abdominal wound dehiscence - university of...
TRANSCRIPT

Abdominal Wound Dehiscence
Presenter: T Mohammed
Moderator: Dr H Pienaar

Introduction
• Wound Dehiscence is the premature "bursting" open of a wound along surgical suture. It is a surgical complication that results from poor wound healing. Risk factors in general are age, diabetes, obesity, poor knotting or grabbing of stitches, and trauma to the wound after surgery. Sometimes a pink (serosanguinous) fluid may leak out.

Introduction
• Abdominal wound dehiscence (burst
abdomen, fascial dehiscence) is a severe
postoperative complication, with mortality rates reported as high as 45%.
The incidence as described in the literature
ranges from 0.4% to 3.5%.

Introduction
• Abdominal wound dehiscence can result in
evisceration, requiring immediate treatment.
Prolonged hospital stay, high incidence of
incision hernia, and subsequent reoperations underline the severity of this complication.
Introduction
• Despite advances in perioperative care and
suture materials, incidence and mortality rates in
regard to abdominal wound dehiscence have not
significantly changed over the past decades. This
may be attributable to increasing incidences of risk factors within patient populations outweighing the benefits of technical achievements.

Types of Wounds
Recent Literature
• In this study by Van Ramshorst et al (World J
of Surg 2010;34:20-27) the objective was to
develop a risk model to recognize high risk
patients and identify independent risk factors
for abdominal wound dehiscence. The study
was conducted at the department of surgery,
Erasmus University Medical Center, Rotterdam,
Netherlands.

Recent Literature
• A total of 363 cases and 1,089 controls were
analyzed. Major independent risk factors were:
age, gender, chronic pulmonary disease, ascites, jaundice, anemia, emergency surgery, type of surgery, postoperative coughing, and wound infection.
Recent Literature
• In the validation population, risk scores were
significantly higher (P<0.001) for patients with
abdominal wound dehiscence (n = 19)
compared to those without (n = 677). Resulting scores ranged from 0 to 8.5, and the risk for abdominal wound dehiscence over this range increased exponentially from 0.02% to 70.1%.

Risk Formula
• The validated risk model shows high predictive
value for abdominal wound dehiscence and
may help to identify patients at increased risk.
The calculation of the probability of abdominal wound dehiscence for an individual surgical patient is performed in two steps.

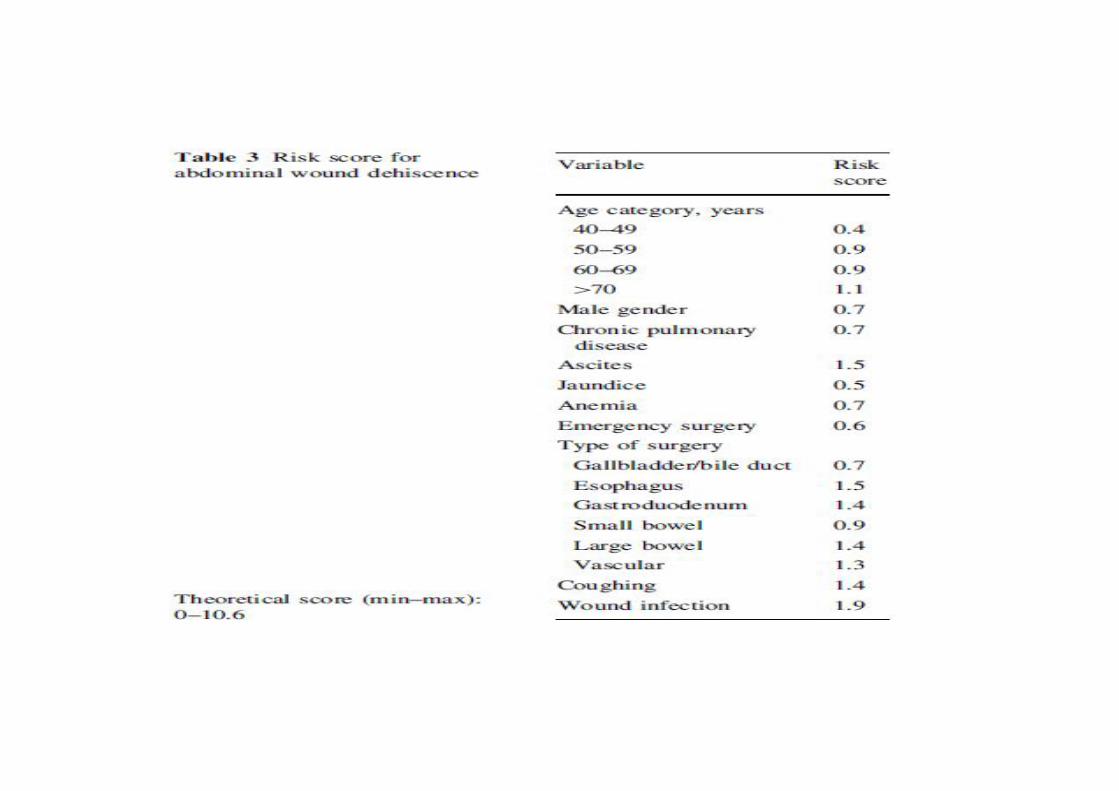
Risk Formula
• First, the total risk score is calculated byadding the weights of the various variablesshown in Table 1. In the second step, theprobability of developing abdominal wounddehiscence, P, is calculated according to thelogistic formula: P= eх/ (1+ex )x100%;where ‘ex’represents the exponential function and ‘x’represents ‘-8.37 + (1.085 x calculated total riskscore)’.

Risk Calculation
• For example, the risk score for a 67-year-old manwho undergoes an elective reconstruction of theabdominal aorta and is known to have a history ofchronic pulmonary disease is 0.9 (score for age 60–69 years) + 0.7 (score for male gender) ? 1.3 (scorefor vascular surgery) + 0.7 (score for chronic pulmonarydisease), for a total of 3.6. The probability, P, of thispatient’s developing abdominal wound dehiscence is:e(-8.37+(1.085x3.6)) /1+e (-8.37+(1.085x3.6)) x100%= 1.1%
Risk Calculation
• An emergency repair in a similar patient with
a ruptured aneurysm and subsequent anemia
results in a total score of 4.9 (i.e., subtotal of
3.6 points + 0.6 emergency + 0.7 anemia). Thus, the absolute risk rises to 4.5%.
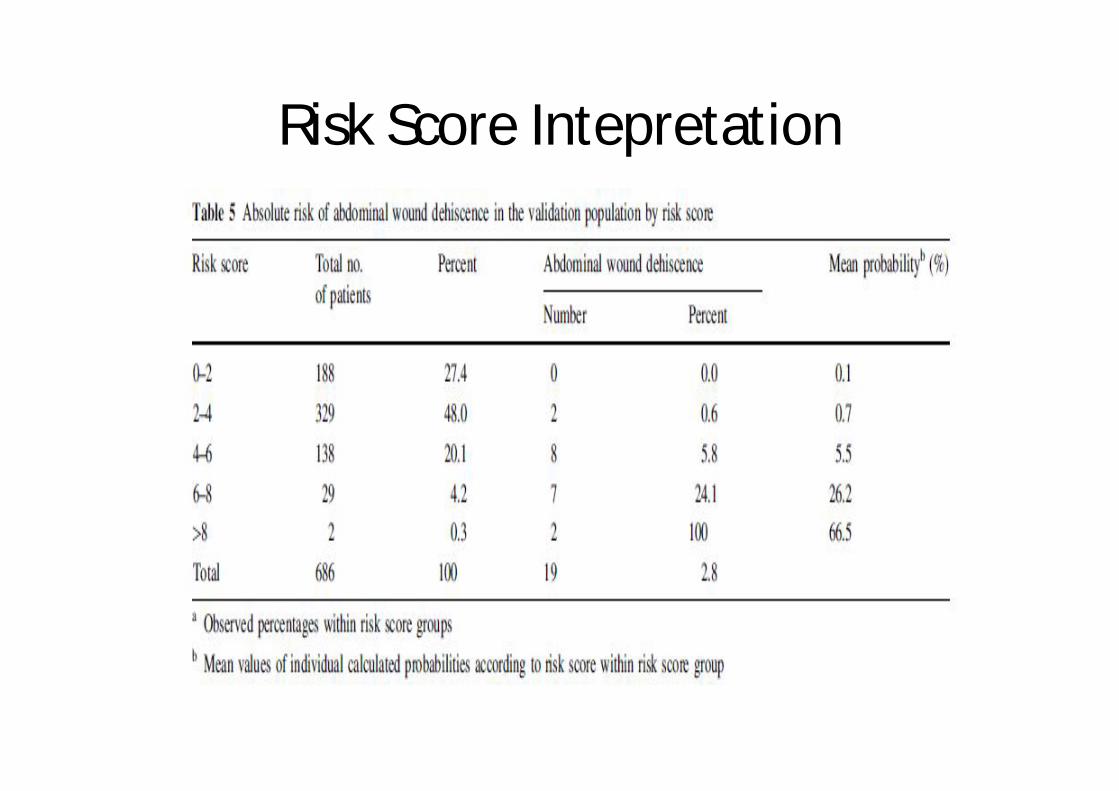
Risk Score Intepretation

Risk factors
• Patients who undergo emergency surgery aregenerally in worse condition and nutritionalstate, and the chance of contamination of thesurgical field is higher than in elective surgery. Moreover, the performance of the surgeon might be affected at night, which could lead tosuboptimal closure of the abdomen at the endof the operation.

Risk factors
• Old age is another independent risk factor for
abdominal wound dehiscence. Age has also
been reported as a risk factor in other studies.
The explanation for this might lie in deterioration
of the tissue repair mechanism in the elderly.
Especially during the first few days of the wound
healing process, the immune system plays a key
role.

Risk Factors
• One of the interesting risk factors found in this
Rotterdam study, is gender. In previous studies, males have been reported to have a higher risk of developing abdominal wound dehiscence.
This was attributed to smoking as a possible
confounder and its effect on tissue repair.

Risk Factors
• Another explanation may be that men build
up higher abdominal wall tension than females.
An increase in intra-abdominal pressure results in higher strain on the wound edges, causing the sutures to cut through the muscles and fascia.

Risk Factors
• In the Rotterdam study, wound infection proved
to be the risk factor with the highest relative
weight. Its importance has been confirmed by
virtually every study on this topic. Continued
presence of bacteria causes influx and
activation of neutrophils and increases in levels
of degradative matrix metalloproteinases(MMPs).

Risk Factors
• In the absence of sufficient tissue inhibitors ofMMPs, wound degradation will occur. Therelease of endotoxins by bacteria leads to theproduction of collagenase, which degradescollagen fibers. Infection thereby causes aprolongation of the inflammatory phase andnegatively affects deposition of collagen and fibroblast activity.

Risk factors
• In wounds of patients with abdominal wound
dehiscence, it has been observed that
degradation of collagen exceeds the synthesis
of collagen, which adversely affects breaking
strength. Adequate tissue breaking strength is
necessary, however, to provide support for the
sutures that hold the wound edges together.
Risk Factors
Low breaking strength can therefore amount to
abdominal wound dehiscence, especially in the
presence of increased intra-abdominal pressure
and abnormal inflammatory response.

Risk factors
• Primary repair can be difficult or impossible
when tissue has low breaking strength, creating the need for the use of mesh or acceptance of the high risk of recurrent abdominal wound dehiscence.

Risk factors
• Risk factors that did not have independent
effects in the Rotterdam study included:
1.hypertension
2.uremia
3. corticosteroid use.
Risk Factors
• The Rotterdam study found no significant effect on the occurrence of abdominal wound dehiscence for diabetes mellitus and previous laparotomy. Malignancy, sepsis, and postoperative vomiting have been identified as risk factors by several authors, but no significant effects were found in the present study.

Risk factors
• This was surprising because it was suspected
that the presence of scar tissue, microvascular
changes due to hypertension and diabetes,
poor tissue perfusion, and poor overall
condition of the patient, associated with sepsis and malignancy, would be risk factors.

Risk factors
• Jaundice, on the other hand, was found to be
an independent risk factor.
The conclusion of The Rotterdam study was that wound healing is affected in jaundiced patients due to the association with low hematocrit and albumin levels and malignancy (i.e., poor nutritional status) and not to raised bilirubin levels.

Risk Factors
• Low protein and albumin levels and
deficiencies of several vitamins and minerals
such as vitamins A, B1, B2, B6, C and zinc,
selenium and copper have been associated with poor wound repair.

Risk Factors
• Anemia is a risk factor that is related to
increased perioperative stress, blood
transfusions, and decreased tissue oxygenation, all of which can affect the immune system and the wound healing process.
American Risk Model
• A similar validation model of risk of dehiscence index was developed by an American group in Salt Lake City Utah in 2003 using data from the Veterans Affairs National Surgical Quality Improvement Program but lacks a formula for calculating the probability of developing dehiscence as in the Rotterdam Study.

American Risk Model
• There are several limitations to this study.
Because the veterans carry more comorbidities than the general population, our results may not be generalizable to the public at large.

Abdominal Wall Closure
For secure abdominal wall closures, the reduced tissue integrity along the border of the acute wound led to development of the concept of an optimal suture length–to–wound length (Suture Length-to-Wound Length) ratio for the primary closure of midline laparotomies .

Abdominal Wall Closure
Well-done, large, prospective studies with the
best follow-up found that a SL-to-WL ratio of
approximately 4:1 minimized the incidence of
fascial dehiscence and incisional hernia
formation; this is where the surgical training
dictum of 1-cm ‘‘bites’’ followed by 1 cm of
progress originated.
Conclusion
• Important risk factors for abdominal wound dehiscence have been identified in the Rotterdam case-control study 2010 including:
• 1. age, • 2. gender • 3. chronic pulmonary disease, • 4.ascites, jaundice, anemia, emergency
surgery, type of surgery, coughing, and wound infection.

Conclusion
• 5.jaundice
• 6.anemia
• 7.emergency surgery
• 8.type of surgery
• 9.coughing
• 10.wound infection

Conclusion
• A number of factors for abdominal wound
dehiscence have been identified but the risk of developing abdominal wound dehiscence can be reduced by preventing pneumonia and
wound infection, and by applying optimal
surgical technique in every patient.

References
• Abdominal wound dehiscence in adults. Van Ramshorst et al. World J of Surg 2010;34:20-27.
• Prognostic models of wound dehiscence. Webster et al. J Surg Research 2003, 109: 130-137.
• The biology of acute wound failure. Dubay et al. Surg Clin North Am 2003,83:464-481