2006 focal points dry_eye.pdf
DESCRIPTION
Dry eye, American Academy Ophthalmology, Focal Points, Guidelines, Occhio secco, linee guida, lubricating, Preferred Practice Patterns, Oculistica, Ophthalmology.TRANSCRIPT
Focal Pointsc l i n i c a l m o d u l e s f o r o p h t h a l m o l o g i s t s
American Academy of Ophthalmology
Reviewers and Contributing Editors
Editor for Cornea, External Disease & Refractive Surgery:
George A. Stern, MD
Basic and Clinical Science Course Faculty, Section 8:
Reza Dana, MD, MPH
Practicing Ophthalmologists Advisory Committee for Education:
John S. Berestka, MD
Consultants
Gary N. Foulks, MD, FACSMitchell Friedlaender, MD
Dry EyeStephen C. Pflugfelder, MD
VOLUME XXIV NUMBER 5 JUNE 2006 (SECTION 2 OF 3)
Cover_Mod_05_Jun06.indd 3 4/27/06 12:51:45 PM

Focal Points Editorial Review BoardDennis M. Marcus, MD, Augusta, GA: Editor-in-Chief, Retina & Vitreous • Thomas L. Beardsley, MD, Asheville, NC: Cataract • Steven V.L. Brown, MD, Evanston, IL: Glaucoma Surgery; Liaison for Practicing Ophthalmologists Advisory Committee for Education • Keith D. Carter, MD, Iowa City, IA: Oculoplastic, Lacrimal, & Orbital Surgery • Jane D. Kivlin, MD, Milwaukee, WI: Pediatric Ophthalmology & Strabismus • Anil D. Patel, MD, Oklahoma City, OK: Neuro-Ophthalmology • George A. Stern, MD, Missoula, MT: Cornea, External Disease & Refractive Surgery; Optics & Refraction • Albert T. Vitale, MD, Salt Lake City, UT: Ocular Inflammation & Tumors
Focal Points StaffSusan R. Keller, Acquisitions Editor • Kim Torgerson, Publications Manager
Clinical Education Secretaries and StaffThomas J. Liesegang, MD, Senior Secretary for Clinical Education, Jacksonville, FL • Gregory L. Skuta, MD, Secretary for Ophthalmic Knowledge, Oklahoma City, OK • Richard A. Zorab, Vice President, Ophthalmic Knowledge • Hal Straus, Director of Publications
Focal Points (ISSN 0891-8260) is published quarterly by the American Academy of Ophthalmology at 655 Beach St., San Francisco, CA 94109-1336. Print or online yearly subscriptions are $145 for Academy members and $205 for nonmembers. The print and online yearly subscription package is $175 for members and $250 for nonmembers. Periodicals postage paid at San Francisco, CA, and additional mailing offices. POSTMASTER: Send address changes to Focal Points, P.O. Box 7424, San Francisco, CA 94120-7424.
The American Academy of Ophthalmology is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians. The American Academy of Ophthalmology designates this educa-tional activity for a maximum of two AMA PRA Category 1 Credits™. Physicians should only claim credit commensurate with the extent of their participation in the activity.
Reporting your CME online is one benefit of Academy membership. Non-mem-bers may request a Focal Points CME Claim Form by contacting Focal Points, 655 Beach St., San Francisco, CA 94109-1336.
The Academy provides this material for educational purposes only. It is not intended to represent the only or best method or procedure in every case, nor to replace a physician’s own judgment or give specific advice for case management. Including all indications, contraindications, side effects, and alternative agents for each drug or treatment is beyond the scope of this material. All information and rec-ommendations should be verified, prior to use, with current information included in the manufacturers’ package inserts or other independent sources and considered in light of the patient’s condition and history. Reference to certain drugs, instruments, and other products in this publication is made for illustrative purposes only and is not intended to constitute an endorsement of such. Some material may include infor-mation on applications that are not considered community standard, that reflect indications not included in approved FDA labeling, or that are approved for use only in restricted research settings. The FDA has stated that it is the responsibility of the physician to determine the FDA status of each drug or device he or she wishes to use, and to use them with appropriate patient consent in compliance with applicable law. The Academy specifically disclaims any and all liability for injury or other damages of any kind, from negligence or otherwise, for any and all claims that may arise out of the use of any recommendations or other information contained herein.
The author(s) listed made a major contribution to this module. Substantive edi-torial revisions may have been made based on reviewer recommendations.
Subscribers requesting replacement copies 6 months and later from the cover date of the issue being requested will be charged the current module replacement rate.
©2006 American Academy of Ophthalmology®. All rights reserved.
Stephen C. Pflugfelder, MD, and Mitchell Fried-laender, MD, state that they have no financial rela-tionship with the manufacturer of any commercial products discussed in their contributions to this mod-ule. Gary N. Foulks, MD, FACS, states that he has a divested interest in the following companies: Aller-gan, Inc., Inspire Pharmaceuticals, Otsuka Pharma-ceuticals, Nascent Pharmaceuticals, and Novartis.
Dry Eye
Introduction
Pathogenesis
Differential DiagnosisIrritation SymptomsTear Film InstabilityAqueous Tear ProductionMeibomian Gland EvaluationConjunctival Goblet CellsOcular Surface Dye Staining
TherapyEnvironmental ModificationArtificial TearsPunctal OcclusionAnti-inflammatory TherapyCyclosporineCorticosteroidsTetracyclinesEssential Fatty AcidsSecretagoguesSerumContact Lenses and Tarsorrhaphy
Conclusion
Clinicians’ Corner
Claiming CME Credit
Academy members: To claim Focal Points CME cred-its, vist the Academy website and access CME Central (http://www.aao.org/cme) to log on, view your Acad-emy transcript, and report the CME credit you have earned. You can claim up to two AMA PRA Category 1 Credits™ per module. This will give you a maxi-mum of 24 credits for the 2006 subscription year.
Non-Academy members: Please send an e-mail to [email protected] or a fax to (415) 561-8575 for assistance.
Mod_05_Jun06.indd 2 4/26/06 10:55:47 AM
June 2006 1 F O C A L P O I N T S
Introduction
Dry eye was defined by the National Eye Institute/Industry workshop in 1993 as a “disorder of the tear film due to tear deficiency or excessive evaporation, which causes damage to the interpalpebral ocular surface and is associated with symptoms of discom-
Learning ObjectivesUpon completion of this module, the reader should be able to:
• Recognize dry eye as a result of disease or dysfunction of the “lacrimal functional unit”
• Discuss changes in tear composition in relationship to the pathogenesis of dry eye
• Base therapy of dry eye on the severity of the signs of ocular surface dryness
• Consider anti-inflammatory therapy in patients with ocular surface disease that is not responsive to artificial tears
Key words: corticosteroid, cyclosporine, dry eye, inflammation, keratoconjunctivitis sicca, lacrimal gland, tetracycline
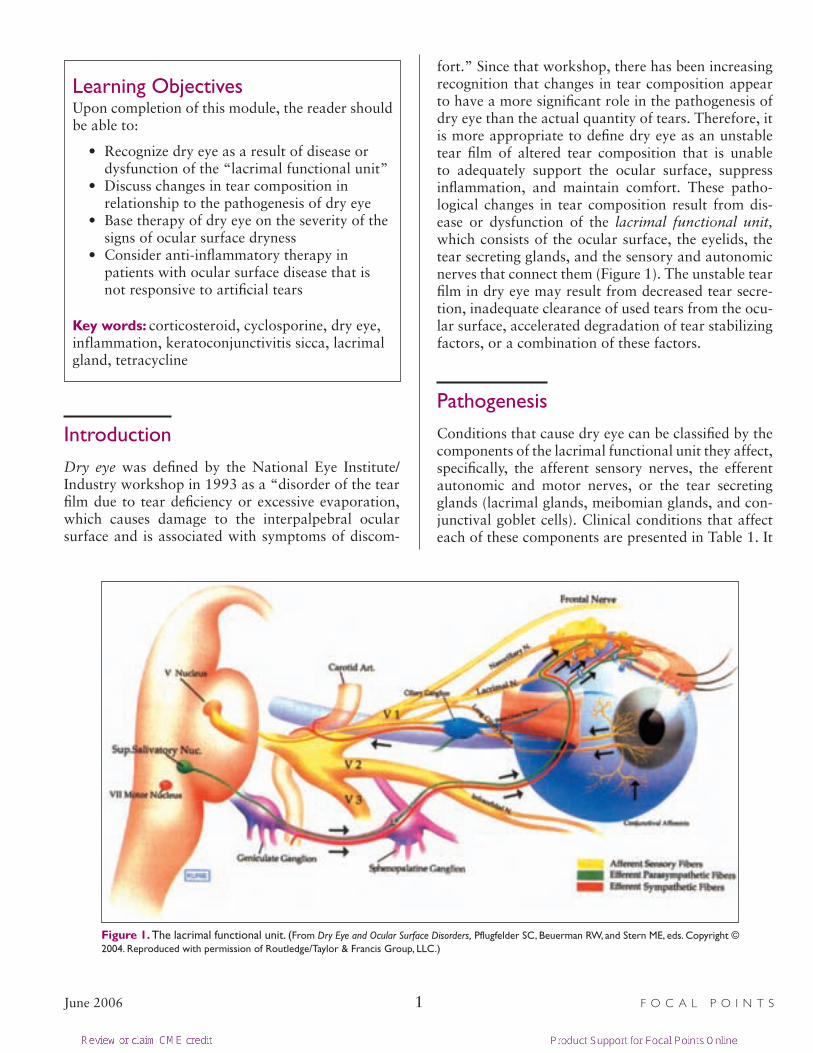
fort.” Since that workshop, there has been increasing recognition that changes in tear composition appear to have a more significant role in the pathogenesis of dry eye than the actual quantity of tears. Therefore, it is more appropriate to define dry eye as an unstable tear film of altered tear composition that is unable to adequately support the ocular surface, suppress inflammation, and maintain comfort. These patho-logical changes in tear composition result from dis-ease or dysfunction of the lacrimal functional unit, which consists of the ocular surface, the eyelids, the tear secreting glands, and the sensory and autonomic nerves that connect them (Figure 1). The unstable tear film in dry eye may result from decreased tear secre-tion, inadequate clearance of used tears from the ocu-lar surface, accelerated degradation of tear stabilizing factors, or a combination of these factors.
Pathogenesis
Conditions that cause dry eye can be classified by the components of the lacrimal functional unit they affect, specifically, the afferent sensory nerves, the efferent autonomic and motor nerves, or the tear secreting glands (lacrimal glands, meibomian glands, and con-junctival goblet cells). Clinical conditions that affect each of these components are presented in Table 1. It
Figure 1. The lacrimal functional unit. (From Dry Eye and Ocular Surface Disorders, Pflugfelder SC, Beuerman RW, and Stern ME, eds. Copyright © 2004. Reproduced with permission of Routledge/Taylor & Francis Group, LLC.)
Mod_05_Jun06.indd 1 4/26/06 10:55:50 AM

F O C A L P O I N T S 2 June 2006
is not uncommon for patients to have more than one dysfunctional component (eg, concurrent lacrimal gland and meibomian gland disease). An excellent example of a combined effect is the dry eye that devel-ops after laser in situ keratomileusis (LASIK) surgery. Amputation of afferent corneal nerves by the micro-keratome during LASIK results in a transient decrease in corneal sensitivity that returns to near the baseline level by 6 months postoperatively. This is accompa-nied by a 25% to 30% decrease in aqueous tear pro-duction and by increased tear film osmolarity, delayed tear fluorescein clearance, and decreased tear break-up time. Improvements in tear production and ocu-lar surface disease parallel the return of corneal sensi-tivity. Other common clinical conditions/factors that affect the lacrimal functional unit include anticholin-ergic medications that interfere with parasympathetic signaling of glandular tear secretion, menopause with decreased levels of circulating hormones to support
the secretory glands, and systemic inflammatory con-ditions (eg, rheumatoid arthritis and chronic hepati-tis C infection) that cause lymphocytic infiltration of the lacrimal glands and inflammatory paralysis of the secretory epithelia.
One change in tear composition that occurs in the majority of dry eye conditions is increased osmolarity. It is recognized that increased tear osmolarity com-bined with other changes in tear composition pro-motes ocular surface disease, termed keratoconjuncti-vitis sicca (KCS). A basic feature of KCS is abnormal differentiation and accelerated loss of superficial ocu-lar surface epithelial cells. The apical corneal epithe-lial cells produce the glycocalyx that coats the corneal surface and that provides a hydrophilic surface to bind and stabilize the overlying tear film. These cells also serve as a barrier to microbial and leukocyte invasion. Loss of superficial corneal epithelial cells exposes the underlying sensory nerve endings to noxious environ-mental insults. This is the underlying cause for the chronic ocular discomfort that patients with dry eye experience.
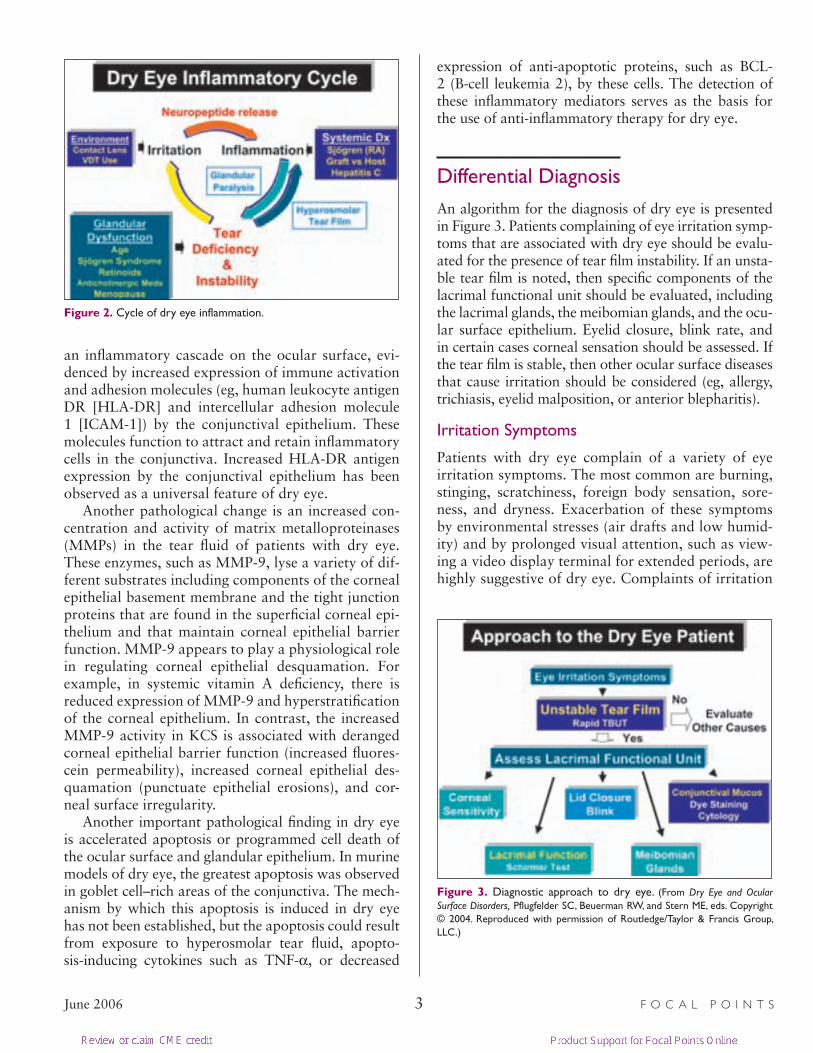
Ocular surface inflammation is both a cause and a consequence of dry eye. Disease or dysfunction of the tear secretory glands leads to changes in tear com-position, such as hyperosmolarity that stimulates the production of inflammatory mediators on the ocular surface, which in turn may cause dysfunction of the tear secreting glands. Inflammation can also be ini-tiated by chronic irritative stress (eg, contact lenses or chronic viewing of a video display terminal) and systemic inflammatory/autoimmune disease (eg, rheu-matoid arthritis). Regardless of the initiating cause, a vicious cycle of inflammation may develop on the ocular surface in dry eye that leads to ocular surface disease (Figure 2).
There is increasing evidence for the inflammatory component of dry eye disease. First, the tear fluid con-centration of natural anti-inflammatory factors, such as lactoferrin, that are secreted by the lacrimal glands may decrease. Second, there appears to be increased production of the pro-inflammatory cytokines inter-leukin-1 (IL-1) and tumor necrosis factor alpha (TNF-α) and certain proteolytic enzymes by stressed ocular surface and glandular epithelial cells, as well as by the inflammatory cells that infiltrate these tissues. Third, there is activation of latent inactive cytokines and proteases that are normally present in the tear fluid and that serve as an early defense mechanism follow-ing ocular surface infection and wounding.
The soluble and cellular inflammatory mediators in the tear fluid, conjunctiva, and lacrimal glands initiate
Table 1. Disorders of the Lacrimal Functional Unit
Afferent
Trigeminal ganglion ablation
Herpes simplex, herpes zoster
Familial dysautonomia (Riley-Day syndrome)
Contact lenses
Diabetic neuropathy
Lattice corneal dystrophy
Surgeries—scleral buckling, penetrating keratoplasty, LASIK
Efferent
Systemic medications with anticholinergic effects—antihistamines, antispasmotics, anti-emetics, and antidepressants
M3 acetylcholine receptor autoantibodies (Sjögren syndrome)
Age-related parasympathetic dysfunction
Bell’s palsy
Glandular
Aging—lobular and diffuse fibrosis and atrophy, periductual fibro-sis, lymphocytic infiltration, decreased EGF and lactoferrin secretion
Cicatricial duct obstruction—trachoma, Stevens-Johnson syn-drome, ocular cicatricial pemphigoid, chemical/thermal injury
Menopause—decrease in supportive hormones (androgens)
Infection/inflammation—HIV, chronic hepatitis C, graft vs host disease, Sjögren syndrome
Nutritional—vitamin A deficiency
Rosacea
Isotretinoin (Accutane) therapy
Mod_05_Jun06.indd 2 4/26/06 10:55:51 AM
June 2006 3 F O C A L P O I N T S
an inflammatory cascade on the ocular surface, evi-denced by increased expression of immune activation and adhesion molecules (eg, human leukocyte antigen DR [HLA-DR] and intercellular adhesion molecule 1 [ICAM-1]) by the conjunctival epithelium. These molecules function to attract and retain inflammatory cells in the conjunctiva. Increased HLA-DR antigen expression by the conjunctival epithelium has been observed as a universal feature of dry eye.
Another pathological change is an increased con-centration and activity of matrix metalloproteinases (MMPs) in the tear fluid of patients with dry eye. These enzymes, such as MMP-9, lyse a variety of dif-ferent substrates including components of the corneal epithelial basement membrane and the tight junction proteins that are found in the superficial corneal epi-thelium and that maintain corneal epithelial barrier function. MMP-9 appears to play a physiological role in regulating corneal epithelial desquamation. For example, in systemic vitamin A deficiency, there is reduced expression of MMP-9 and hyperstratification of the corneal epithelium. In contrast, the increased MMP-9 activity in KCS is associated with deranged corneal epithelial barrier function (increased fluores-cein permeability), increased corneal epithelial des-quamation (punctuate epithelial erosions), and cor-neal surface irregularity.
Another important pathological finding in dry eye is accelerated apoptosis or programmed cell death of the ocular surface and glandular epithelium. In murine models of dry eye, the greatest apoptosis was observed in goblet cell–rich areas of the conjunctiva. The mech-anism by which this apoptosis is induced in dry eye has not been established, but the apoptosis could result from exposure to hyperosmolar tear fluid, apopto-sis-inducing cytokines such as TNF-α, or decreased
expression of anti-apoptotic proteins, such as BCL-2 (B-cell leukemia 2), by these cells. The detection of these inflammatory mediators serves as the basis for the use of anti-inflammatory therapy for dry eye.
Differential Diagnosis
An algorithm for the diagnosis of dry eye is presented in Figure 3. Patients complaining of eye irritation symp-toms that are associated with dry eye should be evalu-ated for the presence of tear film instability. If an unsta-ble tear film is noted, then specific components of the lacrimal functional unit should be evaluated, including the lacrimal glands, the meibomian glands, and the ocu-lar surface epithelium. Eyelid closure, blink rate, and in certain cases corneal sensation should be assessed. If the tear film is stable, then other ocular surface diseases that cause irritation should be considered (eg, allergy, trichiasis, eyelid malposition, or anterior blepharitis).
Irritation Symptoms
Patients with dry eye complain of a variety of eye irritation symptoms. The most common are burning, stinging, scratchiness, foreign body sensation, sore-ness, and dryness. Exacerbation of these symptoms by environmental stresses (air drafts and low humid-ity) and by prolonged visual attention, such as view-ing a video display terminal for extended periods, are highly suggestive of dry eye. Complaints of irritation
Figure 3. Diagnostic approach to dry eye. (From Dry Eye and Ocular Surface Disorders, Pflugfelder SC, Beuerman RW, and Stern ME, eds. Copyright © 2004. Reproduced with permission of Routledge/Taylor & Francis Group, LLC.)
Figure 2. Cycle of dry eye inflammation.
Mod_05_Jun06.indd 3 4/26/06 10:56:01 AM
F O C A L P O I N T S 4 June 2006
are not always accompanied by objective signs of keratoconjunctivitis sicca, such as ocular surface dye staining.
Systemic medication use should be reviewed to identify agents (eg, antihistamines, antidepressants, or estrogen hormone replacement therapy) that are capable of decreasing tear secretion. Patients should be asked if they have a dry mouth, dental caries, and arthritis, conditions that are associated with Sjögren syndrome.
Tear Film Instability
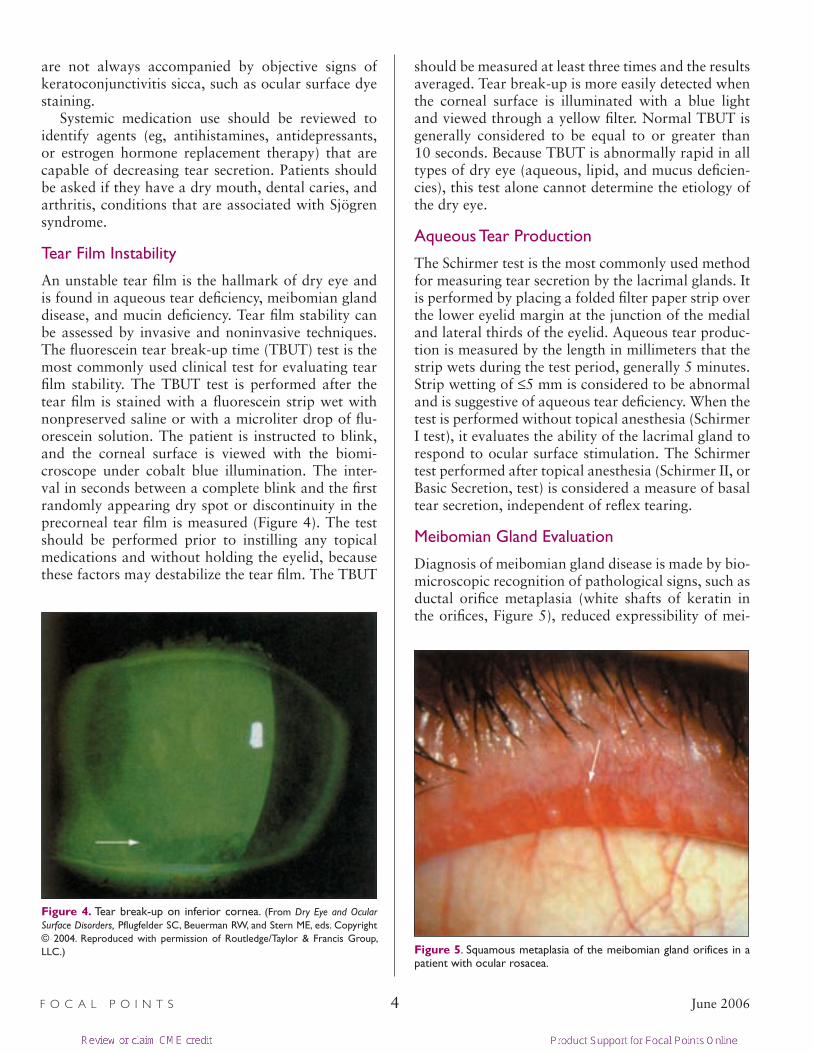
An unstable tear film is the hallmark of dry eye and is found in aqueous tear deficiency, meibomian gland disease, and mucin deficiency. Tear film stability can be assessed by invasive and noninvasive techniques. The fluorescein tear break-up time (TBUT) test is the most commonly used clinical test for evaluating tear film stability. The TBUT test is performed after the tear film is stained with a fluorescein strip wet with nonpreserved saline or with a microliter drop of flu-orescein solution. The patient is instructed to blink, and the corneal surface is viewed with the biomi-croscope under cobalt blue illumination. The inter-val in seconds between a complete blink and the first randomly appearing dry spot or discontinuity in the precorneal tear film is measured (Figure 4). The test should be performed prior to instilling any topical medications and without holding the eyelid, because these factors may destabilize the tear film. The TBUT
should be measured at least three times and the results averaged. Tear break-up is more easily detected when the corneal surface is illuminated with a blue light and viewed through a yellow filter. Normal TBUT is generally considered to be equal to or greater than 10 seconds. Because TBUT is abnormally rapid in all types of dry eye (aqueous, lipid, and mucus deficien-cies), this test alone cannot determine the etiology of the dry eye.
Aqueous Tear Production
The Schirmer test is the most commonly used method for measuring tear secretion by the lacrimal glands. It is performed by placing a folded filter paper strip over the lower eyelid margin at the junction of the medial and lateral thirds of the eyelid. Aqueous tear produc-tion is measured by the length in millimeters that the strip wets during the test period, generally 5 minutes. Strip wetting of ≤5 mm is considered to be abnormal and is suggestive of aqueous tear deficiency. When the test is performed without topical anesthesia (Schirmer I test), it evaluates the ability of the lacrimal gland to respond to ocular surface stimulation. The Schirmer test performed after topical anesthesia (Schirmer II, or Basic Secretion, test) is considered a measure of basal tear secretion, independent of reflex tearing.
Meibomian Gland Evaluation
Diagnosis of meibomian gland disease is made by bio-microscopic recognition of pathological signs, such as ductal orifice metaplasia (white shafts of keratin in the orifices, Figure 5), reduced expressibility of mei-
Figure 4. Tear break-up on inferior cornea. (From Dry Eye and Ocular Surface Disorders, Pflugfelder SC, Beuerman RW, and Stern ME, eds. Copyright © 2004. Reproduced with permission of Routledge/Taylor & Francis Group, LLC.) Figure 5. Squamous metaplasia of the meibomian gland orifices in a
patient with ocular rosacea.
Mod_05_Jun06.indd 4 4/26/06 10:56:05 AM
June 2006 5 F O C A L P O I N T S
bomian gland secretions, increased turbidity and vis-cosity of the expressed secretion, and dropout of glan-dular acini.
Conjunctival Goblet Cells
Conjunctival goblet cell density and epithelial mor-phology can be directly evaluated by impression cytology. However, since this technique is usually per-formed only at academic institutions or referral cen-ters, ocular surface dye staining is typically used as a clinical measure of the integrity of the conjunctival mucus layer.
Ocular Surface Dye Staining
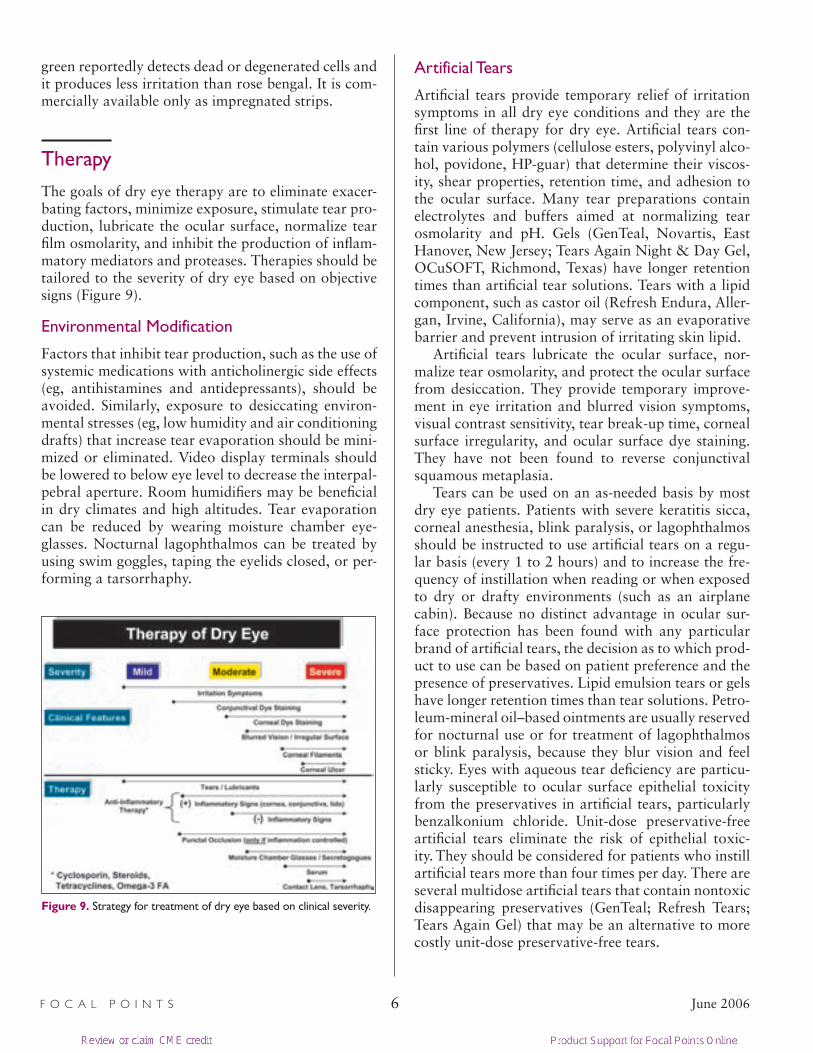
Staining with the diagnostic dyes fluorescein, rose bengal, or lissamine green is the most practical clinical method of assessing the severity of KCS. These dyes have different properties. Fluorescein staining occurs when the epithelial barrier is disrupted due to the loss of apical epithelial cells and/or the breakdown of the tight junctional complexes between superficial epithe-lia. Fluorescein staining is more easily observed in the cornea than the conjunctiva, and it is very well toler-ated by patients. Staining is performed with wet fluo-rescein strips or with a microliter drop of fluorescein solution. Corneal fluorescein staining, which is more easily visualized through a yellow filter, should be observed approximately 2 minutes after instilling the dye. Different patterns of corneal fluorescein stain-ing are seen, depending on the type of tear deficiency. Diffuse exposure zone staining is typically observed with aqueous tear deficiency (Figure 6), while inferior staining is usually seen with meibomian gland disease.
Staining will be limited to the exposed area in patients with lagophthalmos.
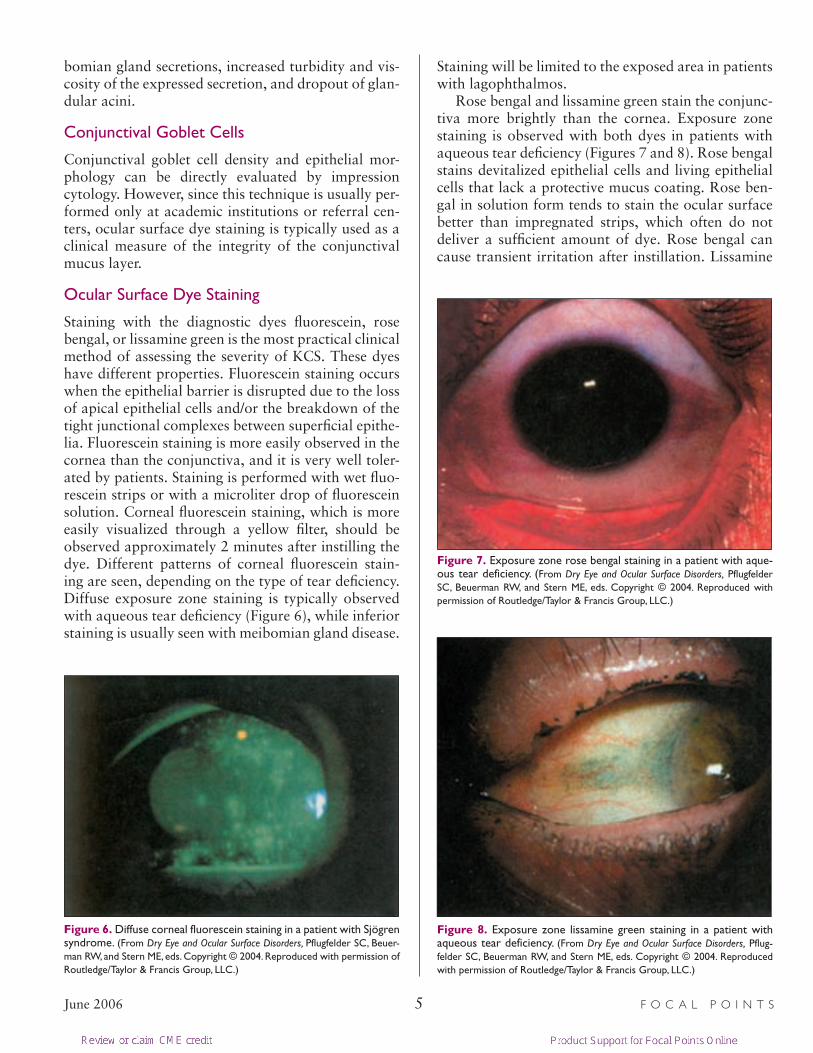
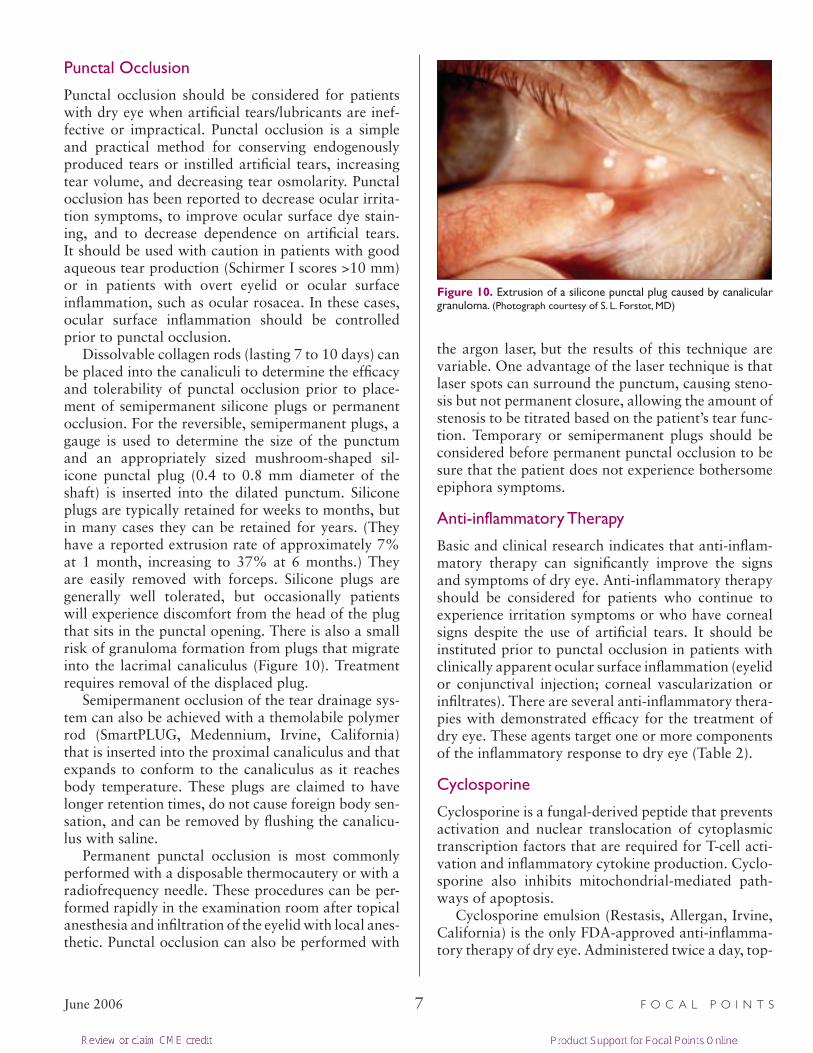
Rose bengal and lissamine green stain the conjunc-tiva more brightly than the cornea. Exposure zone staining is observed with both dyes in patients with aqueous tear deficiency (Figures 7 and 8). Rose bengal stains devitalized epithelial cells and living epithelial cells that lack a protective mucus coating. Rose ben-gal in solution form tends to stain the ocular surface better than impregnated strips, which often do not deliver a sufficient amount of dye. Rose bengal can cause transient irritation after instillation. Lissamine
Figure 6. Diffuse corneal fluorescein staining in a patient with Sjögren syndrome. (From Dry Eye and Ocular Surface Disorders, Pflugfelder SC, Beuer-man RW, and Stern ME, eds. Copyright © 2004. Reproduced with permission of Routledge/Taylor & Francis Group, LLC.)
Figure 7. Exposure zone rose bengal staining in a patient with aque-ous tear deficiency. (From Dry Eye and Ocular Surface Disorders, Pflugfelder SC, Beuerman RW, and Stern ME, eds. Copyright © 2004. Reproduced with permission of Routledge/Taylor & Francis Group, LLC.)
Figure 8. Exposure zone lissamine green staining in a patient with aqueous tear deficiency. (From Dry Eye and Ocular Surface Disorders, Pflug-felder SC, Beuerman RW, and Stern ME, eds. Copyright © 2004. Reproduced with permission of Routledge/Taylor & Francis Group, LLC.)
Mod_05_Jun06.indd 5 4/26/06 10:56:14 AM
F O C A L P O I N T S 6 June 2006
green reportedly detects dead or degenerated cells and it produces less irritation than rose bengal. It is com-mercially available only as impregnated strips.
Therapy
The goals of dry eye therapy are to eliminate exacer-bating factors, minimize exposure, stimulate tear pro-duction, lubricate the ocular surface, normalize tear film osmolarity, and inhibit the production of inflam-matory mediators and proteases. Therapies should be tailored to the severity of dry eye based on objective signs (Figure 9).
Environmental Modification
Factors that inhibit tear production, such as the use of systemic medications with anticholinergic side effects (eg, antihistamines and antidepressants), should be avoided. Similarly, exposure to desiccating environ-mental stresses (eg, low humidity and air conditioning drafts) that increase tear evaporation should be mini-mized or eliminated. Video display terminals should be lowered to below eye level to decrease the interpal-pebral aperture. Room humidifiers may be beneficial in dry climates and high altitudes. Tear evaporation can be reduced by wearing moisture chamber eye-glasses. Nocturnal lagophthalmos can be treated by using swim goggles, taping the eyelids closed, or per-forming a tarsorrhaphy.
Artificial Tears
Artificial tears provide temporary relief of irritation symptoms in all dry eye conditions and they are the first line of therapy for dry eye. Artificial tears con-tain various polymers (cellulose esters, polyvinyl alco-hol, povidone, HP-guar) that determine their viscos-ity, shear properties, retention time, and adhesion to the ocular surface. Many tear preparations contain electrolytes and buffers aimed at normalizing tear osmolarity and pH. Gels (GenTeal, Novartis, East Hanover, New Jersey; Tears Again Night & Day Gel, OCuSOFT, Richmond, Texas) have longer retention times than artificial tear solutions. Tears with a lipid component, such as castor oil (Refresh Endura, Aller-gan, Irvine, California), may serve as an evaporative barrier and prevent intrusion of irritating skin lipid.
Artificial tears lubricate the ocular surface, nor-malize tear osmolarity, and protect the ocular surface from desiccation. They provide temporary improve-ment in eye irritation and blurred vision symptoms, visual contrast sensitivity, tear break-up time, corneal surface irregularity, and ocular surface dye staining. They have not been found to reverse conjunctival squamous metaplasia.
Tears can be used on an as-needed basis by most dry eye patients. Patients with severe keratitis sicca, corneal anesthesia, blink paralysis, or lagophthalmos should be instructed to use artificial tears on a regu-lar basis (every 1 to 2 hours) and to increase the fre-quency of instillation when reading or when exposed to dry or drafty environments (such as an airplane cabin). Because no distinct advantage in ocular sur-face protection has been found with any particular brand of artificial tears, the decision as to which prod-uct to use can be based on patient preference and the presence of preservatives. Lipid emulsion tears or gels have longer retention times than tear solutions. Petro-leum-mineral oil–based ointments are usually reserved for nocturnal use or for treatment of lagophthalmos or blink paralysis, because they blur vision and feel sticky. Eyes with aqueous tear deficiency are particu-larly susceptible to ocular surface epithelial toxicity from the preservatives in artificial tears, particularly benzalkonium chloride. Unit-dose preservative-free artificial tears eliminate the risk of epithelial toxic-ity. They should be considered for patients who instill artificial tears more than four times per day. There are several multidose artificial tears that contain nontoxic disappearing preservatives (GenTeal; Refresh Tears; Tears Again Gel) that may be an alternative to more costly unit-dose preservative-free tears.
Figure 9. Strategy for treatment of dry eye based on clinical severity.
Mod_05_Jun06.indd 6 4/26/06 10:56:22 AM
June 2006 7 F O C A L P O I N T S
Punctal Occlusion
Punctal occlusion should be considered for patients with dry eye when artificial tears/lubricants are inef-fective or impractical. Punctal occlusion is a simple and practical method for conserving endogenously produced tears or instilled artificial tears, increasing tear volume, and decreasing tear osmolarity. Punctal occlusion has been reported to decrease ocular irrita-tion symptoms, to improve ocular surface dye stain-ing, and to decrease dependence on artificial tears. It should be used with caution in patients with good aqueous tear production (Schirmer I scores >10 mm) or in patients with overt eyelid or ocular surface inflammation, such as ocular rosacea. In these cases, ocular surface inflammation should be controlled prior to punctal occlusion.
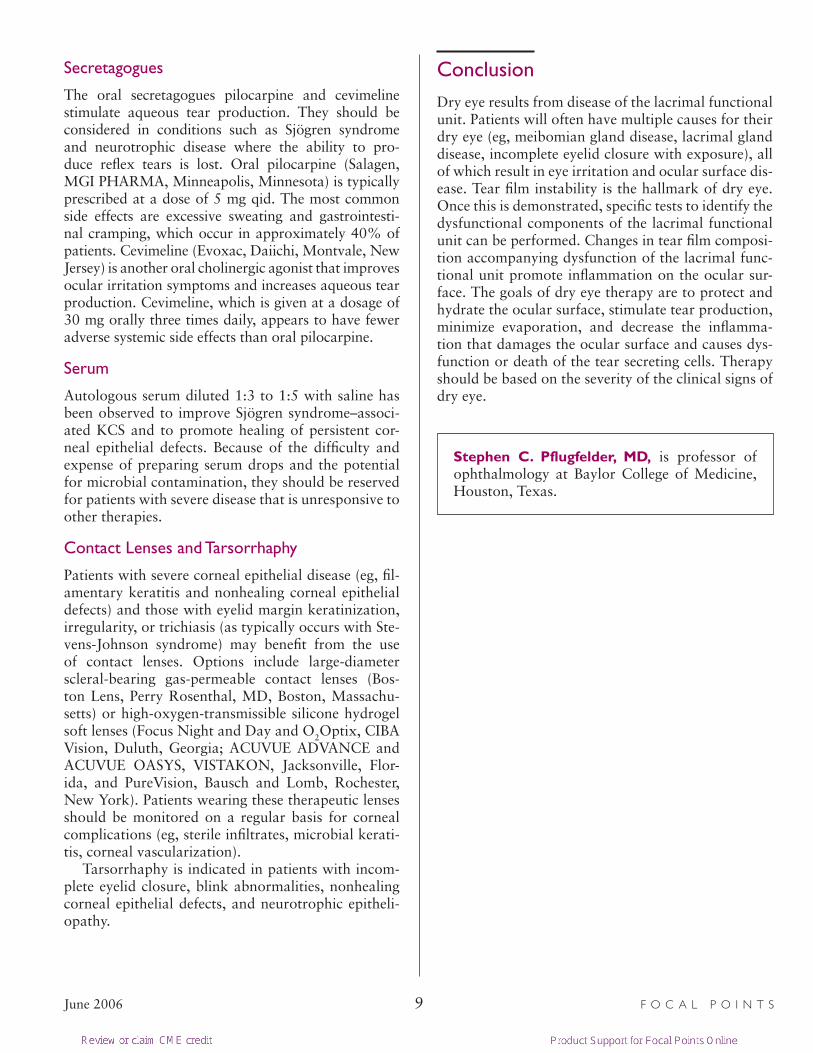
Dissolvable collagen rods (lasting 7 to 10 days) can be placed into the canaliculi to determine the efficacy and tolerability of punctal occlusion prior to place-ment of semipermanent silicone plugs or permanent occlusion. For the reversible, semipermanent plugs, a gauge is used to determine the size of the punctum and an appropriately sized mushroom-shaped sil-icone punctal plug (0.4 to 0.8 mm diameter of the shaft) is inserted into the dilated punctum. Silicone plugs are typically retained for weeks to months, but in many cases they can be retained for years. (They have a reported extrusion rate of approximately 7% at 1 month, increasing to 37% at 6 months.) They are easily removed with forceps. Silicone plugs are generally well tolerated, but occasionally patients will experience discomfort from the head of the plug that sits in the punctal opening. There is also a small risk of granuloma formation from plugs that migrate into the lacrimal canaliculus (Figure 10). Treatment requires removal of the displaced plug.
Semipermanent occlusion of the tear drainage sys-tem can also be achieved with a themolabile polymer rod (SmartPLUG, Medennium, Irvine, California) that is inserted into the proximal canaliculus and that expands to conform to the canaliculus as it reaches body temperature. These plugs are claimed to have longer retention times, do not cause foreign body sen-sation, and can be removed by flushing the canalicu-lus with saline.
Permanent punctal occlusion is most commonly performed with a disposable thermocautery or with a radiofrequency needle. These procedures can be per-formed rapidly in the examination room after topical anesthesia and infiltration of the eyelid with local anes-thetic. Punctal occlusion can also be performed with
the argon laser, but the results of this technique are variable. One advantage of the laser technique is that laser spots can surround the punctum, causing steno-sis but not permanent closure, allowing the amount of stenosis to be titrated based on the patient’s tear func-tion. Temporary or semipermanent plugs should be considered before permanent punctal occlusion to be sure that the patient does not experience bothersome epiphora symptoms.
Anti-inflammatory Therapy
Basic and clinical research indicates that anti-inflam-matory therapy can significantly improve the signs and symptoms of dry eye. Anti-inflammatory therapy should be considered for patients who continue to experience irritation symptoms or who have corneal signs despite the use of artificial tears. It should be instituted prior to punctal occlusion in patients with clinically apparent ocular surface inflammation (eyelid or conjunctival injection; corneal vascularization or infiltrates). There are several anti-inflammatory thera-pies with demonstrated efficacy for the treatment of dry eye. These agents target one or more components of the inflammatory response to dry eye (Table 2).
Cyclosporine
Cyclosporine is a fungal-derived peptide that prevents activation and nuclear translocation of cytoplasmic transcription factors that are required for T-cell acti-vation and inflammatory cytokine production. Cyclo-sporine also inhibits mitochondrial-mediated path-ways of apoptosis.
Cyclosporine emulsion (Restasis, Allergan, Irvine, California) is the only FDA-approved anti-inflamma-tory therapy of dry eye. Administered twice a day, top-
Figure 10. Extrusion of a silicone punctal plug caused by canalicular granuloma. (Photograph courtesy of S. L. Forstot, MD)
Mod_05_Jun06.indd 7 4/26/06 10:56:25 AM

F O C A L P O I N T S 8 June 2006
ical cyclosporine stimulates aqueous tear production by suppressing ocular surface and glandular inflam-mation and by inhibiting apoptosis (programmed cell death) of the tear producing epithelial cells in the lac-rimal glands and on the ocular surface. In clinical tri-als, cyclosporine emulsion was found to be effective in decreasing corneal fluorescein staining, improving blurred vision symptoms, and decreasing artificial tear use in patients with moderate to severe KCS. Clinical improvement may be observed within several weeks and continues for up to 6 months. Preliminary clini-cal experience suggests that cyclosporine may also be effective in patients with less severe disease. Cyclo-sporine emulsion is a nontoxic medication that can be continued indefinitely.
Corticosteroids
Topical corticosteroids also decrease ocular surface inflammation and have been reported to improve cor-neal epithelial disease in dry eye. They are most appro-priately used for pulse therapy, such as three or four times per day for 3 weeks, to minimize side effects. Clinical improvement is usually observed within a week and the therapeutic effect may be sustained for weeks or months after a pulse. Corticosteroid agents with minimal potential to raise intraocular pressure, such as fluorometholone and loteprednol etabonate, should be considered. Topical corticosteroids can be combined with other anti-inflammatory therapies, such as cyclo-sporine, to provide more rapid relief of symptoms and greater improvement of ocular surface disease.
Tetracyclines
Tetracyclines have numerous anti-inflammatory prop-erties. They inhibit the production of inflammatory cytokines, decrease nitric oxide production, and inhibit MMP production. The semisynthetic tetracycline doxy-cycline has been recognized to improve irritation symptoms, increase tear film stability, and decrease the severity of ocular surface disease in ocular rosacea.
Doxycycline has also been reported to be effective for treating recurrent corneal epithelial erosions.
Oral tetracyclines should be considered for patients with ocular rosacea, severe corneal epithelial disease, corneal vascularization, marginal infiltrates, nonheal-ing corneal epithelial defects, and corneal ulceration associated with tear film deficiency. Doxycycline, the best-tolerated tetracycline, is effective in doses of 20 to 50 mg orally twice a day. Patients should be treated for up to 4 weeks and, if they have an improvement in signs and symptoms, the medication can be stopped or tapered to once a day.
Essential Fatty Acids
There is increasing interest in treating dry eye with omega-3 essential fatty acid supplementation. These fatty acids, which are precursors to cell membrane phospholipids, are not present in sufficient quantity in the diet of many Americans. Omega-3 fatty acids have been observed to have anti-inflammatory activ-ity. They have been found to improve ocular irrita-tion symptoms and ocular surface epithelial disease in patients with dry eye. Certain foods, such as cold-water fish (salmon, cod), flax seed, and walnuts, are rich in omega-3 fatty acids. Numerous commercial supplements also contain omega-3 fatty acids.
Table 2. Mechanism of Action of Anti-inflammatory Therapies for Dry Eye
Agent Indications Mechanism of Action
Cyclosporine Dry eyeKCS
Inhibits T-cell activation and epithelial apoptosis
Corticosteroids KCSDelayed tear clearance
Inhibits MMPs, inflammatory cytokine/chemokines, and adhesion molecule production
Tetracyclines Ocular rosaceaKCS
Inhibits MMPs and IL-1 production
Autologous serum KCS Inhibits soluble proteases and inflammatory cytokines
KCS = keratoconjunctivitis sicca; MMP = matrix metalloproteinase; IL-1 = interleukin-1
(Adapted from The Ocular Surface by Stephen C. Pflugfelder, MD. Copyright 2003 by ETHIS COMMUNICATIONS INC. Reproduced with permission of ETHIS COMMUNICATIONS INC. In The Format Journal Via Copyright Clearance Center.)
Mod_05_Jun06.indd 8 4/26/06 10:56:25 AM
June 2006 9 F O C A L P O I N T S
Secretagogues
The oral secretagogues pilocarpine and cevimeline stimulate aqueous tear production. They should be considered in conditions such as Sjögren syndrome and neurotrophic disease where the ability to pro-duce reflex tears is lost. Oral pilocarpine (Salagen, MGI PHARMA, Minneapolis, Minnesota) is typically prescribed at a dose of 5 mg qid. The most common side effects are excessive sweating and gastrointesti-nal cramping, which occur in approximately 40% of patients. Cevimeline (Evoxac, Daiichi, Montvale, New Jersey) is another oral cholinergic agonist that improves ocular irritation symptoms and increases aqueous tear production. Cevimeline, which is given at a dosage of 30 mg orally three times daily, appears to have fewer adverse systemic side effects than oral pilocarpine.
Serum
Autologous serum diluted 1:3 to 1:5 with saline has been observed to improve Sjögren syndrome–associ-ated KCS and to promote healing of persistent cor-neal epithelial defects. Because of the difficulty and expense of preparing serum drops and the potential for microbial contamination, they should be reserved for patients with severe disease that is unresponsive to other therapies.
Contact Lenses and Tarsorrhaphy
Patients with severe corneal epithelial disease (eg, fil-amentary keratitis and nonhealing corneal epithelial defects) and those with eyelid margin keratinization, irregularity, or trichiasis (as typically occurs with Ste-vens-Johnson syndrome) may benefit from the use of contact lenses. Options include large-diameter scleral-bearing gas-permeable contact lenses (Bos-ton Lens, Perry Rosenthal, MD, Boston, Massachu-setts) or high-oxygen-transmissible silicone hydrogel soft lenses (Focus Night and Day and O2Optix, CIBA Vision, Duluth, Georgia; ACUVUE ADVANCE and ACUVUE OASYS, VISTAKON, Jacksonville, Flor-ida, and PureVision, Bausch and Lomb, Rochester, New York). Patients wearing these therapeutic lenses should be monitored on a regular basis for corneal complications (eg, sterile infiltrates, microbial kerati-tis, corneal vascularization).
Tarsorrhaphy is indicated in patients with incom-plete eyelid closure, blink abnormalities, nonhealing corneal epithelial defects, and neurotrophic epitheli-opathy.
Conclusion
Dry eye results from disease of the lacrimal functional unit. Patients will often have multiple causes for their dry eye (eg, meibomian gland disease, lacrimal gland disease, incomplete eyelid closure with exposure), all of which result in eye irritation and ocular surface dis-ease. Tear film instability is the hallmark of dry eye. Once this is demonstrated, specific tests to identify the dysfunctional components of the lacrimal functional unit can be performed. Changes in tear film composi-tion accompanying dysfunction of the lacrimal func-tional unit promote inflammation on the ocular sur-face. The goals of dry eye therapy are to protect and hydrate the ocular surface, stimulate tear production, minimize evaporation, and decrease the inflamma-tion that damages the ocular surface and causes dys-function or death of the tear secreting cells. Therapy should be based on the severity of the clinical signs of dry eye.
Stephen C. Pflugfelder, MD, is professor of ophthalmology at Baylor College of Medicine, Houston, Texas.
Mod_05_Jun06.indd 9 4/26/06 10:56:26 AM
F O C A L P O I N T S 10 June 2006
Clinicians’ Corner provides additional viewpoints on the subject covered in this issue of Focal Points. Consultants have been invited by the Editorial Review Board to respond to questions posed by the Acade-my’s Practicing Ophthalmolo-gists Advisory Committee for Education. While the advisory committee reviews the mod-ules, consultants respond with-out reading the module or one another’s responses.—Ed.
1. Where is dry eye therapy headed? Are there existing ther-apies that have not been ade-quately incorporated into prac-tice patterns?
Dr. Foulks: As our understand-ing of the pathogenesis of dry eye increases, our therapies are being directed at more specific aspects of dry eye disease. With respect to tear film instabil-ity, topical therapies are directed toward restoring aqueous, lipid, and mucin deficiencies of the tear film. With respect to the inflammatory aspects of dry eye disease, anti-inflammatory therapies that are more focused and that have fewer side effects are being included in management. Also, there are topical therapies in clinical trials now that may increase the array of ways we have to stimulate spe-cific tear components and function.
Dr. Friedlaender: Some trends include topical anti-inflammatory treatment of dry eye (cyclosporine, corticosteroids), cell receptor agonists that alter the flow of ions and mucin, and oral cholinergic agents that stimulate secretion from exocrine glands. None of these approaches are commonly used. Some are not yet approved, while others are inferior to stan-dard dry eye therapy (artificial tears, lubricating ointments, and punctal occlusion).
2. In patients referred with dry eye disorders, what do you most often see missed in terms of workup or treatment by the referring doctor?
Dr. Foulks: The most often under-recognized or undertreated aspect is meibomian gland dysfunction. Although patients have been advised to keep the eye-lids clean or to use eyelid scrubs, adequate instruction
in massage of the meibomian glands after the appli-cation of warm compresses is often not emphasized. My first duty is to instruct patients in the technique
of eyelid massage while also eval-uating other features of their dry eye disease. I give patients a writ-ten summary of the techniques of eyelid massage to remind them of the importance of the treatment and the most effective method of massage.
Dr. Friedlaender: Dry eye is overdiagnosed. Most often, doc-tors confuse dry eye with bleph-aritis.
3. How do you tailor your man-agement of chronic blepharitis that is associated with dry eye
syndrome?
Dr. Foulks: The first step in management of chronic blepharitis associated with dry eye disease is to identify whether the problem is anterior or poste-rior blepharitis and whether the condition is related to allergy, chronic low-grade infection, or obstruc-tive meibomian gland disease. I tailor the therapy to the underlying type of blepharitis and particu-larly I evaluate whether the patient has other seba-ceous gland dysfunction such as rosacea. While the primary management is based on local therapy of eyelid hygiene, meibomian gland massage, and judi-cious use of topical antibiotics and corticosteroids when indicated, I will frequently add systemic oral doxycycline or azithromycin if needed and continue it for a month or more. If patients are not respond-ing as anticipated, I ask them to demonstrate their method of eyelid massage in the office. Occasion-ally in a recalcitrant patient I will actually express the meibomian glands while the patient is in the office.
Dr. Friedlaender: I treat blepharitis the same, whether or not dry eye is present. This usually requires eyelid scrubs, and sometime an antibiotic/corticosteroid ointment to the eyelids at night.
4. Where do you put punctal occlusion in the treat-ment strategy for dry eye? How do you prefer to perform your occlusion?
Clinicians’ Corner
Mod_05_Jun06.indd 10 4/26/06 10:56:27 AM
June 2006 11 F O C A L P O I N T S
C L I N I C I A N S ’ C O R N E R
Dr. Foulks: I rely less on punctal occlusion now than I did 5 years ago. I do not occlude puncta unless I am sure that any inflammatory process has been ade-quately controlled. The one exception to this strat-egy is a patient with borderline dry eye who is wear-ing contact lenses with difficulty but who has little evidence of inflammation. In general, punctal occlu-sion is advised after beginning topical cyclosporine therapy if there is evidence of residual discomfort or persistent ocular surface staining. My preferred method of occlusion is to use a flexible punctal plug or the SmartPLUG insert (Medennium, Irvine, Cali-fornia). I do not like the deep canalicular plugs as I have seen some irritation and occasional infection with those devices.
Dr. Friedlaender: Punctal occlusion is highly effec-tive, and it is used when artificial tears and lubri-cating ointments are not adequate for comfort or ocular surface integrity. I prefer removable silicone plugs that fit snugly in the lower puncta.
5. Are there “experimental” or specialized tests for dry eye patients that are not routinely performed in general clinical practice but that you believe should be incorporated into general practice?
Dr. Foulks: Although I have used methods to ana-lyze for tear osmolarity and to measure lactoferrin in the evaluation of dry eye patients, these methods are not part of my routine workup or monitoring. If the equipment were more readily available and easier to use and maintain, those techniques could have merit, particularly in monitoring the effect of therapy.
Dr. Friedlaender: No.
6. How do you prepare a patient with severe dry eye for corneal transplantation?
Dr. Foulks: The most important preparation for patients with dry eye disease prior to corneal trans-plantation is to control meibomian gland disease. Therapy should be maximized to reduce inflamma-tion of the conjunctiva and eyelid margin, includ-ing the use of topical cyclosporine and pulse topical corticosteroids if necessary. It is important to assess the extent of eyelid protection of the surface and the
integrity of the patient’s blink. If there is concern about potential postoperative exposure, part of the immediate postoperative management can include partial closure of the eyelid with an eyelid suture that is removed once the integrity of the corneal graft epi-thelium is confirmed.
Dr. Friedlaender: I instruct the patient to perform liberal pre- and postoperative lubrication of the ocular surface, with artificial tears during the day and ointment or gel at night.
7. How well do autologous serum tears really work? When should clinicians go to the trouble of having these specially prepared?
Dr. Foulks: Autologous serum tears can be highly effective in improving the integrity of the ocular sur-face but are a particular nuisance for both the pre-paring ophthalmologist and the patient. I reserve autologous serum tears for patients with significant epitheliopathy, particularly those with recurrent ero-sive breakdown of the corneal epithelium. I prepare the autologous serum as a 20% solution in 3 ml unpreserved artificial tears and instruct the patient to store unopened containers in the freezer and opened containers in the refrigerator. If other modalities have failed, autologous serum–enhanced tears are worth considering for short-term therapy.
Dr. Friedlaender: I do not use autologous serum, since it is inconvenient and probably no better than commercially available lubricants.
8. How do secondary systemic causes of dry eye syndrome, such as rheumatological diseases or sar-coidosis, differ in presentation and treatment from more common dry eye states?
Dr. Foulks: The autoimmune-associated dry eye states usually are more severe and have the asso-ciated features of inflammatory eye disease. Often the epitheliopathy is more severe, and filamentary keratopathy is frequently present. Mucous and inflammatory debris in the inferior tear meniscus is usually more prominent as well. My approach is to be more aggressive with anti-inflammatory ther-apy; I often use simultaneous cyclosporine and rap-idly tapered topical corticosteroids. If patients have
Mod_05_Jun06.indd 11 4/26/06 10:56:28 AM
F O C A L P O I N T S 12 June 2006
C L I N I C I A N S ’ C O R N E R
not been following their systemic anti-inflamma-tory therapy as prescribed, I emphasize their com-pliance with the therapy prescribed by the rheuma-tologist. This is the group of patients in which I will consider autologous serum therapy if the response to the standard anti-inflammatory therapy is not optimal.
Dr. Friedlaender: They tend to be more severe, and they are usually associated with dryness elsewhere in the body, especially the mouth.
9. How do systemic anti-inflammatory medications affect dry eye syndrome?
Dr. Foulks: Although systemic anti-inflammatory therapy is often an important part of the manage-ment of patients whose systemic autoimmune dis-ease is the basis of their dry eye, most patients with dry eye do not require systemic anti-inflammatory agents, and such agents are not justified because of
the possibility of adverse risk or side effects. The use of systemic essential fatty acid supplementation as an anti-inflammatory strategy in treating dry eye is appealing and early clinical trials are promising, but this therapy requires further validation.
Dr. Friedlaender: Corticosteroids, immunosuppres-sive drugs, and antimalarials may improve dry-ness slightly. Nonsteroidal anti-inflammatory drugs probably have no effect.
Gary N. Foulks, MD, FACS, is a practicing oph-thalmologist at the University of Louisville in Lou-isville, Kentucky.
Mitchell Friedlaender, MD, is head of the Division of Ophthalmology at Scripps Clinic in La Jolla, California, and an adjunct professor at the Scripps Research Institute.
Mod_05_Jun06.indd 12 4/26/06 10:56:29 AM

June 2006 13 F O C A L P O I N T S
S U G G E S T E D R E A D I N G
Avunduk AM, Avunduk MC, Varnell ED, et al. The comparison of efficacies of topical corticosteroids and nonsteroidal anti-inflammatory drops on dry eye patients: a clinical and immu-nocytochemical study. Am J Ophthalmol. 2003;136:593–602.
Balaram M, Schaumberg DA, Dana MR. Efficacy and toler-ability outcomes after punctal occlusion with silicone plugs in dry eye syndrome. Am J Ophthalmol. 2001;131:30–36.
Lemp MA (chairman). Report of the National Eye Institute/Industry workshop on Clinical Trials in Dry Eyes. CLAO J. 1995;21:221–232.
Pflugfelder SC. Anti-inflammatory therapy for dry eye. Am J Ophthalmol. 2004;137:337–342.
Pflugfelder SC, Solomon A. Dry eye. In: Holland EJ, Mannis MJ, eds. Ocular Surface Disease: Medical and Surgical Man-agement. Heidelberg: Springer; 2001.
Pflugfelder SC, Beuerman RW, Stern ME, eds. Dry Eye and Ocular Surface Disorders. New York: Marcel Dekker; 2004.
Pflugfelder SC, Maskin SL, Anderson B, et al. A randomized, double-masked, placebo-controlled, multicenter comparison of loteprednol etabonate ophthalmic suspension, 0.5%, and placebo for treatment of keratoconjunctivitis sicca in patients
with delayed tear clearance. Am J Ophthalmol. 2004;138:444–457.
Pflugfelder SC, Solomon A, Stern ME. The diagnosis and management of dry eye: a twenty-five-year review. Cornea. 2000;19:644–649.
Sall K, Stevenson OD, Mundorf TK, et al. Two multicenter, randomized studies of the efficacy and safety of cyclosporine ophthalmic emulsion in moderate to severe dry eye disease. CsA Phase 3 Study Group. Ophthalmology. 2000;107:631–639.
Stern ME, Beuerman RW, Fox RI, et al. The pathology of dry eye: the interaction between the ocular surface and lacrimal glands. Cornea. 1998;17:584–589.
Tseng SC, Tsubota K. Important concepts for treating ocular surface and tear disorders. Am J Ophthalmol. 1997;124:825–835.
Related Academy MaterialsBlepharitis. Preferred Practice Pattern, 2003.
Dry Eye Syndrome. Preferred Practice Pattern, 2003.
External Disease and Cornea. Basic and Clinical Science Course, Section 8, 2005–2006.
Mod_05_Jun06.indd 13 4/26/06 10:56:30 AM