339: prediction of outcome in twin pregnancy with first and second trimester ultrasound
TRANSCRIPT

338 Cervical length in asymptomatic twin pregnancies:prospective multicenter comparison of predictive indicatorsChristophe Vayssiere1, Christine Leveque2, Romain Favre3,Francois Audibert4, Marie-Pierre Chauvet5, FrancoiseMaillard6, Virginie Ehlinger7, Catherine Arnaud8
1CHU Toulouse and INSERM U1027 (Research Unit on PerinatalEpidemiology, Child Health and Development) Toulouse III Paul SabatierUniversity, Obstetrics and Gynecology, Toulouse, France, 2Hpital Paule deViguier CHU Toulouse, Obstetrics and Gynecology, Toulouse, France,3Centre Medico Chirurgical et Obstetrical, Obstetrics and Gynecology,Schiltigheim, France, 4University of Montreal, Obstetrics and Gynecology,Montreal, QC, Canada, 5CHRU Jeanne de Flandre, Obstetrics andGynecology, Lille, France, 6INSERM U953, Research Unit on Perinatal andWomen’s Health, Paris, France, 7UMR INSERM U1027, Research Unit onPerinatal Epidemiology, Child Health and Development, Toulouse, France,8UMR INSERM U1027, esearch Unit on Perinatal Epidemiology,Child Health and Development, Toulouse, FranceOBJECTIVE: To determine whether cervical shortening between 22 and27 weeks of gestation predicts spontaneous preterm delivery before 34weeks better than a single cervical length (CL) measurement at 22 or27 weeks in asymptomatic twins.STUDY DESIGN: Prospective 13-center study over a 2-year-period re-analysed. CL was measured in 120 consecutive asymptomatic twinpregnancies during their routine ultrasound examination at 22 (21-23) and 27 (26-28) weeks. The results of these measurements wereneither communicated to the patients nor used for their management.The area under the ROC curve was calculated for CL at 22 weeks, CLat 27 weeks, the percentage of cervical shortening between 22 and 27weeks, and the cutoff point providing the best diagnostic perfor-mance, sensitivity and specificity for predicting spontaneous delivery�34 weeks was defined for each. Sensitivity, specificity, positive andnegative likelihood ratios (LR� and LR�) were then calculated withtheir 95% confidence intervals.RESULTS: The study included 120 patients; four were excluded fromthe analysis because of medically indicated delivery before 34 weeks.Of the 116 women, 13 gave birth before 34 weeks (11.2%). The areasunder the ROC curve were 0.67 for CL at 22 weeks, 0.75 for CL at 27weeks, and 0.57 for the change in CL from 22 to 27 weeks. The threeROC curves obtained differed significantly at the 0.05 level (p-value�0.027). Nonetheless, the ad hoc tests performed do not show a signif-icant difference between the ROC curves compared pairwise. The bestcutoff points were CL �35 mm at 22 weeks, CL �25 mm at 27 weeks,and cervical shortening of 20%. For equal sensitivity values (53.9%)for each, specificity for a CL �25 mm at 27 weeks was 87.5 (95% CI:81-94), significantly better than for the other indicators.CONCLUSION: The predictive performance of the cervical shorteningdoes not differ from that of the measurement at either 22 or 27 weeks.However, because of its high specificity, CL �25 mm at 27 weeksappeared to be the most useful indicator for predicting preterm de-livery before 34 weeks in this population.
339 Prediction of outcome in twin pregnancywith first and second trimester ultrasoundClare O’Connor1, Fionnuala Mc Auliffe2, Fionnuala Breathnach3,Michael Geary4, Sean Daly5, John Higgins6, James Dornan7, JohnJ. Morrison8, Gerry Burke9, Shane Higgins10, Patrick Dicker11,Fiona Manning3, Rhona Mahony12, Feargal Malone13
1The Coombe Women and Infants University Hospital, School of Medicine &Medical Science UCD Centre For Human Reproduction, Dublin, Ireland,2National Maternity Hospital, UCD School of Medicine and Medical Science,University College Dublin, Dublin, Ireland, 3Royal College of Surgeons inIreland, Obstetrics and Gynaecology, Dublin, Ireland, 4Rotunda Hospital,Obstetrics and Gynaecology, Dublin, Ireland, 5The Coombe Women andInfants University Hospital, UCD School of Medicine and Medical Science,University College Dublin, Dublin, Ireland, 6Cork University MaternityHospital, Obstetrics, Cork, Ireland, 7Royal Victoria Maternity Hospital,Obstetrics, Belfast, United Kingdom, 8National University of Ireland,Obstetrics & Gynaecology, Galway, Ireland, 9Midwestern Regional MaternityHospital, Obstetrics, Limerick, Ireland, 10National Maternity Hospital,Obstetrics and Gynaecology, Dubin, Ireland, 11Royal College Of Surgeons inIreland, Epidemiology and Public Health, Dublin, Ireland, 12UCD Obstetricsand Gynaecology, School of Medicine and Medical Science, Dublin, Ireland,13Royal College of Surgeons of Ireland, Obstetrics, Dublin, IrelandOBJECTIVE: To establish if first or second trimester biometry (11�0 to21�6 weeks) is a useful adjunct in the prediction of adverse perinataloutcomes in twin pregnancy.STUDY DESIGN: A consecutive cohort of 1028 unselected twin pregnan-cies were enrolled for the Evaluation of Sonographic Predictors ofRestricted growth in Twins (ESPRiT) study, a multicenter prospectivestudy conducted at 8 academic perinatal centers in Ireland. Outcomedata was recorded for 1001 twin pairs that completed the study {200monochorionic (MC) and 801 dichorionic (DC)}. Biometric param-eters obtained between 11 and 22 weeks were evaluated as predictorsof a composite of adverse perinatal outcomes (CO). These includedmortality, hypoxic ischemic encephalopathy, periventricular leu-komalacia, necrotizing enterocolitis, respiratory distress and sepsis.Preterm delivery (PTD) and birthweight discordance greater than18% (18% BW) were also investigated. Outcomes were adjusted forchorionicity and gestational age using Cox Proportional Hazards re-gression.RESULTS: Differences in CRL of 10% or 20% were not predictive ofadverse perinatal outcome in either DC or MC twins. Between 14 and22 weeks, an abdominal circumference (AC) difference of more than10% was the most useful predictor for adverse perinatal outcome,PTD and 18% or more BW discordance in both DC and MC twins.The strongest correlation was observed for biometry obtained be-tween 18 and 22 weeks (Table).CONCLUSION: While first trimester biometry was not useful for pre-dicting adverse outcome, biometry in the early second trimester cansuccessfully identify twin pregnancies at increased risk of poor peri-natal outcome. Intertwin AC difference of greater than 10% between14 and 22 weeks gestation was the best individual predictor of perina-tal risk in both monochorionic and dichorionic twins. Sonographicbiometry in the early second trimester should therefore be utilized toestablish perinatal risk, thus allowing prenatal care to be tailored ac-cordingly.
www.AJOG.org Diabetes, Labor, Medical-Surgical-Disease, Obstetric Quality & Safety, Prematurity, Ultrasound-Imaging Poster Session II
Supplement to JANUARY 2012 American Journal of Obstetrics & Gynecology S159
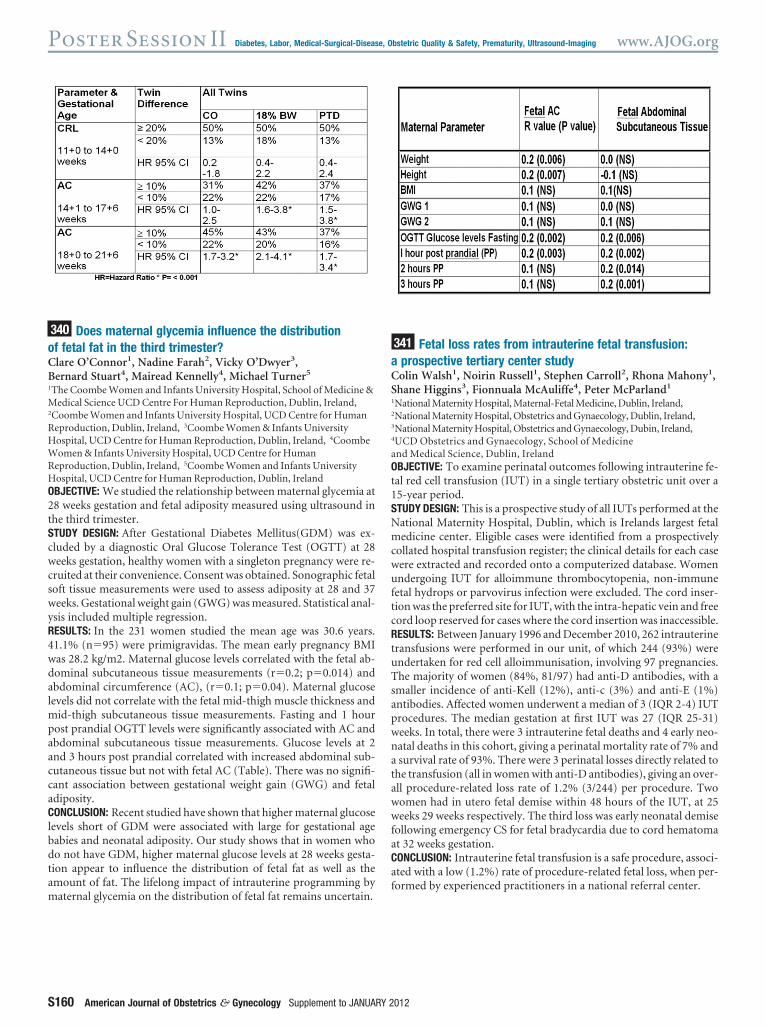
340 Does maternal glycemia influence the distributionof fetal fat in the third trimester?Clare O’Connor1, Nadine Farah2, Vicky O’Dwyer3,Bernard Stuart4, Mairead Kennelly4, Michael Turner5
1The Coombe Women and Infants University Hospital, School of Medicine &Medical Science UCD Centre For Human Reproduction, Dublin, Ireland,2Coombe Women and Infants University Hospital, UCD Centre for HumanReproduction, Dublin, Ireland, 3Coombe Women & Infants UniversityHospital, UCD Centre for Human Reproduction, Dublin, Ireland, 4CoombeWomen & Infants University Hospital, UCD Centre for HumanReproduction, Dublin, Ireland, 5Coombe Women and Infants UniversityHospital, UCD Centre for Human Reproduction, Dublin, IrelandOBJECTIVE: We studied the relationship between maternal glycemia at28 weeks gestation and fetal adiposity measured using ultrasound inthe third trimester.STUDY DESIGN: After Gestational Diabetes Mellitus(GDM) was ex-cluded by a diagnostic Oral Glucose Tolerance Test (OGTT) at 28weeks gestation, healthy women with a singleton pregnancy were re-cruited at their convenience. Consent was obtained. Sonographic fetalsoft tissue measurements were used to assess adiposity at 28 and 37weeks. Gestational weight gain (GWG) was measured. Statistical anal-ysis included multiple regression.RESULTS: In the 231 women studied the mean age was 30.6 years.41.1% (n�95) were primigravidas. The mean early pregnancy BMIwas 28.2 kg/m2. Maternal glucose levels correlated with the fetal ab-dominal subcutaneous tissue measurements (r�0.2; p�0.014) andabdominal circumference (AC), (r�0.1; p�0.04). Maternal glucoselevels did not correlate with the fetal mid-thigh muscle thickness andmid-thigh subcutaneous tissue measurements. Fasting and 1 hourpost prandial OGTT levels were significantly associated with AC andabdominal subcutaneous tissue measurements. Glucose levels at 2and 3 hours post prandial correlated with increased abdominal sub-cutaneous tissue but not with fetal AC (Table). There was no signifi-cant association between gestational weight gain (GWG) and fetaladiposity.CONCLUSION: Recent studied have shown that higher maternal glucoselevels short of GDM were associated with large for gestational agebabies and neonatal adiposity. Our study shows that in women whodo not have GDM, higher maternal glucose levels at 28 weeks gesta-tion appear to influence the distribution of fetal fat as well as theamount of fat. The lifelong impact of intrauterine programming bymaternal glycemia on the distribution of fetal fat remains uncertain.
341 Fetal loss rates from intrauterine fetal transfusion:a prospective tertiary center studyColin Walsh1, Noirin Russell1, Stephen Carroll2, Rhona Mahony1,Shane Higgins3, Fionnuala McAuliffe4, Peter McParland1
1National Maternity Hospital, Maternal-Fetal Medicine, Dublin, Ireland,2National Maternity Hospital, Obstetrics and Gynaecology, Dublin, Ireland,3National Maternity Hospital, Obstetrics and Gynaecology, Dubin, Ireland,4UCD Obstetrics and Gynaecology, School of Medicineand Medical Science, Dublin, IrelandOBJECTIVE: To examine perinatal outcomes following intrauterine fe-tal red cell transfusion (IUT) in a single tertiary obstetric unit over a15-year period.STUDY DESIGN: This is a prospective study of all IUTs performed at theNational Maternity Hospital, Dublin, which is Irelands largest fetalmedicine center. Eligible cases were identified from a prospectivelycollated hospital transfusion register; the clinical details for each casewere extracted and recorded onto a computerized database. Womenundergoing IUT for alloimmune thrombocytopenia, non-immunefetal hydrops or parvovirus infection were excluded. The cord inser-tion was the preferred site for IUT, with the intra-hepatic vein and freecord loop reserved for cases where the cord insertion was inaccessible.RESULTS: Between January 1996 and December 2010, 262 intrauterinetransfusions were performed in our unit, of which 244 (93%) wereundertaken for red cell alloimmunisation, involving 97 pregnancies.The majority of women (84%, 81/97) had anti-D antibodies, with asmaller incidence of anti-Kell (12%), anti-c (3%) and anti-E (1%)antibodies. Affected women underwent a median of 3 (IQR 2-4) IUTprocedures. The median gestation at first IUT was 27 (IQR 25-31)weeks. In total, there were 3 intrauterine fetal deaths and 4 early neo-natal deaths in this cohort, giving a perinatal mortality rate of 7% anda survival rate of 93%. There were 3 perinatal losses directly related tothe transfusion (all in women with anti-D antibodies), giving an over-all procedure-related loss rate of 1.2% (3/244) per procedure. Twowomen had in utero fetal demise within 48 hours of the IUT, at 25weeks 29 weeks respectively. The third loss was early neonatal demisefollowing emergency CS for fetal bradycardia due to cord hematomaat 32 weeks gestation.CONCLUSION: Intrauterine fetal transfusion is a safe procedure, associ-ated with a low (1.2%) rate of procedure-related fetal loss, when per-formed by experienced practitioners in a national referral center.
Poster Session II Diabetes, Labor, Medical-Surgical-Disease, Obstetric Quality & Safety, Prematurity, Ultrasound-Imaging www.AJOG.org
S160 American Journal of Obstetrics & Gynecology Supplement to JANUARY 2012