2015 women's health conference presentations
DESCRIPTION
ÂTRANSCRIPT
Public Funding for Fer0lity Dr Olivia Stuart Fer.lity Specialist

Initial Fertility Consultation
Fer.lity specialist • Public • Private

Private consultation option
• Pa.ents can self refer • Pa.ents can choose their fer.lity specialist • No mandatory tests required pre-‐referral • Fer.lity Associates’ specialists can see new pa.ents within 2 weeks in all our clinics
• consulta.on, scan, organise all their tests, assessed for public treatment, nurse

Public consultation • Condi.ons apply • Referring doctor needs to do a preliminary workup • Wait .me 3-‐4 months • Randomly allocated to one of 3 Auckland units, no choice


Eligibility criteria for public consultation
NZ residency Both partners must have • NZ residency, citizenship or • Work visa showing at > 2 years

Additional criteria for initial consultation

Work-up tests for initial consultation
Female Male
Day 2-3 FSH Oestradiol Semen analysis
Hepatitis B,C HIV syphilis rubella
Hepatitis B,C HIV
Blood Group FBC
Smear
Day 21 Progesterone

Publicly funded treatment
• Clinical Priority Access Criteria (CPAC) form • Criteria are the same across New Zealand • People need > 65 points using the fer.lity CPAC scoring tool • Score > 65 means eligible • All have same wait .me .l treatment
• The CPAC score can only be calculated by a fer5lity specialist.

> 65
CPAC Form
6

100
10
10 1
50
30
20
Couple A – Unexplained Infertility
6

80
10
10 1
40
30
10
Couple B – Male vasectomy
6

70
10
10 1
20
30
20
Couple C – Same sex couple
6

Waitlist for treatment
• The wait to treatment varies across the country • Generally 12–18 months • Pa.ents can access private fer.lity treatment whilst on the public wai.ng list

Second publicly funded packages
• Requires rescoring • All same eligibility criteria apply • S.ll need CPAC score > 65 • wait .me less • Same unit

Treatment pathways to having a baby…

Couple Start Trying
See GP
First Appointment Public ($0)
Laparoscopy Public ($0)
Follow Up Public ($0) Need IVF
Funded Appointment FA ($0)
Funded IVF ($0)
12 Months 3 Months
6 Weeks
6 Weeks
6 Months
12 Months
• Do everything Publicly Funded • Total Cost $0 • Total Time from GP to IVF – 24 months
All public…

Couple Start Trying
See GP
First Appointment FA ($270)
Laparoscopy Public ($0)
Funded IVF ($0)
Follow Up Private ($165) Need IVF
12 Months
6 Months
2 Weeks
2 Weeks
12 Months
• 1st Appointment in Private then Lap and IVF Public • Total Cost $435 • Total Time GP to IVF – 19 Months
Public and private 1…

Couple Start Trying
See GP
First Appointment FA ($270)
Laparoscopy Public ($0)
Follow Up Private ($165) Need IVF
Private IVF ($10,000)
12 Months
6 Months
2 Weeks
4 weeks
2 Weeks
• 1st Appointment in Private then Lap in Public and IVF Private
• Total Cost $10435 • Total Time GP to IVF – 8 Months
Public and private 2…

Couple Start Trying
See GP
First Appointment FA ($270)
Laparoscopy Private (?Insurance)
Follow Up Private ($165) Need IVF
Private IVF ($10,000)
12 Months
2 Weeks 2 Weeks
4 weeks
2 Weeks
• 1st Appointment in Private then Lap and IVF Private • Total Cost $10435 +/-‐ Lap cost (insurance) • Total Time GP to IVF – 10 weeks
All private…

On the horizon…
• Male smokers • Unexplained infer.lity for > 3 years in > 36 year old women
• BMI < 36

Ques0ons?

Infertility Diagnosis
When to refer? What’s New?
Dr Simon Kelly
Medical Director
Fertility Associates, Auckland

Look how far we have come?
The amazing story of IVF: 37 years
and 5 million babies later!

Infertility
Male
30%
Female
30%
Unexplained
25%
Combined
10%
Other
5%
• 1 in 7 couples
• Age single most important factor


When to refer?
• Trying for 12 months
• Ask about contraception

Infertility: (n)
A medical condition that diminishes self-esteem,
your social life as well as your checking and savings
accounts. Causes sudden urges to pee on sticks,
cry,scream and a fear of pregnancy announcements.
Treated by a Medical Specialist who you pay to
knock you up-this does not always work
Affects about 1 in 10 couples
Who to refer?
• Consider early referral if:
• >35yrs
• Irregular or absent periods
• Medical or surgical conditions that may affect fertility
eg endometriosis/pelvic surgery/chemo or radiotherapy
• Family history early menopause
• Recurrent miscarriage
• Genetic conditions amenable to PGD
• Patient Request

Free Nurse Consult - available for your patients
• 15 minute phone consult with a fertility nurse
• Answers questions like: • When to seek help • Treatment options • Costs • Public funding • Their % chance of having a baby
• Chinese speaking Free Nurse Consult now
available

Investigations • Male
• Semen Analysis
• Hep B/C/HIV
• Female
• FSH/Estradiol day 2-4cycle
• Thyroid function
• Rubella status/ Hep B/C HIV
• Prolactin if irreg cycles/galactorhoea
• HSG or HYCOSY if suspect tubal disease or previous PID*
• Ultrasound*
• AMH*
• Chlamydia swabs
• Check smear current

Advice- Improving Fertility
•Start Folic Acid and Iodine
•Minimize alcohol
•Reduce caffeine consumption
•Stop smoking
•Maintain ideal BMI (20-25)
•Improve diet
•Exercise
•Reduce Stress

New Diagnostic Tools
• AMH
– Currently best measure of ovarian reserve
– produced by small follicles as they grow on ovary
• Sperm DNA Fragmentation Testing


AMH

Sperm DNA Fragmentation Testing
• High levels DNA fragmentation may be
associated with:
– Poor fertility outcome
– miscarriage
• Causal Factors:
– Environmental / pollution exposure
– Advanced age
– Varicocoele
– Drug use
– Smoking
– Chronic Disease
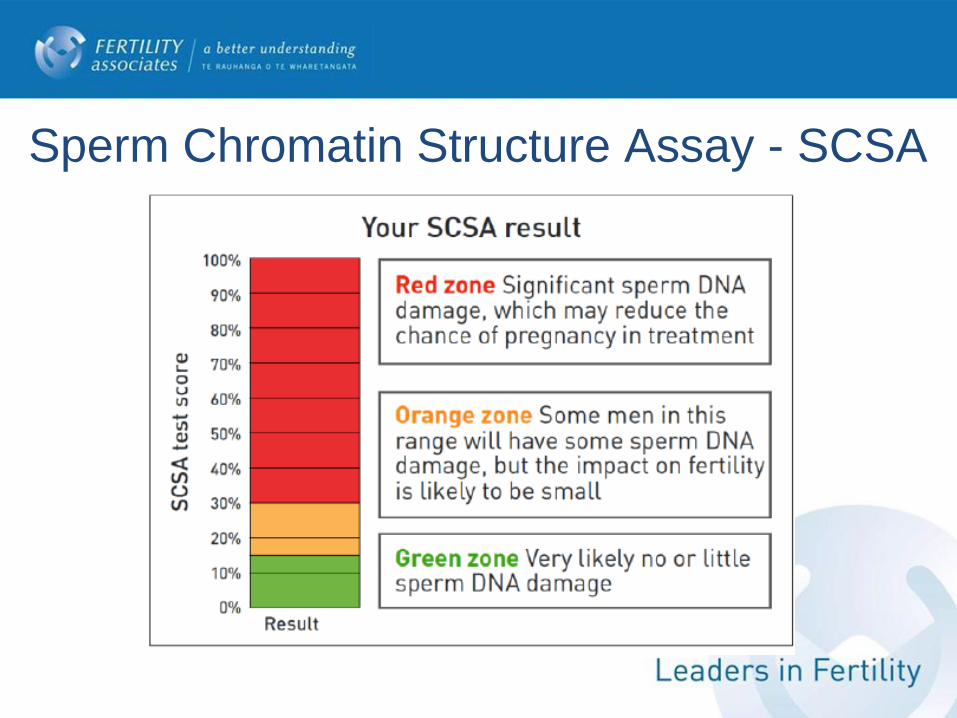
Sperm Chromatin Structure Assay - SCSA
Sperm DNA Fragmentation
How do we treat?
-Antioxidants
-IMSI
-Surgical sperm
retrieval

Technologies
Matthew (Tex) VerMilyea, PhD, HCLD/CC Scientific Director

How to Choose the Best Embryo for Transfer?² Observational Analysis: Embryo Development Morphology Assessment
² Genomic Analysis: Trophectoderm Cell Biopsy
² Transcriptomic / Metabolomic Analysis:
Granulosa cells Cumulus cells Culture medium
TimeLapse Morphometry Imaging
TiMI Embryo Development
One frame at a time




t2: division to 2-cells t3: division to 3-cells t4: division to 4-cells t5: division to 5-cells t8: division to 8-cells
cc1: duration of first cell cycle (cc1 = t2-t1) cc2: duration of second cell cycle (cc2 = t3-t2) cc3: duration of third cell cycle (cc3 = t5-t3) s2: duration of transition from two-blastomere embryo to four-blastomere (s2 = t4-t3) s3: duration of transition from five-blastomere embryo to eight-blastomere (s3 = t8-t5)
Photos courtesy of Matthew (Tex) VerMilyea, PhD, HCLD/CCAdapted from Meseguer et al., 2011
1-cell 2-cells 4-cells 8-cells
t3 t2 t5 t4
cc1 cc2 cc3
t8
s2 s3
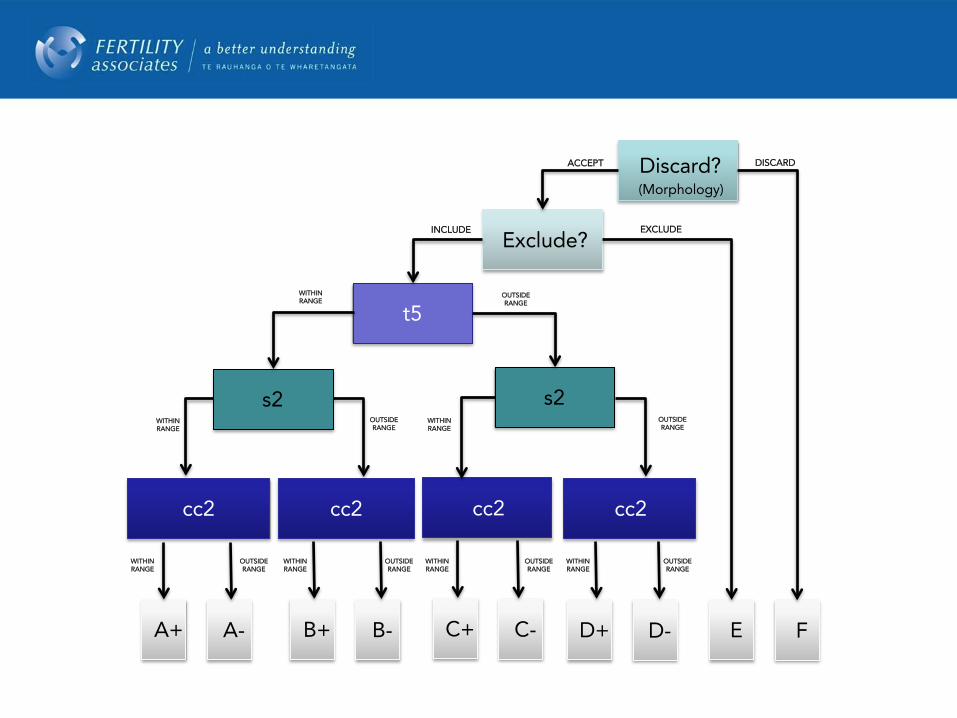
Discard?(Morphology)
Exclude?
t5
s2s2
cc2 cc2 cc2cc2
A+ A- C+ C-B+ B- D+ D- E F
ACCEPT DISCARD
INCLUDE EXCLUDE
WITHINRANGE
OUTSIDE RANGE
WITHINRANGE
OUTSIDE RANGE
WITHINRANGE
OUTSIDE RANGE
WITHINRANGE
OUTSIDE RANGE
WITHINRANGE
OUTSIDE RANGE
WITHINRANGE
WITHINRANGE
OUTSIDE RANGE
OUTSIDE RANGE

Clinical validation of embryo cultureand selection by morphokineticanalysis: a randomized, controlledtrial of the EmbryoScopeIrene Rubio, Ph.D.,a Arancha Gal!an, Ph.D.,a Zaloa Larreategui, Ph.D.,b Fernando Ayerdi, Ph.D.,b
Jose Bellver, M.D.,a Javier Herrero, Ph.D.,a and Marcos Meseguer, Ph.D.a
a Instituto Universitario IVI Valencia, University of Valencia, Valencia; and b IVI Bilbao, Bilbao, Spain
Objective: To determine whether incubation in the integrated EmbryoScope time-lapse monitoring system (TMS) and selectionsupported by the use of a multivariable morphokinetic model improve reproductive outcomes in comparison with incubation in astandard incubator (SI) embryo culture and selection based exclusively on morphology.Design: Prospective, randomized, double-blinded, controlled study.Setting: University-affiliated private in vitro fertilization (IVF) clinic.Patient(s): Eight hundred forty-three infertile couples undergoing intracytoplasmic sperm injection (ICSI).Intervention(s): No patient intervention; embryos cultured in SI with development evaluated only by morphology (control group) andembryos cultured in TMS with embryo selection was based on a multivariable model (study group).Main Outcome Measure(s): Rates of embryo implantation, pregnancy, ongoing pregnancy (OPR), and early pregnancy loss.Result(s): Analyzing per treated cycle, the ongoing pregnancy rate was statistically significantly increased 51.4% (95% CI, 46.7–56.0)for the TMS group compared with 41.7% (95% CI, 36.9–46.5) for the SI group. For pregnancy rate, differences were not statisticallysignificant at 61.6% (95% CI, 56.9–66.0) versus 56.3% (95% CI, 51.4–61.0). The results per transfer were similar: statisticallysignificant differences in ongoing pregnancy rate of 54.5% (95% CI, 49.6–59.2) versus 45.3% (95% CI, 40.3–50.4) and notstatistically significant for pregnancy rate at 65.2% (95% CI, 60.6–69.8) versus 61.1% (95% CI, 56.2–66.1). Early pregnancy losswas statistically significantly decreased for the TMS group with 16.6% (95% CI, 12.6–21.4) versus 25.8% (95% CI, 20.6–31.9). Theimplantation rate was statistically significantly increased at 44.9% (95% CI, 41.4–48.4) versus 37.1% (95% CI, 33.6–40.7).Conclusion(s): The strategy of culturing and selecting embryos in the integrated EmbryoScope time-lapse monitoring system improvesreproductive outcomes.Clinical Trial Registration Number: NCT01549262. (Fertil Steril! 2014;102:1287–94. "2014by American Society for Reproductive Medicine.)Key Words: Early pregnancy loss, embryo culture, embryo selection, implantation, ongoingpregnancy rate, time-lapse
Discuss: You can discuss this article with its authors and with other ASRM members at http://fertstertforum.com/rubioi-embryo-culture-selection-morphokinetic-analysis/
Use your smartphoneto scan this QR codeand connect to thediscussion forum forthis article now.*
* Download a free QR code scanner by searching for “QRscanner” in your smartphone’s app store or app marketplace.
I n recent years, clinical practice ef-forts have been directed towardimproving embryo selection. The
identification of embryos with a highercapacity for implantation means wecan reduce the number of embryos for
transfer without reducing the chancesof pregnancy in a cycle of assistedreproduction. To this end, differentnoninvasive embryo selection methodshave been designed that provide infor-mation on how to distinguish embryoswith better prognosis (1) There aredifferent methods of embryo gradation(2), but they are all based onmorphology, and evaluation ofmorphology under microscope is sub-ject to observer subjectivity (1). One ofthe noninvasive embryo evaluationmethods to have come into the lime-light in recent years is the time-lapse
Received January 17, 2014; revised and accepted July 9, 2014; published online September 11, 2014.I.R. has nothing to disclose. A.G. has nothing to disclose. Z.L. has nothing to disclose. F.A. has nothing
to disclose. J.B. has nothing to disclose. J.H. has nothing to disclose. M.M. has received paymentfor lectures from Ferring and Merck Serono.
The instrumentation, disposables, and utensils used in this study were fully paid for by IVI. IVI is aminor shareholder in UnisenseFertiliTech A/S, but none of the authors have any economicaffiliation with UnisenseFertiliTech A/S.
Reprint requests: Marcos Meseguer, Ph.D., Instituto Valenciano de Infertilidad, Plaza de la PolicíaLocal, 3, Valencia 46015, Spain (E-mail: [email protected]).
Fertility and Sterility® Vol. 102, No. 5, November 2014 0015-0282/$36.00Copyright ©2014 The Authors. Published by Elsevier Inc. on behalf of the American Society for Repro-
ductive Medicine. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/3.0/).
http://dx.doi.org/10.1016/j.fertnstert.2014.07.738
VOL. 102 NO. 5 / NOVEMBER 2014 1287
ORIGINAL ARTICLES: ASSISTED REPRODUCTION
• Time-Lapse and multivariable morphokinetic classification tree improves outcomes compared to standard incubators and traditional morphology assessment.
• Ongoing pregnancy rate increased from 41.7% to 51.4% (95% CI P-value .005)
• Early pregnancy loss decreased from 25.8% to 16.6% (95% CI P-value .01)
• Implantation rate increased from 37.1% to 44.9% (95% CI P-value .02)


ARTICLE
Computer-automated time-lapse analysisresults correlate with embryo implantationand clinical pregnancy: A blinded, multi-centre study
Matthew D VerMilyea a, Lei Tan b, Joshua T Anthony a, Joe Conaghan c,Kristen Ivani d, Marina Gvakharia e, Robert Boostanfar f, Valerie L Baker g,Vaishali Suraj b, Alice A Chen b, Monica Mainigi a, Christos Coutifaris a,Shehua Shen b,*
a Penn Fertility Care, University of Pennsylvania, 3701 Market St. Suite #800, Philadelphia, PA 19104, USA; b Auxogyn, Inc,1490 O’Brien Drive, Suite A, Menlo Park, CA 94025, USA; c Pacific Fertility Center, 55 Francisco Street, Fifth Floor, SanFrancisco, CA 94133, USA; d Reproductive Science Center of the Bay Area, 3160 Crow Canyon Road, San Ramon, CA 94583,USA; e Palo Alto Medical Foundation Fertility, Fertility Physicians of Northern California, 2581 Samaritan Drive, San Jose,CA 95124, USA; f HRC Fertility, 15503 Ventura Blvd, Suite 200, Encino, CA 91436, USA; g Stanford Fertility & ReproductiveMedicine Center, 900 Welch Road, Suite 350, Palo Alto, CA 94304, USA* Corresponding author. E-mail address: [email protected] (S Shen).
Matthew VerMilyea, PhD, HCLD, is Director of Assisted Reproductive Technologies and Andrology Laboratoriesat the University of Pennsylvania, USA, and Scientific Director of Fertility Associates, New Zealand. He gradu-ated from Cornell University, and received training in human embryology at Shady Grove Fertility, USA. Hethen obtained his PhD in Epigenetics from the University of Birmingham, UK. Matthew received a postdoctoralfellowship from the Japanese Society for the Promotion of Science for mammalian molecular embryologyresearch at the RIKEN Institute, Kobe. Research interests include non-invasive and uninterrupted embryoculture protocols, time-lapse video imagery, micro-environment culture settings and early embryo histonemodifications.
Abstract Computer-automated time-lapse analysis has been shown to improve embryo selection by providing quantitative and ob-jective information to supplement traditional morphology. In this multi-centre study, the relationship between such computer-derived outputs (High, Medium, Low scores), embryo implantation and clinical pregnancy were examined. Data were collected fromsix clinics, including 205 patients whose embryos were imaged by the EevaTM System. The Eeva scores were blinded and not consid-ered during embryo selection. Embryos with High and Medium scores had significantly higher implantation rates than those withLow scores (37% and 35% versus 15%; P < 0.0001; P = 0.0004). Similar trends in implantation rates were observed in different IVFcentres each using their own protocols. Further analysis revealed that patients with at least one High embryo transferred had sig-nificantly higher clinical pregnancy rates than those with only Low embryos transferred (51% versus 34%; P = 0.02), although pa-tients’ clinical characteristics across groups were comparable. These data, together with previous research and clinical studies, confirm
http://dx.doi.org/10.1016/j.rbmo.2014.09.0051472-6483/© 2014 Reproductive Healthcare Ltd. Published by Elsevier Ltd. All rights reserved.
Reproductive BioMedicine Online (2014) 29, 729–736
www.sciencedirect .comwww.rbmonl ine.com
37%(41/111)
23%(50/220)
0%
10%
20%
30%
40%
High Low
p = 0.003
Known Implantation
Eeva High
Eeva Low
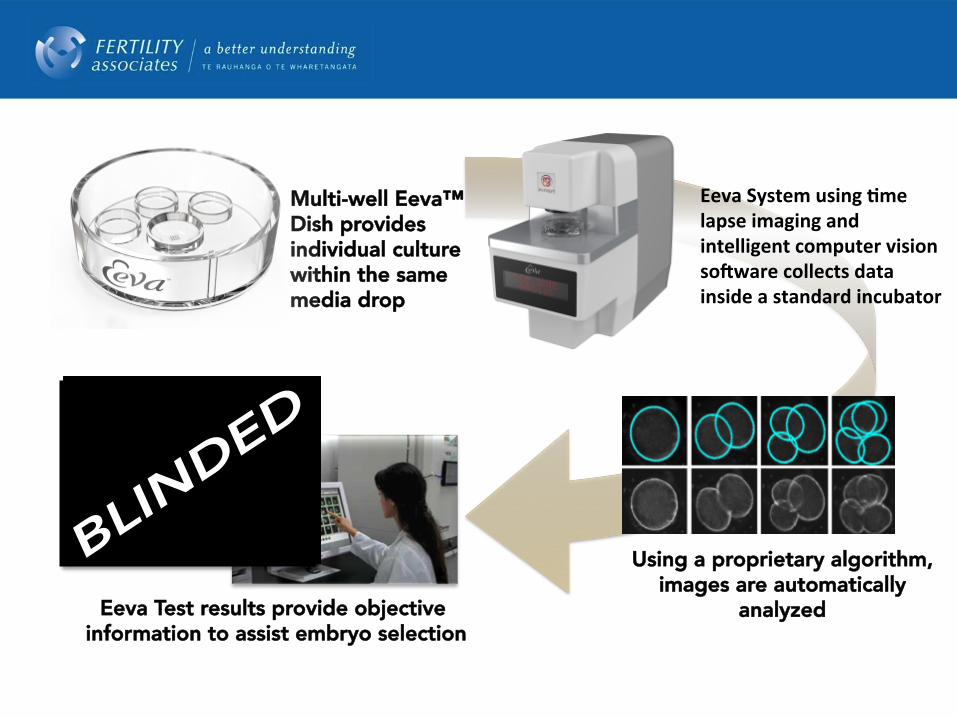
Using a proprietary algorithm, images are automatically
analyzed
Multi-well Eeva™ Dish provides individual culture within the same media drop
Eeva System using /me lapse imaging and intelligent computer vision so6ware collects data inside a standard incubator
Eeva Test results provide objective information to assist embryo selection

PICSI & IMSIChoosing the best sperm
ICSI with PICSI• Washed sperm are tested to see what
proportion bind to a glass microscope slide covered with HA.
• If it is less than 65%, then washed sperm are added to a special Petri dish (PICSI dish) which contains a spot of HA.
• Sperm bound to the HA spot are removed and selected for use with ICSI.
Mature sperm bind to a substance called hyaluronic acid (HA) as they make their way through the cells protecting the egg in the human Fallopian tube. This is one of several mechanisms the body is known to use to select a good sperm to fertilise the egg.
PICSI may improve pregnancy rates and reduce the miscarriage rate. PICSI is suitable for:• Men having ICSI with at least
1 million sperm/ml in their ejaculate.• Men who have less than 65% HA
binding in the test (approximately 15% of men will be affected).
There are several ways to ensure that you are getting the best chance of pregnancy in IVF treatment. This fact sheet summarises the techniques available to help sperm selection in IVF-related treatment.
How to Choose the Best Sperm for Fertilisation?
• Conventional IVF: ~100,000 sperm added to each egg
• ICSI : Poor movement, number and shape
WHO ‘Normal Range’
Semen Volume 1.5 ml or more
Sperm Concentration 15 million /ml or more
Proportion of sperm motile 40% or more
Proportion with progressive motility
32% or more
Proportion of sperm with normal shape, using strict criteria
4% or more

Conventional In-Vitro Fertilisation

Intracytoplasmic Sperm Injection (ICSI)

Intracytoplasmic Morphologically selected Sperm Injection (IMSI)
x100 Magnification x600-6,000 Magnification
Intracytoplasmic Sperm Injection (ICSI)

embryos at the blastocyst stage were transferred into theuterus on day 5 by the TDT catheter set (CCD, Neuilly,France); if blastocysts did not develop, one or two morulawere transfered, whereas lower-cell embryos were nottransfered. Biochemical pregnancy was confirmed by thepositive serum b-hCG test (> 48 mIU/ml) 15 days afterthe embryo transfer, and clinical pregnancy by an ultra-sound scan of the gestational sac and the embryo heartbeats 14 days after the positive b-hCG test.
StatisticsTo evaluate the role of sperm selection by their morphol-ogy, the laboratory and clinical outcomes between theIMSI and ICSI groups of couples were compared. The
SPSS (Statistical Package for the Social Science; SPSS Inc.,Chicago, IL, USA) statistical program for MicrosoftWindows was used for statistical calculations. The labora-tory outcomes were expressed as fertilization rate (numberof fertilized oocytes per injected oocytes), number of blas-tocysts (%), number of blaststocysts per cycle, and numberof cycles with at least one blastocyst (%). The clinical out-comes were expressed as implantation rate (number ofimplanted embryos per transferred embryos), number ofpregnancies, pregnancy rate per cycle, and number ofspontanous abortions. For comparing categorical data, thechi-square (c2) test was performed, and Spearman’s rankcorrelation coefficient was used as a non-parametric mea-sure of statistical dependence between the two variables.
Figure 1 Classification of spermatozoa selected at 6,000 × magnification into 3 different categories. Class I - spermatozoa of goodquality, Class II - spermatozoa of worse quality, and Class III - spermatozoa of poor quality. Legend: a,b,c - spermatozoa of Class I; d,e,f -spermatozoa of Class II; g,h,i - spermatozoa of Class III.
Knez et al. Reproductive Biology and Endocrinology 2011, 9:123http://www.rbej.com/content/9/1/123
Page 4 of 8
• Sperm do not have efficient DNA repair mechanisms.
• Round vacuoles identified in sperm heads are associated with DNA fragmentation.
• DNA damage caused by Reactive Oxygen Species (ROS) can be associated with age, temp, varicocele, smoking, diet, environmental toxins.
• No implantation after >4 embryos transferred.
• Poor embryo development from Day3.
• Recurrent miscarriage from natural miscarriage.

• Intracytoplasmic Morphologically selected Sperm Injection (IMSI) by Ultra-high magnification selection is available and can improve reproductive outcomes.
• Fertility Associates is committed to providing the latest technology to our patients.
• Time Lapse Morphometry Imaging (TiMI) service now available at FA which provides an uninterrupted growth environment and detailed assessment of embryological milestones.

Technologies
Matthew (Tex) VerMilyea, PhD, HCLD/CC Scientific Director
One Healthy Baby at a Time.

Thanks for the opportunity!

Fertility Preservation By Dr Mary Birdsall
Chair, Fertility Associates
Freezing Sperm
•60 years ago first human pregnancy from frozen sperm
•60 years ago first sperm bank
•Able to freeze low numbers
•Use insemination or ICSI

Who Should Freeze Sperm?
•Chemotherapy or radiotherapy or experimental medications
•Surgery eg prostatectomy or major pelvic surgery or orchidectomy
•Pre vasectomy or geographical challenges
•Pre gender reassignment surgery
•Sperm donors
•Klinefelters 47 XXY

Heterosexual couples Single women Lesbian couples
Donor Sperm




Freezing testicular sperm
• Unable to ejaculate
• Spinal injury
• Vasectomy
• Congenital bilateral absence of vas
• Azospermia
• Testicular cancer

Should young men freeze sperm for later?
•Sperm quality reduces with age
• Increase in schizophrenia, autism, achondroplasia with increasing paternal age


Prepubertal boys and fertility preservation
•No mature spermatogenesis
•Testicular tissue currently not being frozen
•No proven method to transform immature germ cells into functional sperm
• In mice: germ cell extraction, cryopreservation and re-injection with recovery of fertility

Spermatogenesis

Funding and the Law
•Pre cancer treatment sperm may be frozen free of charge
•Usual criteria for public funding for partners apply (woman less than 40, non smoker, BMI 19 to 32)
•May be stored for 10 years then must be discarded unless application for extension for storage made to ECART

Women

AMH

Embryo Freezing
•First pregnancy - 1983
•Slow cooling
•Vitrification
•Need consent from both parties to thaw and use
•Who freezes embryos ?: surplus from IVF, pre chemo if have a partner and time, social, reduced ovarian reserve

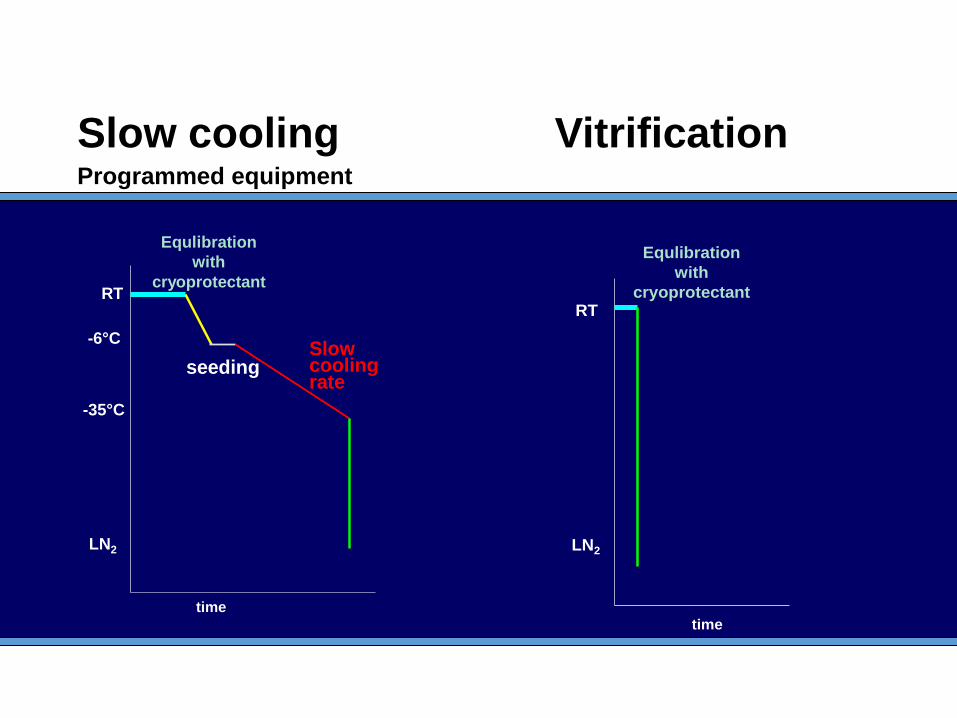
RT
-6°C
-35°C
LN2
Equlibration
with
cryoprotectant
seedingSlow cooling rate
time
Equlibration
with
cryoprotectantRT
LN2
time
Slow cooling Vitrification Programmed equipment

Vitrification 2013
• 262 warming cycles • 289 embryos warmed (1.1 per cycle) • 279 embryos survived (96%) • 258 embryo replacement cycles (98%) • 115 pregnancies (44%)

Perinatal outcomes in Fresh IVF
cycles vs Frozen cycles

Frozen vs Fresh: antepartum haemorrhage

Frozen vs Fresh: SGA

Frozen vs Fresh: perinatal mortality

Fetal Abnormalities Frozen vs Fresh
•Reproductive Technologies and the Risk of Birth Defects M Davies et al NEJM 2012 366 1803-13
•South Australia population cohort study of more than 327,000 births
•Birth defects 8.3% after IVF vs 5.8% in spontaneous OR 1.47 (CI 1.33-1.62)
•No increased risk seen in frozen embryos
Summary Fresh IVF vs Frozen
•Frozen embryo cycles appear to have fewer obstetric and perinatal complications compared with fresh IVF cycles
•Suggests that ovarian stimulation may have a detrimental impact ? on endometrium
•So are frozen embryo pregnancy cycles comparable to spontaneous pregnancies?

Singletons after frozen transfer vs singletons after spontaneous conception
Outcome FET pregnancies Overall effect (RR, 95% CI)
Caesarean section 2947 1.76 (1.65 - 1.87)
Birthweight <2500g 2947 1.27 (1.05 – 1.52)
Birthweight <1500g 2787 1.51 (1.01 – 2.27)
Delivery at < 37 weeks 2947 1.39 (1.20 – 1.61)
Delivery at < 32 weeks 2947 1.45 (0.98 - 2.13)

Egg Freezing
Fertility preservation: cancer, social, religious or ethical objections to embryo freezing, no sperm at IVF, rapid reduction of ovarian reserve
•Vitrification
•Not funded $10,000
•3000 babies



Ovarian Tissue Cryopreservation

Ovarian Tissue Cryopreservation
•Oncological fertility preservation
•Only option for pre-pubescent girls
• Laparoscopy required
•Malignant cells being re-implanted a concern
•32 babies in world
•HRT


Ovarian cryopreservation in NZ
•46 ovarian tissue samples stored
•Permission to store but not yet an approved procedure
•2 pregnancies in Australia


Summary
• Men: can freeze sperm or testicular tissue
• Prepubertal boys: no options
• Couples: can freeze embryos
• Women: can freeze eggs or ovarian tissue or embryos with donor sperm
• Prepubertal girls: can freeze ovarian tissue
Questions from the floor
Babies, bones and body fat percentage Why worry about hypothalamic
amenorrhea?
Dr Megan Ogilvie
The Endocrine Group
Fertility Associates

Outline • What is Hypothalamic Amenorrhea? • Nomenclature
– Female athlete triad – IOC consensus statement – REDs
• How to diagnose – PCOS vs HA
• Why should we worry? – Bone Density – Future Fertility
• What can we do? – Multidisciplinary approach – Timing

Too Fat Too Thin or Just Right?

Kisspeptins
Ovary
Pituitary
Estrogen
Leptin
GnRH
FSH, LH
Energy Deficit
(Weight/ fat mass loss,
reduced nutrition, exercise)
Stress
(Physical or psychological)
Hypothalamus

Hypothalamic Amenorrhoea
Suppressed gonadotropin levels/function due to: chronic energy deficit and/or psychological stress
Lawson EA and Klibanski A (2008) Endocrine abnormalities in anorexia nervosa


IOC consensus Statement: RED-S • Energy deficiency
– Balance between energy intake and expenditure
– No standard method for assessing energy availability
• Specific sports at high risk – Runners, cyclists, jockeys, ballet
• Possibly effects males (need more studies)
– Lowered BMD
– Multisystem presentation, can be subtle (Br J Sports Med 2014;48:289)

Relative Energy Deficiency in Sport (RED-S)
Mountjoy et al, Br J Sports Med 2014;48:491–497.

Anna Smith • 25 year old woman
• Secondary amenorrhea 9 months
• Regular periods prior
• What will you ask her:
– No acne, hirsutism
– Busy lawyer – 60 hour weeks
– Recent relationship break up
– 7 hours/ week at gym, low carb diet, gluten free
– BMI 21, 5 kg weight loss 1 year ago

Polycystic ovarian syndrome vs hypothalamic amenorrhea
PCOS
– Periods weight
– Androgen excess symptoms
– Test, PRL, normal E2
– USS – normal endometrium
HA
– Periods weight
– Lanugo hair
– E2, LH, FSH
– USS – thin endometrium
– Spinal osteopenia
Don’t forget a mixed picture Robin, 2012

Assessment (What to Ask) Take your time with history – often the most informative
Aim is early diagnosis and intervention
Current BMI and pattern of weight change
Period pattern with weight change
Menarchal weight
Eating and exercise patterns - specifics
What else is going on - ?psychological stressors

Assessment (What to Measure)
Weight, BMI, waist circumference
LH, FSH and estradiol levels – FSH 5.4 LH 1 E2 <150
Prolactin, testosterone, TSH, pituitary testing
Venous bicarbonate if concerned about purging
Pelvic USS – thin endometrium
Bone Mineral Density
?Pituitary MRI

Diagnosis o Clinical history
o Less periods with energy deficit
o Psychological stressors
o Personality type – Type A, goal orientated
o Investigations
o Normal prolactin, TSH, T
o Low LH and oestradiol
o Thin endometrium
o Relative spinal bone loss THINK – hypothalamic amenorrhea

Why Worry? • Serious end points without intervention:
– Clinical eating disorders
– Osteoporosis
– Infertility
• Physical and emotional well being
– Decreased physical performance, injury rate
– Decreased cognitive performance
• Endothelial dysfunction due to low oestrogen
• High cortisol levels, low IGF1, low T

Effects on Bone • 90% of peak bone mass attained by 18 years
• Advantage of weight bearing exercise on bone lost in amenorrheic athletes
• Relative spinal BMD loss often seen
• Continued amenorrhea – 2-3% loss
bone mass/year
• OCP ineffective
• Transdermal oestrogen possibly

Effects on Fertility
• Infertility: anovulatory cycles and shortened luteal phase
• Reduced response to treatment: possible reduced pregnancy rates to IVF and increased miscarriage rate
• Adverse pregnancy outcomes: higher risks of pre-term birth and low birth weight

Prevalence of subtle menstrual disturbances among sedentary and exercising
volunteers
Assessed by daily hormone levels
De Souza M et al. Hum. Reprod. 2010;25:491-503
© The Author 2009. Published by Oxford University Press on behalf of the European Society of
Human Reproduction and Embryology. All rights reserved. For Permissions, please email:
A = sedentary women BMI 22.7 =/- 0.9 < 2 hr/week 100% regular periods
B = exercising women BMI 21.3 =/- 0.2 Purposeful exercise > 2 hr/week 7% oligomenorrheic 37% amenorrheic

Association between hours of vigorous physical activity per week and fecundability (BMI < 25)
Wise et al. Fertil Steril. 2012 May;97(5):1136-42.
Women age 18 – 40 yrs Self report of physical activity 12 month study Relationship preserved even when excluding women with BMI < 18.5

Lifestyle Management
Key to the reversal of all complications
Multidisciplinary approach:
– Specialist and GP – Sports physician – Nursing support – Dietician – Psychologist – CBT/hypnotherapy – Psychiatrist – Eating Disorder Unit (urgent: BMI<15.5, >4kg in
6/52, medical complications)
Lifestyle Management Need to find a reason relevant to the patient to
reverse
The art of negotiation
Adequate nutrition and maintenance of BMI within the ‘normal’ range (> 22)
Reduce exercise (at least 1 ‘rest day’ per week)
Minimise high impact exercise as much as possible
Keep addressing the anxiety caused by changes

It can take 9-12 months of stable weight before menstruation resumes
The weight needed for restoration of menses is typically higher than the weight at which menses was lost
Discuss body “burn out”
Warn that fertility may return quickly Monitor gonadotropins – LH increases first
Unclear why some respond quickly
– May be a genetic contribution

Take Home Messages Common diagnosis with the potential for
long term complications
Think about energy balance, not just BMI
Limit cardiovascular exercise fuel for exercise
Often multifactorial cause so discuss the issues and get support early (be alert to disordered eating)
Aim for a multidisciplinary approach

CBT and FHA • 20-week randomized trial CBT vs Ob
• 16 normal-weight women BMI 21-23
• < 10 hours exercise/week, no psychiatric diagnosis
• 16 CBT sessions – Healthy eating, exercise
– Problem solving and coping skills
– Body image
• Ovulation returned in 6/8 (CBT) vs 1/8(observation) BMI unchanged
Berga et al. Fertil Steril 2003;80:976-981.

Performance consequences of RED-S
Mountjoy et al, Br J Sports Med 2014;48:491–497.

The Female Athlete Triad
De Souza M J et al. Br J Sports Med 2014;48:289
Copyright © BMJ Publishing Group Ltd & British Association of Sport and Exercise Medicine. All rights reserved.

Ante Natal Screening An update about the latest screening
available in NZ including the new non-invasive prenatal diagnosis
Professor Peter Stone
Women’s Health Update
14 March 2015

SCOPE
• Antenatal(pre) natal screening-for what
• The role of the GP
• What is currently available
• Problems at present-how is the process performing?
• What is new -NIPT
• what does it mean for screening
• what is it used for
• what are the challenges

?
Are you interested in finding out about the
health of the baby?
We can be specific about what “health” means
NIPT is screening

The offer of prenatal screening
• An offer of prenatal screening provides prospective mothers the option of choosing or declining to receive (genetic) information pertinent to their personal situation prior to conception.
• After conception, prenatal screening-diagnosis provides various benefits: it determines the outcome of pregnancy and identifies possible complications that can arise during birth. It can be helpful in improving the outcome of pregnancy using fetal treatment. Screening can help couples determine whether to continue the pregnancy and prepares couples for the birth of a child with an abnormality
It is all about the offer- what is being offered and why

The role of the GP-primary carer
• At first chance- get involved!
• Lock in pregnancy care
• Be part of “life course” approach
~70% women have pregnancy confirmed by GP or FPC
Many opportunities to influence care are missed
There is evidence that most women-couples want screening There is also evidence that carers often prejudge woman’s approach to screening

% Women with LMCs by gestation and ethnicity

The question is
• What do you
want to know?
• What goes wrong
with babies-
And worries
parents
• Chromosomal
• Genetic-identified-known
De novo
Risk recurrence
• Structural
• Environmental-Infection
Epigenetic?
• Unknown-multiple abns
Cerebral palsy
Neurodevelop.delay

What goes “wrong” with babies Microdeletion syndromes
• DiGeorge 22q11 del
• Miller Dieker 17p13.3 del
• Prader Willi 15q11-13 del
• Smith Magenis 17p11.2 del
• Wolf Hirshhorn 4p16.3 del
• Williams-
Beuren 7q11.23 del
Nonsyndromic Microdel/dup
• 16p11.2 Autism
• 1q21.1 ID, microceph,cardiac cataracts
• 16p13.11 Austism, ID, schizophrenia
ID: Intellectual disability
Postnatally 15-20% by CMA vs 3% by G-band karyotype
T21 may be in the lexicon of many when they really are thinking of other problems
Some NIPT can do some of these

Perceptions T21 could be the lexicon for all this
Spectrum of disability
• Extra help at school
• Sequelae of prematurity-NICU
• ADHD
• Cerebral palsy
• Profound developmental delay-mental retardation
• Outcomes of structural fetal abnormality

What are the problems?
What are we trying to detect and avoid?
• Preeclampsia 3-5%
• Fetal growth restriction 5-10%
• Gestational diabetes 5+%
• Fetal abnormalities* 3%
• Risk of Preterm birth 2-7%
• Obstetric problems current pregnancy 5%
• Historical problems 5% Factors are additive and change risk eg obesity, hypertension, history

What we do now
• Current pathways
• Antenatal and newborn screening
history*-what are key questions?
Bloods, incl HIV,Chlamydia,smear as needed
Screening for Down Syndrome and other conditions
• Newborn metabolic and audiology

The current pathways and outcomes offer
1stT combined
Increased risk Low risk
No action Invasive diagnostic
outcome
+2ndT serum
Nt + 2nd T serum 1st and 2nd T serum
Low risk
62%

National Practitioner Guidelines
Laminated summary sheet


Most common chromosomal abnormalities
• Trisomy 21 (Downs Syndrome)
• Trisomy 18 (Edwards Syndrome)
• Trisomy 13 (Patau’s Syndrome)
• 45XO (Turners Syndrome)
• 47XXY (Klinefelters Syndrome)
• Triploidy 69xxx or 69xxy
• Mosaics/translocations/inversions
NIPT
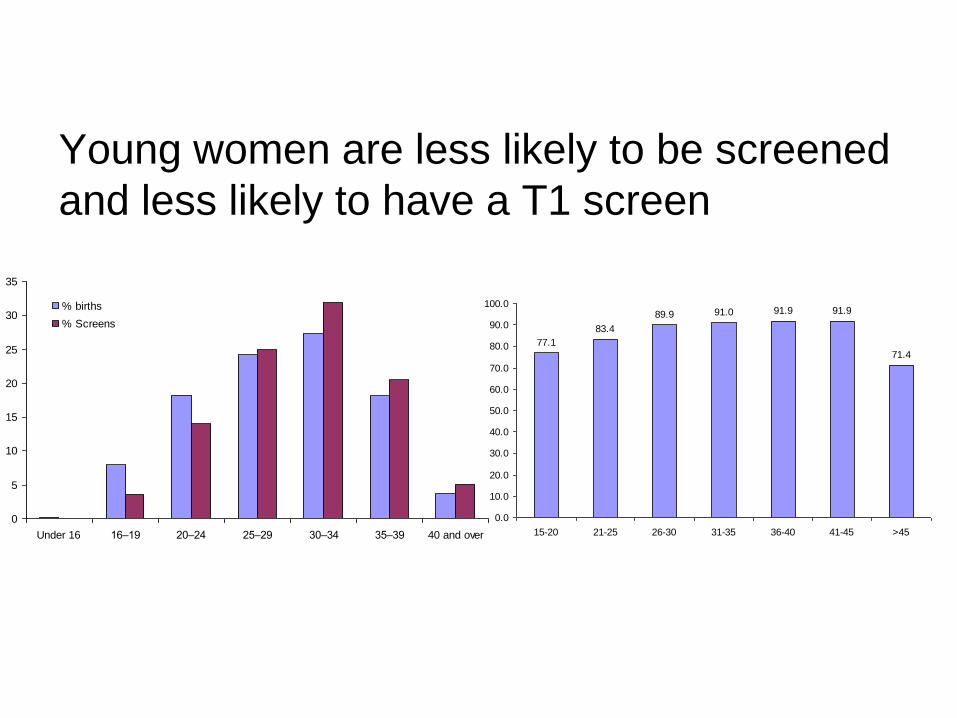
Young women are less likely to be screened
and less likely to have a T1 screen
77.1
83.4
89.9 91.0 91.9 91.9
71.4
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
90.0
100.0
15-20 21-25 26-30 31-35 36-40 41-45 >45
0
5
10
15
20
25
30
35
Under 16 16–19 20–24 25–29 30–34 35–39 40 and over
% births
% Screens
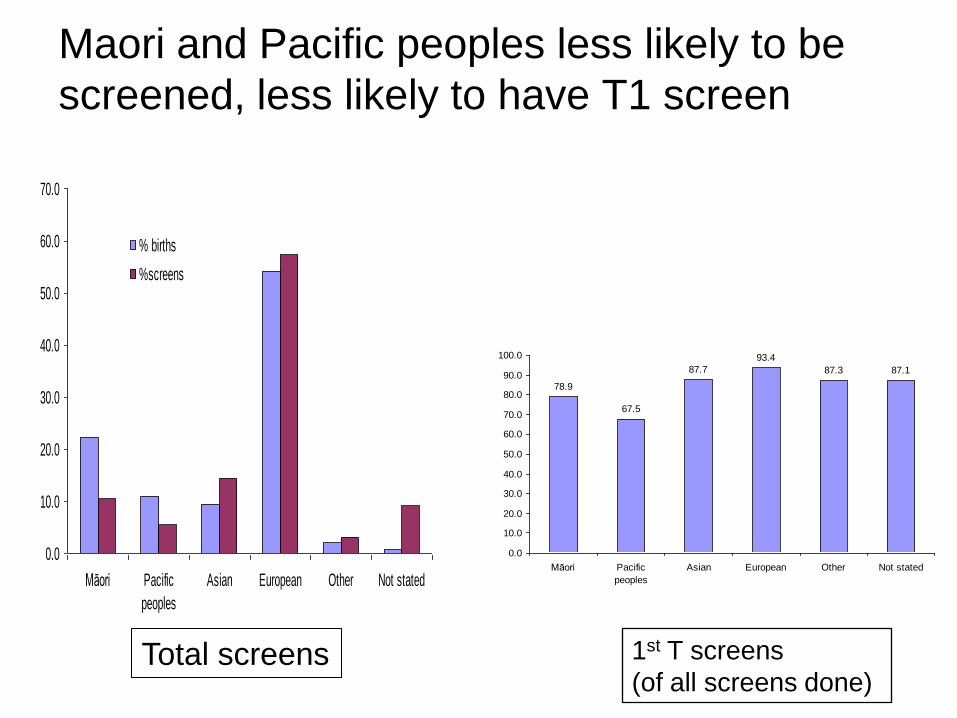
Maori and Pacific peoples less likely to be
screened, less likely to have T1 screen
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
Māori Pacific
peoples
Asian European Other Not stated
% births
%screens
78.9
67.5
87.7
93.4
87.3 87.1
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
90.0
100.0
Māori Pacific
peoples
Asian European Other Not stated
Total screens 1st T screens
(of all screens done)

NZDep v relative amount of screening
R2 = 0.6647
0
20
40
60
80
100
120
140
4 4.5 5 5.5 6 6.5 7 7.5 8
Rich Poor

Ultrasound NT performance standards
Meet standard 22% Too few scans to analyse 40% Underperforming to 0.4mm 31% Unclassifiable 7% (nasal bone reporting very low-2 practices only)
Performance Issues in NZ
Detection rate 78% False pos rate ~3%
>100 sonographers < 25 NT scans /year

We are in a revolution
Non Invasive Prenatal Testing

THE LANCET Vol 350 • August 16, 1997 485
Presence of fetal DNA in maternal plasma and serum Y M Dennis Lo, Noemi Corbetta, Paul F Chamberlain, Vik Rai, Ian L Sargent, Christopher W G Redman, James S Wainscoat

Microarrays
3-4Mb
Single base change
Slide courtesy of Trent Burgess GHSV

Why is NIPT not diagnostic?
• Not only fetal DNA-placental as well
• It is a counting exercise with bioinformatics
and cut offs
• It needs diagnostic tests for confirmation
“Data obtained from a variety of clinical scenarios suggest that the placenta
is the predominant source of the circulating fetal nucleic acids,
although apoptotic haematopoietic cells may contribute to the pool as
well”. Bianchi DW Placenta 2004

53µ
m
73µm
Syncytial knots Or
Syncytial nuclear aggregates
Schmorl 1893

NIPT techniques
• Massively Parallel Sequencing
Fetal chromosome copy number determined by comparing number of sequence reads from chromos of interest to those from reference chromos
• SNPs targetted amplification and sequencing of SNPs
• Microarray based cf DNA analysis

DANSR- digital analysis of selected regions Juneau K et al Fetal Diag Ther 2014

Massively Parallel Sequencing Counting statistics Follow a normal distribution Cut off determines false positive rate 3SD above mean ~0.13% 4SD above mean ~0.003%
No
rmal
ised
ch
rom
oso
me
valu
es
Bianchi D Obstet Gynecol 2012
Factors affecting test performance Maternal Obesity Gestation Chromosome Biology Depth of sequencing Bioinformatics

Effect of Gestation and Maternal weight on fetal fraction
Dars et al 2014

Fetal Fraction- important
Chrom 21 Reference chromo
mat
ern
al
feta
l
Companies need to test and report this It affects the results
Low fetal fraction may occur in: Overweight Low PAPP-A and low bHCG T18 and T13

Performance
1stT Combined screening
• Detect rate 78-88%
• False neg >20%
• False pos 95%
• False pos rate 3-5%
• PPV (NZ) 8%
NIPT
• >99%
• <2%
• <2%
• <1%
• >80%
NIPT is very attractive as those positive-increased chance are highly likely to be a true positive on diagnostic-invasive testing And also fewer false negatives

0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1:40
DOWN SYNDROME SCREENING APPROACH OBSERVED DETECTION RATES FOR 5% FALSE POSITVE RATES
Age 1960
Triple 1970
Quad 1990
Comb 2005
cfDNA 2012
OAPR 1:100 1:60 1:25 1:4 1:5
Int 2005
FPR 0.1% FPR ~3%
Current NZ performance

Meta analysis
• T21 DR99.2%(98.5-99.6) FPR0.09% (0.05-0.14)
• T18 DR 96.3%(94.3-97.9) FPR0.13%(0.07-0.20)
• T13 DR 91.0%(85.0-95.6) FPR 0.13%(0.05-0.26)
• X O DR 90.3%(85.7-94.2) FPR 0.23%(0.14-0.34)
• SCA DR93.0%(85.8-97.8) FPR 0.14% (0.06-0.24)
Ultrasound Obstet Gynecol 2015 DOI: 10.1002/uog.14791 Analysis of cell-free DNA in maternal blood in screening for fetal aneuploidies: updated meta-analysis M. M. GIL, M. S. QUEZADA, R. REVELLO, R. AKOLEKAR, K. H. NICOLAIDES

Summary of NIPT- clinically realistic setting
• T21 DR 100% no false -ve
• Repeat testing 1.16% (Lau et al 2014)
• Non reportable-failure rate 0-4.9% (Benn P 2013)
• T18 DR~100%, T13 DR~91.% (Dan S 2012;Palomaki GE 2012)
Ultrasound Obstet Gynecol 2014; 43: 254–264Non-invasive prenatal testing for fetal chromosomal abnormalities by low-coverage whole-genome sequencing of maternal plasma DNA: review of 1982 consecutive cases in a single centerT. K. LAU, S. W. CHEUNG, P. S. S. LO, A. N. PURSLEY,M. K. CHAN, F. JIANG,H. ZHANG, W. WANG, L. F. J. JONG, O. K. C. YUEN, H. Y. C. CHAN, W. S. K. CHAN K. W. CHOY n=1982cases

Other examples of use of NIPT
• Fetal blood group genotyping* Targeted antenatal AntiD Determining surveillance in sensitised women • Fetal congenital adrenal hyperplasia • Cystic fibrosis • Spinal muscular atrophy etc * Available now

Some Companies • ARIOSA (US) «Harmony» (?array approach)
• VERINATA (US) «verifi» (Illumina)
• NATERA (US) «Panorama» (SNP approach)
• SEQUENOM (US) «MaterniT21»
• BGI (China) «NIFTY»
• LIFE-CODEXX (Germany) «PrenaTest»
Ask about fetal fraction, risk approach, failed test rate, what result is produced, coping with problems such as obesity, claims for twins- “expanded” screens and perhaps lastly cost

From 10 weeks 7 day turn around 21 18 13, ask doctor other SCAs Can do twins Cost-negotiate
basic verifi® Test screens for: T21 (Down syndrome) T18 (Edwards syndrome) T13 (Patau syndrome) Now a wider option is available for sex chromosomes at no extra charge: Monosomy X (MX; Turner syndrome) XXX (Triple X) XXY (Klinefelter syndrome) XYY (Jacobs syndrome) Fetal sex (XX or XY)—aids in stratifying the risk for X-linked disorders such as hemophilia, Duchenne muscular dystrophy, or cases of ambiguous genitalia, such as congenital adrenal hyperplasia
Verifir – by Illumina

Panorama™ provides sensitivity >99% and positive predicted value (PPV) > 91% for Down syndrome. A microdeletion panel (including 22q11.2 deletion syndrome) is also available to provide unparalleled scope and reliability among non-invasive prenatal screens.

MATERNIT21® PLUS
22q deletion syndrome (DiGeorge) 5p (Cri-du-chat syndrome) 15q (Prader-Willi/Angelman syndromes) 1p36 deletion syndrome 4p (Wolf-Hirschhorn syndrome) 8q (Langer-Giedion syndrome) 11q (Jacobsen syndrome) Trisomy 16 Trisomy 22
From 10 weeks From 5 day turnaround Can expand Can do twins
Request form You do need to have counselled patient
and you do need to know
what you are requesting

MATERNIT21® PLUS
The clinician has to explain the results and discuss the limitations In practice, probably no difference from currently and for common trisomies Probably much more straightforward as the difference in likelihood of a true pos or neg result Is very wide compared with current tests ( eg 1:2chance of pos versus 1:1000 if negative)
Main difference is that clinicians are dealing with off shore companies and we have little idea of their QA and science We also take all responsibility for outcomes and it is no easy to “call up the lab”

The pathway and outcomes Current Pathway Future
offer
1stT combined
Increased risk Low risk
No action
Invasive diagnostic
outcome
offer
1stT combined
NIPT
Increased risk Low risk
No action
outcome
Invasive diagnostic
Risk cut off

A radical option?
Offer*
NIPT + scan**
Low risk
outcome
High risk
Invasive-amnio CVS
• *Be clear and simple what is the question? • **scan check list- no NT no part charge • Decide best timing of scan and ?do NIPT after

What might be missed-at this time
cfDNA may not detect:
• rare trisomies
• unbalanced structural rearrangements
• deletions and duplications
• triploidy
• marker chromosomes
• mosaicism.

Challenges
• Making a decision to do it- we have to
-it speaks for itself
• What are “the other conditions”?
- what trade offs - understanding we get what we ask for
- Where would NIPT fit in- for all women or some?
• Costing the format
• Getting started in the Lab and validation
• Impact on invasives- skills of invasive operators

Cost- its not too bad actually
• Funded in Canada
• Insurance pays in USA
• UK study suggests can be cost neutral
(Morris S PLoS 2014)
• Costs vary with
Company
Techniques eg MPS vs SNPs
Volumes
Cutoffs in risk (if contingent)
What is screened for
No one costs false negs
Currently , on bulk contract could get for ~$250 NZ per test

Assumptions
Number screened now 45,000
Serum Costs
Serum 120
Scan 112
Total 232 $10,440,000
FPR 3% 1350
Invasives (75%) 1013@$1,000 $1013000
Missed cases 16 ?$$$
Total 11,453,000
NIPT Costs
NIPT 200
Scan 87
Total 287 12,915,000
False pos ~0.1
Invasives (80%) ~50 50,000
Missed cases 1-2
Total 12,965,000
Not included:
Capital costs to set up
Falling costs with volumes
Doing in a contingent way
Changed costs to patients eg cheaper scans less travel, less anxiety, fewer false pos and false negs
for trisomies
Identifiable costs Screening and invasives

Summary
• NIPT a great new advance- a new paradigm!!
• New era in performance
• Very low false pos and neg
• Much more reassuring for women
• Will further reduce invasive tests
• Provides a platform for the future- can change
• It is here now – lets do it well and ?offer to all

"I feel like the luckiest person alive," Dr Lee, a San Francisco-based anesthesiologist,
When she was 15 weeks pregnant, she underwent a whole-body MRI scan and a 7 cm tumor in the sigmoid colon was detected.
Medscape Medical News > Conference News Test for Fetal Abnormalities Finds Maternal Cancer Neil Osterweil March 06, 2015
With laparoscopic resection, the surgeons were able to completely remove the tumor. Postsurgical staging showed that it was T3N0M0 colon cancer
“The abnormalities seen are not diagnostic of cancer, Dr van den Boom explained. They could come from systemic lupus erythematosus, organ transplant rejection, or other causes, but test results in several cases have come back suggestive of various malignancies”.
As this expands do we need national and bioethical standards and controls?

Click to edit Master title style
Click to edit Master subtitle style
1 3/17/2015 1 3/17/2015 1
Breast Cancer Update
Wayne Jones FRACS

Click to edit Master title style
Click to edit Master subtitle style
2 3/17/2015 2
Click to edit Master title style
2 3/17/2015 2
Topics
• Breast Imaging
• Breast Surgery
• Adjuvant Treatment

Click to edit Master title style
Click to edit Master subtitle style
3 3/17/2015 3
Click to edit Master title style
3 3/17/2015 3
Breast Imaging
• Digital mammography
• Tomosynthesis mammography
• Office ultrasound
• Image guided biopsies
• MRI − High risk screening & specific questions
− ? Lobular Ca & DCIS
− Cost, claustrophobia, over-calls cancer

Click to edit Master title style
Click to edit Master subtitle style
4 3/17/2015 4
Click to edit Master title style
4 3/17/2015 4
Digital Mammography

Click to edit Master title style
Click to edit Master subtitle style
5 3/17/2015 5
Click to edit Master title style
5 3/17/2015 5
Digital Mammography

Click to edit Master title style
Click to edit Master subtitle style
6 3/17/2015 6
Tomosynthesis Mammography

Click to edit Master title style
Click to edit Master subtitle style
7 3/17/2015 7
Office Ultrasound

Click to edit Master title style
Click to edit Master subtitle style
8 3/17/2015 8
Click to edit Master title style
8 3/17/2015 8
U/S Guided Core Biopsy

Click to edit Master title style
Click to edit Master subtitle style
9 3/17/2015 9
Click to edit Master title style
9 3/17/2015 9
Breast MRI

Click to edit Master title style
Click to edit Master subtitle style
10 3/17/2015 10 3/17/2015 10
Breast Surgery

Click to edit Master title style
Click to edit Master subtitle style
11 3/17/2015 11
Mastectomy

Click to edit Master title style
Click to edit Master subtitle style
12 3/17/2015 12
Breast Conservation Surgery

Click to edit Master title style
Click to edit Master subtitle style
13 3/17/2015 13
Breast Conservation Surgery

Click to edit Master title style
Click to edit Master subtitle style
14 3/17/2015 14
Sentinel Node Biopsy
• 40% lymph node involvement
• U/S and FNA biopsy
• Pre-op ID of sentinel node 95%+
• Smaller operation, less morbidity eg shoulder pain, lymphoedema
• No difference in DFS or OS v AND
Nodal Basin
Tumour

Click to edit Master title style
Click to edit Master subtitle style
15 3/17/2015 15
Lymphoscintogram

Click to edit Master title style
Click to edit Master subtitle style
16 3/17/2015 16
Patent Blue V Dye

Click to edit Master title style
Click to edit Master subtitle style
17 3/17/2015 17
Click to edit Master title style
17 3/17/2015 17
Hand-held Gamma Probe

Click to edit Master title style
Click to edit Master subtitle style
18 3/17/2015 18
Hand-held Gamma Probe

Click to edit Master title style
Click to edit Master subtitle style
19 3/17/2015 19
Click to edit Master title style
19 3/17/2015 19
Is Axillary Dissection Needed?
• Currently if − SNB positive have ALND
− SNB negative avoid ALND
• Isolated tumour cells <0.2mm – not significant
• Micrometastases <2mm – increased LR, ? ALND
• Micrometastases >2mm – Do ALND
• If 3 or more nodes involved omit ALND if getting
systemic tx and DXR (Z-0011 trial, IBCSG 23-01)

Click to edit Master title style
Click to edit Master subtitle style
20 3/17/2015 20
Click to edit Master title style
20 3/17/2015 20
Breast Reconstruction
• Offered to all ‘Mastectomy Patients’
• Psycho-social & sexuality reasons
• Immediate or Delayed
• Implants – one or two stage
• TRAM flaps - muscle, fat & skin
• DIEP flaps – fat & skin, microvascular

Click to edit Master title style
Click to edit Master subtitle style
21 3/17/2015 21
Click to edit Master title style
21 3/17/2015 21
Permanent Implants

Click to edit Master title style
Click to edit Master subtitle style
22 3/17/2015 22
How strong are they?

Click to edit Master title style
Click to edit Master subtitle style
23 3/17/2015 23
Click to edit Master title style
23 3/17/2015 23
One Stage Implant
Click to edit Master title style
Click to edit Master subtitle style
24 3/17/2015 24
Click to edit Master title style
24 3/17/2015 24
Two Stage Implant – Pre-op

Click to edit Master title style
Click to edit Master subtitle style
25 3/17/2015 25
Click to edit Master title style
25 3/17/2015 25
Two Stage Implants

Click to edit Master title style
Click to edit Master subtitle style
26 3/17/2015 26
Click to edit Master title style
26 3/17/2015 26
Two Stage Implant - Expansion

Click to edit Master title style
Click to edit Master subtitle style
27 3/17/2015 27
Click to edit Master title style
27 3/17/2015 27
Two Stage Implant – Post-op

Click to edit Master title style
Click to edit Master subtitle style
28 3/17/2015 28
Click to edit Master title style
28 3/17/2015 28
TRAM Flap

Click to edit Master title style
Click to edit Master subtitle style
29 3/17/2015 29
Click to edit Master title style
29 3/17/2015 29
Delayed TRAM flap

Click to edit Master title style
Click to edit Master subtitle style
30 3/17/2015 30
Nipple Reconstruction

Click to edit Master title style
Click to edit Master subtitle style
31 3/17/2015 31
Nipple Reconstruction
Click to edit Master title style
Click to edit Master subtitle style
32 3/17/2015 32
Click to edit Master title style
32 3/17/2015 32
Nipple Sparing Mastectomy
• No increased risk breast cancer if preserve nipple − If >2cm from nipple, not multifocal
− Frozen Section at surgery
• Routine for prophylatic mastectomies
• Selected cancer mastectomies − Not contra-indicated as above
− Can preserve blood supply
• Inferolateral approach or peri-areola

Click to edit Master title style
Click to edit Master subtitle style
33 3/17/2015 33
Click to edit Master title style
33 3/17/2015 33
Nipple Sparing Mastectomy

Click to edit Master title style
Click to edit Master subtitle style
34 3/17/2015 34 3/17/2015 34
Adjuvant Treatment

Click to edit Master title style
Click to edit Master subtitle style
35 3/17/2015 35
Click to edit Master title style
35 3/17/2015 35
Radiotherapy
• All cases of Partial Mastectomy for DXR
• Nodal status important − Was >3 nodes, now 1 node treated (EBCTG 2014)
• Intra-operative DXR − Controversial
− Some patients don’t need DXR at all
− Editorial Int J Rad Onc 2015 91(2), p255-7
• Partial breast irradiation

Click to edit Master title style
Click to edit Master subtitle style
36 3/17/2015 36
Endocrine Therapy
• Aromatase Inhibitors more effective than Tamoxifen − 17% less recurrence, 53% less contralateral cancer
− Less DVT, Hot flushes, uterine Ca, more joint pain, lose bone density
• Can switch to AI after 2y
• Duration – 10y better than 5y
• Primary endocrine therapy if unfit for surgery
• Pre-menopausal women − Use Exemestane & Zoladex (GnRH inhibitor)
− More effective than Tamoxifen (SOFT trial)

Click to edit Master title style
Click to edit Master subtitle style
37 3/17/2015 37
Chemotherapy
• More effective 3rd generation chemo
• Use of multi-agents
eg AC & Taxol, FEC & Taxol
• Tailor treatment eg basal type, gene array analysis
• Neo-adjuvant tx for Her2 +ve & “triple negative”
• Management of Her2 +ve Ca <1cm controversial
• Consider fertility treatment
Click to edit Master title style
Click to edit Master subtitle style
38 3/17/2015 38
Herceptin (Trastuzumab)
• 20% women HER2 +ve
• HERA Study – recurrence ↓46%
• 12m course $80,000
• Give with chemo
• 3m versus 12m?
• Combination with Pertuzumab?
• Need Portacath

Click to edit Master title style
Click to edit Master subtitle style
39 3/17/2015 39

Click to edit Master title style
Click to edit Master subtitle style
40 3/17/2015 40 3/17/2015 40
Questions?