the future of heart failure care delivery
TRANSCRIPT

3/31/2017
1
The Future of Heart Failure Care Delivery
Innovating to Reduce Potentially Preventable Readmissions
Angie Schadler, DNP, MHCDS, ARNPUniversity of Iowa Health Care
AAHFN HF Readmission Symposium: Navigating Transitions in Care
April 8th, 2017
Disclosures
• No financial disclosures
• Completed Master’s of Health Care Delivery Science Degree through Dartmouth 1/2016
Health Care Policy: What do we know?
• We need to reduce cost and provide high value health care– High risk patients
– Care coordination
– Readmission reduction
– Quality improvement
– Process improvement
– Multidisciplinary team management
– Bundled payments

3/31/2017
2
US Health Care
Outcomes of the U.S. health care system
An estimated $750 billion, or as much as 30% of all U.S health care expenditures
add no value
Broken

3/31/2017
3

3/31/2017
4
Heart Failure Hospitalization Variation
Date of download: 10/2/2016 Copyright © The American College of Cardiology. All rights reserved.
From: Geographic Disparities in Heart Failure Hospitalization Rates Among Medicare Beneficiaries
J Am Coll Cardiol. 2010;55(4):294-299. doi:10.1016/j.jacc.2009.10.021
The care patients receive is influenced by where they live and not necessarily what is most appropriate.
Boback Ziaeian. American Heart Journal, Volume 169, Issue 2, 2015, 282–289.e15
3/31/2017
5
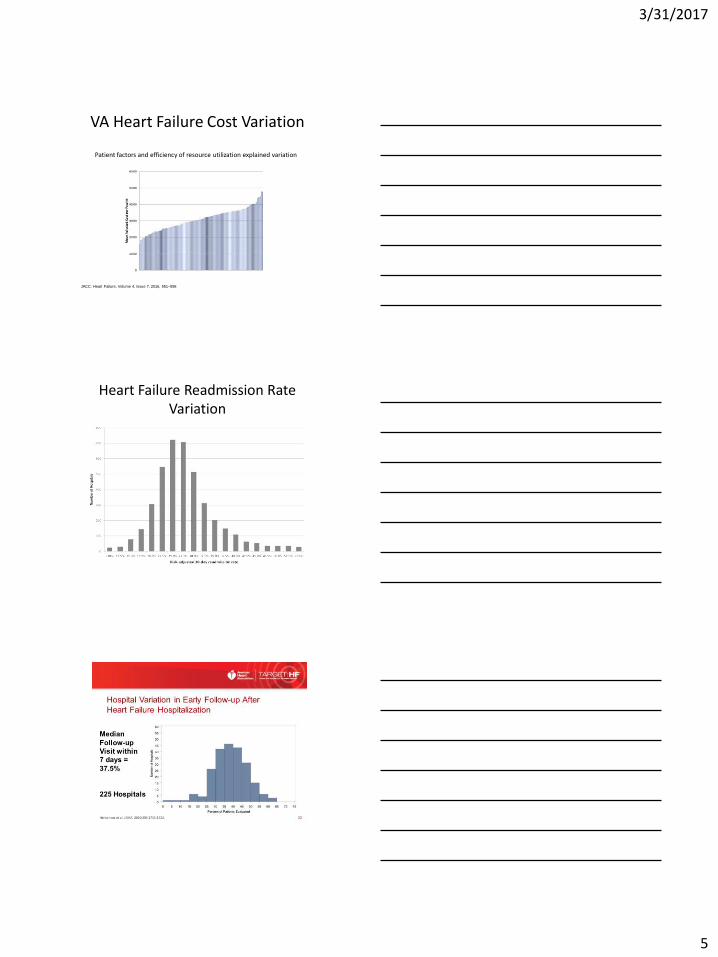
JACC: Heart Failure, Volume 4, Issue 7, 2016, 551–558
VA Heart Failure Cost Variation
Patient factors and efficiency of resource utilization explained variation
Heart Failure Readmission Rate Variation
3/31/2017
6
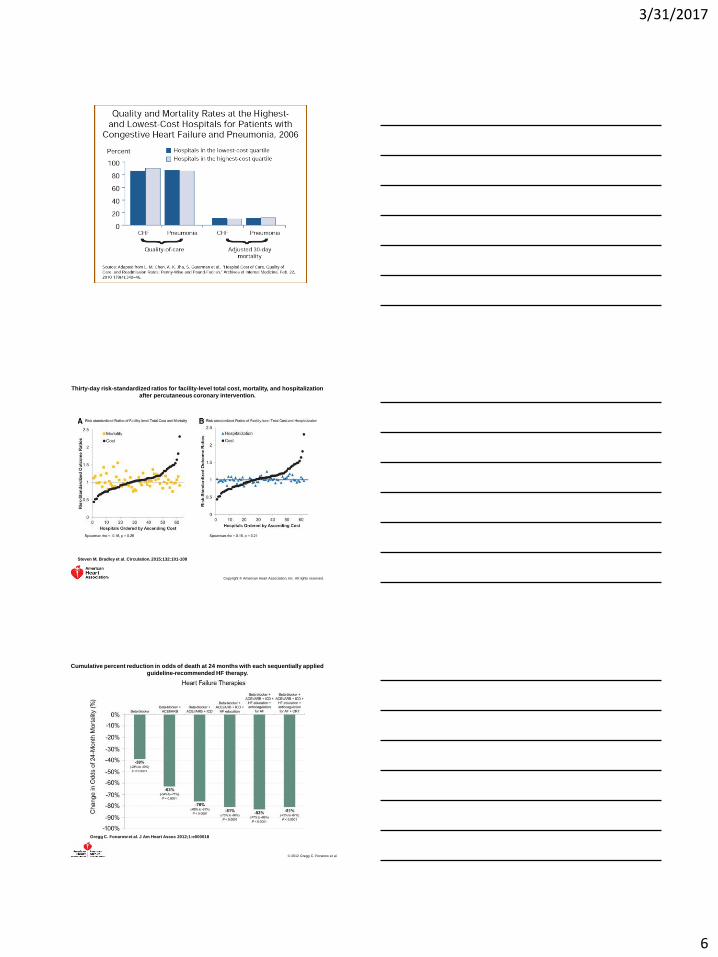
Thirty-day risk-standardized ratios for facility-level total cost, mortality, and hospitalization
after percutaneous coronary intervention.
Steven M. Bradley et al. Circulation. 2015;132:101-108
Copyright © American Heart Association, Inc. All rights reserved.
Cumulative percent reduction in odds of death at 24 months with each sequentially applied
guideline-recommended HF therapy.
Gregg C. Fonarow et al. J Am Heart Assoc 2012;1:e000018
© 2012 Gregg C. Fonarow et al.
3/31/2017
7
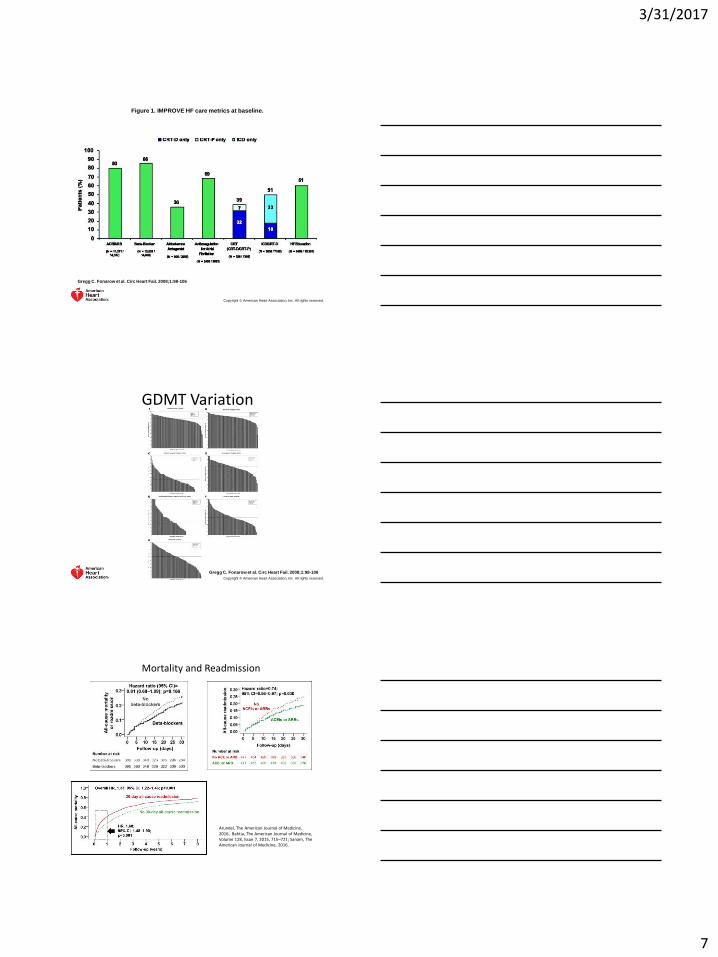
Figure 1. IMPROVE HF care metrics at baseline.
Gregg C. Fonarow et al. Circ Heart Fail. 2008;1:98-106
Copyright © American Heart Association, Inc. All rights reserved.
Gregg C. Fonarow et al. Circ Heart Fail. 2008;1:98-106
Copyright © American Heart Association, Inc. All rights reserved.
GDMT Variation
Arundel, The American Journal of Medicine, 2016; Bahtia, The American Journal of Medicine, Volume 128, Issue 7, 2015, 715–721; Sanam, The American Journal of Medicine, 2016.
Mortality and Readmission

3/31/2017
8
Roth et al. Journal of the American College of Cardiology, Volume 67, Issue 9, 2016, 1062–1069
GDMT Prior to ICD Implant Variation
What do we do?

3/31/2017
9
Where Are Avoidable Costs?
• GMDT• Variability
– Process Assessment– Process Improvement– Standardization of care– Reduce silos
• Quality– Data analytics– Real time reporting– Quality improvement– Integrate care within and outside organizations
• Highest-cost patients– Hot-spotting– Care management/home care/community
Evidence-Based, Guideline Recommended Heart Failure Therapies
Fonarow GC, et al. Am Heart J 2011;161:1024-1030.
Guideline RecommendedTherapy
Relative RiskReduction in Mortality
Number Needed to Treat for Mortality
NNT for Mortality (standardized to 36 months)
Relative Risk Reduction in HF Hospitalization
ACEI/ARB 17% 22 over 42 months
26 31%
Beta-blocker 34% 28 over 12 months
9 41%
Aldosterone Antagonist
30% 9 over 24 months
5 35%
Hydralazine/Nitrate
43% 25 over 10 months
7 33%
CRT 36% 12 over 24 months
8 52%
ICD 23% 14 over 60 months
23 NA
26
Cumulative percent reduction in odds of death at 24 months associated with sequential
treatments compared with no treatment.
Gregg C. Fonarow et al. J Am Heart Assoc 2012;1:e000018
© 2012 Gregg C. Fonarow et al.
3/31/2017
10
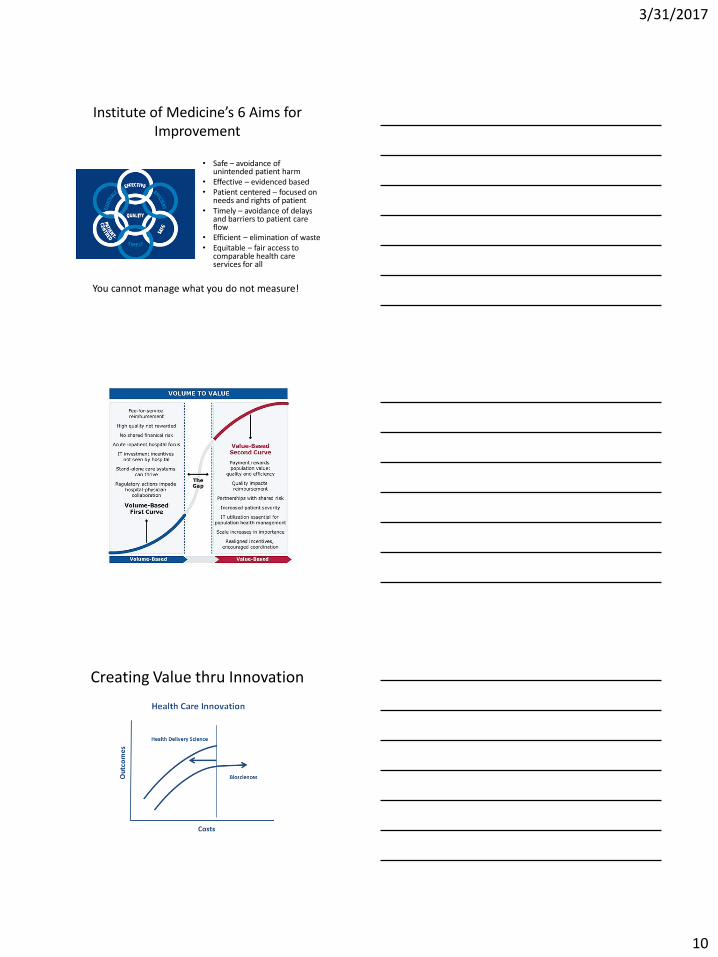
Institute of Medicine’s 6 Aims for Improvement
• Safe – avoidance of unintended patient harm
• Effective – evidenced based• Patient centered – focused on
needs and rights of patient• Timely – avoidance of delays
and barriers to patient care flow
• Efficient – elimination of waste• Equitable – fair access to
comparable health care services for all
You cannot manage what you do not measure!
Creating Value thru Innovation
3/31/2017
11
StandardizationStandard work is a written description of the safest, highest quality and most efficient way to perform a task.
Benefits of standardization:• Clearly defines specific steps• Captures best, safest practices• Reduces variation• Increases consistency• Applies to all settings• Easy to recognize deviation of the norm• Allows for cross-coverage
3/31/2017
12
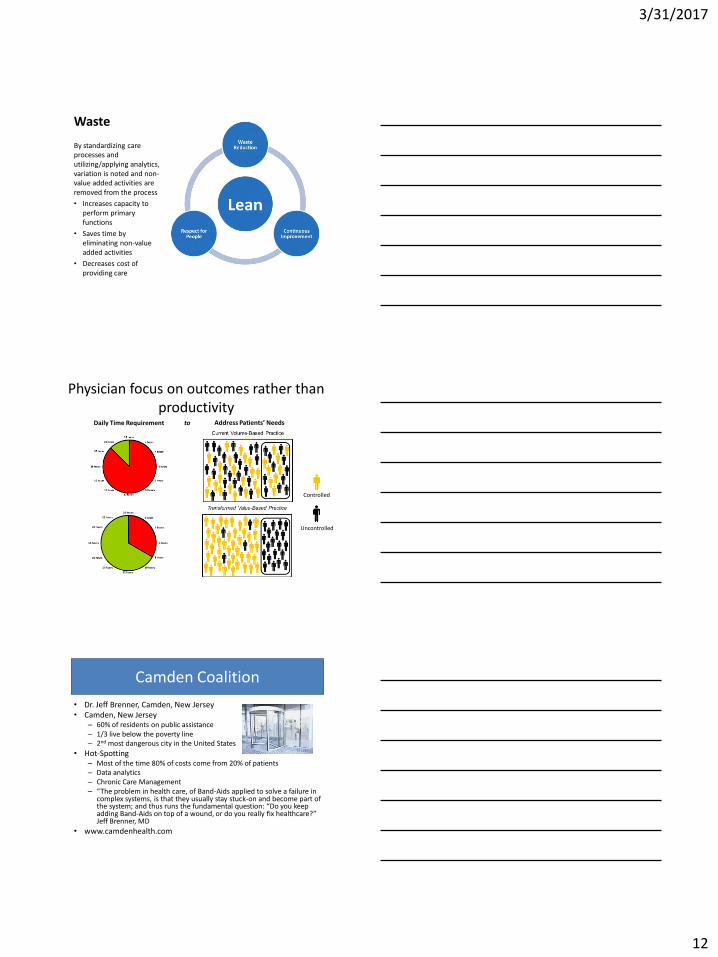
Waste
By standardizing care processes and utilizing/applying analytics, variation is noted and non-value added activities are removed from the process
• Increases capacity to perform primary functions
• Saves time by eliminating non-value added activities
• Decreases cost of providing care
Physician focus on outcomes rather than productivity
Daily Time Requirement Address Patients’ Needsto
Controlled
Uncontrolled
Camden Coalition
• Dr. Jeff Brenner, Camden, New Jersey• Camden, New Jersey
– 60% of residents on public assistance– 1/3 live below the poverty line– 2nd most dangerous city in the United States
• Hot-Spotting– Most of the time 80% of costs come from 20% of patients– Data analytics– Chronic Care Management– “The problem in health care, of Band-Aids applied to solve a failure in
complex systems, is that they usually stay stuck-on and become part of the system; and thus runs the fundamental question: “Do you keep adding Band-Aids on top of a wound, or do you really fix healthcare?” Jeff Brenner, MD
• www.camdenhealth.com
3/31/2017
13
Shouldice Hernia Repair
• Canadian based
• Hospital just for hernia repairs
• Costs including travel 1/3 of normal costs
• Outcomes
– Lower surgical complications
– Improved functional capacity
– Decreased risk of hernia recurrence
Does LEAN Work in Healthcare?
• Group Health of Puget Sound reduced E.R visits by 29% using their medical home redesign at the same time reducing hospital readmissions by 11%
• Akron children’s Hospital reduced cost by $8 M while reducing appointment access wait times by 74,600 days using LEAN
• ThedaCare’s redesigned inpatient Collaborative Care unit has achieved 0 medication reconciliation errors for 4 years running and the cost of inpatient care dropped by 25% www.createhealthcarevalue.com
• Henry Ford reduced infections rates, falls, and medication errors in 2010 resulting in a $4.4 M improvement
• Mercy North Iowa has achieved zero blood specimen tube labeling error for over a year
• Seattle Children’s Hospital avoided $200M in capital expense by freeing capacity with continuous process improvement

3/31/2017
14
Maine Heart Failure System of Care
• Patient from beginning to end of disease process
• Self-Management
• Delivery system design
• Decision Support
• Clinical information systems
• Health System
• Community
Cawley J. The Permanente Journal. Summer 2011; 15(3); 37-42
Maine Heart Failure System of Care
• Maine’s system– Improvements– Enhanced communication and integration– Improved outcomes
• Home health• Readmission rates• Medications
– Efficiency • Improved access• Standardization of patient education and clinician education• Decrease number of meetings• Decrease duplication of services
Cawley J. The Permanente Journal. Summer 2011; 15(3); 37-42

3/31/2017
15
Amber E. Johnson et al. American Journal of Medical
Quality 2014;31:272-278
Copyright © by American College of Medical Quality
Journal of Cardiac Failure, Volume 21, Issue 1, 2015, 27–43
3/31/2017
16
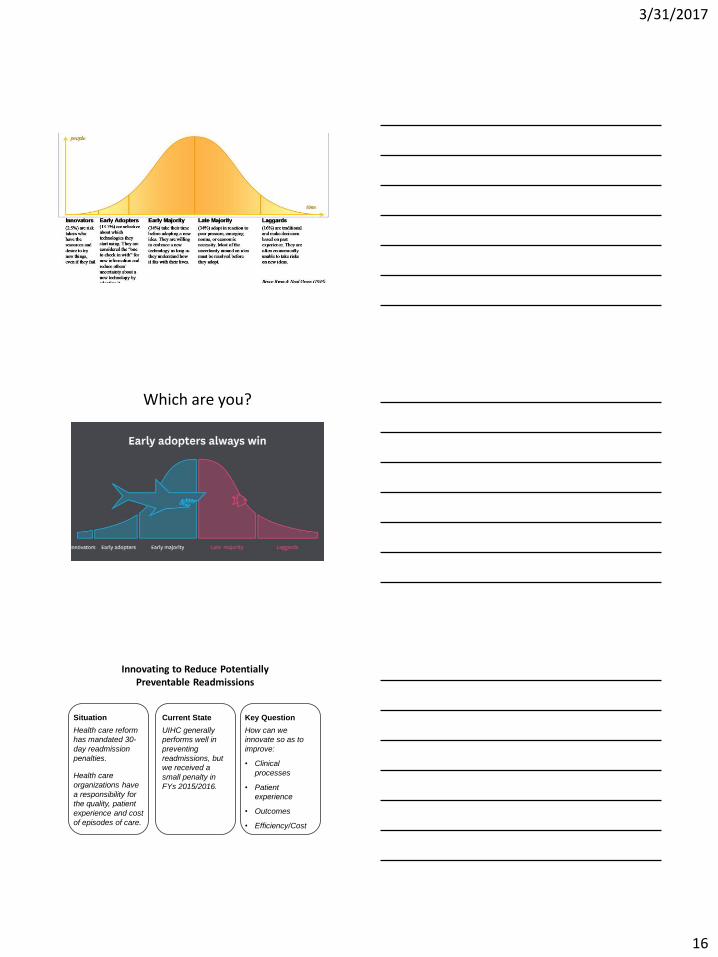
Which are you?
Innovating to Reduce Potentially Preventable Readmissions
Current State
UIHC generally
performs well in
preventing
readmissions, but
we received a
small penalty in
FYs 2015/2016.
Key Question
How can we
innovate so as to
improve:
• Clinical
processes
• Patient
experience
• Outcomes
• Efficiency/Cost
Situation
Health care reform
has mandated 30-
day readmission
penalties.
Health care
organizations have
a responsibility for
the quality, patient
experience and cost
of episodes of care.
3/31/2017
17
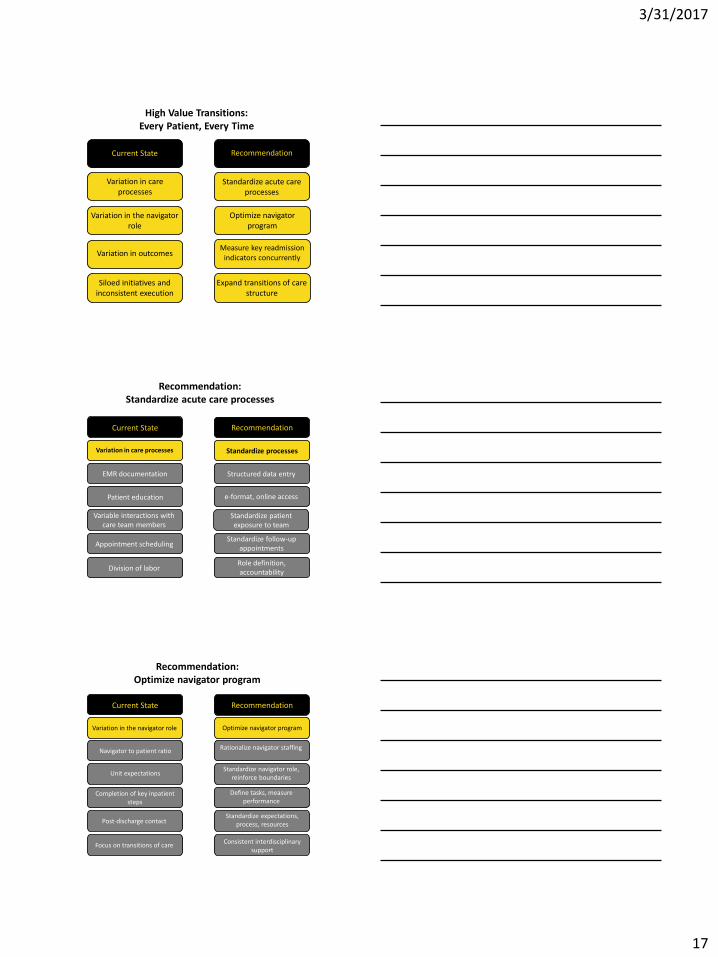
High Value Transitions: Every Patient, Every Time
Current State Recommendation
Standardize acute care processes
Measure key readmission indicators concurrently
Expand transitions of care structure
Optimize navigator program
Variation in care processes
Variation in the navigator role
Siloed initiatives and inconsistent execution
Variation in outcomes
Standardize processes
Recommendation: Standardize acute care processes
Standardize patient exposure to team
EMR documentation
Patient education
Variable interactions with care team members
Appointment scheduling
Division of laborRole definition, accountability
Standardize follow-up appointments
e-format, online access
Structured data entry
Variation in care processes
Current State Recommendation
Optimize navigator program
Recommendation: Optimize navigator program
Completion of key inpatient steps
Navigator to patient ratio
Unit expectations
Post-discharge contact
Focus on transitions of careConsistent interdisciplinary
support
Standardize expectations, process, resources
Define tasks, measure performance
Standardize navigator role, reinforce boundaries
Rationalize navigator staffing
Variation in the navigator role
Current State Recommendation
3/31/2017
18
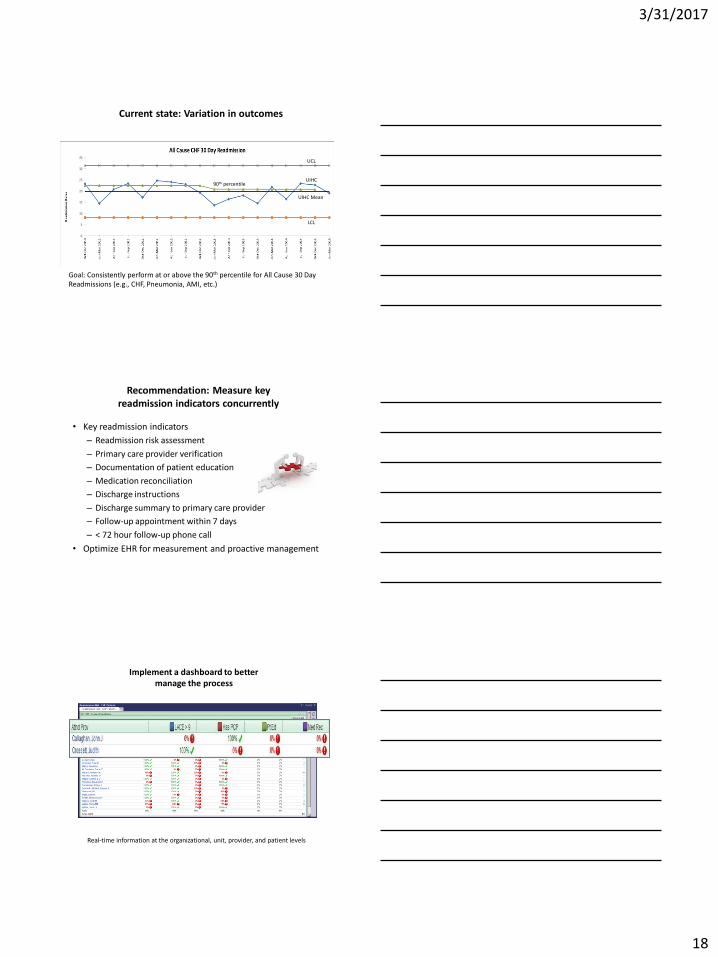
Current state: Variation in outcomes
Goal: Consistently perform at or above the 90th percentile for All Cause 30 Day Readmissions (e.g., CHF, Pneumonia, AMI, etc.)
90th percentile
UCL
UIHC
UIHC Mean
LCL
Recommendation: Measure key readmission indicators concurrently
• Key readmission indicators
– Readmission risk assessment
– Primary care provider verification
– Documentation of patient education
– Medication reconciliation
– Discharge instructions
– Discharge summary to primary care provider
– Follow-up appointment within 7 days
– < 72 hour follow-up phone call
• Optimize EHR for measurement and proactive management
Implement a dashboard to better manage the process
Real-time information at the organizational, unit, provider, and patient levels
3/31/2017
19
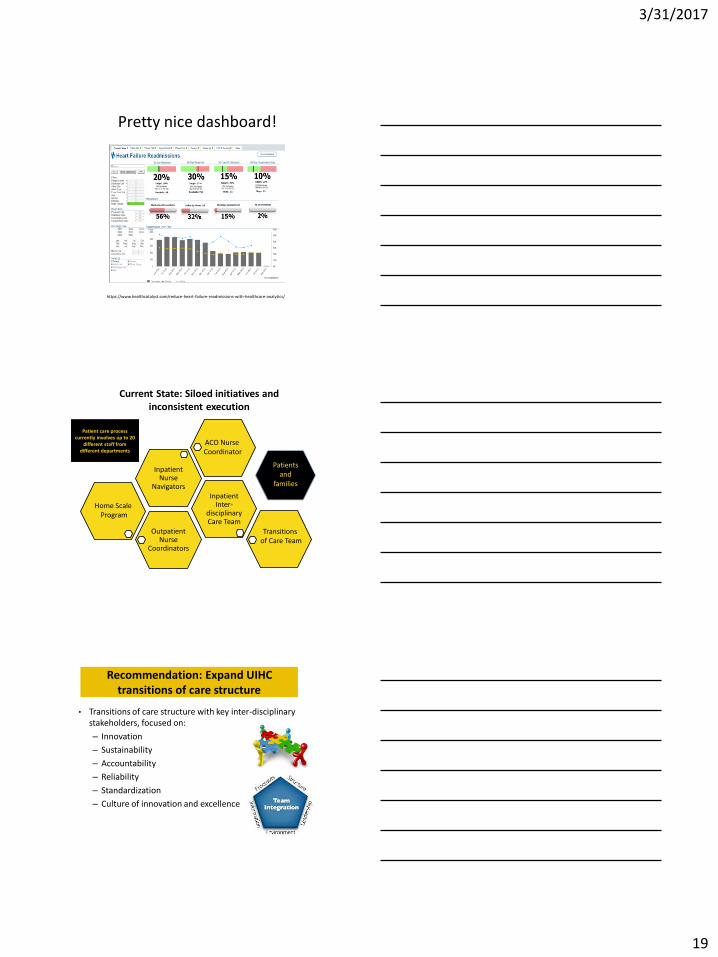
Pretty nice dashboard!
https://www.healthcatalyst.com/reduce-heart-failure-readmissions-with-healthcare-analytics/
Current State: Siloed initiatives and inconsistent execution
Outpatient Nurse
Coordinators
Inpatient Inter-
disciplinary Care Team
Inpatient Nurse
Navigators
Patient care process currently involves up to 20
different staff from different departments
Home Scale Program
ACO Nurse Coordinator
Transitions of Care Team
Patients and
families
Recommendation: Expand UIHC transitions of care structure
• Transitions of care structure with key inter-disciplinary stakeholders, focused on:
– Innovation
– Sustainability
– Accountability
– Reliability
– Standardization
– Culture of innovation and excellence
3/31/2017
20
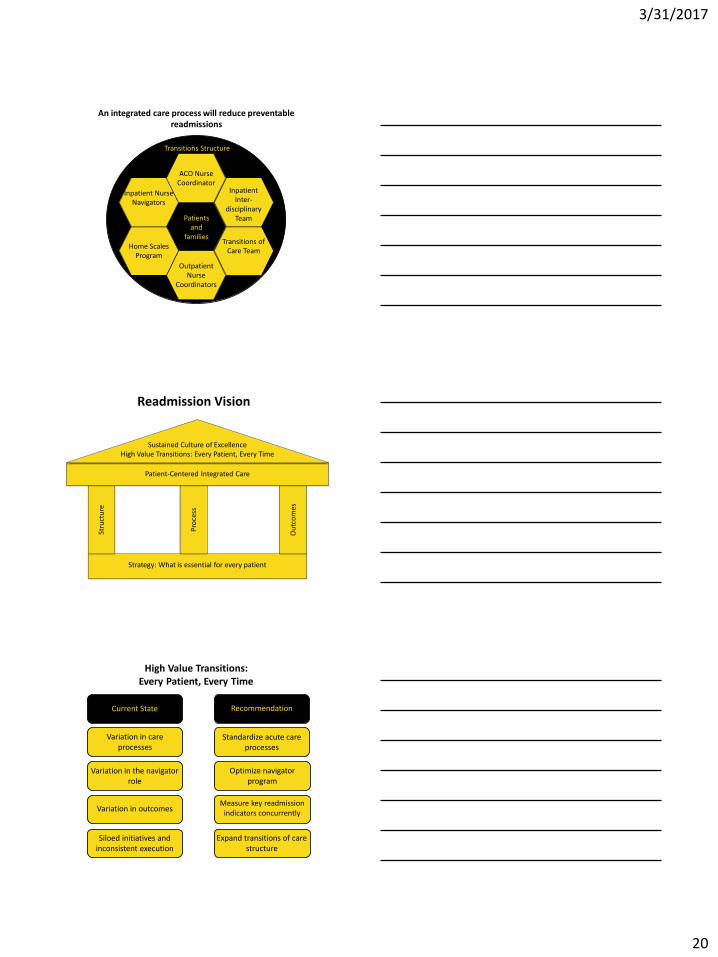
An integrated care process will reduce preventable readmissions
PatientPatients
and families
ACO Nurse Coordinator
Inpatient Inter-
disciplinary Team
Transitions of Care Team
Outpatient Nurse
Coordinators
Home Scales Program
Inpatient Nurse Navigators
Transitions Structure
Readmission Vision
Strategy: What is essential for every patient
Ou
tco
mes
Pro
cess
Stru
ctu
re
Patient-Centered Integrated Care
Sustained Culture of Excellence High Value Transitions: Every Patient, Every Time
High Value Transitions: Every Patient, Every Time
Current State Recommendation
Standardize acute care processes
Measure key readmission indicators concurrently
Expand transitions of care structure
Optimize navigator program
Variation in care processes
Variation in the navigator role
Siloed initiatives and inconsistent execution
Variation in outcomes

3/31/2017
21
High Value Heart Failure CareEvery Patient, Every Time
Heart Failure System of Care
Integration
Coordination Collaboration
Standardization
Communication
Evidenced-Based Practice
Risk Stratification
Accountability
Where Are Avoidable Costs?
• GMDT• Variability
– Process Assessment– Process Improvement– Standardization of care– Reduce silos
• Quality– Data analytics– Real time reporting– Quality improvement– Integrate care within and outside organizations
• Highest-cost patients– Hot-spotting– Care management/home care/community
In Summary…
• Where are avoidable costs?
• What is value-based care?
• Quality improvement
• Process improvement
• Disruptive Innovation