a systematic approach to chronic heart failure care: a ... heart failure care: ... care • nursing...
TRANSCRIPT

A systematic approach to chronic heart failure care: a consensus statement August 2013

2 A systematic approach to chronic heart failure care National Heart Foundation of Australia
ForewordThe Heart Foundation is determined to improve the quality of care received by people living with chronic heart failure. This condition continues to be a pressing problem in Australia, with indicators of poor case detection, discordant management, recurrent hospital admission and disconnected care. Further, the burden is disproportionately greater among the least advantaged populations in our society.
Mortality and hospital readmissions continue to rise, a trend that is likely to continue as the ageing population grows. Prognosis remains poor, often due to late diagnosis and inadequate disease management and support. The following statistics illustrate the extent of the problem:
• 20–30% of patients with mild to moderate heart failure will die within one year
• 50% of patients with severe heart failure will die within one year
• Aboriginal and Torres Strait Islander peoples experience chronic heart failure at a younger age and are more likely to die than non-Indigenous Australians
• costs are estimated to be more than $1 billion per annum.
This consensus statement identifies principles and action-based recommendations required to improve current systems across the chronic heart failure care continuum. We are calling upon governments, policy-makers, clinical networks and clinicians to address the core principles and recommendations through the development and implementation of a national policy framework. These consensus core principles and recommendations should be addressed in the various chronic heart failure systems of care operating across state and territory jurisdictions. There is an opportunity for significant positive change with limited investment.
This document has been developed through expert consensus; the insight, comment and advice provided is greatly valued. We also thank the many individuals and organisations that helped to make this consensus statement possible.
A systematic approach to chronic heart failure care continues the valuable leadership work of the Heart Foundation in seeking innovative solutions to the challenges of delivering better heart health outcomes across our Australian communities.
Dr Lyn Roberts AM Chief Executive Officer – National National Heart Foundation of Australia
Any queries regarding this document should be directed to: Rebecca Lee – Project Officer, Heart Care or Dr Karen Page – National Manager, Health Equity and Secondary Prevention National Heart Foundation of Australia Email: [email protected]
© 2013 National Heart Foundation of Australia ABN 98 008 419 761
This work is copyright. No part of this publication may be reproduced in any form or language without prior written permission from the National Heart Foundation of Australia (national office). Enquiries concerning permissions should be directed to [email protected].
ISBN 978-1-74345-056-7
PRO-150
Suggected citation: National Heart Foundation of Australia. A systematic approach to chronic heart failure care: a consensus statement. Melbourne: National Heart Foundation of Australia, 2013.
Disclaimer: This material has been developed by the Heart Foundation for general information. The statements and recommendations it contains are, unless labelled as ‘expert opinion’, based on independent review of the available evidence. While care has been taken in preparing the content of this material, the Heart Foundation and its employees cannot accept any liability, including for any loss or damage, resulting from the reliance on the content, or for its accuracy, currency and completeness. The information is obtained and developed from a variety of sources including, but not limited to, collaborations with third parties and information provided by third parties under licence. It is not an endorsement of any organisation, product or service. This material may be found in third parties’ programs or materials (including, but not limited to, show bags or advertising kits). This does not imply an endorsement or recommendation by the National Heart Foundation of Australia for such third parties’ organisations, products or services, including their materials or information. Any use of National Heart Foundation of Australia materials or information by another person or organisation is at the user’s own risk.
The entire contents of this material are subject to copyright protection.
3 National Heart Foundation of Australia A systematic approach to chronic heart failure care
ContentsList of figures . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
List of tables . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
Executive summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
Call to action . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
Recommendations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
Scope . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10 Purpose . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10 Policy context . . . . . . . . . . . . . . . . . . . . . . . . . 10Background . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
Definition of chronic heart failure. . . . . . . . . . 11 Symptoms of chronic heart failure . . . . . . . . . 11 Diagnosis of chronic heart failure. . . . . . . . . . 11 Heart failure classifications. . . . . . . . . . . . . . . 11 The chronic heart failure disease trajectory. . . 12Defining the problem: burden of disease . . . . . . . . . 13
Increasing incidence and prevalence . . . . . . . 13 Increasing mortality . . . . . . . . . . . . . . . . . . . . 13 Increasing hospital admissions . . . . . . . . . . . . 13 Hospital length of stay . . . . . . . . . . . . . . . . . . 14 Potentially preventable hospital admissions . . 14 Practice gaps . . . . . . . . . . . . . . . . . . . . . . . . . 15The way forward: principles and recommendations 16
Theme 1 Chronic heart failure care model . . . 17 Theme 2 Access to meaningful data for
management and benchmarking . . . . . . . . . . 20 Theme 3 Workforce planning . . . . . . . . . . . . . 22 Theme 4 Research . . . . . . . . . . . . . . . . . . . . . 23Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
Appendix 1 – Acknowledgements . . . . . . . . . . . . . . . 25
Appendix 2 – Methodology . . . . . . . . . . . . . . . . . . . . 26
Appendix 3 – New York Heart Association Functional Classification . . . . . . . . . . . . . . . . . . . . . . . 26
Glossary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
Definitions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30
List of figuresFigure 1 The typical trajectory of chronic heart failure . . . . . . . . . . . . . . . . . . . . . . . 12Figure 2 Heart failure hospital length of stay by country . . . . . . . . . . . . . . . . . . . . . . 14Figure 3 A framework for systems of chronic heart failure care recommendations. . . . . . . 16Figure 4 State and territory clinical cardiac networks: fostering better system of care. . . . . . . . . . 17Figure 5 Evidence-based guidelines for chronic heart failure and delivery of patient-centred multidisciplinary care. . . . . . . . . . . . 19
List of tablesTable 1 Themes, principles and action-based recommendations . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6

4 A systematic approach to chronic heart failure care National Heart Foundation of Australia
Executive summary
Chronic heart failure remains a major public health issue. Despite significant advances in management, prevalence remains high, clinical outcomes are poor and associated healthcare costs are rising. The management of chronic heart failure remains a pressing problem with many apparent indicators of poor case detection, discordant management, recurrent hospital admission and disconnected care.
On 24 April 2013, the National Heart Foundation of Australia hosted a Roundtable discussion to identify core principles and action-based recommendations required to ensure a systematic approach to heart failure care, which can inform policy and drive system change. The Improving Systems of Care for Chronic Heart Failure Roundtable* and associated stakeholder group included representatives from:
• state and territory cardiac and cardiovascular clinical networks
• Australian Commission on Safety and Quality in Health Care
• nursing and cardiology national peak bodies
• Cardiomyopathy Association of Australia Ltd.
The Roundtable and stakeholder consultation processes enabled consensus to be reached regarding the core principles and associated action-based recommendations that should underpin an optimal system of care for those with chronic heart failure. These core principles are categorised under four key themes:
• chronic heart failure care model
• access to meaningful data for management and benchmarking
• workforce planning
• research.
The Heart Foundation recommends that the core principles described within these consensus recommendations should underpin all system-based policy strategies to facilitate optimal chronic heart failure care. There is opportunity for significant positive change with limited investment.
This paper continues the valuable leadership work of the Heart Foundation in seeking innovative solutions to the challenges of delivering better heart health outcomes across our Australian communities.
Call to actionThe Heart Foundation calls upon governments, policy-makers, clinical networks and clinicians to:
Develop and implement a national policy framework with agreement between states, territories and the federal government addressing the core principles and recommendations described in this consensus document .
These consensus core principles and recommendations should be addressed in the various chronic heart failure systems of care operating across state and territory jurisdictions .
*Roundtable Discussion: Improving Systems of Care for Chronic Heart Failure. National Heart Foundation, 500 Collins St, Melbourne, Victoria. 24 April 2013 (Appendix 1 for list of attendees)

5 National Heart Foundation of Australia A systematic approach to chronic heart failure care
RecommendationsThe core principles and action-based recommendations (Table 1) are those required to ensure a systematic approach to heart failure care that will lead to improved health outcomes; specifically event-free survival (a composite of the number of emergency presentations, hospitalisations and premature deaths). A national policy framework that incorporates these principles and recommendations, with agreement between states, territories and the federal government could see significant improvements in event-free survival and associated costs for both the individual and community.
They have been grouped under four themes:
• chronic heart failure care model
• access to meaningful data for management and benchmarking
• workforce planning
• research.
These principles and action-based recommendations have been identified through a consensus process, which included the Improving Systems of Care for Chronic Heart Failure Roundtable and stakeholder consultation, and are summarised in Table 1.
6 A systematic approach to chronic heart failure care National Heart Foundation of Australia
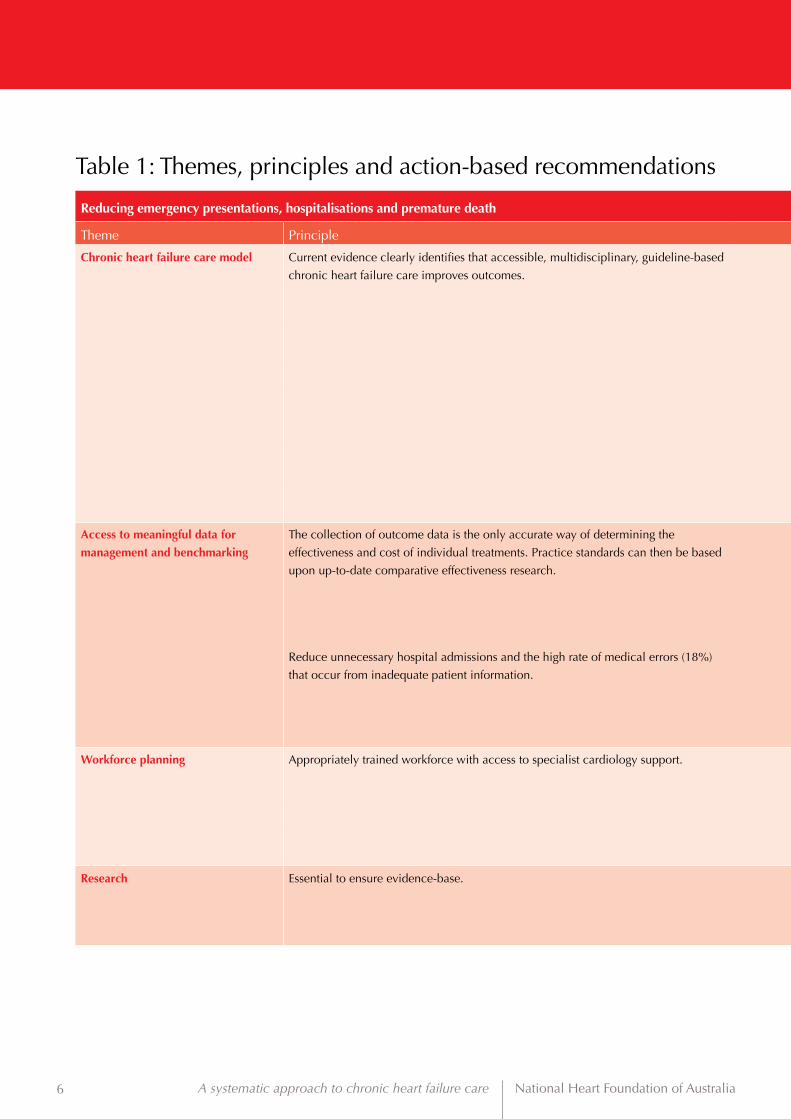
Table 1: Themes, principles and action-based recommendations
Reducing emergency presentations, hospitalisations and premature death
Theme Principle Action-based recommendation
Chronic heart failure care model Current evidence clearly identifies that accessible, multidisciplinary, guideline-based
chronic heart failure care improves outcomes.
1. Support health departments through state and territory clinical networks to continue leading the development of
integrated local care systems and future national quality improvement strategies within and across health services.†
2. Mechanisms to champion the uptake of clinical practice guidelines and delivery of integrated chronic heart failure
services, according to local population need, should be identified and implemented within and across health services.†
3. Develop minimum standards for chronic heart failure multidisciplinary care, which can be used to accredit health
services and recognise best practice health services or networks.
4. Develop robust funding models and examine the role of funded care packages in chronic heart failure care.
5. Establish system protocols and pathways to ensure effective clinical handover and service coordination across care
transitions, and activate appropriate services according to clinical need for an exacerbation, emergency presentation,
hospitalisation or palliation.
6. Streamline care processes to facilitate early diagnosis, self-management, multidisciplinary care planning, including
primary care involvement, and appropriate access to palliative services.
7. Embed mechanisms to promote the rights of the individual/carer to facilitate their active engagement with health
professionals and care systems.
Access to meaningful data for
management and benchmarking
The collection of outcome data is the only accurate way of determining the
effectiveness and cost of individual treatments. Practice standards can then be based
upon up-to-date comparative effectiveness research.
8. Develop national data definitions for chronic heart failure.
9. Expand current cardiac registries, to include those with chronic heart failure.
10. Develop mechanisms to promote data linkage across care transitions.
11. Trial the Personally Controlled e-Health Record (PCeHR) for those diagnosed with chronic heart failure so all current and
future healthcare providers could, with the individual’s consent, have access to the same information where and when
they need it.
Reduce unnecessary hospital admissions and the high rate of medical errors (18%)
that occur from inadequate patient information.
12. Use 12-month event-free survival nationally as an outcome measure to evaluate effectiveness of care systems. Events
would include emergency presentations, hospitalisations and premature death.
13. Establish a national mechanism for monitoring and reporting chronic heart failure care outcomes against a nationally
recognised set of goals and standards.
14. Develop a national set of indicators and standards to evaluate, inform and improve systems of care.
Workforce planning Appropriately trained workforce with access to specialist cardiology support. 15. Develop workforce capacity across health services† to deliver evidence-based care, appropriate to the local population,
as identified in Guidelines for the prevention, detection and management of chronic heart failure in Australia1, 2 and
Multidisciplinary care for people with chronic heart failure.3
16. Develop robust funding models for the delivery of these services.
17. Examine mechanisms to empower general practitioners and healthcare professionals in primary care to deliver evidence
based care for chronic heart failure.
Research Essential to ensure evidence-base. 18. Create investigative teams, such as clinical chronic heart failure research networks, with active consumer collaboration.
19. Investigate approaches to optimise care delivery in Aboriginal and Torres Strait Islander peoples, those from non-
metropolitan areas, those with lower socio-economic backgrounds, and culturally and linguistically diverse (CALD)
populations.

7 National Heart Foundation of Australia A systematic approach to chronic heart failure care
Table 1: Themes, principles and action-based recommendations
Reducing emergency presentations, hospitalisations and premature death
Theme Principle Action-based recommendation
Chronic heart failure care model Current evidence clearly identifies that accessible, multidisciplinary, guideline-based
chronic heart failure care improves outcomes.
1. Support health departments through state and territory clinical networks to continue leading the development of
integrated local care systems and future national quality improvement strategies within and across health services.†
2. Mechanisms to champion the uptake of clinical practice guidelines and delivery of integrated chronic heart failure
services, according to local population need, should be identified and implemented within and across health services.†
3. Develop minimum standards for chronic heart failure multidisciplinary care, which can be used to accredit health
services and recognise best practice health services or networks.
4. Develop robust funding models and examine the role of funded care packages in chronic heart failure care.
5. Establish system protocols and pathways to ensure effective clinical handover and service coordination across care
transitions, and activate appropriate services according to clinical need for an exacerbation, emergency presentation,
hospitalisation or palliation.
6. Streamline care processes to facilitate early diagnosis, self-management, multidisciplinary care planning, including
primary care involvement, and appropriate access to palliative services.
7. Embed mechanisms to promote the rights of the individual/carer to facilitate their active engagement with health
professionals and care systems.
Access to meaningful data for
management and benchmarking
The collection of outcome data is the only accurate way of determining the
effectiveness and cost of individual treatments. Practice standards can then be based
upon up-to-date comparative effectiveness research.
8. Develop national data definitions for chronic heart failure.
9. Expand current cardiac registries, to include those with chronic heart failure.
10. Develop mechanisms to promote data linkage across care transitions.
11. Trial the Personally Controlled e-Health Record (PCeHR) for those diagnosed with chronic heart failure so all current and
future healthcare providers could, with the individual’s consent, have access to the same information where and when
they need it.
Reduce unnecessary hospital admissions and the high rate of medical errors (18%)
that occur from inadequate patient information.
12. Use 12-month event-free survival nationally as an outcome measure to evaluate effectiveness of care systems. Events
would include emergency presentations, hospitalisations and premature death.
13. Establish a national mechanism for monitoring and reporting chronic heart failure care outcomes against a nationally
recognised set of goals and standards.
14. Develop a national set of indicators and standards to evaluate, inform and improve systems of care.
Workforce planning Appropriately trained workforce with access to specialist cardiology support. 15. Develop workforce capacity across health services† to deliver evidence-based care, appropriate to the local population,
as identified in Guidelines for the prevention, detection and management of chronic heart failure in Australia1, 2 and
Multidisciplinary care for people with chronic heart failure.3
16. Develop robust funding models for the delivery of these services.
17. Examine mechanisms to empower general practitioners and healthcare professionals in primary care to deliver evidence
based care for chronic heart failure.
Research Essential to ensure evidence-base. 18. Create investigative teams, such as clinical chronic heart failure research networks, with active consumer collaboration.
19. Investigate approaches to optimise care delivery in Aboriginal and Torres Strait Islander peoples, those from non-
metropolitan areas, those with lower socio-economic backgrounds, and culturally and linguistically diverse (CALD)
populations.
†The term health services is inclusive of area health services, local hospital networks, primary care, Aboriginal community controlled health organisations, aged care services and other appropriate agencies

8 A systematic approach to chronic heart failure care National Heart Foundation of Australia
Introduction
Chronic heart failure, the inability of the heart to provide adequate circulation, is a well recognised highly symptomatic syndrome and a major public health issue. Despite significant advances in management, clinical outcomes are poor and associated healthcare costs are high. In industrialised countries, chronic heart failure affects 2–3% of the population with rates steeply increasing to over 23% in those aged over 65 years.4 Overall prevalence is likely to increase as the population ages; cardiovascular disease survival rates continue to improve; and the prevalence of risk factors continues to increase.
Every year, an estimated 30,000 Australians receive a diagnosis of chronic heart failure.5 More than 45,000 Australians were hospitalised due to chronic heart failure in 2009–2010, equating to over 360,000 bed days.6 The cost of chronic heart failure in Australia has been estimated at over $1 billion per year.7
The management of chronic heart failure remains a pressing problem with many apparent indicators of poor case detection, discordant management, recurrent hospital admission and disconnected care. Additional indications suggest these issues are amplified among marginalised populations.
Heart failure is 1.7 times more common among Aboriginal and Torres Strait Islander peoples than other Australians, and occurs at a younger age.8 Aboriginal and Torres Strait Islander peoples are also significantly more likely to die from heart failure than other Australians.8
There is a higher prevalence of heart disease and risk factor burden among those in non-metropolitan and lower socio-economic areas.9
Best-practice management of chronic heart failure involves multidisciplinary care across the acute and primary care sectors. There is convincing evidence that, among people who have been hospitalised with chronic heart failure, those who receive evidence-based multidisciplinary care have better health outcomes than those who do not.10,11 The key recommendations in the Heart Foundation’s Guidelines for the prevention,
detection and management of chronic heart failure in Australia,12 Multidisciplinary care for people with chronic heart failure,3 and associated consumer documents and resources articulate which evidence-based practices are required to improve care outcomes.
Currently systems of care for those with chronic heart failure and uptake of both best practice guidelines, including the multidisciplinary care recommendations, are very reliant upon the local context and existence of clinical leaders. This approach has meant service development remains very ad-hoc, with considerable heterogeneity across the nation in terms of service type and accessibility. Standards of practice do not currently exist to guide service delivery, so reporting mechanisms and databases tend to be very embryonic and lacking infrastructure to: accurately identify incidence and prevalence; enable outcome monitoring to facilitate national and international benchmarking; and facilitate patient recall.
Broadly speaking, a ‘system-based’ approach to chronic heart failure can be defined as a coordinated and seamless series of activated events which transcend traditional service-delivery boundaries, thereby encompassing the system-based principles of synergy, integration, collaboration and networks.13 The effectiveness of a system of care is significantly influenced by the following variables:13
• leadership, support and guidance from health departments through state and territory clinical networks, area health services, local hospital networks, primary care, Aboriginal community controlled health organisations, aged care services and other agencies
• communication processes between services
• collaboration across service boundaries
• effective discharge planning
• ability to monitor and report outcomes.
Some regions within Australia are currently operating effective systems of care for chronic heart failure, guided by cardiac-focused clinical networks and championed by clinical leaders at the practice level.

9 National Heart Foundation of Australia A systematic approach to chronic heart failure care
Case study 1
Leon is 69 years old, and a year ago he had a heart attack whilst playing golf. Since then he has experienced increasing breathlessness and has noticed swelling of his ankles. He no longer accompanies Ella, his wife, on their shopping trips and has found himself increasingly reluctant to leave their house. Leon and Ella visited their general practitioner (GP), who referred Leon to the cardiologist for further investigations. It was established that Leon had significant heart failure, requiring a new medication regime, insertion of a pacemaker and education to help him manage his heart failure.
Leon was referred to a 10-week heart failure rehabilitation program, and Ella was encouraged to attend with him. During this program they received: physiotherapy-guided exercise; nurse-led education; vital medication information from the pharmacist; and psychologist support to manage their anxieties. Leon’s GP received a discharge summary from the cardiology team clearly identifying his care requirements and the need for titrating his medication. The summary also included information on how to contact the heart failure nurse consultant.
Leon now weighs himself daily and maintains a stable weight. He knows to contact his heart failure nurse if he experiences an increase in weight or becomes breathless. Leon has returned to playing 18 holes of golf at least once each week.
Case study 2
Margaret, an active 75-year-old, was diagnosed with heart failure following an admission for breathlessness. She had uncontrolled hypertension and had experienced two prior heart attacks. Her cardiologist commenced a new medication regimen that required gradual titration by her GP. Margaret was also referred to a heart failure rehabilitation program that was 20 kilometres from her home and not accessible by public transport. Unfortunately, Margaret’s medication regimen was not titrated by her GP and she was unable to attend the rehabilitation program as she did not drive.
Within six months of diagnosis, Margaret had been admitted to hospital four times, with her last visit leaving her feeling very emotional and vulnerable. Following discharge, she saw her GP who had not received any information regarding her hospital admissions and ongoing care requirements. Margaret did not tell her GP that she was not coping and was concerned as to how much longer she could live independently. Within 12 months Margaret died in hospital, following several admissions.

10 A systematic approach to chronic heart failure care National Heart Foundation of Australia
ScopeThis paper identifies principles and action-based recommendations required to improve current systems across the chronic heart failure care continuum. These recommendations have been informed by the current literature and input from a range of experts through the Systems of Care for Chronic Heart Failure Roundtable and stakeholder consultation. This process is described in Appendix 2.
These priority recommendations are not exhaustive and many other changes and actions can be implemented to improve care outcomes for both individuals and organisations.
PurposeThese principles and priority action-based recommendations have been developed to inform a national policy framework with agreement between states, territories and the federal government. The aim is to empower healthcare providers and organisations, peak and government organisations, care regulators, education providers, and consumers to improve health outcomes for chronic heart failure and reduce harm.
Policy contextCardiovascular disease is one of the nine national health priority areas (NHPAs) that Australian Governments have chosen for focused attention due to significant levels of disease burden and injury in the Australian community. Chronic heart failure is responsible for much of this burden with high rates of hospitalisation, morbidity and mortality.7
The principles and recommendations for improving systems of care for chronic heart failure outlined in this document are aligned with the key areas of healthcare system reform identified by the National Healthcare Agreement.14 These are:
• tackling major access and equity issues affecting health outcomes
• redesigning the health system so that it is better positioned to respond to emerging challenges
• creating an agile and self-improving health system for long-term sustainability.
Under the standards associated with healthcare system reform it is clearly articulated that:
• everyone has the right to be able to access healthcare to address their healthcare needs and this right is essential
• the clinical workforce is guided by current best practice and uses clinical guidelines that are supported by the best available evidence
• managers and the clinical workforce have the right qualifications, skills and approach to provide safe, high-quality healthcare.
In addition, they address the objectives of the Rural Primary Health Services (RPHS) program,15 which are to:
• provide and maintain access to supplementary allied health and primary care services that are based on identified health needs in each community
• promote coordinated, multidisciplinary team-based approaches to the provision of integrated primary healthcare services
• establish and maintain effective community consultation practices for the planning, management, flexible delivery and ongoing review of the RPHS program
• provide and maintain access to relevant health promotion and preventative health programs and activities designed to promote health and wellbeing
• encourage people in rural and remote Australia to adopt or modify behaviours to better manage their health and wellbeing.

11 National Heart Foundation of Australia A systematic approach to chronic heart failure care
Background
Definition of chronic heart failureHeart failure is a complex clinical syndrome characterised by high mortality, frequent hospitalisation and reduced quality of life for the individual and their carer.16 Underlying structural abnormality or cardiac dysfunction impairs the ability of the heart to fill or eject blood. This can be caused by ischaemic heart disease, hypertension and idiopathic dilated cardiomyopathy.2
The term chronic is now widely used to describe heart failure where abnormalities of contraction or relaxation have been present for a prolonged period and there is ventricular remodelling.17 Irreversible myocardial damage is present but symptoms can be controlled to optimise the individual’s quality of life.5
Symptoms of chronic heart failure The symptoms of chronic heart failure are important as they are very debilitating, highlight significant deterioration in heart function, and are responsible for individuals presenting to hospital. Breathlessness, fatigue, and ankle swelling are the hallmarks of chronic heart failure.18,19
Individuals experience rapid, shallow breathing accompanied by a terrifying feeling of not being able to obtain enough air.17 This breathlessness commonly occurs when gravitational forces have less effect, such as whilst lying down or upon exertion.17 Increased venous congestion and pressure in the pulmonary capillaries causes fluid to leach into the interstitial lung space, reducing lung compliance and increasing the respiratory muscles’ workload with an associated rise in oxygen demand.20 The sense of fatigue is overwhelming, reducing the enjoyment of day-to-day activities.21 Ankle swelling is caused by the increased systemic pressures, which precipitate the leakage of fluid into the peripheral tissue. Peripheral oedema accumulates in the lower extremities, normally feet and ankles, due to gravity.
Other common symptoms Other common symptoms associated with chronic heart failure are due to increasing systemic pressure and include anorexia, nausea and swelling (oedema) to thighs, genitalia and the abdominal wall. A tachycardia and other cardiac arrhythmias may occur due to the increased circulating catecholamines.22 The abnormal sleep patterns and impaired tissue perfusion can produce dizziness, restlessness, agitation and confusion.17
Diagnosis of chronic heart failureDespite an awareness of chronic heart failure symptoms, diagnosis can still be difficult. The symptoms are not specific to chronic heart failure and have many differential diagnoses. Generally initial diagnosis is based on clinical signs and symptoms, followed by a confirmatory echocardiogram providing objective evidence of structural abnormality and/or cardiac dysfunction.18,23
Due to the many difficulties surrounding the diagnosis of chronic heart failure, many cases go undiagnosed24-26 with many individuals only diagnosed when the disease is well advanced.24,27,28
Heart failure classifications Once heart failure is diagnosed, it is generally classified as left ventricular systolic dysfunction or heart failure with preserved systolic function. Precise classification can be difficult, as those with preserved systolic function frequently have a degree of systolic failure.18,22 At present, an echocardiograph is necessary to differentiate between systolic dysfunction and heart failure with preserved systolic function.
Left ventricular systolic dysfunction Left ventricular systolic dysfunction occurs when the contractility of the left ventricle is impaired and the amount of blood ejected with each beat is reduced.29 There is ineffectual emptying of the venous system resulting in elevation of the systemic and pulmonary pressures. Blood flow is restricted and fluid accumulates in the lungs, liver, gastrointestinal tract and extremities.

12 A systematic approach to chronic heart failure care National Heart Foundation of Australia
Heart failure with preserved systolic functionHeart failure with preserved systolic function, previously known as diastolic heart failure, is usually asymptomatic. The underlying mechanism is thought to be impaired left ventricular relaxation.30 The left ventricular wall thickens reducing ventricular size and compliance impairing ventricular filling and reducing stroke volume.31 The main causes are those associated with ageing: chronic hypertension; ventricular hypertrophy; diabetes;31 and acute coronary syndrome.32
New York Heart Association Functional ClassificationOnce chronic heart failure is classified, a measure of severity is useful. The most widely used measure of severity is the New York Heart Association Functional Classification (Appendix 3).33-35 This functional classification is divided into four classes and enables the effect on daily activities to be quantified by an observer.36 Whilst the New York Heart Association classification is useful, central to the delivery of high quality, cost effective care is a better understanding of the nature of advanced heart failure and, in particular, the end of life phase.37
The chronic heart failure disease trajectoryThe trajectory of chronic heart failure (Figure 1) is comparable to other clinical populations where there is progressive organ failure such as kidney disease; and even to some cancers. However, the course of heart failure is very variable and difficult to predict, and therefore no specific trajectory can be reliably anticipated.37 Clinical deterioration and/or death may occur at any time. Goodlin (2009) has described the five phases of heart failure.37
Phase 1 represents symptom onset, diagnosis and initiation of medical treatment. The individual generally presents to the emergency department with severe breathlessness. Some may even die at this first presentation. For others, symptom onset is more gradual, and they may present to the general practitioner with increasing breathlessness and fluid retention. Evidence based treatment produces a dramatic improvement in
symptoms. During this phase, education on the nature of chronic heart failure and available treatment options is beneficial, as is advice on diet and fluid management strategies. At this point individuals can enter a plateau period of variable duration for several years.
Phase 2 is a stable period when individuals feel well and are generally under the care of their general practitioner. Education focuses on how to monitor their chronic heart failure at home and when to call for help. Autonomy, self-care and adherence to therapy are encouraged.
Phase 3 features periods of instability due to symptom reoccurrence as heart function further deteriorates. Optimising therapies can improve symptoms. However new therapies such as implantable cardiac devices, which improve heart pump performance (cardiac resynchronisation therapy), might be required.
Phase 4 occurs as symptoms increase and are associated with declining physical capacity, despite optimal therapy.
Phase 5 involves marked deterioration and increasing symptoms. Assessment of supportive and palliative care needs is required and specialist palliative care may need to be involved. Review of resuscitation status and reprogramming of cardiac devices may be important management issues, as when the patient enters the terminal phase the situation often progresses rapidly.
Figure 1 The typical trajectory of chronic heart failure
Diagnosis
Supportive and palliative care
Responding to treatment
Clinical instability
Poor response to treatment
Death
Sudden death eventTransplant or ventricular assist device
Time
Phys
ical
func
tion
End of life care
1
23
45
Modified from Goodlin SJ. Palliative care in congestive heart failure. J Am Coll Cardiol 2009; 54(5):386–396. Used with permission from Elsevier.
13 National Heart Foundation of Australia A systematic approach to chronic heart failure care
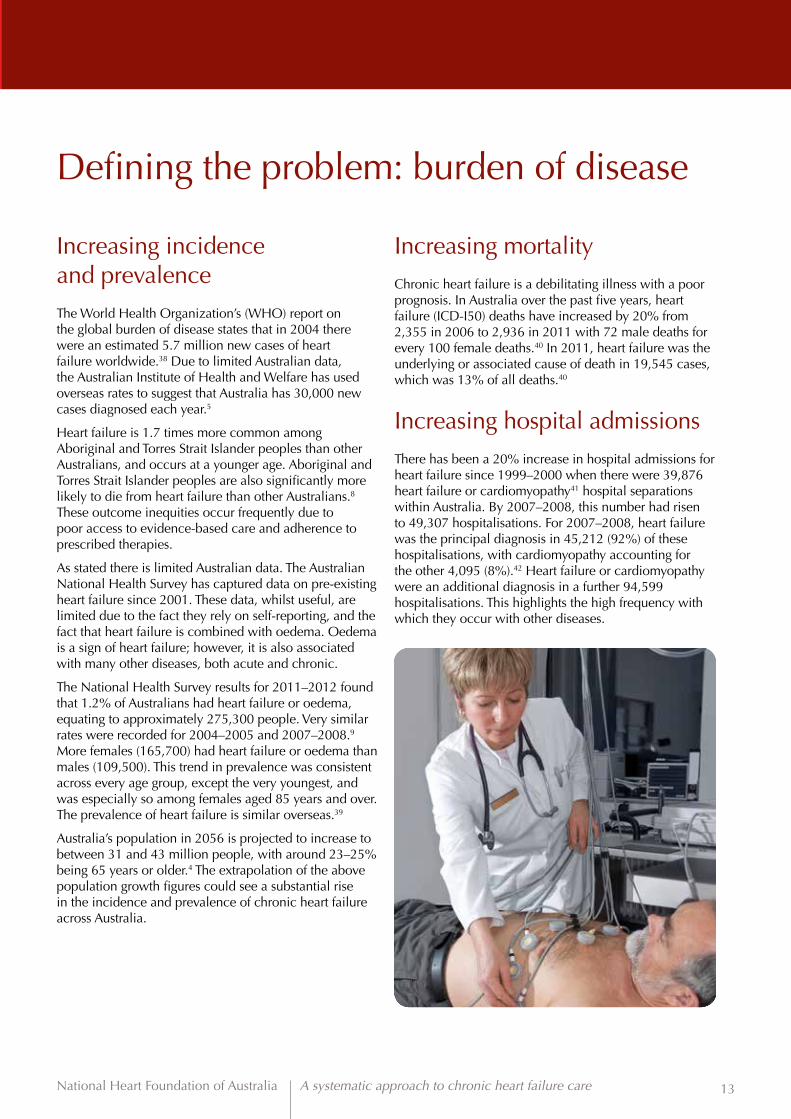
Defining the problem: burden of disease
Increasing incidence and prevalenceThe World Health Organization’s (WHO) report on the global burden of disease states that in 2004 there were an estimated 5.7 million new cases of heart failure worldwide.38 Due to limited Australian data, the Australian Institute of Health and Welfare has used overseas rates to suggest that Australia has 30,000 new cases diagnosed each year.5
Heart failure is 1.7 times more common among Aboriginal and Torres Strait Islander peoples than other Australians, and occurs at a younger age. Aboriginal and Torres Strait Islander peoples are also significantly more likely to die from heart failure than other Australians.8 These outcome inequities occur frequently due to poor access to evidence-based care and adherence to prescribed therapies.
As stated there is limited Australian data. The Australian National Health Survey has captured data on pre-existing heart failure since 2001. These data, whilst useful, are limited due to the fact they rely on self-reporting, and the fact that heart failure is combined with oedema. Oedema is a sign of heart failure; however, it is also associated with many other diseases, both acute and chronic.
The National Health Survey results for 2011–2012 found that 1.2% of Australians had heart failure or oedema, equating to approximately 275,300 people. Very similar rates were recorded for 2004–2005 and 2007–2008.9 More females (165,700) had heart failure or oedema than males (109,500). This trend in prevalence was consistent across every age group, except the very youngest, and was especially so among females aged 85 years and over. The prevalence of heart failure is similar overseas.39
Australia’s population in 2056 is projected to increase to between 31 and 43 million people, with around 23–25% being 65 years or older.4 The extrapolation of the above population growth figures could see a substantial rise in the incidence and prevalence of chronic heart failure across Australia.
Increasing mortality Chronic heart failure is a debilitating illness with a poor prognosis. In Australia over the past five years, heart failure (ICD-I50) deaths have increased by 20% from 2,355 in 2006 to 2,936 in 2011 with 72 male deaths for every 100 female deaths.40 In 2011, heart failure was the underlying or associated cause of death in 19,545 cases, which was 13% of all deaths.40
Increasing hospital admissionsThere has been a 20% increase in hospital admissions for heart failure since 1999–2000 when there were 39,876 heart failure or cardiomyopathy41 hospital separations within Australia. By 2007–2008, this number had risen to 49,307 hospitalisations. For 2007–2008, heart failure was the principal diagnosis in 45,212 (92%) of these hospitalisations, with cardiomyopathy accounting for the other 4,095 (8%).42 Heart failure or cardiomyopathy were an additional diagnosis in a further 94,599 hospitalisations. This highlights the high frequency with which they occur with other diseases.

14 A systematic approach to chronic heart failure care National Heart Foundation of Australia
Hospital length of stayThe average hospital length of stay for heart failure is five days within the public sector and up to eight days within the private sector.6 This equates to 394,456 bed days annually where heart failure is the principal diagnosis, based on 2007–2008 figures. The 2006–2007 average cost of a hospital admission in Victoria for simple heart failure (diagnostic-related group 62B) and complex heart failure (diagnostic-related group 62A) was $3,440 and $7,260, respectively.43 Based on these figures the total costs where heart failure is a principal diagnosis are between A$15 million and A$33 million per annum in Australia.
Hospital length of stay for Aboriginal and Torres Strait Islander peoples appears to be shorter compared to non-Indigenous people. This may be due to a higher proportion of hospitalisations ending in discharge against medical advice, or a lack of cultural safety and competency in the hospital environment.44
The Organisation for Economic Co-operation and Development (OECD) collects, collates and reports on international health data. Its 2009 release reported the average length of stay (ALOS) for a number of conditions, including heart failure (Figure 2). Despite being lower than most of Europe, Australia’s length of stay trends appear to have changed little over the 10 years of the report, with a fair way to go before reaching the lengths of stay of Sweden and the USA.
Figure 2 Heart failure hospital length of stay by country
Modified from Organisation for Economic Co-operation and Development. OECD health data 2009: statistics and indicators for 30 countries. Paris: OECD, 2009.
In terms of cost savings, generally a shorter length of stay is preferable. However, some recent studies have demonstrated that a longer initial length of stay is associated with a lower readmission rate.45
Potentially preventable hospital admissionsA significant proportion of hospital readmissions are due to chronic heart failure.24,46,47 The reported rates for readmission with chronic heart failure are between 29 and 49%, within three to six months of initial discharge.46,48,49 Data from the Euro Heart Survey II on patients hospitalised with chronic heart failure revealed that one quarter (24%) of patients had been re-admitted within 12 weeks of discharge and 14% of patients died between admission and 12 weeks follow-up.50
In many instances, these admissions were preventable and therefore avoidable. Chronic heart failure has been recognised nationally as a potentially avoidable hospitalisation; “an admission to hospital that could have potentially been prevented through the provision of appropriate non-hospital health services”.14 Currently, on a national basis there is limited available data, and the data that is available is from Victoria. It highlights that readmissions within 30 days of discharge can be as high as 20%.51
Among Aboriginal and Torres Strait Islander peoples, potentially preventable hospitalisations for heart failure are three times higher than among non-Indigenous Australians.14 These higher rates reflect the prevalence of chronic conditions in the population and the need to strengthen services that provide earlier prevention, detection and management.
Given the high rate of readmissions, systems change to improve care quality can have a substantial impact on cost and individual quality of life.52,53 The management of chronic heart failure remains a pressing problem, with many apparent indicators of poor case detection, including discordant management with evidence-based treatment, recurrent hospital admission, and disconnected care. Additional indications suggest these issues are amplified among marginalised populations.
19970
2
4
6
8
10
Day
s
12
14
16
1998 1999 2000 2001 2002 2003 2004 2005 2006 2007USAUK Germany France Canada SwedenAustralia

15 National Heart Foundation of Australia A systematic approach to chronic heart failure care
Practice gapsBest-practice management of chronic heart failure involves multidisciplinary care irrespective of heart failure classification. In terms of disease severity most of the evidence is for New York Heart Association Class III and IV.11 There is convincing evidence that, among people who have been hospitalised with chronic heart failure, those who receive multidisciplinary care have better health outcomes than those who do not. The Heart Foundation’s multidisciplinary care resource released in 2010, advocated for improvements in the delivery of this form of care.3
An evidence review and issues paper54 developed prior to the Improving Systems of Care for Chronic Heart Failure Roundtable found that appropriate diagnosis, treatment and ongoing support can improve quality of life and reduce mortality and morbidity. However, recent studies have highlighted significant variations in access to evidence-based care.55,56
It is recognised that many individuals are not diagnosed in a timely manner, and once a diagnosis is made, treatment is frequently sub-optimal. Diagnostic delay is frequently due to under-recognition of early heart failure symptoms by people with chronic heart failure and their health professionals. This results in a large proportion of individuals being diagnosed at a hospital presentation requiring an admission, despite having had symptoms for many months.
This is compounded by a limited capacity to perform public echocardiography. The limited availability of public sector services results in the bulk of echocardiography being undertaken in the private sector. Additionally, echocardiography results are not shared across health services, leading to duplication of investigations.
Any care system should be focused on delivering evidence-based care to all those with, and at risk of, chronic heart failure irrespective of geographical location, socio-economic status and cultural background. Care needs to be delivered systematically to ensure access to all for appropriate and coordinated care. Delivery of care on a systematic basis ensures that it is structured and clearly defined, enabling clarity around the care required. This ensures individuals can be tracked and activities audited for quality improvement.
Models of care for those with chronic heart failure need to be person-centred and systematic to ensure those at high risk, or with established chronic heart failure, are identified in a timely manner. In addition, care delivery needs to be documented and evidence-based, with access and mechanisms for review. The Heart Foundation produces a number of chronic heart failure resources for consumers.57,58 These are designed to help people with chronic heart failure better understand and manage their condition. They also assist health professionals to discuss symptom management, lifestyle changes, medicines and other treatments and complications. These resources have been implemented throughout Queensland’s state-wide service.
Care delivery varies across Australia. Recommendations for chronic disease management must be flexible to enable their implementation in a diverse range of delivery models according to local needs, resources and individual preferences. Frequently there is outreach to the community from hospital, but limited opportunities for valuable in-reach communication from the community to the hospital.
International experience shows that effective person-centred multidisciplinary chronic heart failure care can be implemented in a range of clinical settings and using a range of delivery models, including home-based, clinic-based and telephone-based approaches, or a hybrid of these. Care pathways should include culturally-appropriate discussions with the individual and their carer which highlight chronic heart failure as an illness that will shorten their life expectancy. These discussions can occur at the point of diagnosis, and be re-visited throughout their journey with heart failure. There is also the need for end-of-life care planning.
The priority action-based recommendations associated with a systematic approach to chronic heart failure are summarised over the page.

16 A systematic approach to chronic heart failure care National Heart Foundation of Australia
The way forward: principles and recommendations
The recommendations have been grouped under four themes: chronic heart failure care model; access to meaningful data for management and benchmarking; workforce planning; and research to facilitate person-centred evidence-based care delivery for the symptomatic patient, reducing the likelihood of emergency presentations, hospitalisations and premature death (Figure 3).
Data
Research
W
orkfor
ce
Care
mod
el
Evidence-based care Patient-centred care
Emer
genc
y pr
esen
tation
s Rehospitalisations and premature death
Palpitations/syncope Paroxysmal nocturnal dyspnoea Fatigu
e Oed
ema
Dys
pnoe
a O
rthop
noea
Patient
Policy
Figure 3 A framework for systems of chronic heart failure care recommendations
These action-based recommendations have been developed for consideration by governments and healthcare providers. They are not exhaustive and many other changes and actions can be implemented to improve care outcomes by both individuals and organisations. They are generally broad, rather than prescriptive, and many can be implemented with minimal resourcing. Implementing these recommendations would improve the quality of care provided to individuals with chronic heart failure, reducing associated costs both for the individual and community alike.
Patient symptoms

17 National Heart Foundation of Australia A systematic approach to chronic heart failure care
Theme 1 Chronic heart failure care model
Principle:
• Current evidence clearly identifies that accessible, multidisciplinary, guideline-based chronic heart failure care improves outcomes.
Within Australia cardiac and chronic disease clinical networks exist across a number of jurisdictions (Figure 4). State-based health departments have established these networks to provide strategic direction, clinical governance and leadership, and improve collaboration. Depending on the priorities and resources available in each state, multidisciplinary networks are also involved in the development of cardiac capability frameworks, facilitation of registry development, service mapping including directories, research, training, and areas of new technology. The networks have significant influence in improving care systems and resulting outcomes. They can facilitate improvements in chronic heart failure care by:
• fostering awareness, communication and partnerships across service delivery boundaries (emergency, cardiology, primary healthcare organisations e.g. Medicare Locals)
• providing governments with advice regarding state-wide planning, policy and clinical reforms, including capability frameworks
• promoting links between rural, remote and metropolitan health services
• engaging and supporting clinical leaders to implement evidence-based care
• challenging current processes and structures
• facilitating information exchange across clinical networks.
Figure 4 State and territory clinical cardiac networks: fostering better systems of care
WA Cardiovascular Health Network
NT (Network currently in development)
QLD State-wide Cardiac Clinical Network
NSW Agency for Clinical Innovation – Cardiac Network
VIC Cardiac Clinical Network
SA State-wide Cardiology Network and Integrated Cardiovascular Clinical Network CHSA
Recommendation 1
Support health departments through state and territory clinical networks to continue leading the development of integrated local care systems and future national quality improvement strategies within and across health services.**
Recommendation 2
Mechanisms to champion the uptake of clinical practice guidelines and delivery of integrated chronic heart failure services, according to local population need, should be identified and implemented within and across health services.**
**The term health services is inclusive of area health services, local hospital networks, primary care, Aboriginal community controlled health organisations, aged care services and other appropriate agencies

18 A systematic approach to chronic heart failure care National Heart Foundation of Australia
Best-practice management of chronic heart failure involves evidence-based multidisciplinary care, which is patient centred. It is generally agreed that patient-centred care is respectful of, and responsive to, preferences, needs and values of patients and consumers. Patient-centred care should include dimensions of respect, emotional support, physical comfort, information and communication, care coordination, involvement of family and carers, and access to care. A definition for patient centred care, which satisfies these criteria, is:
“A patient-centred care system is one where patients can move freely along a care pathway without regard to which physician, other healthcare provider, institution or community resource they need at that moment in time. The system is one that considers the individual needs of patients and treats them with respect and dignity.”59
Frequently, planning for multidisciplinary care takes place within the broader context of chronic disease management. It is defined as the provision of person centred care in which health services work with each other and the client to ensure coordination, consistency and continuity of care over time and through the different stages of their condition.60-62
Multidisciplinary chronic heart failure care is distinguishable from generic chronic disease management programs by the special needs of patients with chronic heart failure (e.g. ongoing medicines titration, symptom monitoring and management of devices), which necessitates specialised evidence-based treatment strategies associated with optimal outcomes. Accordingly, effective chronic heart failure care often requires access to specialised knowledge and expertise.
Multidisciplinary care delivery needs to be flexible to enable delivery according to local needs, resources, patient preferences and disease trajectory phase.54 International and national experience shows that effective multidisciplinary chronic heart failure care can be cost-effective and implemented in a range of clinical settings using a range of delivery models, including home-based, clinic-based and telephone-based approaches, or a hybrid of these approaches.3,13 This enables local variations depending on geographical location and cultural background.
Chronic heart failure management plans, including care pathways, are vital to educate and empower the individual and their carer/family to manage this challenging condition.63-65 These plans should take a multidisciplinary approach and be clear about responsibilities among healthcare providers. Enrolment in an evidence-based management program will enhance the role of the care plan in managing chronic heart failure. There has been a rapid expansion of structured multidisciplinary chronic heart failure management programs in Australia.66
However, ensuring access to these programs for all those who would benefit remains a challenge, especially among Aboriginal and Torres Strait Islander peoples, those from non-metropolitan areas, those with lower socio-economic backgrounds, and culturally and linguistically diverse populations.67
Improvements are seen not only in care experienced by patients and their families, but as clinical and operational benefits as well. Implementation of patient-centred care approaches can shorten lengths of stay reducing healthcare costs and improving clinician and patient satisfaction.68-72 In the longer term, other benefits of patient-centred care include reduced emergency department return visits, fewer medication errors, higher functional status, and improved clinical care.73-75 There is convincing evidence that, among people who have been hospitalised with chronic heart failure, those who receive patient centred multidisciplinary care have better health outcomes than those who do not.76
Importantly in Australia we already have developed evidence-based guidelines for chronic heart failure care and delivery of patient centred multidisciplinary care.2,3,12 These resources afford the opportunity to examine whether care is evidence based and provide tools to support and enable practice to be evaluated.

19 National Heart Foundation of Australia A systematic approach to chronic heart failure care
Recommendation 3
Develop minimum standards for chronic heart failure multidisciplinary care, which can be used to accredit health services and recognise best practice health services or networks.
Recommendation 4
Develop robust funding models and examine the role of funded care packages in chronic heart failure care.
Recommendation 5
Establish system protocols and pathways to ensure effective clinical handover and service coordination across care transitions, and activate appropriate services according to clinical need for an exacerbation, emergency presentation, hospitalisation or palliation.
Recommendation 6
Streamline care processes to facilitate early diagnosis, self management, multidisciplinary care planning, including primary care involvement and appropriate access to palliative services.
Recommendation 7
Embed mechanisms to promote the rights of the individual/carer to facilitate their active engagement with health professionals and care systems.
Multidisciplinary care for people with chronic heart failurePrinciples and recommendations for best practice
© 2010 National Heart Foundation of Australia ABN 98 008 419 761
ISBN: 978-1-9211226-90-8
PRO-110
Disclaimer: This document has been produced by the National Heart Foundation of Australia for the information of health professionals. The statements and recommendations it contains are, unless labelled as ‘expert opinion’, based on independent review of the available evidence. Interpretation of this document by those without appropriate medical and/or clinical training is not recommended, other than at the request of, or in consultation with, a relevant health professional. While care has been taken in preparing the content of this material, the National Heart Foundation of Australia and its employees cannot accept any liability, including for any loss or damage, resulting from the reliance on the content, or for its accuracy, currency and completeness.
This material may be found in third parties’ programs or materials (including but not limited to show bags or advertising kits). This does not imply an endorsement or recommendation by the National Heart Foundation of Australia for such third parties’ organisations, products or services, including these parties’ materials or information. Any use of National Heart Foundation of Australia material by another person or organisation is done so at the user’s own risk.
The entire contents of this material are subject to copyright protection.
For heart health information
1300 36 27 87
www.heartfoundation.org.au
A_CHF_MDCReportCover_FINAL.indd 1-2 9/07/10 2:22 PM
Guidelines for the prevention, detection and management of chronic heart failure in AustraliaUpdated October 2011
For heart health information 1300 36 27 87 www.heartfoundation.org.au
© 2011 National Heart Foundation of Australia. All rights reserved.
This work is copyright. No part may be reproduced in any form or language without prior written permission from the National Heart Foundation of Australia (national office). Enquiries concerning permissions should be directed to [email protected].
Based on a review of evidence published up to 30 November 2010.
ISBN 978-1-921748-71-4
PRO-119.v2
Suggested citation: National Heart Foundation of Australia and the Cardiac Society of Australia and New Zealand (Chronic Heart Failure Guidelines Expert Writing Panel). Guidelines for the prevention, detection and management of chronic heart failure in Australia. Updated October 2011.
Disclaimer: This material has been developed for general information and educational purposes only. It does not constitute medical advice. The health information provided has been developed by the Heart Foundation and is based on independent research and the available scientific evidence at the time of writing. The information is obtained and developed from a variety of sources including but not limited to collaborations with third parties and information provided by third parties under licence. It is not an endorsement of any organisation, product or service. While care has been taken in preparing the content of this material, the National Heart Foundation of Australia, its employees and related parties cannot accept any liability, including for any loss or damage, resulting from the reliance on the content, or for its accuracy, currency and completeness. This material may be found in third parties programs or materials (including but not limited to show bags or advertising kits). This does not imply an endorsement or recommendation by the National Heart Foundation of Australia for such third parties organisations, products or services, including their materials or information. Any use of National Heart Foundation of Australia materials or information by another person or organisation is at the user’s own risk.
Guid
elines for the p
revention, d
etection and m
anagement of chro
nic heart failure in Australia | U
pdated October 2011
6mm
spi
ne
allo
cate
d6m
m s
pine
al
loca
ted
Against a background of recent national health reform linking improved person-centred care with performance and funding arrangements there is increasing interest in how to realign care systems accordingly. Research suggests that individuals value easy access to services, coordinated care, and information and honesty about their prognosis.77,78 Establishment of patient/consumer charters and informed consent policies have been introduced; however, there is limited evidence demonstrating consumer engagement influencing change in care delivery.79
Figure 5 Evidence-based guidelines for chronic heart failure and delivery of patient-centred multidisciplinary care

20 A systematic approach to chronic heart failure care National Heart Foundation of Australia
Recommendation 8
Develop national data definitions for chronic heart failure.
Recommendation 11
Trial the Personally Controlled e-Health Record (PCeHR) for those diagnosed with chronic heart failure, so all current and future healthcare providers could, with the individual’s consent, have access to the same information where and when they need it.
Recommendation 9
Expand current cardiac registries, to include those with chronic heart failure.
Recommendation 10
Develop mechanisms to promote data linkage across care transitions.
Theme 2 Access to meaningful data for management and benchmarking
Principle:
• The collection of outcomes data is the only accurate way of determining the effectiveness and cost of individual treatments. Practice standards can then be based upon up-to-date comparative effectiveness research.
• Reduce unnecessary hospital admissions and the high rate of medical errors (18%) that occur from inadequate information.
“Information is fundamental, because any quality improvement is dependent on the capacity to measure change in processes and outcomes, and on stakeholders having access to the information that changes what they do.”80
Measuring the burden of disease related to chronic heart failure is challenging, as there is a paucity of data in Australia resulting in a reliance on overseas research.23,81 Australian data is still being extrapolated from overseas research as we do not have clearly defined processes to identify and record the people at risk of, and with, symptomatic chronic heart failure. This lack of identification prevents efficient patient monitoring and coordinated recall between healthcare providers to ensure appropriate assessments and treatments are completed at pre-agreed intervals.
The Personally Controlled e-Health Record (PCeHR), whilst in the early stages of implementation, potentially offers those with chronic heart failure the ideal tool to track, document and supply the individual, carer and healthcare provider with the appropriate healthcare information on demand to optimise care.
In addition, we do not have standardised outcomes to measure and evaluate care effectiveness and enable international and national benchmarking activity. The definition of a quality indicator must be specific, complete, and clearly worded regarding, for instance, target population and the characteristics of the outcome. It must be verified that different users share the same meaning and therefore make the same observations when, on different occasions, they consult various data sources (e.g. clinic or hospital records).82,83 Other barriers to measuring standardised outcomes are poor data system compatibility across, and within, health services, preventing efficient transfer of data. Data is often duplicated, with each health professional collecting a full medical history each time they see a new patient.
Increasingly hospital readmission is becoming an important indicator of healthcare outcomes as it aims to identify potentially preventable admissions. The operating definition employed by the Australian Council of Healthcare Standards (ACHS), has chosen 28-day readmission to indicate less than optimal management.84

21 National Heart Foundation of Australia A systematic approach to chronic heart failure care
Recommendation 12
Use 12-month event-free survival nationally as an outcome measure to evaluate effectiveness of care systems. Events would include emergency presentations, hospitalisations, and premature death.
Recommendation 13
Establish a national mechanism for monitoring and reporting chronic heart failure care outcomes against a nationally recognised set of goals and standards.
Recommendation 14
Develop a national set of indicators and standards to evaluate, inform and improve systems of care.
Readmission as a sole indicator of the quality of care is problematic as there are issues concerning interpretation and utility in the clinical environment. This includes whether planned and unplanned readmissions are counted. The second issue is how to identify associated readmissions. There is potential for readmissions connected with the initial illness to be missed. An individual discharged with chronic heart failure and then readmitted with shortness of breath (related to fluid overload) may receive a different discharge code for each illness. An operational definition for readmission needs to clearly identify the diagnostic related group and/or major disease classification that are associated with the index admission. The third issue is identifying exactly what the readmission indicator is measuring. It is argued that readmissions occurring within 30 days of discharge are related to the management of the initial complaint and potential sub-optimal care.85,86 Other authors have argued that returns to hospital within a short timeframe cannot be solely blamed on poor quality inpatient care, as individual behaviours also have an impact. These behaviours include non-attendance at outpatient clinics, poor compliance with medicines and diet, and inability to recognise and respond appropriately to symptom change.87,88
Readmissions that occur over a longer time period generally relate to the chronic nature of the disease.89 More frequently in chronic heart failure research, event-free survival has been used as a valid quality indicator.90,91 Events are defined as emergency presentations, hospitalisations and premature death within 12 months.92,93
Despite well-developed guidelines for chronic heart failure care to reduce the number of events such as re-hospitalisations and premature death, it is recognised that there is incomplete implementation of these resources across Australia.56,94 These care variations appear to correlate with outcomes and appear to reflect geographical challenges, workforce, local policy and individual characteristics.55,66,94,95

22 A systematic approach to chronic heart failure care National Heart Foundation of Australia
Theme 3 Workforce planning
Principle:
• Appropriately trained workforce with access to specialist cardiology support.
The Productivity Commission released Australia’s Health Workforce Research Report in 2005 to guide workforce planning for the future.96 It outlined that demand for healthcare services, and thus workforce, would be driven primarily by the ageing population and associated disability rates, as well as changing technology, changing burden of disease, higher incomes and expectations. It is anticipated that with an increasing proportion of the population being over 65 years old, the incidence of chronic heart failure will rise, resulting in increased demand for specialised, multidisciplinary chronic disease workforce support. This increased need means policy choices around specialisation or multi-skilling in the health workforce will be important to ensure health service demands are translated into health workforce supply.97
Australian research suggests that 93% of programs for people with chronic heart failure are based in capital cities, despite 40% of the known chronic heart failure population living in regional centres or rural and remote areas.98 Further, there were no programs available in either the Northern Territory or Tasmania. State and territory clinical networks are well-placed to assess service provision based on the concentration of individuals with chronic heart failure in each area. Mapping of chronic heart failure incidence can be cross-referenced to the National Service Directory for Heart Failure Programs to establish where the gaps in service lie.98,99
To enhance community-based management of chronic heart failure, general practitioners should be empowered to lead care. Reform options proposed the establishment of a Medicare Chronic Disease Program (CDP) to offer one solution for providing incentives to promote the coordination of care and integrated focus in the community, led by the general practitioner and their practice.100 Any incentive arrangements should favour provision of care for Aboriginal and Torres Strait Islander peoples, low socioeconomic, rural, and other high-need populations to ensure appropriate access and provision of chronic disease care in the community.100
Recommendation 15
Develop the workforce capacity across hospital and community services to deliver evidence-based care, appropriate to the local population, as identified in Guidelines for the prevention, detection and management of chronic heart failure in Australia12 and Multidisciplinary care for people with chronic heart failure.3
Recommendation 16
Develop robust funding models for the delivery of these services.
Recommendation 17
Examine mechanisms to empower general practitioners and healthcare professionals in primary care to deliver evidence based care for chronic heart failure.

23 National Heart Foundation of Australia A systematic approach to chronic heart failure care
Theme 4 Research
Principle:
• Essential to strengthen the health system and improve outcomes.
Ongoing chronic heart failure research and effective dissemination of results will improve our health system and outcomes leading to economic benefits and better treatments. Future research activity needs to build processes to ensure the dissemination and translation of valuable knowledge; the creation of ethical and evidence-based research policies; and the promotion, monitoring and implementation of high quality health research evidence.
Research and quality activities arising from this consensus document are those addressing chronic heart failure care models, access to meaningful data for management and benchmarking, and workforce planning. In addition, more work needs to be undertaken amongst those populations where frequent access to mainstream services is limited; namely Aboriginal and Torres Strait Islander peoples, those from non-metropolitan areas, those with lower socio-economic backgrounds, and culturally and linguistically diverse populations.
Individuals with chronic heart failure have specific management needs. Future research should consider specialty care teams such as cardiology, general medical and gerontology, and the role they play in leading inpatient care and the impact on patient outcomes.
Recommendation 18
Create investigative teams, such as clinical chronic heart failure research networks, with active consumer collaboration.
Recommendation 19
Investigate approaches to optimise care delivery in Aboriginal and Torres Strait Islander peoples, those from non-metropolitan areas, those with lower socio-economic backgrounds, and culturally and linguistically diverse populations.

24 A systematic approach to chronic heart failure care National Heart Foundation of Australia
Conclusion
It is highly probable that the numbers of chronic heart failure associated hospitalisations, deaths and morbidity events will continue to steadily increase. The current and future burden of chronic heart failure compels us to strive for equitable outcomes for all Australians. The consensus evidence-based recommendations within this document have been informed by the current literature and input from a range of experts through the Systems of Care for Chronic Heart Failure Roundtable, including consumers and clinical and policy experts. These recommendations can empower healthcare providers and organisations, peak and government organisations, care regulators, education providers, and consumers to improve health outcomes for chronic heart failure and reduce harm.
A national policy framework with agreement between states, territories and the federal government needs to be developed and implemented to address the increasing burden of chronic heart failure. Governments at national and state levels with healthcare networks need to ensure that evidence-based care models for those with chronic heart failure are standardised with equitable access. The core principles and recommendations described in this consensus document should be incorporated into the various chronic heart failure systems of care operating across state and territory jurisdiction.
This standardisation should provide a framework for flexible care delivery, which addresses the needs of the local context, whilst ensuring equitable access nationally. This work needs to be underpinned by nationally recognised standards for outcome measurement, which are universally recognised and easily applied in practice. Data systems need to support evidence-based decision making whist providing feedback on performance relating to standardised performance measures. Our healthcare workforce needs to be equipped to deal with the increasing burden of disease associated with chronic heart failure. There needs to be training, education and research around the delivery of multidisciplinary care in an increasingly complex environment.
These recommendations, if adopted, have the potential to facilitate and promote optimal and equitable health outcomes for all Australians with chronic heart failure.

25 National Heart Foundation of Australia A systematic approach to chronic heart failure care
Appendix 1
AcknowledgementsExpert Specialty/role Representing organisation/body Roundtable
Professor Tom Marwick (Roundtable chair)
Cardiologist Menzies Research Institute Tasmania
Professor Walter Abhayaratna
Cardiologist Canberra Hospital and Health Services and Australian National University
Dr Anu Aggarwal Cardiologist Royal Melbourne Hospital (Vic.)
Associate Professor Andrea Driscoll
Heart Failure Nurse Practitioner Austin Health and Deakin University
Dr Jacquie Garton-Smith Clinical Lead and Hospital Liaison GP Cardiovascular Health Network (WA) and Royal Perth Hospital
Debra Gascard Chronic Disease – Heart Failure Nurse Practitioner
Monash Health (Vic.) and Cardiac Clinical Network (Vic.)
Annabel Hickey Statewide Heart Failure Services Coordinator Prince Charles Hospital (Qld) and Statewide Cardiac Clinical Network (Qld)
Alistair Kerr Consumer representative Cardiomyopathy Association of Australia and Chronic Illness Alliance
Dr Dariusz Korczyk Cardiologist Princess Alexandra Hospital (Qld) and Statewide Cardiac Clinical Network (Qld)
Rhonda Sanders Clinical Nurse Consultant St Vincent’s Hospital Melbourne/Australian College of Critical Care Nursing (ACCCN)
Deborah Spicer Heart Failure Clinical Practice Consultant/Heart Failure Nurse Practitioner
Southern Adelaide Local Health Network and Statewide Cardiac Clinical Network (SA)
Professor Simon Stewart Head of Preventative Health and Director, NHMRC Centre for Research Excellence to Reduce Inequality in Heart Disease
Baker IDI Heart and Diabetes Institute
Dr Rob Grenfell National Director, Cardiovascular Health National Heart Foundation of Australia
Dr Karen Page National Manager, Health Equity and Secondary Prevention
National Heart Foundation of Australia
Vicki Wade Leader, National Aboriginal Health Unit National Heart Foundation of Australia
Julie-Anne Mitchell Director, Cardiovascular Health Programs (NSW) National Heart Foundation of Australia
Rebecca Lee Project Officer, Heart Care National Heart Foundation of Australia
Roundtable (in absentia)
Associate Professor Tom Briffa
Allied Health Practitioner/Epidemiologist University of Western Australia
Professor Patricia Davidson Director, Centre for Cardiovascular and Chronic Care
University of Technology, Sydney
Dr Michael Smith Clinical Director Australian Commission on Safety and Quality in Health Care
Further consultation
Dr Jan Cameron Senior Research Fellow Cardiovascular Research Centre, Australian Catholic University (Vic.)
Rohan Greenland National Director, Government Relations National Heart Foundation of Australia

26 A systematic approach to chronic heart failure care National Heart Foundation of Australia
Appendix 2
Methodology Under the new strategy, For All Hearts, the Heart Foundation committed to developing a consensus paper to articulate those associated policy actions required to achieve a systematic approach to heart failure management in Australia.
The initial scope of the consensus statement was developed internally by the Heart Foundation and reviewed by a panel of Australian clinical experts – the Heart Foundation’s Clinical Issues Committee.
An internal working group then commenced an evidence review and developed an issues paper of key considerations. This issues paper was used as a basis for a Roundtable discussion: Improving Systems of Care for Chronic Heart Failure. A range of experts in chronic heart failure and systems change participated in Melbourne on 24 April 2013 for the Roundtable discussion.
Based on consensus from the Roundtable discussion, this document, A systematic approach to chronic heart failure: a consensus statement, has been developed. Further consultation with members of the Roundtable and additional internal and external stakeholders was undertaken after the completion of this document.
The Heart Foundation’s internal governance committees – Clinical Issues Committee, Cardiovascular Health Advisory Committee, and the National Board have reviewed this document.
Appendix 3 New York Heart Association Functional Classification
Functional classification
Class I
Patients with cardiac disease but without resulting limitations of physical activity. Ordinary physical activity does not cause undue fatigue, palpitation, dyspnoea, or angina pain.
Class II
Patients with cardiac disease resulting in slight limitation of physical activity. They are comfortable at rest. Ordinary physical activity results in fatigue, palpitation, dyspnoea, or angina pain.
Class III
Patients with cardiac disease resulting in marked limitation of physical activity. They are comfortable at rest. Less than ordinary physical activity causes fatigue, palpitation, dyspnoea, or angina pain.
Class IV
Patients with cardiac disease resulting in inability to carry on any physical activity without discomfort. Symptoms of cardiac insufficiency or of the angina syndrome may be present even at rest. If any physical activity is undertaken, discomfort is increased.

27 National Heart Foundation of Australia A systematic approach to chronic heart failure care
Glossary
Acronyms and abbreviations AIHW Australian Institute of Health and Welfare
CHF Chronic heart failure
ICD code International Classification of Diseases
LOS Length of stay
LV Left ventricular
NYHA New York Heart Association
LAH Local area health networks
ACCHO Aboriginal community controlled health organisations
ACSQHC Australian Commission on Safety and Quality in Healthcare
WHO World Health Organization
OECD Organisation for Economic Co-Operation and Development
PCeHR Personally Controlled electronic Health Record
ACHS Australian Council of Healthcare Standards
CDP Chronic disease program
GP General practitioner
CDM Chronic disease management
28 A systematic approach to chronic heart failure care National Heart Foundation of Australia
Definitions
Acute sector This refers to healthcare oriented towards the care of critically ill patients, including emergency care and surgery.
Cardiac registries Cardiac registries are collections of secondary data related to patients with a heart diagnosis, condition, or procedure. They contain demographic and clinical outcome data.
Care continuum Care continuum describes both the horizontal and vertical movement of patients through the health system. That is from identification of disease through to palliation, as well as coordination between primary care to hospital and back to primary care again.
Care pathway Care pathways are described variously as integrated care pathways, clinical pathways, critical pathways, care maps, or anticipated recovery pathways. A care pathway is anticipated care placed in an appropriate time frame, written and agreed on by a multidisciplinary team.
It has locally agreed standards based on evidence, where available, to help a patient with a specific condition or diagnosis move progressively through the clinical experience.
It forms part or all of the clinical record, documenting the care given. It facilitates and demonstrates continuous quality improvement.
Clinical networks Clinical networks bring together health professionals, patients, consumers, carers and stakeholder organisations to work on a collaborative basis and provide leadership for clinical service development across the full spectrum of healthcare. Networks create awareness that all areas are linked within a coordinated system, with each part playing an important role.
Consensus Consensus decision-making is a group decision-making process that seeks the consent of all participants. Consensus may be defined professionally as an acceptable resolution, or one that can be supported, even if not the ‘favourite’ of each individual. It is used to describe both the decision and the process of reaching a decision. Consensus decision-making is thus concerned with the process of deliberating and finalising a decision.
Consumer Consumer engagement informs broader community engagement. Health consumers activelyengagement participate in their own healthcare and in health policy, planning, service delivery and
evaluation at service and agency levels.
Echocardiogram Often referred to as a cardiac echo, this is a sonogram of the heart. It is routinely used in the diagnosis, management and follow-up of patients with any suspected or known heart diseases. It can provide a wealth of helpful information, including the size and shape of the heart (internal chamber size quantification), pumping capacity and the location and extent of any tissue damage.
Event-free survival This is a composite of the number of emergency presentations, hospitalisations and deaths associated with heart failure, measured over a 12-month period.
Exceptional symptoms This refers to a pathophysiological state in which an abnormality in cardiac function is responsible for the failure of the heart to pump blood at a rate commensurate with the requirements of metabolising tissues, or to do so only from an elevated filling pressure.
Flexible care delivery Flexible care addresses the needs of care recipients in ways other than the care provided through mainstream residential and community care.
GP practice network General practice networks were responsible for supporting general practice teams in providing safe, high quality primary healthcare to people in their geographical region. Many have been replaced recently by Medicare Locals.

29 National Heart Foundation of Australia A systematic approach to chronic heart failure care
Hospital networks A hospital network is a group of hospitals that work together to coordinate and deliver a broad spectrum of services to their community.
Incidence This refers to the number of new disease cases in a population over a period of time.
Integrated/ WHO gives the following definition: Integrated care is a concept bringing together inputs,coordinated care delivery, management and organisation of services related to diagnosis, treatment, care,
rehabilitation and health promotion. Integration is a means to improve services in relation to access, quality, user satisfaction and efficiency.101
Local area Similar to hospital networks, these manage the delivery of public hospital services and otherhealth networks community based health services, as determined by the state government.
Length of stay Length of stay refers to the average number of days that patients spend in hospital. It is generally measured by dividing the total number of days stayed by all inpatients during a year by the number of admissions or discharges.
Marginalised This occurs when individuals or entire communities of people are systematically blocked frompopulations rights, opportunities and resources (e.g. housing, employment, healthcare, civic
engagement, democratic participation and due process) that are normally available to members of society and which are key to social integration.
Multidisciplinary This involves a broad range of health professionals and providers from across healthcare whocare are involved in evidence-based guideline management, monitoring signs and symptoms
for changes in condition, supporting patient and family involvement in goal setting and development of individualised management plans, promotion and support of self-care where appropriate, behaviour strategies to support risk modification and adherence, care continuity across healthcare services, and monitoring for quality improvement.
National policy A national policy framework is a policy set by the federal government to define standards of careframework for a major health issue.
Potentially An admission to hospital that could have potentially been prevented through the provisionpreventable of appropriate non-hospital health services is referred to as a ‘potentially preventablehospitalisations hospitalisation’.
Prevalence Prevalence refers to the total number of cases of a disease or condition in a given population at a specific time.
Primary sector Healthcare provided in the community, often by general practice, is known as the primary sector. It is often the first point of contact with the healthcare sector.
System protocols System protocols specify the actions or processes to support the safe delivery of services and efficient management of resources across health services.
System-based This refers to an approach that can be defined as a coordinated and seamless series of activated events which transcend traditional service-delivery boundaries, thereby encompassing the system-based principles of synergy, integration, collaboration and networks.

30 A systematic approach to chronic heart failure care National Heart Foundation of Australia
References
1. Krum H, Jelinek MV, Stewart S, et al. 2011 update to National Heart Foundation of Australia and Cardiac Society of Australia and New Zealand Guidelines for the prevention, detection and management of chronic heart failure in Australia, 2006. Med J Aust 2011; 194(8):405-409.
2. Krum H, Jelinek MV, Stewart S, et al. Guidelines for the prevention, detection and management of people with chronic heart failure in Australia 2006. Med J Aust 2006; 185(10):549-557.
3. National Heart Foundation of Australia. Multidisciplinary care for people with chronic heart failure. Principles and recommendations for best practice. Melbourne: National Heart Foundation of Australia, 2010.
4. Australian Bureau Statistics. Population Projections, Australia, 2006 to 2101. Canberra: ABS, 2011.
5. Australian Institute of Health and Welfare. Heart failure… what of the future? Bulletin no. 6. Canberra: AIHW, 2003.
6. Australian Insititute of Health and Welfare. Australian Hospital Statistics: national emergency access and elective surgery targets 2012. Health Services Series no. 48. Canberra: AIHW, 2012; Cat. no. HSE 131.
7. Krum H, Abraham WT. Heart failure. Lancet 2009; 373(9667):941-955.
8. Woods JA, Katzenellenbogen JM, Davidson PM, et al. Heart failure among Indigenous Australians: a systematic review. BMC Cardiovasc Disord 2012; 12:99.
9. Australian Bureau of Statistics. Australian Health Survey: First Results, 2011-13. 4364055001. Canberra: ABS; 2013.
10. Hauptman PJ, Rich MW, Heidenreich PA, et al. The heart failure clinic: a consensus statement of the Heart Failure Society of America. J Card Fail 2008; 14(10):801-815.
11. McAlister FA, Stewart S, Ferrua S, et al. Multidisciplinary strategies for the management of heart failure patients at high risk for admission: a systematic review of randomized trials. J Am Coll Cardiol 2004; 44(4):810-819.
12. National Heart Foundation of Australia and the Cardiac Society of Australia and New Zealand (Chronic Heart Failure Guidelines Expert Writing Panel). Guidelines for the prevention, detection and management of chronic heart failure in Australia. Updated October 2011. Melbourne: National Heart Foundation of Australia, 2011.
13. Takeda A, Taylor SJC, Taylor RS, et al. Clinical service organisation for heart failure (Review). Cochrane Database of Systematic Reviews 2012, Issue 9.
14. Council of Australian Governments. National Healthcare Agreement 2012. Canberra: COAG, 2012.
15. Australian Government Department of Health and Ageing (DoHa). Rural Primary Health Services (RPHS) Program: Operational Guideline. Canberra: Commonwealth of Australia, 2009.
16. Heart Failure Society of America, Lindenfeld J, Albert NM, et al. HFSA 2010 Comprehensive Heart Failure Practice Guideline. J Card Fail 2010; 16(6):e1-194.
17. Laurent-Bopp D. Heart Failure. In: Woods SL, Sivarajan Froelicher ES, Motzer Underhill S, editors. Cardiac Nursing. 4th edn. Philadelphia: J.B. Lippincott, 2000:560-579.
18. Remme WJ, Swedberg K, Task Force for the Diagnosis and Treatment of Chronic Heart Failure, European Society of Cardiology. Guidelines for the diagnosis and treatment of chronic heart failure. Eur Heart J 2001; 22(17):1527-1560.
19. Hunt SA, Baker DW, Chin MH, et al. ACC/AHA guidelines for the evaluation and management of chronic heart failure in the adult: executive summary. J Heart Lung Transplant 2002; 21(2):189-203.
20. Braunwald E. Disorders of the heart. In: Braunwald E, Fauci AS, Kasper DL, et al, editors. Harrison’s Principles of Internal Medicine. 15th edn. United States: McGraw-Hill, 2001:1309-1331.
21. Watson RD, Gibbs CR, Lip GY. ABC of heart failure. Clinical features and complications. BMJ 2000; 320(7229):236-239.
22. Opie LH. Heart Failure: Neurohumoral Responses. 4th edn. Philidelphia: Lippincott Williams & Wilkins, 2004.

31 National Heart Foundation of Australia A systematic approach to chronic heart failure care
23. Krum H, National Heart Foundation of Australia and Cardiac Society of Australia & New Zealand Chronic Heart Failure Clinical Practice Guidelines Writing Panel. Guidelines for management of patients with chronic heart failure in Australia. Med J Aust. 2001; 174(9):459-466.
24. Akosah KO, Moncher K, Schaper A, et al. Chronic heart failure in the community: missed diagnosis and missed opportunities. J Card Fail 2001; 7(3):232-238.
25. Clark RA, Mclennan S, Dawson A, et al. Uncovering a hidden epidemic: a study of the current burden of heart failure in Australia. Heart Lung Circ 2004; 13(3):266-273.
26. Young JB. The global epidemiology of heart failure. Med Clin North Am. 2004; 88(5):1135-1143, ix.
27. Davis RC, Hobbs FD, Kenkre JE, et al. Prevalence of left ventricular systolic dysfunction and heart failure in high risk patients: community based epidemiological study. BMJ 2002; 325(7373):1156.
28. Fonarow GC, ADHERE Scientific Advisory Committee. The Acute Decompensated Heart Failure National Registry (ADHERE): opportunities to improve care of patients hospitalized with acute decompensated heart failure. Rev Cardiovasc Med. 2003; 4(Suppl 7):S21-S30.
29. Saul L, Shatzer M. B-type natriuretic peptide testing for detection of heart failure. Crit Care Nurs Q. 2003; 26(1):35-39.
30. Vasan RS. Diastolic heart failure. BMJ 2003; 327(7425):1181-1182.
31. Kitzman DW, Little WC, Brubaker PH, et al. Pathophysiological characterization of isolated diastolic heart failure in comparison to systolic heart failure. JAMA. 2002; 288(17):2144-2150.
32. Rodgers JM, Reeder SJ. Current therapies in the management of systolic and diastolic dysfunction. Dimens Crit Care Nurs 2001; 20(6):2-10.
33. McMurray JJ. What are the clinical consequences of anemia in patients with chronic heart failure? J Card Fail 2004; 10(1 Suppl):S10-S12.
34. Klapholz M, Maurer M, Lowe AM, et al. Hospitalization for heart failure in the presence of a normal left ventricular ejection fraction: results of the New York Heart Failure Registry. J Am Coll Cardiol 2004; 43(8):1432-1438.
35. Beta-Blocker Evaluation of Survival Trial Investigators. A trial of the beta-blocker bucindolol in patients with advanced chronic heart failure. New Eng J Med 2001; 344(22):1659-1667.
36. Harvey R, Doyle E, Ellis K. Editorial: Major changes made by Criteria Committee of the New York Heart Association. Circulation 1974; 49(3):390.
37. Goodlin SJ. Palliative care in congestive heart failure. J Am Coll Cardiol. 2009; 54(5):386-396.
38. World Health Organization. The global burden of disease: 2004 update. In: World Health Organization, editor. Geneva, Switzerland: WHO Press, 2008.
39. Go AS, Mozaffarian D, Roger VL, et al. Heart disease and stroke statistics – 2013 update: a report from the American Heart Association. Circulation 2013; 127(1):e6-e245.
40. Australian Bureau Statistics. Causes of death, Australia, 2011. Canberra: ABS, 2011.
41. Australian Institute of Health and Welfare. Chronic diseases and associated risk factors in Australia. Canberra: AIHW, 2001; cat. no. PHE 33.
42. Australian Institute of Health and Welfare. National hospital morbidity data 1997-8 to 2000-01. Available at: http://www.aihw.gov.au/dataonline/index.html. Accessed 17 August 2004.
43. Toh CJ, Jackson B, Gascard DJ, et al. Barriers to Medication Adherence in Chronic Heart Failure Patients during Home Visits. J Pharm Pract Res 2010; 40(1):27-30.

32 A systematic approach to chronic heart failure care National Heart Foundation of Australia
44. Australian Health Ministers’ Advisory Council. Aboriginal and Torres Strait Islander Health Performance Framework 2012 Report. Canberra: AHMAC, 2012.
45. Morales JM, Sarria A. Alternative healthcare models for patients with heart failure: a systematic review. Rev Calidad Asistencial 2006; 21(1):51-60.
46. Rich MW, Beckham V, Wittenberg C, et al. A multidisciplinary intervention to prevent the readmission of elderly patients with congestive heart failure. New Eng J Med 1995; 333(18):1190-1195.
47. Chin MH, Goldman L. Correlates of early hospital readmission or death in patients with congestive heart failure. Am J Cardiol. 1997; 79(12):1640-1644.
48. Westert GP, Lagoe RJ, Keskimaki I, et al. An international study of hospital readmissions and related utilization in Europe and the USA. Health Policy. 2002; 61(3):269-278.
49. Heller RF, Fisher JD, D’Este CA, et al. Death and readmission in the year after hospital admission with cardiovascular disease: the Hunter Area Heart and Stroke Register. Med J Aust 2000; 172(6):261-265.
50. Cleland JG, Swedberg K, Follath F, et al. The EuroHeart Failure survey programme – a survey on the quality of care among patients with heart failure in Europe. Part 1: patient characteristics and diagnosis. Eur Heart J 2003; 24(5):442-463.
51. Victorian Government Department of Human Services. Hospital admission risk program (HARP). Chronic heart failure working party report. Melbourne: Victorian Government Department of Human Services, 2003.
52. Lee WC, Chavez YE, Baker T, et al. Economic burden of heart failure: a summary of recent literature. Heart Lung 2004; 33(6):362-371.
53. Driscoll A, Davidson P, Clark R, et al. Tailoring consumer resources to enhance self-care in chronic heart failure. Confed Aust Crit Care Nurses J 2009; 22(3):133-140.
54. Page K, Lee R. Heart failure issues paper. Melbourne: National Heart Foundation of Australia, 2013.
55. Driscoll A, Worrall-Carter L, McLennan S, et al. Heterogeneity of heart failure management programs in Australia. Eur J Cardiovas Nurs. 2006; 5(1):75-82.
56. Driscoll A, Worrall-Carter L, Hare DL, et al. Evidence-based chronic heart-failure management programmes: reality or myth? BMJ Qual Saf 2011; 20(1):31-37.
57. Azam R, Cameron M, Clark R, et al. Living well with chronic heart failure. Melbourne: National Heart Foundation of Australia, 2008.
58. National Heart Foundation of Australia. Living every day with my heart failure. Melbourne: National Heart Foundation of Australia, 2011.
59. Ontario Medical Association. Policy Paper: Patient-Centred Care, 2010. Available at: https://www.oma.org/Resources/Documents/Patient-CentredCare,2010.pdf. Accessed 30 April 2013.
60. Bodenheimer T, Wagner EH, Grumbach K. Improving primary care for patients with chronic illness: the chronic care model, Part 2. JAMA 2002; 288(15):1909-1914.
61. Bodenheimer T, Wagner EH, Grumbach K. Improving primary care for patients with chronic illness. JAMA 2002; 288(14):1775-1779.
62. Glasgow RE, Funnell MM, Bonomi AE, et al. Self-management aspects of the improving chronic illness care breakthrough series: implementation with diabetes and heart failure teams. Ann Behav Med. 2002; 24(2):80-87.
63. Robertson J, McElduff P, Pearson SA, et al. The health services burden of heart failure: an analysis using linked population health data-sets. BMC Health Serv Res 2012; 12:103.
64. Riegel B, Moser DK, Anker SD, et al. State of the science: promoting self-care in persons with heart failure: a scientific statement from the American Heart Association. Circulation 2009; 120(12):1141-1163.

33 National Heart Foundation of Australia A systematic approach to chronic heart failure care
65. VanSuch M, Naessens JM, Stroebel RJ, et al. Effect of discharge instructions on readmission of hospitalised patients with heart failure: do all of the Joint Commission on Accreditation of Healthcare Organizations heart failure core measures reflect better care?. Qual Saf Health Care. 2006; 15(6):414-417.
66. Driscoll A, Worrall-Carter L, Hare DL, et al. Evidence-based chronic heart-failure management programmes: reality or myth? BMJ Qual Saf 2011; 20(1):31-37.
67. Clark RA, Driscoll A. Access and quality of heart failure management programs in Australia. Confed Aust Crit Care Nurses J. 2009; 22(3):111-6.
68. International Alliance of Patients’ Organizations. What is Patient-Centred Health Care? A Review of Definitions and Principles. London: IAPO, 2007.
69. The Commonwealth Fund. In Focus: Health Care Institutions Are Slowly Learning to Listen to Customers. 2010. Available at: www.commonwealthfund.org/Content/Newsletters/Quality-Matters/2010/February-March-2010.aspx?view=newsletter_print. Accessed 22 May 2013.
70. Institute for Patient- and Family-Centered Care. Advancing The Practice Of Patient- And Family-Centred Care In Hospitals: How to Get Started. Bethesda: IFPCC, 2011.
71. Longtin Y, Sax H, Leape LL, et al. Patient participation: current knowledge and applicability to patient safety. Mayo Clin Proc. 2010; 85(1):53-62.
72. Stewart M, Brown JB, Donner A, et al. The impact of patient-centered care on outcomes. J Fam Pract 2000; 49(9):796-804.
73. Agency for Healthcare Research and Quality. The AHRQ Innovation Exchange: Patient- and Family-Centred Care Initiative is Associated With High Patient Satisfaction and Positive Outcomes For Total Joint Replacement Patients. 2008 [updated 8/05/2013]. Available at: www.innovations.ahrq.gov/content.aspx?id=1764. Accessed 22 May 2013.
74. Flach SD, McCoy KD, Vaughn TE, et al. Does patient-centred care improve provision of preventative services? J Gen Intern Med 2004; 19(10):1019-1026.
75. Jha AK, Orav J, Zheng J, et al. Patients’ perceptions of hospital care in the United States. New Eng J Med 2008; 359(18):1921-1931.
76. Ekman I, Wolf A, Olsson L-E, et al. Effects of person-centred care in patients with chronic heart failure: the PCC-HF study. Eur Heart J 2012; 33(9):1112-1119.
77. Komajda M, Hanon O, Hochadel M, et al. Contemporary management of octogenarians hospitalized for heart failure in Europe: Euro Heart Failure Survey II. Eur Heart J 2009; 30(4):478-486.
78. Lainscak M, Cleland JG, Lenzen MJ, et al. International variations in the treatment and co-morbidity of left ventricular systolic dysfunction: data from the EuroHeart Failure Survey. Eur J Heart Fail 2007; 9(3):292-299.
79. Groene O, Lombarts MJ, Klazinga N, et al. Is patient-centredness in European hospitals related to existing quality improvement strategies? Analysis of a cross-sectional survey (MARQulS study). Qual Saf Health Care 2009; 18(Supp I):i44-i50.
80. World Health Organization. Quality of care: a process for making strategic choices in health systems. Geneva: WHO, 2006.
81. Clark RA, McLennon S, Dawson A, et al. Uncovering a hidden epidemic: a study of the current burden of heart failure in Australia. Heart Lung Circ 2004; 13(3):266-273.
82. Abrahamyan L, Boom N, Donovan LR, et al. An international environmental scan of quality indicators for cardiovascular care. Can J Cardiol 2012; 28(1):110-118.
83. Wijeysundera HC, Mitsakakis N, Witteman W, et al. Achieving quality indicator benchmarks and potential impact on coronary heart disease mortality. Can J Cardiol 2011; 27(6):756-762.
34 A systematic approach to chronic heart failure care National Heart Foundation of Australia
84. Australian Council on Healthcare Standards (ACHS). Australasian Clinical Indicator Report 2004-2011: 13th edition. Sydney: ACHS, 2012.
85. Camberg LC, Smith NE, Beaudet M, et al. Discharge destination and repeat hospitalizations. Med Care 1997; 35(8):756-767.
86. Ashton CM, Del Junco DJ, Souchek J, et al. The association between the quality of inpatient care and early readmission: a meta-analysis of the evidence. Med Care 1997; 35(10):1044-1059.
87. Ghali JK, Kadakia S, Cooper R, et al. Precipitating factors leading to decompensation of heart failure. Traits among urban blacks. Arch Intern Med 1988; 148(9):2013-2016.
88. Gooding J, Jette AM. Hospital readmissions among the elderly. J Am Geriatr Soc 1985; 33(9):595-601.
89. Franklin PD, Noetscher CM, Murphy ME, et al. Using data to reduce hospital readmissions. J Nurs Care Qual 1999; Spec No:67-85.
90. Moser DK, Mann DL. Improving outcomes in heart failure: It’s not unusual beyond usual care. Circulation 2002; 105(24):2810-2812.
91. Stewart S, Horowitz J. Home-based intervention in congestive heart failure: long-term implications on readmission and survival. Circulation 2002; 105(24):2861-2866.
92. Stewart S, Carrington MJ, Marwick T, et al. The WHICH? trial: rationale and design of a pragmatic randomized, multicentre comparison of home- vs. clinic-based management of chronic heart failure patients. Eur J Heart Fail 2011; 13(8):909-916.
93. Stewart S, Carrington MJ, Marwick TH, et al. Impact of home versus clinic-based management of chronic heart failure: the WHICH? (Which Heart Failure Intervention Is Most Cost-Effective & Consumer Friendly in Reducing Hospital Care) multicentre, randomized trial. J Am Coll Cardiol. 2012; 60(14):1239-1248.
94. Driscoll A, Tonkin A, Stewart A, et al. Development of an evidence-based scoring system (HF-IS) to assess the quality of heart failure programmes for patients postdischarge from hospital. J Clin Nurs 2011; 20(21-22):3011-3019.
95. Driscoll A, Worrall-Carter L, Stewart S. Rationale and design of the National Benchmarking and Evidence-based National Clinical Guidelines for Chronic Heart Failure Management Programs Study. J Cardiovasc Nurs 2006; 21(4):276-282.
96. Productivity Commission. Australia’s Health Workforce, Research Report. Canberra: Commonwealth of Australia, 2005.
97. Segal L, Bolton T. Issues facing the future health care workforce: the importance of demand modelling. Aust New Zealand Health Policy 2009; 6:12.
98. Clark RA, Driscoll A, Nottage J, et al. Inequitable provision of optimal services for patients with chronic heart failure: a national geo-mapping study. Med J Aust 2007; 186(4):169-173.
99. National Heart Foundation of Australia. Victorian Heart Maps. 2013. Available at: http://www.heartfoundation.org.au/information-for-professionals/data-and-statistics/Pages/interactive-map-victoria.aspx. Accessed 22 May 2013.
100. Australian Institute for Primary Care. System reform and development for chronic disease management. Melbourne: La Trobe University, 2008.
101. Grone O, Garcia-Barbero M, WHO European Office for Integrated Health Care Services. Int J Integr Care 2001; 1:e21.
35 National Heart Foundation of Australia A systematic approach to chronic heart failure care

© 2013 National Heart Foundation of Australia ABN 98 008 419 761
This work is copyright. No part of this publication may be reproduced in any form or language without prior written permission from the National Heart Foundation of Australia (national office). Enquiries concerning permissions should be directed to [email protected].
ISBN 978-1-74345-056-7
PRO-150
Suggested citation: National Heart Foundation of Australia. A systematic approach to chronic heart failure care: a consensus statement. Melbourne: National Heart Foundation of Australia, 2013.
Disclaimer: This material has been developed by the Heart Foundation for general information. The statements and recommendations it contains are, unless labelled as ‘expert opinion’, based on independent review of the available evidence.
While care has been taken in preparing the content of this material, the Heart Foundation and its employees cannot accept any liability, including for any loss or damage, resulting from the reliance on the content, or for its accuracy, currency and completeness. The information is obtained and developed from a variety of sources including, but not limited to, collaborations with third parties and information provided by third parties under licence. It is not an endorsement of any organisation, product or service.
This material may be found in third parties’ programs or materials (including, but not limited to, show bags or advertising kits). This does not imply an endorsement or recommendation by the National Heart Foundation of Australia for such third parties’ organisations, products or services, including their materials or information. Any use of National Heart Foundation of Australia materials or information by another person or organisation is at the user’s own risk.
The entire contents of this material are subject to copyright protection.
For heart health information1300 36 27 87www.heartfoundation.org.au