5-2-1-0 goes to child care partner ... - 5210 let's go! · 5-2-1-0 goes to child care program...
TRANSCRIPT

5-2-1-0 Goes to Child Care
Partner Implementation
Toolkit

Dear Partner, 5-2-1-0 Goes to Child Care (5-2-1-0 GTCC) is an early childhood obesity prevention program aimed at increasing healthy eating and physical activity in the child care environment. The program is part of a larger project called Let’s Go!. Let’s Go! is a nationally recognized childhood obesity prevention program. It is a program of The Kids CO-OP at The Barbara Bush Children's Hospital at Maine Medical Center, and is implemented in partnership with MaineHealth. Let's Go! is based on the following easy-to-remember message; to learn more the program visit www.letsgo.org.
5-2-1-0 GTCC aims to improve the nutrition and physical activity environment, policies and practices of child care facilities and is implemented through a trained Let’s Go! Partner. The program is designed around 10 evidence-based strategies and has adapted the Nutrition and Physical Activity Self-Assessment for Child Care (NAP SACC) 5-step intervention process and the Let’s Move! Child Care Checklist to help child care facilities implement lasting changes. The entire program is outlined in this toolkit. Our hope is that 5-2-1-0 GTCC will help support child care programs in raising and educating a healthier generation of children. Please direct any feedback, questions, or comments you may have to Let’s Go! at 662.3734, or email [email protected]. Sincerely, The Physical Activity and Nutrition in Early Care Education Committee A state-wide coalition of Physical Activity and Nutrition in Early Care and Education (PAN in ECE) specialists committed to PAN best practices for Maine’s ECE practitioners. The committee acts as a conduit of state and national evidence-based best practice for local dissemination. Member Organizations: Catholic Charities Child and Adult Care Food Program (CACFP) Central Maine Community College, Early Care and Education Program Penquis CACFP Let’s Go! Maine Center for Disease Control and Prevention Maine State CACFP University of Maine Cooperative Extension University of New England, School of Community and Population Health WinterKids
For more information on the PAN in ECE Committee please contact: Emily Cooke, Let’s Go! Early Childhood Program Manager, 207.662.1565, cookee1@mmc .org


The Implementation Toolkit is organized around the 6 steps of program implementation. Under each tab you will find the resources that will be helpful to you in assisting sites with that particular step. This entire toolkit is also available online at www.letsgo.org/representative-implementation-toolkit. PRE-TAB)
Let’s Go! Program Overview 5-2-1-0 Goes to Child Care Program Overview 5-2-1-0 Goes to Child Care Partner Benefits and Expectations Getting 5-2-1-0 Goes to Child Care Started Recruitment Handout for Providers: used to explain what 5-2-1-0 GTCC is and what the child
care facility can expect if they choose to participate in the program.
TAB 1) Step One: Registration Registration Overview Draft Text for Registration Confirmation Email: suggested text to use for email that will be sent
to each site to confirm their registration was successful and ask them to complete the self-assessment.
TAB 2) Step Two: Self-Assessment Self-Assessment Overview Self-Assessment Instruction Sheet: provided for the director when filling out the self-assessment. Blank Copy of Self-Assessment Tool: allows child care facilities to freely assess their own
environment, policies, and practices. Consists of various nutrition, physical activity and screen time sections and will suggest areas for possible improvement.
TAB 3) Step Three: Action Planning Action Planning Overview Blank Copy of Action Planning Document: used to help choose key areas for improvement,
create goals, and action items.
TAB 4) Step Four: Workshops and Trainings Workshops and Trainings Overview Five Workshops and Associated Handouts: designed to inform the staff about nutrition and
physical activity and help them understand why these topics are so important. Blank Copy of Workshop Evaluation Form
TAB 5) Step Five: Technical Assistance Technical Assistance Overview Program Monitoring Guide: provides a way for partners to track the technical assistance they
provide to sites.
TAB 6) Step Six: Evaluate, Revise & Repeat Evaluate, Revise & Repeat Overview Recognition Program one-pager: describes Let’s Go!’s 3-tiered recognition program for participating
sites. Let’s Go!’s Early Childhood Evaluation Plan: a self-assessment highlighted to
show what questions and answers will be measured to determine whether a site is implementing the Let’s Go! Strategies and their level of recognition.
Let’s Go!’s Early Childhood Evaluation Plan Cheat Sheet: a condensed version of the evaluation plan showing just the measured questions organized by strategy.
Table of Contents
04/12 R11/13
Adapted from the NAP SACC Program, Center for Health Promotion and Disease Prevention, The University of North Carolina, Chapel Hill, NC, May 2007.


What is Let’s Go!? Let’s Go!, a program at The Barbara Bush Children’s Hospital at Maine Medical Center, uses a multi-setting approach to reach youth and families where they live, learn, work, and play to reinforce the importance of healthy eating and active living. The program is based on the premise that if families are exposed to the same health promotion messages through several settings, and if those settings have policies and environments that support healthy choices, they will be more likely to adopt or maintain the behaviors in their daily lives.
The Let’s Go! multi-setting model is pictured below and includes the core principles of:
Healthy Places Support Healthy Choices Consistent Messaging Across Settings is Essential Strategies are Based on Science & Recommended by the Medical Community
The Let’s Go! program interventions center on the use of the common message of “5-2-1-0”. These behaviors are supported by science and endorsed as recommendations by medical professionals:
Let’s Go! has identified strategies and created tools to support and evaluate those strategies. All of these settings are supported by a marketing campaign that utilizes multiple methods of communication including social media.
For more information, contact the Let’s Go! Home Office
at 207.662.3734, or email us at [email protected].
5/10 R06/13


5-2-1-0 Goes to Child Care Program Overview
Let's Go! is a nationally recognized childhood obesity prevention program designed to increase healthy eating and active living in children from birth to 18. Let's Go! works in six settings (schools, early childhood, after school, healthcare, workplace and community) to reach children and families where they live, study, work, and play. Let's Go! is centered on the common message of "5-2-1-0".
5-2-1-0 Goes to Child Care is a program of the Let’s Go! early childhood sector. The program focuses its work around the tools developed by Let’s Go!, Nutrition and Physical Activity Self-Assessment for Child Care (NAP SACC), and Let’s Move!. Through the use of the 5-2-1-0 strategies listed below, NAP SACC’s 5-step intervention process, and the Let’s Move! Child Care Checklist, child care programs can address the policies, practices, and environments that influence healthy lifestyle behaviors.
In addition to a toolkit, this program provides Maine state licensing contact hours for completing certain program steps, free educational workshops for staff, and personalized guidance and assistance to support the child care programs in the adoption of the 10 strategies.
1. Provide healthy choices for snacks and celebrations; limit unhealthy choices.
2. Provide water and low fat milk; limit or eliminate sugary beverages.
3. Provide non-food rewards.
4. Provide opportunities for children to get physical activity every day.
5. Limit recreational screen time.
6. Participate in local, state, and national initiatives that support healthy eating and active living.
7. Engage community partners to help support healthy eating and active living at your site.
8. Partner with and educate families in adopting and maintaining a lifestyle that supports healthy eating and active living.
9. Implement a staff wellness program that includes healthy eating and active living.
10. Collaborate with Food and Nutrition Programs to offer healthy food and beverage options.
For more information, contact the Let’s Go! Home Office at 207.662.3734, or email us at [email protected]
05/10 R06/13
Redy icon represents a priority strategy


5-2-1-0 Goes to Child Care Representative Benefits and Expectations
A 5-2-1-0 GTCC Representative is expected to:
Participate in a Train the Trainer session to learn how to facilitate the 5-2-1-0 GTCC program with child care sites in their area (each representative must complete a training session before they are eligible to register sites for 5-2-1-0 GTCC).
Provide registered sites with technical assistance in the form of: Assisting sites in becoming familiar with the “5-2-1-0” message and adopting the message into
their program day. Assisting sites in moving through the steps of the program including:
Assisting sites with development of an Action Plan in a timely manner after they register (most effectively completed in-person either during a 1x1 site visit or a regional group meeting).
Helping facilitate completion of staff workshops or other healthy eating/active living trainings with sites – may provide personally, through a partner agency or via recorded webinars. In-person trainings may be done 1x1 or in a group setting.
Provision of additional technical assistance as needed (may take the form of in-person visits, phone calls or email communication).
Completion of at least two personal check-ins with sites (at least one in-person and a second that may be in-person, via email or by phone. In-person check-ins may be 1x1 or in a group setting. Action Planning visits DO count as a check-in). Note: to be considered a check-in, a site must be engaged in back and forth communication with you.
Help with data collection in the spring by connecting with registered sites to remind and encourage them to complete the post self-assessment.
5-2-1-0 GTCC Representatives can expect to receive:
Regular Partner TA calls facilitated by the Home Office. A minimum of 5 early childhood highlight emails to sites per year (at least one for each priority
strategy) on behalf of the Home Office and Representatives. A hard copy of both the Implementation Toolkit (includes a flash drive) and Provider Toolkit. Assistance with coordination of regional staff workshops including access to recorded online versions
of the 5-2-1-0 GTCC workshops. Additional TA as requested from the Home Office.
Participating Sites can expect to receive: An in-person Action Planning visit (1-2 hours; may be completed 1x1 or in a group setting) plus at least
one additional personal check-in from their 5-2-1-0 GTCC Representative. A minimum of 5 early childhood highlight emails per year (at least one for each priority strategy) sent
by the Home Office. Group sector meetings, if their 5-2-1-0 GTCC Representative chooses to provide. Access to free staff workshops with contact hours (5-2-1-0 GTCC Representatives to provide and/or
coordinate with assistance from the Home Office). A hard copy of the Provider Toolkit (including a laminated Activity Ring for brand new sites), to be
delivered by their 5-2-1-0 GTCC Representative. The opportunity to be recognized as either a Bronze, Silver, or Gold level Let’s Go! child care program
if they achieve the recognition criteria (process managed by the Home Office). The opportunity to apply for competitive mini-grants, if funding is available (process
managed by the Home Office). Additional TA as requested from their 5-2-1-0 GTCC Representative.
05/12 R11/13

Getting a facility committed and excited to participate is critical to successful program implementation. Strong, sustainable nutrition and physical activity environmental improvements begin with an interested, excited and motivated provider. Historically, Let’s Go! has not actively recruited sites to participate; however, if you are having difficulty finding sites to participate, there are two tools available to you: Recruitment Handout for Providers: located in the Pre-Tab section of your Implementation
Toolkit, this handout can be used as part of a mailing to local child care programs or be handed out at Early Childhood-related events/conferences.
“Healthy Habits Begin Early: Prevention of Childhood Obesity” PowerPoint: Located on your flash-drive, this PowerPoint provides an overview of the obesity epidemic, its consequences, Let’s Go!’s model, message and 5-2-1-0 Goes to Child Care Program, and suggests priority areas for Early Childhood programs considering physical activity and nutrition-related changes. Use this presentation at Early Childhood-related conferences or trainings. This presentation can also be helpful in educating newly engaged sites on Let’s Go! and the 5-2-1-0 GTCC program, as well as what to expect as the program year proceeds.
Overview
As you find excited, ready and willing facilities to participate, you are ready to begin implementing the 6 steps of the 5-2-1-0 GTCC program. Let’s Go!’s program year runs from July 1 to June 30; enrollment typically opens in May and closes in November. Steps 2-6 can be completed once or multiple times over the program year until a
provider is satisfied with their nutrition and physical activity environment.
5-2-1-0 GTCC Program Steps
1. Registration
2. Self-Assessment
3. Action Planning
4. Workshops and Trainings
5. Technical Assistance
6. Evaluate, Revise, and Repeat
04/12 R11/13
Getting 5-2-1-0 Goes to Child Care Started...
Adapted from the NAP SACC Program, Center for Health Promotion and Disease Prevention, The University of North Carolina, Chapel Hill, NC, May 2007.


04/12 R11/13
I can help!
Are you too busy to improve the nutrition and physical activity environments at your facility, but care about the health of the children you serve? As a trained 5-2-1-0 Goes to Child Care (5-2-1-0 GTCC) Partner, I’m here to help! The 5-2-1-0 GTCC program is an obesity prevention program that helps child care facilities improve their nutrition and physical activity environment by changing policies and practices. Using the self-assessment instrument you will be able to identify strengths and weaknesses related to your nutrition and physical activity environment. This will be followed by goal setting, staff education, and on-going support and assistance provided by me, your trained 5-2-1-0 GTCC partner. Don’t worry! 5-2-1-0 GTCC is designed to be user friendly, time and resource efficient, and easily integrated into your busy day.
What will you receive?
Free hard copy of a toolkit loaded with resources for both your staff and families Access to free training (with contact hours) for your staff Bi-Monthly e-newsletters Suggestions for and help in improving areas such as fruit, vegetable and fried food consumption,
holiday celebrations, television viewing, and indoor/outdoor active play time, just to name a few Ideas on how to improve your own health Sample policy language for your parent and staff handbooks
What is expected of your facility?
Timely completion of the self-assessment instrument Participation in a goal setting meeting Participation in staff training workshops The commitment to work through your chosen improvements
Are you interested in Changing Your Facility’s Nutrition and
Physical Activity Environment?
Adapted from the NAP SACC Program, Center for Health Promotion and Disease Prevention, The University of North Carolina, Chapel Hill, NC, May 2007.

04/12 R11/13
Why should you care?
Good nutrition and plenty of physical activity are key to a young child’s growth and development. These behaviors begin to be set early in life and are fostered by the environment in which children live and play. Because many children spend much of their day in child care settings, these environments are critical to the development of healthy behaviors. Creating a healthy environment requires leadership and commitment.
Goals of the 5-2-1-0 GTCC Program
1. To provide child care facilities with an easy tool to evaluate their own nutrition and physical activity environment and make changes to support healthy weight behaviors in young children.
2. To promote healthy eating in children from birth to 5 years old in child care settings by serving appropriate foods and role modeling healthy eating behaviors.
3. To promote active play in children from birth to 5 years old in child care settings by providing plenty of indoor and outdoor active playtime and role modeling active lifestyles.
4. To reach out to parents through child care settings to promote healthy weight behaviors at home.
Local 5-2-1-0 Goes to Child Care Partner contact information:
How do you get started?
Congratulations! You have made the important decision to improve the health of young children by making it easier for them to eat healthy and be more active. For more information about Let’s Go! and 5-2-1-0 GTCC in general visit www.letsgo.org. To get started, please contact:
Adapted from the NAP SACC Program, Center for Health Promotion and Disease Prevention, The University of North Carolina, Chapel Hill, NC, May 2007.

What is the Registration Process?
Registration for 5-2-1-0 GTCC is typically open from May to November. Closing registration in November ensures that enrolled programs have plenty of time to both set and achieve their goals for the year before the end-of-year evaluation in May. All sites who wish to participate in 5-2-1-0 GTCC must register via their region’s online registration form. The links to these forms will be provided to Let’s Go! partners when registration opens in May, who will then be responsible for connecting with interested sites to help them register for the program.
Each week, partners will be provided with a list of all facilities that have registered in their region. This will allow partners to send a welcome email and to schedule their Action Planning meeting (see Step Three) with each site. Welcome emails sent to brand new sites should also include a copy of the self-assessment tool and instruction guide (see Step Two).
Working with the Provider
Before registering sites, it is important that the partner is sure they have the capacity to provide adequate technical assistance to each facility they register. In addition, the partner should personally connect with each potential site (including returning sites) to be sure they are ready and willing to participate before they (re-)register.
Upon determining a facility wants to participate, the partner may either send the registration link directly to the site to complete on their own OR complete the form with the site in-person or over the phone. Sites should not be registered without their participation in the process.
Keys to Success
All child care sites register at the ‘Redy 2’ level. There is currently no support in the child care setting for the ‘Redy 1’ level. After the close of registration, sites may enroll as ‘Late Registrants’. Late registrants will receive all early childhood communications and are first in line to register at the Redy 2 level in the coming year (as local capacity allows). There are no expectations of late registrants to complete any of the program steps and no expectations of you, the local partner, in how much technical assistance to provide; you both may do as much or as little as you like. Late registrants will not receive a hard copy of the toolkit, are not surveyed at the end of the program year and are not eligible for the recognition program.
Register sites by physical location instead of classroom. So even though a center or Head Start facility may have multiple classrooms in one location, they register as one participating program.
Step One: Registration
04/12 R11/13
Adapted from the NAP SACC Program, Center for Health Promotion and Disease Prevention, The University of North Carolina, Chapel Hill, NC, May 2007.

Be sure to send sites YOUR region’s personalized registration link. This will ensure their registration is linked to you. Note: Partners NOT affiliated with a Let’s Go! Dissemination Partner share a common “community partner” registration link. These partners must make sure sites know to enter the partner’s first and last name as their ‘Local Let’s Go! Partner’.
Some returning sites may delay completing re-registration because they feel overwhelmed. Wait to re-register existing sites until the evaluation period has ended so sites are not overwhelmed.
Make sure your returning sites carefully select/enter their program name to ensure it matches the name they registered under the prior year.
Make sure your sites know that ‘subsidized slots’ refers to the total number of slots allotted for children receiving any kind of payment discount or assistance. This includes both children enrolled in Head Start and those receiving a state child care voucher.
Step One: Registration
04/12 R11/13
Adapted from the NAP SACC Program, Center for Health Promotion and Disease Prevention, The University of North Carolina, Chapel Hill, NC, May 2007.

Draft Text for Registration Confirmation Emails
Note: The below text is provided as a template for confirming registration with your sites. This is recommended text from the Home Office; however, you may feel free to tailor and adapt for your sites to meet their unique needs. In addition to confirming registration, this is intended to be a relationship building opportunity between you and your sites! To: Individual Completing Registration; Child Care Site Champion
From: 5-2-1-0 Goes to Child Care Partner
Subject: Welcome to Let’s Go!’s Child Care Program
Attach: 1.) Modifiable and Savable PDF of Child Care Self-Assessment
2.) Self-Assessment Instruction Sheet
Email Body Text:
Welcome aboard 5-2-1-0 Goes to Child Care, and congratulations! You have successfully registered for the current program year and are one step closer to providing the healthiest environment for the children in your care, both for today and for years to come! Your next step is to complete the 5-2-1-0 Goes to Child Care self-assessment. A modifiable and savable PDF version of the assessment and an instruction guide are attached. This should take you about 30-45 minutes to complete; however if you are not able to finish it in one sitting, you may stop, save your work and come back to finish the assessment later. Please make sure you click ‘Save As’ to save the document to your computer so your work is not lost. To assist you in completing the assessment, have your staff and parent handbooks at hand and invite any key staff (such as a program chef, lead teachers, etc.). Once you complete the assessment, please email it back to me by attaching it to an email. I will be calling you within the next two weeks to schedule an in-person site visit. During that site visit, we'll go over your self-assessment results and help you create an action plan. I look forward to working with you and helping you achieve your healthy eating and active living goals! In health,
Insert Name Insert Organization Name Your Local Let’s Go! Partner
05/12 R11/13


04/12 R11/13
What is the Self-Assessment Instrument?
Let’s Go! has adapted the Let’s Move! Child Care Checklist for use in step two. The self-assessment instrument is an intervention tool that allows child care facilities to freely assess their own environment, policies, and practices and will suggest key areas for improvement. The adapted self-assessment is broken down by age group and topic area, with specific questions under each area. Each question has a variety of possible answers, representing a continuum of practice, from minimal standard on the far left, through best practice on the far right.
The Let’s Move! initiative has 5 main goals for child care programs to strive for. As child care programs work towards achieving the best practice standards, they will be reaching these goals. Figure 1 shows how these 5 goal areas crossover with Let’s Go!’s message “5-2-1-0”.
Figure 1. Let’s Move! Child Care Goals and “5-2-1-0”
Step Two: Self-Assessment
Adapted from the NAP SACC Program, Center for Health Promotion and Disease Prevention, The University of North Carolina, Chapel Hill, NC, May 2007.
Let’s Move! Child Care Goal Corresponding Let’s Go!
5-2-1-0 Behavior
Food Serve fruits or vegetables at every meal, eat meals family-style whenever possible, and don't serve fried foods.
Infant Feeding For mothers who want to continue breastfeeding, provide their milk to their infants and welcome them to breastfeed during the child care day. Support all new parents' decisions about infant feeding.
Screen Time No screen time for children under 2 years. For children age 2 and older, strive to limit screen time to no more than 30 minutes per week during child care, and work with parents and caregivers to ensure children have no more than 1-2 hours of quality screen time per day (as recommended by the American Academy of Pediatrics).
Physical Activity Provide 1-2 hours of physical activity throughout the day, including outside play when possible.
Beverages Provide access to water during meals and throughout the day, and don't serve sugary drinks. For children age 2 and older, serve low-fat (1%) or non-fat milk, and no more than one 4- to 6-ounce serving of 100% juice per day.
Drink less sugar. Try water and low fat milk instead of soda and drinks with lots of sugar.
Limit recreational TV or computer use to two hours or less each day.
Eat at least five fruits and vegetables a day.
Eat at least five fruits and vegetables a day.
Get one hour or more of physical activity every day.

04/12 R11/13
Figure 2. Let’s Go! Strategies
1. Provide healthy choices for snacks and celebrations; limit unhealthy choices.
2. Provide water and low fat milk; limit or eliminate sugary beverages.
3. Provide non-food rewards.
4. Provide opportunities for children to get physical activity every day.
5. Limit recreational screen time.
6. Participate in local, state, and national initiatives that support healthy eating and active
living.*
7. Engage community partners to help support healthy eating and active living at your site.* 8. Partner with and educate families in adopting and maintaining a lifestyle that supports
healthy eating and active living.
9. Implement a staff wellness program that includes healthy eating and active living.*
10. Collaborate with Food and Nutrition Programs to offer healthy food and beverage
options.†
Working with the Provider
After a site registers for 5-2-1-0 GTCC, their Let’s Go! partner will send them a welcome email with the self-assessment tool and instruction guide attached. Ideally, providers will be able to complete the assessment tool without any assistance. However, if a partner has providers reach out for assistance on how a question applies to them, they may assist them. Let’s Go! Partners should do their best to help a provider simply understand what a question is asking and then let the provider determine the best answer to represent their current practice. Completion of this program step makes the provider eligible for licensing contact hours. Note: It is estimated this step will take 1/2 to 1 hour to complete. Provide a certificate for the actual length of time spent on this step which may be more or less than this estimate.
The Let’s Go! Program is based around 10 key strategies (Figure 2) which are consistent across the school, after school and early childhood sectors and align with the CDC and the Institute of Medicine’s recommendations to prevent childhood obesity. Let’s Go! has aligned these strategies with the self-assessment instrument (see “Let’s Go!’s Early Childhood Evaluation Plan” under Tab 6 - Step Six: Evaluate, Revise & Repeat). As child care programs work to achieve the best practice standards, they are also implementing the Let’s Go! Strategies.
Adapted from the NAP SACC Program, Center for Health Promotion and Disease Prevention, The University of North Carolina, Chapel Hill, NC, May 2007.
Redy icon represents a priority strategy.
* These strategies could not be directly measured by any of the self-assessment questions. Therefore a section titled “Supportive Strategies” was added to the self-assessment to evaluate these strategies. A site may choose to focus on any of these areas as part of their Action Plan.
† This strategy is measured by whether or not the site participates in the Child and Adult Care Food Program which is captured on their registration form for the program year.

04/12 R11/13
Keys to Success
Become very familiar with the self-assessment questions and organization. The more familiar you are with the content, the better able you will be able to help your sites with any questions they may have.
Encourage child care providers to read each question carefully. When going too quickly, it
can be easy to select an answer that inaccurately represents the program’s practices. Remind providers to select ‘Save As’ to save
the self-assessment document to their computer so they do not lose their work. The is allows them to complete the self-assessment in more than one sitting, if necessary.
Encourage providers to set aside at least 30
minutes of uninterrupted time to successfully complete the assessment and to include appropriate personnel (e.g. center food service staff, head teachers) and materials (e.g. staff and parent handbooks). Some providers report the assessment takes them up to 1 hour to compete.
Encourage self-reflection and honesty and be sure to stress that answers will in no way
reflect poorly on the facility or get them into trouble. It is just to be used as a starting point for the intervention.
Refer providers with questions first to the instruction sheet as this will likely answer most
of their questions. Remind providers they may skip questions unrelated to their program (e.g. they don’t
serve a certain age group or do not have TVs or computer available, etc.). There are skip-forward patterns built into the self-assessment to guide providers in automatically doing this.
Particularly with family child care providers, there may be instances where a provider
simply needs to pick the best suited answer to what their practice currently is. When you provide the self-assessment and instructions, set a date for an in-person
meeting to discuss the self-assessment results and start action planning. This should be approximately 2-3 weeks in the future so that (s)he doesn’t feel rushed, but completes the assessment within an appropriate time period.
Provide a small incentive for completing the self-assessment instrument on time, if funding
allows.
Adapted from the NAP SACC Program, Center for Health Promotion and Disease Prevention, The University of North Carolina, Chapel Hill, NC, May 2007.

05/12 R11/13
Self-Assessment Instruction Sheet and Glossary
GENERAL INSTRUCTIONS When completing this instrument, it is important to:
1) Honestly assess your program’s environment and day-to-day practices. This way your local 5-2-1-0 Goes to Child Care Partner can help you set and meet specific nutrition and physical activity-related goals.
2) Keep in mind what your facility does the majority of the time as your practices may fall into more than one category. If no answer seems quite right, just pick the closest fit.
3) Involve any key staff members that are familiar with day-to-day practices and can help in answering questions (e.g. food service staff, lead teachers, etc.).
FAMILY CHILD CARE PROVIDERS This self-assessment was originally designed for child care centers. Because of this, there are some questions where family child care providers may find it hard to choose an answer that accurately represents their day-to-day practices. Let’s Go! knows this is a challenge and is working to address it. For now, here is how Let’s Go! recommends home-based programs think about the assessment questions.
Anywhere the assessment refers to ’facility’ or ‘classrooms’ think of any area of your home used in the care of your enrolled children. So, if you care for children using the kitchen, living room and basement of your home, these areas make up your program’s ‘facility’ and ‘classroom’.
The assessment asks separate questions for the different age groups - infants, toddlers and preschoolers. Many home providers care for infants through preschool-age children all together. While it could be easier to have one question for all age groups, they are broken up because there are different recommended best practices for each age group. Answering separate questions for infants, toddlers and preschoolers, even if they are all being treated the same way, will help you identify potential areas of improvement for different age groups. Your local Let’s Go! partner can help you think in new and creative ways about how to provide all of the children in your care the best experience for their age and stage of development within the limits of your program’s space.
For example - It can be challenging to make sure infants and toddlers receive zero screen time when they are in the same room as preschoolers who may watch television. Answering separate screen time questions for each age group can help identify this as an area for growth that a provider may be interested in working on.
Sometimes you may feel there is just no good answer for you to comfortably choose. Select the closest possible answer to what you do. You will be able to review your answers with your local Let’s Go! partner later when creating an Action Plan for the year. Your partner will be able to help you determine how to apply recommended best practices within the limit’s of your program space. Remember, this assessment is simply a tool to help you find opportunities for growth related to your physical activity and nutrition practices.
GLOSSARY
CTG: Community Transformation Grant; a project of the Maine Center for Disease Control and Prevention (CDC) that Let’s Go! works closely with. CTG Coordinators partner with Let’s Go! and use 5-2-1-0 Goes to Child Care to work with child care providers around healthy eating and active living.
Section 1: Food Served Canned in juice: Canned without additional sugars such as light and heavy syrups.
Adapted from the NAP SACC Program, Center for Health Promotion and Disease Prevention, The University of North Carolina, Chapel Hill, NC, May 2007.
05/12 R11/13
Culturally Appropriate: Materials that are suitable to the culture of children you serve. For example, if you have children who speak primarily Spanish, then there should be some Spanish-language versions of materials displayed.
Family style meals: Food is placed on plates or in bowls on the table and children are allowed and encouraged to serve themselves.
Feeding Plan: A form or plan specific to each child that details what, how much, and how often an infant eats; in addition to listing any allergies and additional instructions.
Formal discussion/education: This may be done using a pre-existing curriculum such as Color Me Healthy or I Moving I Am Learning or it can be lessons put together by the teacher. Formal nutrition education would be part of the lesson plan.
Fruit: Includes all fruits, whether they are fresh, frozen, or canned, including applesauce and dried fruit. This does not include 100% fruit juice.
Informal discussion/education: Discussion with the children by teachers that is not part of a formal lesson. This may include talk about that day’s lunch and how it is good for the body or talk on the playground about how running builds strong muscles.
Materials supplied by commercial entities/manufacturers: Items that have company logos or other advertising as part of the materials that promotes that brand name and/or their products.
Nutrition education for parents: Things such as workshops, activities, take home materials, and health fairs that provide families with information on healthy eating or cooking.
Pre-fried: Often frozen chicken nuggets, fish sticks, French fries and tator tots were fried before processing. Even if you bake these items before serving they have extra fat due to frying.
Self-feeding skills: The skills children acquire learning to feed themselves; includes finger-feeding and using a fork and/or spoon.
Training opportunities on nutrition for providers: May include general information related to infant, toddler, or preschooler nutrition, introduction to a new nutrition curriculum, healthy meal/menu planning, etc. This does not include training on the food program guidelines or food safety/sanitation.
Vegetables: Includes all vegetables and potatoes, unless they are fried. Does not include beans like pinto, kidney and baked beans.
Section 2: Beverages
Beverage education for parents: Things such as workshops, activities, take home materials, and health fairs that provide families with information on best beverage choices for children, strategies on decreasing intake of sugary beverages and/or encouraging more water and milk, etc.
Training opportunities on beverage recommendations for providers: May include general information related to what kinds of beverages and serving sizes are appropriate for infants, toddlers and/or preschoolers, the amount of sugar found in different beverages, strategies on decreasing intake of sugary beverages and/or encouraging more water and milk, etc.
Section 3: Physical Activity
Active play time: Indoor or outdoor play time, which allows children to be able to run, skip, hop, jump, etc. This type of play time does not have any limitations.
Physical activity education for parents: Things such as workshops, activities, take home materials, and health fairs that provide families with information on the importance of physical activity and/or ideas for increasing physical activity.
Standardized curriculum: This can be a pre-existing curriculum such as Color Me Healthy or I Moving I Am Learning or it can be lessons put together by the teacher. Formal physical activity education would be part of the lesson plan.
Adapted from the NAP SACC Program, Center for Health Promotion and Disease Prevention, The University of North Carolina, Chapel Hill, NC, May 2007.

05/12 R11/13
Structured/Teacher-led physical activity: An activity that is led by the teacher, promotes active movements and is designed so all young children are active participants.
Training opportunities in physical activity for providers: Includes education on specific areas related to physical activity such as ways to reduce sedentary time while at child care, ways to increase movement throughout the day, what are developmentally appropriate gross motor activities, etc. Does not include training on playground safety.
Tummy Time: Time babies spend on their stomachs to strengthen neck and back muscles. This should only be done when babies are awake and supervised, not at nap times.
Withholding active play time: Making a child sit inside or outside for an extended period of time or shortening active play time for the entire class. It is not defined by short time-outs.
Section 4 - Screen Time Educational programming: Television and videos that are commercial and advertisement-free and
are solely for educational or learning purposes. Screen time: Includes time viewing television and DVDs in addition to computer time. Screen time reduction/media literacy education for parents: Things such as workshops,
activities, take home materials, and health fairs that provide families with information on recommended screen time limits, strategies to reduce screen time and alternate activities, how media messages are interpreted by children, etc.
Training opportunities on screen time reduction/media literacy for providers: May include education on strategies to reduce screen time, alternate activities, how to understand media messages and/or how messages are interpreted by children, etc.
Section 5 - Supportive Strategies Including community organizations in wellness promotion activities: Using staff or other
resources of organizations within your community to help promote healthy messages at your facility. For example: setting out pamphlets from local dentist’s office on sugar and tooth decay, hosting a healthy food drive at your program for a local food bank, borrowing a StoryWalk from your local library, or visiting a local farm and having the farmer talk with the kids about growing food.
Local, state or national initiatives: Programs or campaigns centered around improving nutrition, physical activity and/or screen time reduction. For example: Local - local gardening or Buy Local programs; State - WinterKids or Hannaford Guiding Stars Program; National - Let’s Move! Child Care or National Nutrition Month.
Staff wellness program: Taking purposeful steps to encourage and make it easier for staff to personally make healthier choices. For example: encouraging walking meetings, supporting healthy staff celebrations, or allowing for physical activity breaks throughout the day.
Section 6 - Program Policies Celebration Foods: Includes food for all events hosted by the facility; for example, birthdays,
Holiday parties (Valentine’s Day, Halloween, etc.), Family Fun Days, etc. Food as a reward: Using food (any kind of food, whether a sweet or a generally “healthy food”) as a
prize or reward. For example: candy for potty training, pizza party for good behavior, extra crackers for listening to directions, etc.
Opportunities for physical activity: Providing the time and space for children to move freely in whatever gross-motor movements are age-appropriate. For example: rolling, crawling and/or scooting for infants; running, climbing, and/or jumping for toddlers and preschoolers.
Adapted from the NAP SACC Program, Center for Health Promotion and Disease Prevention, The University of North Carolina, Chapel Hill, NC, May 2007.


2013-2014 Nutrition and Physical Activity Self-Assessment for Early Care and Education Programs
INTRODUCTION Please read each statement or question carefully and check the response that best fits your child care program. Refer to the instruction sheet for a glossary of terms and phrases. Please enter the following information. Name of child care program: _______________________________________________________________________
Contact name at program: _________________________________________________________________________
Physical Address: ________________________________________________________________________________
Contact phone/email: ____________________________________________________________________________
Date Completed: ________________________
3. Which age groups does your child care program serve? (Check all that apply)
Infant (Birth-1 year) Toddlers (Ages 1-2) Preschoolers (Ages 3- 5)
4. My child care program is: A full day program A half day program 5. Which workshops or webinars did you and your staff participate in during the past program year?
No one from our program attended
(0%)
Some staff attended (less
than 50%)
Most staff attended (at least
50%) All staff attended
(100%)
Supersizing Our Children: The Obesity Epidemic
Eat Right, Grow Strong: Nutrition for Young Children
Moving Children to Good Health: Physical Activity for Young Children
Growing Healthy Kids Together: Working with Families
Stepping Toward a Healthy Lifestyle: Personal Health and Wellness
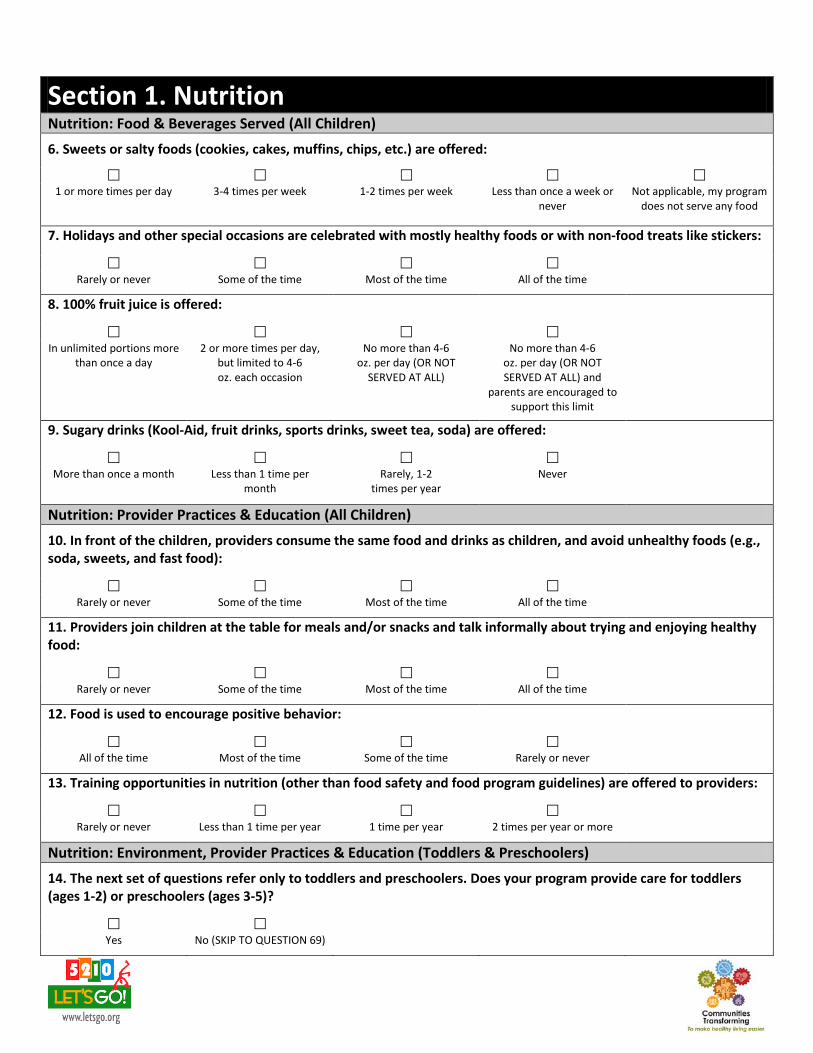
Section 1. Nutrition Nutrition: Food & Beverages Served (All Children)
6. Sweets or salty foods (cookies, cakes, muffins, chips, etc.) are offered:
1 or more times per day 3-4 times per week 1-2 times per week Less than once a week or
never Not applicable, my program
does not serve any food
7. Holidays and other special occasions are celebrated with mostly healthy foods or with non-food treats like stickers:
Rarely or never Some of the time Most of the time All of the time
8. 100% fruit juice is offered:
In unlimited portions more
than once a day 2 or more times per day,
but limited to 4-6 oz. each occasion
No more than 4-6 oz. per day (OR NOT
SERVED AT ALL)
No more than 4-6 oz. per day (OR NOT SERVED AT ALL) and
parents are encouraged to support this limit
9. Sugary drinks (Kool-Aid, fruit drinks, sports drinks, sweet tea, soda) are offered:
More than once a month Less than 1 time per
month Rarely, 1-2
times per year Never
Nutrition: Provider Practices & Education (All Children)
10. In front of the children, providers consume the same food and drinks as children, and avoid unhealthy foods (e.g., soda, sweets, and fast food):
Rarely or never Some of the time Most of the time All of the time
11. Providers join children at the table for meals and/or snacks and talk informally about trying and enjoying healthy food:
Rarely or never Some of the time Most of the time All of the time
12. Food is used to encourage positive behavior:
All of the time Most of the time Some of the time Rarely or never
13. Training opportunities in nutrition (other than food safety and food program guidelines) are offered to providers:
Rarely or never Less than 1 time per year 1 time per year 2 times per year or more
Nutrition: Environment, Provider Practices & Education (Toddlers & Preschoolers)
14. The next set of questions refer only to toddlers and preschoolers. Does your program provide care for toddlers (ages 1-2) or preschoolers (ages 3-5)?
Yes No (SKIP TO QUESTION 69)
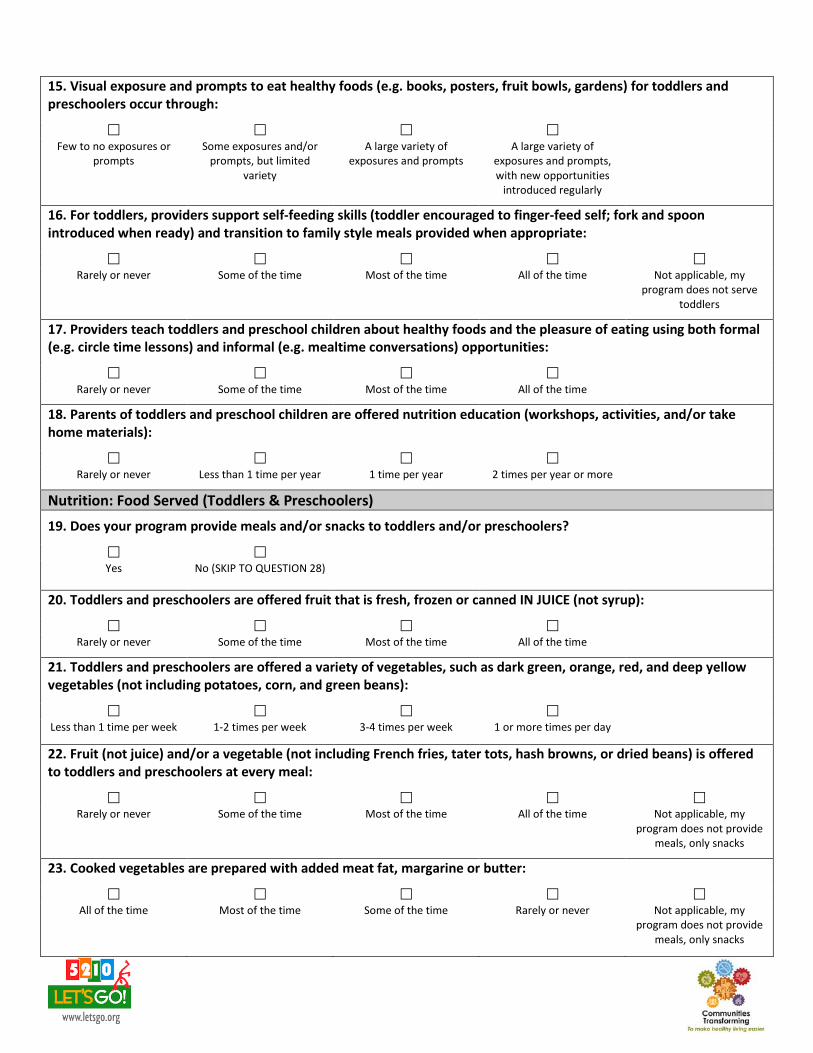
15. Visual exposure and prompts to eat healthy foods (e.g. books, posters, fruit bowls, gardens) for toddlers and preschoolers occur through:
Few to no exposures or
prompts Some exposures and/or
prompts, but limited variety
A large variety of exposures and prompts
A large variety of exposures and prompts, with new opportunities
introduced regularly
16. For toddlers, providers support self-feeding skills (toddler encouraged to finger-feed self; fork and spoon introduced when ready) and transition to family style meals provided when appropriate:
Rarely or never Some of the time Most of the time All of the time Not applicable, my
program does not serve toddlers
17. Providers teach toddlers and preschool children about healthy foods and the pleasure of eating using both formal (e.g. circle time lessons) and informal (e.g. mealtime conversations) opportunities:
Rarely or never Some of the time Most of the time All of the time
18. Parents of toddlers and preschool children are offered nutrition education (workshops, activities, and/or take home materials):
Rarely or never Less than 1 time per year 1 time per year 2 times per year or more
Nutrition: Food Served (Toddlers & Preschoolers)
19. Does your program provide meals and/or snacks to toddlers and/or preschoolers?
Yes No (SKIP TO QUESTION 28)
20. Toddlers and preschoolers are offered fruit that is fresh, frozen or canned IN JUICE (not syrup):
Rarely or never Some of the time Most of the time All of the time
21. Toddlers and preschoolers are offered a variety of vegetables, such as dark green, orange, red, and deep yellow vegetables (not including potatoes, corn, and green beans):
Less than 1 time per week 1-2 times per week 3-4 times per week 1 or more times per day
22. Fruit (not juice) and/or a vegetable (not including French fries, tater tots, hash browns, or dried beans) is offered to toddlers and preschoolers at every meal:
Rarely or never Some of the time Most of the time All of the time Not applicable, my
program does not provide meals, only snacks
23. Cooked vegetables are prepared with added meat fat, margarine or butter:
All of the time Most of the time Some of the time Rarely or never Not applicable, my
program does not provide meals, only snacks

24. Fried or pre-fried potatoes (French fries, tater tots, hash browns) are offered to toddlers and preschoolers:
2 or more times per week 1 time per week Less than 1 time a week Never Not applicable, my
program does not provide meals, only snacks
25. Fried or pre-fried (frozen and breaded) meats (chicken nuggets) or fish (fish sticks) are offered to toddlers and preschoolers:
2 or more times per week 1 time per week Less than 1 time a week Never Not applicable, my
program does not provide meals, only snacks
26. Beans or lean meats (baked or broiled chicken, turkey, or fish) are offered to toddlers and preschoolers:
Less than 1 time per week 1-2 times per week 3-4 times per week 1 or more times per day Not applicable, my
program does not provide meals, only snacks
27. Preschooler meals and/or snacks are served family style (children are encouraged to serve themselves with limited help):
Rarely or never Some of the time Most of the time All of the time Not applicable, my
program does not serve preschoolers
Nutrition: Beverages Served (Toddlers & Preschoolers)
28. Drinking water is available:
Upon request Upon request or during
designated water breaks Inside only, where it is
visible and freely available Inside and outside, where it is visible and available
for self-serve
29. During indoor and outdoor play, providers prompt children to drink water:
Rarely or never Some of the time Most of the time All of the time
30. Water is offered to children over the age of 1 year (but not as a substitute for milk when it is a required food component):
Rarely or never 1 time per week or less 2-4 times per week 1 time per day or more
31. Milk served to children ages 2 years and older is:
Whole or regular Only 2% reduced fat Always 1-2% low-fat Always 1% or
skim/nonfat Not applicable, my program does not
serve any milk
Not applicable, my program does not
provide care for children ages 2 years and older

32. Flavored milk is served to children:
More than once a month Less than 1 time per
month Rarely, 1-2
times per year
Never Not applicable, my program does not serve
any milk
Nutrition: Beverages Served, Provider Practices & Education (Toddlers & Preschoolers)
33. Beverages offered to toddlers over 1 year are offered in a bottle:
All of the time Most of the time Some of the time Rarely or never Not applicable, my
program does not provide care for toddlers
34. Training opportunities on juice and other beverage recommendations for toddlers and preschoolers are offered to providers:
Rarely or never Less than 1 time per year 1 time per year 2 or more times per year
35. Parents of toddlers and preschoolers are offered education on juice and other beverage recommendations (e.g., special programs, newsletters, information sheets):
Rarely or never Less than 1 time per year 1 time per year 2 or more times per year
Section 2. Physical Activity/Screen Time for Preschoolers
36. The next set of questions refer only to preschoolers (ages 3-5). Does your program provide care to preschoolers?
Yes No (SKIP TO QUESTION 58)
Physical Activity: Time Provided (Preschoolers)
37. Active play time (indoor and outdoor) is provided to all preschool children, including children with special needs:
45 minutes or less each
day 46-90 minutes each day 91-120 minutes each day More than 120 minutes
each day
38. In preschool classrooms, structured (or teacher-led) activities are provided to all children, including children with special needs:
1 time per week or less 2-4 times per week 1 time per day 2 or more times per day
39. Outdoor active play time is provided to all preschool children, including children with special needs:
1 time a day for 30
minutes or less 1 or more times a day for a
total of 30-45 minutes 1 or more times a day for a
total of 45-60 minutes 2 or more times each day
for a total of 60 minutes or more

40. During a typical day, excluding naps and meals, preschool children are expected to remain seated:
More than 30 minutes at a time, or 15-30 minutes on
3 or more occasions
15-30 minutes on 2 occasions
15-30 minutes but only 1 occasion
No more than 15 minutes at a time
Physical Activity: Provider Practices & Education (Preschoolers)
41. In preschool classrooms, active play time is:
Often withheld for
misbehavior Sometimes withheld for
misbehavior Never withheld for
misbehavior Never withheld for
misbehavior and we have a written policy
42. During preschool children’s active play time, providers:
Supervise play only (mostly sit or stand)
Sometimes encourage children to be active
Sometimes encourage children to be active and
join children in active play
Often encourage children to be active and join
children in active play
43. Training opportunities in physical activity for preschool children (not including playground safety) are offered to providers:
Rarely or never Less than 1 time per year 1 time per year 2 or more times per year
44. Parents of preschool children are offered physical activity education (e.g., special programs, newsletters, information sheets):
Rarely or never Less than 1 time per year 1 time per year 2 or more times per year
Physical Activity: Environment (Preschoolers)
45. Indoor gross motor play area for preschool children, including those with special needs, consists of:
Space only suitable for
quiet play Space for limited
movement (jumping and rolling)
Ample space for some active play (jumping, rolling, and skipping)
Space for all activities including running
46. Outdoor play areas for preschool children, including those with special needs, consists of:
1-2 different play areas
(e.g., sandbox, swing set) but no open space for
running or track/path for wheeled toys
2-3 different play areas, but limited space for running and use of
wheeled toys
Multiple play areas, and either an open space for
running or a track/path for wheeled toys
Multiple play areas, open space for running, and a track/path for wheeled
toys
47. Portable play equipment (e.g., wheel toys, balls, hoops, ribbons) for preschool children consists of:
Limited variety and
children must take turns Some variety but children
must take turns Good variety both indoors and outdoors but children
must take turns
Lots of variety both indoors and outdoors for
children to use at the same time

Screen Time: Availability (Preschoolers)
48. The next set of questions refer to screen time for preschoolers. Does your program have a television or a computer?
Yes, my program has a
television and/or a computer
No, my program does not have a television or a
computer (SKIP TO QUESTION 58)
49. In preschool classrooms, televisions are:
Located in every classroom
(100%) Located in most
classrooms (at least 50%) Located in some
classrooms (less than 50%) Stored outside of classrooms,
except for occasional use
Not applicable, my program does not have
a television
50. For preschool children, the total amount of screen time:
Is not limited At child care, we strive to
achieve 2 hours or less per week
At child care, we strive to achieve no more than 1
hour per week
At child care, we strive to achieve no more than 30
minutes per week, and we work with parents/caregivers
to ensure that children have no more than 1-2 hours per day
51. For preschool children, television/DVD viewing includes:
All types of programming and videos, with limited
coordination with the curriculum
Educational and some commercial programming and videos, some of which
are integrated with the curriculum
Mostly educational, age-appropriate programming and videos, many of which
are integrated with the curriculum
Only commercial-free, age-appropriate, educational
programming that is integrated with the
curriculum
Not applicable, my program does not have a television, nor do we view shows using the
internet
52. For preschool children, television/DVD viewing during meals or snack times occurs:
All of the time Most of the time Some of the time Rarely or never Not applicable, my
program does not have a television, nor do we view shows using the
internet
53. Television/video viewing is used as a reward in preschool children’s classrooms:
All of the time Most of the time Some of the time Rarely or never Not applicable, my
program does not have a television, nor do we view shows using the
internet
54. Among preschool children, computers are:
Available for use all of the time, and time allowed per
child is unlimited
Available several times during the day and each child is allowed between
30 and 45 minutes per day
Available only during a set time of day, and each child is allowed between 15 and
30 minutes per day
Available only during a set time of day, and each child is limited to 15 minutes per day
Not applicable, my program does not have
a computer
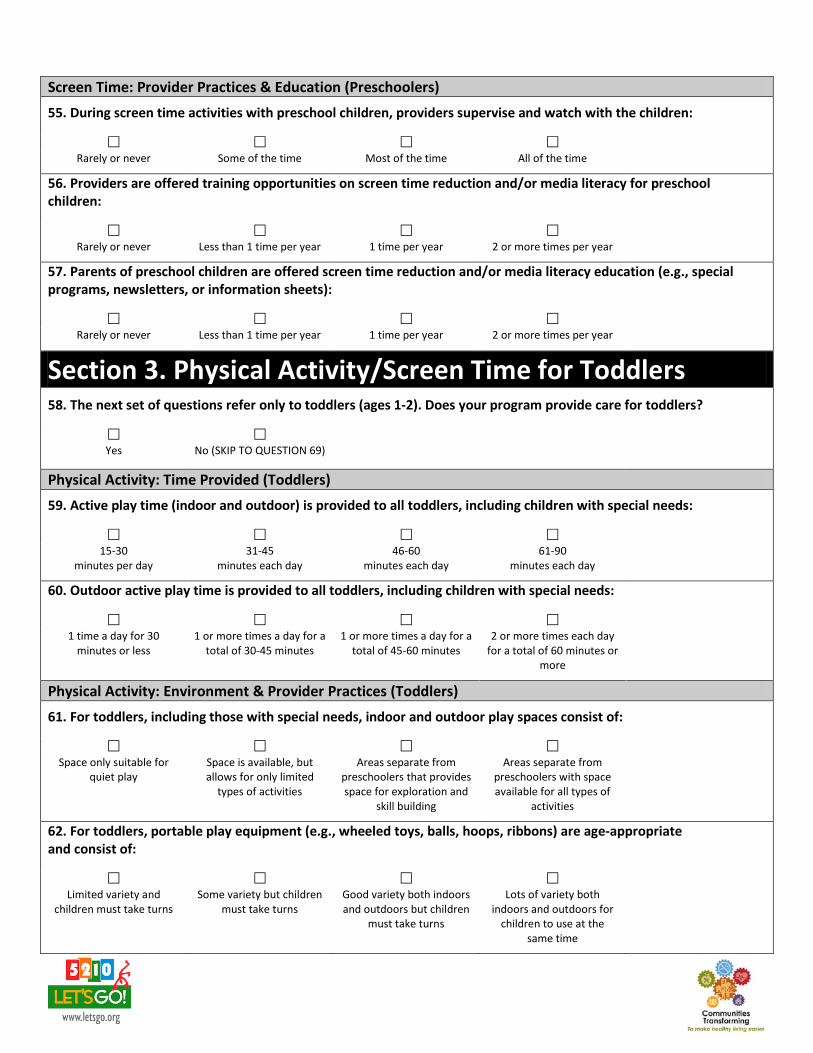
Screen Time: Provider Practices & Education (Preschoolers)
55. During screen time activities with preschool children, providers supervise and watch with the children:
Rarely or never Some of the time Most of the time All of the time
56. Providers are offered training opportunities on screen time reduction and/or media literacy for preschool children:
Rarely or never Less than 1 time per year 1 time per year 2 or more times per year
57. Parents of preschool children are offered screen time reduction and/or media literacy education (e.g., special programs, newsletters, or information sheets):
Rarely or never Less than 1 time per year 1 time per year 2 or more times per year
Section 3. Physical Activity/Screen Time for Toddlers
58. The next set of questions refer only to toddlers (ages 1-2). Does your program provide care for toddlers?
Yes No (SKIP TO QUESTION 69)
Physical Activity: Time Provided (Toddlers)
59. Active play time (indoor and outdoor) is provided to all toddlers, including children with special needs:
15-30
minutes per day 31-45
minutes each day 46-60
minutes each day 61-90
minutes each day
60. Outdoor active play time is provided to all toddlers, including children with special needs:
1 time a day for 30
minutes or less 1 or more times a day for a
total of 30-45 minutes 1 or more times a day for a
total of 45-60 minutes 2 or more times each day
for a total of 60 minutes or more
Physical Activity: Environment & Provider Practices (Toddlers)
61. For toddlers, including those with special needs, indoor and outdoor play spaces consist of:
Space only suitable for
quiet play Space is available, but allows for only limited
types of activities
Areas separate from preschoolers that provides space for exploration and
skill building
Areas separate from preschoolers with space available for all types of
activities
62. For toddlers, portable play equipment (e.g., wheeled toys, balls, hoops, ribbons) are age-appropriate and consist of:
Limited variety and
children must take turns Some variety but children
must take turns Good variety both indoors and outdoors but children
must take turns
Lots of variety both indoors and outdoors for
children to use at the same time

63. During toddlers’ active play time, staff:
Supervise play only (mostly sit or stand)
Sometimes encourage children to be active
Sometimes encourage children to be active and
join children in active play
Often encourage children to be active and join
children in active play
Physical Activity: Education (Toddlers)
64. Training opportunities in physical activity for toddlers (not including playground safety) are offered to providers:
Rarely or never Less than 1 time per year 1 time per year 2 or more times per year
65. Parents of toddlers are offered physical activity education (e.g., special programs, newsletters, information sheets):
Rarely or never Less than 1 time per year 1 time per year 2 or more times per year
Screen Time: Availability & Education (Toddlers)
66. Toddlers are allowed to watch television/videos:
1 or more times each day 2-4 times per week 1 time per week or less Never Not applicable, my
program does not have a television, nor do we view
shows/videos using the internet
67. Training opportunities on screen time reduction and/or media literacy for toddlers are offered to providers:
Rarely or never Less than 1 time per year 1 time per year 2 or more times per year
68. Parents of toddlers are offered screen time reduction and/or media literacy (e.g., special programs, newsletters, or information sheets):
Rarely or never Less than 1 time per year 1 time per year 2 or more times per year
Section 4. Breastfeeding
69. The next set of questions refer to infants and breastfeeding. Does your program provide care for infants (birth-1 year) OR any older breastfed children?
Yes No (SKIP TO QUESTION 95)
Breastfeeding: Environment
70. A designated area for mothers to breastfeed their infants, other than a bathroom, is:
Not available Only available upon
request Always available, has
appropriate seating, but lacks either privacy or an
electrical outlet
Always available, has appropriate seating,
provides complete privacy, and has an electrical outlet

71. Culturally appropriate breastfeeding support materials (e.g., pictures, posters, brochures, pamphlets), not including those produced or supplied by commercial entities and/or manufacturers of infant formula, are:
Not displayed Displayed, but are limited Displayed and include
multiple types of materials Displayed in several areas of the facility and include
pictures, posters, brochures, pamphlets, and
other resources
72. For breastfeeding mothers needing to store expressed milk, the facility provides:
No refrigerator or freezer
space Limited refrigerator and
freezer space, but it is not consistently available
Sufficient refrigerator and freezer space that is
available most of the time
Sufficient refrigerator and freezer space that is
always available
73. Learning and play materials for children which normalize breastfeeding (e.g., books that contain pictures of breastfeeding, baby dolls that are nursing), include:
No toys and books
portraying breastfeeding are available
A few toys and books portraying breastfeeding
Toys and books portraying breastfeeding in most
classrooms
Toys and books portraying breastfeeding in all
classrooms
74. A feeding plan filled out by a parent/guardian and/or healthcare provider is:
Not used by my program Posted Posted, but not updated
regularly Posted and updated
regularly Posted, regularly updated,
and is used to provide a daily report to parents
75. As part of the feeding plan, support for breastfeeding is:
Not explicitly included Sometimes included, but
relies on the provider to add additional information
to standard form
Usually included, and part of the standard form to be
filled in by parents
Always included, and covers age-appropriate
introduction of solid food, feeding in response to
baby’s cues, and inviting the mother to come to the
facility to nurse
Not applicable, my program does not use feeding plans for our
children
Breastfeeding: Education
76. Training on age-appropriate infant feeding practices, including safe storage/handling of human milk, is offered to providers:
Rarely or never Only as part of new staff
orientation 1 time per year 2 or more times per year
77. Training on promoting and supporting breastfeeding, including exclusive breastfeeding, is offered to providers:
Rarely or never Only as a part of new staff
orientation
1 time per year 2 or more times per year
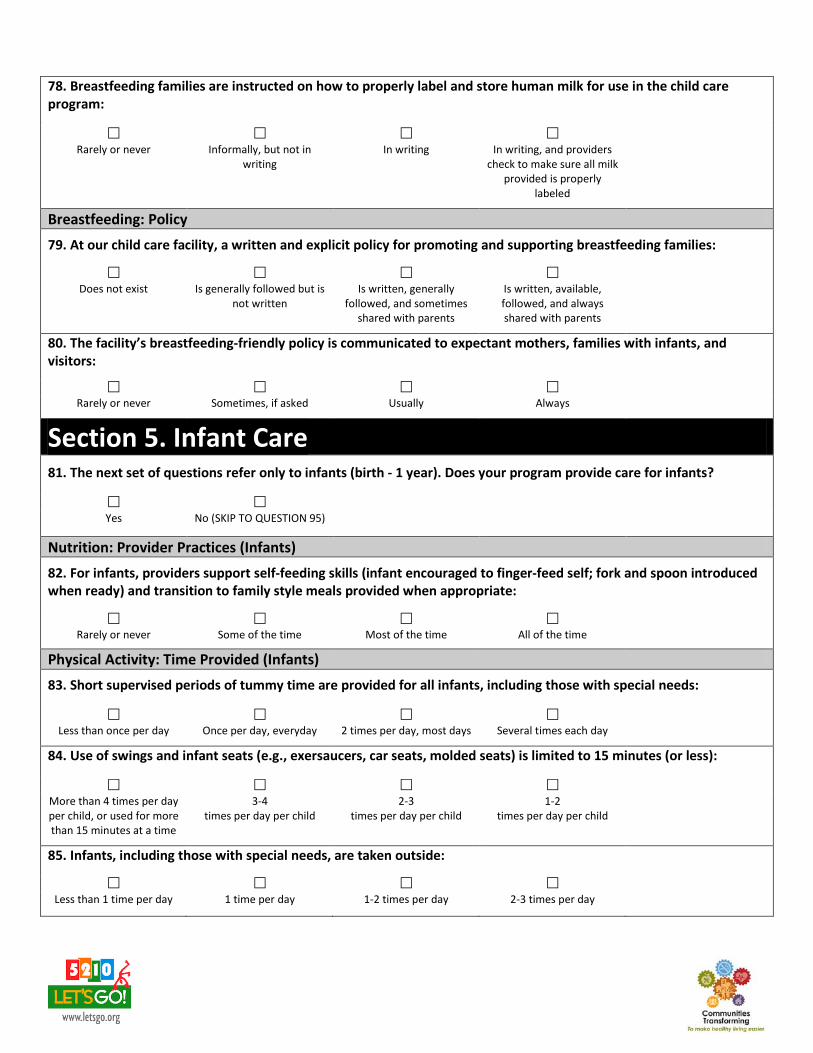
78. Breastfeeding families are instructed on how to properly label and store human milk for use in the child care program:
Rarely or never Informally, but not in
writing In writing In writing, and providers
check to make sure all milk provided is properly
labeled
Breastfeeding: Policy
79. At our child care facility, a written and explicit policy for promoting and supporting breastfeeding families:
Does not exist Is generally followed but is
not written Is written, generally
followed, and sometimes shared with parents
Is written, available, followed, and always shared with parents
80. The facility’s breastfeeding-friendly policy is communicated to expectant mothers, families with infants, and visitors:
Rarely or never Sometimes, if asked Usually Always
Section 5. Infant Care
81. The next set of questions refer only to infants (birth - 1 year). Does your program provide care for infants?
Yes No (SKIP TO QUESTION 95)
Nutrition: Provider Practices (Infants)
82. For infants, providers support self-feeding skills (infant encouraged to finger-feed self; fork and spoon introduced when ready) and transition to family style meals provided when appropriate:
Rarely or never Some of the time Most of the time All of the time
Physical Activity: Time Provided (Infants)
83. Short supervised periods of tummy time are provided for all infants, including those with special needs:
Less than once per day Once per day, everyday 2 times per day, most days Several times each day
84. Use of swings and infant seats (e.g., exersaucers, car seats, molded seats) is limited to 15 minutes (or less):
More than 4 times per day per child, or used for more than 15 minutes at a time
3-4 times per day per child
2-3 times per day per child
1-2 times per day per child
85. Infants, including those with special needs, are taken outside:
Less than 1 time per day 1 time per day 1-2 times per day 2-3 times per day
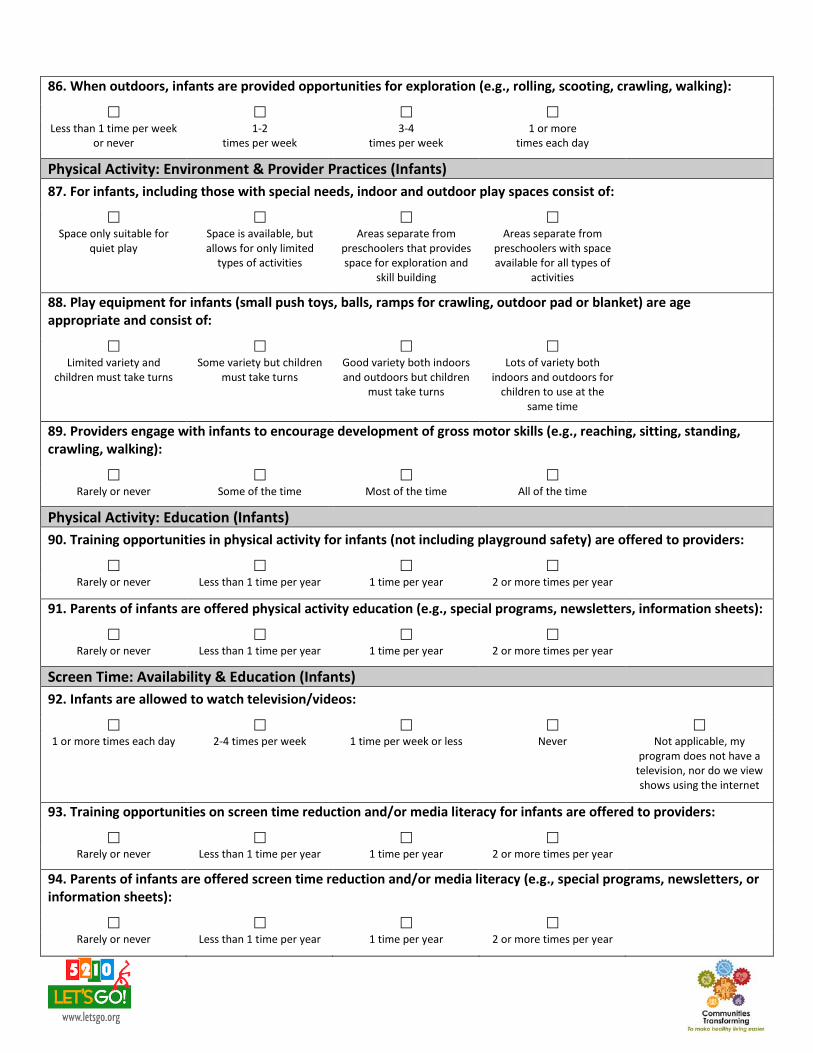
86. When outdoors, infants are provided opportunities for exploration (e.g., rolling, scooting, crawling, walking):
Less than 1 time per week
or never
1-2 times per week
3-4 times per week
1 or more times each day
Physical Activity: Environment & Provider Practices (Infants)
87. For infants, including those with special needs, indoor and outdoor play spaces consist of:
Space only suitable for
quiet play Space is available, but allows for only limited
types of activities
Areas separate from preschoolers that provides space for exploration and
skill building
Areas separate from preschoolers with space available for all types of
activities
88. Play equipment for infants (small push toys, balls, ramps for crawling, outdoor pad or blanket) are age appropriate and consist of:
Limited variety and
children must take turns Some variety but children
must take turns Good variety both indoors and outdoors but children
must take turns
Lots of variety both indoors and outdoors for
children to use at the same time
89. Providers engage with infants to encourage development of gross motor skills (e.g., reaching, sitting, standing, crawling, walking):
Rarely or never Some of the time Most of the time All of the time
Physical Activity: Education (Infants)
90. Training opportunities in physical activity for infants (not including playground safety) are offered to providers:
Rarely or never Less than 1 time per year 1 time per year 2 or more times per year
91. Parents of infants are offered physical activity education (e.g., special programs, newsletters, information sheets):
Rarely or never Less than 1 time per year 1 time per year 2 or more times per year
Screen Time: Availability & Education (Infants)
92. Infants are allowed to watch television/videos:
1 or more times each day 2-4 times per week 1 time per week or less Never Not applicable, my
program does not have a television, nor do we view shows using the internet
93. Training opportunities on screen time reduction and/or media literacy for infants are offered to providers:
Rarely or never Less than 1 time per year 1 time per year 2 or more times per year
94. Parents of infants are offered screen time reduction and/or media literacy (e.g., special programs, newsletters, or information sheets):
Rarely or never Less than 1 time per year 1 time per year 2 or more times per year

Section 6. Supportive Strategies
95. Within the past year, did your program participate in any local, state or national initiatives that support healthy eating/active living (other than 5-2-1-0 Goes to Child Care)?
No Not yet, we’re still in
the planning stage Yes, in some or a few classrooms (less than
50%)
Yes, in most classrooms (at least
50%)
Yes, program-wide (100%)
Yes, program-wide before this year and we continued it this
year
96. Within the past year, did your program engage community organizations (e.g., farms, grocery stores, food banks, local doctors' offices) to help support healthy eating/active living at your program?
No Not yet, we’re still in
the planning stage Yes, in some or a few classrooms (less than
50%)
Yes, in most classrooms (at least
50%)
Yes, program-wide (100%)
Yes, program-wide before this year and we continued it this
year
97. Has your program implemented a staff wellness program that includes healthy eating and active living?
No No, but we have started to
work on it Yes, we implemented it
this year Yes, we implemented it before this year and we
continued it this year
Not applicable, I am the only staff member
Section 7. Program Policies
Please refer to your program's policies for these last several questions. **You may need to connect with your director to answer this section.** Let's Go! will audit a sample of responses to verify them, and will also reach out to you to ask you to submit copies of your policies to Let's Go!.
The following words INDICATE A POLICY IS NOT REQUIRED: encourage, may, can, could, should, might, suggest, will strive to, will work to, try
The following words INDICATE A POLICY IS REQUIRED: shall, will, must, have to, insist, require, comply, enforce
Policy: Nutrition
98. Our policies require that snacks provided to children by our program (not sent in from home) must be healthy.
False, this is not required by our
policies True, this is required by our policies but it is not usually
enforced in our program
True, this is required by our policies and is usually enforced in our program, and our director has
verified this
Not applicable, my program does not provide any snacks
99. Our policies require that celebration foods, whether brought in from home or supplied by our program, must be healthy.
False, this is not required by our
policies True, this is required by our policies but it is not usually
enforced in our program
True, this is required by our policies and is usually enforced in our program, and our director has
verified this
Not applicable, my program practices only non-food
celebrations

100. Our policies prohibit using food as a reward.
False, this is not required by our
policies True, this is required by our policies but it is not usually
enforced in our program
True, this is required by our policies and is usually enforced in our program, and our director has
verified this
101. Our policies require that the availability of sugary beverages (including juice) is limited.
False, this is not required by our
policies True, this is required by our policies but it is not usually
enforced in our program
True, this is required by our policies and is usually enforced in our program, and our director has
verified this
Policy: Physical Activity & Screen Time
102. Our policies require that all children have opportunities for physical activity every day.
False, this is not required by our
policies True, this is required by our policies but it is not usually
enforced in our program
True, this is required by our policies and is usually enforced in our program, and our director has
verified this
103. Our policies require that recreational screen time (includes television, computer and DVDs) for all children is limited.
False, this is not required by our
policies True, this is required by our policies but it is not usually
enforced in our program
True, this is required by our policies and is usually enforced in our program, and our director has
verified this
Final Comments
104. Is there any other information about your work with CTG or Let's Go! this year that you would like to share?
Thank you very much for completing this survey! Your answers will help us understand what changes have occurred and will help us improve CTG and the Let's Go! programs. You will have an opportunity to review your completed survey with your CTG district coordinator or 5-2-1-0 Goes to Child Care representative.

04/12 R10/13
What is Action Planning?
Action planning begins after completion of the self-assessment. This is when the child care provider sets S.M.A.R.T. goals (Specific, Measurable, Attainable, Relevant, Time-Bound) around key areas for improvement. Providers then brainstorm action steps and resources needed to meet these goals. There is an Action Planning Document designed to help in this process. Completion of this program step makes the provider eligible for licensing contact hours. Note: It is estimated this step will take 1 to 2 hours to complete. However, provide a certificate for the actual length of time spent on this step which may be more or less than this estimate. Tools to have on hand for the Action Planning meeting:
1) A copy of the site’s completed self-assessment to guide the discussion. 2) Two blank copies of the Action Planning Document. 3) A copy of the 5-2-1-0 Goes to Child Care Provider Toolkit. 4) The NAP SACC Representative Technical Assistance Manual, if desired (electronic
copy available on your flash drive).
Working with the Provider
Once the provider has completed their self-assessment, it is time to review it, looking for areas of potential improvement. This is also your opportunity to get to know a provider and their child care program. Discussing a site’s self-assessment with them will help you learn about the history and interests of the program and give you insight as to where they hope 5-2-1-0 GTCC will help them go. It is best to set aside 1 to 2 hours for this meeting. Thoroughly review answers to the self-assessment and discuss possible areas/questions the provider could set goals around. Ask providers what they are interested in improving. Some will have very clear ideas, while others will need more guidance from you. Illicit suggestions and ideas from the provider but encourage him/her to choose 2-3 topic areas or questions to set goals around. We suggest choosing at least 1 nutrition and 1 physical activity or screen time-related area. Use the action planning document to help guide the provider in thinking through their goals so they are S.M.A.R.T. This will break potentially large goals into small, attainable steps and ensure there is a timeline for completion. Sites will be required to complete a post-assessment again in May to measure improvement.
Step Three: Action Planning
Adapted from the NAP SACC Program, Center for Health Promotion and Disease Prevention, The University of North Carolina, Chapel Hill, NC, May 2007.
04/12 R10/13
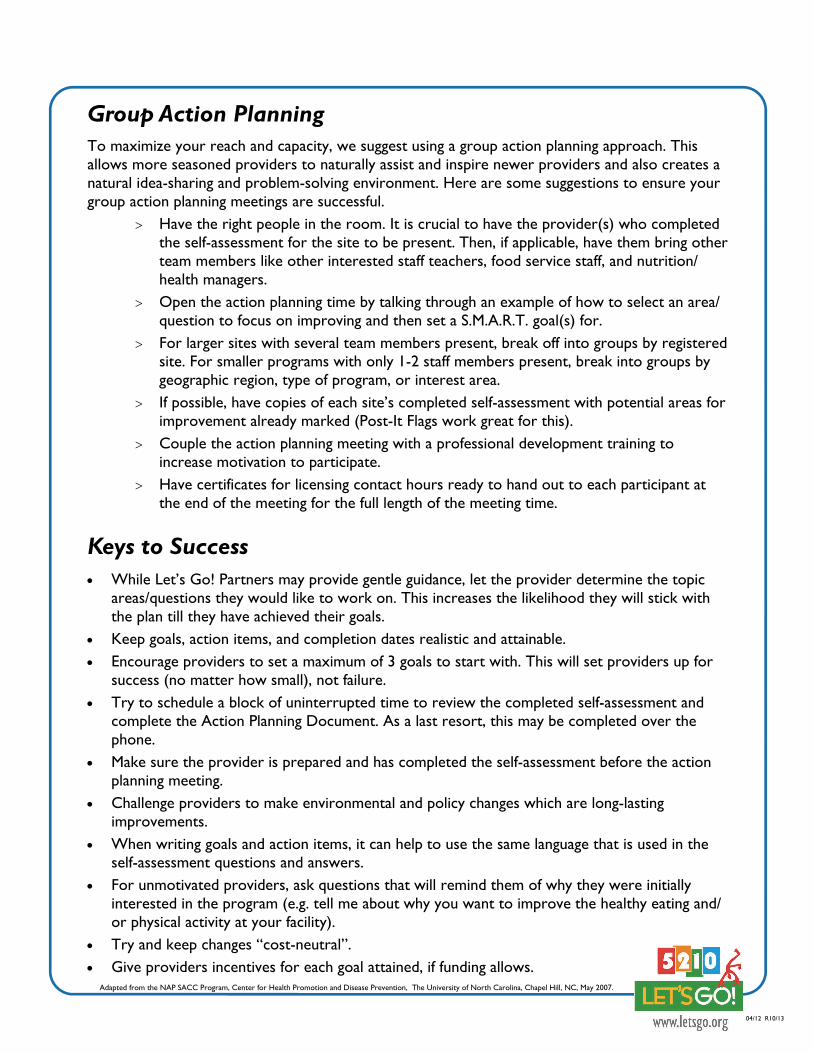
Group Action Planning To maximize your reach and capacity, we suggest using a group action planning approach. This allows more seasoned providers to naturally assist and inspire newer providers and also creates a natural idea-sharing and problem-solving environment. Here are some suggestions to ensure your group action planning meetings are successful.
Have the right people in the room. It is crucial to have the provider(s) who completed the self-assessment for the site to be present. Then, if applicable, have them bring other team members like other interested staff teachers, food service staff, and nutrition/health managers.
Open the action planning time by talking through an example of how to select an area/question to focus on improving and then set a S.M.A.R.T. goal(s) for.
For larger sites with several team members present, break off into groups by registered site. For smaller programs with only 1-2 staff members present, break into groups by geographic region, type of program, or interest area.
If possible, have copies of each site’s completed self-assessment with potential areas for improvement already marked (Post-It Flags work great for this).
Couple the action planning meeting with a professional development training to increase motivation to participate.
Have certificates for licensing contact hours ready to hand out to each participant at the end of the meeting for the full length of the meeting time.
Keys to Success
While Let’s Go! Partners may provide gentle guidance, let the provider determine the topic areas/questions they would like to work on. This increases the likelihood they will stick with the plan till they have achieved their goals.
Keep goals, action items, and completion dates realistic and attainable. Encourage providers to set a maximum of 3 goals to start with. This will set providers up for
success (no matter how small), not failure. Try to schedule a block of uninterrupted time to review the completed self-assessment and
complete the Action Planning Document. As a last resort, this may be completed over the phone.
Make sure the provider is prepared and has completed the self-assessment before the action planning meeting.
Challenge providers to make environmental and policy changes which are long-lasting improvements.
When writing goals and action items, it can help to use the same language that is used in the self-assessment questions and answers.
For unmotivated providers, ask questions that will remind them of why they were initially interested in the program (e.g. tell me about why you want to improve the healthy eating and/or physical activity at your facility).
Try and keep changes “cost-neutral”. Give providers incentives for each goal attained, if funding allows.
Adapted from the NAP SACC Program, Center for Health Promotion and Disease Prevention, The University of North Carolina, Chapel Hill, NC, May 2007.
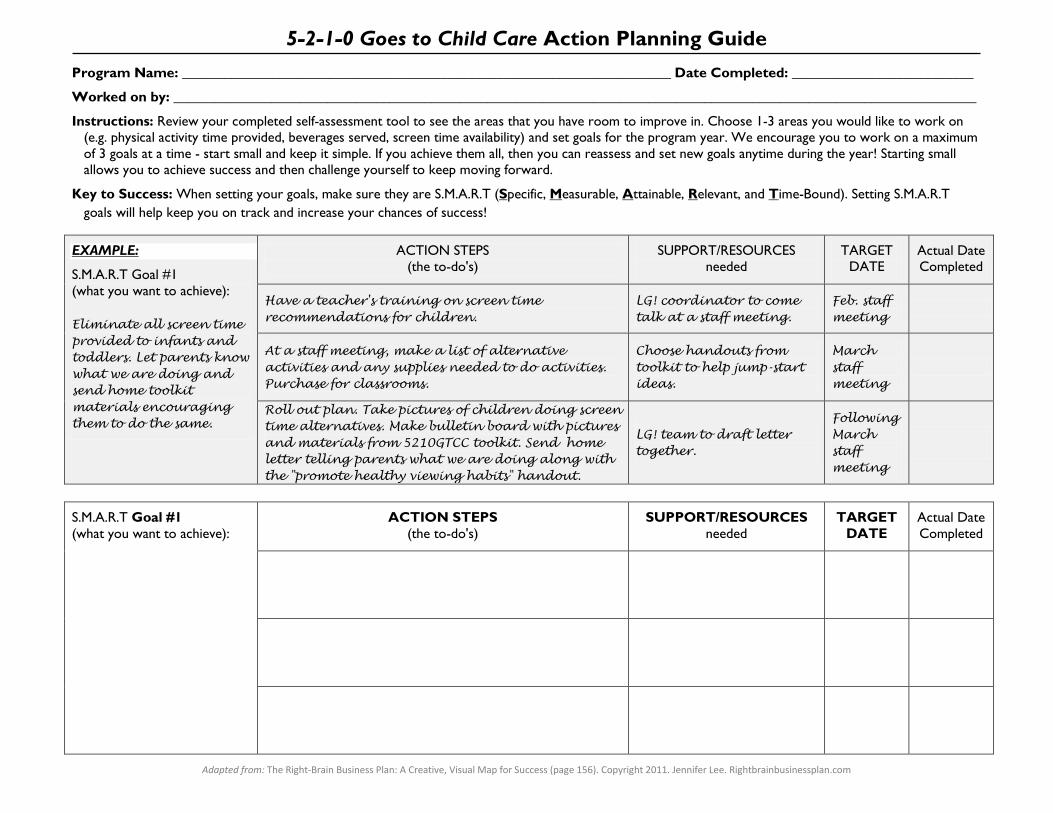
Adapted from: The Right-Brain Business Plan: A Creative, Visual Map for Success (page 156). Copyright 2011. Jennifer Lee. Rightbrainbusinessplan.com
5-2-1-0 Goes to Child Care Action Planning Guide Program Name: ______________________________________________________________________ Date Completed: __________________________
Worked on by: ___________________________________________________________________________________________________________________
Instructions: Review your completed self-assessment tool to see the areas that you have room to improve in. Choose 1-3 areas you would like to work on (e.g. physical activity time provided, beverages served, screen time availability) and set goals for the program year. We encourage you to work on a maximum of 3 goals at a time - start small and keep it simple. If you achieve them all, then you can reassess and set new goals anytime during the year! Starting small allows you to achieve success and then challenge yourself to keep moving forward.
Key to Success: When setting your goals, make sure they are S.M.A.R.T (Specific, Measurable, Attainable, Relevant, and Time-Bound). Setting S.M.A.R.T goals will help keep you on track and increase your chances of success!
EXAMPLE:
S.M.A.R.T Goal #1 (what you want to achieve):
Eliminate all screen time provided to infants and toddlers. Let parents know what we are doing and send home toolkit materials encouraging them to do the same.
ACTION STEPS (the to-do's)
SUPPORT/RESOURCES needed
TARGET DATE
Actual Date Completed
Have a teacher's training on screen time recommendations for children.
LG! coordinator to come talk at a staff meeting.
Feb. staff meeting
At a staff meeting, make a list of alternative activities and any supplies needed to do activities. Purchase for classrooms.
Choose handouts from toolkit to help jump-start ideas.
March staff meeting
Roll out plan. Take pictures of children doing screen time alternatives. Make bulletin board with pictures and materials from 5210GTCC toolkit. Send home letter telling parents what we are doing along with the "promote healthy viewing habits" handout.
LG! team to draft letter together.
Following March staff meeting
S.M.A.R.T Goal #1 (what you want to achieve):
ACTION STEPS (the to-do's)
SUPPORT/RESOURCES needed
TARGET DATE
Actual Date Completed

Adapted from: The Right-Brain Business Plan: A Creative, Visual Map for Success (page 156). Copyright 2011. Jennifer Lee. Rightbrainbusinessplan.com
S.M.A.R.T Goal #2 (what you want to achieve):
ACTION STEPS (the to-do's)
SUPPORT/RESOURCES needed
TARGET DATE
Actual Date Completed
S.M.A.R.T Goal #3 (what you want to achieve):
ACTION STEPS (the to-do's)
SUPPORT/RESOURCES needed
TARGET DATE
Actual Date Completed
Additional Notes:

04/12 R11/13
What are the Workshops and Trainings?
Providers and their staff should be completing workshops and other professional development trainings related to physical activity and nutrition (PAN) every year. 5-2-1-0 GTCC has 5 staff workshops available to help fill this requirement on the following topics: Childhood Obesity, Nutrition for Young Children, Physical Activity for Young Children, Personal Health and Wellness for Staff, and Working with Families to Promote Healthy Weight Behaviors. A brief description of each has been provided (Figure 4). Participating in PAN-related professional development will inform staff about healthy nutrition and physical activity environments and practices and why they are so important. Additionally, center directors and program owners, who typically are facilitating most of the improvements, can use trainings to increase staff buy-in to be healthy role models and also advocates for healthy home environments for the children in their care. Providers are eligible for licensing contact hours upon completion of each workshop. Note: It is estimated that each workshop will take about 1 hour to present. However, provide a certificate for the actual length of time of participation which may be more or less than this estimate.
Working with the Provider
The 5-2-1-0 GTCC workshops are designed to be delivered in a number of ways. PowerPoint presentations with scripted facilitator notes are provided in this toolkit and online. This allows for presentation to a large group in a “lecture-like” format, presentation to small groups, or one-on-one in a discussion format. Additionally, the workshops can be presented all together in one longer workshop, or separately, with each workshop lasting anywhere between 30 and 60 minutes. The workshops can be presented in any order, but it is helpful to deliver the Childhood Obesity workshop first. This provides the background to staff as to why healthy eating and physical activity during the child care day are so important.
To assist with the delivery of the workshops, there is a recorded version of each one in a web-based format available at www.letsgo.org. While it is best for providers and staff to complete the workshops at a live training so that they may ask questions and engage in discussion, there are many reasons why providers may be unable to reasonably do so. Partners may direct these sites to the online webinars. Staff will be able to watch the webinars when it is convenient for them, complete a short post-test and print off a certificate of completion for licensing contact hours.
Step Four: Workshops and Trainings
Adapted from the NAP SACC Program, Center for Health Promotion and Disease Prevention, The University of North Carolina, Chapel Hill, NC, May 2007.

04/12 R08/13/12
Keys to Success
Particularly if you have not worked with a program before, check in with the owner/director for input on how they think the staff workshops could best be delivered.
Consider your audience and the facility before presenting the workshops. Is the space conducive to PowerPoint or would it be better to hold a round table discussion? Are the staff quiet or more highly engaged?
Use icebreakers to start off the workshop series. This will get the group laughing and break tension. This may make the group more comfortable and willing to participate.
Child care staff love door prizes! If you have small items such as recipe books, pedometers, or coupons, or the ability to purchase some, use them as a way to encourage participation.
Be flexible with the facility as much as possible. While presenting the workshops to the staff during naptime might be ideal for some, for others it is impossible without additional staff to take over child care responsibilities. Because of this, child care programs often prefer holiday, evening or weekend workshops so all staff can attend. Head start programs can often capture all staff during a mandatory staff meeting.
Try planning group workshop sessions open to all the providers you work with in a regional area. You may want to provide 2 or more of the workshops at one time. Check with any child care center’s you work with to see if they have a large space they are willing to allow you to use for a group training.
When using a group training approach, consider planning a handful of sessions on different dates and times to give providers a choice sessions to register for.
Work with other Let’s Go! Partners in your area to coordinate and offer a day-long training day to all providers in each of your regions. Try offering all 5 workshops and/or bringing in other trainers on additional topics related to physical activity and nutrition to expand the offerings.
For sites that complete the online versions of workshops, follow-up with a phone call to the owner/director to discuss how the workshop(s) went and highlight major take-away points, especially as they apply to the site’s Action Plan for the year.
Adapted from the NAP SACC Program, Center for Health Promotion and Disease Prevention, The University of North Carolina, Chapel Hill, NC, May 2007.

04/12 R11/13
Figure 4. List of 5-2-1-0 GTCC Workshops
Workshop
Description
Supersizing our Children: Childhood Obesity
Introduces the problem of obesity in children birth to age 5 and the consequences of being overweight/ obese. Also, describes the role of child care staff in helping to prevent this problem.
Eat Right, Grow Strong: Nutrition for Young Children
Overviews not only what should be offered to children, but how and why those foods should be offered. Also, describes the role of child care staff in helping shape children’s eat-ing behaviors.
Moving Children to Good Health: Physical Activity for Young Children
Discusses the importance of physical activity for young children in child care settings and how activity can be integrated into all parts of a preschool day.
Stepping Toward a Healthy Lifestyle: Personal Health and Wellness
Provides information to staff about their own healthy eating and physical activity behaviors, touching specifically upon mindful eating techniques. It describes barriers to making these important lifestyle changes and provides an opportunity to brainstorm some solutions to these problems.
Growing Healthy Kids Together: Working with Families to Promote Healthy Weight Behaviors
Describes how child care providers can communicate healthy weight behavior messages to parents so that children are receiving the same messages at home as they are during their time in the child care setting. It also provides strategies to best communicate these messages.
Adapted from the NAP SACC Program, Center for Health Promotion and Disease Prevention, The University of North Carolina, Chapel Hill, NC, May 2007.


Adapted from the NAP SACC Program, Center for Health Promotion and Disease Prevention, The University of North Carolina, Chapel Hill, NC, 2007.
5-2-1-0 Goes to Child Care Workshop Evaluation
Name of Presenter ______________________________
Your Name____________________________________
Your Job Title___________________________________
1. The workshop learning objectives were clear to me.
strongly agree agree disagree strongly disagree
2. The content of the workshop was related to the learning objectives.
strongly agree agree disagree strongly disagree
3. The topic was important or relevant to me.
strongly agree agree disagree strongly disagree
4. The workshop was well-organized.
strongly agree agree disagree strongly disagree
5. The presenter effectively taught the workshop.
strongly agree agree disagree strongly disagree
6. The training I received will be useful to me in my work environment.
strongly agree agree disagree strongly disagree
7. The training I received will be useful to me on a personal level.
strongly agree agree disagree strongly disagree
8. The topic presented was interesting to me.
strongly agree agree disagree strongly disagree
9. The presenter used handouts that were helpful during the workshop.
strongly agree agree disagree strongly disagree none used
10. The presenter used visual aids that were helpful during the workshop.
strongly agree agree disagree strongly disagree none used
11. Would you be interested in a follow-up session on this topic?
yes no
11a. If yes, what areas would you like to learn more about?
12. Comments/Suggestions:
Thank you for taking time to complete this evaluation.


What is Technical Assistance?
Let’s Go! Partners provide ongoing technical assistance to facilities in support of their chosen improvements. This step of the program tends to be the most overlooked and may be the most important. Providers need technical assistance, not only as a reminder to work on their goals, but for additional knowledge and support in achieving these goals.
Working with the Provider
Partners are responsible for completing at least two personal check-ins with sites per program year (at least one in-person and a second that may be in-person, via email or by phone. In-person check-ins may be 1x1 or in a group setting. Action Planning visits DO count as a check-in). Note: to be considered a check-in, a site must be engaged in back and forth communication with you. You will be able to gauge the level of technical assistance a site may need beyond these two check-ins based on the completed self-assessment and action plan. If a site needs more support, it may be important to set up regular contact through phone calls, emails and/or site visits. Partners know their providers and can best determine how often they should check in. Let’s Go! will send a minimum of five highlight emails each program year and will coordinate yearly mini-grant opportunities (if funding is available). Note: Let’s Go! will also facilitate regular technical assistance calls for Partners.
Keys to Success
For in-person meetings, schedule meetings in advance and send reminders close to the day. To save time, schedule a quick follow-up phone call or meeting prior to or after delivering a workshop.
Be flexible. If a director says they just do not have the time to devote to the project, encourage them to focus on just 1 or 2 small goals of their action plan, or to even just maintain what they have done to date and be willing to revisit their action plan with you again later in the year.
Use the 5-2-1-0 GTCC Provider Toolkit to provide resources and help. Use incentives to help providers move through their action items to reach proposed goals when funding allows.
Encourage and support providers. It is important to keep them motivated and encouraged throughout the process.
Discuss the barriers the providers may need to overcome in order to meet his/her goals, or revise the goals to make them more simple and attainable.
Participate in the technical assistance calls for partners. These calls will provide an opportunity to strategize with other partners around challenges you may be facing implementing the program.
Step Five: Technical Assistance
04/12 R11/13
Adapted from the NAP SACC Program, Center for Health Promotion and Disease Prevention, The University of North Carolina, Chapel Hill, NC, May 2007.


Adapted from the NAP SACC Program, Center for Health Promotion and Disease Prevention, The University of North Carolina, Chapel Hill, NC, November 2007.
1
Program Name: ______________________________________________________________________ Champion Name/Contact Info: ________________________________________________________
1. Initial Self-Assessment Completed
Date Distributed: ___________
Date Returned: ____________
2. Action Plan Developed
Date Completed: ___________ attach a copy to monitoring guide
3. Date Workshops Completed:
Childhood Obesity: ___________________________________
Healthy Eating: ______________________________________
Physical Activity: _____________________________________
Personal Health: _____________________________________
Working with Families: ________________________________
Other PAN-related trainings completed:________________________________________________ ____________________________________________________________________________________________________________________________________________________________
4. Technical Assistance Follow-up:
1. Date Completed: ______________________
In-Person
Telephone 2. Date Completed: ______________________
In-Person
Telephone
5-2-1-0 Goes to Child Care Monitoring Guide
Adapted from the NAP SACC Program, Center for Health Promotion and Disease Prevention, The University of North Carolina, Chapel Hill, NC, November 2007.
2
3. Date Completed: ______________________
In-Person
Telephone 4. Date Completed: ______________________
In-Person
Telephone 5. Date Completed: ______________________
In-Person
Telephone 6. Date Completed: ______________________
In-Person
Telephone 5. End-of-year Evaluation Date Completed: _________
Interested in continuing? _________ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ Notes and General Comments:

What is Evaluate, Revise, and Repeat?
This program step provides a much needed opportunity for providers to celebrate accomplishments, reflect upon barriers, and think about how to move forward. Providers do not have to accomplish everything in their first effort. Let’s Go!’s goal is to take child care programs from where they are to where they want to be. The idea is to see continual change over time, even if changes are small, and repeat the process when necessary. We would love to see facilities achieve all 10 Strategies, meet all the best practice guidelines, and reach Gold recognition status. However, this may not be realistic for some programs. Providers may repeat steps 2-6 as many times as they would like over the course of a program year; yet, Let’s Go! only collects a completed self-assessment at the end of each program year. When sites complete their year-end assessment, they are eligible for recognition and also are completing their baseline assessment for the next program year.
Working with the Provider
Every May at the end of the program year, an electronic version of the self-assessment will be emailed to all registered sites as their end-of-year evaluation with directions for how to complete it. When providers complete the assessment, it is automatically submitted to the home office. Let’s Go! partners should follow-up with each of their registered sites to remind them to complete the year-end self-assessment. For programs who elect to re-register, their post-assessment will serve as the next year’s pre-assessment.
* Please refer to your Let’s Go! Early Childhood Evaluation Plan to see exactly which self-assessment questions will be measured to determine a program’s level of implementation and recognition.
Keys to Success
Celebrate all accomplishments, no matter how small, and assure providers that they can revisit goals when they have more time to devote to the program.
Don’t force additional improvements upon a provider or facility. They may not want to continue at this time, but may regain interest. Keep in contact with providers to gauge future interest. To assist in this, anyone who has been involved with Let’s Go! will continue to receive the early childhood highlight emails regardless of registration status unless they opt out.
Encourage your site champions to read all questions and answers closely and take extra care when completing their year-end evaluation. The results of this assessment will determine their recognition level for the year.
Step Six: Evaluate, Revise, and Repeat
04/12 R11/3
Adapted from the NAP SACC Program, Center for Health Promotion and Disease Prevention, The University of North Carolina, Chapel Hill, NC, May 2007.


Recognition Program for Let’s Go! Schools, After School Programs and Child Care Programs
We are excited to announce a new Let's Go! recognition program for schools, after school programs and child care programs. This has been created as a way to acknowledge all the hard work that is happening out there! Beginning this spring, we will recognize three levels of accomplishment, described below. While we hope lots of schools and after school and child care programs will be energized by this program, we know that achieving recognition, especially at the higher levels, will take time. We are here to help! It is our goal to provide the tools and support needed to help schools and after school and child care programs sustain the great work they are doing and be recognized for it! Bronze Level Any school or program that implements all 5 Let’s Go! priority strategies. Silver Level Any school or program that:
implements all 5 Let’s Go! priority strategies; requires at least 1 and up to 4 of the priority strategies in written policy; and enforces the written policy.*
Gold Level Any school or program that:
requires all 5 Let’s Go! priority strategies in written policy, and enforces the written policy.*
We will use the surveys that we send out in the spring to determine which schools and programs have met the recognition criteria, and those sites will receive a certificate from Let’s Go! and will be recognized on the Let’s Go! web page. If you have any questions about the recognition program, please contact your local Let’s Go! partner or the Let’s Go! Home Office at 207.662.3734.
01/12 00/00
Five Priority Strategies 1. Provide healthy choices for snacks and celebrations; limit unhealthy
choices. 2. Provide water and low fat milk; limit or eliminate sugary beverages. 3. Provide non-food rewards. 4. Provide opportunities for children to get physical activity every day. 5. Limit recreational screen time.
*We will ask principals or directors to sign a statement verifying that the policy is enforced.

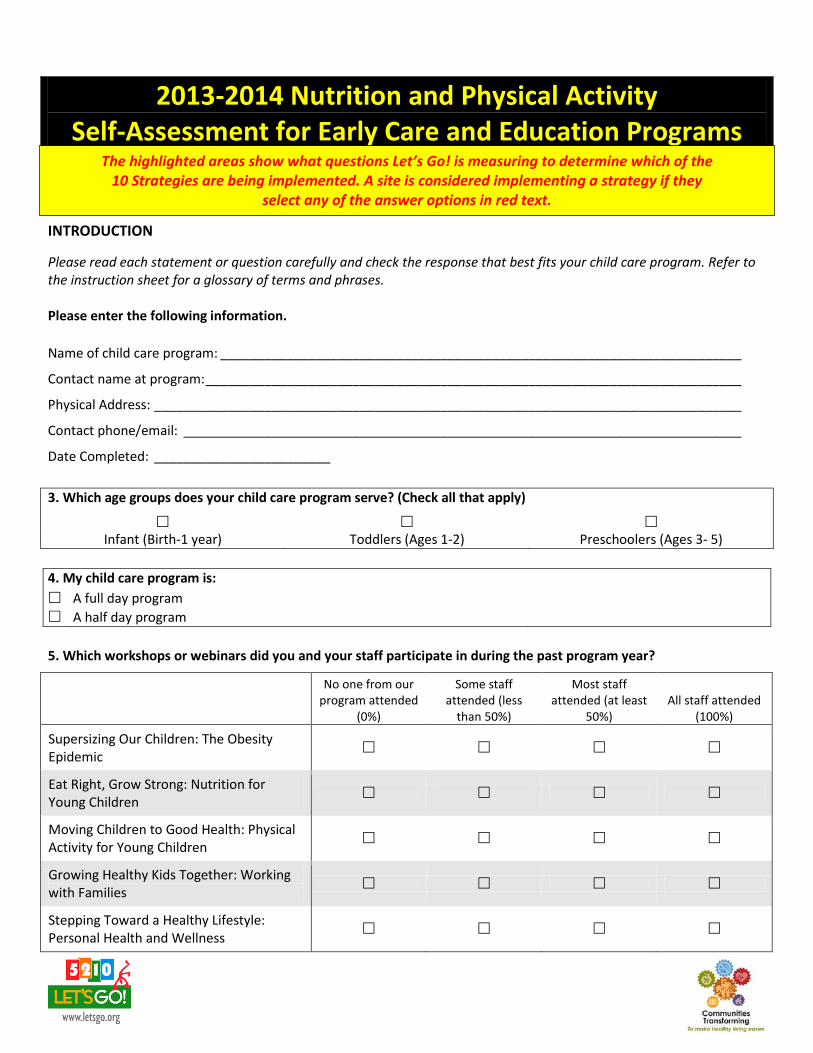
2013-2014 Nutrition and Physical Activity Self-Assessment for Early Care and Education Programs
INTRODUCTION Please read each statement or question carefully and check the response that best fits your child care program. Refer to the instruction sheet for a glossary of terms and phrases. Please enter the following information. Name of child care program: _______________________________________________________________________
Contact name at program: _________________________________________________________________________
Physical Address: ________________________________________________________________________________
Contact phone/email: ____________________________________________________________________________
Date Completed: ________________________
3. Which age groups does your child care program serve? (Check all that apply)
Infant (Birth-1 year) Toddlers (Ages 1-2) Preschoolers (Ages 3- 5)
4. My child care program is: A full day program A half day program 5. Which workshops or webinars did you and your staff participate in during the past program year?
No one from our program attended
(0%)
Some staff attended (less
than 50%)
Most staff attended (at least
50%) All staff attended
(100%)
Supersizing Our Children: The Obesity Epidemic
Eat Right, Grow Strong: Nutrition for Young Children
Moving Children to Good Health: Physical Activity for Young Children
Growing Healthy Kids Together: Working with Families
Stepping Toward a Healthy Lifestyle: Personal Health and Wellness
The highlighted areas show what questions Let’s Go! is measuring to determine which of the 10 Strategies are being implemented. A site is considered implementing a strategy if they
select any of the answer options in red text.

Section 1. Nutrition
Nutrition: Food & Beverages Served (All Children)
6. Sweets or salty foods (cookies, cakes, muffins, chips, etc.) are offered:
1 or more times per day 3‐4 times per week 1‐2 times per week Less than once a week or
never Not applicable, my program does not serve any food
7. Holidays and other special occasions are celebrated with mostly healthy foods or with non‐food treats like stickers:
Rarely or never Some of the time Most of the time All of the time
8. 100% fruit juice is offered:
In unlimited portions more
than once a day 2 or more times per day,
but limited to 4‐6 oz. each occasion
No more than 4‐6 oz. per day (OR NOT SERVED AT ALL)
No more than 4‐6 oz. per day (OR NOT SERVED AT ALL) and
parents are encouraged to support this limit
9. Sugary drinks (Kool‐Aid, fruit drinks, sports drinks, sweet tea, soda) are offered:
More than once a month Less than 1 time per
month Rarely, 1‐2
times per year Never
Nutrition: Provider Practices & Education (All Children)
10. In front of the children, providers consume the same food and drinks as children, and avoid unhealthy foods (e.g., soda, sweets, and fast food):
Rarely or never Some of the time Most of the time All of the time
11. Providers join children at the table for meals and/or snacks and talk informally about trying and enjoying healthy food:
Rarely or never Some of the time Most of the time All of the time
12. Food is used to encourage positive behavior:
All of the time Most of the time Some of the time Rarely or never
13. Training opportunities in nutrition (other than food safety and food program guidelines) are offered to providers:
Rarely or never Less than 1 time per year 1 time per year 2 times per year or more
Nutrition: Environment, Provider Practices & Education (Toddlers & Preschoolers)
14. The next set of questions refer only to toddlers and preschoolers. Does your program provide care for toddlers (ages 1‐2) and/or preschoolers (ages 3‐5)?
Yes No (SKIP TO QUESTION 69)
Strategy #2
Strategy #1
Strategy #1
Strategy #2
Strategy #3
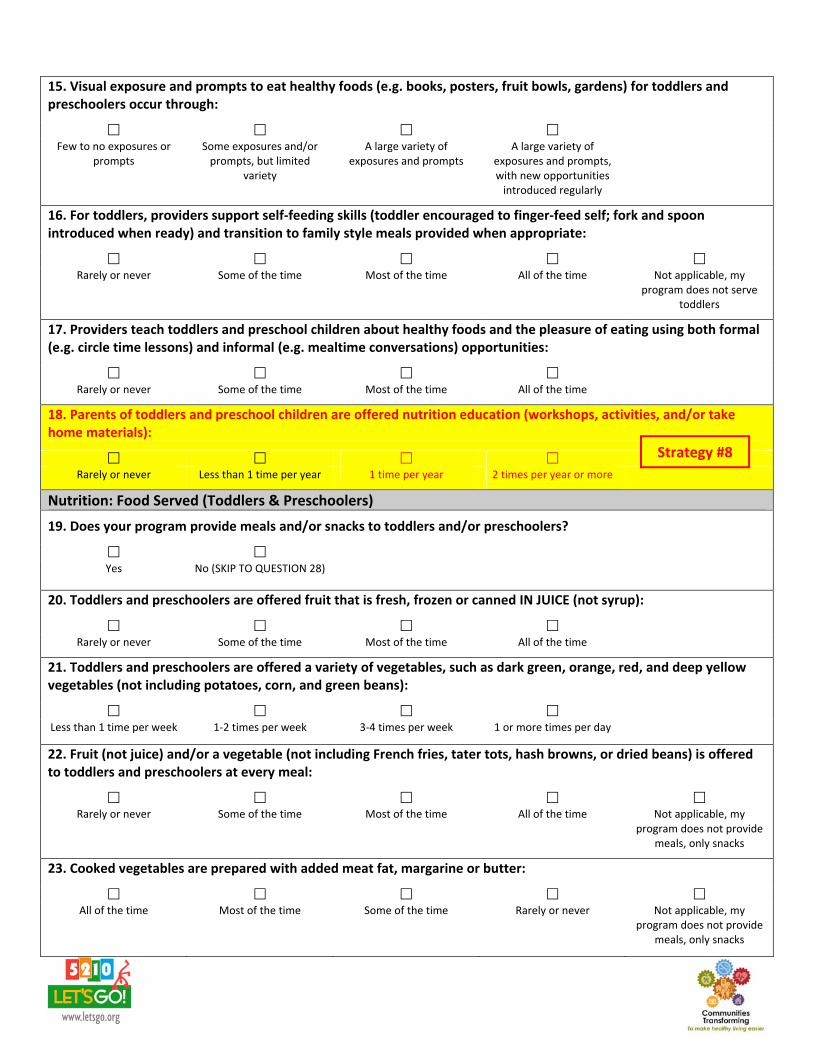
15. Visual exposure and prompts to eat healthy foods (e.g. books, posters, fruit bowls, gardens) for toddlers and preschoolers occur through:
Few to no exposures or
prompts Some exposures and/or prompts, but limited
variety
A large variety of exposures and prompts
A large variety of exposures and prompts, with new opportunities introduced regularly
16. For toddlers, providers support self‐feeding skills (toddler encouraged to finger‐feed self; fork and spoon introduced when ready) and transition to family style meals provided when appropriate:
Rarely or never Some of the time Most of the time All of the time Not applicable, my
program does not serve toddlers
17. Providers teach toddlers and preschool children about healthy foods and the pleasure of eating using both formal (e.g. circle time lessons) and informal (e.g. mealtime conversations) opportunities:
Rarely or never Some of the time Most of the time All of the time
18. Parents of toddlers and preschool children are offered nutrition education (workshops, activities, and/or take home materials):
Rarely or never Less than 1 time per year 1 time per year 2 times per year or more
Nutrition: Food Served (Toddlers & Preschoolers)
19. Does your program provide meals and/or snacks to toddlers and/or preschoolers?
Yes No (SKIP TO QUESTION 28)
20. Toddlers and preschoolers are offered fruit that is fresh, frozen or canned IN JUICE (not syrup):
Rarely or never Some of the time Most of the time All of the time
21. Toddlers and preschoolers are offered a variety of vegetables, such as dark green, orange, red, and deep yellow vegetables (not including potatoes, corn, and green beans):
Less than 1 time per week 1‐2 times per week 3‐4 times per week 1 or more times per day
22. Fruit (not juice) and/or a vegetable (not including French fries, tater tots, hash browns, or dried beans) is offered to toddlers and preschoolers at every meal:
Rarely or never Some of the time Most of the time All of the time Not applicable, my
program does not provide meals, only snacks
23. Cooked vegetables are prepared with added meat fat, margarine or butter:
All of the time Most of the time Some of the time Rarely or never Not applicable, my
program does not provide meals, only snacks
Strategy #8

24. Fried or pre‐fried potatoes (French fries, tater tots, hash browns) are offered to toddlers and preschoolers:
2 or more times per week 1 time per week Less than 1 time a week Never Not applicable, my
program does not provide meals, only snacks
25. Fried or pre‐fried (frozen and breaded) meats (chicken nuggets) or fish (fish sticks) are offered to toddlers and preschoolers:
2 or more times per week 1 time per week Less than 1 time a week Never Not applicable, my
program does not provide meals, only snacks
26. Beans or lean meats (baked or broiled chicken, turkey, or fish) are offered to toddlers and preschoolers:
Less than 1 time per week 1‐2 times per week 3‐4 times per week 1 or more times per day Not applicable, my
program does not provide meals, only snacks
27. Preschooler meals and/or snacks are served family style (children are encouraged to serve themselves with limited help):
Rarely or never Some of the time Most of the time All of the time Not applicable, my
program does not serve preschoolers
Nutrition: Beverages Served (Toddlers & Preschoolers)
28. Drinking water is available:
Upon request Upon request or during
designated water breaks Inside only, where it is
visible and freely available Inside and outside, where it is visible and available
for self‐serve
29. During indoor and outdoor play, providers prompt children to drink water:
Rarely or never Some of the time Most of the time All of the time
30. Water is offered to children over the age of 1 year (but not as a substitute for milk when it is a required food component):
Rarely or never 1 time per week or less 2‐4 times per week 1 time per day or more
31. Milk served to children ages 2 years and older is:
Whole or regular Only 2% reduced fat Always 1‐2% low‐fat Always 1% or
skim/nonfat Not applicable, my program does not serve any milk
Not applicable, my program does not
provide care for children ages 2 years and older
Strategy #2
Strategy #2

32. Flavored milk is served to children:
More than once a month Less than 1 time per
month Rarely, 1‐2
times per year
Never Not applicable, my program does not serve
any milk
Nutrition: Beverages Served, Provider Practices & Education (Toddlers & Preschoolers)
33. Beverages offered to toddlers over 1 year are offered in a bottle:
All of the time Most of the time Some of the time Rarely or never Not applicable, my
program does not provide care for toddlers
34. Training opportunities on juice and other beverage recommendations for toddlers and preschoolers are offered to providers:
Rarely or never Less than 1 time per year 1 time per year 2 or more times per year
35. Parents of toddlers and preschoolers are offered education on juice and other beverage recommendations (e.g., special programs, newsletters, information sheets):
Rarely or never Less than 1 time per year 1 time per year 2 or more times per year
Section 2. Physical Activity/Screen Time for Preschoolers
36. The next set of questions refer only to preschoolers (ages 3‐5). Does your program provide care to preschoolers?
Yes No (SKIP TO QUESTION 58)
Physical Activity: Time Provided (Preschoolers) 37. Active play time (indoor and outdoor) is provided to all preschool children, including children with special needs:
45 minutes or less each
day 46‐90 minutes each day 91‐120 minutes each day More than 120 minutes
each day
38. In preschool classrooms, structured (or teacher‐led) activities are provided to all children, including children with special needs:
1 time per week or less 2‐4 times per week 1 time per day 2 or more times per day
39. Outdoor active play time is provided to all preschool children, including children with special needs:
1 time a day for 30 minutes or less
1 or more times a day for a total of 30‐45 minutes
1 or more times a day for a total of 45‐60 minutes
2 or more times each day for a total of 60 minutes or
more
Strategy #8
½ DAY PROGRAMS ONLY
Strategy #4
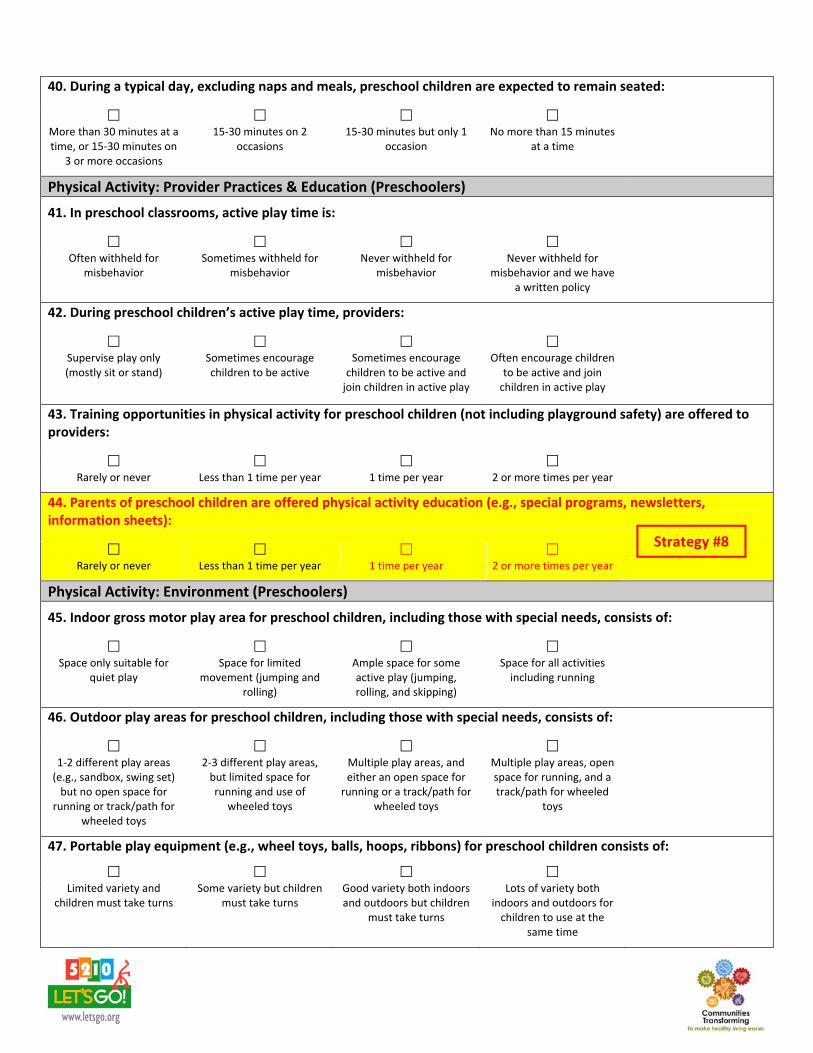
40. During a typical day, excluding naps and meals, preschool children are expected to remain seated:
More than 30 minutes at a time, or 15‐30 minutes on
3 or more occasions
15‐30 minutes on 2 occasions
15‐30 minutes but only 1 occasion
No more than 15 minutes at a time
Physical Activity: Provider Practices & Education (Preschoolers)
41. In preschool classrooms, active play time is:
Often withheld for
misbehavior Sometimes withheld for
misbehavior Never withheld for
misbehavior Never withheld for
misbehavior and we have a written policy
42. During preschool children’s active play time, providers:
Supervise play only (mostly sit or stand)
Sometimes encourage children to be active
Sometimes encourage children to be active and join children in active play
Often encourage children to be active and join children in active play
43. Training opportunities in physical activity for preschool children (not including playground safety) are offered to providers:
Rarely or never Less than 1 time per year 1 time per year 2 or more times per year
44. Parents of preschool children are offered physical activity education (e.g., special programs, newsletters, information sheets):
Rarely or never Less than 1 time per year 1 time per year 2 or more times per year
Physical Activity: Environment (Preschoolers)
45. Indoor gross motor play area for preschool children, including those with special needs, consists of:
Space only suitable for
quiet play Space for limited
movement (jumping and rolling)
Ample space for some active play (jumping, rolling, and skipping)
Space for all activities including running
46. Outdoor play areas for preschool children, including those with special needs, consists of:
1‐2 different play areas (e.g., sandbox, swing set) but no open space for
running or track/path for wheeled toys
2‐3 different play areas, but limited space for running and use of
wheeled toys
Multiple play areas, and either an open space for running or a track/path for
wheeled toys
Multiple play areas, open space for running, and a track/path for wheeled
toys
47. Portable play equipment (e.g., wheel toys, balls, hoops, ribbons) for preschool children consists of:
Limited variety and
children must take turns Some variety but children
must take turns Good variety both indoors and outdoors but children
must take turns
Lots of variety both indoors and outdoors for children to use at the
same time
Strategy #8

Screen Time: Availability (Preschoolers)
48. The next set of questions refer to screen time for preschoolers. Does your program have a television or a computer?
Yes, my program has a television and/or a
computer
No, my program does not have a television or a computer (SKIP TO QUESTION 58)
49. In preschool classrooms, televisions are:
Located in every classroom
(100%) Located in most
classrooms (at least 50%) Located in some
classrooms (less than 50%) Stored outside of classrooms, except for occasional use
Not applicable, my program does not have
a television
50. For preschool children, the total amount of screen time:
Is not limited At child care, we strive to
achieve 2 hours or less per week
At child care, we strive to achieve no more than 1
hour per week
At child care, we strive to achieve no more than 30 minutes per week, and we
work with parents/caregivers to ensure that children have no more than 1‐2 hours per day
51. For preschool children, television/DVD viewing includes:
All types of programming and videos, with limited coordination with the
curriculum
Educational and some commercial programming and videos, some of which are integrated with the
curriculum
Mostly educational, age‐appropriate programming and videos, many of which are integrated with the
curriculum
Only commercial‐free, age‐appropriate, educational
programming that is integrated with the
curriculum
Not applicable, my program does not have a television, nor do we view shows using the
internet
52. For preschool children, television/DVD viewing during meals or snack times occurs:
All of the time Most of the time Some of the time Rarely or never Not applicable, my
program does not have a television, nor do we view shows using the
internet
53. Television/video viewing is used as a reward in preschool children’s classrooms:
All of the time Most of the time Some of the time Rarely or never Not applicable, my
program does not have a television, nor do we view shows using the
internet
54. Among preschool children, computers are:
Available for use all of the time, and time allowed per
child is unlimited
Available several times during the day and each child is allowed between 30 and 45 minutes per day
Available only during a set time of day, and each child is allowed between 15 and
30 minutes per day
Available only during a set time of day, and each child is limited to 15 minutes per day
Not applicable, my program does not have
a computer
Strategy #5
Strategy #5

Screen Time: Provider Practices & Education (Preschoolers)
55. During screen time activities with preschool children, providers supervise and watch with the children:
Rarely or never Some of the time Most of the time All of the time
56. Providers are offered training opportunities on screen time reduction and/or media literacy for preschool children:
Rarely or never Less than 1 time per year 1 time per year 2 or more times per year
57. Parents of preschool children are offered screen time reduction and/or media literacy education (e.g., special programs, newsletters, or information sheets):
Rarely or never Less than 1 time per year 1 time per year 2 or more times per year
Section 3. Physical Activity/Screen Time for Toddlers
58. The next set of questions refer only to toddlers (ages 1‐2). Does your program provide care for toddlers?
Yes No (SKIP TO QUESTION 69)
Physical Activity: Time Provided (Toddlers)
59. Active play time (indoor and outdoor) is provided to all toddlers, including children with special needs:
15‐30
minutes per day 31‐45
minutes each day 46‐60
minutes each day 61‐90
minutes each day
60. Outdoor active play time is provided to all toddlers, including children with special needs:
1 time a day for 30 minutes or less
1 or more times a day for a total of 30‐45 minutes
1 or more times a day for a total of 45‐60 minutes
2 or more times each day for a total of 60 minutes or
more
Physical Activity: Environment & Provider Practices (Toddlers)
61. For toddlers, including those with special needs, indoor and outdoor play spaces consist of:
Space only suitable for
quiet play Space is available, but allows for only limited types of activities
Areas separate from preschoolers that provides space for exploration and
skill building
Areas separate from preschoolers with space available for all types of
activities
62. For toddlers, portable play equipment (e.g., wheeled toys, balls, hoops, ribbons) are age‐appropriate and consist of:
Limited variety and
children must take turns Some variety but children
must take turns Good variety both indoors and outdoors but children
must take turns
Lots of variety both indoors and outdoors for children to use at the
same time
Strategy #8
½ DAY PROGRAMS ONLY
Strategy #4

63. During toddlers’ active play time, staff:
Supervise play only (mostly sit or stand)
Sometimes encourage children to be active
Sometimes encourage children to be active and join children in active play
Often encourage children to be active and join children in active play
Physical Activity: Education (Toddlers)
64. Training opportunities in physical activity for toddlers (not including playground safety) are offered to providers:
Rarely or never Less than 1 time per year 1 time per year 2 or more times per year
65. Parents of toddlers are offered physical activity education (e.g., special programs, newsletters, information sheets):
Rarely or never Less than 1 time per year 1 time per year 2 or more times per year
Screen Time: Availability & Education (Toddlers)
66. Toddlers are allowed to watch television/videos:
1 or more times each day 2‐4 times per week 1 time per week or less Never Not applicable, my
program does not have a television, nor do we view shows/videos using the
internet
67. Training opportunities on screen time reduction and/or media literacy for toddlers are offered to providers:
Rarely or never Less than 1 time per year 1 time per year 2 or more times per year
68. Parents of toddlers are offered screen time reduction and/or media literacy (e.g., special programs, newsletters, or information sheets):
Rarely or never Less than 1 time per year 1 time per year 2 or more times per year
Section 4. Breastfeeding
69. The next set of questions refer to infants and breastfeeding. Does your program provide care for infants (birth‐1 year) OR any older breastfed children?
Yes No (SKIP TO QUESTION 95)
Breastfeeding: Environment
70. A designated area for mothers to breastfeed their infants, other than a bathroom, is:
Not available Only available upon
request Always available, has
appropriate seating, but lacks either privacy or an
electrical outlet
Always available, has appropriate seating,
provides complete privacy, and has an electrical outlet
Strategy #8
Strategy #5
Strategy #8

71. Culturally appropriate breastfeeding support materials (e.g., pictures, posters, brochures, pamphlets), not including those produced or supplied by commercial entities and/or manufacturers of infant formula, are:
Not displayed Displayed, but are limited Displayed and include
multiple types of materials Displayed in several areas of the facility and include
pictures, posters, brochures, pamphlets, and
other resources
72. For breastfeeding mothers needing to store expressed milk, the facility provides:
No refrigerator or freezer
space Limited refrigerator and freezer space, but it is not consistently available
Sufficient refrigerator and freezer space that is
available most of the time
Sufficient refrigerator and freezer space that is always available
73. Learning and play materials for children which normalize breastfeeding (e.g., books that contain pictures of breastfeeding, baby dolls that are nursing), include:
No toys and books
portraying breastfeeding are available
A few toys and books portraying breastfeeding
Toys and books portraying breastfeeding in most
classrooms
Toys and books portraying breastfeeding in all
classrooms
74. A feeding plan filled out by a parent/guardian and/or healthcare provider is:
Not used by my program Posted Posted, but not updated
regularly Posted and updated
regularly Posted, regularly updated, and is used to provide a daily report to parents
75. As part of the feeding plan, support for breastfeeding is:
Not explicitly included Sometimes included, but
relies on the provider to add additional information
to standard form
Usually included, and part of the standard form to be
filled in by parents
Always included, and covers age‐appropriate
introduction of solid food, feeding in response to baby’s cues, and inviting the mother to come to the
facility to nurse
Not applicable, my program does not use feeding plans for our
children
Breastfeeding: Education
76. Training on age‐appropriate infant feeding practices, including safe storage/handling of human milk, is offered to providers:
Rarely or never Only as part of new staff
orientation 1 time per year 2 or more times per year
77. Training on promoting and supporting breastfeeding, including exclusive breastfeeding, is offered to providers:
Rarely or never Only as a part of new staff
orientation
1 time per year 2 or more times per year

78. Breastfeeding families are instructed on how to properly label and store human milk for use in the child care program:
Rarely or never Informally, but not in
writing In writing In writing, and providers
check to make sure all milk provided is properly
labeled
Breastfeeding: Policy
79. At our child care facility, a written and explicit policy for promoting and supporting breastfeeding families:
Does not exist Is generally followed but is
not written Is written, generally
followed, and sometimes shared with parents
Is written, available, followed, and always shared with parents
80. The facility’s breastfeeding‐friendly policy is communicated to expectant mothers, families with infants, and visitors:
Rarely or never Sometimes, if asked Usually Always
Section 5. Infant Care
81. The next set of questions refer only to infants (birth ‐ 1 year). Does your program provide care for infants?
Yes No (SKIP TO QUESTION 95)
Nutrition: Provider Practices (Infants)
82. For infants, providers support self‐feeding skills (infant encouraged to finger‐feed self; fork and spoon introduced when ready) and transition to family style meals provided when appropriate:
Rarely or never Some of the time Most of the time All of the time
Physical Activity: Time Provided (Infants)
83. Short supervised periods of tummy time are provided for all infants, including those with special needs:
Less than once per day Once per day, everyday 2 times per day, most days Several times each day
84. Use of swings and infant seats (e.g., exersaucers, car seats, molded seats) is limited to 15 minutes (or less):
More than 4 times per day per child, or used for more than 15 minutes at a time
3‐4 times per day per child
2‐3 times per day per child
1‐2 times per day per child
85. Infants, including those with special needs, are taken outside:
Less than 1 time per day 1 time per day 1‐2 times per day 2‐3 times per day
½ DAY PROGRAMS ONLY
Strategy #4

86. When outdoors, infants are provided opportunities for exploration (e.g., rolling, scooting, crawling, walking):
Less than 1 time per week
or never
1‐2 times per week
3‐4 times per week
1 or more times each day
Physical Activity: Environment & Provider Practices (Infants)
87. For infants, including those with special needs, indoor and outdoor play spaces consist of:
Space only suitable for
quiet play Space is available, but allows for only limited types of activities
Areas separate from preschoolers that provides space for exploration and
skill building
Areas separate from preschoolers with space available for all types of
activities
88. Play equipment for infants (small push toys, balls, ramps for crawling, outdoor pad or blanket) are age appropriate and consist of:
Limited variety and
children must take turns Some variety but children
must take turns Good variety both indoors and outdoors but children
must take turns
Lots of variety both indoors and outdoors for children to use at the
same time
89. Providers engage with infants to encourage development of gross motor skills (e.g., reaching, sitting, standing, crawling, walking):
Rarely or never Some of the time Most of the time All of the time
Physical Activity: Education (Infants)
90. Training opportunities in physical activity for infants (not including playground safety) are offered to providers:
Rarely or never Less than 1 time per year 1 time per year 2 or more times per year
91. Parents of infants are offered physical activity education (e.g., special programs, newsletters, information sheets):
Rarely or never Less than 1 time per year 1 time per year 2 or more times per year
Screen Time: Availability & Education (Infants)
92. Infants are allowed to watch television/videos:
1 or more times each day 2‐4 times per week 1 time per week or less Never Not applicable, my
program does not have a television, nor do we view shows using the internet
93. Training opportunities on screen time reduction and/or media literacy for infants are offered to providers:
Rarely or never Less than 1 time per year 1 time per year 2 or more times per year
94. Parents of infants are offered screen time reduction and/or media literacy (e.g., special programs, newsletters, or information sheets):
Rarely or never Less than 1 time per year 1 time per year 2 or more times per year
Strategy #8
Strategy #5
Strategy #8

Section 6. Supportive Strategies
95. Within the past year, did your program participate in any local, state or national initiatives that support healthy eating/active living (other than 5‐2‐1‐0 Goes to Child Care)?
No Not yet, we’re still in
the planning stage Yes, in some or a few classrooms (less than
50%)
Yes, in most classrooms (at least
50%)
Yes, program‐wide (100%)
Yes, program‐wide before this year and we continued it this
year
96. Within the past year, did your program engage community organizations (e.g., farms, grocery stores, food banks, local doctors' offices) to help support healthy eating/active living at your program?
No Not yet, we’re still in
the planning stage Yes, in some or a few classrooms (less than
50%)
Yes, in most classrooms (at least
50%)
Yes, program‐wide (100%)
Yes, program‐wide before this year and we continued it this
year
97. Has your program implemented a staff wellness program that includes healthy eating and active living?
No No, but we have started to
work on it Yes, we implemented it
this year Yes, we implemented it before this year and we continued it this year
Not applicable, I am the only staff member
Section 7. Program Policies
Please refer to your program's policies for these last several questions. **You may need to connect with your director to answer this section.** Let's Go! will audit a sample of responses to verify them, and will also reach out to you to ask you to submit copies of your policies to Let's Go!.
The following words INDICATE A POLICY IS NOT REQUIRED: encourage, may, can, could, should, might, suggest, will strive to, will work to, try
The following words INDICATE A POLICY IS REQUIRED: shall, will, must, have to, insist, require, comply, enforce
Policy: Nutrition
98. Our policies require that snacks provided to children by our program (not sent in from home) must be healthy.
False, this is not required by our
policies True, this is required by our policies but it is not usually enforced in our program
True, this is required by our policies and is usually enforced in our program, and our director has
verified this
Not applicable, my program does not provide any snacks
99. Our policies require that celebration foods, whether brought in from home or supplied by our program, must be healthy.
False, this is not required by our
policies True, this is required by our policies but it is not usually enforced in our program
True, this is required by our policies and is usually enforced in our program, and our director has
verified this
Not applicable, my program practices only non‐food
celebrations
Strategy #6
Strategy #7
Strategy #9
Answers from this section determine whether or not a site is eligible for recognition at the Silver or Gold level.
Strategy #1
Strategy #1

100. Our policies prohibit using food as a reward.
False, this is not required by our
policies True, this is required by our policies but it is not usually enforced in our program
True, this is required by our policies and is usually enforced in our program, and our director has
verified this
101. Our policies require that the availability of sugary beverages (including juice) is limited.
False, this is not required by our
policies True, this is required by our policies but it is not usually enforced in our program
True, this is required by our policies and is usually enforced in our program, and our director has
verified this
Policy: Physical Activity & Screen Time
102. Our policies require that all children have opportunities for physical activity every day.
False, this is not required by our
policies True, this is required by our policies but it is not usually enforced in our program
True, this is required by our policies and is usually enforced in our program, and our director has
verified this
103. Our policies require that recreational screen time (includes television, computer and DVDs) for all children is limited.
False, this is not required by our
policies True, this is required by our policies but it is not usually enforced in our program
True, this is required by our policies and is usually enforced in our program, and our director has
verified this
Final Comments
104. Is there any other information about your work with CTG or Let's Go! this year that you would like to share?
Thank you very much for completing this survey! Your answers will help us understand what changes have occurred and will help us improve CTG and the Let's Go! programs. You will have an opportunity to review your completed survey with your CTG district coordinator or 5‐2‐1‐0 Goes to Child Care representative.
Strategy #3
Strategy #2
Strategy #4
Strategy #5
Please Note:
To be recognized as implementing STRATEGY 8, sites must offer parents education on Nutrition, IN ADDITION TO education on EITHER Physical Activity OR Screen Time, For ANY of the age groups.
STRATEGY 10 will be measured by whether or not the site participates in the Child and Adult Care Food Program which is captured on the registration form.
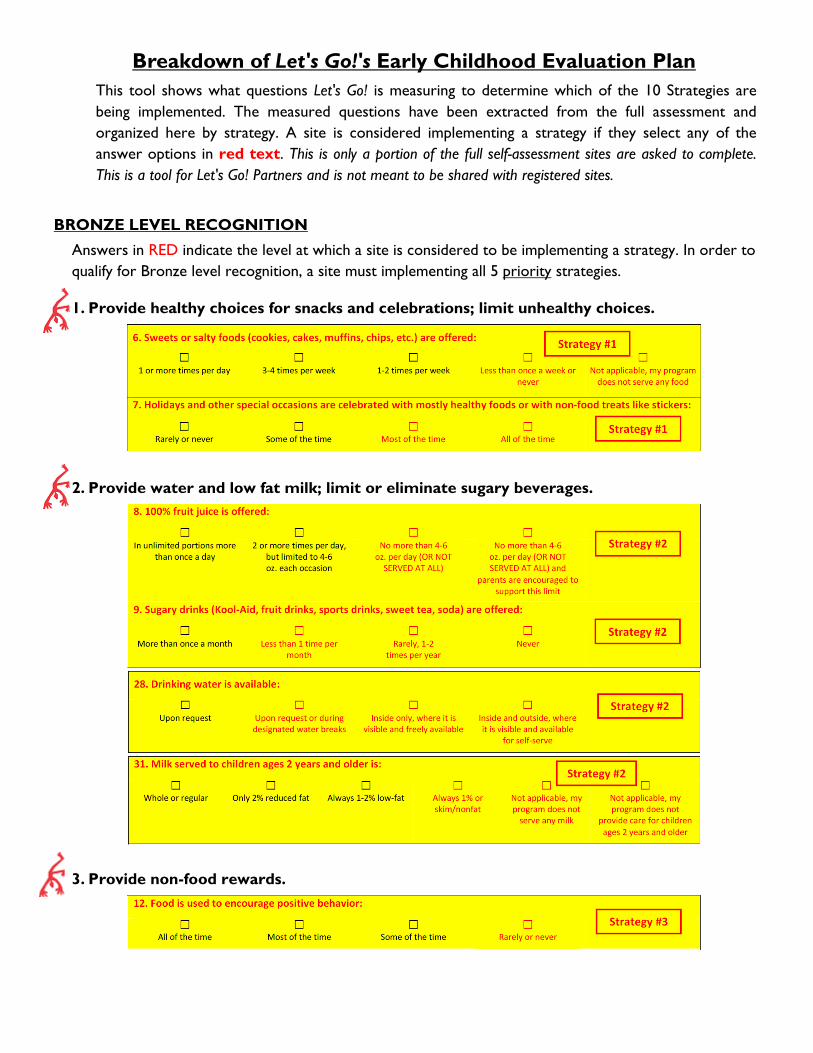
Breakdown of Let's Go!'s Early Childhood Evaluation Plan This tool shows what questions Let's Go! is measuring to determine which of the 10 Strategies are being implemented. The measured questions have been extracted from the full assessment and organized here by strategy. A site is considered implementing a strategy if they select any of the answer options in red text. This is only a portion of the full self-assessment sites are asked to complete. This is a tool for Let's Go! Partners and is not meant to be shared with registered sites.
BRONZE LEVEL RECOGNITION
Answers in RED indicate the level at which a site is considered to be implementing a strategy. In order to qualify for Bronze level recognition, a site must implementing all 5 priority strategies.
1. Provide healthy choices for snacks and celebrations; limit unhealthy choices.
2. Provide water and low fat milk; limit or eliminate sugary beverages.
3. Provide non-food rewards.
4. Provide opportunities for children to get physical activity every day.
5. Limit recreational screen time.
6. Participate in local, state, and national initiatives that support healthy eating and active
living.

7. Engage community partners to help support healthy eating and active living at your site.
8. Partner with and educate families in adopting and maintaining a lifestyle that supports
healthy eating and active living. *To be recognized as implementing Strategy 8, sites must offer parents education on Nutrition, IN ADDITION TO education on EITHER Physical Activity OR Screen Time, for ANY of the age groups.*
OR
AND THEN
OR
OR
OR
OR
OR

9. Implement a staff wellness program that includes healthy eating and active living.
10. Collaborate with Food and Nutrition Programs to offer healthy food and beverage options.
SILVER AND GOLD LEVEL RECOGNITION
Answers to the policy questions below determine whether a site is eligible for recognition at the Silver or Gold level.
SILVER: A site must have written, enforced policies requiring at least 1 and up to 4 of the priority strategies.
GOLD: A site must have written, enforced policies requiring all 5 of the priority strategies.