9 nutrition and feeding handout - mother baby university pdf no… · 1 nutrition and feeding judy...
TRANSCRIPT
1
Nutrition and Feeding
Judy Philbrook, NNP-BC
Microsoft Clip Art
n 32 day old growing preemie now at 33 weeks adjusted age. 1700 grams
n Feedings: Breast milk 33 ml every 3 hours
n Nippling 3 times/day and doing well n Baby has a 6 ml residual
n What things would you want to consider when evaluating this?
2
n 630 gram 24 week female n Day 1 of life:
n On the ventilator n UAC and UVC: GIR 6 mg/kg/min n Sodium 150, potassium 4.5 n On GI Priming feeds of breast milk
n What total fluid volume should be given?
n What should be monitored to assess nutritional and electrolyte status?
n Should feedings be increased?
n 6 day old 28 week infant on the ventilator
n Oxygen requirement 50% n Feedings 2ml 3 hours on and 1 hour off n Echocardiogram with moderate PDA
and indocin started n Should feedings be continued?
n 27 week infant; now 18 days old n Post-op: exploratory lap due to NEC n On TPN and lipids n Replogle to LIWS
n 58 ml output in the past 8 hours n Sodium 134, Potassium 3.1
n Options?

3
n 36 day old 31 week adjusted age female
n On SC 24cal/oz at 155ml/kg/day n Growth is at the 8.6th percentile
n Options?
Microsoft Clip Art
Anatomy & Physiology of the GI tract
n GI tract resembles that of a term newborn by 20 weeks gestation
n Functional development is limited before 26 weeks
n Biochemical and physiologic capacities for digestion and absorption are present at 28 weeks

4
n Sucking occurs in utero at 13-15 weeks, but is not developed before 31-34 weeks
n Digestive enzymes for carbohydrates are functionally active >28 weeks
n Protein enzyme activity increases after birth in premature and term infants
n Preterm – limited production of gut digestive enzymes and growth factors
n Premature infants have: n Lack of sucking coordination n Decreased esophageal sphincter tone n Delayed gastric emptying n Slow intestinal transit
n Peristalsis begins to mature after 30-32 weeks – remains less organized until near term
n Major factor in growth and function – DIET – influences the enzyme activities and gut flora
Nutrient Store Deficiencies of Preterm Infants n Energy
n Fat n Carbohydrate
n Vitamins and minerals n Essential nutrients
n Inadequate nutrition affects all organ systems.
5
Fat n At 24 weeks – 2% stored fat, 5% at 32
weeks, 15% at 40 weeks n Increased accretion between 24 and 40 wks n Essential fatty acids are needed for brain and
retinal growth and function n Sources:
n Adipose tissue stores n From human milk or formula (50% of calories) n IV lipids
Carbohydrate n Second major energy source n Brain is dependent on glucose –
accounts for 75% of glucose consumption
n Stored as glycogen in the liver in the 3rd trimester n Preterm infants have limited fat and
glycogen stores
Standards for Growth n Growth curves – weight, length and
head circumference n Postnatal growth curves for preterm
infants should be used
http://school.discoveryeducation.com/clipart/images/graph.gif
6
Nutrition Requirements n Water n Calories n Protein n Fat n Carbohydrates n Electrolytes n Vitamins and Minerals
Nutrition Requirements n Healthy newborns
n 98-108 cal/kg/day for growth and development n 150-180 ml/kg/day of 20 cal/oz formula or breast
milk
n Protein, fat and carbohydrate intake: n Protein: 7-12% n Fat: 35-55% n Carbohydrate: 35-55%
Preterm Requirements n Recommendations are guidelines n Individual needs must be considered
n Gestational age n Birth weight n Clinical status
n Minimal intake is 120-150 ml/kg/day for a growing preterm infant on feeds
n OR 120-150 ml/kg/day on parenteral fluids

7
Factors that Increase Fluid Requirements n Abnormal fluid losses (ileostomy, chest tube) n Labile body temp, fever, stress n Phototherapy n Prematurity n Radiant warmers n Renal dysfunction n Third spacing
Factors that Decrease Fluid Requirements
n HIE n BPD n PDA n Post-operative n CHF n Meningitis n Renal failure
Factors that Increase Caloric Requirements n Acute or chronic lung disease n Temperature fluctuations n Hypothermia/hyperthermia n Increased cardiac output n Increased muscle activity (agitation, pain) n Infection n Malabsorption or short gut n SGA n Periods of rapid growth
8
Preterm Guidelines n Protein: 7-12% of caloric intake
n Adequate protein can not be achieved with unfortified breast milk!
n Fat: 35-55% of caloric intake n Human milk – 50% of energy from fat; formula
40-50%
n Carbohydrates: 35-55% of total calories n Usual amount of glucose is 4-6 mg/kg/min n Can be achieved with D10W at 60-90 ml/kg/day
Preterm Guidelines n Electrolytes
n Sodium, potassium and chloride n Increased urinary sodium excretion and
insensible losses during transition n Stable growing preterm needs 2-4 mEq/kg/
day of sodium n Vitamins and Minerals
n Exact requirements needed have not been established
Where to Start! n Suggested initial admission fluid intake
for newly born infants: < 1 kg 100 ml/kg/day 1-2.5 kg 80 ml/kg/day >2.5 kg 60 ml/kg/day Calcium is added (1.5 mEq/kg/day) on
admission for babies with BW > 1.5 kg

9
What fluid? n TPN is ordered on admission if <1500
grams n D5 or D10 W n 1.5 mEq/kg of calcium n 1.5 grams/kg of amino acids n 1.5 grams/kg lipids
n Minimal enteral nutrition (GI priming) is also ordered
Parenteral Nutrition n Indications
n Birth weight < 1500 grams; gestational age < 32 weeks
n GI disorders (gastroschisis, TEF, malrotation, NEC) n Short gut n Severe respiratory or cardiac disease n Renal failure
n Administration n Peripheral n Central
Guidelines for TPN Administration n Calories: 20% less than enteral n Water: 100-150 ml/kg/day (next slide!) n Protein: 2-4 g/kg/day n Fat: 10 or 20% - 3g/kg/day n Carbohydrates: 5 or 10% glucose n Glucose infusion rate: 4-6 grams/kg/min; max
12-14 mg/kg/min n Calcium and phosphorus n Vitamins and minerals

10
Complications of TPN Administration
n Metabolic disturbances n Cholestasis and jaundice n Hyperglycemia/hypoglycemia n Rickets n IV infiltrates n Infection
Enteral feedings n Human milk is ideal!
n 20 cal/oz initially n 24 cal/oz when feeds are half volume –
increase calories and nutrients
n Formula – 24 cal/oz – is used if breast milk is not available
n OG/NG/PO
Microsoft clip art
Advantages of breast milk n Improved gastric emptying n Enhanced absorption and digestion n Optimal distribution of calories n Anti-infective properties n Low renal solute load n Long chain fatty acids n Maternal involvement

11
Supplementation with Breast Feeding
n Iron supplementation n 2mg/kg/day for all preterm infants at 2
months or when birth weight is doubled n Required if baby is being treated for
physiologic anemia with erythropoietin
n Poly-vi-sol with iron 0.5 ml bid when on full feedings
Formula n Milk based n Soy based
n Lactose intolerance, galactosemia n Not for babies <1800 grams
n Elemental n Protein intolerance n Fat malabsorption
Microsoft clip art
Advantages to Early Feeding (GI Priming; Minimal Enteral Feedings)
n Promotes gut mucosal development n Stimulates GI activity n Increased secretion of GI hormones n Colonization with normal flora n Improved metabolic status n Reduced cholestasis and lower bili levels n May decrease NEC n Improved lactase activity

12
How to Feed n Minimal enteral feedings (GI priming) n Breast milk or 24cal/oz formula within
the first 24 hours of life n 1001-1500 grams - 2ml every 8 hours n 751-1000 grams - 1 ml every 8 hours n <750 grams – 0.5 ml every 8 hours
n Do not check residuals!
How to Feed (cont) n Trophic feedings – started at 48-72
hours of age; continue 24-48 hours n Continuous – <1200 grams n Bolus - every 3 hours > 1200 grams
n Feedings are increased 20 ml/kg/day n TPN is decreased to accommodate enteral
increase, or increased to give more volume if baby is only a few days old
n Lipids are stopped when enteral calories are > 80 cal/kg/day
n TPN is stopped when enteral fluid volume is > 120 ml/kg/day

13
Total # IV Days: 401-1500g BW
0
5
10
15
20
25
30
35
1996 1997 1998 1999 2000 2001 2002 2003 2004*
Reasons to Withhold feeds n Severe apnea and bradycardia n Decreased peristalsis (not stooling,
decreased bowel sounds) n Meconium obstruction of prematurity n PDA – decreased GI perfusion n Acute sepsis
Oral feedings n Facilitate digestive capacity n Allows infant to self regulate feeding n Promotes social behavior states n May have increased risk of aspiration if
suck/swallow are not coordinated n Should be able to nipple at 34 weeks n Can try breast feeding at 32 weeks

14
Gavage Feeding n < 32 weeks n OG vs. NG n Residuals of 2-4 ml/kg or one hour of
volume are considered normal and should be refed
n Administer by gravity or pump in 15-30 min.
Transpyloric feeds n Recommended if there is a high risk of
aspiration n Bypass stomach – fat malabsorption n Verify location by x-ray
Gastrostomy tube feedings n Inability to suck and swallow n Congenital anomalies of the GI tract n Need for long term gavage
15
Nutritional Assessment n Weight n Head and length n Monitor intake n Monitor lab values
Feeding Tolerance n Bowel sounds n Abdominal assessment n Girth n Stools
Post Discharge Formula n NeoSure 22 cal/oz for babies receiving
formula n Breast milk – may supplement with a
couple feedings of 22 cal/oz NeoSure n NeoSure is continued until 6 months
adjusted age
16
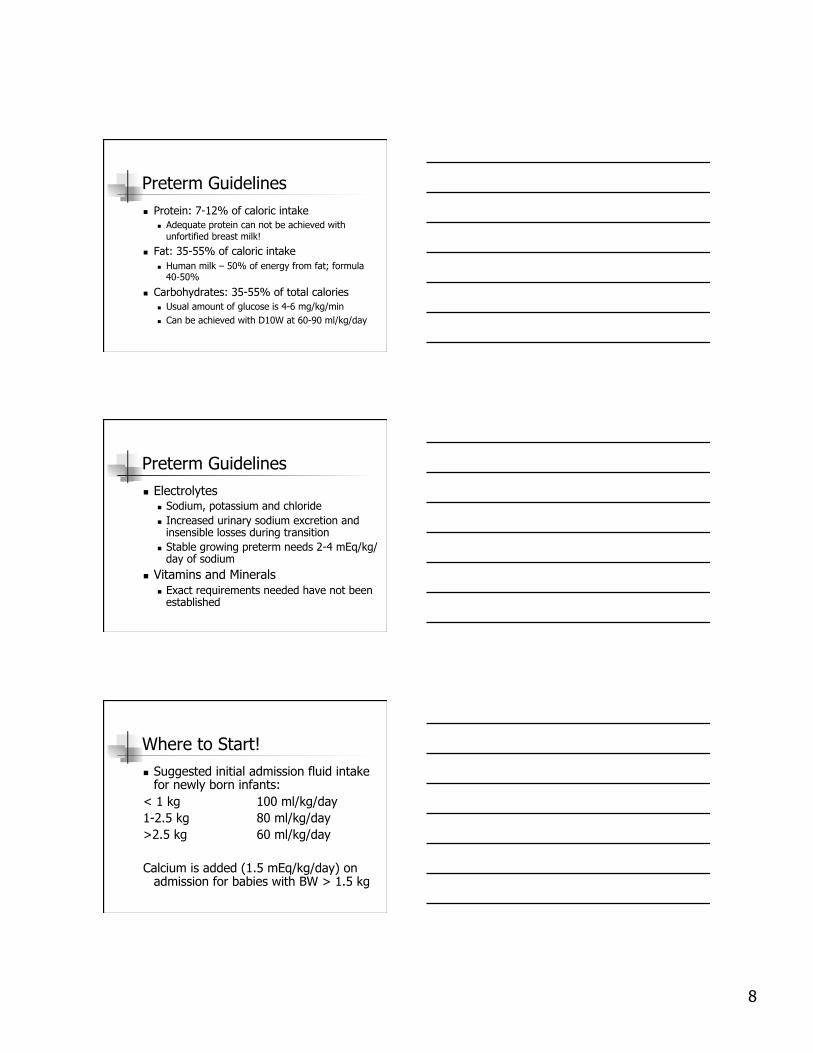
40
45
50
55
60
65
70
2003 2004 2005 2006 2007 2008 2009 2010
Days
Length of Stay: 501-1500 grams (mean)
Vermont Oxford Database
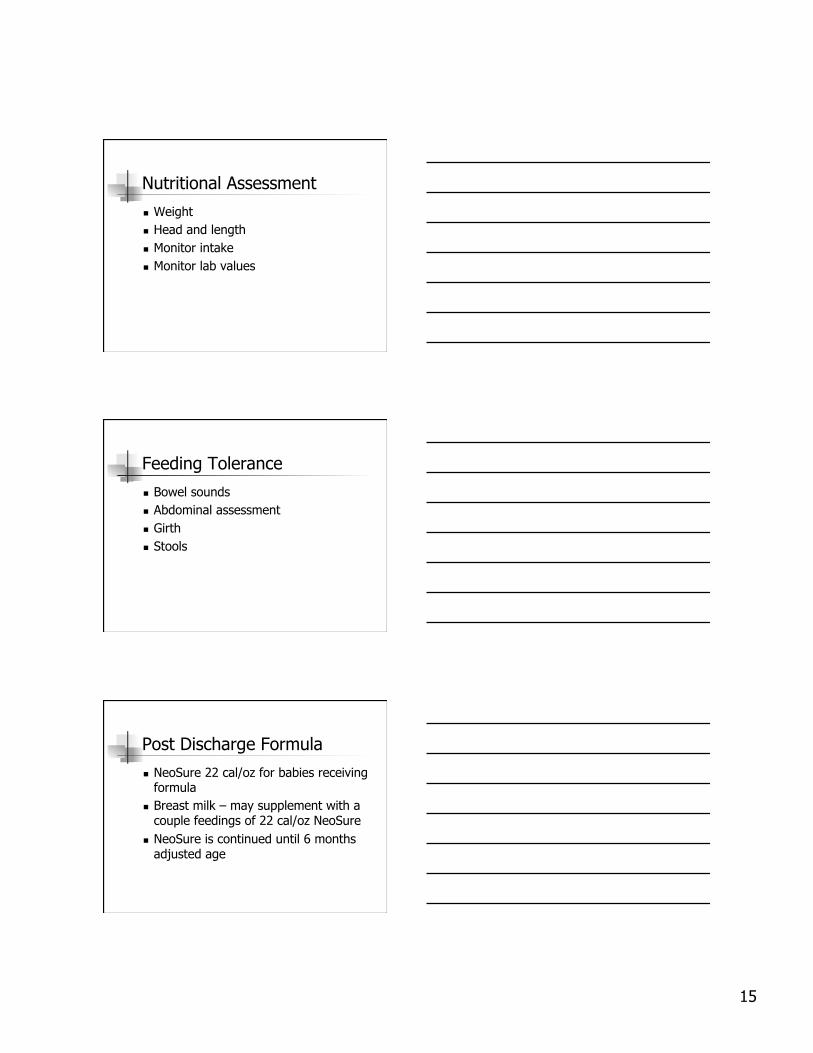
0102030405060708090
100
2005 2006 2007 2008 2009 2010 2011
Breast milk andfortifierFormula only
Feedings at Discharge; all VLBW Infants
Vermont Oxford Database
References n Verklan, et. al.; Core Curriculum for
Neonatal Intensive Care Nursing, Elsevier, Philadelphia, 2004.