99mtc-edda/hynic-toc and 18f-fdg in thyroid cancer patients with negative 131i whole-body scans
TRANSCRIPT
European Journal of Nuclear Medicine and Molecular Imaging Vol. 31, No. 3, March 2004
Abstract. Several studies have reported on the expres-sion of somatostatin receptors in patients with differenti-ated thyroid cancer (DTC). The aim of this study was toevaluate the imaging abilities of a recently developedtechnetium-99m labelled somatostatin analogue, 99mTc-EDDA/HYNIC-TOC (99mTc-TOC), in terms of preciselocalisation of disease. The study population comprised54 patients (24 men, 30 women; age range 22–90 years)with histologically confirmed DTC who presented withrecurrent or persistent disease as indicated by elevatedTg levels after initial treatment. All patients were nega-tive on the iodine-131 post-therapy whole-body scans.Fluorine-18 fluorodeoxyglucose positron emission to-mography (18F-FDG PET) was performed in a subgroupof 36 patients. The study population consisted of twogroups: Group A (n=22) comprised patients with diseaserecurrence as shown by elevated Tg levels but withoutdetectable pathology. In group B (n=32), pre-existing le-sions were known. Among the 54 cases, SSTR scintigra-phy was true positive in 33 (61.1%), true negative in 4(7.4%) and false negative in 17 (31.5%) cases, which re-sulted in a sensitivity of 66%. A total of 138 tumour fociwere localised in 33 patients. The fraction of true posi-tive 99mTc-TOC findings was positively correlated(P<0.01) with elevated Tg levels (higher than 30 ng/ml).Despite two false positive findings, analysis on a lesionbasis demonstrated better diagnostic efficacy with 18F-FDG PET (P<0.001); however, it also revealed substan-tial agreement between the imaging techniques [Cohen’skappa of 0.62 (0.47–0.78)]. In conclusion, scintigraphywith 99mTc-TOC might be a promising tool for treatmentplanning; it is easy to perform and showed sufficient ac-
curacy for localisation diagnostics in thyroid cancer pa-tients with recurrent or metastatic disease.
Keywords: Technetium-99m – Somatostatin – Tyrosine-octreotide – Scintigraphy – FDG-PET – Thyroid carci-noma
Eur J Nucl Med Mol Imaging (2004) 31:330–341DOI 10.1007/s00259-003-1376-x
Introduction
The overall prognosis of differentiated thyroid carcino-ma (DTC) is generally rather good, with low metastaticpotential and a high chance of definitive cure [1]; how-ever, carcinoma type, stage and histological grading in-fluence the individual outcome. Therefore, clinical sur-veillance after surgery and radio-ablation is very impor-tant for early detection of residual disease or recurrence.For this purpose, thyroglobulin (Tg) measurement hasbecome a very important clinical tool. Tg determinationis considered the most sensitive and specific marker ofDTC [2, 3, 4]. If laboratory monitoring shows increasingTg levels or other conventional imaging modalities aresuspicious for tumour recurrence, iodine-131 (131I) stud-ies under TSH stimulation (either after withdrawal of L-thyroxine therapy or after recombinant human TSH stim-ulation) are required. In the event of pathological uptake,patients may undergo administration of high-dose radio-iodine therapy. Importantly, detectable serum Tg levelsnot infrequently occur in association with negative 131Iwhole-body scans in patients with DTC. If malignant le-sions are no longer taking up radioiodine, many othertechniques are used for precise localisation of malignantfoci, since the treatment regimen of thyroid carcinomapatients especially depends on the size and extent of tu-mour when detected [5]. For localisation diagnostics atan early stage, especially if radioiodine scanning is nega-
Michael Gabriel (✉)Department of Nuclear Medicine, University of Innsbruck, Anichstrasse 35, 6020 Innsbruck, Austriae-mail: [email protected].: +43-512-5042677, Fax: +43-512-5042683
Original article
99mTc-EDDA/HYNIC-TOC and 18F-FDG in thyroid cancer patientswith negative 131I whole-body scansMichael Gabriel1, Franz Froehlich1, Clemens Decristoforo1, Christian Ensinger2, Eveline Donnemiller1, Elisabeth von Guggenberg1, Dirk Heute1, Roy Moncayo1
1 Department of Nuclear Medicine, University of Innsbruck, Innsbruck, Austria2 Department of Pathology, University of Innsbruck, Austria
Received: 9 August 2003 / Accepted: 1 October 2003 / Published online: 19 November 2003© Springer-Verlag 2003

331
European Journal of Nuclear Medicine and Molecular Imaging Vol. 31, No. 3, March 2004
tive, fluorine-18 fluorodeoxyglucose positron emissiontomography (18F-FDG PET) has already proven of value[6, 7, 8], even when other diagnostic procedures [ultra-sound, computed tomography (CT), magnetic resonanceimaging (MRI)] are normal. Therefore, 18F-FDG PET,which characterises hypermetabolic tumour tissue, hasgained widespread acceptance as a very sensitive methodin the follow-up of thyroid cancer patients, although itremains an expensive procedure which is not easilyavailable and needs adequate preparation of patients, i.e.a fasting period of at least 6 h before PET scanning. Be-sides 18F-FDG, other unspecific oncotropic radiopharma-ceuticals, e.g. 99mTc-sestamibi or 99mTc-tetrofosmin, areused for the diagnosis of recurrent and metastatic disease[9, 10, 11]. The uptake mechanism of these lipophiliccationic agents is different from that of 18F-FDG, in thataccumulation occurs within the mitochondria. These99mTc-labelled tracers are advantageous in terms of avail-ability and performance, i.e. results are independent ofthe blood glucose level, preparation is simple and the ra-diation dose is lower. However, sensitivity and specifici-ty are moderate compared with other imaging techniquesused for the follow-up of thyroid cancer [12, 13].
Another approach for localisation diagnostics is basedon specific binding of radiopharmaceuticals on somato-statin receptor (SSTR)-expressing tumour lesions. SSTRscintigraphy has become a reliable, non-invasive andhighly sensitive procedure for detection of a variety ofendocrine and non-endocrine tumours [14, 15, 16, 17,18].
Several studies have also reported on the expressionof somatostatin receptors in DTC [19, 20, 21, 22, 23, 24,25, 26, 27] using 111In-DTPA-octreotide (Octreoscan) asthe gold standard in SSTR scintigraphy. However, someresults of these studies were not clearly convincing, sothere is still no consensus concerning the clinical valueof this technique. Taking into consideration that smalland heterogeneous patient groups were investigated, i.e.several tumour types and grades showing different io-dine avidity were included, the differences might havebeen largely related to variable and sometimes decreaseddensity of somatostatin receptors in these tumours [28].For our study a new 99mTc-labelled compound, 99mTc-EDDA/HYNIC-TOC (99mTc-TOC), with high SSTR-af-finity, was used [29, 30]. The favourable imaging prop-erties of 99mTc-TOC as compared with 111In-DTPA-oct-reotide [31] makes this radiopharmaceutical a good can-didate for visualisation of SSTR-expressing tumours, es-pecially those with variable and lower receptor expres-sion. 99mTc-TOC combines advantages of improvedpharmacokinetics with higher spatial resolution due tothe use of the 99mTc label. The purpose of this study wasto evaluate the efficacy of the new 99mTc-labelled com-pound for detection of SSTR-positive lesions in a largerseries of patients with recurrent or metastatic disease asshown by elevated Tg levels. All patients were negativein the post-therapy whole-body radioiodine scans. In a
subset of patients we prospectively compared the SSTRprofile with the metabolic pattern using 18F-FDG PET inorder to obtain a more complete biochemical understand-ing of the disease.
Materials and methods
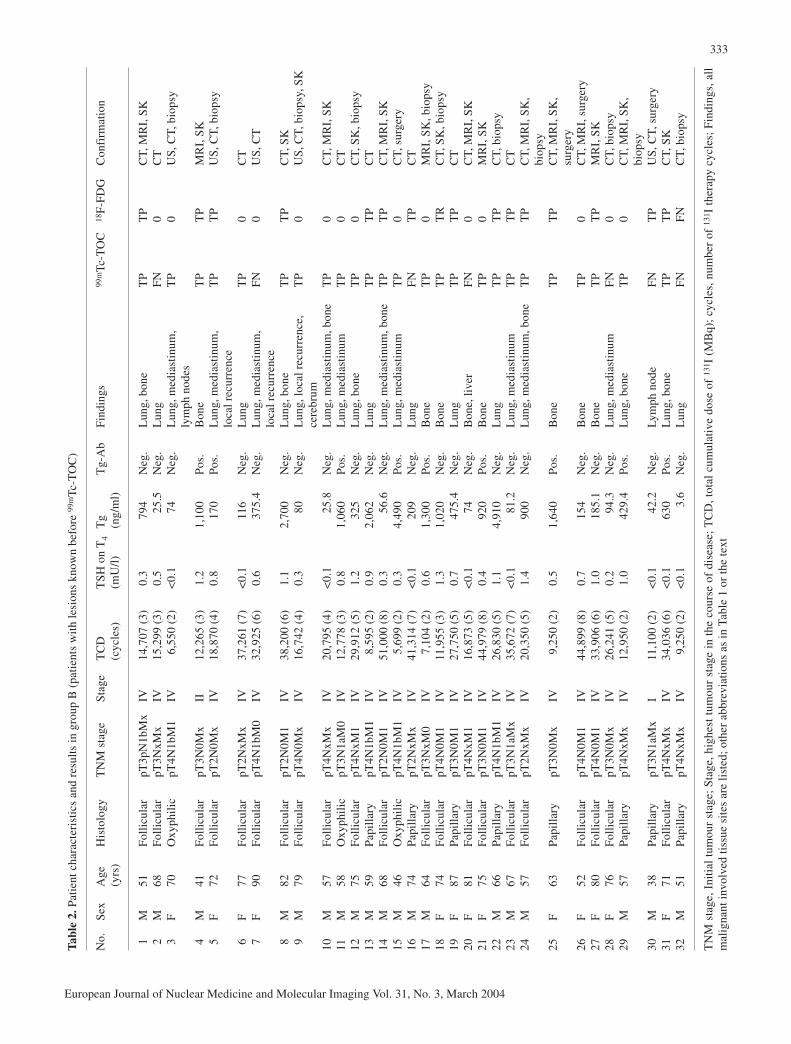
Patient eligibility criteria. Fifty-four patients (24 men, 30 women;age range 22–90 years; mean age ± SD, 63.9±15.9 years) with his-tologically confirmed DTC were included for localisation diagnos-tics. The patients had undergone near-total thyroidectomy and ra-dioactive ablation of the remnants and presented with either recur-rent or persistent disease as indicated by elevated Tg levels. Allpatients showed negative results of 131I post-therapy whole-bodyscans performed within 3 months prior to scintigraphy with 99mTc-TOC. The study population was subdivided into two groups:Group A (n=22) comprised patients with disease recurrence asshown by elevated Tg levels in serum for a minimum of two ob-servations but without detectable pathology. Group B (n=32) con-sisted of patients with pre-existing lesions. Out of the 54 patients,32 suffered from follicular, 16 from papillary and 6 from Hürthlecell carcinoma. The TNM classification according to Union Inter-nationale Contre Cancer (UICC) [32], edition 1997, was used toclassify the primary tumour. Initial pathologic tumour stages wereas follows: T2 in 11 patients, T3 in 22 patients and T4 in 21 pa-tients. The lymph node status was as follows: 21 patients werenode negative (N0), 12 patients were node positive (N1a=3, andN1b=9), and 21 patients had no information concerning lymphnode metastasis (Nx). Among the 54 patients, 13 initially had dis-tant metastases (M1). The clinical staging represented the higheststage achieved during the patient’s course and was determined ac-cording to the American Joint Committee on Cancer (AJCC) clas-sification [33]; stage I was present in 5 patients, stage II in 3 pa-tients, stage III in 4 patients to stage IV in 42 patients. Patientcharacteristics are given in Tables 1 and 2. The study was ap-proved by the local ethical committee and was performed in accor-dance with the Declaration of Helsinki. All patients gave theirwritten informed consent to participation.
Pretreatment evaluation and post-therapy scanning. Because ofincreasing serum Tg levels during TSH suppression, patients werereferred to our department for administration of high-dose radioio-dine therapy under TSH stimulation (in 41 patients 4 weeks afterL-thyroxine withdrawal and in 13 patients after recombinant hu-man TSH stimulation). X-ray of the chest and ultrasound of theneck were regularly performed in all patients, and CT of the chest(without contrast medium) was obtained in 24 patients. It was thesecond therapy for 15 patients, the third for 9, the fourth for 7, thefifth for 7, the sixth for 10, the seventh for 3 and the eighth for 3.Whole-body scans were carried out with a double-headed camera(Elscint HELIX, Haifa, Israel) 4–6 days after the therapeutic doseusing a high-energy collimator. Whole-body scan results werenegative.
Radiopharmaceutical. 99mTc-EDDA/HYNIC-TOC was preparedas recently described [29]. Briefly, 20 µg HYNIC-TOC was heatedwith 10 mg EDDA, 20 mg tricine, 15 µg stannous chloride dihy-drate and 1 GBq 99mTc-pertechnetate in 2 ml 0.05 M phosphatebuffer pH 6 at 100°C for 10 min. The solution was purified usinga SepPak mini cartridge (Waters, Milford, Mass., USA) elutedwith 80% ethanol and diluted with 5 ml saline. The purified radio-

332
European Journal of Nuclear Medicine and Molecular Imaging Vol. 31, No. 3, March 2004
Tab
le1.
Pat
ient
cha
ract
eris
tics
and
res
ults
in g
roup
A (
pati
ents
wit
hout
det
ecta
ble
path
olog
y pr
ior
to 9
9mTc
-TO
C)
No.
Sex
Age
H
isto
logy
TN
M s
tage
Sta
geT
CD
(cy
cles
)T
SH
on
T4
Tg
on T
4T
g-A
bF
indi
ngs
99m
Tc-T
OC
18F
-FD
GC
onfi
rmat
ion
(yrs
)(m
U/l
)(n
g/m
l)
1F
77F
olli
cula
rpT
3N0M
xIV
22,7
47 (
4)0.
340
1.2
Neg
.L
ung
FN
TP
CT
2F
70P
apil
lary
pT3a
NxM
xIV
19,7
50 (
4)<
0.1
32.8
Neg
.M
edia
stin
umF
NT
PB
iops
y3
M22
Pap
illa
rypT
2NxM
xI
29,8
44 (
6)0.
580
.5N
eg.
Lym
ph n
ode
FN
0U
S, s
urge
ry4
F66
Fol
licu
lar
pT2N
xMx
IV24
,536
(5)
0.3
1,95
0N
eg.
Lun
gT
PT
PC
T, b
iops
y5
F75
Fol
licu
lar
pT2N
xMx
IV27
,780
(6)
0.6
283.
3N
eg.
Med
iast
inum
FN
TP
Bio
psy
6M
42O
xyph
ilic
pT4N
xMx
II27
,280
(6)
<0.
19.
1N
eg.
Med
iast
inum
FN
TP
Bio
psy
7F
74F
olli
cula
rpT
3N0M
xIV
17,5
52 (
4)<
0.1
5.2
Neg
.L
ung
FN
FN
CT
8F
39P
apil
lary
pT3N
xMx
I5,
631
(2)
0.3
16N
eg.
Loc
al r
ecur
renc
eF
NT
PU
S, s
urge
ry9
F77
Oxy
phil
icpT
2NxM
xIV
22,2
00 (
4)0.
461
.8N
eg.
Med
iast
inum
TP
TP
Sur
gery
10M
44P
apil
lary
pT4N
1bM
xIV
14,8
00 (
3)1.
065
0N
eg.
Lym
ph n
ode
TP
0U
S, s
urge
ry11
M53
Pap
illa
rypT
3N0M
0IV
15,8
91 (
3)<
0.1
13.4
Neg
.L
ymph
nod
eT
PT
PU
S, s
urge
ry12
F85
Fol
licu
lar
pT3N
1bM
0IV
29,6
75 (
6)<
0.1
67N
eg.
Lym
ph n
ode
TP
0U
S, s
urge
ry13
F59
Fol
licu
lar
pT3N
0M0
IV10
,954
(2)
0.3
22.4
Neg
.L
ung,
med
iast
inum
FN
FN
CT
14F
24P
apil
lary
pT4N
0M0
I9,
749
(2)
<0.
110
.4N
eg.
Loc
al r
ecur
renc
eT
P0
Sur
gery
15F
72F
olli
cula
rpT
3N0M
0IV
28,1
73 (
6)0.
549
7.5
Neg
.B
one
TP
TP
MR
I, S
K16
F60
Fol
licu
lar
pT4N
0M0
III
11,6
00 (
2)0.
49.
4N
eg.
No
TN
FP
15-m
onth
FU
17F
52P
apil
lary
pT4N
1bM
xII
I10
,034
(2)
0.1
11.5
Neg
.N
oT
NT
N12
-mon
th F
U18
F90
Fol
licu
lar
pT3N
0M0
IV13
,657
(3)
<0.
136
.8N
eg.
Lun
gF
NF
NC
T19
F63
Fol
licu
lar
pT4N
0M0
III
33,9
06 (
6)<
0.1
24.8
Neg
.L
ocal
rec
urre
nce
FN
TP
Sur
gery
20F
34P
apil
lary
pT2N
xMx
I5,
343
(2)
<0.
17
Neg
.N
oT
NF
P13
-mon
th F
U21
M72
Oxy
phil
icpT
3NxM
xII
I5,
550
(2)
0.5
1,03
0N
eg.
Loc
al r
ecur
renc
e,
TP
TP
Bio
psy
lym
ph n
ode
22F
72F
olli
cula
rpT
3NxM
xII
12,6
43 (
3)<
0.1
13.2
Neg
.N
oT
NT
N15
-mon
th F
U
TN
M s
tage
, In
itia
l tu
mou
r st
age;
Sta
ge,
high
est
tum
our
stag
e in
the
cou
rse
of d
isea
se;
TC
D,
tota
l cu
mul
ativ
e do
se o
f 13
1 I (
MB
q);
cycl
es,
num
ber
of 1
31I
ther
apy
cycl
es;
Fin
d-in
gs,
all
mal
igna
nt i
nvol
ved
tiss
ue s
ites
; F
U,
foll
ow-u
p.F,
Fem
ale;
M,
mal
e; T
CD
, to
tal
cum
ulat
ive
dose
of
131 I
; T4,
thyr
oxin
e; T
g, th
yrog
lobu
lin;
TP,
true
pos
itiv
e; T
N, t
rue
neg-
ativ
e; F
P, f
alse
pos
itiv
e; F
N, f
alse
neg
ativ
e; F
U, f
ollo
w-u
p; S
K, b
one
scin
tigr
aphy
; ot
her
abbr
evia
tion
s as
def
ined
in th
e te
xt
333
European Journal of Nuclear Medicine and Molecular Imaging Vol. 31, No. 3, March 2004
Tab
le2.
Pat
ient
cha
ract
eris
tics
and
res
ults
in g
roup
B (
pati
ents
wit
h le
sion
s kn
own
befo
re 9
9mTc
-TO
C)
No.
Sex
Age
H
isto
logy
TN
M s
tage
Sta
geT
CD
T
SH
on
T4
Tg
Tg-
Ab
Fin
ding
s99
mTc
-TO
C18
F-F
DG
Con
firm
atio
n(y
rs)
(cyc
les)
(mU
/l)
(ng/
ml)
1M
51F
olli
cula
rpT
3pN
1bM
xIV
14,7
07 (
3)0.
379
4N
eg.
Lun
g, b
one
TP
TP
CT,
MR
I, S
K2
M68
Fol
licu
lar
pT3N
xMx
IV15
,299
(3)
0.5
25.5
Neg
.L
ung
FN
0C
T3
F70
Oxy
phil
icpT
4N1b
M1
IV6,
550
(2)
<0.
174
Neg
.L
ung,
med
iast
inum
, T
P0
US
, CT,
bio
psy
lym
ph n
odes
4M
41F
olli
cula
rpT
3N0M
xII
12,2
65 (
3)1.
21,
100
Pos
.B
one
TP
TP
MR
I, S
K5
F72
Fol
licu
lar
pT2N
0Mx
IV18
,870
(4)
0.8
170
Pos
.L
ung,
med
iast
inum
, T
PT
PU
S, C
T, b
iops
ylo
cal r
ecur
renc
e6
F77
Fol
licu
lar
pT2N
xMx
IV37
,261
(7)
<0.
111
6N
eg.
Lun
gT
P0
CT
7F
90F
olli
cula
rpT
4N1b
M0
IV32
,925
(6)
0.6
375.
4N
eg.
Lun
g, m
edia
stin
um,
FN
0U
S, C
Tlo
cal r
ecur
renc
e8
M82
Fol
licu
lar
pT2N
0M1
IV38
,200
(6)
1.1
2,70
0N
eg.
Lun
g, b
one
TP
TP
CT,
SK
9M
79F
olli
cula
rpT
4N0M
xIV
16,7
42 (
4)0.
380
Neg
.L
ung,
loca
l rec
urre
nce,
T
P0
US
, CT,
bio
psy,
SK
cere
brum
10M
57F
olli
cula
rpT
4NxM
xIV
20,7
95 (
4)<
0.1
25.8
Neg
.L
ung,
med
iast
inum
, bon
eT
P0
CT,
MR
I, S
K11
M58
Oxy
phil
icpT
3N1a
M0
IV12
,778
(3)
0.8
1,06
0P
os.
Lun
g, m
edia
stin
umT
P0
CT
12M
75F
olli
cula
rpT
4NxM
1IV
29,9
12 (
5)1.
232
5N
eg.
Lun
g, b
one
TP
0C
T, S
K, b
iops
y13
M59
Pap
illa
rypT
4N1b
M1
IV8,
595
(2)
0.9
2,06
2N
eg.
Lun
gT
PT
PC
T14
M68
Fol
licu
lar
pT2N
0M1
IV51
,000
(8)
0.3
56.6
Neg
.L
ung,
med
iast
inum
, bon
eT
PT
PC
T, M
RI,
SK
15M
46O
xyph
ilic
pT4N
1bM
1IV
5,69
9 (2
)0.
34,
490
Pos
.L
ung,
med
iast
inum
TP
0C
T, s
urge
ry16
M74
Pap
illa
rypT
2NxM
xIV
41,3
14 (
7)<
0.1
209
Neg
.L
ung
FN
TP
CT
17M
64F
olli
cula
rpT
3NxM
0IV
7,10
4 (2
)0.
61,
300
Pos
.B
one
TP
0M
RI,
SK
, bio
psy
18F
74F
olli
cula
rpT
4N0M
1IV
11,9
55 (
3)1.
31,
020
Neg
.B
one
TP
TR
CT,
SK
, bio
psy
19F
87P
apil
lary
pT3N
0M1
IV27
,750
(5)
0.7
475.
4N
eg.
Lun
gT
PT
PC
T20
F81
Fol
licu
lar
pT4N
xM1
IV16
,873
(5)
<0.
174
Neg
.B
one,
live
rF
N0
CT,
MR
I, S
K21
F75
Fol
licu
lar
pT3N
0M1
IV44
,979
(8)
0.4
920
Pos
.B
one
TP
0M
RI,
SK
22M
66P
apil
lary
pT4N
1bM
1IV
26,8
30 (
5)1.
14,
910
Neg
.L
ung
TP
TP
CT,
bio
psy
23M
67F
olli
cula
rpT
3N1a
Mx
IV35
,672
(7)
<0.
181
.2N
eg.
Lun
g, m
edia
stin
umT
PT
PC
T24
M57
Fol
licu
lar
pT2N
xMx
IV20
,350
(5)
1.4
900
Neg
.L
ung,
med
iast
inum
, bon
eT
PT
PC
T, M
RI,
SK
, bi
opsy
25F
63P
apil
lary
pT3N
0Mx
IV9,
250
(2)
0.5
1,64
0P
os.
Bon
eT
PT
PC
T, M
RI,
SK
, su
rger
y26
F52
Fol
licu
lar
pT4N
0M1
IV44
,899
(8)
0.7
154
Neg
.B
one
TP
0C
T, M
RI,
sur
gery
27F
80F
olli
cula
rpT
4N0M
1IV
33,9
06 (
6)1.
018
5.1
Neg
.B
one
TP
TP
MR
I, S
K28
F76
Fol
licu
lar
pT3N
0Mx
IV26
,241
(5)
0.2
94.3
Neg
.L
ung,
med
iast
inum
FN
0C
T, b
iops
y29
M57
Pap
illa
rypT
4NxM
xIV
12,9
50 (
2)1.
042
9.4
Pos
.L
ung,
bon
eT
P0
CT,
MR
I, S
K,
biop
sy30
M38
Pap
illa
rypT
3N1a
Mx
I11
,100
(2)
<0.
142
.2N
eg.
Lym
ph n
ode
FN
TP
US
, CT,
sur
gery
31F
71F
olli
cula
rpT
4NxM
xIV
34,0
36 (
6)<
0.1
630
Pos
.L
ung,
bon
eT
PT
PC
T, S
K32
M51
Pap
illa
rypT
4NxM
xIV
9,25
0 (2
)<
0.1
3.6
Neg
.L
ung
FN
FN
CT,
bio
psy
TN
M s
tage
, Ini
tial
tum
our
stag
e; S
tage
, hig
hest
tum
our
stag
e in
the
cou
rse
of d
isea
se;
TC
D, t
otal
cum
ulat
ive
dose
of
131 I
(M
Bq)
; cy
cles
, num
ber
of 1
31I
ther
apy
cycl
es;
Fin
ding
s, a
llm
alig
nant
invo
lved
tiss
ue s
ites
are
list
ed; o
ther
abb
revi
atio
ns a
s in
Tab
le1
or th
e te
xt

labelled peptide was sterilised by filtration and 350–400 MBq ofthe resulting solution was used for each patient study. Radiochem-ical purity was greater than 95% using analytical techniques basedon high-performance liquid chromatography and thin-layer chro-matography as described elsewhere [34].
99mTc-TOC imaging. Whole-body imaging was performed with adouble-headed camera (Elscint HELIX, Haifa, Israel). For the99mTc whole-body studies, the camera was equipped with a low-energy all-purpose parallel-hole collimator, window setting140 keV, width 10%. For tomographic acquisition, the same dou-ble-headed gamma camera was used. Acquisition parameterswere: 60 projections, 25 s/projection, matrix 64×64, zoom 1.99mTc-TOC studies were performed 4 h p.i. and additional 2-h p.i.images were acquired if the clinical interest was related to the ab-domen in order to avoid pitfalls due to unspecific bowel activity.Abdominal single-photon emission tomography (SPET) was per-formed in 22 patients 4 h p.i. SPET of the neck and chest was ob-tained in all patients and SPET of the head was obtained in 12 pa-tients. Since many SPET acquisitions were carried out, primarilyfor reasons of patient convenience, given the length of the proce-dure, complementary scintigraphic planar images were only ac-quired in a small group of patients (n=14). For SPET analysis rawdata were transferred to a HERMES system (Nuclear Diagnostics,London, UK) and filtered (Wiener filter) before reconstruction.
Bone scintigraphy. The same doubled-headed gamma camera asmentioned before was used for planar bone scintigraphy. Data ac-quisition was started 2–3 h after intravenous injection of 740 MBq99mTc-DPD (Teceos, Schering). At least 1.5 million counts wererequired for each head.
18F-FDG PET. Thirty-six patients received 370 MBq (10 mCi)18F-FDG (FDG-TUM, Munich) after a fasting period of 6–12 hwhile still under thyroxine therapy. Between 50 and 60 min afterintravenous injection of the tracer, transaxial imaging was per-formed using an Advance PET scanner (General Electric MedicalSystem, Milwaukee, WI) with an axial field of view of 15.2 cm.The emission scan was acquired from the head to the upper legswith five to six bed positions, at 6 min per bed position. A trans-mission scan was acquired with a 68Ge/68Ga rod source for attenu-ation correction of the PET emission data, at 4 min per bed posi-tion. Iterative image reconstruction was performed with an or-dered subset-expectation maximisation (OSEM) algorithm (2 iter-ations, 28 subsets). A visually abnormal focus of 18F-FDG uptakewas rated as a positive finding when the focal uptake clearly ex-ceeded the activity profile of the surrounding tissue without con-nection to organs showing physiologically increased uptake andno similar activity was seen in the contralateral side of the body.
CT and MRI. Abdominal, chest and head CT scanning (Hi speedAdvantage CT scanner; GE Medical System, Milwaukee, WI) wasperformed with 5-mm contiguous sections using a 512×512 matrix,before and after rapid i.v. infusion of contrast medium. All MR ex-aminations were performed on a 1.5-T whole-body scanner (Mag-neton Vision; Siemens Medical Systems, Erlangen, Germany) byusing a phased-array surface coil. T1- and T2-weighted spin-echoimages were obtained with and without fat suppression. Lesionswithin parenchymatous organs were rated as organ metastases ifthey were not clearly identified as benign lesions according to stan-dard criteria (attenuation or signal intensity and enhancement pat-tern after administration of contrast medium). Lymph nodes werestaged morphologically according to the standard criterion of nodal
diameter, i.e. lymph nodes with a diameter of more than 1 cm inthe longest axis were rated as lymph node metastases. CT and/ orMRI were performed on a routine basis in all patients.
Sonography. High-resolution neck ultrasound was also performedon a routine basis using a real-time, high-frequency (7.5- to 10-MHz), small-part probe transducer. Ultrasound scanning coveredthe entire neck region to visualise the submandibular glands, thethyroid bed, the supra- and infraclavicular area, the superior medi-astinum as far as possible and areas lateral to the carotid arteryand jugular vein.
Thyroglobulin measurement. Blood samples for measuring serumTg and anti-Tg antibody were taken prior to scintigraphy duringsuppression therapy. The Tg levels were determined in duplicateby a sensitive, commercially available radio-immunoassay(Brahms Dynotest Tg-S, Brahms Diagnostics, Berlin, Germany).A reference recovery value for exclusion of unspecific interactionsin the serum (e.g. antibodies) was determined using the zero stan-dard and was classified as abnormal if values >1 ng/ml were foundduring TSH suppression.
Image and data analysis. Somatostatin receptor images were inter-preted by two nuclear medicine physicians (M.G., R.M.) blindedto the results of conventional or PET examinations. Any focaltracer accumulation exceeding normal regional tracer uptake wasrated as a pathological finding (tumour uptake). Linear, non-focallimited intestinal uptake was rated as non-specific, non-pathologi-cal uptake. In relevant areas, SPET images were available to theviewer. All data were analysed on a HERMES system (NuclearDiagnostics, London, UK). In both groups, readers of the scanswere blinded to the underlying pathology and to the results of thestandard staging procedures, including PET data. All images werevisually evaluated and abnormal scintigraphic findings were clas-sified according to the sites typical for recurrences or metastases(local recurrence, lymph node of the neck, mediastinum, lungs,bone structures) and other sites. The reference standard againstwhich the results of the 99mTc-TOC procedure were measured wasbased on the results of all of the imaging procedures, with inclu-sion of serial follow-up morphological imaging and histopatholo-gy of surgical specimens or biopsy in 28 patients. All patients un-derwent ultrasound of the neck and imaging with either CT (n=37)or MRI (n=14), or both (n=9). Bone scanning was performed in 19 patients.
18F-FDG PET was additionally performed in 18 patients ofgroup A and 18 patients of group B. The time interval between99mTc-TOC scintigraphy and 18F-FDG PET did not exceed 4 weeks and both techniques were prospectively compared. Theviewers of the studies were blinded to findings of other methods.Corresponding studies were compared for the final analysis lesionby lesion.
Statistical analysis. 99mTc-TOC images were classified as true pos-itive, true negative, false positive or false negative by consideringthe gold standard (histopathology or other imaging techniques), asdescribed above. The sensitivity, specificity and accuracy werecalculated using the standard method. The sensitivity was calculat-ed for the recognition of any lesion in the tissue belonging to fivecategories including local recurrence, lymph node of the neck, me-diastinum, lungs and bone structures in each patient. The χ2 testfor independence, or the Fisher exact test when appropriate, wasused to evaluate differences in lesion detectability with 99mTc-TOC when subgroups of the patients being investigated were sta-
334
European Journal of Nuclear Medicine and Molecular Imaging Vol. 31, No. 3, March 2004

335
European Journal of Nuclear Medicine and Molecular Imaging Vol. 31, No. 3, March 2004
tistically compared. All P values below 0.05 were considered toindicate statistical significance. The McNemar test of correlatedproperties was used to assess the statistical significance of the dif-ference between the scintigraphic results of 99mTc-TOC and 18F-FDG PET. Analysis was performed both on a lesion and on a pa-tient basis. Two-sided P values less than 0.05 were considered sig-nificant. Cohen’s kappa with confidence intervals of 95% was cal-culated to show the degree of association between the two tech-niques. Statistical analysis was carried out with SPSS software.
Results
Tables 1 and 2 contain a detailed summary of clinical in-formation for each patient. Among the 54 cases, SSTRscintigraphy was true positive (TP) in 33 (61.1%), truenegative (TN) in 4 (7.4%) and false negative (FN) in 17(31.5%) cases. No false positive (FP) scan result was ob-served. In group A (n=22), which comprised patientswithout detectable pathology, the scan result was TP ineight, TN in four and FN in ten cases. In group B, whichconsisted of patients with known lesions (n=32), the scanresult was TP in 25 patients and FN in seven patients. Inthree patients of this group, previously unknown lesions(two bone metastases and one pulmonary metastasis)were additionally detected with 99mTc-TOC, and laterconfirmed by other imaging modalities. No statisticallysignificant difference was observed in terms of positivefindings with 99mTc-TOC (P=0.12) when the two groupswere compared. Twenty patients with follicular thyroidcancer were positive with 99mTc-TOC, as were 8 of 15patients with papillary and five of six with Hürthle cellcarcinoma. Overall, the sensitivity of 99mTc-TOC foridentification of thyroid cancer was 66% on a patient ba-sis, with a specificity of 100% and an accuracy of68.5%. For higher stages (n=46), i.e. stages III and IV,sensitivity (70.4%) was higher than for stages I and II(n=8), in which there were only two positive scan re-sults. Site-related findings are listed in Table 3. When99mTc-TOC was correlated with other imaging modalitiesor histopathology for analysis on a lesion basis, 138 tu-mor foci were localised in 33 patients, affecting the fol-lowing five tissues: local recurrence (n=5 patients),lymph node metastases in the neck (n=5), mediastinum(n=10), pulmonary metastases (n=19) and bone (n=16).In addition to a pulmonary metastasis and local tumourrecurrence as assessed by biopsy, 99mTc-TOC identified asolitary brain metastasis in patient 9 of group B. In 17
patients, 46 lesions were not detected; an example waspatient 21 of group B, with multiple bone and also twoliver metastases of a follicular thyroid carcinoma. Only alarge osteolytic metastasis in the sternum was visible.Malignancy was assessed in 28 cases by histopathologyand in 38 cases by different imaging modalities: (repeat-ed) CT (n=33), MRI (n=13), ultrasound (n=10) and bonescintigraphy (n=17). Tumour foci were confirmed byhistopathology and the sum of imaging procedures in 16cases.
99mTc-TOC and thyroglobulin
Patients were categorised into two groups in order toevaluate the influence of the current Tg level on detect-ability with 99mTc-TOC: those with initial serum Tg lev-els of <30 ng/ml (n=14) and those with initial serum Tglevels of >30 ng/ml (n=40). None of the group with Tglevels below 30 ng/ml had anti-Tg antibodies above thenormal range, whereas anti-Tg antibodies were elevatedin nine patients of the second group. In the group withelevated Tg levels (n=40), the scan result was true posi-tive in 30 cases and false negative in seven. In the 14 pa-tients with Tg levels lower than 30 ng/ml, scanning wasnegative in 11 patients, including four true negative andseven false negative results. Three cases were true posi-tive. The fraction of true positive 99mTc-TOC findingswas positively correlated with elevated Tg levels, i.e.levels higher than 30 ng/ml, showing a significant differ-ence (P<0.01).
The lowest Tg level with unequivocal positive 99mTc-TOC findings was 10.4 ng/ml (patient 14 of group A, inwhom local tumour growth was revealed), and the high-est Tg level with false negative 99mTc-TOC scintigraphywas 401.1 ng/ml (patient 1 of group A). This patient pre-sented with multiple pulmonary metastases, all of whichwere smaller than 1 cm.
99mTc-TOC and 18F-FDG
True positive results were obtained in 20 patients out of36 with 99mTc-TOC (55.5%) and in 28 patients with 18F-FDG (77.7%). In 16 cases (44.4%), scintigraphy wasnegative with 99mTc-TOC, while 18F-FDG PET was neg-ative in six cases (16.6%). Of the 16 negative scinti-
Table 3. Scintigraphic findings: analysis per lesion
Local Neck Mediastinum Lung Bone Other Overallrecurrence (lymph node)
99mTc-TOC + 5 5 27 71 29 1 13899mTc-TOC − 2 2 5 25 10 2 46No. of lesions 7 7 32 96 39 3 184

336
European Journal of Nuclear Medicine and Molecular Imaging Vol. 31, No. 3, March 2004
graphic studies using 99mTc-TOC in four patients (11.1%;patients 16, 17, 20 and 22 of group A), further clinicalexaminations did not reveal any pathological findingsand serum Tg levels also remained stable over a follow-up period of at least 1 year, so these cases were consid-ered true negative. Two of them showed suspicious up-take using 18F-FDG PET, leading to false positive re-sults. In patient 16, focal tracer accumulation was foundin the right neck due to an inflammatory reaction. Asym-metrical uptake was detected in the thyroid bed in patient20, mimicking recurrent local disease, but further cytodi-
agnosis confirmed granulomatous tissue. False negativescan results were obtained in 12 cases (33.3%) with99mTc-TOC and in four cases (11.1%) with 18F-FDGPET. Overall, 99mTc-TOC yielded a per-patient sensitivi-ty of 62.5%, a specificity of 100% and an accuracy66.7%, whereas 18F-FDG showed a sensitivity of 87.5%,a specificity of 50% and an accuracy of 83.3% (Table 4).An analysis per patient comparing the scan results of99mTc-TOC and 18F-FDG showed statistically significantbetter results for PET (P<0.004) using the McNemartest. This correlation was based on 36 observations.
In addition, a site-specific evaluation was performed.Tissue-related abnormal uptake is reported in Fig. 1. Outof 105 malignant foci, 18F-FDG PET revealed 77 tumoursites (73.3%) and 99mTc-TOC, 63 (60%). There were nofalse positive findings with 99mTc-TOC, whereas 18F-FDG showed two false positive findings, as mentionedabove. Analysis on a lesion basis also emphasised the im-proved diagnostic efficacy of 18F-FDG PET, with a P val-ue of <0.001. Cohen’s kappa of 0.62 (0.47–0.78), howev-er, revealed substantial agreement between the imagingtechniques. The difference in detection rate was mostpronounced for lung lesions: 32 of 55 lesions (58.1%)were positive with 99mTc-TOC, whereas 42 lesions werecorrectly identified with 18F-FDG (76.3%) (Fig. 2).
Clinical impact of 99mTc-TOC
Especially in group B, a high proportion of patientsshowed extended tumour disease that limited the thera-peutic options. Therefore, further therapeutic strategieswere not significantly influenced by 99mTc-TOC find-ings in many cases. However, scintigraphic findings af-fected the further treatment decision in ten patients.Three patients were referred to external beam radiationtherapy because their lesions were not amenable to surgical excision; such was the case in patient 15 of
Table 4. 99mTc-TOC and 18F-FDG results
Parameter 99mTc-TOC 18F-FDG
Sensitivity 62.5% (20/32) 87.5% (28/32)Specificity 100% (4/4) 50% (2/4)Accuracy 66.7% (24/36) 83.3% (30/36)
Number of patients is shown within parentheses
Fig 1. Number of abnormal findings revealed by 99mTc-TOC and18F-FDG PET in 36 patients and comparison with other imagingmodalities and histology, i.e. the gold standard
Fig 2a, b. A 77-year-old pa-tient with follicular thyroidcancer. A solitary pulmonarymetastasis, which was smallerthan 1 cm, was identified with18F-FDG FDG (a), while99mTc-TOC was negative (b)

337
European Journal of Nuclear Medicine and Molecular Imaging Vol. 31, No. 3, March 2004
group A (Fig. 3). A bone metastasis in the thoracicspine was identified with 99mTc-TOC, and also con-firmed by 18F-FDG. Another bone metastasis, located inthe right humerus, was irradiated in patient 12 of groupB. This lesion was initially described with 99mTc-TOC,whereas the other pulmonary metastases were alreadyknown before the scan. In patient 26 of group B, the in-tention was to remove surgically a large lesion in thelateral orbital wall. Close to this known lesion, theSPET acquisition additionally showed a smaller bonemetastasis in the skull (Fig. 4), so this patient was
spared from further surgical intervention and externalradiotherapy was performed.
Patient 11 (Fig. 5) and patient 12 of group A showedtracer uptake in a cervical lymph node metastasis. Bothpatients were successfully treated by lymph node dissec-tion, which resulted in a decrease in Tg levels withoutdetectable pathology in the further follow-up. Only pa-tient 21 of group A showed another increase in Tg 6months after resection of malignant involved lymphnodes and recurrent local disease, which were initiallyvisualised with 99mTc-TOC.
Fig 3a–c. A 72-year-old patientwith follicular thyroid cancer.A matching scan result be-tween 99mTc-TOC (a) and 18F-FDG (b) was obtained for asmall bone lesion in the thorac-ic spine, which was not depict-ed on the post-therapy 131Iwhole-body scan (c)
Fig 4a–d. A 52-year-old pa-tient with follicular thyroidcancer presented with an osse-ous metastasis in the lateral or-bital wall on the right side. Thislesion was clearly delineatedwith SPET in the coronal (a),transverse (b) and sagittal (c)sections, and confirmed withCT (d). However, a smallerbone lesion (arrow) was addi-tionally detected close to thelarge metastasis in the skull onthe SPET acquisition (b),which affected further treat-ment planning. This patientwas subsequently treated byexternal beam radiation, andspared surgery

338
European Journal of Nuclear Medicine and Molecular Imaging Vol. 31, No. 3, March 2004
Five patients (nos. 1, 5, 10, 13 and 25 of group B)were referred to receptor-mediated radionuclide therapyusing 90Y-DOTA-TOC. Intense uptake behaviour of the99mTc-labelled radiopharmaceutical was found in severaltumour lesions. All patients had extended disease withmore than one affected tissue site. Each of them respond-ed under this therapy regimen, and stable disease wasachieved for at least 5 months in all patients. Each pa-tient was well informed about this new treatment optionand each of them received three or four cycles with1,850 MBq per interval cycle. The therapy was well tol-erated. In the event of tumour progression under therapy,treatment with 90Y-DOTA-TOC was terminated.
Discussion
Several studies have reported on the high level of SSTRexpression on various tumour cells, which provides themolecular basis for successful somatostatin receptor im-aging. Despite the lack of SSTR subtype 2 in certain thy-roid tumours, relatively high tumour uptake of 111In-DTPA-octreotide has been observed [28]. However, thesensitivity of 111In-DTPA-octreotide varies markedlyamong studies, which might be especially related to thevariable and sometimes low expression of the receptorsin DTC. Our study was performed to investigate the clin-ical potential of 99mTc-TOC for tumour localisation in alarger series of patients. The study was initiated becauseof the more favourable imaging characteristics and thehigher sensitivity of this new compound as assessed byhigher tumour to organ ratios, which might be based onbetter pharmacokinetics and the higher spatial resolutionof the 99mTc label [31]. The results of the present study
reflect the favourable imaging abilities of the new tracerin patients with DTC, with an overall sensitivity of 66%for detection of tumour foci in the presence of elevatedTg levels and negative radioiodine scintigraphy. The re-sults indicate that although lesions had lost their abilityto take up radioiodine, a high percentage still showed ex-pression of SSTR. Comparing the results with those ofother studies using 111In-DTPA-octreotide in patientswith DTC, the overall sensitivity of the present study isgenerally comparable or even higher [19, 20, 23, 25, 26,27]. A limiting issue in all these studies has been thesmall number of patients included.
Many lesions in different body regions showed posi-tive tracer uptake, i.e. 138 of 184 lesions were detectedin 33 patients, with higher probability for a positive scanresult in patients with higher Tg levels exceeding30 ng/ml, which might be mainly attributed to the tu-mour load. However, the spatial resolution of the 99mTc-labelled compound is insufficient to detect smaller le-sions, e.g. in the presence of widespread pulmonary me-tastases. In our series of patients, 25 of 96 lung lesionsescaped detection, and in these cases the lesion diameterwas usually less than 1 cm. Although tumour load andTg levels were sometimes high in these cases, the scanresult was inconclusive, as exemplified in Fig. 6. The pa-tient with the highest Tg level with false negative 99mTc-TOC scintigraphy (patient 1 of group A) also presentedwith multiple pulmonary metastases, all of which weresmaller than 1 cm.
When comparing 99mTc-TOC and 18F-FDG, a pro-nounced difference was also found concerning the rate ofdetection of pulmonary metastases, which was 58.1%and 76.3% respectively. One explanation might be thehigher spatial resolution of PET. However, a biological
Fig. 5a–c. SSTR imagingshows a small cervical lymphnode metastasis (a) in a patientwith papillary thyroid cancer.This lesion was also intenselydelineated by 18F-FDG PET(b), but missed by post-therapy131I whole-body scan (c). This53-year-old patient was suc-cessfully treated by lymphnode dissection

339
European Journal of Nuclear Medicine and Molecular Imaging Vol. 31, No. 3, March 2004
phenomenon cannot be excluded, which could imply thatsome hypermetabolic lesions do not express SSTR. Inparagangliomas and carcinoid tumours, Le Rest et al.showed that the different mechanism of uptake resultedin variation in tumour affinity for 111In-DTPA-octreotidecompared with 18F-FDG, i.e. Octreoscan identified somelesions which were negative with 18F-FDG PET and viceversa [35].
In the 36 patients of the present study who underwent18F-FDG PET, the diagnostic efficacy was statisticallysignificantly higher for 18F-FDG PET than for 99mTc-TOC, although two false positive findings on 18F-FDGPET were negative on 99mTc-TOC. However, there wassubstantial overlap in the lesions detected by each mo-dality, which implies high agreement between the meta-bolic pattern and the SSTR status in non-iodine-avid le-sions. From the clinical point of view, both techniquescan easily be performed without withdrawal of L-thyrox-ine, as long as some precautions are taken in the case ofPET, e.g. a 6-h fasting period before scanning. Althoughthere is no evidence that serum TSH levels influence therate of somatostatin receptor expression, higher glucoseconsumption in tumour foci can be observed under TSHstimulation, which could improve the accuracy of 18F-FDG PET [36]. In accordance with the prospective de-sign of the present study, all investigations were per-formed under TSH suppression.
High 18F-FDG uptake suggests more aggressive tu-mour cell growth in those types of lesion which have lostthe sodium-iodine symporter activity. In such cases, it ishighly doubtful whether high-dose radioiodine therapywill have an impact on the tumour growth [37]. If suchlesions are not accessible to surgical treatment, e.g. lo-calised disease, only a few non-invasive treatment op-tions are available, with a low impact on the individualprognosis. Recently, it was reported that the metabolicactivity as assessed by 18F-FDG PET decreased in tu-mour lesions after the use of a long-acting octreotide an-alogue in patients with metastatic thyroid cancer that ex-
hibited somatostatin receptors [38]. This new approach,with the aim of inhibiting the proliferation of neoplastictissue, seems very promising considering the benefit ofsomatostatin analogues in patients suffering from otherSSTR-expressing malignancies, e.g. neuro-endocrine tu-mours of the gastroenteropancreatic system [39]. Long-acting somatostatin analogues can also be used in multi-morbid patients, e.g. elderly patients with reduced kid-ney function.
High expression of somatostatin receptors in thyroidcarcinoma lesions also offers another treatment optionusing radionuclide targeted therapy, e.g. 90Y-DOTA-TOC[40]. We have followed this rationale in five patientswith advanced tumour stage who had a very high tumourload. These patients showed intense tumour uptake of99mTc-TOC. Prior to the use of either 90Y-labelled or un-labelled long-acting derivatives, the assessment of SSTRstatus in tumour lesions seems mandatory. In differentclinical settings, somatostatin receptor imaging with99mTc-TOC easily allows non-invasive selection of thesubset of patients who would benefit from such thera-pies.
In the case of DTC, 99mTc-sestamibi is currently apreferred radiopharmaceutical. 99mTc-sestamibi, howev-er, exhibits only a moderate detection rate with respect tolymph node metastases [41]. By contrast, we found that99mTc-TOC provided high spatial resolution in the neck,given that five of seven sites in the neck correspondingto lymph node metastases and also five of seven cases oflocal tumour recurrences were correctly identified. Be-side accurate anatomical localisation to permit adequatetreatment planning, 99mTc-TOC could help in the devel-opment of new surgical techniques, e.g. probes for mini-mally invasive radio-guided surgery, avoiding extensivesurgery in the neck. A similar approach has been takenwith 99mTc-sestamibi in a small series of patients with re-current thyroid cancer [42], but there is as yet no evi-dence whether this technique is accurate enough to de-tect malignant involved cervical lymph nodes. Since the
Fig. 6a, b. This 77-year-old patient with a serum Tg of116 ng/ml suffered from multi-ple pulmonary metastasis of afollicular thyroid carcinoma, asshown in the chest X-ray (a).Positive 99mTc-TOC uptake wasonly found in the two largestlesions in the right lung (b)

mechanism of uptake of the lipophilic cationic agent isdifferent from that of 99mTc-TOC, further investigationsare needed to evaluate which of the two 99mTc-labelledcompounds is better in terms of localisation diagnosticsand treatment stratification in patients with recurrent ormetastatic disease.
In conclusion, somatostatin receptor imaging using99mTc-TOC is a promising and easy-to-perform tech-nique for accurate anatomical localisation of malignantfoci in thyroid cancer patients with elevated Tg levelsand negative 131I scans. Although 18F-FDG showed ahigher sensitivity in our series of patients, with the ad-vent of new therapeutic approaches, e.g. minimally inva-sive radio-guided surgery or application of SST ana-logues, this new technique might be an effective tool toimprove treatment strategies in DTC.
Acknowledgements. We especially wish to thank Prof. G. Ricca-bona, Prof. Emeritus, University of Innsbruck, for his help andsupport in initiating this study.
References
1. Pacini F, DeGroot LJ. Thyroid neoplasia. In: DeGroot LJ,Jameson JL, eds. Endocrinology, 4th edn. Philadelphia: Saunders; 2001:1541–1566.
2. Ronga G, Fiorentino A, Paserio E, et al. Can iodine-131whole-body scan be replaced by thyroglobulin measurement inthe post surgical follow-up of differentiated thyroid carcino-ma. J Nucl Med 1990; 31:1766–1771.
3. Ozata M, Suzuki S, Miyamoto T, Tsuan Liu RT, Fierro-RenoyF, Degroot LJ. Serum thyroglobulin in the follow-up of pa-tients with treated differentiated thyroid cancer. J Clin Endo-crinol Metab 1994; 79:98–105.
4. Lubin E, Mechli-Frish S, Zatz S, et al. Serum thyroglobulinand iodine-131 whole-body scan in the diagnosis and assess-ment of treatment for metastatic differentiated thyroid carcino-ma. J Nucl Med 1994; 35:257–262.
5. Schlumberger MJ. Diagnostic follow-up of well-differentiatedthyroid carcinoma: historical perspective and current status.J Endocrinol Invest 1999; 22 (11 Suppl):3–7.
6. Feine U, Lietzenmayer R, Hanke JP, Held J, Woehrle H, Mueller-Schauenburg W. Fluorine-18-FDG and iodine-131-iodide uptake in thyroid cancer. J Nucl Med 1996; 37:1468–1472.
7. Schlueter B, Bohuslavizki KH, Beyer W, Plotkin M, BuchertR, Clausen M. Impact of FDG PET on patients with differenti-ated thyroid cancer who present with elevated thyroglobulinand negative131I scan. J Nucl Med 2001; 42:71–76.
8. Helal BO, Merlet P, Toubert ME, et al. Clinical impact of 18F-FDG PET in thyroid carcinoma patients with elevated thyro-globulin levels and negative 131I scanning results after therapy.J Nucl Med 2001; 42:1464–1469.
9. Briele B, Hotze A, Kroopp J, et al. A comparison of 201Tl and99mTc-MIBI in the follow-up of differentiated thyroid carcino-mas. Nuklearmedizin 1991; 30:115–124.
10. Lind P, Gallowitsch HJ, Langsteger W, Kresnik E, Mikosch P,Gomez I. Technetium-99m-tetrofosmin whole-body scintigra-phy in the follow-up of differentiated thyroid carcinoma. J Nucl Med 1997; 38:348–354.
11. Miyamoto S, Kasagi K, Misaki T, Alam MS, Konishi J. Evalu-ation of technetium-99m-MIBI scintigraphy in metastatic dif-ferentiated thyroid carcinoma. J Nucl Med 1997; 38:352–356.
12. Rubello D, Mazzarotte R, Casara D. The role of technetium-99m methoxyisobutylisonitrile scintigraphy in the planning oftherapy and follow-up of patients with differentiated thyroidcarcinoma after surgery. Eur J Nucl Med 2000; 27:431–440.
13. Ng DCE, Sundram FX, Sin AE. 99mTc-sestamibi and 131Iwhole-body scintigraphy and initial serum thyroglobulin in themanagement of differentiated thyroid carcinoma. J Nucl Med2000; 41:631–635.
14. Krenning EP, Kwekkeboom DJ, Bakker WH, et al. Somatosta-tin receptor scintigraphy with [111-In-DTPA-D-Phe] and [123-I-Tyr]-octreotide: the Rotterdam experience with more than1000 patients. Eur J Nucl Med 1993; 20:716–731.
15. Krenning EP, Kwekkeboom DJ, de Jong M, et al. Essentials ofpeptide receptor scintigraphy with emphasis on somatostatinanalog octreotide. Semin Oncol 1994; 21 (Suppl 13):6–14.
16. Lamberts SWJ, Reubi JC, Krenning EP. Somatostatin and theconcept of peptide receptor scintigraphy in oncology. SeminOncol 1994; 21 (Suppl) 13:1–5.
17. Kwekkeboom D, Krenning EP, de Jong M. Peptide receptorimaging and therapy. J Nucl Med 2000; 41:1704–1713.
18. Balon HR, Goldsmith SJ, Siegel BA, et al. Procedure guide-lines for somatostatin receptor scintigraphy with 111In-pent-etreotide. J Nucl Med 2001; 42:1134–1138.
19. Tenenbaum F, Lumbroso J, Schlumberger M, Caillou B, FraguP, Parmentier C. Radiolabeled somatostatin analog scintigra-phy in differentiated thyroid carcinoma. J Nucl Med 1995;36:807–810.
20. Baudin E, Schlumberger M, Lumbroso J, Travagli JP, CaillouB, Parmentier C. Octreotide scintigraphy in patients with dif-ferentiated thyroid carcinoma: contribution for patients withnegative radioidine scan. J Clin Endocrinol Metab 1996;81:2541–2544.
21. Ahlman H, Tisell LE, Wangberg B, et al. The relevance of so-matostatin receptors in thyroid neoplasia. Yale J Biol Med1997; 70:523–533.
22. Gulec SA, Serafini AN, Sridhar KS, et al. Somatostatin recep-tor expression in Hürthle cell cancer of the thyroid. J NuclMed 1998; 39:243–245.
23. Garin E, Devillers A, Le Cloirec J, et al. Use of indium-111pentetreotide somatostatin receptor scintigraphy to detect re-current thyroid carcinoma in patients without detectable iodineuptake. Eur J Nucl Med 1998; 25:687–694.
24. Kolby L, Wangberg B, Ahlman H, et al. Somatostatin receptorsubtypes, octreotide scintigraphy, and clinical response to oct-reotide treatment in patients with neuroendocrine tumors.World J Surg 1998; 22:679–683.
25. Valli N, Catargi B, Ronci N, et al. Evaluation of indium-111pentetreotide somatostatin receptor scintigraphy to detect re-current thyroid carcinoma in patients with negative radioio-dine scintigraphy. Thyroid 1999; 9:583–589.
26. Haslinghuis LM, Krenning EP, De Herder WW, Reijs AE,Kwekkeboom DJ. Somatostatin receptor scintigraphy in thefollow-up of patients with differentiated thyroid cancer. J En-docrinol Invest 2001; 24:415–422.
27. Goerges R, Kahaly G, Mueller-Brand J, Maecke H, Roser HW,Bockisch A. Radionuclide-labeled somatostatin analogues fordiagnostic and therapeutic purposes in nonmedullary thyroidcancer. Thyroid 2001; 11:647–659.
340
European Journal of Nuclear Medicine and Molecular Imaging Vol. 31, No. 3, March 2004

36. Petrich T, Boerner AR, Otto D, Hofmann M, Knapp WH. In-fluence of rhTSH on [18F]fluorodeoxyglucose uptake by dif-ferentiated thyroid carcinoma. Eur J Nucl Med Mol Imaging2002; 29:641–647.
37. Wang W, Larson SM, Tuttle RM, et al. Resistance of [18F]-flu-orodeoxyglucose-avid metastatic thyroid cancer lesions totreatment with high-dose radioactive iodine. Thyroid 2001;11:1169–1175.
38. Robbins RJ, Hill RH, Wang W, Macapinlac HH, Larson SM.Inhibition of metabolic activity in papillary thyroid carcinomaby a somatostatin analogue. Thyroid 2000; 10:177–183.
39. Arnold R, Simon B, Wied M. Treatment of neuroendocrineGEP tumours with somatostatin analogues: a review. Diges-tion 2000; 62 Suppl 1:84–91.
40. Waldherr C, Schumacher T, Pless M, et al. Radiopeptide trans-mitted internal irradiation of non-iodophil thyroid cancer andconventionally untreatable medullary thyroid cancer using[90Y]-DOTA-D-Phe1-Tyr3-octreotide: a pilot study. Nucl MedCommun 2001; 22:673–678.
41. Hsu CH, Liu FY, Yen RF, Kao CH. Tc-99m MIBI SPECT indetecting metastatic papillary thyroid carcinoma in patientswith elevated human serum thyroglobulin levels but negativeI-131 whole body scan. Endocr Res 2003; 29:9–15.
42. Rubello D, Piotto A, Pagetta C, Pelizzo MR, Casara D.99mTc-MIBI radio-guided surgery for recurrent thyroid carci-noma: technical feasibility and procedure, and preliminaryclinical results. Eur J Nucl Med Mol Imaging 2002; 29:1201–1205.
341
European Journal of Nuclear Medicine and Molecular Imaging Vol. 31, No. 3, March 2004
28. Forssell-Aronsson EB, Nilsson O, Benjegard A, et al. 111In-DTPA-D-Phe1-octreotide binding and somatostatin receptorsubtypes in thyroid tumors. J Nucl Med 2000; 41:636–642.
29. Decristoforo C, Melendez-Alafort L, Sosabowski JK, MatherSJ. 99mTc-HYNIC-[Tyr3]-octreotide for imaging somatostatin-receptor-positive tumors: preclinical evaluation and compari-son with 111In-octreotide. J Nucl Med 2000; 41:1114–1119.
30. Decristoforo C, Mather SJ, Cholewinski W, Donnemiller E,Riccabona G, Moncayo R. 99mTc-EDDA/HYNIC-TOC: a new99mTc-labelled radiopharmaceutical for imaging somatostatinreceptor-positive tumours: first clinical results and intra-pa-tient comparison with 111In-labelled octreotide derivates. Eur JNucl Med 2000; 27:1318–1325.
31. Gabriel M, Decristoforo C, Donnemiller E, et al. An intrapa-tient comparison of 99mTc-EDDA/HYNIC-TOC with 111In-DTPA-octreotide for diagnosis of somatostatin receptor ex-pressing tumors. J Nucl Med 2003; 44:708–716.
32. Sobin LH, Wittekind C. International Union Against Cancer.TNM classification of malignant tumours, 5th edn. New York:Wiley-Liss, 1997.
33. American Joint Committee on Cancer. AJCC cancer stagingmanual, 5th edn. In: Part II: 8. Thyroid Gland. Philadelphia,New York: Lippincott-Raven; 1997:59–61.
34. Decristoforo C, Mather SJ. Preparation, 99mTc-labelling and invitro characterisation of HYNIC and N3S modified RC-160and [Tyr3]-octreotide. Bioconjug Chem 1999; 10:431–438.
35. Le Rest C, Bomanji JB, Costa DC, Townsend CE, Visvikis D,Ell PJ. Functional imaging of malignant paragangliomas andcarcinoid tumours. Eur J Nucl Med 2001; 28:478–482.