achalasie – Übersicht therapieoptionen · 3 gastroenterologie poem - demofilm gastroenterologie...
TRANSCRIPT
1
Gastroenterologie
Achalasie -
Endoskopische Therapieoptionen
Patrick Aepli Gastroenterologie / Hepatologie
Astra Fokus
Gastroenterologie
Achalasie – Übersicht Therapieoptionen
MEDIKAMENTÖS1,2,3
- Nitrate - Calciumantagonisten - Phosphodiesterase-Inhibitoren (zB Viagra)
ENDOSKOPISCH - Botoxinjektion - Pneumatische Ballondilatation - in klinischer Erprobung: Stents & POEM
CHIRURGISCH - Myotomie - Ösophagektomie
1) Gelfond M et al. Isosorbide dinitrate and nifedipine treatment of achalasia: a clinical, manometric and radionuclide evaluation. Gastroenterology 1982;83:963-969. 2) Coccia G et al. Return of esophageal peristalsis after nifedipine therapy in patients with idiopathic esophageal achalasia. Am J Gastroenterol 1992;87:1705-1708. 3) Bortolotti M et al. Effects of sildenafil on esophageal motility of patients with idiopathic achalasia. Gastroenterology 2000;118:253-257.
Gastroenterologie
Endoskopische Botoxinjektion (EBTI)1,2
Allgemein
- Botox = Acetylcholinesterasehemmer - total 80-100 U, verteilt in alle LES-Quadranten - sicher, leicht zu applizieren, nicht teuer und (zumindest
kurzzeitig) effektiv
Indikation - dort, wo andere Therapie-Optionen „relativ“ kontraindiziert
sind, zB - alte, morbide Patienten
1) Pasricha PJ et al. Treatment of achalasia with intrasphincteric injection of botulinum toxin. A pilot trial. Ann Intern Med 1994;121:590-591. 2) Pasricha PJ et al. Intrasphincteric botulinum toxin for the treatment of achalasia. N Engl J Med 1995;332:774-778.
Gastroenterologie
EBTI – good to know
Therapie-Erfolg1,2,3
- nach max. 2 Injektionen (in 3 Mt) sind nach 1y 40-60% klinisch beschwerdefrei
- Rezidive entsprechend häufig - besseres Ansprechen: ältere Patienten & spastischer Ac-Typ
Problem der Kostenübernahme - 100 U = CHF 418
Einfluss auf andere Therapie-Optionen4
- vormalig mit Botox behandelte Patienten haben schlechteres Outcome bei nachfolgender Myotomie
1) Dughera L et al. Botulinum toxin treatment of oesophageal achalasia in the old old and oldest old: a 1-year follow-up study. Drugs Aging 2005;22(9):779-783. 2) D‘Onofrio V et al. Long-term follow-up of achalasic patients treated with botulinum toxin. Dis Esophagus 2000;13(2):96-101. 3) Campos GM et al. Endoscopic and surgical treatments for achalasia: a systematic review and meta-analysis. Ann Surg 2009;249:45-57. 4) Smith CD et al. Endoscopic therapy for achalasia before Heller myotomy results in worse outcomes than Heller myotomy alone. Ann Surg 2006;243:579-584.
Gastroenterologie
Pneumatische Ballondilatation - Vorbereitung / Intervention
Informed consent PPI 1 Wo vor Dilatation am Tag vor Intervention flüssige Kost, nüchtern 6 h vor
Intervention Intubation Ösophagus in Linksseitenlage (Aspirationsrisiko minim) allfällige, ösophageale Speisereste absaugen Führungsdraht ins Magenantrum Einführen Ballon über Führungsdraht (1. Dilatation mit 30 mm) Ballon mittig auf Höhe Z-Linie platzieren Ballon aufdehnen bis Taillierung verschwindet Ballon ablassen und entfernen Endoskopische Kontrolle (Perforation?)
Gastroenterologie
Pneumatische Ballondilatation – unter endoskopischer Kontrolle

2
Gastroenterologie
Pneumatische Ballondilatation – unter BV-Kontrolle
Gastroenterologie
Pneumatische Ballondilatation - postinterventionell
Überwachung für 2-4 h, dann Entlassung möglich Analgesie (Paracetamol, NSAID) Gastrographinpassage (falls V. a. Leckage) PPI für 4 Wo
klinische Re-Evaluation nach 2 - 4 Wo - falls Symptome persistieren, erneute Dilatation(en) mit
zunehmendem Ballondurchmesser (35 resp. 40 mm)
"non Responder" trotz 3 Dilatationen (bis max. 40 mm) sollten zwecks lap Myotomie den Chirurgen zugewiesen werden
Gastroenterologie
Pneumatische Ballondilatation - Zusammenfassung1,2,3,4,5
effektive Therapie für operable Patienten Ballondilatatoren 30, 35 und 40 mm nach Bedarf 2-3 Dilatationen (ggfs mehrere Serien)
Therapie-Erfolg - Beschwerdefreiheit oder deutliche –besserung in 70-85% für > 1y
oder länger - nach etwa 5y aber in etwa 30-50% der Fälle Re-Dilatation nötig
Komplikationen - Perforation 3-5% (meist anlässlich 1. Dilatation) - Reflux 0-9%
Prädiktive Faktoren - LES-Druck nach Dilatation < 10 mmHg -> gutes Outcome - Frauen und Alter > 40y -> besseres Ansprechen auf Dilatation
1) Hulselmans M et al. Long-term outcome of pneumatic dilation in the treatment of achalasia. Clin Gastroenterol Hepatol 2010;8:30-835. 2) Chuah SK et al. Clinical remission in endoscope-guided pneumatic dilation for the treatment of esophageal achalasia: 7-year follow-up results. J Gastrointest Surg 2009;13:862-867. 3) West RL. Long term results of pneumatic dilation in achalasia followed for more than 5 years. Am J Gastroenterol 2002;97:1346–1351. 4) Campos GM et al. Endoscopic and surgical treatments for achalasia: a systematic review and meta-analysis. Ann Surg 2009;249:45–57. 5) Vela MF et al. The long-term efficacy of pneumatic dilatation and Heller myotomy for the treatment of achalasia. Clin Gastroenterol Hepatol 2006;4:580–587.
Gastroenterologie
Pneumatische Ballondilatation (PD) vs Laparoskopische Myotomie (LHM)1
Therapie-Erfolg - nach 1y 90% (PD) vs 93% (LHM) - nach 2y 86% (PD) vs 90% (LHM)
Komplikationen - Perforation 4% (PD) vs mukosale Schleimhauteinrisse 12% (LHM) - Reflux 15% (PD) vs 23% (LHM)
LES-Druck nach 2y - 12 mmHg (PD) vs 10 mmHg (LHM)
Vorteile PD - ambulant, minimale Sz, geringes Refluxrisiko, kann bei jeder Altersgruppe
sowie während Schwangerschaft durchgeführt werden, behindert nicht spätere LHM, primär billiger als LHM
Vorteile LHM - einzeitige Intervention, Kontrolle der Dysphagie oft anhaltender (auf Kosten
eines erhöhten Refluxrisikos), evtl effizienter bei jüngeren Patienten (va Männer)
1) Boeckxstaens GE et al. Pneumatic dilation versus laparoscopic Heller‘s Myotomy for idiopathic achalasia. NEJM 2011;364:1807-1816.
Gastroenterologie
Stent1
kardiaüberbrückende Einlage (für 4-5 d) eines Nitinol-Metallstents (30 mm)
klinisch anhaltende Beschwerdefreiheit nach 10 Jahren von >80%
mögliche Komplikationen - Migration 5% - Reflux 20% - Th-Sz 35% - keine Perforation
1. Zhao JG et al. Long-term safety and outcome of a temporary self-expanding metallic stent for achalasia: a prospective study with a 13-year single-center experience. Eur Radiol 2009;19:1973–1980.
Gastroenterologie
POEM – peroral orifical esophageal myotomy1,2,3
1. Pasricha PJ et al. Submucosal endoscopic esophageal myotomy: a novel experimental approach for the treatment of achalasia. Endoscopy. 2007;39:761-764. 2. Inoue H et al. Peroral endoscopic myotomy (POEM) for esophageal achalasia. Endoscopy 2010;42:265-271. 3. Van Rentelen D et al. Peroral Endoscopic Myotomy for the Treatment of Achalasia: a prospective single center study. Am J Gastroenterol 2012;107:411-417.
Form von NOTES endoskopische Myotomie in Vollnarkose Therapie-Erfolg3
- in 94% - LES-Druck 27 mmHg -> 12 mmHg - Reflux in 6%
Fazit vielversprechende, neue Therapieoption mit sehr gutem Outcome
(vergleichbar mit LHM) weitere Studien notwendig bzgl Langzeit-Outcome und Vergleich mit
bisherigen Therapieoptionen
3
Gastroenterologie
POEM - Demofilm
Gastroenterologie
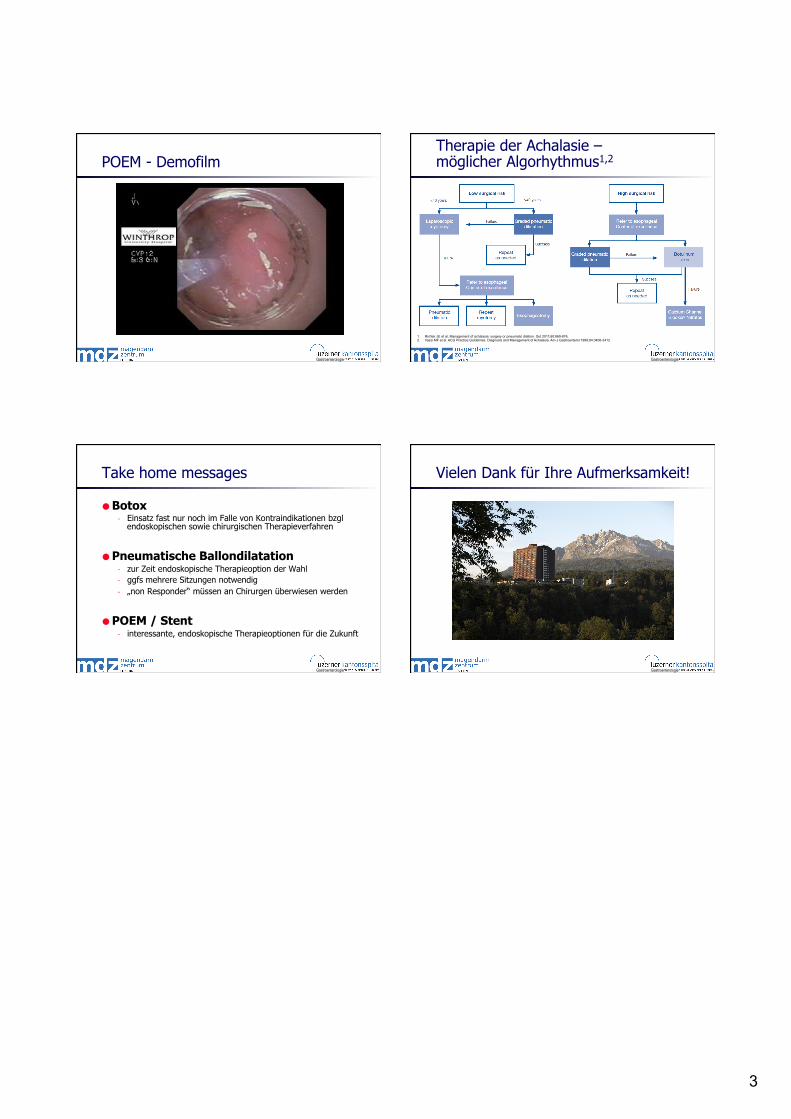
Therapie der Achalasie – möglicher Algorhythmus1,2
1. Richter JE et al. Management of achalasia: surgery or pneumatic dilation. Gut 2011;60:869-876. 2. Vaezi MF et al. ACG Practice Guidelines. Diagnosis and Management of Achalasia. Am J Gastroenterol 1999;94:3406-3412.
Gastroenterologie
Take home messages
Botox - Einsatz fast nur noch im Falle von Kontraindikationen bzgl
endoskopischen sowie chirurgischen Therapieverfahren
Pneumatische Ballondilatation - zur Zeit endoskopische Therapieoption der Wahl - ggfs mehrere Sitzungen notwendig - „non Responder“ müssen an Chirurgen überwiesen werden
POEM / Stent - interessante, endoskopische Therapieoptionen für die Zukunft
Gastroenterologie
Vielen Dank für Ihre Aufmerksamkeit!