a further turkish case of griscelli syndrome with new rab27a mutation
TRANSCRIPT
Jason C. Sluzevich, MD, Hugh J. Gloster, MD, andDiya F. Mutasim, MD
Department of Dermatology, the University ofCincinnati College of Medicine
Funding sources: None.
Conflicts of interest: None declared.
Reprint requests: Hugh J. Gloster MD, Departmentof Dermatology, University of Cincinnati Collegeof Medicine, PO Box 670592, Cincinnati, OH45267-0592
REFERENCES
1. Papac RJ. Spontaneous regression of cancer: possible mecha-
nisms. In Vivo 1998;12:571-8.
2. Cerroni L, Peris K, Legge A, Chimenti S. Angiosarcoma of the
face and scalp: a case report with complete spontaneous
regression. J Dermatol Surg Oncol 1991;17:539-42.
3. Wilson Jones E. Malignant vascular tumors. Clin Exp Dermatol
1976;1:298-312.
4. Maddox JC, Evans HL. Angiosarcoma of skin and soft tissue:
a study of forty-four cases. Cancer 1981;48:1907-21.
5. Gunduz K, Shields JA, Shields CL, Eagle RC, Nathan F. Cutaneous
angiosarcoma with eyelid involvement. Am J Ophthalmol
1998;125:870-1.
doi:10.1016/j.jaad.2007.04.029
J AM ACAD DERMATOL
VOLUME 58, NUMBER 5
Letters S115
A further Turkish case of Griscelli syndromewith new RAB27A mutation
To the Editor: Griscelli syndrome (GS) is a rareautosomal recessive disorder characterized by partialalbinism, hepatosplenomegaly, variable cellular im-mune deficiency, and hemophagocytic lymphohis-tiocytosis.1 Similar features have been described intwo other syndromes, Chediak-Higashi syndromeand Elejalde syndrome. Differential diagnosis ofthese syndromes is given in Table I. Approximately50 cases with GS have been reported up date.2 GS iscaused by a defect in either the RAB27A or MYO5Agene.3 Patients with GS and MYO5A defect (type 1)show neurologic symptoms and no immunologicabnormalities whereas those with RAB27A defect(type 2) show immunodeficiency resulting in fatalhemophagocytic syndrome.4 Large, clumped mela-nosomes on microscopy of hair shafts are diagnosticin patients with GS. Bone-marrow transplantation isthe only curative treatment of the disease.
A 3-month-old boy was referred to our hospitalwith a high fever, hepatosplenomegaly, and abnor-mal hematologic parameters. His birth weight,length, and head circumference were normal. Hewas the first child of healthy parents. No consanguin-ity was described but both parents were from thesame small village. His postnatal course was normaluntil the age of 3 months.
On admission he had high fever, significant pallor,and silvery gray hair. Physical examination revealedhepatosplenomegaly (both liver and spleen werepalpable 8 cm below the costal margins). Otherwisehe was normal.
Laboratory tests showed a hemoglobin of 7.9 g/dL(9.5-14.5), hematocrit of 22.6% (31-41), leukocytecount of 3730 cells/mm3 (6000-18,000), and plateletsof 41,300 cells/mm3 (150,000-450,000). Serum bio-chemistry revealed a fibrinogen level of 114 mg/dL(200-400), total protein of 5 g/dL (6.1-7.9), albuminof 2.8 g/dL (3.9-5), lactate dehydrogenase of 773 U/L(180-430), alanine aminotransferase of 14 U/L (0-45),aspartate aminotransferase of 36 U/L (0-35), totalcholesterol of 84 mg/dL (0-200), and triglyceride of478 mg/dL (\150). On bone-marrow examinationhemophagocytosis without any evidence of infiltra-tive or malignant process was observed. The cere-brospinal fluid was normal. Serum IgG levels werenormal for his age whereas IgM and IgA levels wereslightly low.
Light microscope examination of the hair shaftshowed large aggregates of pigment granules con-sistent with GS (Fig 1). Chest radiography and thoraxcomputerized tomography showed pneumonic con-solidation in lungs. Cranial magnetic resonanceimaging showed patchy areas of altered signalintensity in both cerebral hemispheres and globuspallidus, suggestive of hemophagocytic lymphohis-tiocytic infiltration. With the clinical and laboratory
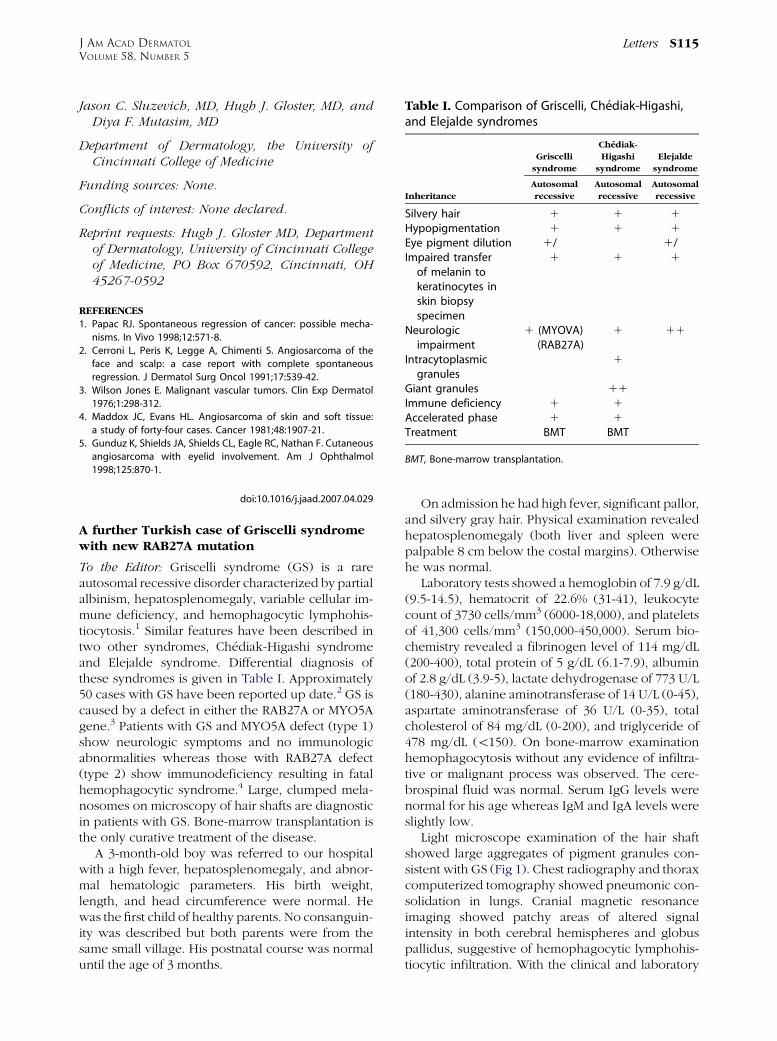
Table I. Comparison of Griscelli, Chediak-Higashi,and Elejalde syndromes
Griscelli
syndrome
Chediak-
Higashi
syndrome
Elejalde
syndrome
Inheritance
Autosomal
recessive
Autosomal
recessive
Autosomal
recessive
Silvery hair 1 1 1
Hypopigmentation 1 1 1
Eye pigment dilution 1/� � 1/�Impaired transfer
of melanin tokeratinocytes inskin biopsyspecimen
1 1 1
Neurologicimpairment
1 (MYOVA) 1 11
� (RAB27A)Intracytoplasmic
granules� 1 �
Giant granules � 11 �Immune deficiency 1 1 �Accelerated phase 1 1 �Treatment BMT BMT �
BMT, Bone-marrow transplantation.

A novel ATP2A2 missense mutationp.Asp254Gly in Darier disease restrictedto the extremities
To the Editor: Darier disease is an autosomal dom-inant hereditary skin disorder showing hyperkera-totic follicular papules distributed mainly on theseborrheic areas of the face, scalp, and trunk.1 Wereport here a Japanese female with Darier diseaseonly on her extremities. This patient harbored anovel ATP2A2 missense mutation.
A 34-year-old woman presented a 20-year historyof itchy and foul-smelling skin lesions which wereexacerbated during the summer months. She had nofamily history of skin disease. On physical examina-tion, irregular-shaped, slightly reddish, hyperkera-totic, malodorous plaques were seen restricted to theextremities, especially on the forearms and lowerlegs (Fig 1). The palms and soles were spared. Noeruptions were seen at the usual sites of Darierdisease, such as the face and over seborrheic regionsof the trunk. She exhibited neither neurologic norpsychiatric problems. Routine laboratory examina-tions revealed no remarkable abnormalities. A skinbiopsy was performed which histologically showedtypical features of Darier disease, including ortho-keratotic hyperkeratosis, suprabasal acantholysis,eosinophilic dyskeratotic cells in the spinous layers(corps ronds), and stratum corneum (grains; Fig 2,A). ATP2A2 mutation analysis using the patient’sgenomic DNA from peripheral blood cells revealeda novel missense mutation p.Asp254Gly (c.761A[G;Fig 2, B). This mutation was not found in 100 normal,unrelated Japanese alleles (50 individuals) by se-quence analysis, and was unlikely to be a polymor-phism. She was diagnosed with Darier disease andtreated with urea ointment, showing only a moderateresponse.
Darier disease is caused by mutations in ATP2A2,the gene encoding the sarco-endoplasimic reticu-lum calciumeATPase type 2 isoform (SERCA2).2
This Ca21 pump is thought to play a critical role inintracellular Ca21 signaling.3 ATP2A2 defects maydisturb cell-cell adhesion and keratinocyte differen-tiation and signalling.3 Andersen et al4 reported thatthe N-terminal half of the M3 domain comprising thethird transmembrane segment is involved in the
J AM ACAD DERMATOL
MAY 2008
S116 Letters
findings described above, the patient was given thediagnosis of GS type 2. Sequencing of the RAB27Agene showed a new homozygous mutation, 514 delCAAGC, in the sixth exon of the RAB27A gene. Bothparents were heterozygous for the same mutation.Interestingly, this new frame shift mutation is veryclose to the mutation 510delAAGCC, which wasdescribed before in identical Turkish twins.5
His pneumonic infiltration was treated with anti-biotics. Hemophagocytic syndrome responded wellto treatment with dexamethasone, etoposide, cyclo-sporine A, and blood transfusion. Bone-marrowtransplantation has been planned. The patient isnow 20 months old and on regular follow-up.
Huseyin Onay, MD, PhD,a Can Balkan, MD,b
Ozgur Cogulu, MD,a,b Yesim Aydinok, MD,b
Deniz Yılmaz Karapinar, MD,b and FerdaOzkinay, MDa,b
Departments of Medical Genetics a and Pediatrics,b
Ege University Faculty of Medicine, Izmir
Funding sources: None.
Conflicts of interest: None declared.
Reprint requests: Huseyin Onay, MD, PhD, EgeUniversitesi Tip Fakultesi, Tibbi Genetik Anabi-lim Dali, 35100 Bornova/Izmir Turkey
E-mail: [email protected]
REFERENCES
1. Griscelli C, Durandy A, Guy-Grand D, Daguillard F, Herzog C,
Prunieras M. A syndrome associating partial albinism and
immunodeficiency. Am J Med 1978;65:691-702.
2. Kurugol Z, Ozkinay F, Vardar F, Karacali S, Kutukculer N, Deveci
R, et al. Griscelli syndrome: report of a case and review of the
literature. Pediatr Int 2001;43:298-301.
3. Pastural E, Ersoy F, Yalman N, Wulffraat N, Grillo E, Ozkinay F,
et al. Two genes are responsible for Griscelli syndrome at the
same 15q21 locus. Genomics 2000;63:299-306.
Fig 1. Microscopic examination of hair showing aggrega-tion of large pigment granules. (Original magnification:3400.)
4. Malhotra AK, Bhaskar G, Nanda M, Kabra M, Singh MK, Ramam
M. Griscelli syndrome. J Am Acad Dermatol 2006;55:337-40.
5. Sarper N, Ipek IO, Ceran O, Karaman S, Bozaykut A, Inan S. A rare
syndrome in the differential diagnosis of hepatosplenomegaly
and pancytopenia: report of identical twins with Griscelli
disease. Ann Trop Paediatr 2003;23:69-73.
doi:10.1016/j.jaad.2007.05.002