a surgical guide for accurate mesiodistal paralleling of implants
TRANSCRIPT

7/27/2019 A Surgical Guide for Accurate Mesiodistal Paralleling of Implants
http://slidepdf.com/reader/full/a-surgical-guide-for-accurate-mesiodistal-paralleling-of-implants 1/3
site preparation in most circumstances. However, asimple guide for the arrangement of implant angula-tion is often missing from stents or templatesfabricated as shells.
Implant parallelism occurs in both the buccolingualand mesiodistal directions. The buccolingual angula-tion of an implant often is restricted by the structuralform and angulation of the available bone, which may be determined and provided by direct visualizationduring surgery.10 However, the mesiodistal parallelingof implants could be ensured with the use of surgical
stents provided by prosthodontists. This articledescribes a modification of the conventional surgicalstent that will guide the surgeon in parallel placementof implants in the posterior edentulous mandible.
TECHNIQUE
1. Obtain diagnostic casts of both dental arches by making irreversible hydrocolloid impressions (CA 37; Cavex, Haarlem, Holland). Mount the diag-nostic casts in a semiadjustable articulator (model8500; WhipMix Corp, Louisville, Ky.), and com-plete the diagnostic setup of the implant-supported
A surgical guide for accurate mesiodistal paralleling of implants in theposterior edentulous mandible
Kıvanç Akça, DDS, PhD,a Haldun Iplikçioglu, DDS, PhD,b and Murat C. Çehreli, DDS, PhDc
Faculty of Dentistry, Hacettepe University, Ankara, Turkey
Malaligned implants often complicate the clinical and laboratory procedures employed for the fabricationof superstructures. Due to improper load distribution, an overall increase in stress concentrations on sup-porting implants may occur; in the long run, this may compromise the maintenance of the bone-implantinterface. The utilization of surgical stents is imperative for optimum implant installation. This articledescribes a modified surgical stent that serves as a guide to proper mesiodistal paralleling of dentalimplants. (J Prosthet Dent 2002;87:233-5.)
A stent is an appliance used either for radi-ographic evaluation during treatment planning forimplant placement or during surgical procedures toprovide optimum implant placement.1 Correct posi-
tioning of dental implants is largely dependent on theexperience and attention of the surgeon since conven-tional surgical guides include a single-diameter guidechannel that allows only one drill to pass through.Utilization of such surgical guides may result inmalaligned implants, particularly in the posteriorregion when low bone density exists. Eventually,implant placement in a recipient site that does notcoincide with the predetermined 3-dimensionalimplant location2 may compromise the entire treat-ment.3
Osseointegration of implants is the most important
but not the only requirement for a successful implant-supported prosthesis. Several studies have demonstratedthat an esthetic4 and functional5 implant-supportedprosthesis depends on the optimal placement of osseointegrated implants. Dual-purpose stents can facil-itate correct implant placement.6 From a biomechanicalperspective, since the strains in bone around implantsappear to be below physiologic limits, it may be hypoth-esized that the angulation of a load-bearing implant inthe anterior region would not necessarily affect implantsuccess. Accordingly, implant failure specifically attrib-uted to malangulation is not reported for the anteriormaxillary region. The incidence of biomechanical failure
increases, however, for implant applications in the pos-terior region.8
Non-parallel placement of implants is the primary cause of nonaxial loading during function. Althoughoff-set loading is not the only factor that contributesto the loss of osseointegration,9 axial loading of implants should be provided if possible. Conventionalsurgical stents are frequently and efficiently used for
FEBRUARY 2002 THE JOURNAL OF PROSTHETIC DENTISTRY 233
aAssistant , Department of Prosthodontics.bAssociate Professor, Department of Prosthodontics.cAssistant , Department of Prosthodontics.
Fig 1. Diagnostic setup of planned implant-supported fixedpartial denture.
7/27/2019 A Surgical Guide for Accurate Mesiodistal Paralleling of Implants
http://slidepdf.com/reader/full/a-surgical-guide-for-accurate-mesiodistal-paralleling-of-implants 2/3
fixed partial denture planned for the mandibularposterior edentulous arch (Fig. 1).
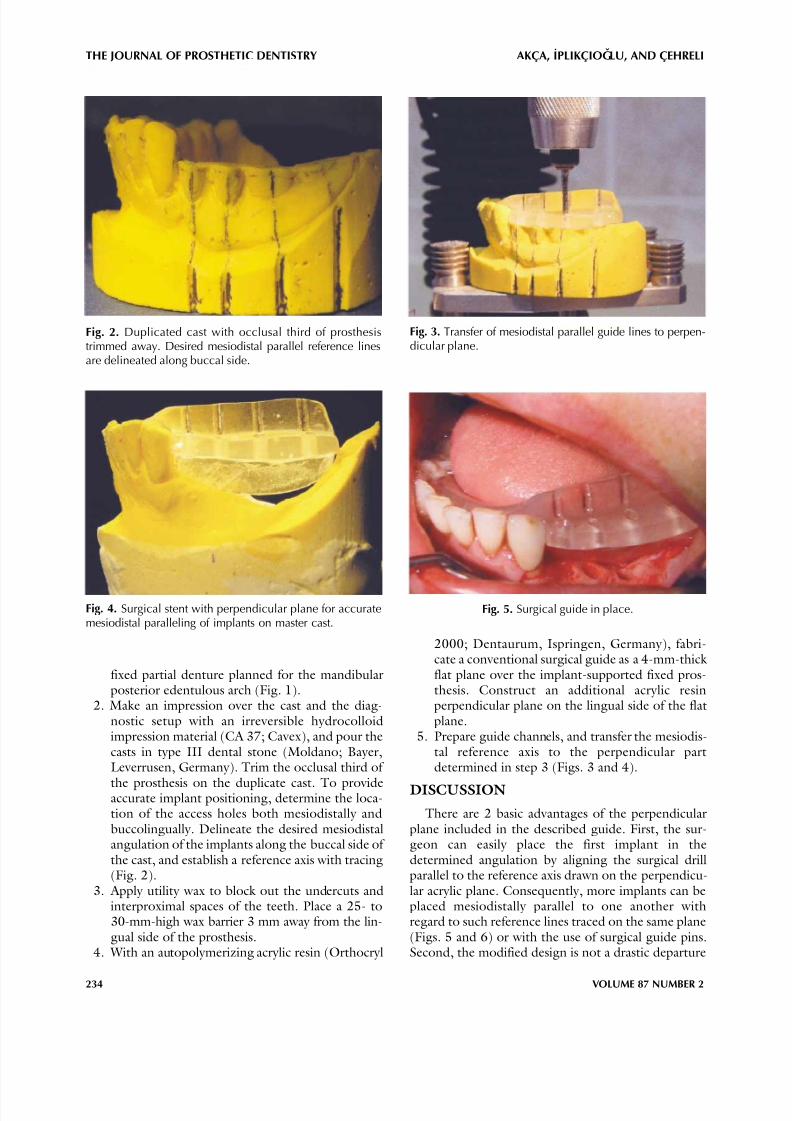
2. Make an impression over the cast and the diag-nostic setup with an irreversible hydrocolloidimpression material (CA 37; Cavex), and pour thecasts in type III dental stone (Moldano; Bayer,Leverrusen, Germany). Trim the occlusal third of
the prosthesis on the duplicate cast. To provideaccurate implant positioning, determine the loca-tion of the access holes both mesiodistally andbuccolingually. Delineate the desired mesiodistalangulation of the implants along the buccal side of the cast, and establish a reference axis with tracing(Fig. 2).
3. Apply utility wax to block out the undercuts andinterproximal spaces of the teeth. Place a 25- to30-mm-high wax barrier 3 mm away from the lin-gual side of the prosthesis.
4. With an autopolymerizing acrylic resin (Orthocryl
THE JOURNAL OF PROSTHETIC DENTISTRY AKÇA, IPLIKÇIOG ˇLU, AND ÇEHRELI
234 VOLUME 87 NUMBER 2
2000; Dentaurum, Ispringen, Germany), fabri-cate a conventional surgical guide as a 4-mm-thick flat plane over the implant-supported fixed pros-thesis. Construct an additional acrylic resinperpendicular plane on the lingual side of the flatplane.
5. Prepare guide channels, and transfer the mesiodis-tal reference axis to the perpendicular partdetermined in step 3 (Figs. 3 and 4).
DISCUSSION
There are 2 basic advantages of the perpendicularplane included in the described guide. First, the sur-geon can easily place the first implant in thedetermined angulation by aligning the surgical drillparallel to the reference axis drawn on the perpendicu-lar acrylic plane. Consequently, more implants can beplaced mesiodistally parallel to one another withregard to such reference lines traced on the same plane(Figs. 5 and 6) or with the use of surgical guide pins.Second, the modified design is not a drastic departure
Fig. 2. Duplicated cast with occlusal third of prosthesistrimmed away. Desired mesiodistal parallel reference linesare delineated along buccal side.
Fig. 3. Transfer of mesiodistal parallel guide lines to perpen-dicular plane.
Fig. 4. Surgical stent with perpendicular plane for accuratemesiodistal paralleling of implants on master cast.
Fig. 5. Surgical guide in place.

7/27/2019 A Surgical Guide for Accurate Mesiodistal Paralleling of Implants
http://slidepdf.com/reader/full/a-surgical-guide-for-accurate-mesiodistal-paralleling-of-implants 3/3
from conventional acrylic stents. Complicated stentdesigns may interfere with site preparation and cause
improper implant placement. The one feature addedto this modified stent is intended to facilitate ease inthe establishment of implant angulation. The perpen-dicular plane also retracts the mucoperiosteal flaplingually and provides improved visualization duringsite preparation. Thus, the design is user-friendly.
The inability to determine the buccolingual angula-tion of implants is the primary disadvantage of themodified stent. Buccolingual imaging of the bone with2-dimensional computed tomography, along with theuse of diagnostic stents with radiopaque markers, is themost accurate technique.11 However, even with this
approach, modification of the stent through accuratetransfer of the radiographic information is mandatory for surgical purposes.12
The width and angulation of available bone canserve as a useful and restrictive guide for establishingbuccolingual implant angulation. Wide residual ridgesthat allow various buccolingual angulations forimplant placement are uncommon. The high cost, lim-ited availability, and exposure to ionizing radiationassociated with computed tomography,13 in additionto the complicated procedures associated with many dual-purpose stents, all appear less necessary whenconventional radiographic techniques can reveal suffi-
cient residual bone dimensions for implant placement.SUMMARY
A modification of the conventional surgical stent formesiodistal implant parallelism has been described.
AKÇA, IPLIKÇIOG ˇLU, AND ÇEHRELI THE JOURNAL OF PROSTHETIC DENTISTRY
FEBRUARY 2002 235
When computerized tomography is not required toevaluate the buccolingual angulation of available bone,the simple design and function of the modified stentmake it advantageous for use in the posterior edentu-lous mandible.
REFERENCES
1. Verde MA, Morgano SM. A dual-purpose stent for the implant-supportedprosthesis. J Prosthet Dent 1993;69:276-80.
2. Takeshita F, Suetsugu T. Accurate presurgical determination for implantplacement by using computerized tomography scan. J Prosthet Dent1996;76:590-1.
3. Caplanis N, Kan JY, Lozada JL. Osseointegration: contemporary conceptsand treatment. J Calif Dent Assoc 1997;12:843-51.
4. Garber DA, Belser UC. Restoration-driven implant placement withrestoration-generated site development. Compend Contin Educ Dent1995;16:796-802, 804.
5. Taylor TD, Belser U, Mericske-Stern R. Prosthodontic considerations.Clin Oral Implants Res 2000;11(Suppl 1):101-7.
6. Cehreli MC, Sahin S. Fabrication of a dual-purpose surgical template forcorrect labiopalatal positioning of dental implants. Int J Oral MaxillofacImplants 2000;15:278-82.
7. Clelland NL, Gilat A, McGlumphy EA, Brantley WA. A photoelastic andstrain gauge analysis of angled abutments for an implant system. Int JOral Maxillofac Implants 1993;8:541-8.
8. Rangert B, Krogh PH, Langer B, Van Roekel N. Bending overload andimplant fracture: a retrospective clinical analysis. Int J Oral MaxillofacImplants 1995;10:326-34.
9. Taylor TD, Agar JR, Vogiatzi T. Implant prosthodontics: current perspec-tive and future directions. Int J Oral Maxillofac Implants 2000;15:66-75.
10. Lekholm U. Clinical procedures for treatment with osseointegrated den-tal implants. J Prosthet Dent 1983;50:116-20.
11. Schwarz MS, Rothman SL, Rhodes ML, Chafetz N. Computed tomogra-phy: Part I. Preoperative assessment of the mandible for endosseousimplant surgery. Int J Oral Maxillofac Implants 1987;2:137-41.
12. Cehreli MC, Aslan Y, Sahin S. Bilaminar dual-purpose stent for placementof dental implants. J Prosthet Dent 2000;84:55-8.
13. Clark DE, Danforth RA, Barnes RW, Burtch ML. Radiation absorbed fromdental implant radiography: a comparison of linear tomography, CT
scan, and panoramic and intra-oral techniques. J Oral Implantol1990;16:156-64.
Reprint requests to:
DR KIVANÇ AKÇA
ÇETIN EMEÇ BULVARI 6.CADDE 54/506460 ÖVEÇLER
ANKARA, TURKEY
FAX: (90)312-311-3741E-MAIL: [email protected]
Copyright © 2002 by The Editorial Council of The Journal of Prosthetic Dentistry.
0022-3913/2002/$35.00 + 0. 10/1/120900
doi:10.1067/mpr.2002.120900
Fig. 6. Mesiodistal angulation of implants on master cast.Note near-parallelism.