aetiologies and epidemiology of subdural haematoma in infancy
TRANSCRIPT

ACTAUNIVERSITATIS
UPSALIENSISUPPSALA
2021
Digital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 1702
Aetiologies and Epidemiology ofSubdural Haematoma in Infancy
JACOB ANDERSSON
ISSN 1651-6206ISBN 978-91-513-1072-5urn:nbn:se:uu:diva-426036

Dissertation presented at Uppsala University to be publicly examined in Fåhraeussalen,Rudbecklaboratoriet, Dag Hammarskjölds väg 20, Uppsala, Friday, 15 January 2021 at 09:00for the degree of Doctor of Philosophy (Faculty of Medicine). The examination will beconducted in English. Faculty examiner: Professor Andreas Buettner (Universität Rostock).
AbstractAndersson, J. 2021. Aetiologies and Epidemiology of Subdural Haematoma in Infancy.Digital Comprehensive Summaries of Uppsala Dissertations from the Faculty of Medicine1702. 37 pp. Uppsala: Acta Universitatis Upsaliensis. ISBN 978-91-513-1072-5.
According to scientific studies, subdural haematoma (SDH) in combination with retinalhaemorrhage and encephalopathy (usually denoted as the triad) during infancy is highly specificfor abusive head trauma/shaken baby syndrome, if a fall from over one meter, a trafficaccident and certain medical conditions have been excluded. Other studies have challengedthis notion since there are witnessed falls from less than one meter which has caused acuteSDH, birth-related SDH which have been confirmed to develop into chronic SDH, and externalhydrocephalus that can be complicated by a spontaneous SDH or an SDH from minor trauma.
These aetiologies have not been taken into consideration in prior studies on abusive headtrauma.
An independent review on infant abusive shaking from the Swedish Agency for HealthTechnology Assessment concluded that there was insufficient evidence for determining thespecificity of the triad for isolated shaking.
The aim of this thesis was to increase the understanding of the aetiologies and theepidemiology of infant SDH. This was accomplished by studying registry data (Paper I and II),descriptive reviews of infants with SDH (paper I, III and IV) and infants subjected to witnessedor spontaneously admitted shaking (paper V).
The maximum incidence of fatal AHT in Sweden, 0.6/100 000, was at least 10 times lowerthan in other Western countries and the risk of unreported fatal AHT was low (Paper I). Amajority of the deceased infants had neonatal conditions, several were twins and/or preterm, onehad a cerebral vascular condition, and one signs of metabolic disorder (Paper I). Approximately12 infants every year are diagnosed with SDH beyond the first week of life and the case-fatalityrate for all SDH diagnosis categories is 6.2% (Paper II). Males, preterm born and twins havea higher risk to develop SDH in general, and those having an abuse diagnosis had increasedodds of being born preterm and small-for-gestational age (Paper II). Chronic SDH has a higherfreqency of male and premature infants and a lower mortality rate than acute SDH (Paper III).Infants with chronic CSDH, but not with acute SDH, tend to have findings on neuroimaging anda head circumference that are suggestive of external hydrocephalus complicated by spontaneousSDH or SDH from minor trauma (Paper IV). Intracranial and ocular findings in infants subjectedto abusive shaking were rare, seen in 2 out of 36 infants, both with pre-existing intracranialpathology, and of non-specific character (Paper V).
In conclusion this thesis provides evidence that non-abusive aetiologies for SDH in infancymay have been overlooked in previous research.
Keywords: Abusive Head Trauma, Shaken Baby Syndrome, Subdural Haematoma, Externalhydrocephalus
Jacob Andersson, Department of Surgical Sciences, Forensic Medicine, Dag Hammarskjöldsväg 20, Uppsala University, SE-75237 Uppsala, Sweden.
© Jacob Andersson 2021
ISSN 1651-6206ISBN 978-91-513-1072-5urn:nbn:se:uu:diva-426036 (http://urn.kb.se/resolve?urn=urn:nbn:se:uu:diva-426036)

Dedicated to my family


List of Papers
This thesis is based on the following papers, which are referred to in the text by their Roman numerals.
I Andersson J, Thiblin I. National study shows that abusive head
trauma mortality in Sweden was at least 10 times lower than in other Western countries. Acta Paediatrica 2018;107:477–83. doi:10.1111/apa.14138
II Högberg U, Andersson J, Squier W, et al. Epidemiology of sub-dural haemorrhage during infancy: A population-based register study. PLOS ONE 2018;13:e0206340. doi:10.1371/jour-nal.pone.0206340
III Andersson J, Wikström J, Högberg U, Wester K, Thiblin I. Dif-ferent vulnerability profiles in acute compared to chronic sub-dural haematoma amongst infants with suspected abusive head trauma. Submitted to Acta Radiologica.
IV Andersson J, Wikström J, Högberg U, Wester K, Thiblin I. Dif-ferences in head circumference and neuroimaging characteristics – what can they tell about the aetiologies of infant subdural hae-matoma? Manuscript (preprint).
V Thiblin I, Andersson J, Wester K, et al. Medical findings and symptoms in infants exposed to witnessed or admitted abusive shaking: A nationwide registry study. PLOS ONE 2020;15:e0240182. doi:10.1371/journal.pone.0240182
Reprints were made with permission from the respective publishers.


Contents
Introduction ................................................................................................... 11 The SBU-report ........................................................................................ 14 The association of classical metaphyseal lesions and rib fractures to SDH .......................................................................................................... 15 The pit-falls of a definitive theory ............................................................ 16 The base-line for infants to develop spontaneous or accidental SDH is not known ................................................................................................. 17 The nomenclature of infant abuse ............................................................ 18 Meta-reviews and case reports in the abusive head trauma-literature ...... 19
Aim of thesis ................................................................................................. 20 Aim of each paper ..................................................................................... 20
Material and Methods .................................................................................... 22 Study design and participants ................................................................... 22
Paper I .................................................................................................. 22 Paper II ................................................................................................. 22 Paper III ............................................................................................... 23 Paper IV ............................................................................................... 23 Paper V ................................................................................................. 23
Statistical analyses and software .............................................................. 24 Paper I .................................................................................................. 24 Paper II ................................................................................................. 24 Paper III ............................................................................................... 24 Paper IV ............................................................................................... 24 Paper V ................................................................................................. 25
Results ........................................................................................................... 26 Paper I ....................................................................................................... 26 Paper II ..................................................................................................... 26 Paper III .................................................................................................... 26 Paper IV .................................................................................................... 26 Paper V ..................................................................................................... 27
Discussion ..................................................................................................... 28 Methodological considerations ................................................................. 30

Future perspectives ........................................................................................ 31 Medico-legal implications ........................................................................ 31 Research implications ............................................................................... 31
Acknowledgements ....................................................................................... 33
References ..................................................................................................... 34

Abbreviations
AHT Abusive head trauma ASDH Acute subdural haematoma CSDH Chronic subdural haematoma CCW Cranio-cortical width CML Classical metaphyseal lesion HC Head circumference IHW Interhemispheric width RH Retinal haemorrhage SDH Subdural haematoma SCW Sino-cortical width SSW Subarachnoid space width


11
Introduction
The aetiology of subdural haematoma (SDH) in infants has been widely de-bated from the late 19th century and forward. Sherwood reviewed the history of chronic SDH stating that it is suspected in an infant with enlargement of the head and convulsions. Haemorrhages in the eyegrounds, if present, furnish additional evidence to help confirm the diagnosis: ”Chronic subdural haema-toma occurs most frequently in infants during the first year and in adults past middle life. A serosanguinous xantochromic encapsulated fluid is found under the dura, which condition in infants often causes enlargement of the head, vomiting, irritability, haemorrhages in the eyegrounds, downward displace-ment of the eyes and symptoms of the central nervous system, the most prom-inent being convulsions”. Sherwood discussed a wide variety of aetiologies for SDH in infants ranging from birth trauma to syphilis, scurvy, colds, prior trauma and described an incidence ranging from 2-14 percent in autopsied infants. Many authors also found an association to rickets in infants presenting with chronic SDH. Sherwood’s own conclusion was that “the aetiology re-mains obscure” and “no one factor has been found to account for every case”
[1]. Ingraham and Matson stated that the increasing incidence of SDH during in-fancy which they encountered was not a true increase, rather that “the fre-quency with which SDH is found in infancy is proportional the intensity with which it is sought” [2]. Furthermore, they stressed the challenge in diagnosis considering that many infants had other concurrent diseases including low cal-cium tetany, infections and malnutrition. They considered that the most com-mon cause of SDH in infancy was the result of birth trauma. The hypothesis that shaking can lead to SDH, retinal haemorrhages (RH) and encephalopathy, usually denoted as the triad, was first put forward by the neu-rosurgeon Norman Guthkelch in 1971 [3]. He had noticed that some infants which presented with SDH did not have external signs of injury, and proposed that shaking was a possible mechanism which could explain the findings in absence of external injury. Guthkelch referred to an experiment by the neuro-surgeon Ayoub Ommaya in which 50 rhesus monkeys had been subjected to a single whiplash injury by securing them in a sled and delivering a blow of

12
force to the rear of the sled with a piston. There were 19 monkeys which con-tracted concussion and of these 15 had visual evidence of surface haemor-rhages which were primarily subdural and 11 had neck injuries. None of the non-concussed monkeys had macroscopic evidence of brain injury [4]. In 1974 Caffey coined the term Whiplash Shaken Infant Syndrome in an article where he cited Guthkelch and Ommaya and referred to a newspaper-story of an infant nurse who had confessed to shaking infants. Caffey stated that “Cur-rent evidence, though manifestly incomplete and largely circumstantial, war-rants a nationwide educational campaign on the potential pathogenicity of ha-bitual, casual whiplash shaking of infants” [5]. After Caffeys article, several studies were published in which the definition of abuse versus control was not clearly stated.
When the notion that the triad is pathognomonic for shaking arose is not clear, but RH was mentioned to be pathognomonic for abuse by Eisenbrey in 1979
[6]. When reading the early literature on shaken baby syndrome, they usually con-sist of small case-series and lack a proper definition of how the conclusion of shaking was drawn [7]. In 1984, Ludwig investigated 20 infants, 14 boys and six girls which had met their criteria for shaking (not further stated) [8], none of the care-givers had admitted to shaking but three stated that they shook the infants in an effort to perform resuscitation and recent accidental injury was mentioned in eight cases. However, Ludwig states that “diagnosis depends on a high index of suspicion and the physical findings of a bulging fontanelle, head circumference greater than the 90th percentile and retinal haemorrhage”. In Sweden the Stockholm regional guidelines for infant abuse states that “The combination of subdural haematoma and brain injuries with oedema or bleed-ings strongly suggests abuse if a history of a traffic accident or a fall from high altitude is missing. If there are also retinal haemorrhages then the diagnosis of abuse is from a medical point of view complete” [9]. The first article to question the theory of shaken baby syndrome was a clinical, pathological and biomechanical study by Duhaime et al. They investigated fatal cases of the shaken baby syndrome and found that all infants had signs of impact. Further, they performed a biomechanical comparison of the forces from shaking and impact. Whilst impact reached the angular acceleration and angular velocity required to cause diffuse axonal injury and subdural haema-toma in a majority of the cases, shaking alone never came close to the required forces [10].

13
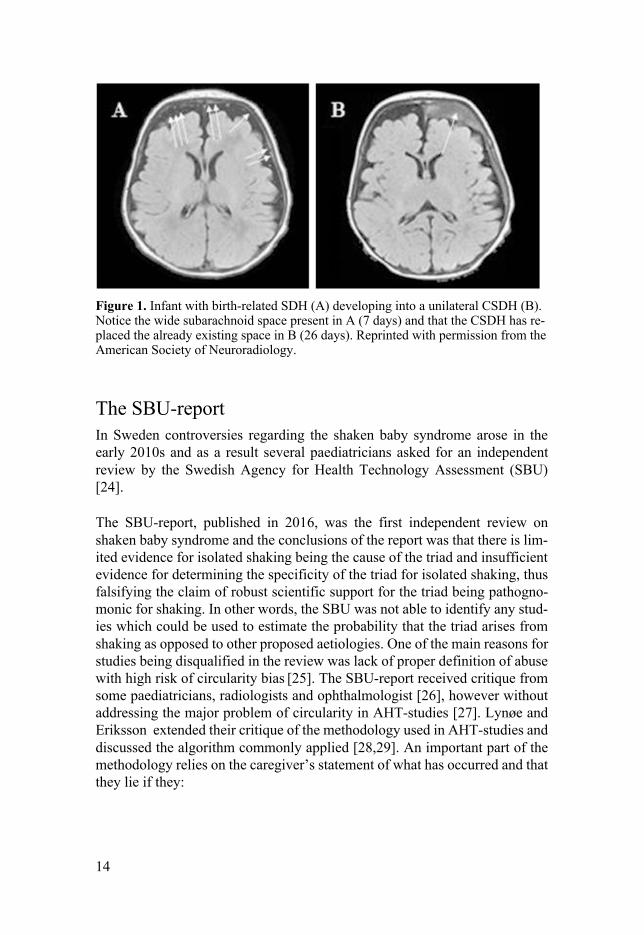
The critique of the shaken baby syndrome sparked again in 1997 when Louise Woodward, a 19-year old au-pair was accused and convicted of shaking an infant to death [11,12]. Ayoub Ommaya, neurosurgeon and the conductor of the experiment on rhesus monkeys, served as one of the expert witnesses on behalf of the defence. Ommaya wrote an article a few years later stating that his findings in the 1967 article on SDH in rhesus monkeys had been misinter-preted by Guthkelch and Caffey, considering that the injuries the monkeys sustained were comparable to a single impact load and not to shaking. He also discussed the potential for short falls leading to SDH [13]. Patrick Barnes, a neuro-radiologist, witnessed on behalf of the prosecution in the Woodward trial, stating that the infant had been shaken. He later came to change his opinion in the matter and published an article regarding imaging of non-accidental trauma and its mimics and discussed the lack of proper evi-dence for the triad [14]. In the early 2000s, Geddes performed neuropathological studies on infants which were supposed to have been shaken. Prior, the injuries seen in these infants were believed to be the result of diffuse traumatic axonal injury, but when Geddes investigated the infants with suspected AHT she found trau-matic injuries solely in the infants which had external signs of trauma, the infants which lacked external signs of trauma had hypoxic-ischemic injuries. The injuries were similar to those seen in infants which had suffered from intrauterine hypoxia with the proposed mechanism being global hypoxia, cer-ebral oedema and increased intracranial pressure leading to venous and capil-lary blood leakage [15–17]. A similar hypothesis related to brief resolved un-explained event, commonly referred to as BRUE, has recently been proposed to be related to the findings usually associated to shaking [18]. Further critique arose considering that birth-related SDH appear in up to 45 % of asymptomatic infants [19]. One infant had a re-bleed seen at 26 days of age (Figure 1), but the authors concluded that SDH in asymptomatic term neonates after delivery is limited in size and location. However, as Gabaeff pointed out, 1/101 infants had a bleeding which is usually attributed to abuse and when applying that frequency on the 2 000 000 births that occur every year in the United States, the possibility of a re-bleed from a birth-related SDH needs to be taken into consideration [20]. Several studies have also confirmed that relatively short falls can cause the triad [21–23]
14
Figure 1. Infant with birth-related SDH (A) developing into a unilateral CSDH (B). Notice the wide subarachnoid space present in A (7 days) and that the CSDH has re-placed the already existing space in B (26 days). Reprinted with permission from the American Society of Neuroradiology.
The SBU-report In Sweden controversies regarding the shaken baby syndrome arose in the early 2010s and as a result several paediatricians asked for an independent review by the Swedish Agency for Health Technology Assessment (SBU) [24]. The SBU-report, published in 2016, was the first independent review on shaken baby syndrome and the conclusions of the report was that there is lim-ited evidence for isolated shaking being the cause of the triad and insufficient evidence for determining the specificity of the triad for isolated shaking, thus falsifying the claim of robust scientific support for the triad being pathogno-monic for shaking. In other words, the SBU was not able to identify any stud-ies which could be used to estimate the probability that the triad arises from shaking as opposed to other proposed aetiologies. One of the main reasons for studies being disqualified in the review was lack of proper definition of abuse with high risk of circularity bias [25]. The SBU-report received critique from some paediatricians, radiologists and ophthalmologist [26], however without addressing the major problem of circularity in AHT-studies [27]. Lynøe and Eriksson extended their critique of the methodology used in AHT-studies and discussed the algorithm commonly applied [28,29]. An important part of the methodology relies on the caregiver’s statement of what has occurred and that they lie if they:

15
• Describe a history of trauma which is not accepted by the multidiscipli-nary team (usually falls < 1 meter)
• Don’t present a history of trauma • Describes a lucid interval between a trauma and the presentation of en-
cephalopathy • Changes the story • Admits to shaking after a collapse
And that they tell the truth if they: • Admits to abusing the infant • Presents a history of a fall > 1 meter Using this reasoning the parents are only considered to tell the truth if they admit to abusing the infant, which in turn is dependent on several auxiliary or ad hoc hypotheses as further discussed by Lynøe et al. [30].
The association of classical metaphyseal lesions and rib fractures to SDH Long before Caffey assumed that the triad was a result of shaking, he had noticed an association between SDH and classical metaphyseal lesions (CML) in infants without external signs of trauma which he called “metaphyseal fra-gility” [31]. In 1957, Weston and Hutt studied three infants with CML which they suggested to be the result of obstetric trauma in two cases and direct trauma in one case[32]. Astley described it as a generalised bone disease with-out history of trauma and little disturbance or pain and that the lesions are only discovered on X-ray [33]. Silverman assumed that these lesions were the re-sult of battering [34]. Little was then written regarding occult rib fractures and CML being the result of abuse until 1962 when Kempe coined the term “the battered child syndrome”, which he claimed should be suspected in any infant “exhibiting evidence of fracture of any bone, subdural haematoma, failure to thrive, soft tissue swelling or skin bruising, any child which dies suddenly, or where the degree and type of injury is at variance with the history given re-garding the occurrence of the trauma” [35]. During the 1980s and early 90s, Kleinman published several studies in which he ascribed rib fractures and CMLs to shaking and he considered the only accepted differential diagnosis to be osteogenesis imperfecta [36–38], which earlier had been mistaken to be caused by abuse [39].

16
The conclusions by Kleinman were challenged by Paterson and Monk who argued that the rib fractures and CML are the result of a temporary condition in infancy they denoted “temporary brittle bone disease” [40]. Holick et al. suggested that hypermobility disease in combination with vitamin-D defi-ciency is a cause of rib fractures and CML in infants after finding evidence that the parents of infants with multiple occult fractures to a larger extent were suffering from different forms of hypermobility [41]. Högberg et al. found that metabolic bone disease was the major cause of fractures during early infancy [42]. The reasons for the association between SDH and occult fractures in infants without a history of trauma has not been systematically studied. Possible ex-planations are non-reported trauma or non-traumatic conditions predisposing for both SDH and certain kinds of fractures.
The pit-falls of a definitive theory Shaken baby syndrome is by many doctors viewed as a definitive theory. Na-rang et al. made an interview study which showed that 88% of the respondents agreed with the statement that SDH, RH and coma or death are caused by shaking and that besides a motor vehicle collision, no alternative theories of causation are generally accepted [43]. The conclusions which have been drawn regarding shaken baby syndrome are a consequence of the prior notion that only shaking can cause these injuries [30]. In other words, a connection between shaking and the triad has been assumed, developed into a theory and when that theory is being taught in uni-versities and used by multidisciplinary teams, other findings will start to be-come associated with the triad, henceforth by proxy to shaking. However, for these associations to be viewed as cause and effect, the main assumption needs to be correct. If the main assumption is incorrect - in this case simply meaning that there are other aetiologies for the triad - circularity bias is enhanced. An important part of the pathophysiological explanation of the findings and symptoms associated to shaken baby syndrome is that they are independent of each other. In other words, the SDH is a result of ruptured veins, the RH of vitreo-retinal traction and the encephalopathy (e.g. apnoea, seizures, vomiting, reduced consciousness) of traumatic brain injury with diffuse axonal damage. Examples of assumptions which are the result of the main assumption are:

17
• That falls less than 0.9-1.2 meters do not cause the triad [44]. If a care-giver would provide a history of a fall of less than 1.2 meters then this would be viewed as inconsistent with the injuries. Thus this “false history” will be seen as further evidence that the triad in fact was a result of abuse, and when implemented as a criterion in future study designs result in en-hanced circularity bias.
• The claim that the time when the head circumference started to increase in an infant with SDH, is a key sign in dating a supposed shaking [45], thereby ignoring that the increased head circumference could be the result of external hydrocephalus and the SDH could have arisen spontaneously [46–49]. External hydrocephalus usually presents with increased head circumference, bulging fontanelle and downward displacement of the eyes [50]. When recalling the advice on when to suspect chronic SDH in infants by Sherwood [1] and the characteristics of infants deemed to have been shaken by Ludwig [8] it becomes clear that the presentation could represent external hydrocephalus complicated by an SDH.
• The presence of a mixed SDH, which is frequently encountered in cases of suspected shaking, has been viewed as proof of shaking at several oc-casions and an isolated chronic SDH as the result of a prior shaking epi-sode [51]. Taking in regard another assumption which states that the symptoms always occur immediately after the shaking episode [52], it does not follow logically that a chronic SDH would be the result of shak-ing since the chronic SDH is discovered when the infant has symptoms and is taken to the hospital. If the symptoms were a result of direct shear-ing brain injury from shaking, logically they would arise in close proxim-ity to the shaking and not days or weeks after.
The base-line for infants to develop spontaneous or accidental SDH is not known As a result of the SBU-report, the assumed gold standard for defining abuse versus accident (the triad) is no longer valid and the base-line for accidental or spontaneous SDH in infants is to this date not known. This baseline is re-quired when estimating the positive predictive value (true positive cases / true positive cases + false positive cases). The risks of not acknowledging the positive predictive value of findings which appear in child abuse were discussed as early as in 1978 [53]. Daniel et al warned that in the case of low prevalence the risk of misclassification is very high even with good sensitivity and specificity.

18
“If one assumes a one percent prevalence, as did Light, and a 90% Sensitivity and 95% Specificity, this would lead to an 85% frequency of false positives among all test positives. Unless the negative implications of such labelling can be totally removed we doubt that society will tolerate this kind of cost… The low prevalence of child abuse combined even with the most optimistic esti-mates of screening effectiveness implies that any child abuse program will yield large numbers of false positives – non-abusing families labelled as abus-ing or potentially abusing” [53]. Considering that neither the incidences of abuse, accidental SDH or spontane-ous SDH are known, there is a high risk of false positive cases, especially since all other causes for SDH needs to be compared to SDH which unequiv-ocally can be attributed to abuse.
The nomenclature of infant abuse There have been many denotations for suspected abuse of infants which pre-sent with a SDH: non-accidental head injury; the whiplash shaken infant syn-drome; shaken baby syndrome and the most recent; abusive head trauma
[5,8,54,55]. As discussed by Fleming and Byard in an editorial to Acta Paedi-atrica, all of them contain a description of intent [56]. They proposed that the name should be changed to blunt cranio-cerebral trauma, since it does not im-ply intent. However, this general term would not further the understanding of SDH in infancy considering there are non-traumatic and birth-related causes of SDH. Even though asthma and chronic obstructive pulmonary disease can have a similar presentation, we do not use a general term for them because they are separate entities with different causes, outcomes and treatments. In other words, when studying SDH in infancy, it is important to separate a case with acute SDH, shear injury, skull fracture and external injuries from a case with chronic SDH and no signs of trauma, as discussed in a response to Fleming and Byard [57]. Norman Guthkelch argued that his hypothesis of shaking lead-ing to the triad had been taken out of proportion and criticised the development of the concept, suggesting that the descriptive “retino-dural haemorrhage of infancy” would be more appropriate [58]

19
Meta-reviews and case reports in the abusive head trauma-literature Some meta-reviews have claimed to support the assumption that the triad or its components with or without other signs of trauma are specific for AHT [59,60]. Even if the results of a review are impressive, they will always be limited by the quality of the original studies. If the original studies do not con-tain a proper method for defining abuse versus control cases, the results of the review are invalid. Considering that AHT has been viewed as a definitive theory, a single case report is enough to disprove a statement proposing that except for shaking; a motor vehicle collision or multi-story fall are the only accepted alternative causes of the findings behind the AHT diagnosis [43]. In other words, one corroborated short fall leading to the triad [21–23] is enough evidence to dis-prove the statement that short falls never cause the triad. All studies which have concluded that falls lower than 0.9 meters cannot give rise to the triad becomes falsified, considering that this was a criterion to determine abuse ver-sus accident and where a caregiver presenting a history of a short fall has been considered to be lying.

20
Aim of thesis
As a result of the methodological flaws, circular reasoning in particular, in prior studies on AHT, there is a lack of population-based studies which inves-tigates in what frequency natural causes or accidents could have caused the triad or other findings such as rib fractures or classical metaphyseal fractures, which are sometimes associated to AHT. Because of the above discussed the-ory that the triad and rib fractures are highly specific or even pathognomonic for AHT, large scale studies with the aim of investigating the incidence of e.g. external hydrocephalus as a cause of spontaneous SDH are lacking. Usually the knowledge of these findings being the result of natural causes or accidents are based on small studies or case reports and are regularly viewed as anoma-lies. Considering the rarity of these findings in general, all other causes, no matter how unusual they are, need to be estimated, to be able to establish a base-line for SDH which cannot be attributed to abuse. Subsequently, the out-comes can be compared to those of definite abuse. There is a need for further investigation on a larger population to investigate the nature of SDH in infants.
Aim of each paper Paper I: To investigate the accuracy of the Swedish death records with regard to abusive head trauma. Paper II: To analyse subdural haemorrhage (SDH) during infancy in Sweden by incidence, SDH category, diagnostic distribution, age, co-morbidity, mor-tality, and maternal and perinatal risk factors; and its association with acci-dents and diagnosis of abuse. Paper III: To investigate the type of subdural effusion in infants referred to medico-legal investigation due to suspected abusive head trauma and compare risk factors in infants with acute and chronic SDH. Paper IV: To investigate to what extent external hydrocephalus may lay be-hind findings and symptoms interpreted as signs of abusive head trauma. Paper V: To investigate the hypothesis that shaking causes SDH, RH, en-cephalopathy, rib fractures, or CMLs, using a definition of physical abuse by

21
shaking that is independent of medical findings. Symptoms and medical find-ings in infants subjected to admitted or witnessed shaking with or without blunt force impact were evaluated to address this question.

22
Material and Methods
Study design and participants Paper I The study had a retrospective register-based design in three parts. • All death certificates from infants (aged 0-1 years) autopsied at the Na-
tional Board of Forensic Medicine in Sweden between 1994-2014 (n=733) were reviewed regarding SDH.
• All infants with diagnoses of sudden infant death or unknown cause of death (R95, R96.1, R98, 798A and 798X from the ICD-9) were scruti-nized to exclude a missed diagnosis of SDH.
• Infants which died between 2006-2013 with undetermined cause of death (R99 from the ICD-10), which had not been subjected to medico-legal investigation were retrieved from the National Board of Health and Wel-fare were investigated with regard to place of death, age of the infant and why the board had coded the case as undetermined.
Paper II The study had a population-based register design including all infants (aged 0-1 years) born between 1997-2014 (1 855 267) diagnosed with SDH accord-ing to the ICD-10. Four referents without diagnosis in the in-patient registry were selected for statistical comparison. Outcome measures were
• Incidence and distribution • Co-morbidity • Fall accidents by SDH-category • Risk factors for SDH during the first week of life • Risk factors for SDH for infants older than one week • Risk factors for infants with the diagnosis traumatic SDH, acute non-trau-
matic and SDH with abuse diagnosis.

23
Paper III This study was a descriptive review of a national series of infants (age 0-1 years) with an SDH or a hygroma with available neuroimaging at the time of diagnosis, that had not been a complication to a traffic accident, a multi-story fall, or similar high energy trauma, and that have been recorded in the com-puterised register of the Swedish National Board of Forensic Medicine be-tween January 1994 and December 2018. A total of 85 cases comprise the study population which were analysed with regard to type of SDH, age at di-agnosis, sex, prematurity, multiple birth and death. Infants with a subdural fluid which was uniformly hyperattenuating compared to adjacent cortex were defined as having acute SDH, whilst infants with an iso/hypodensity and mixed density fluid were defined as having chronic SDH.
Paper IV The 85 infants identified in Paper III, 69 with chronic SDH and 16 with acute SDH, were reviewed with regard to available clinical head circumference measurements (HC), HC measured on CT at the time of diagnosis and radio-logical characteristics of external hydrocephalus, such as cranio-cortical width (CCW), sino-cortical width (SCW), frontal interhemispheric width (IHW) and subarachnoid space width (SSW). The correlation between the contralateral SSW and the ipsilateral CCW and SDH width was investigated in infants with unilateral SDH located at the foramen of Monro (n=10). Two definitions were used since there is no consensus regarding what radio-logical criteria to use t diagnose external hydrocephalus. One according to Lam et al. which found that these measurements were age dependent and sug-gested that infants with measurements over the 95th percentile should be re-garded as suffering from external hydrocephalus [61]. The other definition was according to Hussein et al. who did not find an association to age and instead suggested that infants with all measurements > 5 mm in combination with clinical signs of external hydrocephalus should be used [62].
Paper V This study was a case series of 239 infants which received a maltreatment diagnosis according to ICD-10 during 1997-2014. Medical records were re-trieved from respective hospital. Witnessed shaking was defined as directly observed or filmed. Admitted shaking was defined as a spontaneously deliv-ered history of shaking. The outcomes were frequency of findings on neuroim-aging, fundoscopy, whole-body x-ray, clinical examination and registered symptoms.

24
Statistical analyses and software Paper I Incidence was calculated as cases per 100 000.
Paper II Incidence was calculated as cases per 100 000. Age distributions and fall-ac-cidents were visualized using the ggplot2 package in R. The IBM software SPSS was used for statistical analysis. Fisher´s exact test or Mantel-Haenszel Chi-square were used for non-parametric variables and analysis of variance. Maternal and perinatal outcomes were described with crude and adjusted odds ratios.
Paper III All analyses and visualizations were carried out in R using the tidyverse and rstatix packages. Age distributions were visualized with plots using the tidyverse package in R. Fisher´s exact test was used to calculate difference between groups. The proportional test was used to assess the gender distribution with an ex-pected male-to-female ratio of 0.5.
Paper IV All analyses and visualizations were carried out in R using the tidyverse, rstatix and ggpubr packages. The proportion of infants with CSDH and ASDH with normal or increased head circumference were compared with Fisher´s exact test. International HC charts with standard deviations were imported into R and the HC at the time of diagnosis was plotted. CCW, SCW, IHW and SSW were compared using Wilcoxon’s signed ranked test due to non-normal distribution of the data. The correlation between the contralateral SSW and the ipsilateral CCW and SDH width was calculated with Spearman rank order correlation due to non-linearity and non-normal distribution of the data. The calculations for normal values found in Lam et al were used to construct a plot in which the CCW, SCW and IHW values were inserted. Infants with CCW, SCW or IHW > 95th percentile were compared to infants with these measure-ments < 95th percentile with regard to type of SDH with Fisher´s exact test. Infants with CCW, SCW and IHW > 5 mm and increased HC were compared with regard to type of SDH with Fisher´s exact test.

25
Paper V Plots were created using the tidyverse package in R. The Z-statistic in the MedCalc software was used for comparison of the observed sex disproportion with an assumed null hypothesis of 50%.

26
Results
Paper I The maximum incidence of lethal AHT, 0.6/100 000 infants, was at least 10 times lower than in other Western countries. There was a low risk of unre-ported lethal AHT. Eight of the 12 cases had concomitant disease or perinatal illness, five were born prematurely and three were twins.
Paper II The incidence of SDH was 16.5 / 100 000 infants. The case-fatality rate was 6.2 %. Twenty-four percent of the cases occurred during the first week of life, mean and median ages for all SDH were 3.3 and 2.5 months respectively. Male sex was overrepresented in all SDH-categories. One third of all infants had a reported fall accident. Infants older than one week with the diagnosis acute non-traumatic SDH had an association to prematurity, multiple birth and small for gestational age. Infants with SDH and abuse diagnosis (14%), had in-creased odds for being preterm and small for gestational age.
Paper III A majority of the infants had CSDH (79%). Infants with CSDH had signifi-cantly higher prematurity rate (p<0.05) and a significantly lower mortality rate (p<0.001). The proportion of males compared to an expected frequency of 0.5 was significantly higher in infants with CSDH (p < 0.01) but not in infants with ASDH (p = 0.8). The peak incidence for infants with CSDH occurred during the third month of life and for infants with ASDH during the first month of life.
Paper IV Infants with CSDH had significantly higher CCW, SCW, IHW and SSW than infants with ASDH (p < 0.05). The ipsilateral CCW (R = 0.92, p < 0.001) and

27
SDH width (R = 0.8, p < 0.01) was correlated to the contralateral SSW. In-creased HC was more prevalent in Infants with CSDH (71%) than in infants with ASDH (14%) (p < 0.01). Fifty-three infants had clinically recorded HC, 42, all with CSDH, had at least one measurement ≥ 95th percentile. Twenty infants, all with CSDH, had CCW, SCW and IHW > 5 mm and increased HC.
Paper V In total 36 infants had been shaken, six of these also had information indicat-ing blunt impact immediately after shaking. Two infants, one subjected to iso-lated shaking and one to both shaking and impact, both with pre-existing vul-nerability, had possible acute intracranial injury. The infant subjected to iso-lated shaking was three weeks old and had an acute subarachnoid haemor-rhage and a bilateral CSDH or hygroma. The infant subject to both shaking and blunt impact was born preterm and had non-specific frontal cortical changes, a hyperdense SDH, hyperdense subarachnoid haemorrhage, RH and suspected cortical vein thrombosis. No infants had clinical or radiological signs of extracranial fractures.

28
Discussion
The aim of this thesis was to investigate the aetiologies and epidemiology of SDH during infancy. The main result was that external hydrocephalus complicated by a spontane-ous SDH or SDH following minor trauma could be an underestimated aetiol-ogy of SDH in infants. This was shown by finding a male preponderance (Pa-per II and III), different risk factors and age distributions (Paper III), number of infants with increased HC and significantly higher measurements of CCW, SCW, IHW and SSW for infants with CSDH compared to infants with ASDH (Paper IV). These findings were not observed in infants exposed to confirmed shaking (Paper V). The correlation between the SSW on the contralateral side of the SDH to the CCW and SDH on the ipsilateral side of the SDH also indi-cates that an SDH could replace an already existing widened subarachnoid space (Paper IV) (Figure 1 and 2).
Figure 2. Infant with unilateral CSDH (A) and infant with bilateral CSDH (B). No-tice the wide subarachnoid space on the contralateral side of the CSDH in the infant with unilateral SDH and that there still is a subarachnoid space in the infant with bi-lateral CSDH. See also the similarities between the infant with unilateral SDH (A) to the infant in Figure 1 with birth-related CSDH and wide subarachnoid spaces.

29
Findings associated with AHT in infants subjected to witnessed or admitted isolated shaking (Paper V) were rare and of non-specific nature, making the presence or non-presence of medical findings of limited value for identifying or rule out abusive shaking. This is the first study which uses witnessed or spontaneously confessed AHT as inclusion criteria and does not rely on diag-nosis by a multidisciplinary team, i.e. diagnosis based on interpretation of findings. One of the 30 infants with isolated shaking had the combination of a chronic subdural haemorrhage and an acute subarachnoid haemorrhage. This finding indicate that meningeal haemorrhage can be caused by isolated shak-ing in infants with pre-existing intracranial pathology. There were however no infants in the study with isolated shaking which had ASDH. Fall accidents were reported in a third of all infants diagnosed with an SDH in paper II and the most common type of fall was fall being carried. The study design did however not make it possible to ascertain whether the clinical find-ings were in accordance to the reported history of a fall. The incidence for SDH during infancy in Sweden has been established via an extensive registry study (Paper II) and have shown that approximately 16 in-fants per year develops SDH with a case-fatality rate of 6.2 %. Furthermore, the incidence of fatal AHT with SDH (0.6 / 100 000) in Sweden is at least 10 times lower than in other western countries and the risk for unreported lethal AHT is low (Paper I). Six infants in paper I had chronic or mixed density SDH, eight had some comorbidity and three were twins which raises the question if some of the infants died from natural causes.
The registry data in Paper II showed that male infants are at higher risk to develop SDH, and male sex and small-for gestational age had increased odds for an abuse diagnosis. A limit was that the ICD-10 does not differentiate be-tween acute or chronic SDH. This was addressed in Paper III which showed that 79% of the infants referred to forensic medicine with suspected AHT had CSDH. In conclusion, the results of this thesis show that • Fatal AHT is rare in Sweden compared to other Western countries
• Infantile SDH is rare in Sweden with approximately 12 infants every year
being diagnosed after the first week of life
• Male sex, prematurity and multiple birth are risk factors for developing SDH.

30
• Infants diagnosed with AHT share some risk profile factors with those related to CSDH.
• Infants with ASDH and CSDH have different risk profiles.
• External hydrocephalus complicated by spontaneous SDH or SDH after minor trauma, birth-related CSDH in infants with wide subarachnoid spaces may have been overlooked and misdiagnosed as AHT.
• Isolated abusive shaking is unlikely to cause SDH, RH or fractures in healthy infants
Taken together, the results of this thesis indicate that there are two major infant populations diagnosed with SDH when excluding birth-related injuries found in connection to delivery. One population is characterized by ASDH related to blunt force head trauma, with an expected even sex distribution. The other is characterized by chronic SDH or mixed density SDH, an overrepresentation of male sex, and certain vulnerability factors such as preterm birth, small-for-gestational age and findings indicative for external hydrocephalus. AHT was suspected in both groups, hence the referral to forensic medicine, making it possible that there were other explanations for the SDH than abuse in both groups, i.e. false positives either due to a fall accident or non-traumatic con-ditions. The rarity of medical findings in infants subjected to witnessed or ad-mitted abusive shaking with or without blunt force trauma shows that the non-presence of SDH and other findings such as fractures or bruises does not rule out AHT, i.e. that SDH has a low sensitivity for AHT. If SDH is considered to have a high sensitivity for AHT, there is a risk for false negatives.
Methodological considerations The retrospective design of these studies makes them dependent on the infor-mation which had been registered, with missing data as a consequence. Swe-dish registries tend to be of high quality, but are not validated for child abuse. Paper II includes 1 855 265 infants, extends over several years and has a large reference group which provides strength regarding comparisons and comor-bidity. It does however lack details which are important when studying aeti-ology. Study III and IV was an attempt to complement this lack of detail. There is no consensus on how to diagnose external hydrocephalus on neu-roimaging which provides some limitation to Paper IV. It is complicated to study a criminal act. However, Paper V is unique compared to other studies on AHT since it has proven that it is possible to study the outcome after known, as opposed to supposed, exposure to shaking.

31
Future perspectives
Medico-legal implications ASDH and CSDH are different entities and need to be evaluated accordingly. The current guide-lines for investigating ASDH are acceptable, however it is important to take in the evidence that short falls can cause ASDH and to per-form an MR to rule out central venous thrombosis and vascular malfor-mations. The guidelines for investigating the aetiology of CSDH, on the other hand, needs to be updated with a risk factor analysis related to pregnancy and neo-natal period and with a neuroradiological and clinical investigating with atten-tion to external hydrocephalus or birth-related SDH developing into CSDH. The majority of the infants in study V did not have any clinical findings or symptoms, despite witnessed or confessed abuse by shaking and/or impact. Consequently, the absence of SDH, RH or fractures in an infant does not rule out abuse, and should not lead to termination of an investigation by the social services if there are other circumstances indicating abuse.
Research implications To increase the understanding of infant SDH it is important that future studies separate ASDH and CSDH since they are likely, at least to some extent, to have different risk factors, outcomes and aetiologies. Controlled studies with well-defined cases and controls allowing for calculat-ing the diagnostic accuracy of medical findings have not been performed. The results of the present thesis (Paper V) indicate that such studies are possible to perform. This thesis has not investigated the hypotheses related to immaturity and hy-poxia. Future studies on this issue are of importance.

32
Studies aimed at investigating whether the findings and symptoms constitut-ing the triad are independent of each other or if the encephalopathy and RH as secondary to the intracranial pathology are needed. The subpopulation of infants with both SDH and fractures needs further char-acterization. Intracranial pathology and extra-cranial fractures are obviously independent of each other and are sometimes clearly the result of trauma. To what extent, if any, these findings have non-traumatic cause is a key question in the medico-legal setting. Considering the infrequent occurrence of medical findings in infants subjected witnessed abusive shaking or spontaneously confessed abusive shaking, fur-ther studies on parental risk factors for AHT is an area of interest. Such studies may facilitate the detection of parents at risk and thereby contribute to estab-lishing preventive measures aimed at reducing child abuse.

33
Acknowledgements
Several people contributed significantly to my research, not only to the con-tent but also by making my doctoral studies joyful. I have gained new friends and experiences for which I am forever thankful. Ingemar Thiblin for making this project possible, teaching me scientific theory and for always being supportive, helpful and available for large as well as small problems. Knut Wester for his many visits to Uppsala and Stockholm to help me with neuroimaging, English, thoroughness and contributing significantly in my process of formulating research questions related to external hydrocephalus. Ulf Högberg who has always in a humble and most professional way given substantial comments to my manuscripts and for his knowledge in Epidemi-ology. Johan Wikström for his neuroradiological expertise and making study III and IV possible. Jonas Wallinder for introducing me to the programming language R which has increased my understanding of data management and statistics. Camilla Lundblad for assistance with retrieving neuroimaging and medical journals. Fredrik Tamsen, Tommie Olofsson, Anna Ybo, Håkan Sandler and Göran Högberg for providing a supportive and intellectual environment. My family and my fiancé Reem Emad.

34
References
1 Sherwood D. CHRONIC SUBDURAL HEMATOMA IN INFANTS. Am J Dis Child 1930;39:980–1021. doi:10.1001/archpedi.1930.01930170065007
2 Ingraham FD, Matson DD. Subdural hematoma in infancy. J Pediatr 1944;24:1–37.
3 Guthkelch AN. Infantile Subdural Haematoma and its Relationship to Whiplash Injuries. Br Med J 1971;2:430–1. doi:10.1136/bmj.2.5759.430
4 Ommaya AK, Faas F, Yarnell P. Whiplash Injury and Brain Damage: An Exper-imental Study. JAMA 1968;204:285–9. doi:10.1001/jama.1968.03140170001001
5 Caffey J. The Whiplash Shaken Infant Syndrome: Manual Shaking by the Ex-tremities With Whiplash-Induced Intracranial and Intraocular Bleedings, Linked With Residual Permanent Brain Damage and Mental Retardation. Pediatrics 1974;54:396–403.
6 Eisenbrey AB. Retinal Hemorrhage in the Battered Child. Pediatr Neurosurg 1979;5:40–4. doi:10.1159/000119800
7 Ellison PH, Tsai FY, Largent JA. Computed Tomography in Child Abuse and Cerebral Contusion. Pediatrics 1978;62:151–4.
8 Ludwig S, Warman M. Shaken baby syndrome: A review of 20 cases. Ann Emerg Med 1984;13:104–7. doi:10.1016/S0196-0644(84)80571-5
9 Flodmark O. Stockholm läns landsting regional vårdprogram: Vid misstanke om fysisk misshandel av späda barn (in Swedish): Stockholm County Regional Guidelines: When suspecting physical abuse of newborn babies. 2008.Available at: http://www.viss.nu/Global/Bilagor/RV_Misstanke_om_barnmisshan-del_del%20I.pdf
10 Duhaime AC, Gennarelli TA, Thibault LE, et al. The shaken baby syndrome. A clinical, pathological, and biomechanical study. J Neurosurg 1987;66:409–15. doi:10.3171/jns.1987.66.3.0409
11 Haberman C. Shaken Baby Syndrome: A Diagnosis That Divides the Medical World. N. Y. Times. 2017.https://www.nytimes.com/2015/09/14/us/shaken-baby-syndrome-a-diagnosis-that-divides-the-medical-world.html
12 Plunkett J. Shaken baby syndrome and the death of Matthew Eappen: a forensic pathologist’s response. Am J Forensic Med Pathol 1999;20:17–21.
13 Ommaya AK, Goldsmith W, Thibault L. Biomechanics and neuropathology of adult and paediatric head injury. Br J Neurosurg 2002;16:220–42. doi:10.1080/02688690220148824
14 Barnes PD. Imaging of Nonaccidental Injury and the Mimics: Issues and Contro-versies in the Era of Evidence-Based Medicine. Radiol Clin North Am 2011;49:205–29. doi:10.1016/j.rcl.2010.08.001
15 Geddes JF, Vowles GH, Hackshaw AK, et al. Neuropathology of inflicted head injury in childrenII. Microscopic brain injury in infants. Brain 2001;124:1299–306. doi:10.1093/brain/124.7.1299

35
16 Geddes JF, Hackshaw AK, Vowles GH, et al. Neuropathology of inflicted head injury in childrenI. Patterns of brain damage. Brain 2001;124:1290–8. doi:10.1093/brain/124.7.1290
17 Geddes JF, Tasker RC, Hackshaw AK, et al. Dural haemorrhage in non-traumatic infant deaths: does it explain the bleeding in ‘shaken baby syndrome’? Neuropa-thol Appl Neurobiol 2003;29:14–22. doi:10.1046/j.1365-2990.2003.00434.x
18 Lynøe N, Eriksson A. Is there a common denominator for Brief Resolved Unex-plained Events, Sudden Infant Death Syndrome, and alleged Shaken Baby Syn-drome? Med Hypotheses 2020;144:109939. doi:10.1016/j.mehy.2020.109939
19 Rooks VJ, Eaton JP, Ruess L, et al. Prevalence and Evolution of Intracranial Hemorrhage in Asymptomatic Term Infants. Am J Neuroradiol 2008;29:1082–9. doi:10.3174/ajnr.A1004
20 Gabaeff SC. Investigating the possibility and probability of perinatal subdural he-matoma progressing to chronic subdural hematoma, with and without complica-tions, in neonates, and its potential relationship to the misdiagnosis of abusive head trauma. Leg Med Tokyo Jpn 2013;15:177–92. doi:10.1016/j.legal-med.2012.12.003
21 Atkinson N, van Rijn RR, Starling SP. Childhood Falls With Occipital Impacts. Pediatr Emerg Care Published Online First: 6 June 2017. doi:10.1097/PEC.0000000000001186
22 Nobuhiko A. Infantile Acute Subdural Hematoma with Retinal Hemorrhage Caused by Minor Occipital Impact Witnessed by an ICU Nurse: A Case Report. J Pediatr Neurol Neurosci 2020;4. doi:10.36959/595/406
23 Plunkett J. Fatal Pediatric Head Injuries Caused by Short-Distance Falls. Am J Forensic Med Pathol 2001;22:1–12.
24 Otterman G, Ludvigsson JF, Söder O, et al. ”Skakvåld ger hjärnskador hos tiotals spädbarn varje år”. DN.SE. 2014.https://www.dn.se/debatt/skakvald-ger-hjarnskador-hos-tiotals-spadbarn-varje-ar/
25 Lynøe N, Elinder G, Hallberg B, et al. Is accepting circular reasoning in shaken baby studies bad science or misconduct? Acta Paediatr Oslo Nor 1992 Published Online First: 13 June 2017. doi:10.1111/apa.13947
26 Choudhary AK, Servaes S, Slovis TL, et al. Consensus statement on abusive head trauma in infants and young children. Pediatr Radiol 2018;48:1048–65. doi:10.1007/s00247-018-4149-1
27 Lynøe N, Eriksson A. Is the procedure of diagnosing abusive head trauma a purely medical matter? Pediatr Radiol 2019;49:422–3. doi:10.1007/s00247-019-04344-1
28 Lynøe N, Eriksson A. The Unspoken Shaken Baby Lie Detector Algorithm—An Analysis of Diagnostic Procedures in Cases of Allegedly Abusive Head Trauma without External Signs of Trauma. J Res Philos Hist 2020;3:52. doi:10.22158/jrph.v3n2p52
29 Lynøe N, Juth N, Eriksson A. From Child Protection to Paradigm Protection—The Genesis, Development, and Defense of a Scientific Paradigm. J Med Philos Forum Bioeth Philos Med doi:10.1093/jmp/jhy015
30 Lynøe N, Juth N, Brook CB, et al. Do Child Abuse Pediatricians Search for a “Pediatric Vulcan Planet”? Comparison of Controversies about the Vulcan-Must-Exist-Theory and the Infant-Must-Have-Been-Shaken-Theory. J Res Philos Hist 2020;3:162. doi:10.22158/jrph.v3n2p162
31 CAFFEY J. Multiple fractures in the long bones of infants suffering from chronic subdural hematoma. AJR Am J Roentgenol 1946;56:163–73.
32 Weston WJ. Metaphysial fractures in infancy. Bone Jt J 1957;39:694–700.

36
33 Astley R. Multiple Metaphyseal Fractures in Small Children (Metaphyseal Fra-gility of Bone). Br J Radiol 1953;26:577–83. doi:10.1259/0007-1285-26-311-577
34 Silverman FN. The roentgen manifestations of unrecognized skeletal trauma in infants. Am J Roentgenol Radium Ther Nucl Med 1953;69:413–27.
35 Kempe CH, Silverman FN, Steele BF, et al. The Battered-Child Syndrome. In: C. Henry Kempe: A 50 Year Legacy to the Field of Child Abuse and Neglect. Springer, Dordrecht 2013. 23–38. doi:10.1007/978-94-007-4084-6_5
36 Kleinman PK, Blackbourne BD, Marks SC, et al. Radiologic contributions to the investigation and prosecution of cases of fatal infant abuse. N Engl J Med 1989;320:507–11. doi:10.1056/NEJM198902233200807
37 Kleinman PK. Diagnostic imaging in infant abuse. Am J Roentgenol 1990;155:703–12. doi:10.2214/ajr.155.4.2119097
38 Kleinman PK, Marks SC, Richmond JM, et al. Inflicted skeletal injury: a post-mortem radiologic-histopathologic study in 31 infants. AJR Am J Roentgenol 1995;165:647–50. doi:10.2214/ajr.165.3.7645487
39 Paterson CR. Osteogenesis imperfecta in the differential diagnosis of child abuse. Child Abuse Negl 1977;1:449–52. doi:10.1016/0145-2134(77)90025-4
40 Paterson CR, Monk EA. Temporary brittle bone disease: relationship between clinical findings and judicial outcome. Pediatr Rep 2011;3. doi:10.4081/pr.2011.e24
41 Holick MF, Hossein-Nezhad A, Tabatabaei F. Multiple fractures in infants who have Ehlers-Danlos/hypermobility syndrome and or vitamin D deficiency: A case series of 72 infants whose parents were accused of child abuse and neglect. Der-matoendocrinol 2017;9:e1279768. doi:10.1080/19381980.2017.1279768
42 Högberg U, Andersson J, Högberg G, et al. Metabolic bone disease risk factors strongly contributing to long bone and rib fractures during early infancy: A pop-ulation register study. PLOS ONE 2018;13:e0208033. doi:10.1371/jour-nal.pone.0208033
43 Narang SK, Estrada C, Greenberg S, et al. Acceptance of Shaken Baby Syndrome and Abusive Head Trauma as Medical Diagnoses. J Pediatr 2016;177:273–8. doi:10.1016/j.jpeds.2016.06.036
44 Chadwick DL, Chin S, Salerno C, et al. Deaths from Falls in Children: How Far is Fatal? J Trauma Acute Care Surg 1991;31:1353.
45 Adamsbaum C, Rey-Salmon C. Head Circumference: A Key Sign in Dating Abu-sive Head Trauma. Am J Neuroradiol 2015;36:E36–E36. doi:10.3174/ajnr.A4306
46 Piatt JH. A pitfall in the diagnosis of child abuse: external hydrocephalus, subdu-ral hematoma, and retinal hemorrhages. Neurosurg Focus 1999;7:E5. doi:10.3171/foc.1999.7.4.6
47 McNeely PD, Atkinson JD, Saigal G, et al. Subdural Hematomas in Infants with Benign Enlargement of the Subarachnoid Spaces Are Not Pathognomonic for Child Abuse. Am J Neuroradiol 2006;27:1725–8.
48 Vinchon M, Delestret I, DeFoort-Dhellemmes S, et al. Subdural hematoma in infants: can it occur spontaneously? Data from a prospective series and critical review of the literature. Childs Nerv Syst 2010;26:1195–205. doi:10.1007/s00381-010-1105-2
49 Ravid S, Maytal J. External hydrocephalus: a probable cause for subdural hema-toma in infancy. Pediatr Neurol 2003;28:139–41. doi:10.1016/S0887-8994(02)00500-3
50 Zahl SM, Egge A, Helseth E, et al. Benign external hydrocephalus: a review, with emphasis on management. Neurosurg Rev 2011;34:417–32. doi:10.1007/s10143-011-0327-4

37
51 Feldman KW, Sugar NF, Browd SR. Initial clinical presentation of children with acute and chronic versus acute subdural hemorrhage resulting from abusive head trauma. J Neurosurg Pediatr 2015;16:177–85. doi:10.3171/2014.12.PEDS14607
52 De Leeuw M, Beuls EA, Jorens PG, et al. History of an Abusive Head Trauma Including a Lucid Interval and a Retinal Hemorrhage Is Most Likely False. Am J Forensic Med Pathol 2013;34:271–276. doi:10.1097/PAF.0b013e3182a0a454
53 Daniel JH, Newberger EH, Reed RB, et al. Child abuse screening: Implications of the limited predictive power of abuse discriminants from a controlled family study of pediatric social illness. Child Abuse Negl 1978;2:247–59. doi:10.1016/0145-2134(78)90023-6
54 Christian CW, Block R, Committee on Child Abuse and Neglect, et al. Abusive head trauma in infants and children. Pediatrics 2009;123:1409–11. doi:10.1542/peds.2009-0408
55 Brown JK, Minns RA. NON-ACCIDENTAL HEAD INJURY, WITH PARTIC-ULAR REFERENCE TO WHIPLASH SHAKING INJURY AND MEDICO-LE-GAL ASPECTS. Dev Med Child Neurol 1993;35:849–69. doi:10.1111/j.1469-8749.1993.tb11563.x
56 Fleming P, Byard RW. Subdural haemorrhage in infants: abuse or natural causes? The importance of thorough child death review. Acta Paediatr Oslo Nor 1992 Published Online First: 27 December 2017. doi:10.1111/apa.14185
57 Andersson J, Thiblin I. It is important not to assume an aetiology for the triad before the outcomes of diagnostic investigations. Acta Paediatr 2018;107:1308–9. doi:10.1111/apa.14276
58 Guthkelch AN. Problems of Infant Retino-Dural Hemorrhage with Minimal Ex-ternal Injury. Houst J Health Law Policy 2011;12:201–8.
59 Kemp AM, Jaspan T, Griffiths J, et al. Neuroimaging: what neuroradiological features distinguish abusive from non-abusive head trauma? A systematic review. Arch Dis Child 2011;96:1103–12. doi:10.1136/archdischild-2011-300630
60 Maguire SA, Watts PO, Shaw AD, et al. Retinal haemorrhages and related find-ings in abusive and non-abusive head trauma: a systematic review. Eye Lond Engl 2013;27:28–36. doi:10.1038/eye.2012.213
61 Lam WW, Ai VH, Wong V, et al. Ultrasonographic measurement of subarach-noid space in normal infants and children. Pediatr Neurol 2001;25:380–384.
62 Hussain ZB, Hussain AB, Mitchell P. Extra-axial cerebrospinal fluid spaces in children with benign external hydrocephalus: A case-control study. Neuroradiol J 2017;30:410–7. doi:10.1177/1971400917719298

Acta Universitatis UpsaliensisDigital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 1702
Editor: The Dean of the Faculty of Medicine
A doctoral dissertation from the Faculty of Medicine, UppsalaUniversity, is usually a summary of a number of papers. A fewcopies of the complete dissertation are kept at major Swedishresearch libraries, while the summary alone is distributedinternationally through the series Digital ComprehensiveSummaries of Uppsala Dissertations from the Faculty ofMedicine. (Prior to January, 2005, the series was publishedunder the title “Comprehensive Summaries of UppsalaDissertations from the Faculty of Medicine”.)
Distribution: publications.uu.seurn:nbn:se:uu:diva-426036
ACTAUNIVERSITATIS
UPSALIENSISUPPSALA
2021