4. assessment of cep (nxpowerlite)
TRANSCRIPT

CEP Workshop Series 2013 Module 4: Assessment
Fraser Todd and Michelle Fowler 2013

Workshop Introduction

Workshop Agenda
Mihi and Introductions
Housekeeping & Workshop overview
Levels of Assessment
Screening
Brief Assessment
Comprehensive Assessment and Formulation
Action Planning

Three Dimensions of CEP Practice Spirit – Principles - Techniques:
Spirit
7 Key Principles
Techniques
1. Cultural Considerations
2. Recovery & Well-being
3. Engagement 4. Motivation
5. Assessment
6. Management
7. Integrated Care
Person-focused care
Well-being orientated care Integrated care
Walk the Talk

Exercise 1: Mindfulness Introduction

Levels of Assessment and Intervention
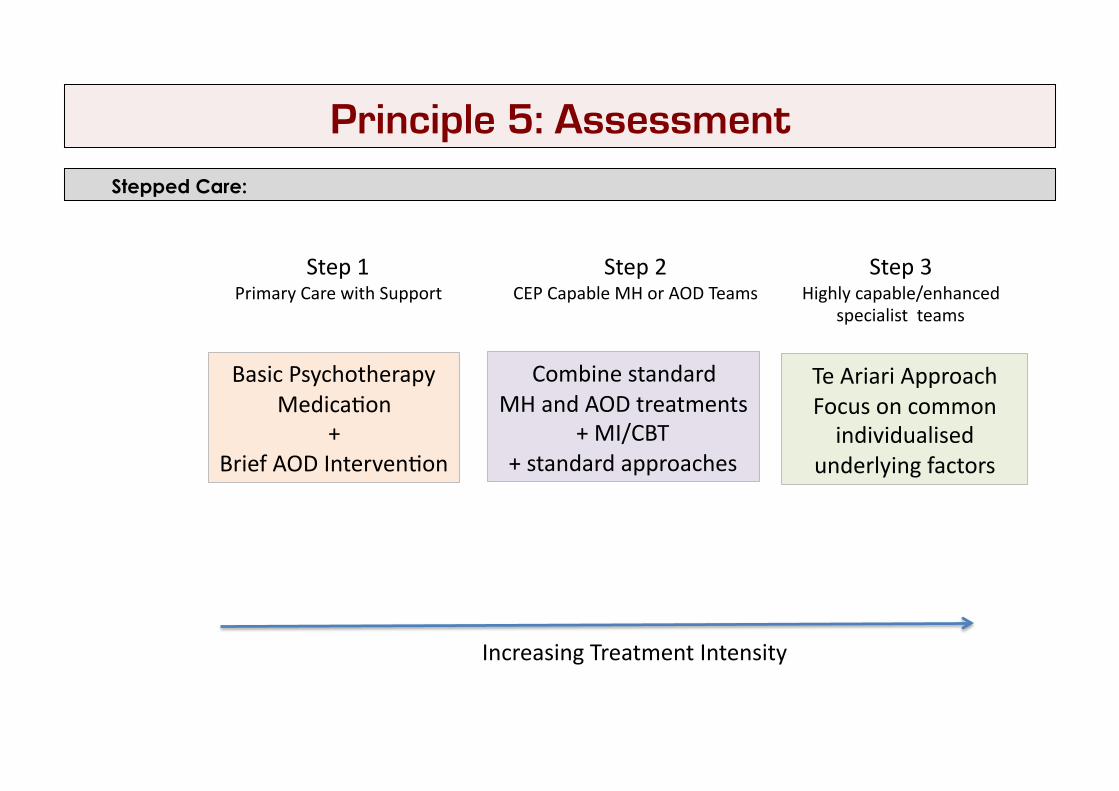
Principle 5: Assessment Stepped Care:
Step 1 Primary Care with Support
Basic Psychotherapy Medica7on
+ Brief AOD Interven7on
Step 2 CEP Capable MH or AOD Teams
Step 3 Highly capable/enhanced
specialist teams
Te Ariari Approach Focus on common individualised
underlying factors
Combine standard MH and AOD treatments
+ MI/CBT + standard approaches
Increasing Treatment Intensity

Mild dependence/problems
Principle 5: Assessment Levels of Assessment:
Step 1
Screening
Step 2 Step 3
Comprehensive Assessment 1
Mul7-‐dimensional /Comprehensive Assessment 2
Brief Assessment
Increasing Problem Complexity
No further ac7on Brief Interven7on Step 3+
Moderate-‐Severe

Screening

Principle 5: Assessment Recommended Screening Instruments:
• WHO-‐ASSIST • Substances and Choices Scale (SACS) -‐ adolescents • AUDIT (alcohol only) • Modified MINI Screen for mental health • EIGHT Gambling Screen

Exercise 2: Screening
See workbook

Brief Assessment and Intervention
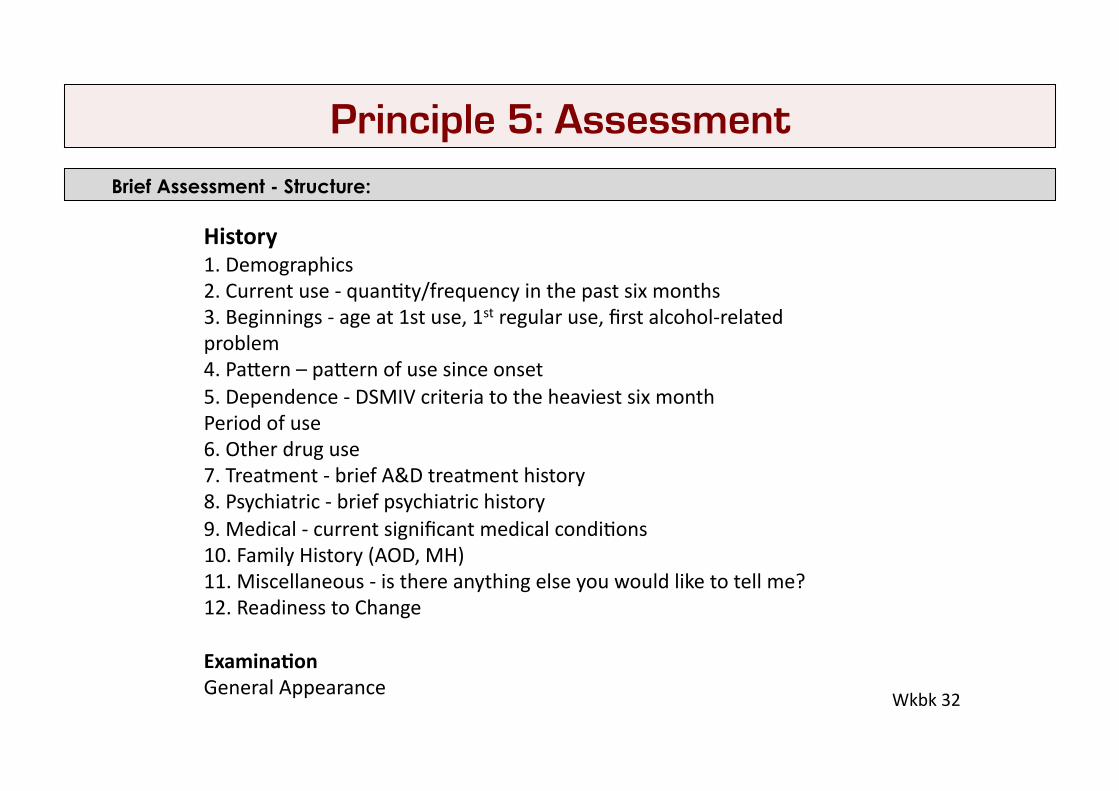
Principle 5: Assessment Brief Assessment - Structure:
History 1. Demographics 2. Current use -‐ quan7ty/frequency in the past six months 3. Beginnings -‐ age at 1st use, 1st regular use, first alcohol-‐related problem 4. PaXern – paXern of use since onset 5. Dependence -‐ DSMIV criteria to the heaviest six month Period of use 6. Other drug use 7. Treatment -‐ brief A&D treatment history 8. Psychiatric -‐ brief psychiatric history 9. Medical -‐ current significant medical condi7ons 10. Family History (AOD, MH) 11. Miscellaneous -‐ is there anything else you would like to tell me? 12. Readiness to Change
Examina.on General Appearance
Wkbk 32
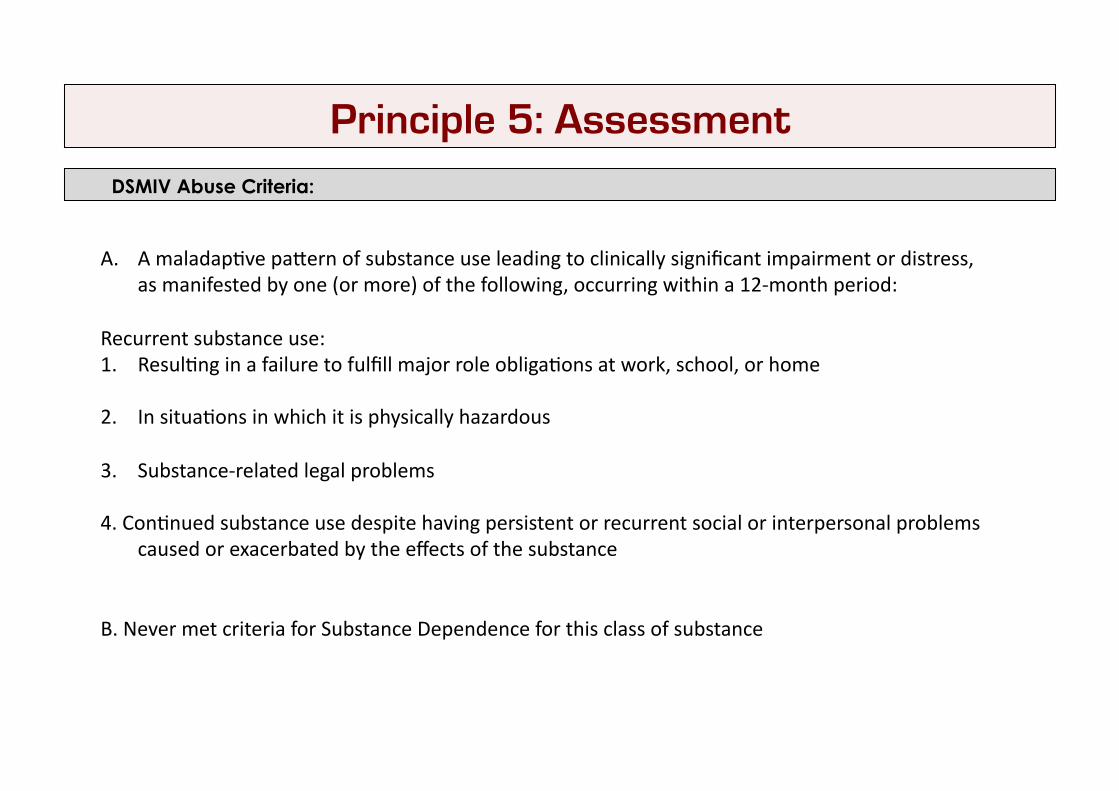
Principle 5: Assessment DSMIV Abuse Criteria:
A. A maladap7ve paXern of substance use leading to clinically significant impairment or distress, as manifested by one (or more) of the following, occurring within a 12-‐month period:
Recurrent substance use: 1. Resul7ng in a failure to fulfill major role obliga7ons at work, school, or home
2. In situa7ons in which it is physically hazardous
3. Substance-‐related legal problems
4. Con7nued substance use despite having persistent or recurrent social or interpersonal problems caused or exacerbated by the effects of the substance
B. Never met criteria for Substance Dependence for this class of substance
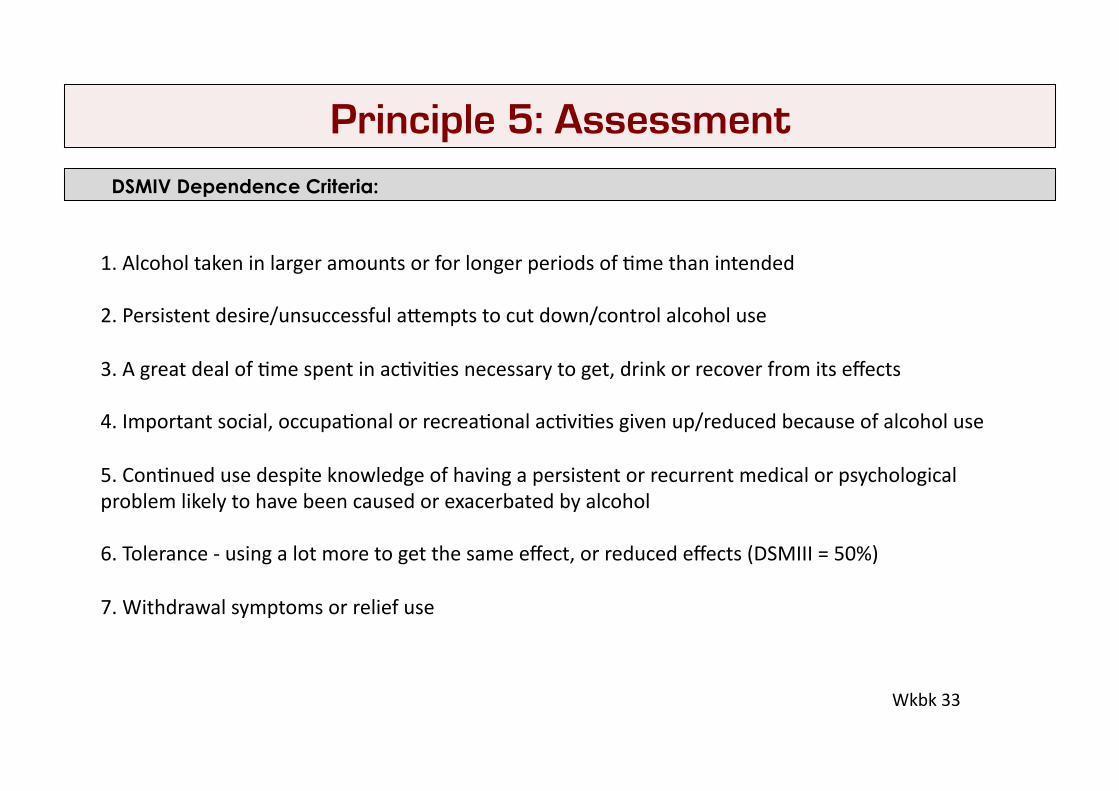
Principle 5: Assessment DSMIV Dependence Criteria:
1. Alcohol taken in larger amounts or for longer periods of 7me than intended
2. Persistent desire/unsuccessful aXempts to cut down/control alcohol use
3. A great deal of 7me spent in ac7vi7es necessary to get, drink or recover from its effects
4. Important social, occupa7onal or recrea7onal ac7vi7es given up/reduced because of alcohol use
5. Con7nued use despite knowledge of having a persistent or recurrent medical or psychological problem likely to have been caused or exacerbated by alcohol
6. Tolerance -‐ using a lot more to get the same effect, or reduced effects (DSMIII = 50%)
7. Withdrawal symptoms or relief use
Wkbk 33
Principle 5: Assessment DSM5 Substance Use Disorder Criteria:
• 11 criteria
Abuse + Dependence
-‐ Legal
+ Craving

Principle 5: Assessment Brief Intervention – FRAMES for AOD:
(Ask permission)
Feedback • Feedback based on screening instrument/brief assessment re substance use
Responsibility • Acknowledge the client is responsible for their own behaviour and decisions
Advice • Clear objec7ve advice regarding how to reduce harms associated with con7nued use
Menu • Menu of op7ons or strategies to reduce/stop use
Empathy • Support self-‐efficacy (MI)
Summarise • Summarise and reflect clients concerns
(Nego7ate follow-‐up)
Principle 5: Assessment HPA Safe Drinking Guidelines:
Reduce long-‐term health risks by drinking no more than:
Females: 2 standard drinks a day 4 standard drinks on any single occasion 10 standard drinks a week
Males: 3 standard drinks a day 5 standard drinks on any single occasion 15 standard drinks a week
and at least two alcohol-‐free days every week.
Advice for pregnant women or those planning to get pregnant: no alcohol for pregnant women or those planning to get pregnant (no known safe level of alcohol use at any stage of pregnancy)

Principle 5: Assessment HPA safe drinking guidelines:
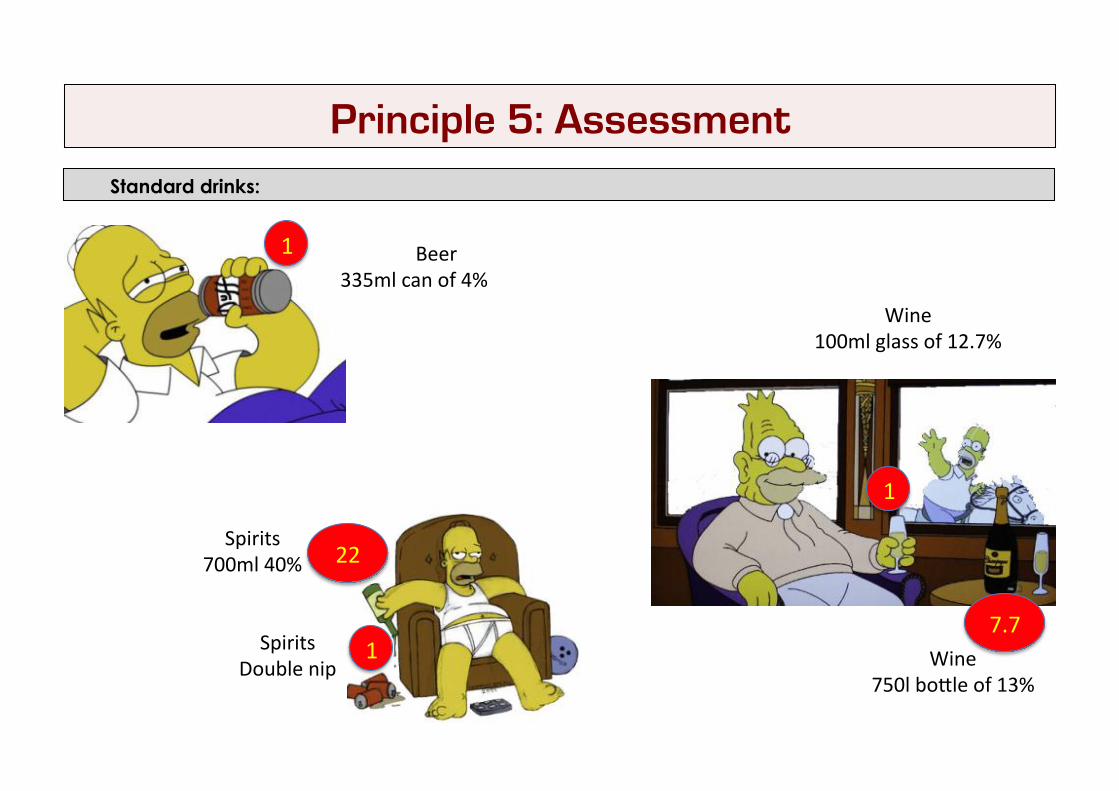
Principle 5: Assessment Standard drinks:
Standard
Beer 335ml can of 4%
Wine 100ml glass of 12.7%
Spirits 700ml 40%
1
1
1
22
Spirits Double nip Wine
750l boXle of 13%
7.7
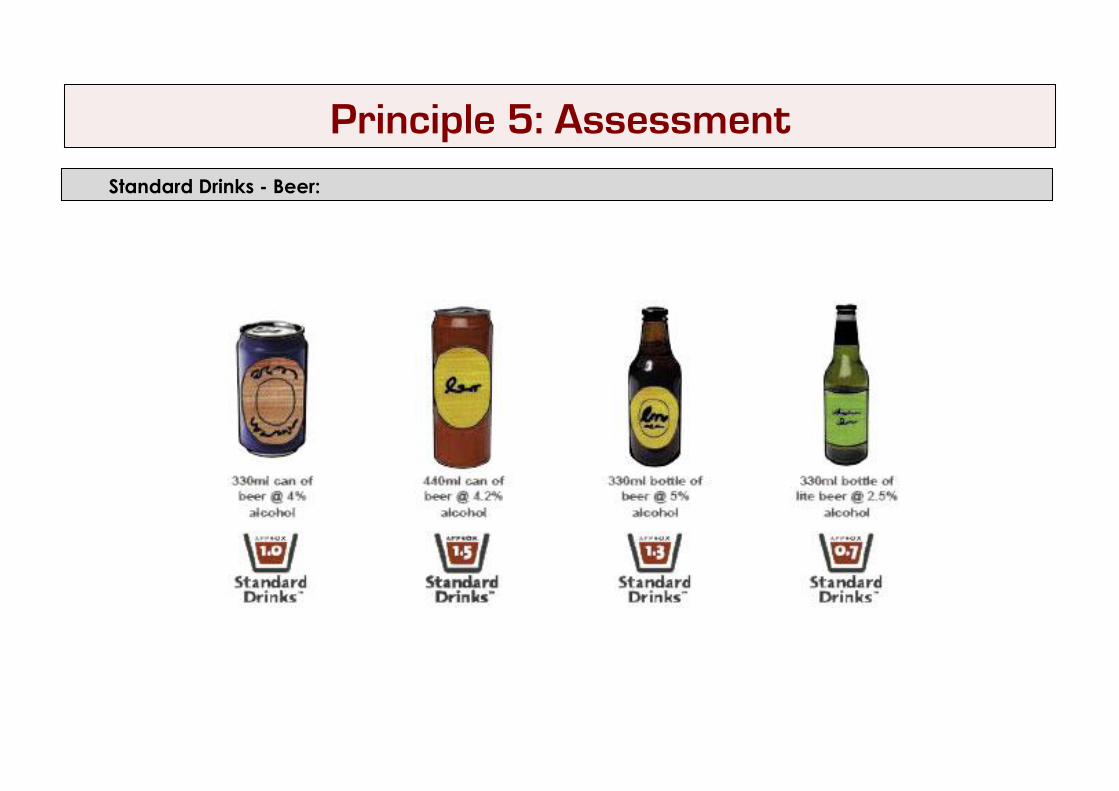
Principle 5: Assessment Standard Drinks - Beer:
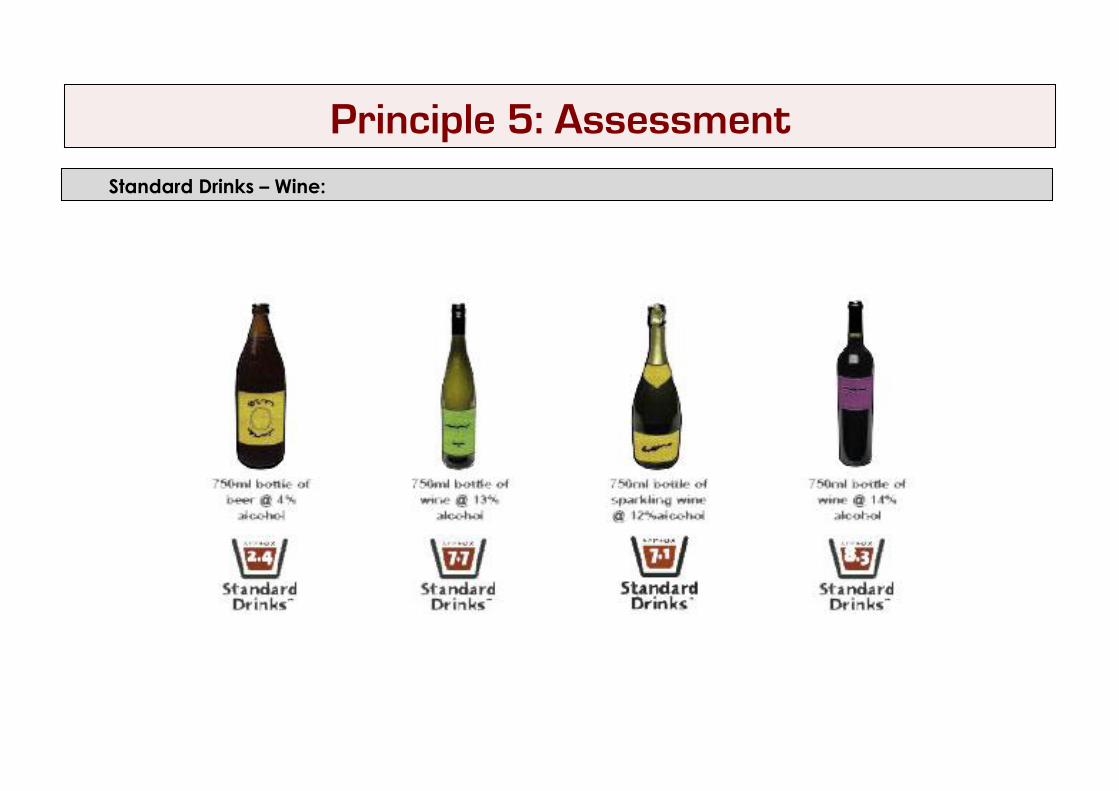
Principle 5: Assessment Standard Drinks – Wine:
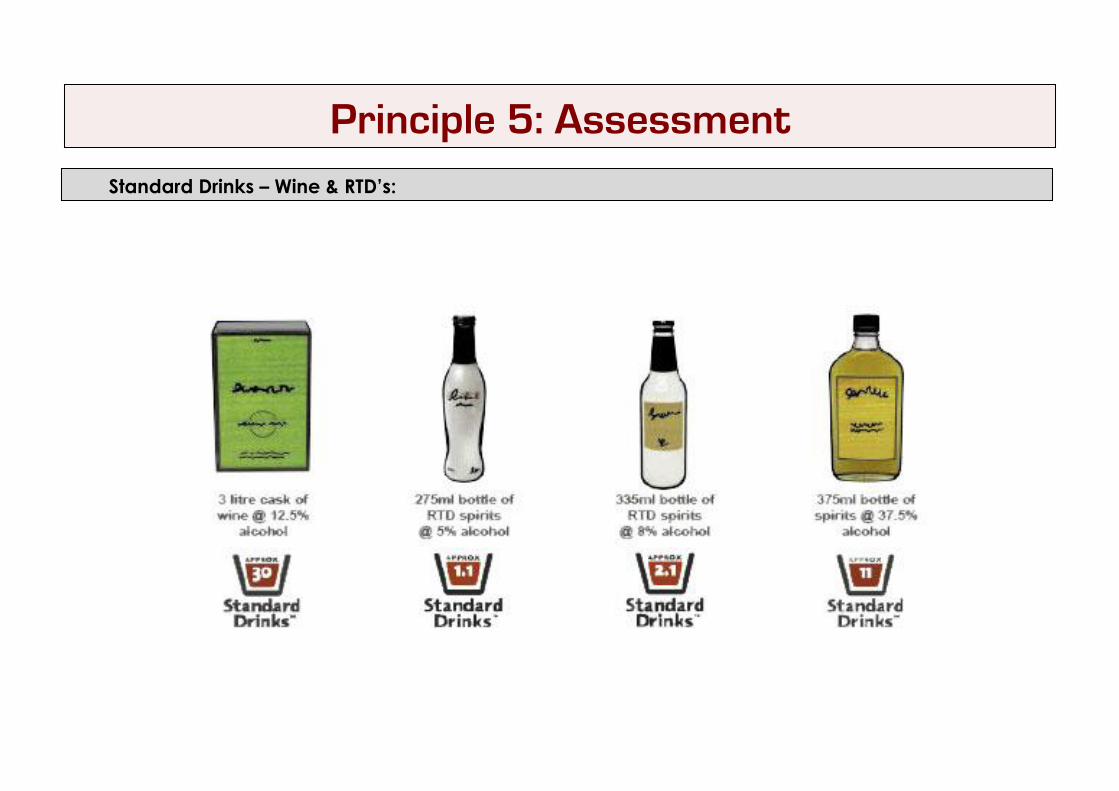
Principle 5: Assessment Standard Drinks – Wine & RTD’s:
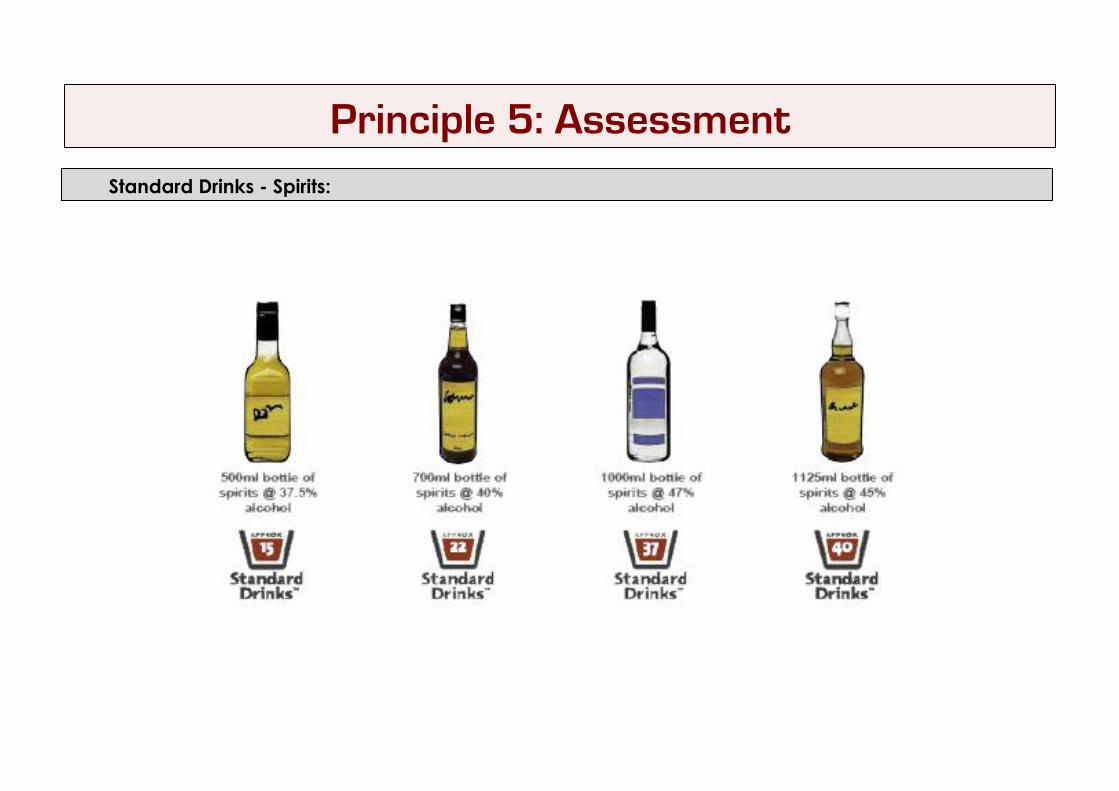
Principle 5: Assessment Standard Drinks - Spirits:
Principle 5: Assessment Brief Alcohol Intervention:
Step 1: Summarise Assessment Findings • Drinking paXern (quan7ty and frequency) • Drinking-‐related problems • Symptoms of dependence • Presence of contra-‐indica7ons • Posi7ve family history
Step 2: Brief Tutorial • Outline ALAC drinking guidelines • Educate about what is a standard drink • Relate these guidelines to their own drinking, by calcula7ng number of standard drinks consumed per session/week, and presence of contraindica7ons (driving, liver damage etc) • Give the informa7on that about 20-‐30% of New Zealanders misuse alcohol • Invite their comment
Step 3: Giving Advice • Advise of risk of con7nued heavy drinking (individualise) • Advise drinking within the ALAC drinking guidelines which may include abs7nence • In an engaging interac7ve way, suggest several drinking behaviour changes
Step 4: Nego.a.ng Change • Nego7ate what a new drinking goal and/or change in drinking behaviour will be • Nego7ate how this reduc7on will be brought about • Nego7ate when a review of this goal (normally less than three months) can occur
Wkbk 35

Principle 5: Assessment Strategy for the Assessment of Mental Health Problems:
1. For condi7ons where there is a clear trigger or onset (e.g. PTSD)
2. For condi7ons where there is NO clear trigger or onset
1. Onset 2. Dx at Maximal Intensity
4. Current func7on and Dx criteria
3. Periods symptoms free or mild
1. Current func7on and Dx criteria
2. Periods like this in the past?
4. Course (mild/no symptoms)
3. Onset (vague)
The Comprehensive Assessment & Aetiologicl Formulation

Principle 5: Assessment Assessing the relationship between Mental Health and Substance Use:
1. Likely rela7onship between substances and MH
2. Timing of onset
3. Family history
4. Symptoms during abs7nence
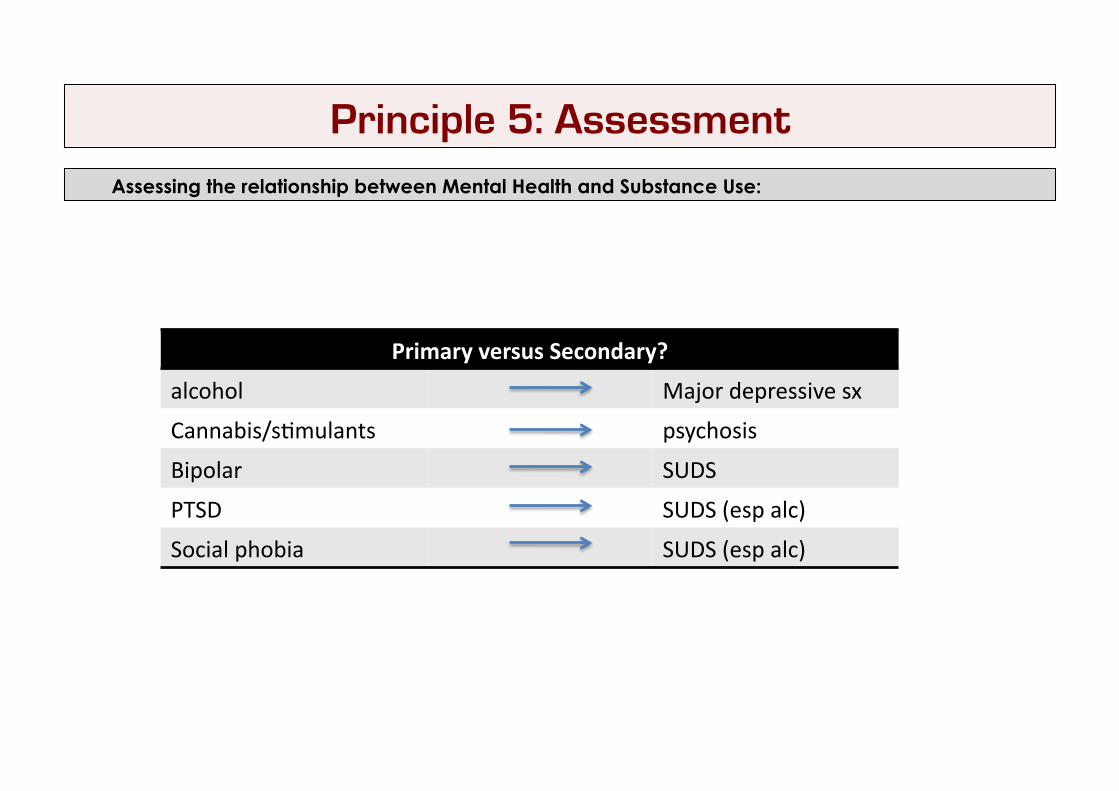
Principle 5: Assessment Assessing the relationship between Mental Health and Substance Use:
Primary versus Secondary?
alcohol Major depressive sx
Cannabis/s7mulants psychosis
Bipolar SUDS
PTSD SUDS (esp alc)
Social phobia SUDS (esp alc)

Principle 4: Assessment Functional analysis:
The Payoff Matrix
Using substance Not using substances
Advantages
Disadvantage
What the behaviour (substance use) maximizes and minimizes in a person’s life

Principle 5: Assessment TImelines:

Exercise 4:
See Workbook Pg 46
The Aetiological (Causal) Formulation
Principle 5: Assessment The Opinion:
Three perspec.ves given equal weight:
1. Diagnos7c (nomothe7c)
2. Individualised (idiographic)
3. Ae7ological (causal)
Principle 5: Assessment :

• INTEGRATES mul7ple theore7cal perspec7ves
• makes MEANING of tangata whaiora’s situa7on • HEALING in its own right
• iden7fies important DEEPER factors that are important targets of treatment • EXTENDS the clinician beyond commonly recognized paXerns
• grows clinicians INTUITION • TRANSITIONS novice to expert assessor
Why is the Formulation Important?

1. Iden7fy key explanatory factors from history
2. Draw a 4x4 Grid
4. Enter factors in each box of the grid
3. Label the grid: bio/psycho/social/spiritual predisposing/precipita7ng/perpetua7ng/protec7ng
5. Four paragraphs to make a narra7ve paXern/predisposing&precipita7ng/perpetua7ng/protec7ng
How Do You Do a Formulation?
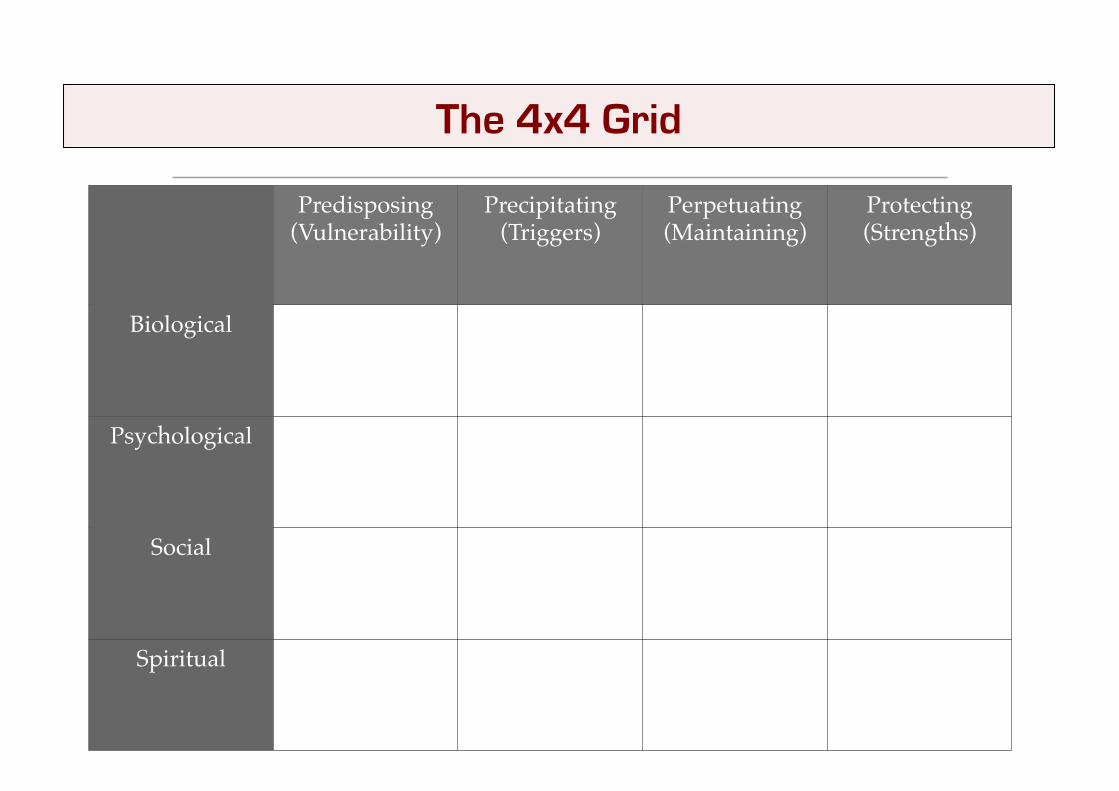
Predisposing (Vulnerability)!
Precipitating (Triggers)!
Perpetuating (Maintaining)!
Protecting (Strengths)!
Biological!
Psychological!
Social!
Spiritual!
The 4x4 Grid

• Chose factors that predict treatments
• No right or placement in grid • Specula7ve but evidence-‐informed
• Basic -‐ use whatever models you are familiar with • Advanced -‐ use complex, evidence-‐informed models
Choice of Factors

PaXern: Descrip(on of the pa0erns of the presenta(on e.g. chronic, relapsing, mul(-‐problem self-‐sustaining system, intermi0ent etc
Predisposing and Precipita7ng Factors:
Perpetua7ng Factors:
Protec7ng Factors:
Four Paragraphs

The main targets are ooen the perpetua7ng/maintaining and protec7ve/strengths factors
Priori7ze: Urgent issues (safety & stabiliza7on), serious problems, pivotal issues from the formula7on, easily achieved goals
Set key goals for early, middle, late and independence stages of treatment in decreasing detail
Goal Setting

Exercise 4: Rachel – Aetiological Formulation
See Workbook pg 37

Aetiological Models
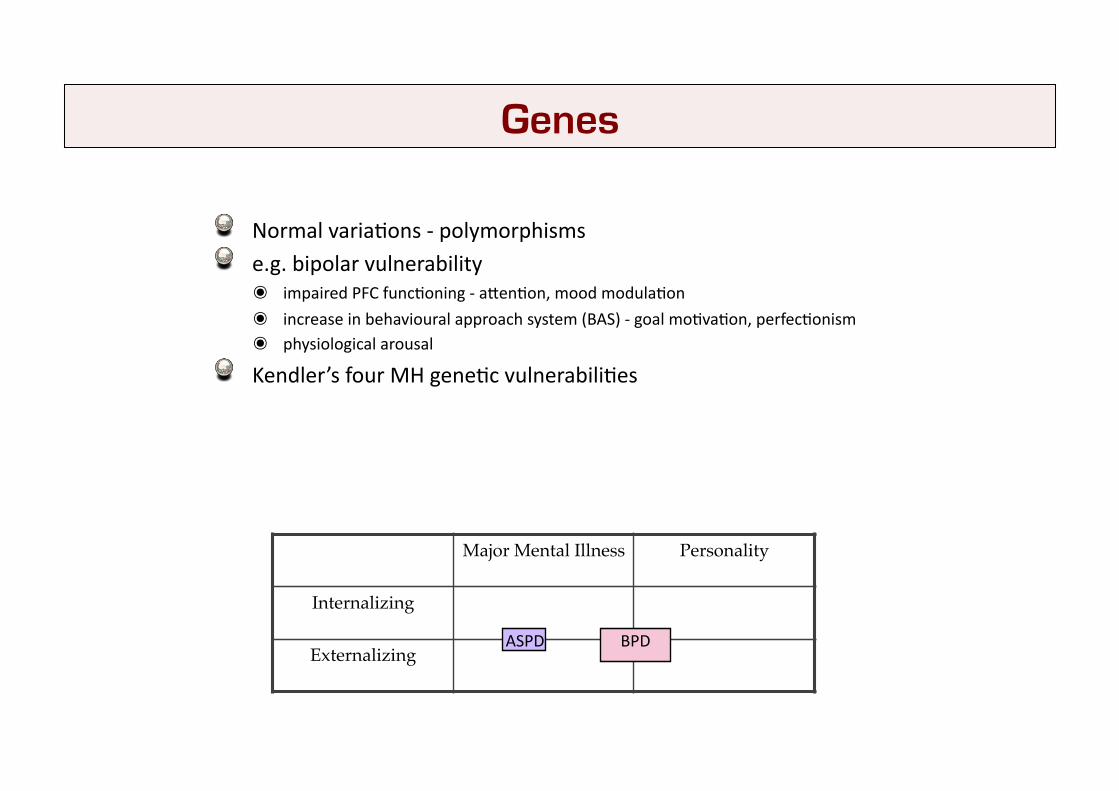
" Normal varia7ons -‐ polymorphisms " e.g. bipolar vulnerability
๏ impaired PFC func7oning -‐ aXen7on, mood modula7on
๏ increase in behavioural approach system (BAS) -‐ goal mo7va7on, perfec7onism ๏ physiological arousal
" Kendler’s four MH gene7c vulnerabili7es
Major Mental Illness! Personality!
Internalizing!
Externalizing!ASPD BPD
Genes
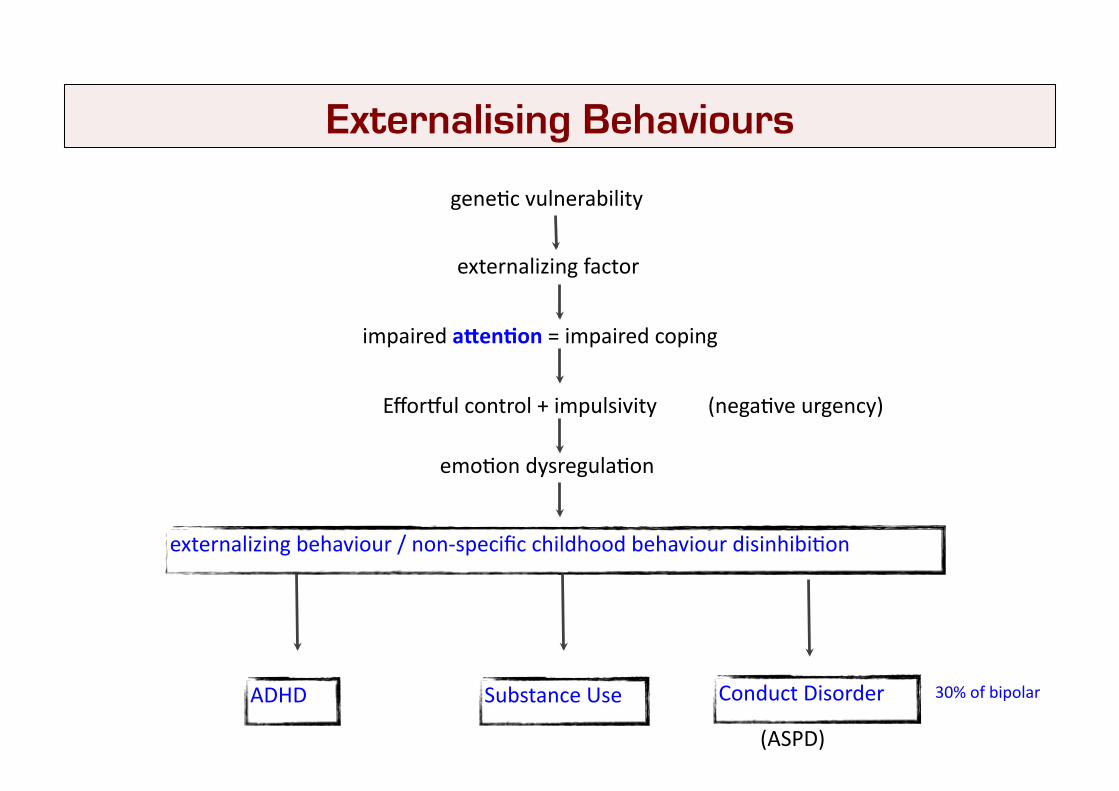
gene7c vulnerability
externalizing factor
externalizing behaviour / non-‐specific childhood behaviour disinhibi7on
impaired aVen.on = impaired coping
emo7on dysregula7on
ADHD Substance Use Conduct Disorder
(ASPD)
30% of bipolar
Efforqul control + impulsivity (nega7ve urgency)
Externalising Behaviours

THREAT PERCEIVED APPRAISAL STRESS RESPONSE!
CHRONIC!
ACUTE
HPA Activation!
Flight/Fright!
CRH/Cortisol/Adrenaline!
Prefrontal Cortex Damage!attention!working memory!emotional control!behaviour control!
Stress

Coping Resources Coping Processes
✴ optimism!✴ mastery!✴ self-esteem!✴ social support!
Coping +!=!
approach!v!
avoidance!
Coping resources lower cor7sol/ physiological ac7va7on
Lessens the impact of chronic stress
Coping resources predict more approach coping
Emo7onal social support = oxytocin = powerful anxioly7c
Approach coping = lower stress
Avoidance coping = increased stress
Coping
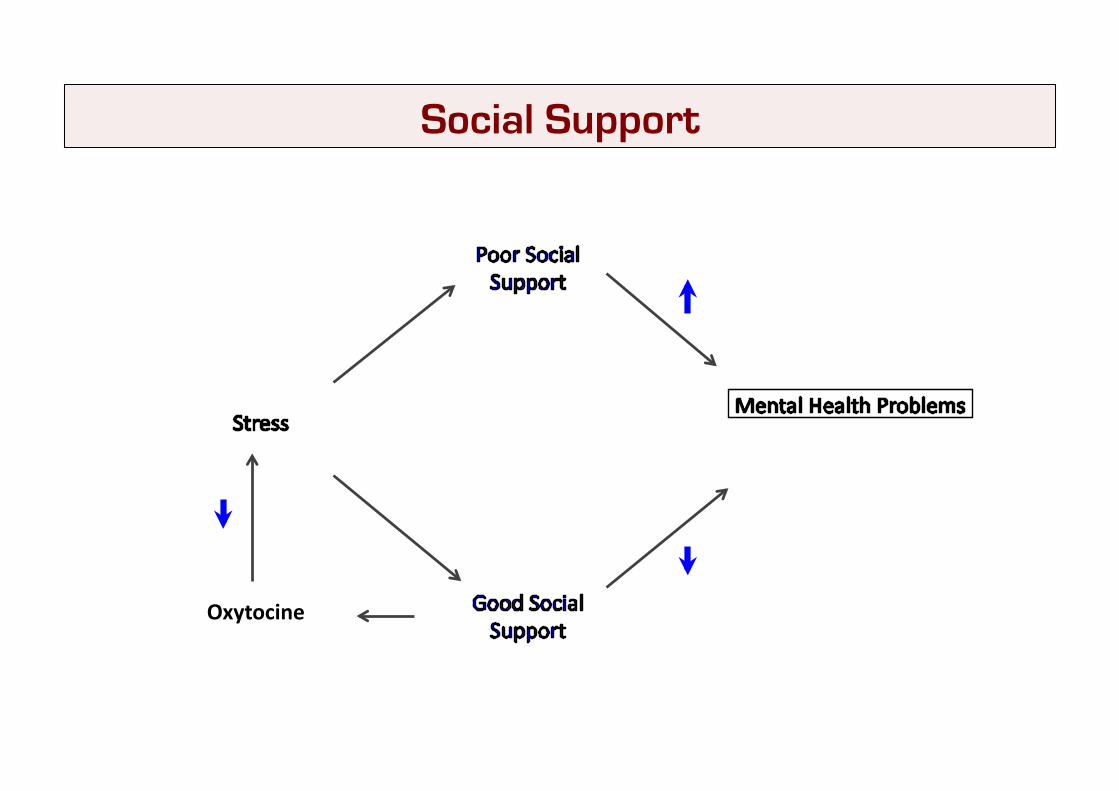
Oxytocine
Social Support
Emotional vulnerability heightened sensitivity and reactivity, delayed return to baseline high anxiety temperament a crucial predisposing factor
Invalidating environment punishing, ignoring or trivializing of thoughts and emotions abuse
Emotional dysregulation intense experiences and expressions of emotion
Borderline Personality Disorder 1

Emotional vulnerability
Invalidating environment Emotional dysregulation
Disrupted emotional, cognitive and behavioural responses
Maladaptive patterns of coping (self-harm, binge eating, substance abuse)
Borderline Personality Disorder 2

Mild genetic influence – both for anxiety in general and for social anxiety
Temperament – behavioral inhibition - children respond to new situations with caution withdrawal and a tendency not to avoid
Cognitive/Thinking Distortions in social information processing and thoughts, attitudes and beliefs = thoughts that social interactions will lead to negative outcomes
Anticipate negative outcomes, evaluate their own performance more negatively higher level of negative cognitions about social tasks – limited to social situations Often have recurrent negative spontaneous memories of negative social interactions
Vicious cycle – see next slide
Social Phobia 1

Social Phobia 2
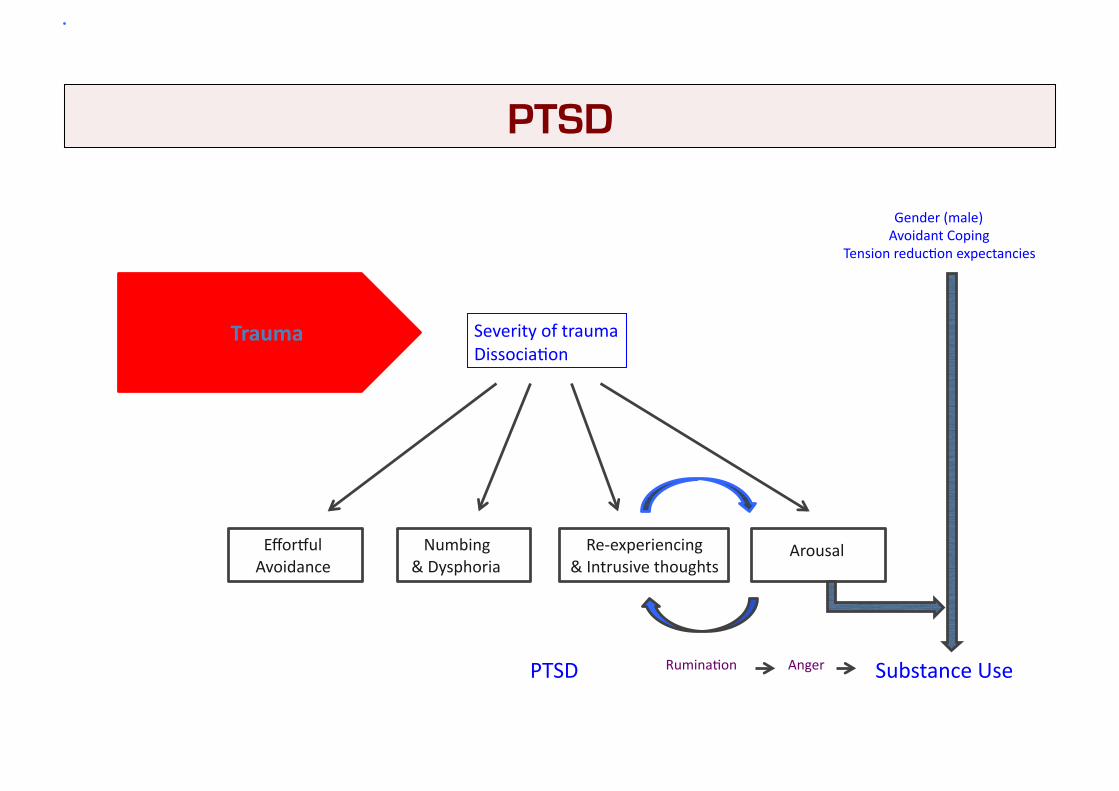
Trauma Severity of trauma Dissocia7on
Efforqul Avoidance
Re-‐experiencing & Intrusive thoughts
Numbing & Dysphoria
Arousal
Substance Use
Gender (male) Avoidant Coping
Tension reduc7on expectancies
Rumina7on Anger PTSD
PTSD