strevens, Director of Finance (AS) Alex Whitfield, Chief Operating Officer Southampton and County Services (AW) Sarah Austin, Chief Operating Officer, Portsmouth and Commercial Director (SA) Dan Meron, Chief Medical Officer (DM) Mandy Rayani, Chief Nurse (MR) Jon Pittam, Non-Executive Director (JPi) Mick Tutt, Non-Executive Director (MT) Jane Sansome, Non-Executive Director (JS) Francis Davis, Non-Executive Director (FD) Mike Watts, Non-Executive Director (MW) Rachel Cheal, Associate Director of Corporate Affairs and Company Secretary (RC)
Attendees: Jayne Edwards, Corporate Support Manager/Assistant company Secretary (JE) Observers: Gary Ashton OE Cam (GA) Ashley Towers, Paediatrics, Solent NHS Trust (AT) Simon Sturgeon, Chief Information Officer (SS), (item 10 only)
1 Chairman’s Welcome & Update
1.1 AMS welcomed Gary Ashton and Ashley Towers to the meeting.
1.2 AMS reported that it was AW’s last Board meeting and thanked her for her contribution as Chief Operating Officer. AMS acknowledged the sad passing of Public Governor Dave Lickman.
2 Register of Interest & Declaration of Interests
2.1 There was no further updates to declare.
3 Confirmation that meeting is Quorate
3.1 The meeting was confirmed as quorate.
4 Minutes of Last Meeting and action tracker
4.1 The minutes of the meeting held on 28th November were agreed as an accurate record.
5 Matters Arising
5.1 JPi highlighted that he had not yet received a schedule of Board to Floor visits for the year. MR to investigate and arrange distribution as soon as possible. Action: MR
5.2 The following actions were confirmed as complete: 533, 534, 535, 536, 537, 538, 539, 541, 523, 529, 530 and 531.
Item 4.1
Solent NHS Trust Headquarters, Highpoint Venue, Bursledon Road, Southampton, SO19 8BR Telephone: 023 8060 8900 Fax: 023 8053 8740 Website: www.solent.nhs.uk
Page 1 of 9

6 Any Other Business
6.1 No further business was requested.
7. Safety and Quality First – including feedback from recent Board to Floor Visits
7.1 AMS enquired whether there are any pressing quality and safety issues that the Board needs to be aware of. SA informed the Board of local acute trusts declaration of a black position which is impacting on Solent teams. SA reported on difficulties with increasing patient flow due to a lack of domiciliary care. It was noted that teams are balancing associated risks against the risks faced by acute trusts.
7.2 AMS asked if the Trust knew how many patients were not being discharged due to the lack of domiciliary care. SA updated the Board and the fragility of the health care system and the importance of domiciliary care funding were noted.
7.3 AS provided feedback following a visit to the Spinnaker Ward in Portsmouth on 9th January 2017. The following observations were made: • The team are the last to receive the IT system roll out however are optimistic on its use. • Issues were identified with regards to accessing PHT notes causing downtime with logging in
procedures. • There were also issues with regards to accessing GP notes due to a number of GPs not being on
the same system. AW provided assurance that there are only two more surgeries remaining to be put onto the system.
• A good discussion was held in relation to the possibility of opening two extra beds. • Service users spoken to were very complimentary about the team and felt involved in their care.
They also commented on the quality of the cleanliness throughout the environment and complimented the food.
AS reported that the overall visit was very uplifting.
7.4 MR briefed the Board on a CAMHs visit on 14th November 2016. It was confirmed that the team and the overall visit were positive. MR informed the Board of an unannounced CQC visit associated with the Mental Health Act and the initial feedback given that provided assurance of no significant issues identified. MR reported on a further unannounced visit to PRRT Social Care. It was noted that initial feedback is positive however formal feedback is awaited. The Board noted the update provided.
8 Chief Executive’s Report including the Hampshire and Isle of Wight Sustainability & Transformation Plan
8.1 SH publically acknowledged the departure of AW and offered congratulations on her appointment as CEO of Hampshire Hospitals. SH acknowledged AW’s significant contributions during her time with Solent and commented on looking forward to a close working relationship going forward.
8.2 SH reported on the STP emerging process particularly around governance across Hampshire and the Isle of Wight and of the need to agree and understand the Trust’s role. SH explained the adoption of local delivery systems across STP and on further work and STP Board debates to be held on how systems will work.
Solent NHS Trust Headquarters, Highpoint Venue, Bursledon Road, Southampton, SO19 8BR Telephone: 023 8060 8900 Fax: 023 8053 8740 Website: www.solent.nhs.uk
Page 2 of 9

8.3 The Board discussed STP growth values in contracts.MT queried how the Trust can achieve parity of esteem requirements AS provided explanation concerning the national tariff uplift and CCG growth allocations. SH reported on the importance of maintaining constructive relationships with commissioners.
8.4 JPi asked how the Board can be assured that the significant IT investment is worthwhile and further investment will not be required due to the STP requirements. It was noted that the IT strategy will be later presented.. SH reported that STP figures are aspirational around IT investment with the possibility of further investment needed from the STP centre. AW provided an example of where the Trust would benefit as a result of the IT STP workstream.
8.6 JS asked if the Trust is ensuring that any IT projects are complimenting the STP work. SH confirmed this to be the case and explained the STP structure and how work is being undertaken.
8.7 Regarding organisation development, MW asked if consideration is being given to define the support package for emergent thinking. SH reported that the Leadership Academy is working on this however acknowledged that further work is required.
8.8 AW provided an overview of business transacted at the TMT meeting held on 25th January 2017 including agreeing revised Terms of Reference. The Recruitment and Retention Strategy was discussed and a presentation was received on the IT strategy and Releasing Time to Care programme.
8.9 MT commended the clear presentation of the Board Assurance Framework in the report that clearly presents operational and strategic risks.
8.10 MT informed the Board of recently chairing a consultant appointment panel for the Child and Adolescent Mental Health Service and explained the process used of being interviewed by young people who access the service. MT suggested that DM reflect on the method for all front facing candidates. AMS asked if candidates provided feedback on the method used. MT confirmed that positive feedback was received.
8.11 AMS requested clarification that the CQC ‘should dos’ are actively being addressed. SH confirmed detailed discussions held at the Assurance Committee where it was identified that just one action has not progressed due to a delay in recruiting to a particular post. It was noted that the post has been filled and a start date is awaited. SH provided confirmation that all actions have now commenced.
8.12 AMS challenged the unmitigated score concerning the IT risk. It was agreed that AW review the BAF score. Action: AW
8.13 AMS asked if the Board could be updated with regards to the Ligature Policy as discussed at TMT. MR briefed the Board on the policy and engagement undertaken. SH confirmed that Care Groups also have an oversight of ligature risks. The Board noted the Chief Executive Report and further updates.
9 Quality Improvement Programme - Quarter 3 Update Report
Solent NHS Trust Headquarters, Highpoint Venue, Bursledon Road, Southampton, SO19 8BR Telephone: 023 8060 8900 Fax: 023 8053 8740 Website: www.solent.nhs.uk
Page 3 of 9

9.1 MR briefed the Board on various projects that are at different stages within the Quality Improvement Programme. MR reported on the positive alliance with NHS Elect who are now running the majority of the programme. It was noted that a Celebration Event is taking place on 3rd February.MR reported that the second cohort of work is the development of a Quality Improvement Academy. Although currently aspirational, the need to progress at an increased pace is recognised.
9.2 RC referred to item 3.3 of the report regarding the need to involve patients more with change within the Dental Service and suggested a more holistic approach to ensure business as usual. MR acknowledged the importance of stakeholder involvement in service mapping. It was agreed that the Board reflect on a strategy for public involvement and patient engagement at a future Seminar. RC to add to the agenda. Action: RC
9.3 MW asked when outputs will be available as quality measures. MR confirmed that quality measures are beginning to emerge from the first cohort of work and improvements are expected to be evident of metrics embedding and linking to quality goals. The Board noted the Quality Improvement Quarter 3 report.
10 ICT Strategy 2016/17 – 2012/22
10.1 Simon Sturgeon arrived at this point of the meeting. • SS presented on IT work being undertaken around the STP work and the individual needs of the
Trust. • It was noted that the strategy is a 5 year rolling document with a 6 month internal review to
refine its content. • SS circulated a copy of the tube map diagram and explained the format.
10.2 JPi commented that he would like to have seen a generic reporting area of overall impact of transformation on workforce efficiency and activity and commented on the freeing up of capacity in the home with Telehealth.
10.3 SS provided explanation as to funding availability in relation to the STP and associated anticipated delivery timescales.
10.4 SA commented on the need for the strategy to reflect the complex integrated environment.
10.5 FD commented on coproduction and managing data that is not contained within the Trust’s own systems.
10.6 SH asked if there is a risk that STP will delay the Trust’s IT program and highlighted the need for the Board to understand risks to our services associated with any delays. SS acknowledged there to be some risks.
10.7 MW commented on the need to understand which parts of the strategy puts the Trust in a strong position and which do not. AW informed the Board of the engagement undertaken with services to encourage strategic thinking concerning IT as an enabler.
10.8 AS reported that benchmarking data should be considered, once available.
Solent NHS Trust Headquarters, Highpoint Venue, Bursledon Road, Southampton, SO19 8BR Telephone: 023 8060 8900 Fax: 023 8053 8740 Website: www.solent.nhs.uk
Page 4 of 9

10.9 AMS asked if the tasking and dispatch system to maximise community service efficiency, is supported by clinical staff. SS explained that the system relates to the ambulance service and 111 and acknowledged that it is expected that teams will be sceptical due to the monitoring nature of the system. The Board confirmed that it agrees that the strategy accurately reflects the ICT needs of the organisation and approved ICT teams to proceed with delivery according to the strategy.
11 Safe Staffing Report (6 monthly)
11.1 MR highlighted an inaccuracy in WTE figures on the table detailed on page 3 and circulated the revised information. Update to be uploaded onto the website. Action: JE
11.2 The following points were raised: • that the care hours by day guidance relates to acute services and is not fully adoptable by the
Trust however provides an insight into how to progress. • that the Shelford Care Tool is being used and reviewed in Jubilee House. It was noted that the
current guidance is inpatient focused and Mental Health needs to be considered. It was noted that care hours per patient is currently nursing focused and needs to include practitioners and other staff groups.
• The Board was informed of improvements in recruitment within Portsmouth community teams. • The Board was informed of work progressing on professional standards and regulations
associated with the quality of e-rostering.
11.3 MT asked if the Assurance Committee should receive a deep dive on workforce issues in relation to not fully addressing all staff groups in care hours per patient. MR agreed the need to present to ensure clarity around new models in an ever changing environment. It was agreed to present to the March Committee. Action: MR / JE for agenda
11.4 SH highlighted the need to reflect on workforce issues and ensure a robust workforce committee is in place. It was noted that the use of E-rostering should be driven as an operational key enabler.
11.5 AS informed the Board of work being undertaken with services and the Quality Team to address workforce issues .The Board noted the Safe Staffing Report and further discussion.
12 Professional Leadership Report
12.1 MR provided a summary of progress with professional leadership, particularly with regards to the Allied Health Professionals (AHPs) Framework in line with STP developments. It was noted that the Trust is expecting to be a follower of the NMC regulated AHP role. The importance of having appropriate governance arrangements in place was highlighted. MR highlighted a national recognition achieved by the Family Nurse Partnership Team.
12.2 AMS asked if the Mental Health Alliance could do more to support mature students going forward. SH reported on the need to consider through the local Workforce Action Board and of a presentation being provided at Portsmouth University to discuss workforce change going forward in light of STP. The Board noted the progress being made on Professional Leadership.
13 Performance Report
Solent NHS Trust Headquarters, Highpoint Venue, Bursledon Road, Southampton, SO19 8BR Telephone: 023 8060 8900 Fax: 023 8053 8740 Website: www.solent.nhs.uk
Page 5 of 9

13.1 Operations – Southampton and County Services AW highlighted the following exceptions: • A more positive position for Podiatric surgery was confirmed. It was noted that a small number
of service users will roll over after March. • AS reported that following the Finance Committee, a positive meeting was held with
commissioners with a resolve and settlement for 2016/17 expected by March.
13.2 JPi asked if the reported reductions to Public Health and possibly domiciliary care within Solent services would impact this financial year only and whether the Trust is engaged with city councils with regards to the issue. AW reported that Solent is engaged with the consultation process. SA highlighted the need for a funded approach to domiciliary and social care within the Portsmouth area and commented on strategic issues being the biggest concern.
13.3 Quality and Risk MR highlighted the following exceptions: • A reduction in the number of incidents was reported and a downturn in the number of
complaints incidents during November and December. SH commented on the increasing number of pressure ulcers arriving into Solent’s care and for the need to consider if the lack of domiciliary care is having an impact on numbers being seen. MR acknowledged the need for further discussion. SA reported on concerns raised with regards to service users being seen from PHT and nutritional based home care required. It was noted that a wider system approach is critical.
13.4 Finance AS highlighted the following exceptions: • It was confirmed that the Trust is on track to deliver to the £3.3m deficit plan. • The Board was informed of work undertaken as requested by NHSI to review capital spend for
this financial year and a reduction achieved. AMS commented on the difficulty in reading the finance tables detailed within the report and asked that the font size is increased in future reports. Action: AS
13.5 Workforce AS highlighted the following exceptions: • As a result of continued high agency spend, actions have been agreed including the monitoring
of the closure of workforce shifts. A change of bank payment rates has also been agreed. • Recruitment and retention strategies are being reviewed and actions considered for
improvement going forward. It was noted that a downward trend is expected during March/April.
13.6 MT asked other than reputational damage, if any other sanctions are expected as a consequence of breaching figures. AS confirmed there to be no further sanctions. It was noted that further information is to be reported to Confidential Board. The Board acknowledged workforce associated risks.
13.7 ICT & Transformation Nothing further to report.
Solent NHS Trust Headquarters, Highpoint Venue, Bursledon Road, Southampton, SO19 8BR Telephone: 023 8060 8900 Fax: 023 8053 8740 Website: www.solent.nhs.uk
Page 6 of 9

13.8 Infrastructure Nothing further to report. The Board noted the Performance Report.
14 Quarter 3 2016/17 – Business Plan Review
14.1 AS reported a current position of amber rating however it was noted that good progress has been made with objectives and milestones. RC commented on the need to reflect in future, whether joint objectives with partners are achievable due to differing priorities.
14.2 MT referred to the reference ‘Treat people with respect, giving equal emphasis to physical and mental health’, commenting on the Trust’s transposed priority. It was agreed to change wording to ‘mental health including physical health’. Action: AS
14.3 AMS asked if the Trust understands the acuity of caseload for mental health. SA reported on a 5 year trend of data available and highlighted issues with regards to lack of secure accommodation. It was agreed that SA raise concerns with NHS Improvement. Action: SA
14.4 MT reported that last year’s benchmarking report provided by Matthew Hall reported that Solent had become the second highest detainer of people under the Mental Health Act where previously had always been the lowest. It was agreed that Matthew Hall present the benchmarking report to the March Board. Action: JE to add to agenda cycle. The Board noted the Trust’s progress against the Operating Plan at the Quarter 3 of 2016/17.
15 Current and contemporary conversations with external partners
15.1 Nothing further to report.
*Reporting Committees
16 *Chairs report on Members Council
16.1 Next meeting to be held on 9th February 2017 at an external venue in Portsmouth. The meeting will discuss governor vacancies and how to take forward and the change of approach of devolution and overarching financial challenges. The Board received the report.
17 *Complaints Review Panel
17.1 JS briefed the Board on discussions held at the recent meeting as follows: • The panel discussed complaints management due to comments made by the CQC. • An increase in the number of complaints received was noted and the panel discussed the
possibility of drafting letters centrally. • Response timescales were discussed and are being looked at as part of an internal review. • The need to consider how to respond in a patient focused way was acknowledged. • JS confirmed that the newly established panel is going well and is attended by external
agencies. The Board noted the exception report.
Solent NHS Trust Headquarters, Highpoint Venue, Bursledon Road, Southampton, SO19 8BR Telephone: 023 8060 8900 Fax: 023 8053 8740 Website: www.solent.nhs.uk
Page 7 of 9

18 *Charitable Funds Committee Minutes & Chairs update
18.1 FD reported that the terms of reference have been amended to reflect a change in attendees and quorum.
18.2 Regarding item 11.4, JPi queried if the terms of reference should still include reference to an independent examination of accounts. It was agreed that the wording of 11.4 be further amended. Action: RC The Board approved the terms of reference subject to final amendments to 11.4 and exception report.
19 *Assurance Committee Chairs update
19.1 • MT informed the Board that the committee terms of reference have been amended due to changes to Clinical Director participation and the inclusion of Information Governance matters.
• The Committee received a deep dive presentation from the Health and Safety Advisor. SA reported that a schedule of estates work detailing prioritisation of risk assessments has been requested and is being chased by AS.
• Thematic Leads for Falls and Dementia provided a deep dive presentation. The need for a revised Falls protocol was highlighted and significant work required to mitigate current inaccuracies with the safeguarding training recording matrix was discussed.
SH provided assurance however that training information is gathered within audits and is not purely reliant on the matrix. • The Committee received an update on changes to Information Governance legislation and an
increase in demand to the Trust as a consequence. • It was agreed at the Committee that Freedom to Speak Up is to be included as a regular item
with Safety and Quality at future meetings.
19.2 JPi asked if there is a risk of the Board losing contact with Operational and Clinical Directors as a result of changes to Assurance Committee membership. MR reported that issues are managed through the Quality Improvement and Risk Group with an invitation for further discussion at Assurance Committee if required and appropriate. The Board discussed membership and the reporting process to QIR and Assurance Committee.
19.3 The Committee ratified the following policies: • Isolation Policy • Staff Reward and Recognition Policy • Organisation Change and Consultation Policy • Policy on Obtaining and Providing References • Ant-Fraud, Corruption and Bribery Policy • Urinary Catheter Policy • Management of Allegations of Abuse Against Staff Under Safeguarding Procedure • Consent to Examination and Treatment Policy • Information Governance Policy The Board noted the exception report, approved the Committee terms of reference and the above listed policies.
20 *Mental Health Act Scrutiny Committee Chairs update
Solent NHS Trust Headquarters, Highpoint Venue, Bursledon Road, Southampton, SO19 8BR Telephone: 023 8060 8900 Fax: 023 8053 8740 Website: www.solent.nhs.uk
Page 8 of 9

20.1 Next meeting to be held on 16th February 2017.
21 *Governance and Nominations Committee
21.1 AMS briefed the Board on business transacted at the Governance and Nominations Committee. • MW agreed to attend Associate Hospital Management Training. • The Board were informed of the nominations to the Deputy Chair and Senior Independent
Director role. • The amended terms of reference of the Committee were approved. • The Committee approved the Trust standing orders.
The Board approved the NED Committee membership as detailed in the exception report, the Lead NED and Deputy Chair and Senior Independent Director roles. The Board also approved the Standing Orders acknowledging that further action will be required following a further amendment to the scope of the MHASC following the February meeting. The Board approved the revised MHASC terms of reference.
22 Audit and Risk Committee
22.1 Next meeting to be held on 9th February 2017.
Any other business
23 Items to cascade to other committees
23.1 There were no items for cascading.
24 Governor comments and questions
24.1 No governors in attendance and no questions raised by observers.
25 Any other business & future agenda items
25.1 No further business was requested.
26 Close and move to Confidential meeting
26.1 No further business was discussed and the meeting was closed.
Solent NHS Trust Headquarters, Highpoint Venue, Bursledon Road, Southampton, SO19 8BR Telephone: 023 8060 8900 Fax: 023 8053 8740 Website: www.solent.nhs.uk
Page 9 of 9

Action tracker – In Public Board
Action no.
Date of Meeting
Agenda item ref: Concerning Action detail
Exec Lead / Manager Update for February 2017 meeting
543 30.01.2017 5 Matters arising - Board to Floor
JPi highlighted that he had not yet received a schedule of Board to Floor visits for the year. MR to investigate and arrange distribution as soon as possible. MR
Complete. Schedule reviewed and reissued.
544 30.01.2017 8.12 CEO Report and STP Plan
AMS challenged the unmitigated score concerning the IT risk. It was agreed that AW review the BAF score. AW
Complete - the unmitigated risk score has been reduced.
545 30.01.2017 9.2
Quality Improvement Programme - Qtr 3 Update Report
RC referred to item 3.3 of the report regarding the need to involve patients more with change within the Dental Service and suggested a more holistic approach to ensure business as usual. MR acknowledged the importance of stakeholder involvement in service mapping. It was agreed that the Board reflect on a strategy for public involvement and patient engagement at a future Seminar. RC to add to the agenda RC
Complete - Scheduled on agenda for April Seminar
546 30.01.2017 11.1 Safe Staffing Report (6 monthly)
MR highlighted an inaccuracy in WTE figures on the table detailed on page 3 and circulated the revised information. Update to be uploaded onto the website JE Complete
547 30.01.2017 11.3 Safe Staffing Report (6 monthly)
MT asked if the Assurance Committee should receive a deep dive on workforce issues in relation to not fully addressing all staff groups in care hours per patient. MR agreed the need to present to ensure clarity around new models in an ever changing environment. It was agreed to present to the March Committee.
MR/JE for agenda Complete -Added to the agenda cycle.
548 30.01.2017 13.4 Performance Report - Finance
AMS commented on the difficulty in reading the finance tables detailed within the report and asked that the font size is increased in future reports. AS Considered for all future reports
Item 4.2
Page 1 of 2

Action no.
Date of Meeting
Agenda item ref: Concerning Action detail
Exec Lead / Manager Update for February 2017 meeting
549 30.01.2017 14.2 Qtr 3 2016/17 Business Plan Review
MT referred to the reference ‘Treat people with respect, giving equal emphasis to physical and mental health’, commenting on the Trust’s transposed priority. It was agreed to change wording to ‘mental health and physical health’. AS
For full year review wording to be amended
550 30.01.2017 14.3 Qtr 3 2016/17 Business Plan Review
AMS asked if the Trust understands the acuity of caseload for mental health. SA reported on a 5 year trend of data available and highlighted issues with regards to lack of secure accommodation. It was agreed that SA raise concerns with NHS Improvement. SA Complete
551 30.01.2017 18.2 Charitable Funds Committee Minutes
Regarding item 11.4, JPi queried if the terms of reference should still include reference to an independent examination of accounts. It was agreed that the wording of 11.4 be further amended RC Complete - TOR amended
540 28/11/2016 20.3
Third party contractor policy compliance
JS enquired whether third party contractors must comply with Solent policies. In response SA described the work being undertaken to provide assurance in relation to contracts and subcontracts, however it was agreed that consideration be deferred to the Commercial Subcommittee in relation to policy compliance. Action: SA. SA
Jan 2017 - Due to Commercial Group in January 2017. Particularly complete. Commercial to work with Quality HT to create something pragmatic. March 2017 - Work complete, presented at commercial committee, due to be presented at assurance committee.
Page 2 of 2

Title of Paper CEO Report –March 2017
Author(s)
Sue Harriman, Chief Executive Officer Executive Sponsor
Link to strategic Objective(s)
Improving outcomes Working in partnership Ensuring sustainability
Link to CQC Key Lines of Enquiry (KLoE)
Safe Effective Caring Responsive Well Led
Date of Paper 17th March 2017 Committees presented
N/A
Action requested of the Board
To receive For decision
1. Statement on quality, finance and performance This is covered in full within the integrated performance report. 2. Strategic update Sustainability and Transformation Plans (STP) Solent NHS Trust remains totally committed to working with partners in Hampshire and the Isle of Wight (HIOW) to deliver the transformation programmes with the HIOW STP. As we move from planning phase to delivery we have considered how to strengthen the governance and decision making required to ensure successful delivery. To support this it is clear that some of the plans must be delivered at a local level and so Local Delivery Systems have been created. These systems will ensure the plan is delivered with a focus on local need, issues and opportunities. There will still be a need for us to work at scale with the whole STP footprint so that the services provided by our Trust benefit from the opportunity that scale creates. A contemporary update will be provided at Board. NHS Statement of Support for Tobacco Control. Solent has signed up to the NHS Statement of Support for tobacco control. This is a statement which has been endorsed by Public Health England, the Care Quality Commission and the British Medical Association. Many CCG’s and Trusts have signed the commitment. Signing the statement provides a visible opportunity to commit to taking action to reduce the harm caused by smoking. It commits organisations to actively support local work to reduce smoking prevalence and health inequalities. It is entirely in line with our values and services offered. Information Governance- General Data Protection Regulations The European Union (EU) Parliament & Council announced on the 27th April 2016 a new General Data Protection Regulation (GDPR) that became law on the 24th May 2016 and will come into enforce on the 25th May 2018. The GDPR will supersede the Data Protection Act (DPA) 1998. It has been confirmed that as the UK will still be part of the EU on the 25th May 2018, that the GDPR will be mandatory for the UK, for at least the period in which it remains part of the EU. What will change? Data Subjects (Patients and Staff) will notice more empowerment: • Wider rights of subject access and information about processing • Greater transparency about processing, and, • Stricter conditions for consent and right to object
x x x
Item 8.1
x
X
Page 1 of 7

Organisations will notice the focus on increased accountability and pro-active, evidence-based compliance • Thorough risk assessments, and the principles of ‘privacy by design’ and ‘data protection
by default’ • Requirement to maintain accurate records of all data processing activities, • Increased regulatory enforcement powers and penalties • Stricter breach notification to regulators and to individuals affected It is important to note that this is not a waiting game until May 2018 and involves a huge amount of preparation work, involving a change in processes, practices, documentation and organisational culture. The GDPR will see organisations needing to demonstrate greater openness, accountability and needing to be pro-active with regards to the use, sharing and security of data. The key aspects of work that Solent NHS Trust needs to implement ahead of May 2018 are; • Appointing a Senior Data Protection Officer (DPO), with the appropriate (high level)
accountability, responsibility and qualifications for Data Protection. This role will need to be appointed ASAP (advised by April 2017), so that the work programme (available upon request from the Information Governance Team) that the Data Protection Officer will be accountable for can be rolled out, ensuring Trust compliance with the GDPR. This role will need to be embedded within the organisational culture and a key advisor to the Board and CEO on all matters that directly or indirectly affect Personally Identifiable Data.
• Review of all documentation and processes that support the collecting of, sharing of, storing of and security of data. The Data Protection Officer needs to be fully embedded within these processes. These include
o Contract review, compliance and sign-off o Information Sharing Agreement processes, review and sign-off o Privacy Impact Assessment processes, review and sign-off o Data Flow Mapping, Corporate Record Inventory, etc… monitoring and
compliance o Privacy Notice Implementation – to meet new standards o Resource Reviews to ensure Information Governance and GDPR compliance
• The Trust will need to review its consent processes, with regards to the sharing of information, as the GDPR no longer accepts implied consent
• Organisational culture change. The GDPR and the DPO must be fully embedded within the organisation post May 2018, to ensure Privacy by Design / Default.
It is important to note that the ICO have stated that Directors and CEO’s could be held personally liable and fined for Data Breaches, where they have knowingly failed to provide adequate security and resources to prevent such breaches and comply with requirements of the GDPR, including that of the Data Protection Officer and ensuring they are fully resourced in order to carry out their duties. The full detailed report as presented to the Assurance Committee will be circulated separately to Board meetings. Update on Executive Team We have successfully appointed to the Chief People Officer position following the assessment centre held on 9th March 2017. Helen Ives will be joining the Executive Team in April following the Easter break.
Page 2 of 7

Following the departure of Alex Whitfield, Chief Operating Officer for Southampton and County Services, Lesley Munro has been appointed as Interim COO and a recruitment process for the substantive appointment has commenced. Mandy Rayani, Chief Nurse will also be leaving the Trust to be the new Executive Director of Nursing, Quality and Patient Experience at Hywel Dda University Health Board in Wales. We are also recruiting to this position and Assessment centres for both posts will take place in April. CQC inspection The CQC action plan is being monitored via the CPMO with individual service lines, via Care Group and Quality Improvement and Risk meetings and the Assurance Committee. The CPMO are monitoring progress of actions through completion and validation of evidence. To date, 7 actions (4%) are yet to be started ,80 (44% ) are in progress and 93 (52%) are completed and are awaiting validation. As part of the assurance of the CQC action plan process a number of Quality Review (QR) visits are planned in March which will test, validate and challenge service responses to the CQC Must /Should Do actions. The outcome of the QR visits will be documented and reported to Assurance Committee. County Services Mobilisation within Sexual Health services continues and will be in place for 1st April, with the final details being negotiated on prior to contract signature. Southampton System There has been a strong executive level oversight of system wide performance within Southampton and South West Hampshire. There has been a target to reduce delayed transfers of care within University Hospitals Southampton NHS Foundation Trust, to below 100 by the end of March. Whilst improvements have been seen within Southampton, and patient flow has been maintained, an increase in delayed transfers of care has also been evident within our community inpatient beds. Work continues with Southampton City Council to reduce these. Attendances at the Emergency Department are not significantly higher, for the cohort of patients we would be involved with, as can be seen from the numbers of patients seen and returned home with support by the Community Emergency Department team. Specific details can be seen within the performance report. The “Assess at Home” work, previously reported on has continued to be further embedded within the system and an additional 22 patients will be able to be accommodated from April. This is already having a positive impact on the system and Delayed Transfers of Care. Work has begun to progress with University Hospitals Southampton NHS Foundation Trust, actively exploring what further pathways could be better integrated across the system. This work is also being replicated with Southampton Primary Care Limited (SPCL) to maximise opportunities with primary care, and there is a plan to do a similar piece of work with other providers. Mobilisation continues with two other services, with a new contractual model, by 1st April. This relates to the new Behaviour Change Service, and Community Wellbeing Service. An Interim Operations Director has been appointed to backfill Lesley Munro and will take up the role on a secondment basis from 24th April 2016. Portsmouth System The Portsmouth system continues to be challenged in urgent care performance with the outcome that people are in the wrong part of the system and there are AE and ambulance
Page 3 of 7

delays.A significant factor is the inability to discharge from Portsmouth Hospital Trust caused partly by simple discharge processes, and partly by a backlog in medically fit patients waiting for access to domiciliary care and care homes. The backlog needs to be cleared and proposals are being worked up to urgently address this. The same problem is also impacting the community wards and a recent audit is indicating inappropriate use of community beds. Significant work to mitigate staffing pressures in Mental Health and adults continues to be a priority for the services. The CCG are supporting Solent and the Primary Care Alliance to develop a change programme focused on improving community based services and are keen to see an alliance contract formed between the parties to signal a commitment to a more formal partnership in due course. The alliance contract is really a Memorandum of Understanding (MOU) and commitment to formal working on transformation. We are currently amending this to ensure it is flexible enough and does not place any undue commitment or risk on Solent The new Clinical Director – Adults Services has commenced in post. Tim Trebble has a split role between Solent leading the service line and making a major contribution to leading the change with primary care, and also as a medical consultant at PHT. Priorities for the year ahead A summary of our priorities are outlined below; Our Plan We will provide great care This means that we:
• design care based on peoples’ needs, using best evidence • support people to be safe and well in our community • treat people with respect, giving equal emphasis to physical and mental health • ensure services are safe and effective, and give good experience
We will create a great place to work This means that we:
• focus on employee health and wellbeing • behave in accordance with our core values • provide our staff with the opportunity to learn and develop • value staff option and carefully listen and respond to what staff say.
We will deliver great value for money This means that we:
• deliver joined-up health and social care • collaborate with our partners to spend money effectively • involve our community in decisions about how our services could be redesigned • enable services to have more time to provide care.
Our 2017-19 business priorities Great Care
1. Improve quality in line with CQC inspection requirements 2. Provide safe staffing 3. Use Technology to work differently
Page 4 of 7

Great place to work 4. Plan for long term sustainable staffing 5. Enhance our leadership throughout the organisation 6. Provide training that enables us to deliver great care
Great value for money
7. Further pathway integration with other providers 8. Benchmark our services to improve productivity 9. Change front line and corporate service to live within our income.
Finance The YTD deficit is £3.1m (plan £3.4m deficit) with a forecast out-turn of £3.3m deficit (plan £3.5m deficit). If this is achieved, Solent will receive an additional £0.2m STF income, decreasing our reported deficit to £3.1m. ICT Work continues with our IT service provider (CGi) to complete the move to the new IT network solution, while this work is largely progressing to plan there have been some specific delays on the Royal South Hants hospital site due to the need to replace some of the local infrastructure. This work continues to be a priority and the network stability has continued to improve as this work has progressed. Work is also underway to roll out Solent’s new telephony and communications solution which will combine the use of traditional phones and Skype style instant messaging and calling. This will provide the Solent teams with improved functionality and will significantly reduce call charges across the organisation.
3. Current news Current Trust news is available on the trust website www.solent.nhs.uk 4. Complaints A total of 22 Complaints were received in February 2017 and 32 different concerns were raised across these complaints. The individual details of each complaint are available but the breakdown of concerns is detailed in the table below:
Appointments 5 Attitude of staff 7 Clinical treatment 12 Communication 8
Adults Portsmouth received the highest number of complaints (6). Key themes identified are missed or delayed visits, communication and attitude of staff. The service senior leadership team are reviewing the available information and investigating the specific complaints to determine the action required. At the end of February 2017 there were 56 open complaints awaiting a response. The Complaints team has proactively worked with the Services to support liaison with complainants and facilitate the closure of the complaints. There are currently four complaints which are open to investigation with the PHSO, one of which was referred in February.
Page 5 of 7

5. Update from the Trust Management Team (TMT) meeting - February 15th 2017 Following the approval of the revised Terms of Reference (see Item 8.2) the first of the revised meeting formats was held. Notably; • Membership has now been broadened to include Clinical Directors and Associate
Corporate Directors as well as Operational Directors • The meeting is now held in three parts; Part 1: CEO update, Part 2: Wicked Issues and
Part 3: Formal Business Highlights from the meeting are as follows; • Part 1: A contemporary update was provided by the CEO in relation to STP
developments • Part 2: The Committee agreed the priority areas of focus concerning the ‘wicked issues’.
An update was provided with regards to a review being conducted in relation to corporate and service line interfacing meetings and planned review of the organisations’ hierarchy.
• Part 3: The Committee were briefed on the Board Assurance Framework, delivery of the financial plan, care group business plans and exception reports from reporting subgroups and service lines.
The next meeting will be held on 29th March 2017. 6. Board Assurance Framework and Corporate Risk Register
Board Assurance Framework
BAF number Concerning Lead exec Raw score Mitigated score
(Current score)
Movement since last reported
(and previous
score)
Target score
13 ICT Dan Meron S4x L4 = 16 S4 x L3 = 12 (12) S3 X L3 = 9
55 Workforce capacity Andrew Stevens S5 X L4 = 20 S4 X L3 =12 (12) S3XL3= 9
57 Quality Governance and quality improvement Mandy Rayani S4 XL4 = 16 S4 X L3 =12
(12) S3 x L2 = 6
58 Future organisational function Sue Harriman
S5 X L4= 20 S4 X L4 = 16 (16) S3 X L2 = 6
59 Business as Usual Andrew Strevens
S4 XL4 = 16 S3 X L4 = 12 (12) S3 XL2 = 6
KEY: = same as previous, increase in score decrease in score
Corporate Risk Register The Risk register is a ‘live’ register of the risks identified by service lines. New risks are added to the register and existing risks and associated mitigation arrangements are reviewed each month. The following have the greatest prevalence on the risk register:
• Estates • Staffing • Contracts • Information Technology • Access to services
Page 6 of 7

As of the 1st March, the highest scoring risk on the register (25) is staffing on the Adult Mental Health Ward Hawthorns with a target risk score of 8. There are an additional 4 high risks scoring 20.
• Three relate to estates projects each with a target risk score of 10 and • the fourth is a Sexual Health Service risk detailing the insufficient online testing;
with a target score of 6. Sealings No items to report Signings No items to report Sue Harriman Chief Executive
Page 7 of 7

Page 1 of 5
Solent NHS
Trust Management Team Meeting
1 CONSTITUTION 1.1 The Trust Management Team Meeting (TMT) oversees the effective operational management of
the Trust. Its primary purposes are to;
be the key forum for sharing contemporaneous intelligence concerning the health and care system and other strategic matters from the CEO with the Senior Leadership Team
facilitate resolution of ‘wicked issues’
ensure delivery of the Trust’s annual operating plan and financial plan.
1.2 The TMT is an Executive Led committee.
1.3 The TMT has established a number of groups to execute its responsibilities as follows :
Workforce Group
Equality and Diversity Group
Information and Technology Group (inc. ICT, informatics and IG)
Care Group Boards
Performance Subcommittees (Portsmouth, Southampton & County, Corporate)
Partnership Management Groups
Task and finish groups as necessary (for example time sensitive programme boards)
and will receive reports from the Finance and Commercial Group (decisions above financial threshold to be escalated to the Finance Committee).
The TMT Sub-committees/working groups are directly accountable to the TMT. 1.4 The meeting will be structured as follows (unless determined by the Chair)
Section 1: 1 hour – CEO Update
Section 2: 1 hour – Wicked issues
Section 3: 1 hour – Formal committee business / information sharing 2 DUTIES 2.1 Section 1: CEO update
The CEO or their deputy will provide contemporary intelligence regarding the national and local health and social care system and strategic updates of significance to Solent NHS Trust. The Leadership team will be responsible for the relevant consideration and cascade as appropriate.
2.2 Section 2: ‘Wicked issues’ On an annual basis the Committee will determine the ‘wicked issues list’ for the year ahead. The list for 2017 includes the following:
risk register,
workforce planning and performance management of,
e-rostering,
complaints,
SIRIs,
mortality,
e-learning (and wider learning culture),

Page 2 of 5
estates/support for relocations and moves,
individual staff/talent management,
meeting culture/behaviours and delivery The above list is not exhaustive and the Committee may identify other issues during the course of the year. Senior leaders are expected to establish ‘task and finish’ groups and work collectively to identify effective mitigations and resolutions, escalating issues to the Executives as appropriate.
2.3 2.3.1
Section 3: Formal Committee business Development and delivery
Responsible for the development of the o Annual Operating Plan, o Financial plan and o associated workforce plan and annual corporate objectives, prior to approval at Board.
To establish delivery programmes against the plans referenced above and seek assurance that the plans are being appropriately delivered.
To seek assurance against the delivery of other key plans and programmes of work including; o Sustainability & Transformation Plan (STP) workstreams
2.3.2 Operational Oversight
To oversee the operational delivery of the Trust by receiving assurances from the Performance Subcommittees. As escalated by the Performance Subcommittees, to deal with significant and unresolved variance concerning targets/projections and agree mitigation plans. To ensure mitigations plans are followed through.
2.3.3 Matters of escalation
To deal with matters escalated from the operational service lines/care groups. To receive exception reports from the Chief Operating Officers concerning their respective care groups.
To provide assurance on matters as appropriate to the Trust Board or its Committees and to escalate issues as necessary.
To execute executive actions from the Trust Board or Board Committees as directed.
2.3.4 Risk Management
To oversee the appropriateness of risks included within the Board Assurance Framework and seek assurance that plans are appropriately being executed to mitigate the risks to the target/tolerable level
To oversee the appropriateness of risks included within the Corporate Risk Register and seek assurance that plans are appropriately being executed to mitigate the risks to the target/tolerable level
Executive directors to flag all risks >12 (including those relating to the STP workstreams) to TMT associated with the delivery of plans or operational matters and to ensure risks are incorporated on the Corporate Risk Register or Board Assurance Framework as necessary. TMT to oversee the mitigating actions associated with the identified risks.
Page 3 of 5
2.3.5 Reports from subcommittees
To receive exception reports from the Chairs of each of the reporting subcommittees.
To deal with unresolved issues as escalated.
3 Membership 3.1 The TMT comprises:
Chief Executive (Chair)
The Executive Team o Chief Operating Officer Southampton & County (Deputy Chair) o Chief Operating Officer Portsmouth & Commercial Director o Director of Finance & Performance o Chief Nurse o Chief Medical Officer o Director of HR and OD
(or their deputy where the Executive Director send their apologies)
Representatives from Services Lines – either the Operational Directors and/or Clinical Directors
Corporate Associate Directors / Corporate ‘Heads of’
Chairs of the reporting Groups listed in section 1.3
3.3 Attendance by Members: Members are required to send an appropriate deputy where they themselves cannot attend. Members are expected to have devolved accountability for their lead areas and be aware of the key issues to raise a TMT and to endorse/support TMT decision making.
4 Attendees 4.1
The following will be attendees
The relevant Director may request that their deputies/first line reports attend some or all of the meetings as appropriate.
4.2 The TMT may call upon any employee to attend the meeting.
5 Secretary 5.1 The Company Secretary shall nominate a secretary to the committee.
5.2 The administration of the meeting shall be supported by nominated secretary who will take
minutes of the meeting and provide appropriate support to the Chairman and committee members.
5.3 The agenda and any working papers shall be circulated to members five working days before the date of the meeting.
6 Quorum 6.1 No business shall be transacted at the meeting unless the following are present;
the Chair or their nominated deputy;
a minimum of two Executive Directors
The CEO or the Director of Finance must always be in attendance.
7 Frequency 7.1 The TMT will meet ten times a year

Page 4 of 5
8 Notice of meetings 8.1 Meetings of the committee shall be summoned by the secretary of the committee at the request
of the Chairman.
8.2 Unless otherwise agreed, notice of each meeting confirming the venue, time and date together
with an agenda of items to be discussed, shall be forwarded to each member of the committee, any other person required to attend and all other non-executive directors, no later than 5 working days before the date of the meeting. Supporting papers shall be sent to committee members and to other attendees as appropriate, at the same time.
9 Minutes of meetings 9.1 Minutes of the meeting will be shared with the members following agreement by the Chair.
10 Authority 10.1 The TMT has no powers, other than those specifically delegated in these Terms of Reference.
10.2 The TMT is authorised:
to seek any information it requires from any employee of the Trust in order to perform its duties
to call any employee to be questioned at a meeting of the TMT as and when required.
10.3 The Chief Executive, through the TMT, will hold Directors via their service, managers, senior managers and clinicians, accountable for the operational management of their areas of responsibility.
11 Reporting 11.1 All reports to the Committee will be presented in accordance with the agreed corporate
templates.
11.2 The Chief Executive will report by exception to the Board on a monthly basis via a formal written report.
11.3 The Chief Executive will report by exception to the Board on any significant risk matters that could impact on the Trusts’ strategic objectives, via the presentation of the Board Assurance Framework on a monthly basis.
11.4 The TMT shall make whatever recommendations to the Board it deems appropriate via the Chief Executive Report.
11.5 All reporting Groups are required to report to the TMT via exception reporting. 11.6 The TMT shall identify the matters for cascade to the rest of the organisation /groups as
appropriate. Version 10.0
Agreed at TMT Date: 25thJanuary 2017
Date of Next Review Date: January 2018

Page 5 of 5
Trust Management
Team Meeting
Solent NHS Trust
Operational Governance Structure
CEO REPORT TO BOARD
CEO
Workforce Group
Information and
Technology Group(Inc. ICT, Informatics
and IG)
Weekly Directors
meetings
Chair – Chief Executive
Equality &
Diversity
Care Group
Boards
1. Southampton
2. Portsmouth
3. County - tbe
Performance
Subcommittees
1. Portsmouth
2. Southampton /
County
3. Corporate
Finance and
Commercial Group
Chair – Chief Executive
Portsmouth /
Southampton
Estates
Rationalisation
Programme Boards
Working
Differently Board
Partnership
Management
Groups
[xxx]
[xxx]
CPMO Reporting
Monthly
At each meeting
Monthly
Monthly Quarterly Every 2 months
Every 2 months
Monthly Weekly

Board Report – In Public Meeting
Title of Paper Foundation Trust (FT) pipeline considerations
Author(s)
Andrew Strevens, Director of Finance & Performance
Date of Paper 13TH March 2017 Committees presented
n/a
Action requested of the Board
To receive For decision
Link to CQC Key Lines of Enquiry (KLoE)
Safe Effective Caring Responsive Well Led
Although Solent NHS Trust has stepped off the FT pipeline process, it does not mean that it could (or should) not restart the process at a suitable time. This paper has been written to consider the key issues that the Board would need to address in making this decision.
1. Current guidelines
Since the joint working of Monitor and the Trust Development Authority (TDA) under the banner of NHS Improvement (NHSI), no new technical guidance has been issued and there is currently no pipeline of aspirant trusts wanting to become FTs. Therefore, the Monitor publication “Guide for applicants – updated October 2015” remains the most relevant document. This document lays out the authorisation criteria, being:
• Is the trust well-led? • How effective are the governance arrangements in practice? • Is the applicant legally constituted?
Whilst Solent can provide evidence to support the first and third bullet point, the recent CQC rating of “Requires Improvement” means that Solent fails the second test (for the purpose of authorisation). In addition, the recent history of financial deficits and the planned deficits for 2017/18 and 2018/19 would impact on any assessment.
2. Impact of Single Oversight Framework (“SOF”)
The SOF came into operation on 1 October 2016, replacing the Monitor “Risk Assessment Framework” and the NHS Trust Development Authority “Accountability Framework”. In essence, the level of support and/or scrutiny being offered by NHSI is not dependent on whether the provider is a Trust or a Foundation Trust; in addition, the “freedoms” of being a FT are significantly curtailed.
Planning for the financial years 2017/18 and 2018/19 has been managed by NHSI in a top-down way, with each provider organisation being given a control total, with specific levels of non-recurrent support being linked to the agreement of the control totals. Again, there has been no difference in the way Trusts or FTs have been treated.
3. Impact of Sustainability and Transformation Plans (“STPs”)
The STPs that have been produced across England indicate that the future provision of health services will change, with more integrated working. Simon Stevens (CEO of NHS England) recently
Item 9
x
x
Page 1 of 2

stated to the Public Accounts Committee that between 6 and 10 of the STPs would rapidly morph into accountable care organisations or systems.
In addition, Simon Stevens has also described the STPs as having executive decision making powers in the future, i.e. decisions can be made without the formal consent of individual stakeholders.
Therefore, the direction of travel seems to be that there will be fewer organisations in the future. This will impact on Solent (and our local partners) irrespective of our constituted form.
4. Costs
A significant sum of expenditure was spent on the previous application. Although not all tasks would need to be repeated, it is probable that costs of at least £0.5m would be required to complete a successful application. In the light of a tight financial environment, it does not appear that this would represent a good use of taxpayers’ money.
Recommendation
Further to the above considerations, the Board is asked to confirm that it is not an appropriate time for Solent NHS Trust to commence a FT application.
Page 2 of 2

Board Report – In Public Meeting
Title of Paper Annual Staff Survey Results 2016
Author(s)
Helen Ives Executive Sponsor Andrew Strevens
Link to strategic Objective(s)
Improving outcomes Working in partnership Ensuring sustainability
Link to CQC Key Lines of Enquiry (KLoE)
Safe Effective Caring Responsive Well Led
Date of Paper 20th March 2017 Committees presented
Action requested of the Board
To receive For decision
References Solent Strategy: We will be a great place to work Quarter 1 (2016-2017) Mid-Year Engagement Survey and Staff Friends and Family Test (SFFT): September 2016
The purpose of this paper is to update the Board on the Annual Staff Survey results from 2016, provide a comparison with previous results and give assurance on the continuing improvement plan through the Great Place to Work programme.
.
Board Recommendation: The Board is asked to receive and note this report and outcomes.
X
X
Item 10
X
Page 1 of 7

Annual Staff Engagement Survey Results 2016 1. EXECUTIVE SUMMARY The response rate was 55.3%, which is up 10.9% from last year and compares favourably with the national average of 46.5%.; this is a good leading indicator of engagement which is borne out in the actual results and continues the positive trend we have seen through the quarterly Friends & Family Tests. Key points: • Compared to last year, scores are significantly better on 53 questions and significantly worse on
only 2 questions. • Compared to other Mental Health Community (MHC) Trusts surveyed by Pickers, we are
significantly better on 29 questions, average on 53 and worse on 6. • Our overall Engagement score measured by NHS England is 3.83 compared to 3.69 last year. The investment in the Great Place to Work Programme has yielded positive results with a greater focus on People through Learning & Development, Leadership and Health & Wellbeing. Our collective effort to strengthen our culture through continued focus on values and behaviours is taking us in the right direction. Examples of initiatives include the GCC wellbeing challenge, Dragon’s Den, leadership development programmes and improved internal communications. We will need to maintain and strengthen our efforts in order to continue the positive improvements throughout the next year. 2. SUMMARY RESULTS 2.1 Overall Comparison with 2015 and Other Organisations Note: As in previous years, results are reported as either a % or scale summary score (minimum score 1 and the maximum 5). Figure 1. Improvement since 2015
The questions that have significantly decreased are: • Not put myself under pressure to work when not feeling well enough (9% falling to 6%) • Last experience of physical violence reported (82% falling to 72%)
Page 2 of 7
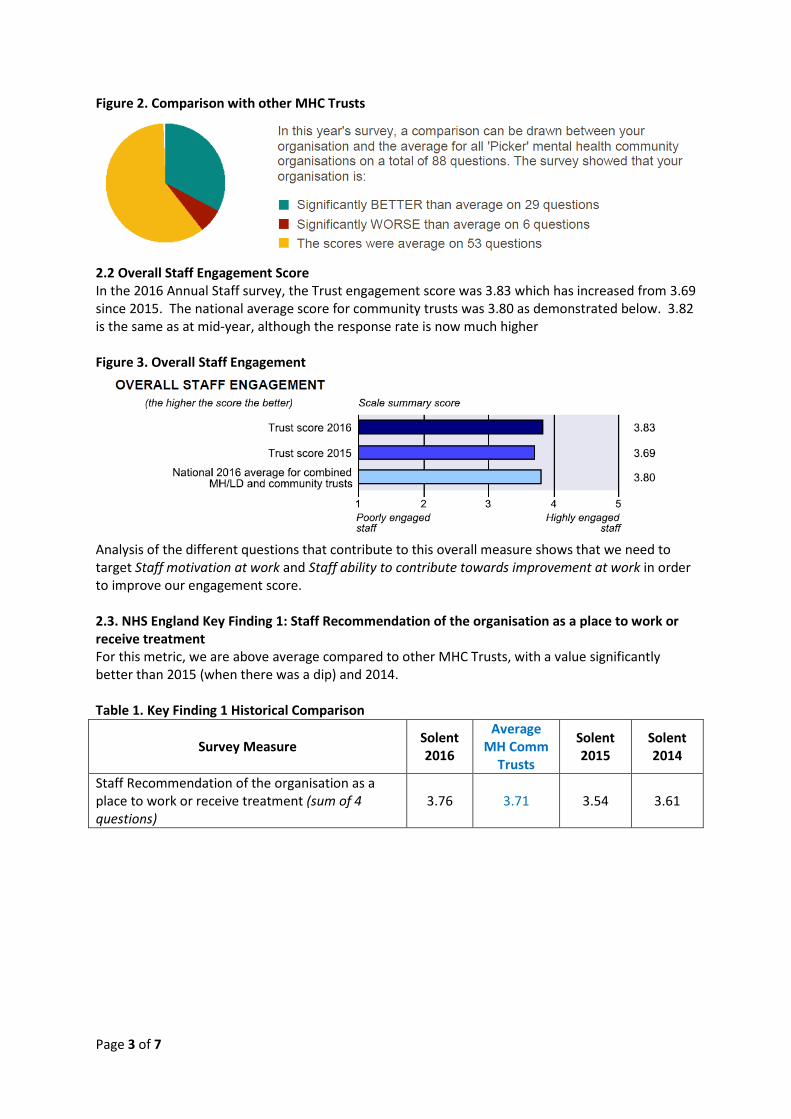
Figure 2. Comparison with other MHC Trusts
2.2 Overall Staff Engagement Score In the 2016 Annual Staff survey, the Trust engagement score was 3.83 which has increased from 3.69 since 2015. The national average score for community trusts was 3.80 as demonstrated below. 3.82 is the same as at mid-year, although the response rate is now much higher Figure 3. Overall Staff Engagement
Analysis of the different questions that contribute to this overall measure shows that we need to target Staff motivation at work and Staff ability to contribute towards improvement at work in order to improve our engagement score. 2.3. NHS England Key Finding 1: Staff Recommendation of the organisation as a place to work or receive treatment For this metric, we are above average compared to other MHC Trusts, with a value significantly better than 2015 (when there was a dip) and 2014. Table 1. Key Finding 1 Historical Comparison
Survey Measure Solent 2016
Average MH Comm
Trusts
Solent 2015
Solent 2014
Staff Recommendation of the organisation as a place to work or receive treatment (sum of 4 questions)
3.76 3.71 3.54 3.61
Page 3 of 7

Graph 1. Organisational Questions Comparison
2. DETAILED RESULTS
2.1 Top & Bottom 5 Results Table 2. Top 5 Ranking Scores
Key Findings Solent 2016 Average
MH/Comm Trusts
Staff confidence and security in reporting unsafe clinical practice
3.89 3.71
Percentage of staff experiencing physical violence from patients, relatives or the public in last 12 months
9% 15%
Percentage of staff experiencing harassment, bullying or abuse from patients, relatives or the public in last 12 months
28% 22%
Percentage of staff appraised in last 12 months 92% 96% Fairness and effectiveness of procedures for reporting errors, near misses and incidents
3.86 3.77
It is positive that the openness culture that the Trust has developed is demonstrated in people feeling able to report unsafe clinical practice if found and that procedures for reporting errors are considered to be fair and effective. Taken together, there is a strong indicator that we have an open and transparent climate for matters of patient quality and care. We have a low % of staff experiencing physical violence; however, from Table 3 below, we can also see that we have a low score on % of staff reporting the last incidence of violence. The same can be said of harassment and bullying. We may, therefore, need to take the strong climate we have for patient quality and care and broaden those principles to include issues relating directly to employee safety and wellbeing. We have appointed Freedom to Speak Up Guardians and early feedback indicates that this is a good opportunity to engage with employees. Staff appraisal completion remains strong, however there are 4 survey questions relating to quality of appraisals where employees report least satisfaction. There will be increased development for managers at a core skills level this year in order to improve the quality of conversation.
75% 78%
56%
74%
0%10%20%30%40%50%60%70%80%90%
Care of patients/ service users is my
organisation’s top priority
My organisation acts onconcerns raised by
patients/ service users
I would recommend myorganisation as a place
to work
If a friend or relativeneeded treatment, Iwould be happy withthe standard of care
provided by thisorganisation
Solent 2014
Solent 2015
Solent 2016
Average MH CommTrusts
Page 4 of 7

Table 3. Bottom Ranking Scores
Key Findings Solent 2016 Average
MH/Comm Trusts
Percentage of staff/ colleagues reporting most recent experience of violence
74% 88%
Staff satisfaction with resourcing and support 3.28 3.33 Staff satisfaction with the quality of work and care they are able to deliver
3.81 3.89
Percentage of staff/ colleagues reporting most recent experience of harassment, bullying or abuse
57% 58%
Effective team working 3.86 3.87 There is an opportunity to improve staff satisfaction with resourcing and support, which may also be linked to effective team working and staff satisfaction with the quality of work and care they are able to deliver. Organisational priorities for 17/18 include sustainable staffing, safe staffing and productivity improvement and service line business plans will deliver against these. 2.2 Employee Comments & Themes Respondents are given the opportunity to comment in a free text box at the end of the survey. We received 301 comments and identified the following themes as the main areas requiring further attention and discussion:
• Lack of learning and career development • Funding restraints • Staffing Levels • Feeling undervalued and low morale • Stress
Positive comments related to supportive team spirit and management. 3. SERVICE LINE RESULTS Overall engagement scores for service lines are currently being recalculated by our service provider and will be provided in due course. See Appendix 1 for a graph of results for the questions:
• Would recommend as a place to work • If friend/ relative needed treatment would be happy with standard of care provided by
organisation Adult Services Southampton, Primary Care and Corporate Services have high scores across both measures. Children’s Locality West has low scores. More detailed analysis will be provided when all results can be considered.
Page 5 of 7

4. Conclusions Actions we have taken over the last year to improve employee engagement include:
• Launch of the Great Place to Work programme, which puts a focus on the development of leaders, teams and our culture through the HEART values
• Greater focus on Health & Wellbeing through initiatives like the GCC Challenge • Increased access to learning and development, including leadership programmes and clinical
skills • Ability for people to get involved and feel empowered, e.g. Dragon’s Den and Quality
Improvement Programme • Improved internal communications and engagement
It is extremely positive to see that we have seen the largest changes since 2015 in our areas of focus. Table 4. Largest Changes since 2015
Key Findings Solent 2016 Solent 2015
Staff satisfaction with level of responsibility and involvement 3.90 3.80 Organisation and management interest in and action on health & wellbeing
3.79 3.62
Staff recommendation of the organisation as a place to work or receive treatment
3.77 3.54
Quality of non-mandatory training, learning or development 3.99 4.08 In addition, 7 of 11 leadership/management questions have increased since 2015 and every measure has shown improvement since 2012, which evidences the positive outcome of the investment made in leadership development over time. Employees tell us that the quality of leadership (line and senior manager) is vital to their satisfaction at work and an area where we must continue to pay attention. 5. Next Steps It is recommended that we continue to focus our organisational efforts for the year ahead on building employee engagement through the following:
• Great Place to Work programme - development of leaders, teams and our culture through the HEART values
• Health & Wellbeing • Learning and development • Involvement and empowerment • Internal communications
In addition, it is critical to ensure that organisational priorities of safe and sustainable staffing and productivity improvements are effectively led and monitored through the service line business plans. A more empowering approach to action planning has been designed where teams work with their managers to determine their Top 3 Actions for the year ahead. They then feedback what the Top 3 should be for Solent as a whole. This will be monitored through an Engagement Forum framework, where each segment of our workforce is represented by employees and sponsored by an Executive. The significant improvement in results for 2016 demonstrates that with organisational commitment and leadership support we can continue to drive improvement over the next year.
Page 6 of 7

APPENDIX 1: Service Line Results for two Organisational Questions
Page 7 of 7
Mental Health Services Benchmarking Report
2016
Matthew Hall Clinical Director – Mental Health
Item 11
NHS Benchmarking Network
• Collaborative organisation for NHS Trusts/providers – not statutory!
• Purpose is to allow comparison of service provision and outcomes between Trusts
• All Mental Health Trusts take part • Produce a number of annual and occasional
reports
Inpatient and Community Mental Health Benchmarking Annual Report • Compares each NHS provider across 31 areas
– Service provision – Outcomes – Quality – Staffing
• Data sources: HSCIC, HES, CQC, ONS, Trusts’ own data submission • Individual Report for each Trust, showing relative position in each
metric against others.
• Report helpful in service planning, quality improvement and contractual discussions

Example data set

Key Findings for Solent NHS Trust
DATA GUIDANCE
Difficulties in the of calculation of working age adults population for Portsmouth have led to some challenges in
interpretation of a few data sets.
All findings shown are in categories not affected by working age adults population size.
The implementation of a new Clinical Records System,
partway through the sampling period means that some categories were not fully reportable this year.

Working Age Adults - admissions
• Longer lengths of stay are associated with decreased disability
• CQC guide optimum bed occupancy 85%. Portsmouth people always have a Portsmouth bed!
• Increased proportion of MHA
admissions reflects low bed use. Portsmouth in fact is a low user of the Mental Health Act.
• Lower cost of admissions allows more to be spent on community and crisis care

Older Adults - admissions
• Slightly more reliant on hospital beds than average
• Still more likely than average to admit than treat in community
• Progress made in “right-
sizing” bed stock and developing out of hospital care in past 12 months – continuing work on developing community care support, before any further changes.

Community mental health services
• Within the usual benchmarking range for: – Total caseload sizes – Proportion of different diagnoses – Contacts – Patient satisfaction
• Lower than average contacts with people
considered “difficult to engage”. We are working on the local rationale for this result, including determining if it is a real finding or a question of different use of diagnostic coding.

Quality
• Ongoing national nurse recruitment challenge, BUT we can secure good quality Agency staff.
• Serious incidents reported on
wards are above average. This reflects a good reporting culture (100% of staff independently surveyed on behalf of the CQC stated that they reported incidents that could hurt staff or other patients).
• Reports of violence towards
staff is above average(although patient on patient violence is low). Most of the incidents relate to a very small number of individual patients.

Quality
Solent has the lowest rate of these types of incidents in the region: • Ligature incidents • Use of restraint (overall) • Use of prone restraint

SUMMARY
• Solent inpatient services for working age adults are
performing well and are safe and good value, BUT we need to continue monitoring to ensure standards remain high.
• We continue to be slightly over-reliant on beds for
Older Adults – this is not the most effective way of providing care. This has improved in the past 12 months, however.
• Recruitment of Qualified Nurses in inpatient services
remains our greatest challenge.

Solent NHS Trust Headquarters, Highpoint Venue, Bursledon Road, Southampton, SO19 8BR
Telephone: 023 8060 8900 Fax: 023 8053 8740 Website: www.solent.nhs.uk
Document Control The latest approved version of this document supersedes all other versions, upon receipt of the latest approved version all other versions should be destroyed, unless specifically stated that previous version (s) are to remain extant. If any doubt, please contact the document author.
Approval Sign-off (For formal issue)
Approver Role Signature Date Version
Alasdair Snell Head of Performance 20/03/17 V0.1
February 2017
Performance Report Part I
STATEMENT OF PURPOSE To provide the Trust Board with the Performance Report
DOCUMENT OWNER Andrew Strevens, Director of Finance & Performance
TARGET AUDIENCE Trust Board
FOR INTERNAL OR EXTERNAL PUBLISHING
External Publishing
MARK AS APPROPRIATE
May be published via our public website: Yes
Commercial Sensitive / Confidential – for internal use only: No
Restricted circulation: No
VERSION:
V0.1
Version Date Author / Editor Details of Change File Reference
V0.1 16/03/17 Alasdair Snell – Head of Performance
Document Creation
R:\Provider Services\Trust Board Reports\2016‐17\Trust Board\February\M11 – February\Board Report Part I FebruaryV0.1.pdf

1. Operations Performance ............................................................................................................................................ 2
1.1 Solent Hotspot Report ................................................................................................................................... 2 1.2 Southampton and County Care Groups – Month 11 Chief Operating Office Review ................................... 3 1.3 Portsmouth Care Group – Month 11 Chief Operating Office Review ............................................................ 5
2. Quality & Risk .............................................................................................................................................................. 6
2.1 Quality Performance ...................................................................................................................................... 6 2.2 Serious Incidents ........................................................................................................................................... 7
3. Finance......................................................................................................................................................................... 8
3.1 Month 11 2016/17 Actual and Full Year Forecast ......................................................................................... 8 3.2 Capital ............................................................................................................................................................ 9
4. Workforce .................................................................................................................................................................. 10
4.1 Workforce Establishment ........................................................................................................................... 10 4.2 Staff Turnover ............................................................................................................................................ 12 4.3 OD Programme & Staff Survey .................................................................................................................. 12
5. ICT & Transformation ............................................................................................................................................... 13
5.1 Clinical Records System Replacement ........................................................................................................ 13 5.2 ICT Transition .............................................................................................................................................. 13 5.3 Business As Usual ....................................................................................................................................... 14 5.4 Patient Systems ........................................................................................................................................... 14 5.5 Enterprise Data Warehouse and Data Assurance ....................................................................................... 15 5.6 Information Governance .............................................................................................................................. 15
Contents
Trust Board Performance Report Part II Solent NHS Trust
February 2017 Page 1 of 15

1. Operations Performance Report
1.1 Solent Hotspot Report
SMS Southampton
Paediatric Therapy Waits
Dental General Anaesthetic Lists
Health Visitors Recruitment
Sexual Health Mobilisation
CQC Review –Delivery of Action
Plan
Data Quality –Systm 1
Podiatric Surgery
Agency Spend
AMH Vacancies
UDA Delivery
Continuing Care Staffing
Community Nursing Vacancies
Delayed Transfers of Care136 Suite
Behavioural Change
Mobilisation
Portsmouth CAMHS Waiting
Times
Trust Board Performance Report Part II Solent NHS Trust
February 2017 Page 2 of 15

2. Chief Operating Officer Report – Southampton & County Wide Care Group
1.2 Care Groups’ Performance ‐ 2016/17 Month 11
An Interim Operational Director for Adults Southampton has been recruited to; Catherine Smith will be joining Solent on 24th April from Southern Health Foundation Trust.
System Pressures
As reported in the CEO report, there has been ongoing weekly executive oversight of system wide delayed transfers of care. The aim has been to get the levels of delayed transfers of care below 100, which has not yet been achieved. The table below shows the breakdown of some of this information. A workshop is being scheduled for April to agree next steps and additional actions that all partner organisations can take.
Performance Hot Spots
Behaviour Change ‐ The Behaviour Change Service is being mobilised for April 1 2017 as a partnership arrangement with two voluntary sector organisations, SCA and Southampton Voluntary Services (SVS), however there are still a number of outstanding contractual issues that require resolving between the partner organisations before April 1, which are being closely worked on.
Trust Board Performance Report Part II Solent NHS Trust
February 2017 Page 3 of 15

GA Waiting Lists ‐ There is continued concern over the waiting lists for General Anaesthetic (GA) appointments within the Special Care Dental Service; however positive conversations are on‐going with all theatre providers to secure additional theatre space in order to reduce the backlog. The biggest area of concern is the waiting lists at University Hospital Southampton (UHS) and Basingstoke. A dedicated working group has been formed to address the issues.
UDA Delivery ‐ Despite a new tariff being agreed with NHS England for Units of Dental Activity (UDAs), the service faces a challenge to meet the minimum contracted target for 2016/17. The final year‐end position will not be known until May which is in line with the submission deadlines for activity.
Podiatric Surgery Waiting Lists ‐ Further progress has been made regarding the Podiatric Surgery waiting lists, and all patients have now been allocated to a provider and will be seen by the end of Q1 17/18. However, of the remaining 12 patients to be seen under the block contract with NHS Portsmouth CCG, 10 will be seen by the end of March and the remaining two on 1 April.
Sexual Health Service Mobilisation ‐ The mobilisation of the new Sexual Health Services contract is well underway; however concerns around the unknown impact of the closure of services at Frimley Park Hospital (FPH) are increasing. Due to the open‐access nature of Sexual Health Services, the volume of activity previously delivered at Frimley, which may transfer to Solent clinics (likely Aldershot), is unknown and as a result capacity planning is having to be modelled around assumptions. There are active negotiations taking place to mitigate or eliminate concerns and issues.
Roster Sign‐Off – The Trust are putting concerted efforts into signing off their rosters 4‐6 weeks in advance to ensure appropriate staffing levels and minimise agency utilisation. A significant improvement has been seen in the second month of monitoring, particularly in the Special Care Dental Service.
Community Wellbeing service – This is a redesigned service within community nursing which will go live from 1 April. The lead provider is Solent Medical Services with whom we are working closely as we move into live mobilisation. There are no specific outstanding issues with this mobilisation.
Trust Board Performance Report Part II Solent NHS Trust
February 2017 Page 4 of 15

1. Chief Operating Officer Report – Portsmouth City Care Group
1.3 Care Group Performance ‐ 2016/17 Month 11
System Pressures
The first meeting of a combined Adult Delivery Board for Portsmouth was held in February, bringing together colleagues from Community, Mental Health and Primary Care Services as well as the City Council and CCG, with a view to creating a single plan and direction for the city.
The reduction in Delayed Transfers of Care in the Portsmouth Community and Mental Health Wards has continued into Month 11, after increased Social Care provision in the management of packages of care.
There are early indications of a rising demand for community services; capacity and demand analysis is now urgently underway.
The acute trust continues to experience pressures in the urgent care pathway, and the backlog of medically fit for discharge patients is part of the problem. The backlog is caused in the main by lack of access to domiciliary care and an alternative approach is to be proposed.
Whilst the backlog continues and wards cannot be closed, the funds flow to deliver discharge to assess remains at risk.
Performance Hot Spots
AMH Staffing ‐ Although there has been recruitment within AMH in recent months, temporary staffing continues to be high and an area of concern and cost pressure. A full analysis and proposed staffing approach has been reviewed and approved in principle by the Chief Nurse and Chief Operating Officer, which recognises an ongoing reliance on block booked agency.
CAMHS Waiting Times ‐ The Future in Mind funding received by the Children & Adolescent Mental Health Services (CAMHS) saw the waiting list reduced temporarily while additional capacity was filled. Due to mental health complexities, the duration on the caseload varies between patients and existing capacity is not sufficient to reduce the current waiting lists to within the 8 week threshold. The service is working with commissioners to review the model moving forwards to best serve patients.
136 Suite ‐ The current arrangements for staffing and provision of the 136 Suite were due to end as at March 2017, however it is now expected to be extended potentially for a further year, due to the complexities of a model that serves multiple populations safely.
Southampton Substance Misuse Services ‐ Agreement in principle reached with Southampton City Council (SCC) regarding the transfer of the Substance Misuse Service. Awaiting final confirmation from SCC regarding novation date and incoming provider.
SMS three month prescriber review standard continues to receive focus as it is not achieving the agreed trajectory.
Trust Board Performance Report Part II Solent NHS Trust
February 2017 Page 5 of 15

2. Quality, Risk and Professional Standards Performance Report
2.1 Quality Performance
Overall, Solent NHS Trust showed positive movements across most elements of Quality measurements in February.
The total number of incidents reported this month is the lowest this financial year, but replicates the picture from February 2016. The number of clinical incidents continues to rise which reflects the improving reporting culture, but the number of patient, staff and visitor accidents / incidents have all reduced this month, the most significant being within the patient accident / incidents category.
Following a reduction in the number of Serious Incidents (SIs) in January (the lowest for the year), there were 15 incidents in February. It is important to note that nine of the SI’s that occurred are category 3 or 4 pressure ulcers acquired in Solent’s care. The number of grade 4 pressure ulcers reported as acquired in Solent’s care, has been stable since August. Despite this, Adults Portsmouth continues to report the highest number of grade 4 pressure ulcers.
The number of Serious Incident investigations breaching the 60 day deadline remains a concern. It is important to note there has been a slight improvement during February. Increased support by the Quality and Risk team is planned for Adult Mental Health
The trend in information governance breaches continues to decline. The Information Governance Team started to deliver bespoke IG training at the end of June 2016 and it was anticipated that there would be in an increase in IG incidents for a short period of time, as staff become aware of what they should be reporting, which took place. However it was also expected that this would start to decrease as staff become greater aware of the safeguards that should be in place to prevent breaches and this is evident that between December 2016 and February 2017, IG incidents have gone down.
Within Patient Experience we have seen the number of service concerns increase for a second month and have now surpassed the total received in 2015‐16; this reflects the aim of the Trust that complaints are dealt with and resolved at the local level. This has been reflected in a reduction in the overall number of formal complaints received. The number of formal complaints not completed within 30 days remains above target but has fallen for the second consecutive month, with only 2 breaching this month. The Complaints team is completing a review of the response times and the findings will be presented to the Complaints Scrutiny Panel.
The actions arising out of our Care Quality Commission (CQC) visit continue to be monitored and reviewed at Service Level, reporting to the Quality Improvement and Risk Group and by exception to the Assurance Committee. We will triangulate evidence of completion and the embedding of change and actions at the Quality Review visits that are planned for March.
Trust Board Performance Report Part II Solent NHS Trust
February 2017 Page 6 of 15

22.2 Serious Incidents Requiring Investigation (SIs)
SI’s February 2017
A total of 15 incidents occurred in the month of February 2017 which met the threshold for serious incident investigation. The table below outlines the areas where the incidents occurred and a reference to the type of the incident:
Directorate Category Number of Incidents
Adults Portsmouth Information Governance 1
Adults Portsmouth Pressure Ulcer 4
Adults Southampton Pressure Ulcer 5
Adults Southampton Treatment Delay 1
Adults Mental Health Unexpected Death 2
Childrens Information Governance 1
Childrens Unexpected Death 1
Grand Total 15
In addition to the incidents identified above, ten incidents classified as High Risk incidents requiring investigation took place as tabled below:
Directorate Category Number of Incidents
Adults Mental Health Unexpected Death 2
Children and Family Self‐Harm 1
Primary Care Treatment Delay 5
Primary Care Information Governance Breach 1
Primary Care Sub Optimal Care 1
Grand Total 10
All incidents are being investigated in line with Trust policy.
Trust Board Performance Report Part II Solent NHS Trust
February 2017 Page 7 of 15
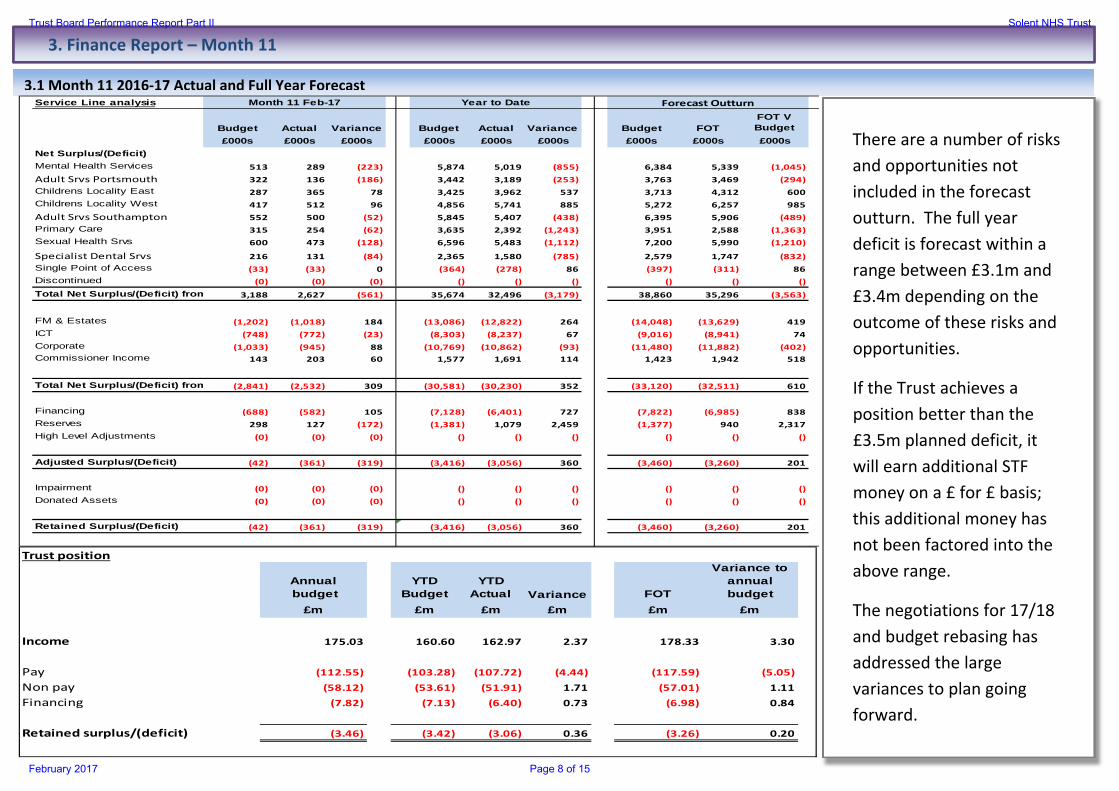
3. Finance Report – Month 11
3.1 Month 11 2016‐17 Actual and Full Year Forecast
Service Line analysis
Budget Actual Variance Budget Actual Variance Budget FOTFOT V Budget
£000s £000s £000s £000s £000s £000s £000s £000s £000sNet Surplus/(Deficit)
R1Mental Health Services 513 289 (223) 5,874 5,019 (855) 6,384 5,339 (1,045)
R1Adult Srvs Portsmouth 322 136 (186) 3,442 3,189 (253) 3,763 3,469 (294)
R1Childrens Locality East 287 365 78 3,425 3,962 537 3,713 4,312 600
R1Childrens Locality West 417 512 96 4,856 5,741 885 5,272 6,257 985
R1Adult Srvs Southampton 552 500 (52) 5,845 5,407 (438) 6,395 5,906 (489)
R1Primary Care 315 254 (62) 3,635 2,392 (1,243) 3,951 2,588 (1,363)
R1Sexual Health Srvs 600 473 (128) 6,596 5,483 (1,112) 7,200 5,990 (1,210)
R1Specialist Dental Srvs 216 131 (84) 2,365 1,580 (785) 2,579 1,747 (832)
R1Single Point of Access (33) (33) 0 (364) (278) 86 (397) (311) 86
R1Discontinued (0) (0) (0) () () () () () ()
Total Net Surplus/(Deficit) from 3,188 2,627 (561) 35,674 32,496 (3,179) 38,860 35,296 (3,563)
R1FM & Estates (1,202) (1,018) 184 (13,086) (12,822) 264 (14,048) (13,629) 419
R1ICT (748) (772) (23) (8,303) (8,237) 67 (9,016) (8,941) 74
R1Corporate (1,033) (945) 88 (10,769) (10,862) (93) (11,480) (11,882) (402)
R1Commissioner Income 143 203 60 1,577 1,691 114 1,423 1,942 518
Total Net Surplus/(Deficit) from (2,841) (2,532) 309 (30,581) (30,230) 352 (33,120) (32,511) 610
R1Financing (688) (582) 105 (7,128) (6,401) 727 (7,822) (6,985) 838
R1Reserves 298 127 (172) (1,381) 1,079 2,459 (1,377) 940 2,317
High Level Adjustments (0) (0) (0) () () () () () ()
Adjusted Surplus/(Deficit) (42) (361) (319) (3,416) (3,056) 360 (3,460) (3,260) 201
74Impairment (0) (0) (0) () () () () () ()
47Donated Assets (0) (0) (0) () () () () () ()
Retained Surplus/(Deficit) (42) (361) (319) (3,416) (3,056) 360 (3,460) (3,260) 201
Month 11 Feb-17 Year to Date Forecast Outturn
Trust position
Annual budget
YTD Budget
YTD Actual Variance FOT
Variance to annual budget
£m £m £m £m £m £m
Income 175.03 160.60 162.97 2.37 178.33 3.30
Pay (112.55) (103.28) (107.72) (4.44) (117.59) (5.05)
Non pay (58.12) (53.61) (51.91) 1.71 (57.01) 1.11
Financing (7.82) (7.13) (6.40) 0.73 (6.98) 0.84
Retained surplus/(deficit) (3.46) (3.42) (3.06) 0.36 (3.26) 0.20
There are a number of risks and opportunities not included in the forecast outturn. The full year deficit is forecast within a range between £3.1m and £3.4m depending on the outcome of these risks and opportunities.
If the Trust achieves a position better than the £3.5m planned deficit, it will earn additional STF money on a £ for £ basis; this additional money has not been factored into the above range.
The negotiations for 17/18 and budget rebasing has addressed the large variances to plan going forward.
Trust Board Performance Report Part II Solent NHS Trust
February 2017 Page 8 of 15

3.2 Capital
Capital Expenditure Description Project Status M11 YTD £000
M12 FOT £000
Total FOT £000
Plan 16/17
Variance Under / (Over)
TOTAL PROJECTS COMPLETED 288 288 295 7
Backlog Maintenance 2016-17 In progress 1,622 (2) 1,620 1,404 (216)CRS phase 3 In progress 111 22 133 280 147Enterprise Data Warehouse In progress 297 27 324 284 (40)Orchards Soton CF In progress 13 67 80 50 (30)WIFI In progress 29 25 54 242 188Clinical Research RSH In progress 43 18 61 30 (31)SMH Catering CPU In progress 78 78 229 151RSH Receipt & Distribution In progress 75 75 (75)ICT End User Devices In progress 466 72 538 1,049 511Medical Equipment In progress 52 9 61 450 389St James Oven In progress 22 19 41 (41)TOTAL PROJECTS IN PROGRESS 2,733 332 3,065 4,018 953
Falcon Relocation to Battenburg Approved, not started 15 15 30 160 130Portsmouth Estates Reconfiguration Phase 2 Approved, not started 422 38 460 2,354 1,894St James Hosp phase 1 Approved, not started 24 125 149 136 (13)Kite Not approved 4 11 15 53 38Jubilee House Not approved 13 9 22 (22)Thornhill / Woolston Not approved 14 11 25 119 94SJH / SMH Reception Integration Not approved 50 50Bitterne Health Centre Not approved 50 50
Capital Reserve Not started 150 150TOTAL PROJECTS NOT STARTED 492 209 701 3,072 2,371
TOTAL PROJECT SPEND 3,513 541 4,054 7,385 3,331
The full year capital expenditure forecast is £4.1m, within our revised Capital Resource Limit (CRL) of £4.2m
The planned CRL of £7.4m includes £2.4m spend on Portsmouth Estates Reconfiguration, to be funded by a capital loan. The loan application has been delayed due to on‐going negotiations with NHS Property Services and so the spend has not occurred in this financial year. This, along with lower spend on ICT end user devices, has contributed towards a £3.3m underspend against the planned CRL.
The spend on Portsmouth Estates Reconfiguration YTD reflects the detailed design costs that were necessary when the Trust went out to tender; tendered costs were reflected in the approved business case. Contracts have not yet been awarded due to the delays in agreeing the contribution to costs with NHS PS.
Trust Board Performance Report Part II Solent NHS Trust
February 2017 Page 9 of 15

4. Workforce Performance Report
4.1 Workforce Establishment
Staff in post has increase from 2809.6 in month 10 to 2822.6; this is currently 164.4 WTE above plan not including additional staffing.
All planned reductions within year should now have been realised and whilst there are reasons why plans have not been delivered the increasing gap between planned and actual continues to be of concern, particularly with consistently high additional staffing requirements.
Additional Staffing Additional staffing is 16.8 WTE higher than last month and 60.4 WTE over plan for this month. Each additional staffing type has exceeded target, with bank usage seeing an increase of 16.6 WTE whilst agency increased slightly from 59.1 to 61.3 WTE. All areas except Adults Portsmouth and Estates have seen a decrease in demand. The majority of additional staffing is being used in: Mental Health Services ‐ 69.1 (Orchards, Limes, Oakdene) Adult Services Southampton ‐ 30.4 (Kite, Fanshawe) Adult Services Portsmouth ‐ 26.6 (Jubilee, South Locality) FM & Estates ‐ 23.1 (Housekeeping) Corporate ‐ 20.1 (Commercial Development, Data Assurance Team) Table 1: Additional staffing by service
Trust Board Performance Report Part II Solent NHS Trust
February 2017 Page 10 of 15

Agency ‐ Compliance with NHSi Ceiling
Our reported spend is £472k against a monthly target of £224k in Month 11, we have now exceeded our total annual agency cap by £693k;
The highest spend is within Adult Mental Health due to MH 136 suite cover and vacancies, sickness and high acuity/clinical pressures.
Portsmouth Community services agency usage continues to be high due to high sickness levels and vacancies, staffing levels are currently being reviewed weekly by OD.
Bank continues to secure the best framework rates associated with long term planning and block bookings, with rolling recruitment in place to recruit to current vacancies as well as on‐going recruitment for bank RMN’s and HCA’s .
Newly qualified adverts have produced 40 applicants, interviews will follow through March. Review of e rostering in hotspot agency usage areas underway along with dedicated
resource to address high sickness in key areas.
Table 2: Monthly Agency Spend against NHSI Ceiling
Table 3: Agency Spend against NHSI Ceiling YTD
Trust Board Performance Report Part II Solent NHS Trust
February 2017 Page 11 of 15

4.2 Staff Turnover
4.3 OD Programme & Staff Survey
Turnover decreased to 15.5% this month and is still above plan. The net effect of lower starter numbers compared to leavers is likely to see turnover remain above plan throughout 16/17. Children’s West 21.2%, Adults Southampton 18.2%, Mental Health Services 17.1%, Primary Care 17.1%, and Children’s East/Adults Portsmouth 16.1% have the highest turnover rates. Organisational change and the competitiveness of the local job market are also having a noticeable effect.
At a national level, results have improved this year and it’s good to see all of the various initiatives underway to work on employee engagement. The results from our survey demonstrate a marked improvement for Solent:
Compared to last year, scores are significantly better on 53 questions and significantly worse on only 2 questions
Compared to other Mental Health Community Trusts surveyed by Pickers, we are significantly better on 29 questions, average on 53 and worse on 6
The overall engagement score has increased from 3.82 to 3.69 from last year
The investment in the Great Place to Work Programme has yielded positive results with a greater focus on People through Learning & Development, Leadership and Health & Wellbeing. Our collective effort to strengthen our culture through continued focus on values and behaviours is taking us in the right direction. Examples of initiatives include the GCC wellbeing Challenge, Dragon’s Den, Leadership Development programmes and improved Internal Communications.
Trust Board Performance Report Part II Solent NHS Trust
February 2017 Page 12 of 15

5.1 Clinical Records System Replacement
5.2 ICT Transition
The Patient Systems project team has initiated Phase 3 of the Trust’s Clinical Records System Programme. The aim is to help staff to maximise the benefits of the electronic patient record providing enhanced SystmOne functionality. The team will be working with each applicable clinical service to implement:
Electronic ordering and receipt of pathology tests Internal referrals External electronic communications SystmOne Viewer
Delivering more enhanced SystmOne functionality has progressed this month, specifically:
1. Piloting electronic ordering and receipt of pathology tests with Snowdon Ward and Podiatry as they use all the functions. Our Spinnaker/Jubilee/MSK wards/services declined to be pilot sites;
2. Linking in with the Southampton Adults project to standardise referrals; 3. Making sure the team include requirements from the NHS Standard Contract 2016/17,
relating to sending documents to patients/Referrers in Future State maps; 4. Presenting at Portsmouth GP’s Target meeting, with 150 Practice staff; 5. Electronic ordering supplier Sunquest’s link to Southampton Lab is working for the Snowdon
Unit. A test can be requested and results received back electronically.
Unified Comms (UC)
The ICT team have been working with Bitterne Health Centre to pilot the migration to Skype and Mitel telephony solutions (Unified Comms). This technology is intended to replace multiple legacy telephony solutions with a streamlined Mitel switchboard solution where fixed phones are required (reception desks, consulting rooms etc). The Skype element will provide telephony to other team members via their laptop or PC and will be fully integrated with the existing Skype functionality so will support instant messaging, video conferencing etc.
The final switch over from ‘old world’ to ‘new world’ phones will be completed by 17 March. However, the users on site have already been enabled with Skype telephony and are using the new system to receive calls and contact patients.
The lessons learnt from the pilot site are now being used to support the plan for the roll out of this functionality to the rest of the organisation over the coming months. The Unified Comms team is working with Services to define their public facing telephone numbers and the call handling needs ahead of their transition.
5. ICT & Transformation
Trust Board Performance Report Part II Solent NHS Trust
February 2017 Page 13 of 15

5.3 Business As Usual
5.4 Patient Systems
In preparation for the transition the Skype telephony functionality has been switched on for all staff and training events have been run daily through March with more planned for April and May.
SharePoint
The SharePoint project, which will ultimately provide a replacement for the Trust’s internal facing Intranet site and file management solution, has formally been initiated. Cloud2 have been agreed as the Trust’s SharePoint supplier. The commercials have now been formalised, Cloud2 has signed a contract with CGI and allocated resource. Current priorities are for CGI to finish the project plan for circulation and recruitment to begin for a Solent SharePoint support role.
The Project team has engaged with each of the services and invited the key stakeholders to attend a SharePoint online WebEx booked in the diary for 30 March and on-site workshops booked for 26 and 27 April at Highpoint. Both the WebEx and workshops will be run by Cloud 2. The WebEx will provide a demonstration of a ‘demo’ SharePoint site for staff to see how it will look and operate. The workshops will be the opportunity for services and corporate teams to share their specific requirements which will be fed directly into the configuration.
Housekeeping activities on electronic files including archiving and removing duplicates continues to be a priority for this project. Information Governance has put forward a business case to the ICT Committee for resource to complete this task. This work is essential to ensure the migration to the new solution is as efficient as possible.
Network changes continue with various items of network hardware being replaced at the Royal South Hants Hospital (RSH) to mitigate risk and improve network traffic speeds. There was a network outage at the RSH due to a power test where one of the backup power supplies for the main communications room failed and caused an outage. This was fixed by CGI within an hour.
The team continues to investigate into the eLearning issue. The issue has been pin pointed to the national servers and CGI is working with IBM to resolve the issue.
The Trust has agreed a local rollout plan with all local commissioners regarding greater use of NHS eReferrals. This involves examining how we enable it for some of our services and ensuring it still gives a streamlined referral process for patients and referrers.
The team continues to support the Sexual Health mobilisation project. This is to ensure that the new sexual health contract for 1st April 2017 can operate from day one.
The team continues to support Portsmouth City Council with local smartcard and SystmOne configuration and access.
Trust Board Performance Report Part II Solent NHS Trust
February 2017 Page 14 of 15

5.6 Information Governance
5.5 Enterprise Data Warehouse and Data Assurance
Viewpoint’s roll out to our Service Line pilots took place on week commencing 13 February. Initial feedback was generally positive with room for improvement. Pilot sites have provided detailed feedback which is reviewed and discussed by the Project Team before adding to a continuing development log. Each issue on the log will be addressed by Information Sub Group attendees. Performance issues have been identified and the EDW team are working with our IT supplier to resolve. The Data Warehouse Team efforts are focused on the completion of 2017-18 Commissioner dashboards and KPIs (alongside Performance) and readying ViewPoint for the full Trust roll (not withstanding technical issues) by the end of March.
Information Governance (IG) training compliance is currently 92% (as of 10/02/17) of staff having been trained in IG since the 1 April 2016. However, the majority of non-compliant staff are within the Bank Service. Bank Service have been advised that if Bank Staff do not complete the IG Training by 17/03/17 their contracts will be terminated and therefore not included in our final figures. Minus the outstanding Bank Staff, Solent NHS Trust has achieved 95% compliance.
The IG Team will be completing the annual IG Toolkit Submission on the 31st March 2017 and will be scoring Level 2 / 3 on all requirements, which will make us compliant.
The IG Team will start preparations for implementing the new General Data Protection Regulations, in April. The Trust is required to be fully compliant by May 2018 with this new Regulation
Trust Board Performance Report Part II Solent NHS Trust
February 2017 Page 15 of 15

PATIENT FEEDBACK MAKING A DIFFERENCE
QUARTERLY PATIENT EXPERIENCE REPORT
QUARTER 3
(October-December)
2016/7
SOLENT NHS TRUST VALUES
Item 13
Page 1 of 22
CONTENTS
1. INTRODUCTION
2. PATIENT FEEDBACK MAKES A DIFFERENCE
3. QUARTER 3 PATIENT FEEDBACK
4. CONCERNS AND COMPLAINTS
5. PLAUDITS
6. COMMUNICATING TO OUR PATIENTS THE ACTIONS TAKEN BASED ON THEIR FEEDBACK
7. CARERS
8. ACCESSIBLE INFORMATION AND VOLUNTEERS
9. RECOVERY AND PEER WORKERS
10. PATIENT STORIES
11. CLAIMS
12. SUMMARY AND RECOMMENDATIONS
Page 2 of 22

1. INTRODUCTION
This is the quarter three (Q3) patient experience report for Solent NHS Trust for the period 1 October 2016 to 31 December 2016. Patient experience is one of the 3 domains of quality together with patient safety and clinical effectiveness. The aim of this quarterly report is to bring together a range of ways in which we receive feedback from our patients and their families and to review this feedback to give us insight into patient experience. This insight helps us to know what we are doing well and where we may need to make improvements.
Solent NHS Trust has a quality goal for 2016-2019 to:
Focus on what matters to service users and carers
Information is gathered from a range of methods of feedback, including patient experience activity and complaints. Each source of data provides rich information and is viewed comparatively in this report to determine if there are patterns emerging, enabling the Trust to identify challenges and concerns that need addressing. Where the report highlights areas for improvement the service concerned develops an action plan in order for issues to be addressed effectively and efficiently to ensure the Trust is continually improving.
The Patient Experience report can be viewed on our public website. It is also discussed at the Patient Experience Forum and Board meetings to ensure patient experience is reported and reviewed at the highest level.
At Board level, the Chief Nurse has responsibility for patient experience which includes delivery of the organisation’s patient experience strategy for 2015-2018 and demonstrating that we have used patient experience feedback to improve the experience of care.
For the purpose of this report, the term patient will be used to encompass the alternative terms of client or service user.
2. PATIENT FEEDBACK MAKES A DIFFERENCE
Patient experience is the responsibility of every member of staff. Solent’s Patient Experience Strategy 2015-2018 sets out a commitment to improve experience by putting people at the centre, listening to people’s views, gathering information about their perceptions and personal experience and using that information to further improve care. Solent NHS Trust receives feedback via a number of different methods and although the majority of this feedback is complimentary, we recognise that we do not always get it right and that every comment, concern or complaint that we receive is an opportunity to learn and make improvements. Similarly, compliments and positive free text comments provide the opportunity for us to know what matters to our patients and share with staff to ensure we keep doing what we do well and recognise and acknowledge our staff for the care they provide.
3. QUARTER 3 PATIENT FEEDBACK
3.1 FRIENDS AND FAMILY TEST (FFT) - The FFT gives patients the opportunity to submit feedback to providers of NHS funded care or treatment, using a simple question which asks how likely, on a scale ranging from extremely likely to extremely unlikely; they are to recommend the service to their friends and family if they needed similar care or treatment. The FFT is intended as a service improvement tool, measuring performance continually and enabling increased responsiveness to
Page 3 of 22

near real time feedback. It is also a mechanism to encourage and motivate staff and reinforce good practice.
Bar Chart 1: Trust Overall Percentage of Patients who would and would not recommend Solent services (October-December responses)
The FFT results show an encouraging and consistently high level of satisfaction throughout the quarter for the organisation overall. In Q1, Q2 and Q3 the proportion of patients who have responded that they would recommend Solent services has been maintained at the Trust internal target of 95% and above.
In Q3 Solent received a total of 3719 responses to the FFT across the organisation. This is an increase in comparison to Q2 when 3231 responses were received. During Q3, 3565 people responded they would be extremely likely or likely to recommend Solent services, 58 responded they would not recommend Solent services and 96 responded either they did not know or would be neither likely nor unlikely to recommend.
Solent results in comparison to national FFT results: At the time of writing this report national FFT results for October 2016 are the most recent national results available to compare with Solent’s Q3 results. National results are presented for community services and mental health services separately.
Info graphic data for National FFT Results for Community and Mental Health Services for October 2016
N.B Mental Health data results include Child and Mental Health Services (CAMHS).
Page 4 of 22

Bar Chart 2: Solent Community Results for Q3
Comparing the national results to Solent’s Q3 community results (Bar chart 2) shows that Solent’s community services overall exceed the national results on the measure for those who would recommend community services.
Bar Chart 3: Solent Mental Health Results for Q3
The mental health services results, which include CAMHS and older person mental health services, for Q3 show that Solent mental health services overall have consistently exceeded the national October results on the measure for those who would recommend Solent’s mental health services and that there has been consistency between Q2 and Q3 results. However, in October there was an increase in the proportion who would not recommend Solent Mental Health service. The free text comments included a number of comments about staffing levels in October:
Service Line Level Results for Q3
The FFT feedback is reviewed at service level to provide more detailed understanding of patient experience and the results are accessible to services direct from the technology platform used. In addition, on a monthly basis the Patient Experience team extract the results and the free text comments and distribute to the services enabling as near real time feedback as possible, action planning and learning.
‘more staff are needed as they are not miracle workers’
Page 5 of 22

Table1: FFT Results by Service Line for Quarter 3 (aggregated –October-December results)
Comparing Q2 and Q3 results, there has been an increase in responses within Adults Southampton and the Sexual Health Service. During November the Sexual Health Service launched a 3 month pilot to use email as the method of gaining FFT feedback as responses in the service had been low. Within the first month of the pilot the completion rate improved, and continues to do so. Although the pilot is not yet complete, it is likely the service will continue with this and other service lines are considering implementing this method of gaining FFT. The free text comments provide the detail from which to gain insight into patients experience and this is discussed at a later section of this report.
The Monkey survey, introduced by Children’s services in Q2, is an inclusive version of FFT which empowers very young people to be able to give their own feedback, rather than solely relying on the feedback of parents or guardians. In this format the FFT question is adapted and free text comments are gathered from the young person in a drawn picture format, in place of writing, enabling the sentiment of their experience to be interpreted.
3.2 TRUST SURVEY
The core questions in this survey are those that the research evidence has shown matters most to people who use our services, based on the findings of the Warwick Patient Experience Framework, (2014), and agreed locally with Solent’s Patient Experience Forum.
This survey includes the FFT as the initial question and is followed by 5 ‘I statements’ which ask for a response of either strongly agree, agree, don’t know, strongly disagree or disagree. The number of responses and percentage results for each question are detailed in table 2. There is variance in returns across the service lines as the method of survey feedback varies and in some clinical settings the FFT postcard which asks the FFT question alone is used. The decision on the most suitable survey is made by the clinical service.
In Q3 there has been an increase in the number of teams offering patients the opportunity to provide feedback via these questions (62 teams in Q3 compared to 25 teams in Q2). Of these 62 teams the response rates to the survey ranged from 1 to 159.
Page 6 of 22

Table 2: Core Question survey results for Q3
The responses to these questions from the patients in the AMH service who completed this survey are below the Trusts standard 90% target on all questions. Although there were relatively small numbers of returns of this survey over the quarter, this is disappointing and was also the position in Q2.
The results from all other service lines show an overall high level of satisfaction in relation to these key questions, meeting or exceeding the trust target of 90% on most questions. However, these are aggregated results of all teams in each service line which can mask variances at team level. For example, in response to each ‘I statement’ 12 team’s scores were below the trust target on the statement regarding ‘knowing who to contact’.
Therefore, deeper analysis at service and team level is necessary to gain detailed insight alongside review of the free text comments received. Services are sent monthly reports and an extraction of the free text comments received to enable learning and plan improvements from this form of patient feedback. The Chief Nurse also reviews this detailed information.
3.3. THEMES FROM FREE TEXT COMMENTS AND IMPROVEMENT PLANS
Although the quantitative FFT and survey results are encouraging, and the overwhelming flavour of the feedback the trust receives is positive, it is the free text comments from patients that provide the richest source of information. All free text comments are examined as, even when quantitative results are positive and complimentary, the comments may include suggestions of small changes that can be implemented to improve the experience of our patients.
Page 7 of 22

3.4. Examples of Complimentary comments received in Q3 by each service line:
Comments & Compliments
This display contains positive comments received from service users during Q3 Oct - Dec 2016.
It gives a good grounding for parents to go away and
practice with their child at home.
Children and Families
Caring staff members always positive, helped me reduce my anxiety. Thank you all.
Specialist Dental Services
Practioner was a lovely kind and gentle person. Interventions put
in place have had a hugely positive effect.
Adults Southampton
Happy girls who made it enjoyable to exercise. They are encouraging and fun. Thank you
for your patience and professionalism.
Adults Portsmouth
Without the care, patience and kindness of the staff and patients, I would not have recovered from my
breakdown.
Adult Mental Health
It was lovely to have somebody so caring and thoughtful to attend me.
Primary Care
When using the online service, I found it excellent, quick and
discrete
Sexual Health
Page 8 of 22

3.5 Examples of ‘YOU SAID - WE DID’ learning/ actions from FFT for quarter 3
You said, we did
This display shows improvements that have been in response to patient feedback received during Q3 Oct - Dec 2016.
You said: ‘more staff are needed as they are not miracle workers’
We did: We had a number of vacancies in the crisis resolution and home treatment team which have now been recruited to and staff sickness levels have reduced.
You said: Dinner plates are not hot enough.
We did: Housekeepers now place the dinner plates in the serving trolley to warm
You said: you are unhappy with the timeliness of advising people that they can’t be seen.
We did: We are about to launch a 3 month pilot as a quality improvement project which is aimed at improving patient access and overall experience in accessing the service
and are planning a change in delivery of the way the service is managed
You Said: Broken toilets
We did: The two broken toilets have now been repaired.
Page 9 of 22
3.6 Working Together- Example of a Partnership Approach
During Q3, Solent’s and Southern Health Foundation Trust’s services for people with multiple sclerosis (MS) provided an information day for people with recently diagnosed MS. The day was attended by 14 patients and 6 of their supporters and provides an example of how Solent works collaboratively with patients and partner organisations. The information day included a session provided by a patient titled ‘MS – What it has meant to me – Patient Perspective’. Examples of comments received from this session are:
The feedback from patients and their supporters will be used for planning future information days.
4. CONCERNS AND COMPLAINTS Everyone counts. We take all negative feedback very seriously. Our Chief Executive is notified of all complaints when they arrive in the Trust and reads all responses personally before they are issued. Complaints handling and any trends or themes identified from them are shared and discussed regularly by the Executive Team and the Board. Concerns and complaints are also reviewed within each of the service lines at their monthly governance meetings.
Between October and the end of December 2016 the Patient Advice and Liaison Service (PALS) and complaints Team received a total of 56 new complaints (including one professional feedback and one MP query) and 55 service concerns.
This compares to 69 new complaints and 55 service concerns in Quarter 2 (July – September 2016). The figures show a slight decrease in the number of complaints being raised in Q3. However, it is important to recognise that any reduction in the number of complaints and service concerns is not, as a single factor, an indicator of improved satisfaction. It is also essential to ensure our complaints process is accessible to all our patients.
Services should inform the PALs and complaints team of all concerns they receive and the outcomes so that they are recorded centrally in order to provide an overall understanding of what is important to our patients. Although some service concerns are later escalated to formal complaints, either because the person who raised the concern is not satisfied with the response provided at the local level or because the service are unable to adhere to the time limit that applies, only one concern escalated to a complaint in Q3.
Down to earth and useful
What a super inspiration
Positive knowing everything
Page 10 of 22

Bar chart 4: Number of complaints received by Service Line in Quarter 3 (2016/7)
The position in Q3 is similar to that of Q2. Primary Care received the highest number of complaints but in relation to the number of patient interactions this service line provides by the musculoskeletal and podiatry services in Southampton, Portsmouth and parts of Hampshire, as well as three GP surgeries in Southampton, this is not a proportional variance. The number of complaints related to the AMH service is the same in Q3 as in Q2 (13). However, during Q3 responsibility for Older Persons Mental Health (OPMH) was transferred to AMH from Adults Portsmouth and three of the complaints received by AMH would previously have been considered by Adults Portsmouth. The themes of complaints from this service generally concern issues related to discharge from an in-patient ward or from the Access to Intervention (A2I) team, and issues related to clinical treatment. Complaints received by the AMH service are often made by family members on behalf of patients. Although these complaints are investigated, issuing a response to the person who has made the complaint may be delayed or not possible if the patient has not given their informed consent for this to happen. The pattern of complaints received in Q3 for Adults Portsmouth has not changed since Q2 in relation to the number of complaints received and themes of complaints (sporadic visits, issues relating to clinical care and communication). Children’s Services received fewer complaints in Q3 compared to Q2 (10 to 6 respectively) but the complaints received by Childrens services are often complex and involve more than one service provider.
Page 11 of 22

Bar Chart 5: showing Complaints by Theme and Service Line for Q3
Bar chart 2 illustrates the break down in categories across complaints and provides an indicator of emerging themes. The themes arising from complaints in Q3 reflect a similar pattern to Q1 and Q2 and involve clinical issues (e.g. dissatisfied with medication or diagnosis); appointments (availability of); communication (e.g. lack of guidance, failure to inform about cancelled appointments and failure to follow up); and attitude of staff (e.g. they are perceived as being rude or disinterested in the patient’s condition). Some complaints include more than one theme, for example a complaint may be about a patient’s discharge from the service and the way this was communicated. It is for this reason that in Q3, although 56 complaints are recorded, there are 86 categories identified. Complaints are recorded and categorised to help the Trust identify themes and trends and identify improvement and actions in response to the findings. A monthly complaints report and tracker is produced to enable the services and Trust overall to monitor the categories of complaints and concerns so that issues can be addressed at both Trust wide level and service level in a timely way.
4.1 LOCAL RESOLUTION MEETINGS (LRM) As part of the complaints process a local resolution meeting (LRM) is offered to people who have reason to complain. This will either form part of the initial complaints process to enable additional information to be obtained from the complainant in relation to what they would like investigating or, alternatively, it may form part of the final resolution process when the complainant wants to discuss the formal response they have received.
Solent NHS Trust values the opportunity to meet with people at a LRM so that they can discuss their concerns direct with the service and wherever possible receive an early answer to the issues of concern rather than waiting for a formal response. However, this is the choice of the individual and we recognise that in some circumstances people prefer to pursue the formal complaints process and receive a response from our Chief Executive.
In Q3 the PALs and Complaints Team attended four LRMs as part of the resolution process.
Page 12 of 22
Examples of outcomes and actions following LRMs:
• Safeguarding - A meeting was held to explain and clarify the reasons behind the rapid response process and why information was shared in the meeting. The family felt that they were now better informed about the purpose and reasons for the process and the meetings.
• Sexual Health Service - a second LRM was held as a patient continued to have concerns about the treatment provided for their condition. The service was able to demonstrate that they had learnt from the patient’s experience and changes to clinical procedures have been introduced.
4.2 PROFESSIONAL FEEDBACK
It is important for other clinicians and agencies to be able to provide professional feedback in relation to Solent NHS Trust Services. They, or one of their patients, may have had an unsatisfactory interaction with a service or they may be unfamiliar with processes and require clarification about a particular service. Professional feedback is also an important way for receiving suggestions on how services can improve.
In Q3 in response to professional feedback from GPs in a previous quarter, Adults Services Portsmouth have put a system in place for the community nurse localities to be linked to specific GP practices so that the GPs have a direct contact if they need to escalate any concerns over patient care. This is enabling concerns to be addressed at service level and is preventing the need for a formal escalation via the professional feedback mechanism.
4.3 PERFORMANCE TARGETS
The only nationally prescribed target applies to formal complaints which should be acknowledged within three working days. Although this does not include service concerns, MP queries or professional feedback, the PALs and complaints team aim to meet this target across all concerns raised.. At the time of writing this report, the Trust has achieved 100% compliance for this target in Q3.
Responses
There is no nationally set time frame for responding to a complaint. Solent NHS Trust has set itself a deadline of 30 working days to investigate and respond to the complaints. It is not possible to provide the full figures for Q3 in this report as some complaints submitted in that period are still within the 30 working day deadline. However, for July and August this target was achieved for 78% of complaints compared to the annual figure of 40% for 2015/6. This reflects the work being carried out by, the PALs and complaints team as well as the services, to ensure that complaints are responded to in a timely manner.
When the target is not met the PALs and complaints team are responsible for ensuring communication with complainants to keep them fully informed that the response will breach the deadline. Breaches occur for a number of reasons including that the complaint is in depth and requires a more detailed investigation, the complaint due to its severity may be subject to the serious investigation (SI) process, there may be delays in accessing all the information required for the investigation of the complaint or delays related to staffing issues. In addition complaints may involve more than one organisation which makes achieving the response target more complex and
Page 13 of 22

each provider may have differing response targets. Solent NHS Trust is part of the NHS England Wessex Area Complaints Manager Forum and the protocol for managing joint responses is currently under review.
4.4 COMPLAINTS REFERRED TO THE PARLIAMENTARY HEALTH SERVICE OMBUDSMAN (PHSO)
The PHSO is the second and final stage in the complaints process. In 2013/4 the PHSO released a 5 year plan with a focus in 2014/5 on increasing the number of complaints investigated. In view of this we recognise that our contact with the PHSO may increase, although in Q3 there were no approaches from the PHSO.
The PHSO did conclude one investigation in Q3 relating to the care provided to a patient on one of our Older Persons Mental Health (OPMH) wards. The PHSO did not uphold this complaint and found that the clinical treatment provided was appropriate.
4.5 LEARNING FROM COMPLAINTS
The Trust recognises the opportunity complaints bring to learn and share learning across the organisation to effect improvement for the benefit of our service users and staff. During 2016/17 we have introduced a new complaints tracker to ensure monitoring and completion of actions agreed as a consequence of learning from complaints. This tracker is shared on a weekly basis with the Chief Executive Officer, the Chief Operating Officers, the Medical Director, Chief Nurse, the Clinical and Operational Directors of each service line and Clinical Governance Leads. In addition, the tracker is reviewed on a monthly basis at the Quality Improvement and Risk Group and at monthly service line governance groups. We strive to demonstrate the changes that have been made as a result of the learning from complaints and to sustain the changes for long term improvement. The table below provides examples of themes that have arisen in complaints and the action and learning that has taken place as a consequence:
Table 3: Examples of Complaint themes and actions /learning in Q3
Complaint theme Actions taken
Clinical – delay in communication to patient regarding test results
As a result of this complaint the service has made changes to the way results of specimens (blood, urine, stools) are reported. The results are now reported to the GP or Consultant for actioning. This was a powerful complaint that led to positive changes in practice.
Communication/ staff attitude
The team apologised that incorrect information had been provided regarding the provider of advocacy. Clinical teams have now been made aware of the new provider.
Missed home appointments
A review of the visit triage system is underway to ensure improved prioritisation. Arrangements for recruitment to key positions have been reviewed.
Appointment wait times
The service has reviewed processes for managing waiting times and implemented improved signage at the bespoke clinics.
Onward referral process
The process has been discussed with the clinician concerned to ensure that they action referrals in a timely manner to prevent delay and distress to patients.
Page 14 of 22

Information governance breach
The service has made changes to the printing of letters following clinical appointments as a patient received their letter together with information relating to another patient. Since the new process has been in place there have been no further breaches. This complaint was escalated to a high risk incident and investigated independently of the service. The patient has received an apology.
4.6 COMPLAINTS REVIEW PANEL The complaints review panel met for its second meeting in December 2016. This panel is chaired by one of our Non-Executive Directors together with our Chief Nurse. Membership includes a Healthwatch colleague and senior clinical representatives from each of our service lines. The purposes of the panel are to drive quality improvement in relation to managing complaints and to provide a mechanism for cross organisational learning from complaints. The outcomes and learning from four complaints were discussed and reviewed at the meeting in December. The agenda also included discussion regarding managing persistent or unreasonable complaints and complaint response times. The learning that was shared included:
• Patient expectations concerning the level of service available needs to be managed as early as possible.
• Early attempts at resolution may result in a de-escalation of a complaint
• A policy to manage the process when community patients transfer to our care has been introduced
• The decision concerning whether a patient is considered housebound should be considered holistically
The panel agreed that the current Managing Concerns and Complaints policy requires amendment and strengthening in regards to the management of persistent and unreasonable complaints. It was also agreed that the target for responding to complex complaints will be reviewed by the Head of Patient Experience in consultation with the Chief Nurse, commissioners and the complaints panel members.
4.7 COMPLAINANT SATISFACTION SURVEY The statements of expectations outlined in the user-led vision for raising concerns and complaints in health and social care developed by the PHSO, Healthwatch England and the Local Government Ombudsman provide the framework for our complainant satisfaction survey:
Page 15 of 22

Diagram 1: A user-led vision for raising concerns and complaints in health and social care ‘My expectations for raising concerns and complaints’ PHSO, NHS England, LGO (2014)
All complainants are offered the complainant satisfaction survey at closure of their complaint. Both historically and nationally there tends to be a low response to complainant satisfaction surveys. In Q1 the organisation received only 2 responses with a slight increase in Q2 when 7 surveys were returned. However, the response rate has dropped again in Q3 with only 4 surveys received. The overall proportion of satisfaction across all the questions asked in the survey is 82.5%. All respondents confirmed that they :
• Knew they had a right to complain
• Felt their complaint had been handled fairly
• Felt the outcome they received directly addressed their complaint
• Felt the response was personal to them and the specific nature of their complaint.
However, two of the respondents felt that they did not always know what was happening with their complaint. This is an area where we need to improve as this is a theme that has recurred from Q2.
In the free text comments one commented that they did not feel that their complaint had been answered. However, in contrast, another respondent confirmed that they were ‘…. very pleased and grateful with the outcome. We thank you so much keeping us updated with each step of the way.’
5. PLAUDITS
Plaudits may be received from patients, their family, or members of public, expressing their thanks and appreciation for the care provided. During Q3, 326 plaudits were received, an increase since Q2, and these were spread across all service lines.
Examples of plaudits received in quarter 3:
Children’s Services: ‘I really appreciate all the attention that you've given to **** over the last 2 years, and I understand now why the decision has been reached to close ***** case. Thank you, as always, for all the work you've done with **** over the last 2 years. It's always been much appreciated.’
Page 16 of 22

Adults Portsmouth: ‘Thank you for all of your help with management of COPD to give people the motivation and get up and have a go with your cheerful and bouncy natures. You are a credit to your profession, you are doing a great job'.
Adults Southampton: ‘It is very easy to take the NHS Service for granted, but we would like to put on record how well the service is running and how reassuring all the points of contact were at a worrying time. The calm efficiency of the Nurses who came out to my **** and the nurse who volunteered help and delivered antibiotic tablets to our home late evening were so helpful. With our grateful thanks to all who helped us at a difficult time, we say a big thank you.’
Specialist Dental Services ‘My son was so nervous on his first visit but was helped to relax accept that there may be some pain but assured that it would be better after the treatment. All in all a first class surgery that deserves recognition for their hard work and caring nature.’
Sexual Health Service: ‘* was very friendly and made me feel at ease during the session remaining very professional throughout, 10/10 would let him screen me again.’
Adult Mental Health: ‘To all the staff, Doctors/Nurses at * ward, I am so thankful for all you have done for me, I've never had someone to care for me like you all did, I will miss you all loads, you all are wonderful people, all the best for the future to you all, I am so grateful and appreciated all that you did for me, thank you so much. Take care.’
Primary Care ‘Thank you so very much for all the care, treatment and advice you have given me over the past very important weeks to aid my recovery. A huge enormous thank you! Both * and myself will always be grateful for the support you gave us.’
6. COMMUNICATING TO OUR PATIENTS THE ACTIONS TAKEN BASED ON THEIR FEEDBACK
Actions taken as a result of patient feedback are communicated to both staff and patients by a variety of channels:
• Direct to the patient, e.g. via complaints letters
• ‘You said, we did’ noticeboards at ward and outpatient clinic waiting areas
• Newsletters to staff
• Quarterly reports including this report
• Trust website and intranet
• At the patient experience forum
7. CARERS
A carer is someone who provides support to family or friends who could not manage without this help. This may be caring for a relative, partner or friend who is ill, frail, disabled or has mental health or substance misuse problems. All the care they give is unpaid.
National Carers Rights Day took place on Friday 25th November and was entitled: Missing out? Know your Rights as a Carer.
Page 17 of 22

Solent used this national day of focus on carers to launch our Staff Carers Pledge Permit. This is a communication tool intended to help capture information about how an individual member of staff’s carer responsibilities may impact on their work. It also provides a framework to help staff open up a conversation with their manager and develop a proactive plan to help maintain their wellbeing and performance in work alongside their personal carer responsibilities.
Angela, a Solent member of staff, shares her story of working alongside her caring responsibilities: My father was diagnosed with Oesophageal Cancer at the beginning of January 2016. Up until this point my Father was very capable and able to drive and maintain his own independence and also care for my Mother. However, during this period of time he found it difficult to absorb the amount of information he was given and along with the numerous appointments he needed to attend. Leading up to his treatment, it became very stressful with appointments not being made and needing to be chased many times over. Treatment started in the February 2016; five weeks of Chemo therapy (once week) and Radiotherapy (5 days per week) began. I was extremely lucky to have the most amazing support from my Managers and colleagues. My managers were absolutely amazing allowing me to swop my working days, take annual leave, use my lunch periods in order for me to support my Father through this process. They consistently asked how I was and ensured that I could juggle my hours in order for me to still have some annual leave for myself. They took time to talk to me and I truly felt incredibly supported throughout this whole period. Thinking that once the five weeks were over all would be well, however, Dad was admitted three times after treatment and not once did I feel that I was a burden to the team, instead that genuine support continued throughout this very difficult and emotional period. I cannot express enough how the support from the Managers and my lovely colleagues helped to get me through this tough time and I regard myself as incredibly lucky to be part of such an amazing team. The flexibility shown enabled me to maintain my mental health, continue working and still have some annual leave which I so very much needed at the end of his treatment. In Q3, Adults Services Portsmouth has commenced joint working with Portsmouth Carers Centre to support building effective communication with carers. This joint initiative will form part of a quality improvement programme over the next 12 months. It will aim to ensure carers are identified,
Page 18 of 22

involved, provided with accessible information about services to manage expectations and signposted to support. During Q3, 87 carers gave feedback via the FFT. The proportion who would recommend Solent services in this quarter is 98.85% (86 respondents) and those who would not are 1.15% (1 respondent). The feedback reflects a similar level of positive sentiment to that of the patient FFT and is overall an encouraging finding.
8. ACCESSIBLE INFORMATION (AI) AND VOLUNTEERS
Accessible Information or AI is the name given to the process of making information easier for people with communication and/or information needs. Across Solent NHS Trust it is estimated that 10,000 people struggle to access standard spoken and written information, which in turn impacts on all aspects of their healthcare. From June 2016, all health and social care services must comply with the NHS England Accessible Information Standard.
‘Building Networked Power’
Building on the success of the accessible information training in the summer, in Q3, the newly trained champions have formed the ‘Solent Accessible Information Network’. This network is aimed at supporting collective intelligence and social learning (peer-to-peer) to improve accessible information practice across the Trust. Monthly meetings take place chaired by the clinical lead and the champions are actively engaging in the rolling agenda items (illustrated right). An impressive amount of quality improvement work is evidenced in this meeting and it appears to be an effective way of supporting Trust wide developments at both scale and speed. Solent’s AI Portfolio – ‘Supporting Information for All’, led by Dr Clare Mander, has been selected as a finalist in the national Patient Experience network (PEN) Awards for 2016. Winners will be selected at a celebration event on 21 March 2017.
Page 19 of 22

Recovery is: Living a life worth living – with or without on-going
symptoms
To support the work of the AI network, two types of volunteering roles have been developed ‘Accessible Information Patient Volunteers’ and ‘Accessible Information Support Volunteer’. Our patient volunteers will be people who have communication and/or information needs. Through our collaborative work during the training project, we have identified a patient pioneer ‘Keith’ who is working with us to develop the inclusivity of the volunteering policy. To date, Keith has supported the design of an Easy Read leaflet (left) that explains volunteering and has piloted Talking Mat resources that explore the types of activities our volunteers can support.
It is recognised that some of the patient volunteers may require support to fully engage in activities; therefore support volunteers are also being recruited. To date, we have two volunteers from a local university who are studying a BSc in Human Communication and have previously helped on the training project in a work experience capacity. During Q3 the Specialist Dental Service has been focussing on improving patient experience by developing their accessible information resources for patients attending the General Anaesthetics (GA) clinics concentrating on the Poswillo Centre in Portsmouth and the service based at University Hospital in Southampton. With support from the service a parent of a young person who has autism has developed a story board to help prepare her son before going for the GA. This improved the young person’s experience as he was well prepared for his visit to the dental service and his procedure. Both his mother and his school had talked through the story board with him in the 2 weeks prior to his appointment. Examples of AI resources for GA clinics
In Q4 the service will be asking patients for feedback on the AI resources they have developed. 9. RECOVERY PEER WORKERS In April 2016 a Trust Lead for Recovery & Peer Workers was introduced. This role is designed to explore how the Recovery Approach can improve outcomes for patients, carers and services. We have learnt that a key element in this is to harness the expertise of people who have themselves used the service or had similar health conditions.
Page 20 of 22

Drawing on national and local evidence we find that greatest improvements are made when we move beyond ‘listening’ to people, to using coproduction. This approach means working equally with people who use a service to consider problems, develop and deliver solutions together. Working in this way has been shown to develop more innovative and sustainable results with improved wellbeing for those participating. This can happen in different ways in different services.
Early developments and examples where this work is taking place include:
- A benchmarking exercise is being undertaken to identify where this work is taking place, to gather best practice examples and identify any training needs of staff.
- The Trust’s Volunteer Policy now has specific guidance for Peer Volunteers – people undertaking voluntary roles in which they will use their personal experience to support another (for example someone who used to attend an outpatient service now helping to deliver a group for people who still attend that service).
- Service users in Adult Mental Health have co-developed and co-delivered a training package for staff about how to improve the experience of having their risk of suicide assessed.
- A project to use a Patient Reported Outcome Measure in Adult Mental Health used the
coproduction approach from the beginning including a staff training and consultation process led by service users.
- A work stream to engage adults with Learning Disabilities in the recruitment of staff; service
audits and evaluation has been established.
- Project underway to recruit peer volunteers who live well with diabetes to work with people accessing the diabetic foot clinic. The aim is to improve wellbeing through improved self-management.
- Work underway with a Community Nursing team to enhance methods of gaining patient experience feedback from a vulnerable and disparate client group through projects to tackle social isolation and improve wellbeing.
- Solent Recovery College based in Portsmouth is an exemplar of the benefits of coproduction. In partnership with Solent Mind and Highbury Further Education College, we provide education courses about mental health for people who use mental health services and carers & staff. All courses are developed and delivered by adult mental health staff and peer trainers (people who have / have had mental health issues). We continue to host national and international visitors wishing to learn from our model. Our student outcomes are consistently positive and the power of being taught by someone ‘who has been there’ is consistently identified as a source of inspiration and motivation to make change. We are now working to expand this model for people with other long term conditions.
10. PATIENT STORIES
Patient stories are an extremely powerful way to find out how we make a difference to our patients. The blend of emotion, insight and candour captured from a story is used to facilitate learning and improvements.
Page 21 of 22

Patient stories are heard at our Board meetings, either by patients attending to tell their story direct, by the story being presented by the member of staff or by a video recording.
In Q3, Solent hosted its first Allied Health Professions (AHP) conference which was chaired by NHS England’s Chief AHP Officer. The conference opened with stories from patients who are receiving care from each of Solent’s AHPs (art therapy, physiotherapy, clinical psychology, occupational therapy, podiatry, social work, and speech and language therapy). Patients talked about their personal experience and the difference that the interventions from each allied health profession had made to them.
11. CLAIMS During Q3, two personal injury claims and four Clinical Negligence Claims were received by the Trust.
12. SUMMARY AND RECOMMENDATIONS
The patient experience report aims to bring together a range of sources of feedback to give us insight to better understand what matters to our patients, what we do well and where service improvements are needed. The report evidences how we use the many rich sources of information gathered from patients, how we value patient views, how we listen, how we learn and how we act on feedback to improve the experiences of people who use our services.
Overall patients are reporting a positive experience of care. However, it must be acknowledged that this high level of reporting masks variances and a deeper, granular level of analysis at team level is necessary to fully identify the specific areas where improvements are needed based on our patient’s feedback. This level of analysis takes place by the services and is beyond the scope of this report.
This report has identified specific actions where we need to strive to make improvements in Q4:
• Ensure people who have made a complaint are kept informed on the progress of the investigation of their complaint
• Review of the response time frames for complex complaints • A focus on increasing feedback from carers • Continued roll out of phase 3 of the AI project • Service and team level insight of what matters to their patients and evidence of
improvements made that are communicated to patients • Roll out of new methods for gaining FFT including trial of email and text messaging • Measures to increase feedback on the complaints handling process • Continued roll out of training to staff on managing concerns and complaints
This report has aimed to give as comprehensive a view as possible on what our patients have told us in Q3 and our actions as a consequence. However, inevitably a report cannot capture, nor do justice to, all the ways in which staff strive, on a daily basis, to provide great care. Ann Rice
Head of Patient Experience and Allied Health Professions
16/02/2017
Page 22 of 22

Board Report – In Public Meeting
Title of Paper Chairman’s report on Members Council
Author(s)
Jayne Edwards, Corporate Support Manager/Assistant Company Secretary
Executive Sponsor Dr. Alistair Stokes, Chairman
Date of Paper 27 March 2017 Committees presented
n/a
Action requested of the Board
To receive For decision
Link to CQC Key Lines of Enquiry (KLoE)
Safe Effective Caring Responsive Well Led
Since the report to the January 2017 Board, the following governor activities have taken place:
• The Members Council meeting was held on Friday 10th March where discussions took place regarding the future role of the Members Council in light of the Trust’s previous decision to step off the Foundation Trust pipeline, changing external environment and implications concerning the Sustainability and Transformation Plans (STP). It was agreed that a working group be set up for executives and governors to consider further and produce a recommendation by the end of April.
Forthcoming meetings • Membership Engagement Group meeting to be held on 27th April 2017 at Trust
Headquarters. • A refreshed Planning and Strategy meeting date is to be arranged and will be led by Claire
Budden, Head of Commercial for the Commercial Team.
There are no other matters concerning the Members Council to be brought to the attention of the Board.
Recommendation
• The Board is asked to receive the update above in relation to Members Council activities.
Item 15
x
x

Exception and recommendation report
Committee /Subgroup name
Assurance committee
Date of meetings
14th February & 14th March 2017
Chair Mick Tutt Report to Trust Board
Key issues to be escalated These were the second and third meetings of the – substantially – revised Assurance committee; following previous discussion generated by a series of governance reviews and other comments regarding our approach to the seeking assurance of high quality service delivery and regulatory compliance – on behalf of the Board. As such, we recognised that the revised working arrangements; particularly with a more explicit recourse to the Quality Improvement & Risk group (QIR) for operational matters – and the subsequent alterations to regular attendance – are ‘works-in-progress’ (such as the style of some reports and the collaboration to be achieved between Exception reports from the Chief Operating Officers and from the QIR). In recognition of this, and conscious of the requirement not to dispense ‘babies-with-bathwater’, we agreed to ask our Internal Auditors to review the revised arrangements during the course of 2017/8 and provide a view of ‘fitness-for-purpose’ We received a brief verbal up-date on those actions from the CQC Action Plan, arising from the Comprehensive Inspection during June 2016, which our management colleagues had ‘rag-rated’ as ‘red’ at the February meeting – together with an explanation for the allocated status The March meeting received a more ‘in-depth’ report, which confirmed Directors’ concerns regarding the apparent lack of progress in reaching an agreement with:-
i) NHSEngland regarding an escalation process where forensic or secure provision was indicated
ii) the commissioners for the wheelchair service, provided by a third-party, but where issues and risks were experienced by people accessing Solent services
iii) resolving the concerns raised by the CQC regarding the Substance Misuse service in Southampton
The, apparent, lack of progress with regard to concerns raised about the Children & Adolescent Mental Health Service were also raised by one of the Non Executive Director Members Action being taken was explained, in detail and contingency plans; for future escalation, if required, were outlined It was agreed that the committee would receive a simple schedule, which set out:- those recommendations which had been actioned and were complete those recommendations where action was not yet complete – but there was
(management) confidence of completion within the specified time-frame those recommendations where action was not complete and there was
(management) concern that this would not be achieved
We agreed to receive a formal up-date in 3 months, with matters arising and escalations as required
Item 18.1
acexceptionandrecommendationsreportfebruarymarch17 page 1

We continued the ‘rolling-programme’ of deep-dives – into specific aspects of governance – focussing on Clinical Audit & Effectiveness and Research & Development, together with the work of the Serious Incident Requiring Investigation (SIRI) Panel, at the February meeting and Medicines Management at the March meeting, where we also received a quarterly up-date on Information Governance (IG) compliance We looked, particularly, for assurance regarding the dissemination of learning from our clinical audit and research & development activity – mindful of the comments made during our CQC Inspection; regarding how this could be enhanced. We heard how effective cascade arrangements were in operation within Service Lines and Care Groups, but identified a potential area for further development across the Trust – which, again, was a feature of CQC comment. We asked for Chief Operating Officers (COOs) to consider, with the Clinical and Operational Directors, how this could be progressed and received a full Clinical Audit Plan at our March meeting We also noted the annual R&D ‘celebration’ of activity – this year scheduled for 11th july Our third deep-dive, in February, reviewed SIRI activity – which also incorporated reviews of High Risk Incidents (HIRIs) and Mortality Reviews. Although we were provided with the operational detail, around numbers and compliance with reporting expectations (which, we agreed, could routinely be dealt with by QIR), we focussed on the more strategic issues of Duty of Candour and Non Executive Director (NED) participation in the Panel deliberations The intention to involve people accessing services and their carers in the investigation process was welcomed and we agreed to establish a rota for all NEDs to attend Panel meetings We received a deep-dive report from our new Chief Pharmacist, at the March meeting; which focussed on the:-
i) revised arrangements being made to strengthen medicines management – particularly from the clinical perspective
ii) actions arising from the CQC Inspection, not covered earlier iii) policies, procedures and Patient Group Directives which had been discussed
We clarified the escalation process for these activities and agreed to receive a further up-date in six months The IG compliance was the regular quarterly up-date of Trust compliance with the expectations of the IG Toolkit; which, again, was met. Further discussion, however, centred on the provision of meaningful learning & development associated with IG and the requirement for a ‘cost-benefit analysis’ of the value for striving for a higher IG rating We had planned, also, to receive an up-date on the Trust’s Mortality Review process at the March meeting, but agreed to defer this; because of the ‘Learning from Deaths...new responsibilities for board members’ report launched on 21st March – which, we understood, would shape our future approach to the process. The conference to launch the report was attended by the Chief Medical Officer and the chair of the Assurance committee and the output will be a revised policy and process; which will be progressed as quickly as possible We then looked to our COOs to identify the major risks to high quality services and continued compliance with regulatory requirement, in the two Care Groups The arrangements to provide interim cover for the departure of the COO for Southampton & County were outlined, and the interim COO attended the March meeting
acexceptionandrecommendationsreportfebruarymarch17 page 2

We were informed of the intention to implement the Smoking Cessation policy, ratified last year by the committee, within Adult Mental Health services was scheduled for July ’17. The COO has asked for further confirmation of the realism of this stated intention, for the April meeting We looked for the Quality Improvement & Risk group to both underpin and enhance the assurance received from the COOs and received a report which both:- collaborated some of the issues raised by COOs, particularly of an operational nature raised other issues, largely of a strategic or ‘cross-cutting’ nature
which tended to suggest that the combination of COO and QIR exception reports might be a useful mechanism for triangulating the assurance being provided by various Directors, from the individual perspectives We received the Annual Governance Statements (AGS) from Service Lines, at the February meeting – which will be used to ‘aggregate-up’ a Trust-wide AGS, for inclusion within the Annual Accounts. We made some suggestions for amendments and will look for these within the aggregated AGS We received a quarterly review of achievement against our Quality Priorities at the March meeting, and also discussed the content of the draft Quality Account for 2016/7 – which will build upon the previous years’ work. We noted the timescales for submission of comments on both documents and that the Quality Account, together with the aggregated AGS, would be part of the Annual Accounts; being prepared for the summer
Decisions made at the meeting We ratified the following policies:- At the March meeting:
• Investigation Policy Chairs action was also taken on the following policies following non-material updates:
• Suspension, Exclusion and Transfer Policy • Suspect Package Policy
At the February meeting:
• Dental Radiation Policy • Emergency Lockdown Policy
Chairs action was also taken on the following policies following non-material updates: • Pay Protection Policy
We agreed at the February meeting that the policies submitted; Physical Security Management Policy and the Suspect Package Policy, required further work; which, if completed prior to the next meeting, could be ratified via Chair’s Action We agreed that, contrary to the January ’17 Board discussion, detailed consideration of the workforce concerns, arising from the continuing inability to recruit fully to all our practitioner posts, would take place at the Workforce group; with the Assurance committee considering any quality delivery and regulatory compliance issues which flowed from this
Recommendations to the Trust Board
acexceptionandrecommendationsreportfebruarymarch17 page 3
the Board are asked to note the issues set out above
Other risks to highlight (not previously mentioned)
none of note
acexceptionandrecommendationsreportfebruarymarch17 page 4

Exception and recommendation report
Committee /Subgroup name
Mental Health Act Scrutiny Committee
Date of meeting 16th February 2017
Chair Mick Tutt Report to Trust Board
Key issues to be escalated we noted that, apparently, the Clinical Director (CD) for Children & Families – who was
attempting to investigate an incident involving a young person under 18 years of age who had been taken to the s136 suite, last summer – had yet to conclude this investigation. We asked that the relevant Chief Operating Officer (COO) look into the circumstances around this apparent lack of progress
were informed that the death of a person, detained under the Mental Health Act 1983 (MHA), had occurred in September 16 and that this was, currently, subject to a Serious Incident Requiring Investigation (SIRI) process and, therefore, would be tracked through the reporting arrangements from the SIRI Panel to the Assurance committee
noted the improvement in compliance with the expectations of s132 MHA (ensuring people were ‘read their rights’), and documentation generally, and asked that practitioners were thanked for this up-turn in compliance over the past six months
received a further up-date on the provision of the s136 suite, and received improved data, which was necessary for the committee to scrutinise that the use of the suite fell within contemporary expectation we also heard of the service preparation for the reduction in the time period for holding people under s136, as a consequence of the Policing & Crime Act 2017 – from 72 to 24 hours – and were assured of more detailed arrangements at the next meeting, which will be around the time the change takes effect. The major impact is likely to be for people from outside the Portsmouth locality being conveyed to the suite; because of the difficulties, already experienced, with availability of beds within Southern Health Foundation NHST and the non-attendance of Approved Mental Health Practitioners from Hampshire County Council
we also noted that the next meeting would receive an up-date from the relevant Chief Operating Officer (COO) regarding the anticipated up-grade to the physical environment of the suite received revised reports on the use of restraint and seclusion. These contained some
confirmation that the use of restraint had been within the expectations of the Code of Practice, within mental health services, and more substantive assurance for the Kite Unit, although they were using an alternative method of restraint – which the Chief Nurse requested was reviewed. The reason for limited assurance with regard to the former was because of (electronic) recording issues; but we were assured that these had now been addressed and the next report would be more substantive we were assured that the episodes of seclusion, all within Maples ward, met the expectations of the Code of Practice. We were however informed of one incident which did not comply with the Trust Policy on Seclusion and we asked for an urgent management review of whether the policy required amendment
noted an exchange of letters, between the Deputy Chief Inspector (and lead for mental health), CQC and the Chief Medical Officer, regarding Second Opinion Approved Doctor engagement with our services
Item 19
mhascexceptionreportfebruary17 Page 1

Decisions made at the meeting we noted the revised Terms of Reference for the committee, discussed at the November
meeting and then endorsed by the January 17 Board, but noted that further changes were, probably, necessary; to more accurately reflect the expanded role to include scrutiny of the use of the Deprivation of Liberties Safeguards (DoLS) and the provision of training in both the Mental Capacity Act 2005 and Mental Health Act 1983 we also noted that this would require changes in the Guidance document which accompanied the substantive agenda item for the committee; setting out the statutory expectations
also noted that the Fact Sheet for prospective Associate Hospital Managers required up-dating; to reflect the Code of Practice introduced during 2016
confirmed the style of reporting required for scrutiny of the DoLS activity across the Trust and outlined the expectations for reporting on the provision of training. The former will be received from the next meeting and the latter will be, finally, agreed there
reviewed the degree of assurance provided, through scrutiny of activity, compared to the findings of the recently published CQC annual review of activity; and confirmed that – generally speaking – we were confident that we received information regarding matters which the CQC had drawn attention to
agreed that further thought should be given, initially by the chair, Chief Medical Officer and Chief Nurse, to the involvement and engagement with people who access services (in parallel with similar discussions regarding the Assurance committee)
Recommendations to the Trust Board
the Board are asked to note the issues set out above
Other risks to highlight (not previously mentioned)
Since the meeting the Law Commission have published their recommendations for the reform of Mental Capacity and Deprivation of Liberty, following presentation to the House of Lords The Mental Capacity & Mental Health Acts lead has prepared a short summary of the implications of the publication, which the committee will consider at its meeting in May ‘17
mhascexceptionreportfebruary17 Page 2
Exception and recommendation report
Committee /Subgroup name
Audit and Risk Committee
Date of meeting 9th February 2017
Chair Jon Pittam Report to Trust Board
Key issues to be escalated The following items are escalated for the Board’s attention:
• The outcomes of the two internal audit reports as detailed below concerning Nursing staff arrangements and workforce capacity and Key Financial Systems and in response propose that progress on workforce planning is presented to a future Board Seminar.
Decisions made at the meeting
The Committee:
• noted the Counter Fraud Progress Report – the Committee were informed of the imminent changes to NHS Protect’s remit, which will focus solely on fraud from 1st April 2017. As a consequence it was acknowledged that there are uncertainties in relation to security leadership at a national level.
• approved the Anti-Fraud Bribery and Corruption Policy, acknowledging that the policy will need to be adjusted post 1st April following the changes to NHS Protect.
• received a progress report from the External Auditor, Ernst & Young where it was confirmed that the fee associated for the Charitable Funds Audit has been reduced due to an overall improvement in the quality of the draft financial statements and supporting working papers.
• were informed of the need for national clarification with regards to the accounting treatment of Trusts in recurrent deficit positions in light of the 3 year break even rule and it was suggested that the Director of Finance and Performance raise this matter with NHSI
• received an internal audit progress report from PwC and received the following internal audit reports;
Audit Risk classification Nursing staff arrangements and workforce capacity
Medium
Key Financial Systems Low In light of the Nursing staff arrangements audit the Committee raised concerns in relation to the adequacy of workforce planning and compliance with the policy to agree staff rostering 6 week in advance. Concerns too were raised in relation to the amount of aged debt – however assurance was provided that regular reports will be presented to the Finance Committee in relation to debt recovery.
• noted the timetable associated with the financial audit timetable • received a deep dive presentation from the Chief Nurse in relation to Risk Management
following a number of external reviews and recommendations from the CQC. It was agreed that a further report on progress against recommendations be presented at the August Committee meeting
• received a summary of progress on mechanisms for shared learning and examples of improvement as a result of clinical audit
• received a report on information and cyber security and the mechanisms in place to protect assets and information
• considered key questions in relation to the effectiveness of the Board Assurance Framework and acknowledged that further visibility at a Board level is required concerning the
Item 21.1

Corporate Risk Register, especially the top 5 risks. • Approved the revised Terms of Reference (recommended for Board approval – see Item
22.3)
Recommendations to the Trust Board
The Board are asked to approve the amended Terms of Reference (tracked changes highlighted)
Other risks to highlight (not previously mentioned)
None to report

AUDIT & RISK COMMITTEE
TERMS OF REFERENCE
Reference to “the Committee” shall mean the Audit & Risk Committee. Reference to “the Board” shall mean the Trust Board
1. Constitution
1.1 Solent NHS Trust Board hereby resolves to establish a committee of the Board to be known as the
Audit & Risk Committee (‘the Committee’). The Committee is a non executive Committee of the Board and has no executive powers, other than those specifically delegated by the Board in these Terms of Reference which are incorporated within the Trust’s Standing Orders.
1.2 The Terms of Reference reflect the particular nature of Audit Committees in the NHS and the growing
role of the Committee in developing integrated governance arrangements and providing assurance that NHS bodies are well managed across the whole range of their activities.
2. Purpose 2.1 The Committee is responsible for assuring the Board on matters concerning: governance (including
financial governance, corporate governance and clinical audit): risk management; and internal control, seeking assurance from internal and external audit and counter fraud.
3 Duties
3.1 The duties of the Committee can be categorised as follows: 3.2 Governance, Risk Management and Internal Control 3.2.1 The Committee will seek assurance that the Trust’s activities are efficient, effective and represent
value for money
3.2.2 The Committee shall review the establishment and maintenance of an effective system of integrated governance, risk management and internal control, across the whole of the Trust’s activities (both clinical and non-clinical), that supports the achievement of the Trust’s objectives.
3.2.3 In particular, the Committee will review the adequacy and effectiveness of:
• all risk and control related disclosure statements (in particular the Annual Governance Statement and will review processes to ensure continued compliance with the Care Quality Commission), together with any accompanying Head of Internal Audit statement, external audit opinion or other appropriate independent assurances, prior to endorsement by the Board.
• the underlying assurance processes that indicate the degree of the achievement of corporate
objectives, the effectiveness of the management of principal risks (including ensuring effective use of the Board Assurance Framework) and the appropriateness of the above disclosure statements.
• the policies for ensuring compliance with relevant regulatory, legal and code of conduct
requirements and related reporting and self certification.
Item 21.2

• the policies and procedures for all work related to fraud and corruption as set out in Secretary
of State Directions and as required by the NHS Counter Fraud (NHS Protect) and Security Management Service
• the Trust’s Quality Accounts
3.2.4 In carrying out this work, the Committee will primarily utilise the work of Internal Audit, External Audit
and other assurance functions, but will not be limited to these sources. It will also seek reports and assurances from directors and managers as appropriate, concentrating on the overarching systems of integrated governance, risk management and internal control, together with indicators of their effectiveness.
3.2.5 This will be evidenced through the Committee’s use of an effective Assurance Framework to guide its
work and that of the audit and assurance functions that report to it. 3.3 Internal Audit 3.3.1 The Committee shall ensure that there is an effective internal audit function that meets the Public
Sector Internal Audit Standards, 2013 and provides appropriate independent assurance to the Committee, Chief Executive and Board. This will be achieved by:
• consideration of the provision of the Internal Audit service, the cost of the audit and any
questions of resignation and dismissal. • review and approval of the Internal Audit strategy, operational plan and more detailed
programme of work, ensuring that this is consistent with the audit needs of the organization as identified in the Assurance Framework.
• consideration of the major findings of internal audit work (and management’s response), and
ensure co-ordination between the Internal and External Auditors to optimise the use of audit resources.
• ensuring that the Internal Audit function is adequately resourced and has appropriate standing
within the organisation.
• monitoring the effectiveness of internal audit and carrying out an annual review
• ensuring the periodic re-tendering of the internal audit function 3.4 External Audit 3.4.1 The Committee shall review and monitor the work and findings of the External Auditor and consider
the implications and management’s responses to their work. This will be achieved by:
• consideration of the appointment, cost and performance of the External Auditor, as far as the rules governing the appointment process permit.
• discussion with the External Auditor, before the audit commences, of the nature and scope of
the audit as set out in the Annual Plan, and ensure coordination, as appropriate, with other External Auditors in the local health economy.
• discussion with the External Auditors of their local evaluation of audit risks and assessment of
the Trust and associated impact on the audit fee.
Page 2 of 7

• review all External Audit reports, including the report to those charged with governance,
agreement of the annual audit letter before submission to the Board and any work undertaken outside the annual audit plan, together with the appropriateness of management responses.
3.4.2 In accordance with the Local Audit and Accountability Act 2014, the Committee shall establish an
‘Auditor Panel’ to advise on the appointment of external auditors (membership of the panel will be approved by the Board). The Panel shall recommend the appointment of external auditors to the Board.
3.4.3 To ensure objectivity and independence, the Committee will agree acceptable thresholds and
safeguards for non-audit services conducted by the external auditors. Any such work will be disclosed within the Annual Report. Auditors are expected to identify to the Committee principal conflicts of interest that may be reasonably considered to affect objectivity and independence.
3.5 Other Assurance Functions 3.5.1The Audit & Risk Committee shall review the findings of other significant assurance reviews, both internal
and external to the Trust, and consider the implications for the governance of the Trust. These will include, but will not be limited to, any reviews by Department of Health Arms Length Bodies or Regulators/Inspectors (e.g.TDA, NHS Improvement, CQC, NHS Litigation Authority, Monitor etc.), professional bodies with responsibility for the performance of staff or functions (e.g. Royal Colleges, accreditation bodies, etc.)
3.5.3 In reviewing the work of the below listed committees, and issues around clinical risk management, the
Audit & Risk Committee will wish to satisfy itself on the assurance that can be gained from the clinical audit function.
3.5.4 In addition, the Committee will review the work of other committees within the Trust, whose work can
provide relevant assurance to the Committee’s own scope of work. The Committee may request that the Chairs of the following Board committees attend to provide exception reports;
Committees include:
• Governance & Nominations Committee • Remuneration Committee • Assurance Committee • Finance Committee • Mental Health Act Scrutiny Committee • Charitable Funds Committee
3.5.5 The Audit & Risk Committee will also scrutinise the annual governance review of the Board
Committees conducted by the Governance & Nominations Committee, satisfying itself that committees are appropriately constituted and functioning in accordance with their Terms of Reference.
2.5.6 The Committee will also annually review the accounting policies of the Trust and make appropriate
recommendations to the Board. 3.6 Counter Fraud 3.6.1 The Committee shall satisfy itself that the Trust has adequate arrangements in place for countering
fraud and shall review the outcomes of counter fraud work.
Page 3 of 7

3.7 Management 3.7.1 The Committee shall request and review reports and positive assurances from directors and managers
on the overall arrangements for governance, risk management and internal control. 3.7.2 The Committee may also request specific reports from individual functions within the organisation
(e.g. clinical audit) as may be appropriate to the overall arrangements. 3.8 Financial Reporting 3.8.1 The Committee shall monitor the integrity of the financial statements of the Trust and any formal
announcements relating to the Trust’s financial performance. 3.8.2 The Committee should ensure that the systems for financial reporting to the Board, including those of
budgetary control, are subject to review as to completeness and accuracy of the information provided to the Board.
3.8.3 The Committee shall review the annual report/accounts and financial statements before submission to the Board, focusing particularly on:
• the wording in the Annual Governance Statement and other disclosures relevant to the
Terms of Reference of the Committee • changes in, and compliance with, accounting policies, practices and estimation techniques • unadjusted miss-statements in the financial statements • significant judgements in preparation of the financial statements • significant adjustments resulting from the audit • letters of representation • qualitative aspects of financial reporting • reported losses and compensation
3.8.5 The Committee should also ensure that the systems for financial reporting to the Board, including
those of budgetary control, are subject to review as to completeness and accuracy of the information provided to the Board.
3.9 Whistleblowing /Freedom to Speak Up
3.9.1 The committee shall review the effectiveness of the Trust’s arrangements for its employees to raise
concerns, in confidence, about possible improprieties in financial, clinical or safety matters. The Committee shall ensure that these arrangements allow proportionate and independent investigation of such matters and appropriate follow up action.
4 Membership
4.1 The Committee shall be appointed by the Board from amongst the Non-Executive directors of the
Trust and shall consist of not less than three members at least one of whom shall have recent and relevant financial experience. One of the members will be appointed Chair of the Committee by the Trust Board
4.2 The Chairman of the Trust Board shall not be a member of the committee. 4.3 In the absence of the Committee Chairman and/or an appointed deputy, the remaining members
present shall elect one of themselves to chair the meeting.
Page 4 of 7

5 Quorum 5.1 The quorum necessary for the transaction of business shall be 2 members. A duly convened meeting of
the Committee at which a quorum is present shall be competent to exercise all or any of the authorities, powers and discretions vested in or exercisable by the committee.
6. Attendance 6.1 The Director of Finance and Performance (DoF) and appropriate representatives from External and
Internal Audit will normally attend every meeting.
the external auditor shall be afforded the opportunity at least once per year to meet with the Audit & Risk Committee without executive directors present.
the Committee members shall be afforded the opportunity to meet at least once per year with no others present, at their request.
6.2 The Chief Executive shall be invited to attend all meetings (except when the Committee is meeting in
private). 6.3 The local Counter Fraud (CF) representative will be invited to attend Committee meetings whenever
necessary to report on CF issues. Alternatively the local CF representative may brief the DoF who will provide a report on CF issues.
6.4 The Chief Nurse or Medical Director will be required to attend any meeting where clinical assurance is
required, whilst other Executive Directors or senior managers may be invited to attend, particularly when the Committee is discussing areas of risk or operation that are the responsibility of that Director.
6.5 The Company Secretary, or their nominee shall attend all meetings. 7 Access 7.1 The Head of Internal Audit, representative of external audit and counter fraud specialist have a right of
direct access to the Chair of the Committee. 8. Frequency 8.1 The Committee shall meet at least on a quarterly basis at appropriate times in the reporting and audit
cycle and otherwise as required. 8.2 The Committee will meet in private with External and Internal Audit representatives without any
member of the Executive present on at least one occasion each year. 8.3 The Accountable Officer, external auditors or Head of Internal Audit may request an additional
meeting if they consider that one is necessary. 9. Authority 9.1 The Committee is authorised:
• to investigate any activity within its terms of reference
• to seek any information it requires from any employee of the Trust in order to perform its duties and all employees are directed to cooperate with any requests made by the Committee
Page 5 of 7

• to obtain, at the Trust’s expense, outside legal or other professional advice on any matter within
its terms of reference, and • to call any employee to be questioned at a meeting of the Committee as and when required. • to secure the attendance of outsiders with relevant experience and expertise if it considers this
necessary 10. Secretary 10.1 The Corporate Support Manager or their nominee shall act as the secretary of the committee and will
provide administrative support and advice. The duties of the secretary in this regard include but are not limited to:
• agreement of the agenda with the Chair of the Committee and attendees together with the
collation of connected papers
• taking the minutes and keeping a record of matters arising and issues to be carried forward
• aAdvising the Committee as appropriate 10.2 The agenda and any working papers shall be circulated to members five working days before the date
of the meeting. No papers will be accepted after the original documentation is circulated – except with the express consent of the Chair.
11. Minutes of meetings 11.1 The secretary shall minute the proceedings of all meetings of the committee, including recording the
names of those present and in attendance. 11.2 The secretary shall ascertain, at the beginning of each meeting, the existence of any conflicts of
interest and minute them accordingly. 11.3 Minutes of Committee meetings shall be circulated promptly to all members of the Committee once
agreed. 12. Reporting responsibilities 12.1 The minutes of all meetings of the Audit & Risk Committee shall be formally recorded and submitted,
together with recommendations where appropriate to the Board.The Chair of the Committee shall draw to the attention of the Trust Board any issues that require disclosure to the Board, or require executive action.
12.2 The Committee will recommend to the Board the approval of the Accounts and Quality Accounts. 12.3 The Audit & Risk Committee will report annually to the Board in respect of the fulfilment of its
functions in connection with these terms of reference. Such report shall include but not be limited to:
• providing an objective opinion to the Board on the performance of all of the Board Committees (and as included within the Annual Report)
• functions undertaken in connection with the statement of internal control
• the assurance framework
Page 6 of 7

• the effectiveness of risk management within the Trust
• the holistic nature of governance arrangements and
• any pertinent matters in respect of which the Audit & Risk Committee has been engaged
12.4 The Committee shall make necessary recommendations to the Board on areas relating to the appointment, re-appointment and removal of auditors, the level of remuneration and terms of engagement as it deems appropriate.
12.5 The Trust’s annual report shall include a section describing the work of the Audit & Risk Committee in
discharging its responsibilities and the Committee’s Terms of Reference will be made publicly available. The annual report should explain to members:
• how, if the auditor provides non-audit services, auditor objectivity and independence is
safeguarded
• details of the full external auditor appointment process
• where the Board decides not to accept the recommendations of the Committee with regard to the appointment of an auditor, a statement of the reasons
• where the auditor’s contract is terminated in disputed circumstances, the removal process and the underlying reasons for that action.
12.6 Members attendance at Committee meetings will be disclosed in the Trust’s Annual Report. Version 15 Agreed at Audit & Risk Committee Date: February 2017 Date of Next Review Date: February 2018
Page 7 of 7