aspects ofinterhemispheric subdural haematoma, … neurosurgery, andpsychiatry, 1978,41, 72-75...
TRANSCRIPT
Journal ofNeurology, Neurosurgery, and Psychiatry, 1978, 41, 72-75
Aspects of interhemispheric subdural haematoma,including the falx syndromeJAMES S. OGSBURY, STUART A. SCHNECK, ANDRALPH A. W. LEHMAN
From the Division of Neurosurgery and the Department of Neurology, University of ColoradoMedical Center, Denver, Colorado, USA
S UM M A R Y Two cases of interhemispheric subdural haematoma are reported. The firstpatient presented with a falx syndrome of contralateral hemiparesis, most marked in the lowerextremity. The second patient had vertex headaches and was diagnosed with computerisedtomography. Serial studies suggested that the interhemispheric haematoma may have migratedto a lateral position over the cerebral convexity.
Although subdural haematomas generally occurover the convexity of the hemispheres, theyoccasionally present in the interhemispheric fissure(Aring and Evans, 1940; Jacobsen, 1955; Gannon,1961; Wollschlaeger and Wollschlaeger, 1964;Isfort, 1967; Clein and Bolton, 1969; Sibayan etal., 1970). In the past, the importance of cerebralangiography has been emphasised in these cases(Jacobsen, 1955; Gannon, 1961; Wollschlaegerand Wollschlaegar, 1964; Isfort, 1967; Clein andBolton, 1969; Sibayan et al., 1970). We haverecently had the opportunity to treat two patientswith interhemispheric subdural haematomas. Thefirst patient presented with a constellation of signsand symptoms which might have pointed to thediagnosis before angiography. The diagnosis inthe second case was made by computerisedtomography.
Case reports
CASE 1A 70 year old physician was well until she wasknocked over by her dog and struck her occiputon a table without losing consciousness. Threehours later she developed a diffuse headache, andsubsequently became nauseated and vomited.Neurological examination 24 hours later wasentirely normal. However intermittent headacheand vomiting persisted, and, 36 hours after injury,
Address for reprint requests: Dr Ralph A.W. Lehman, Division ofNeurosurgery, University of Colorado Medical Center, 4200 E. 9thAvenue, Denver, Co. 80262, USA.Accepted 9 August 1977
72
she developed numbness and weakness of her leftleg and then her left arm. Examination at thattime revealed a blood pressure of 152/80 mmHgand a pulse rate of 60 per minute. She was alertand fully oriented, and had normal fundi, pupils,and extraocular movements. There was a lefthemiparesis, severe in the leg, mild in the arm,and minimal in the face. Deep tendon reflexeswere slightly less brisk on the left than theright. Sensation was intact. Skull radiographswere normal with the pineal calcification in themidline.
In view of the dramatic leg paresis in the faceof a normal mental status it was thought that shemight have developed an anterior cerebral arterythrombosis as a result of dehydration secondary tovomiting. The possibility of a post-traumatic intra-cranial haematoma was considered to be lesslikely. Twelve hours after admission left sidedseizures occurred predominantly in the lowerextremity. Angiography disclosed a right inter-hemispheric mass (Figs. 1 and 2), and was followedby a craniotomy with subtotal removal of aninterhemispheric blood clot extending the lengthof the falx. Postoperatively she was somnolentand required tracheotomy but gradually improved,and was discharged 25 days after surgery. By threemonths after the operation she had recovered hernormal leg strength and was beginning to resumefull professional activities.
CASE 2A 44 year old man suffered a blow to the headduring a wrestling match. He was not knocked
Protected by copyright.
on 22 July 2019 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.41.1.72 on 1 January 1978. D
ownloaded from
Aspects of interhemispheric subdural haematoma, including the falx syndrome
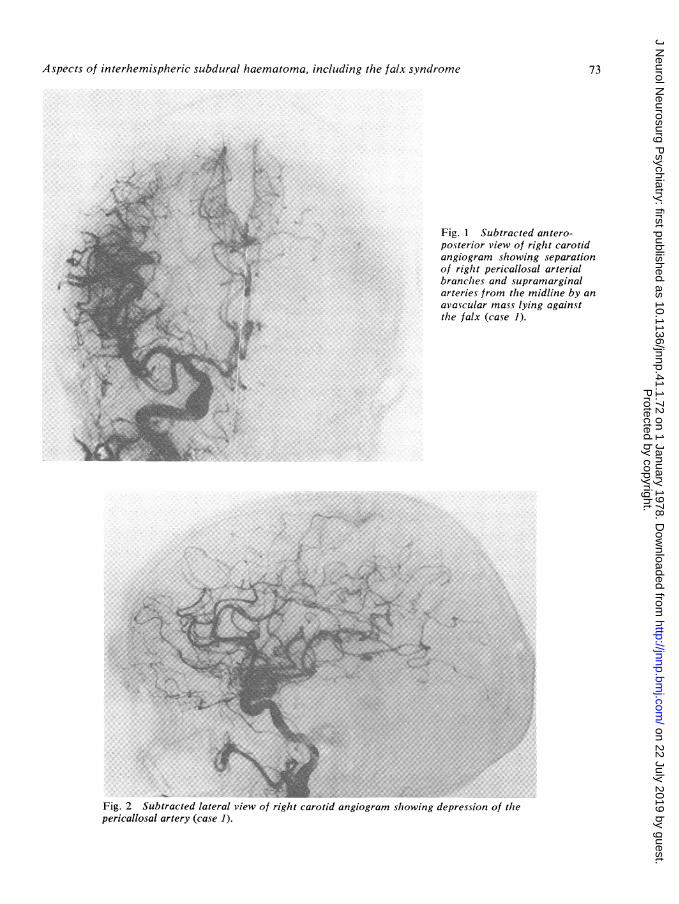
Fig. 1 Subtracted antero-posterior view of right carotidangiogram showing separationof right pericallosal arterialbranches and supramarginalarteries from the midline by anavascular mass lying againstthe falx (case 1).
,.... -- a- u ... z]aS.
.. \ o..e t+4.. 's. .. .W . . 3|9, . . .
*. w -....
Fig. 2 Subtracted lateral view of right carotid angiogram showing depression of thepericallosal artery (case 1).
73
I
4;k.
X
.to-;.,.,-41.1. 0--
111ho
'.N... ki .........N
Protected by copyright.
on 22 July 2019 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.41.1.72 on 1 January 1978. D
ownloaded from
James S. Ogsburv, Stuart A. Schneck, and Ralph A. W. Lehman
out but several hours later developed persistentvertex headache. About four days after his injuryhe had a grand mal seizure. Neurological examina-tion at one week revealed only slight confusion.Computerised tomography disclosed an inter-hemispheric mass having the density of clottedblood which lay against the left side of the falx(Fig. 3). There was a very slight shift of the mid-line structures to the right. No other lesions wereevident. He was admitted to the hospital, and overthe next few days his headache disappeared.Computerised tomography two weeks after injuryshowed partial resolution of the interhemispherichaematoma but a slight increase of the left toright shift. During the next week the patient againdeveloped headache. A third computerised tomo-graphic scan revealed an even larger left to rightshift but no masses were seen. Angiography wasperformed and showed an extracerebral mass overthe left hemisphere. A liquid subdural haematomawas removed through burr holes. A computerisedscan one week after operation revealed minimalmidline shift. A mild right postoperative hemi-paresis cleared, and the patient was discharged10 days after surgery.
Discussion
As shown by our two cases as well as seven ofeight clinical reports (Aring and Evans, 1940;
Jacobsen, 1955; Gannon, 1961; Wollschlaeger andWollschlaeger, 1964; Isfort, 1967; Sibayan et al.,1970), interhemispheric subdural haematomas areusually unilateral. Most patients with inter-hemispheric subdural haematomas have acharacteristic clinical picture although this is notcommonly realised. Of the five reported patientsfor whom sufficient description of hemiparesis isprovided, four presented with dramatic paresis orseizures of the contralateral leg or both. In thesefour patients and in one of ours, weakness in thearm and face has been of much lesser degree(Aring and Evans, 1940; Jacobsen, 1955; Woll-schlaeger and Wollschlaeger, 1964; Sibayan et al.,1970). The same clinical picture has been foundin patients with interhemispheric subduralempyema (Keith, 1949; List, 1950, 1955; Kristian-sen and Zimmer, 1958; Hitchcock and Andreadis,1964; Patton and Hitchcock, 1968; Wilkins andGoree, 1970) and has been called the falx syn-drome (List, 1955). In cases of subdural empyema,these symptoms have been ascribed to thrombo-phlebitis (Hitchcock and Andreadis, 1964).However, thrombophlebitis would not be expectedto occur in cases of subdural haematoma. More-over mass effect seen angiographically withempyema is identical to that of interhemisphericsubdural haematomas (List, 1950, 1955; Kristian-sen and Zimmer! 1958; Hitchcock and Andreadis.1964; Patton and Hitchcock, 1968; Wilkins and
I-
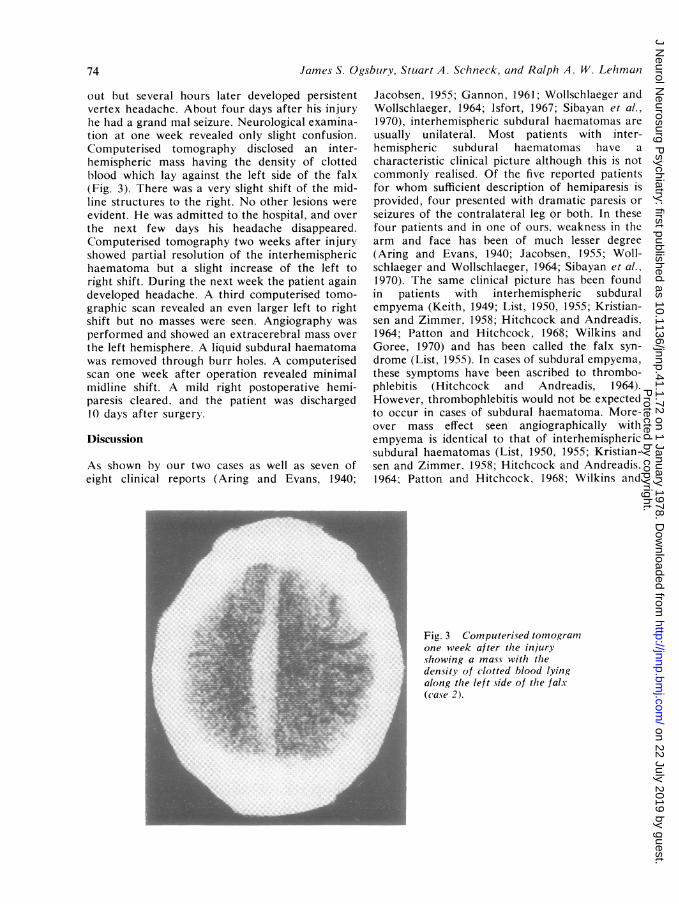
' Fig. 3 Computerised tomogramri one week after the injury
showing a mass with thedensity of clotted blood lying
. along the left side of the falx(case 2).
74
Protected by copyright.
on 22 July 2019 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.41.1.72 on 1 January 1978. D
ownloaded from
Aspects of interhemispheric sulbduiral haematoma, inclulding the falx syndrome
Goree, 1970). This suggests that both interhemi-spheric empyemas and subdural haematomas mayproduce the falx syndrome by virtue of their masseffect.Both subdural haematomas and empyemas of
the interhemispheric space appear to be quiteuncommon. On the other hand, occlusion of ananterior cerebral artery is a much more frequentoccurrence and also produces the clinical pictureof the falx syndrome. For these reasons, wethought initially that our first patient probablyhad symptoms related to vascular insufficiencyrather than a post-traumatic haematoma.Our second case illustrates the possibility that
occasional cases of chronic subdural haematomasof the convexity may originate as acute inter-hemispheric clot. The sequence of radiographicstudies suggests that the initial clot was confinedto the interhemispheric space whereas it was laterlimited to the space over the cerebral convexity.This possibility, that interhemispheric haematomasmay move as they liquefy, may provide an alterna-tive to early surgery. While removal of a solidclot from the interhemispheric space has provedto be successful, this can be a dangerous proceduredue to the proximity of the sagittal sinus andbridging veins (Gannon, 1961). It is. therefore,conceivable that if a patient with an acute inter-hemispheric haematoma is relatively asympto-matic, initial conservative management might befollowed by migration of the clot to a positionover the convexity where removal is considerablyless dangerous.
References
Aring. C. D.. and Evans. J. P. (1940). Aberrantlocation of subdural hematoma. Archives of Neuro-logy and Psychiatry (Chicago), 44, 1296-1306.
Clein. L. J.. and Bolton. C. F. (1969). Interhemisphericsubdural haematoma: a case report. Journal ofNeurology, Neurosurgery, and Psychiatry, 32, 389-392.
Gannon, W. E. (1961). Interhemispheric subduralhematoma, case report. Journal of Neurosurgery,18, 829-830.
Hitchcock, E.. and Andreadis. A. (1964). Subduralempyema: a review of 29 cases. Journal ofNeurology, Neurosurgery, and Psychiatry, 27, 422-434.
Isfort, A. (1967). Angiographische Befunde beimHamatom und Empyem im Interhemispharenspalt.Fortschrifte auf dem Gebiete der Rontgenstrahlen,107, 127-130.
Jacobsen, H. H. (1955). An interhemisphericallysituated haematoma. case report. Acta Radiologica.43, 235-236.
Keith, W. S. (1949). Subdural empyema. Journal ofNeurosurgery, 6, 127-139.
Kristiansen, K., and Zimmer, J. (1958). Interhemi-spheric subdural abscess. British Journal ofRadiology, 31, 278-279.
List. C. F. (1950). Interhemispheric subdural sup-puration. Journal of Neurosurgery, 7, 313-324.
List, C. F. (1955). Diagnosis and treatment of acutesubdural empyema. Neurology (Minneapolis), 5,663-670.
Patton, J. T., and Hitchcock, E. (1968). Angiographicfeatures of falcine subdural empyema. ClinicalRadiology, 19, 229-232.
Sibayan, R. Q., Gurdjian, E. S., and Thomas, L. M.(1970). Interhemispheric chronic subdural hema-toma, report of a case. Neurology (Minneapolis),20, 1215-1218.
Wilkins, R. H., and Goree, J. A. (1970). Interhemi-spheric subdural empyema: angiographic appear-ance. Journal of Neurosurgery, 32, 459-462.
Wollschlaeger, P. B., and Wollschlaeger, G. (1964).The interhemispheric subdural or falx hematoma.A merican Journal of Roentgenology, 92, 1252-1254.
75
Protected by copyright.
on 22 July 2019 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.41.1.72 on 1 January 1978. D
ownloaded from