a not so minor problem.. presentor: angelo catacutan, md, mba moderator: dr. carmela kasala, md...
TRANSCRIPT

A Not So Minor Problem..
Presentor: Angelo Catacutan, MD, MBAModerator: Dr. Carmela Kasala, MDReactor: Dr. Joseph Vincent Alba, MD

Objectives
• To present a case of a newborn who presented with jaundice at <24 HOL
• To discuss the approach to a jaundiced newborn
• To discuss about alloimmune hemolytic anemia in the newborn, its manifestations, approach to diagnosis, treatment, and prevention

Patient Data
• K.M.• Newborn• Female• Filipino• DOB: June 15, 2013• Delivered via emergency CS
– (for repeat CS in labor)• Place of Birth: The Medical City
Chief Complaint
Jaundice

Maternal History
• 42 year old G4P4(4003)• Filipino• College graduate• Office worker• Non-smoker, non-alcoholic beverage
drinker

Maternal History
• Regular prenatal check-ups• OGCT screen normal• HBsAg nonreactive• Denies infection, exposure to viral
exanthems, teratogens, or radiation• Blood type B+

Maternal History
• Complete Blood Count
• Urinalysis
Hgb Hct WBC Neut Lymp Mono Eo Plt115 34 8.8 65 20 10 5 318
RBC WBC Epith CastBacteri
a
13 2 2 0 34

Family History
• (-) hypertension• (-) diabetes• (-) asthma• (-) atopy• (-) hematologic disorders

Obstetric History
• G1 (2000)– Female– Term, NSD at a local hospital– Live, with no problems

Obstetric History
• G2 (2005)– Female– Term, Primary CS for Cephalopelvic
disproportion– Died shortly after birth
• “congenital heart problem”
Obstetric History
• G3 (2006)– Female– Live, Term, Repeat CS – TMC– Diagnosis: Hemolytic Disease of the
Newborn• Underwent phototherapy, double-volume
exchange transfusion and IVIg infusion– No antibody identification done on the
mother

Obstetric History
• G4 (2013)– Present pregnancy

Physical Examination(upon birth)• General Status
– Clear amniotic fluid– No cord coil– Good cry and activity

Physical Examination(upon birth)• Blood Pressures:
– 68/41(right arm), 69/40 (left arm)– 63/48 (right foot), 67/36 (left foot)
• Cardiac rate: 146bpm• Respiratory Rate: 48/min• Temperature: 36.5˚C

Physical Examination(upon birth)• APGAR 9,9• Anthropometrics
– BW: 2850g (50th percentile)– BL: 49cm (40th percentile)– HC: 36cm (90th percentile)– CC: 33cm– AC: 27cm

Physical Examination(upon birth)• HEENT
– Patent nares, formed ears, (-) cleft lip/palate
• Pulmonary– No deformities, no retractions, good air
entry, equal breath sounds• Cardiac
– Adynamic precordium, normal cardiac rate, regular rhythm, (-) murmurs

Physical Examination(upon birth)• Abdominal
– Globular– Soft with no palpable masses– Umbilicus: 2 arteries, 1 vein
• Genitalia– Grossly female, no deformities
• Anus– patent
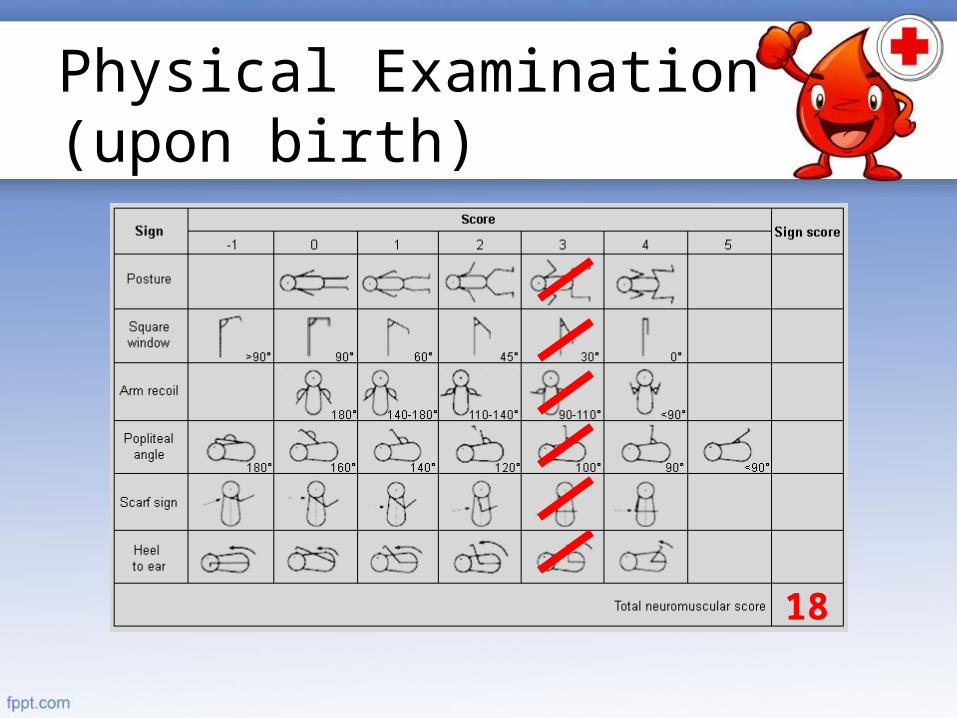
Physical Examination(upon birth)
18

Physical Examination(upon birth)
20

Physical Examination(upon birth)• Neuromuscular Maturity = 18• Physical Maturity = 20• Total Maturity Raiting = 38
• 39 Weeks• Appropriate for Gestational Age

Admitting Diagnosis
Live, term, baby girl, delivered via emergency repeat CS (for repeat CS
in labor) to a 42 year old G4P4 (4003) at 38 6/7 weeks AOG
BW 2850g BL 49cm HC 36cm CC 33cm AC 27cm. AS 9,9, MT 39 weeks
AGA

COURSE IN THE WARDS

Upon Delivery
• Essential newborn care rendered• Diagnostics:
– Blood typing– Hearing screening (24th – 48th HOL)– Newborn screening (24th – 48th HOL)

Upon Delivery
• Therapeutics: – Vitamin K 0.1mL/IM– Erythromycin eye ointment– Hepatitis B vaccine 0.5mL/IM
• Roomed-in at the 4th HOL• Exclusively breastfed
24th hour of life
Subjective
• Breastfed every 3 hours
• Good suck and activity
• Adequate UO• Meconium passage
Objective
• HR 132bpm, RR 34/min T 36.7C BP 70/40
• Weight: 2880g (+30g)
• Light jaundice to face
• Good air entry• Regular cardiac
rhythm• Soft abdomen• Full pulses
Assessment
• Term baby girl• t/c
Hyperbilirubinemia, unspecfied

35th hour of life
Subjective
• Breastfed every 3 hours
• Good suck and activity
• Adequate UO• Meconium passage
Objective
•HR 135bpm, RR 34/min T 37C BP 70/40•Generalized jaundice•Good air entry•Regular cardiac rhythm•Soft abdomen•Full pulses
Assessment
• Term baby girl• Hyperbilirubinema,
unspecified• R/O Sepsis
35th hour of life
Plan
• Transfer to NICU• Diagnostics:
• Bilirubin levels• CBCPC, Blood culture and sensitivity• CRP• Reticulocyte count• Maternal blood typing
• Therapeutics:• Single Phototherapy• IV fluids (50cc/kg/hr x 6 hours)• Continue oral feeding
• Refer to neonatology

Laboratories
Date Hgb Hct WBC Band Neu Lym Mon Eos Plt
6/16/13 118 35 15.2 02 71 21 4 2 325Macroc
ytic
Peripheral Blood Smear
Smear shows macrocytic RBCs. No abnormal WBCs. Adequate platelet.
CRP (0-0.5 mg/dL)
0.16 mg/dL
Reticulocyte count(0.005 – 0.015)
0.484
Blood Type
B+

42nd Hour of Life
TB mg/dL
DBmg/dL
IBmg/gL
42nd HOL
30.38 1.31 29.57High risk
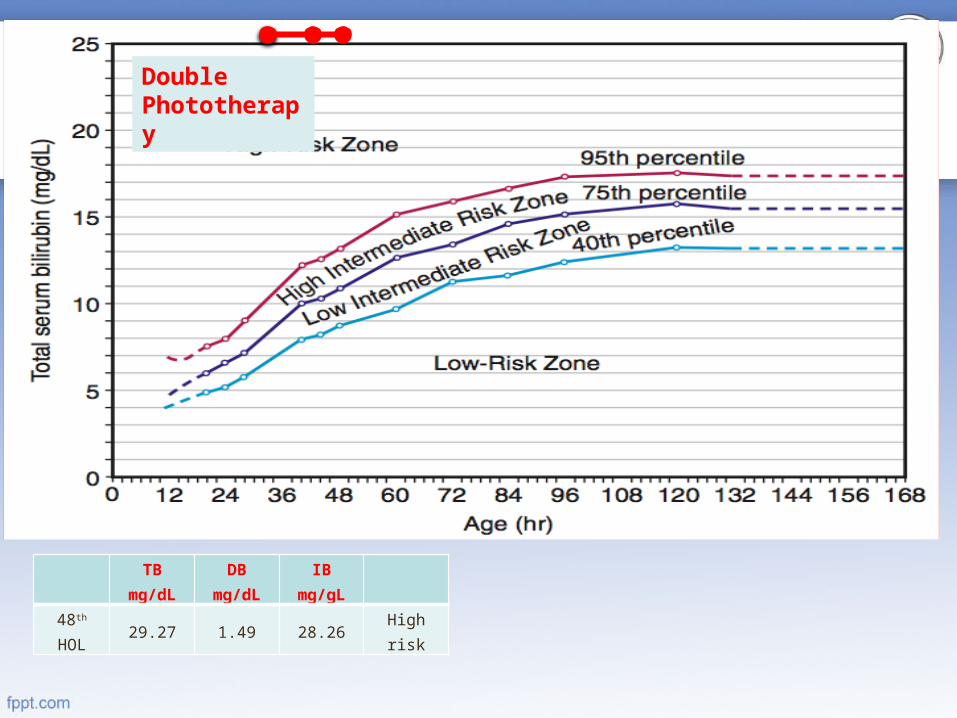
Plan: Double Phototherapy

42nd Hour of Life
• Persistently jaundiced• Repeat bilirubin levels extracted

42nd Hour of Life
TB mg/dL
DBmg/dL
IBmg/gL
42nd HOL
30.38 1.31 29.57 High risk
Double Phototherapy
48th Hour of Life
Subjective
• Good suck and activity
Objective
• Generalized jaundice
Assessment
• Hyperbilirubinemia• t/c Hemolytic
disease of the newborn
2nd Day of Life
Plan
• Diagnostics:• Coomb’s test (Direct and Indirect)• Repeat bilirubin levels• CBCPC
• Therapeutics:• Maintain Double Phototherapy• IV fluids• Continue oral feeding
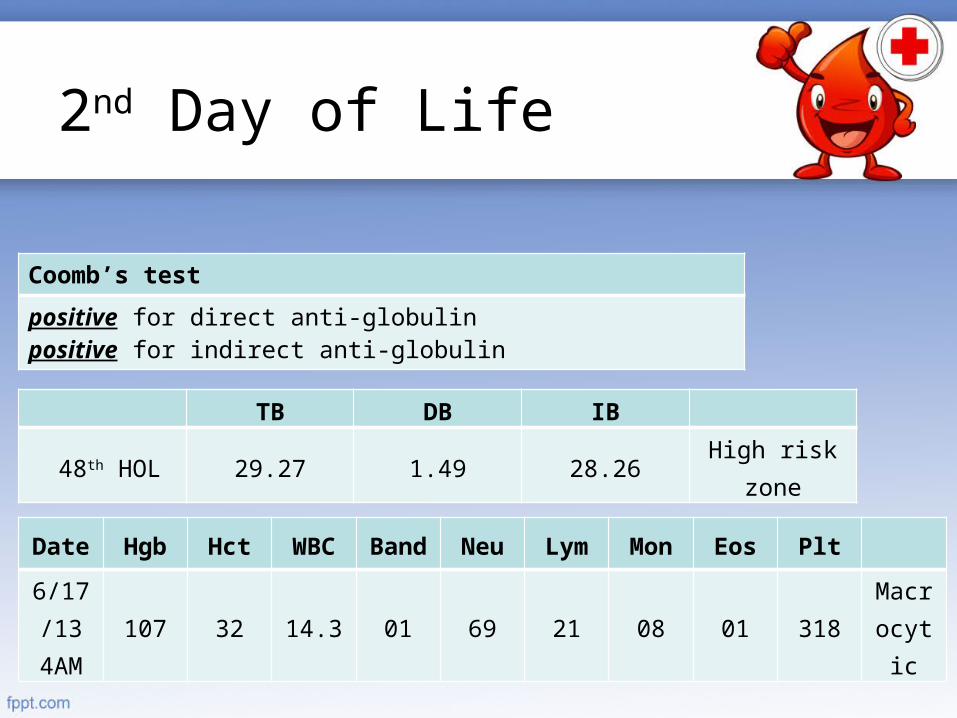
Coomb’s test
positive for direct anti-globulinpositive for indirect anti-globulin
TB DB IB
48th HOL 29.27 1.49 28.26High risk
zone
Date Hgb Hct WBC Band Neu Lym Mon Eos Plt
6/17/13 4AM
107 32 14.3 01 69 21 08 01 318Macrocytic
2nd Day of Life
42nd Hour of Life
TB mg/dL
DBmg/dL
IBmg/gL
48th HOL
29.27 1.49 28.26 High risk
Double Phototherapy

2nd Day of Life
Assessment
• Hemolytic Disease of the Newborn
Plan
• Double-volume exchange transfusion
• Human IVIg 1.5g/IV (526.3mg/kg/dose)
• Ampicillin (87.7 mkday) (post-DVET)
• Amikacin (10.52 mkday) (post-DVET)

For Double-VolumeExchange Transfusion• To use: type B whole blood <48
hours old, crossmatched with the mother’s blood– Not available in the blood bank
• Alternative: Reconstitued whole blood– Type O pRBC + type AB FFP,
crossmatched– 5 packs reactive
• IVIg 1.5g IV was started
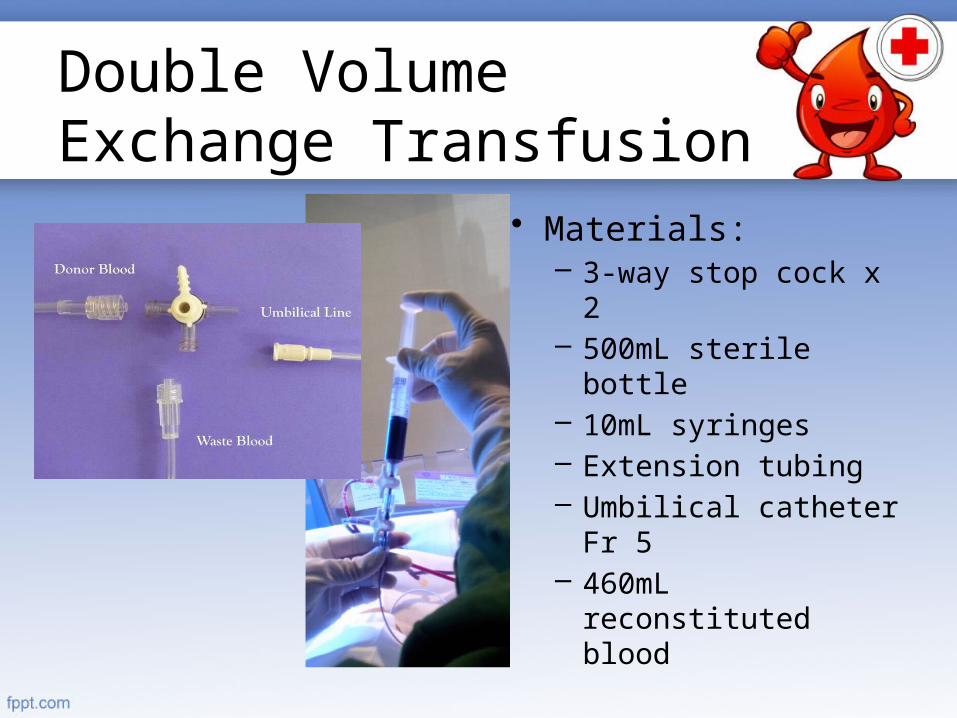
Double VolumeExchange Transfusion
• Materials:– 3-way stop cock x 2– 500mL sterile bottle– 10mL syringes– Extension tubing– Umbilical catheter
Fr 5– 460mL
reconstituted blood

Double VolumeExchange Transfusion
• Procedure– Umbilical vein
catheterization– 46 cycles, 10mL
per aliquot– VS every 15
minutes
Waste Blood Donor Blood

Post-Transfusion Plans
• To start Ampicillin and Amikacin for antibiotic coverage
• For repeat bilirubin levels 6 hrs post-transfusion
• Send maternal blood for antibody identification

6 Hours Post-Transfusion
TB DB IB
6/17/13 11pm67th HOL
16.41 mg/dL 0.93 15.75 High risk zone
Na mmol/L130 - 145
K mmol/L3.7 – 5.9
iCal mg/dL3.9 – 6.0
6/17/13 11pm 135 3.70 3.72
Date Hgb Hct WBC Band Neu Lym Mon Eos Plt
6/17 11pm
164 50 9 0 78 13 8 1 188

42nd Hour of Life
TB mg/dL
DBmg/dL
IBmg/gL
67th
HOL16.41 0.93 15.75
High risk zone
Double Phototherapy
DVET

3rd Day of Life
Subjective
• 20-40mL of milk
• Good suck and activity
Objective
• Jaundice to upper chest
• Mild bipedal edema
Assessment
• Hemolytic disease of the newborn
• s/p DVET
Plan
• Maternal antibody screening
• Repeat bilirubin levels
• 2nd dose of IVIG
• Continue Phototherapy

3rd Day of Life
TB DB IB
6/18/13 11am 79th HOL
15.94 mg/dL 0.88 15.32 HIRZ
Maternal antibody identification
Allo-anti EAllo anti-c

42nd Hour of Life
TB mg/dL
DBmg/dL
IBmg/gL
79th
HOL15.94 0.88 15.32
High inter-
mediate
Double Phototherapy
DVET
Double Phototherapy
42nd Hour of Life
TB mg/dL
DBmg/dL
IBmg/gL
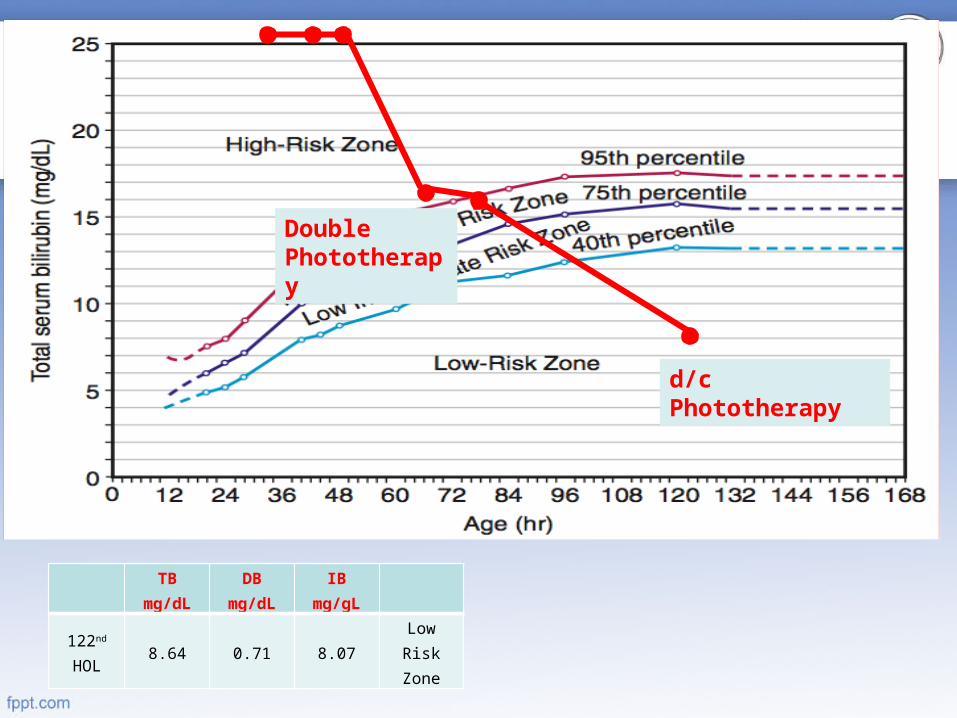
122nd
HOL8.64 0.71 8.07
Low Risk Zone
d/c Phototherapy
Double Phototherapy

5th Day of Life
Subjective
• Tolerates 30-60mL of milk
• Good suck and activity
• UO 2.8mL/kg/hr
• (+)BM
Objective
• Light jaundice to flexural areas
Assessment
• Hemolytic disease of the newborn
Plan
• Discharged

Final Diagnosis
Live, term, baby girl, delivered via emergency repeat CS (for repeat CS in labor) to a 42 year
old G4P4 (4003) at 38 6/7 weeks AOGBW 2850g BL 49cm HC 36cm CC 33cm AC
27cm. AS 9,9, MT 39 weeks AGA
Hemolytic Disesase of the Newborn secondary to Minor Rh Incompatibility
s/p Double-Volume Exchange Transfusions/p IVIg infusion

DISCUSSION

Salient Features
• Term, baby girl• Generalized jaundice before 24th HOL• Serum bilirubin levels of 34mg/dL• History of a sibling with history of
jaundice, underwent phototherapy, IVIg infusion, and exchange transfusion

JAUNDICE IN THE NEWBORN

Jaundice andHyperbilirubinemia• Yellow discoloration
of the skin secondary to deposition of bilirubin

Jaundice andHyperbilirubinemia• Etiology
– Increased bilirubin load / heme catabolism
– Decreased enzyme activity• Genetic predisposition• Competitive inhibition(drugs)
Nelson’s Textbook of Pediatrics 19th ed

Jaundice andHyperbilirubinemia
Jaundice
Physiologic Pathologic

Jaundice andHyperbilirubinemia
Physiologic• Appears at 2nd or 3rd
day of life
• Peaks at 2nd to 4th day of life
• Rises at a rate of <5mg/dL/day
Pathologic• Appears at the 24th
HOL or earlier– >12mg/dL in a term
infant– >10-14mg/dL in a
preterm infant• Persists to 10th-14th
day of life• Rises at a rate of
>5mg/dL/day
Nelson Textbook of Pediatrics, 19th ed,

AAP Guidelines. 2004
Approach to a Jaundiced Newborn

AAP Guidelines. 2004
Laboratory Evaluation

Nelson Textbook of Pediatrics, 19th ed,

Alloimmune HemolyticDisease of the Newborn• “Erythroblastosis Fetalis”• Destruction of RBC by maternal IgG
against RBC antigens that access the fetal circulation transplacentally– ABO, Rhesus (Rh factor), other blood
group antigens
Nelson Textbook of Pediatrics, 19th ed,

RBC Antigens
• Transmembrane proteins• Either synthesized by the RBC or
adsorbed from the plasma• 29 blood group systems• 250 antigens
Wintrobe’s Clinical Hematology, 12e. 2009

Rh Blood Group
• Discovered by Landsteiner and Weiner in 1940 from the rhesus monkey
• Has 3 nomenclature systems– Weiner system (Rh1, Rh2…)– Fisher-Race (Cc, Dd, Ee)– Rosenfield (Rho, rh’, rh’’…)
Wintrobe’s Clinical Hematology, 12e. 2009
Rh Blood Group
• Highly immunogenic (70%)• An individual is Rh+ if the RBC
expresses the D antigen• 50-70% of antibody response to Rh
antigens are due to the D antigen
Wintrobe’s Clinical Hematology, 12e. 2009

Rh Blood Group
AntigenCaucasian
sBlacks Asians
D 85% 92% 99%
C 68% 27% 93%
E 29% 22% 39%
c (little c) 80% 96% 47%
e (little e) 98% 98% 96%
Dean. Blood Groups and Red Cell Antigens. 2005
Prevalence of Rh Antigens in Racial Groups

HDN Caused byRh Incompatibility• Antibody formation when an Rh-
woman receives Rh+ blood (>1mL)• Once sensitization occurs, small
doses of Rh+ blood can increase titers (IgM and IgG)
Wintrobe’s Clinical Hematology, 12e. 2009
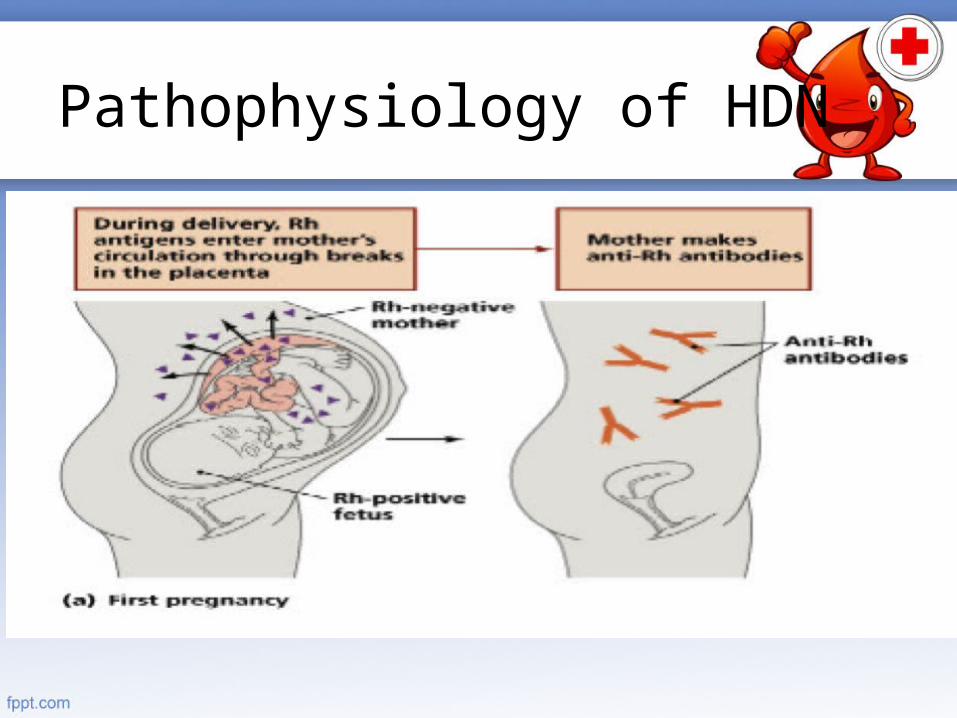
Pathophysiology of HDN

Pathophysiology of HDN

Rh and ABOIncompatibility• Concomitant ABO incompatibility is
protective against Rh sensitization– Confers almost ninefold protection– Rapid removal of fetal Rh+ from
maternal circulation
Wintrobe’s Clinical Hematology, 12e. 2009
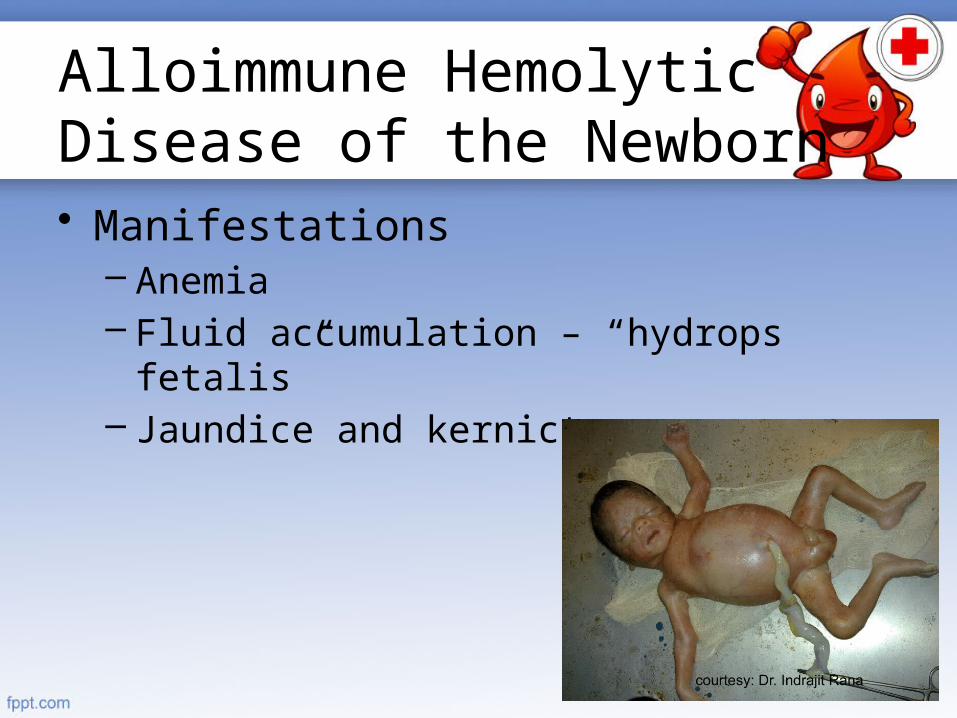
Alloimmune HemolyticDisease of the Newborn• Manifestations
– Anemia– Fluid accumulation – “hydrops fetalis”– Jaundice and kernicterus
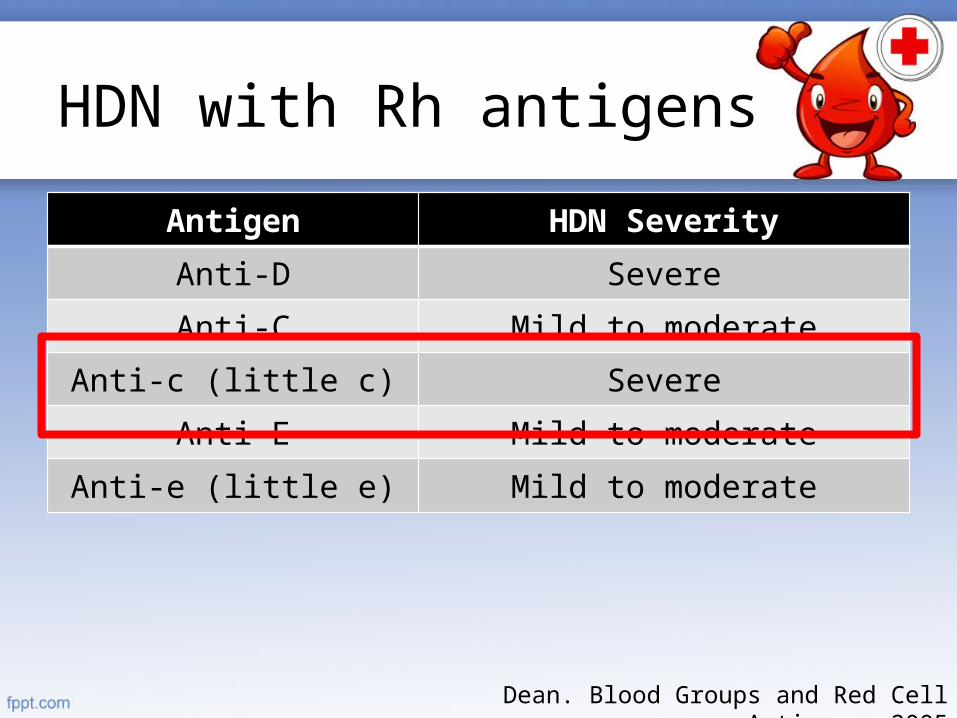
HDN with Rh antigens
Antigen HDN Severity
Anti-D Severe
Anti-C Mild to moderate
Anti-c (little c) Severe
Anti-E Mild to moderate
Anti-e (little e) Mild to moderate
Dean. Blood Groups and Red Cell Antigens. 2005
Alloimmune HemolyticDisease of the Newborn• Laboratory Evaluation
– Total serum bilirubin– CBC– Reticulocyte count– Direct Coomb’s test
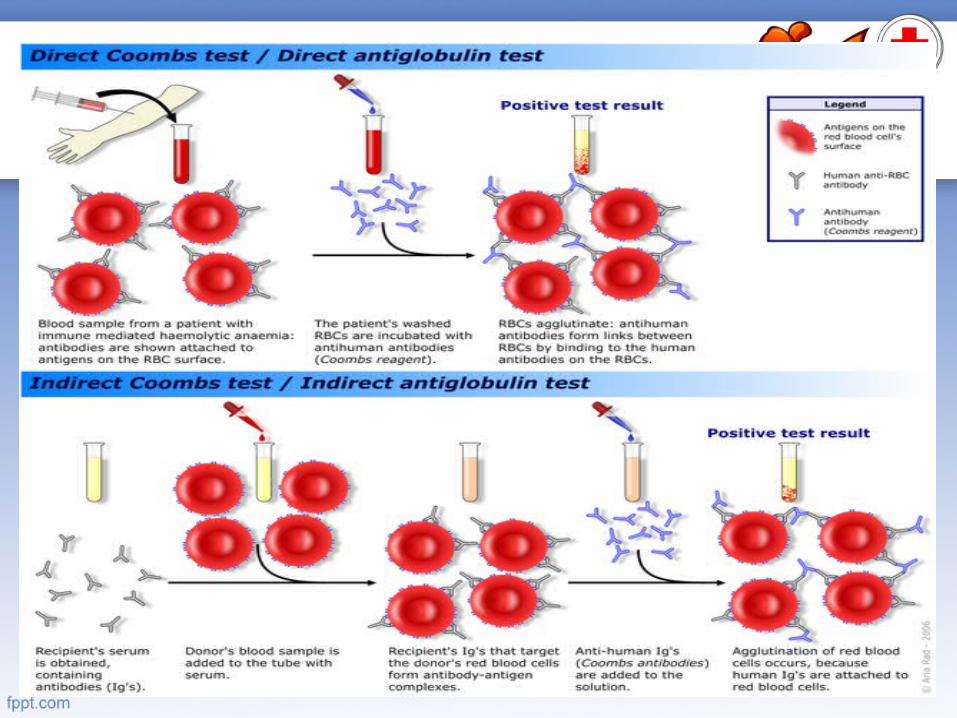
Coomb’s Test

Alloimmune HemolyticDisease of the Newborn• Antenatal Diagnosis
– Percutaneous umbilical blood sampling– Ultrasonography
• Definitive Diagnosis– Demonstration of blood incompatibility
antibody identification

Alloimmune HemolyticDisease of the Newborn• Treatment Goals
– Avoid intrauterine and extrauterine death from anemia and hypoxia
– Avoid neurotoxicity from hyperbilirubinemia

Treatment for HDN
• For unborn infants– Intravascular fetal transfusion
• For liveborn infants– Exchange Transfusion– Phototherapy– IV Immunoglobulins

Management ofJaundice and HDN• Phototherapy
– Exposure to high-intensity light to reduce indirect bilirubin levels
– Maximal at blue range (420-470nm)• 15-20cm from infant
– Photo-isomerization• 4Z,15Z-bili 4Z, 15E-bili

Management ofJaundice and HDN

Management ofJaundice and HDN• Complications of phototherapy
– Loose stools and rash due to porphyrinemia
– Dehydration– Retinal damage– Bronze baby syndrome – skin
discoloration

Management ofJaundice and HDN• Intravenous Immunoglobulin
– For isoimmune hemolytic disease– Recommended when
• serum bilirubin levels are increasing despite phototherapy
• Serum levels become close to exchange levels
– Dose: 0.5-1.0 g/kg/dose– Shown to have decreased the need for
exchange transfusion

Mechanism of Actionof IVIg

Management ofJaundice and HDN• Double-Volume Exchange Transfusion
– If intensive phototherapy fails to reduce bilirubin levels to non-ET requiring range
– removes about 60% of bilirubin from the plasma, • clearance of about 30 -40 % of the total
bilirubin
Gomella. Neonatology: Management, Procedures, On-Call Problems, Diseases, and Drugs

Management ofJaundice and HDN• Other indications of ET
– Sepsis– DIC– Metabolic disorders leading to severe
acidosis– Severe fluid or electrolyte imbalance– Polycythemia

Management ofJaundice and HDN• Double-Volume Exchange Transfusion
– RBC units should be O, Rh-, or ABO/Rh type specific blood, compatible with the mother’s serum

Management ofJaundice and HDN• Complications
• metabolic acidosis• electrolyte imbalance• Hypoglycemia• infection

6 Hours Post-Transfusion
TB DB IB
6/17/13 11pm67th HOL
16.41 mg/dL 0.93 15.75 High risk zone
Na mmol/L130 - 145
K mmol/L3.7 – 5.9
iCal mg/dL3.9 – 6.0
6/17/13 11pm 135 3.70 3.72
Date Hgb Hct WBC Band Neu Lym Mon Eos Plt
6/17 11pm
164 50 9 0 78 13 8 1 188

Management ofJaundice and HDN

Prevention of HDN fromRH Incompatibility• Early identification
– Pre-/Antenatal identification of antigens (i.e. Blood typing)
• Avoid further sensitization– Indirect Coomb’s test– Anti-D immunoglobulin (RhoGAM)– Family Planning

Prevention ofRh Sensitization• Human anti-D globulin (RhoGAM)
– eliminate ≈ 10 mL of potentially antigenic fetal cells from the maternal circulation

Prevention ofRh Sensitization (ACOG)• Antenatal
– 300µg RhIG IM at 28 wks AOG (unless father is known to be RhD-
• Postpartum– 300µg after delivery

Prevention ofRh Sensitization (RCOG)• Antenatal
– 100µg RhIG IM at 28 wks AOG (unless father is known to be RhD-
– 100µg at 34 wks AOG• Postpartum
– 100µg after delivery
• Same protective rates but more visits

What is our Role?

The Role of theGeneral Pediatrician• Advise regular follow-up• Repeat blood typing
– Especially on the 90-120th day post-transfusion
• Vaccinations– May be given– Measles or MMRV may have to be
delayed
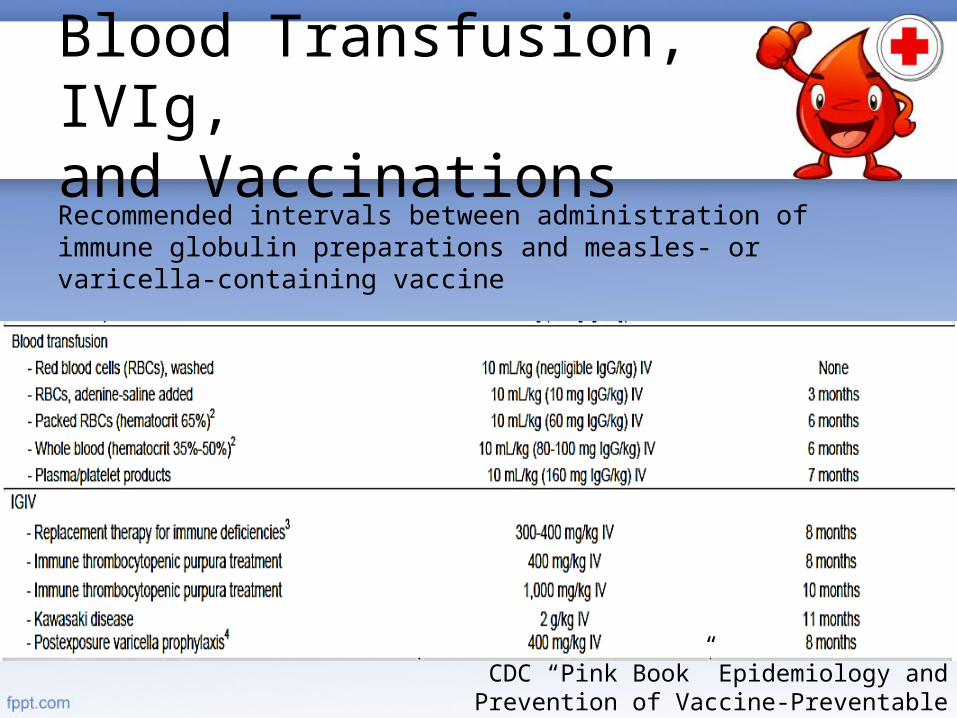
Blood Transfusion, IVIg,and VaccinationsRecommended intervals between administration of immune globulin preparations and measles- or varicella-containing vaccine
CDC “Pink Book” Epidemiology and Prevention of Vaccine-Preventable Diseases 12th ed. 2012

Patient Updates
• 4 months old – ~7kg• Has regular check-ups with her
attending pediatrician• Developmentally at par with age• No reports of recurrent jaundice or
anemia• Vaccinations are up-to-date

Summary
• Presented a case of a newborn who had early jaundice
• Discussed the approach on a jaundiced newborn
• Tackled on alloimmune hemolytic in the newborn, its manifestations, approach to diagnosis, treatment, and prevention

Thank You!