1993 clinico-pathological conferencearchive.nmji.in/.../clinico-pathological-conference.pdf ·...
TRANSCRIPT
228 THENATIONALMEDICALJOURNALOFINDIA VOL.6, NO.5, 1993
Clinico-pathological Conference
A young female with a stroke and limb gangrene
POSTGRADUATE INSTITUTE OF MEDICAL EDUCATION AND RESEARCH,
CHANDIGARH
THE CASEA 24-year-old woman who had delivered a full term normalbaby at home, two-and-a-half months ago, was found un-conscious in a drain. She regained consciousness 15 minutesafter being found and was then noticed to have diminishedmovements of the right upper and lower limbs. At the firstexamination in our hospital we found that she had aphasiaand right hemiplegia. There was right upper motor neuroneVII nerve palsy, grade 0-1 power in the right upper and lowerlimbs and mute plantar responses. There was no precedinghistory of headache or vomiting.
The haemoglobin was 9.3 g/dl and the total leucocytecount was 12 OOO/cmmwith 88% polymorphonuclear leuco-cytes. The reticulocyte count was 3% and the erythrocytesedimentation rate (ESR) was 20 mm in the first hour. Herperipheral blood smear showed mild anisocytosis with micro-cytes, macrocytes and a few spherocytes; the number ofplatelets seemed to be adequate. The serum biochemistryand chest X-ray were normal.
Echocardiography showed a normal mitral valve with theposterior valve leaflet moving posteriorly. No vegetationswere seen.
Computerized tomographic (CT) scanning of the headrevealed a haemorrhagic infarct with 'luxury' perfusion in theterritory of the left middle cerebral artery (MCA). She was,therefore, diagnosed to have had a left MCA thromboembolicstroke. She showed remarkable improvement with anti-platelet drugs and was discharged on dispirin.
She was re-admitted a month later, with a history ofgradual swelling and a blackish discoloration of the left footover the preceding ten days. There was no history of fever,chest pain, sudden breathlessness, cough, skin rash, jointpains, Raynaud's phenomenon, oral ulceration, photo-sensitivity, haematuria, urinary disturbance or intake of oralcontraceptives.
Examination revealed no peripheral signs of infectiveendocarditis. The left foot showed gangrene up to the anklewith induration extending further up the leg. The right footfelt cold. The left femoral and right posterior tibial arterypulses were hot palpable and the left radial pulse was weak.The carotid, subclavian and brachial pulses were normal.
Her blood pressure was 156/94 mmHg in the left arm,126/90 in the right arm, 200/144 in the right leg and it couldnot be recorded in the left leg. The jugular venous pressurewas not raised. There was a pansystolic murmur at the apexof the heart radiating to the axilla. The heart sounds werenormal and there were no added sounds. The chest was clear
and the liver and spleen were not palpable. Central nervoussystem examination showed that there was a right uppermotor neurone VII nerve palsy, right-sided hemiplegia andnormal power in the left limbs. All the reflexes were brisk onthe right side with upgoing plantars. Fundoscopy showedgrade II hypertensive changes.
The patient was started on heparin, gentamycin, cloxacillinand metronidazole. A below-knee amputation of the left legwas attempted, but as the muscles did not bleed, this wasconverted to an above-knee amputation. A 12 em clot wasextracted from the left femoral artery using a ballooncatheter. Two days after the operation, the patient hada cardiac arrest and could not be revived.
DIFFERENTIAL DIAGNOSISDR HARINDERK. BALI:This young lady delivered a full-termbaby two-and-a-half months ago under unsupervised,probably unsterile conditions and then developed right-sidedhemiplegia due to a haemorrhagic infarct in the territory ofthe left middle cerebral artery. During this time she wasdiagnosed to have mild mitral regurgitation and polymorpho-nuclear leucocytosis. All other investigations to find a causefor the stroke were negative and she was discharged onantiplatelet drugs. Subsequently, after a short period whenshe remained relatively asymptomatic she developedgangrene of her left foot. Clinical examination at this timerevealed the left femoral, right posterior tibial and rightdorsalis pedis arterial pulses to be absent and the right radialpulse to be weak. Before she died her right carotid arterypulse was found to be weak, both brachials were absent andgangrene developed in both upper limbs.
This patient therefore had occlusive disease of the largevessels-the carotid, subclavian and femoral arteries. Theocclusion of the vessels appeared suddenly with the develop-ment of gangrene. The history and clinical examination didnot suggest that there was any long-standing stenotic diseaseof her arteries. There are three conditions which can producesuch a clinical picture. I think the first possibility is occlusionfrom an embolus arising from the heart or the ascending aorta.The embolus can originate from a thrombus, vegetation ortumour. The points under discussion in this patient are,therefore, the nature of her mitral regurgitation and theembolizing material.
Rheumatic mitral valve disease with a thrombus in the leftatrium is the commonest source of such an occlusion. Asclinical examination and echocardiography have excluded thepossibility of rheumatic disease, I shall not discuss this any
CLINICO-PATHOLOGICALCONFERENCE
further. Infective endocarditis is another common cause ofperipheral embolization. In fact, most features in this patientsupport a diagnosis of infective endocarditis. She developedthe disease a few weeks after an unsupervised home deliveryand the presence of mitral regurgitation, microscopichaematuria, peripheral embolization and a progressivelyrising ESR complete the picture. Although there is no argu-ment against a diagnosis of infective endocarditis, otherconditions which closely mimic this disease also needconsideration.
At this point, I would like to highlight a few importantfeatures in the clinical protocol. The mitral regurgitationwas mild and did not progress over a period of time, asevidenced by the absence of left atrial and left ventricularenlargement on echocardiography as well as the absence ofheart failure. Secondly, she had relatively large vesselembolization. Thirdly, she had constantly raised polymorpho-nuclear leucocyte counts. These features indicate that shehad a large polypoidal vegetation on normal valves and thatthe infective process had not caused major damage to theleaflets. Both these features suggest infection by a relativelyless virulent organism on a normal valve or infection of analready diseased valve by a common organism such as Strep-tococcus viridans. Mitral valve prolapse (MVP) is a commonlesion which may cause no haemodynamic instability and yetdevelop infection. It is considered by pathologists to be anexample of normal valve endocarditis. Organisms such ascertain Gram-negative bacteria may infect normal valves andcause large vegetations without much destruction of thevalve tissue. However, most often these organisms causeendocarditis in a patient who is in an immunocompromisedstate. Our patient did not have any evidence to suggest thatshe was, although, some workers would include the puer-perium in this category. 1
Myxomas are the commonest intracardiac tumours and theleft atrium is a common site for their occurrence. They have,however, been described in all the cardiac chambers andeven on valves. In fact, a case of myxoma on the tricuspidvalve has been described from this Institute.? Myxomas mayembolize into peripheral vessels either spontaneously orafter becoming infected particularly with Staphylococcusalbus. They usually present as obstruction to the left atrialinflow or as mitral regurgitation. However, peripheralembolization may be the only presenting feature. I do notthink our patient had a myxoma as echocardiography hadshown nodules on the mitral valve and in an extensive reviewof the literature I could not find any report of a myxoma onthe mitral valve. Moreover, I will have to postulate thatthe myxoma was present on both leaflets of the valve. Thepresence of polymorphonuclear leucocytosis with a shift tothe left is another feature against this diagnosis.
Could it be a case of in situ thrombus formation in thevessels? Thrombosis may occur in arteries in a variety ofdiseases such as protein C, protein S and anti-thrombin IIIdeficiency. However, I do not think that any of these condi-tions is likely because in all of them venous rather thanarterial thrombosis is common and moreover it will notexplain the presence of the cardiac lesion and the poly-morphonuclear leucocytosis. A condition which should beconsidered is the presence of antiphospholipid antibodyor lupus anticoagulant. Although lupus anticoagulant wasoriginally described in systemic lupus erythematosus (SLE),
229
it has been reported in some normal individuals as wellas those with other collagen disorders, viral infections,malignancies and after the intake of certain drugs.
Recently, a syndrome called primary anti phospholipid(PAPS) disorder has been described. Its salient features arevenous and arterial thromboses, thrombocytopenia andpulmonary thromboembolism. Our patient had some featuresof PAPS because some cardiac lesions have been describedin this condition. In a recent series+involvement ofthe mitraland aortic valve producing regurgitation were found to be thecommonest lesions and occurred in as many as 30% ofpatients. The valves have either localized or diffuse thicken-ing and the regurgitation so produced may vary in severity.At times it may be difficult on echocardiography to differen-tiate the nodules on these valves from those produced byinfective endocarditis. However, I do not think. PAPS is alikely diagnosis because there was no thrombocytopenia andno history of repeated foetal loss-two important features ofthis syndrome. Moreover such a diagnosis does not accountfor the polymorphonuclear ieucocytosis or the raised ESR.
Could this be some form of vasculitis? I think the onlytype of vasculitis which comes to my mind is non-specificaortoarteritis. There is inequality of the arterial pulses andhypertension. But in this patient there was no bruit over anyvessel and gangrene of the limbs is very uncommon in non-specific aortoarteritis.
DR HARINDER BALI'S DIAGNOSIS
- Infective endocarditis of a morphologically normal mitralvalve (probably fungal) with embolism to the left femoral,both axillary, right carotid and renal arteries.
CLINICAL DISCUSSIONDR S. K. MEHTA:Before further discussion I would like to
make a clarification. It has been mentioned in the file thatthere was a left supraclavicular lymph node, 2 to 3 ern indiameter. This, I think, should not have been ignored.
DR S. K. PRABHAKAR:When a young patient presents witha stroke, endocarditis has first to be ruled out. During herfirst admission, the peripheral pulses were normal and theechocardiogram showed no endocarditis. During the secondadmission the patient had mitral valve vegetations, evidenceof multiple emboli and infection. I think the most likelydiagnosis is an infective endocarditis.
PATHOLOGICAL DISCUSSIONDR KUSUM JOSHI: An incomplete autopsy (without removalof the brain) was performed. The left leg had been amputatedand the other limbs showed peripheral discoloration andearly gangrene. The amputated leg specimen confirmed thepresence of gangrene. There were fresh thrombi in thefemoral and popliteal arteries and veins and organizingthrombi with luminal occlusion and recanalization in thesmaller arteries. There was no vasculitis.
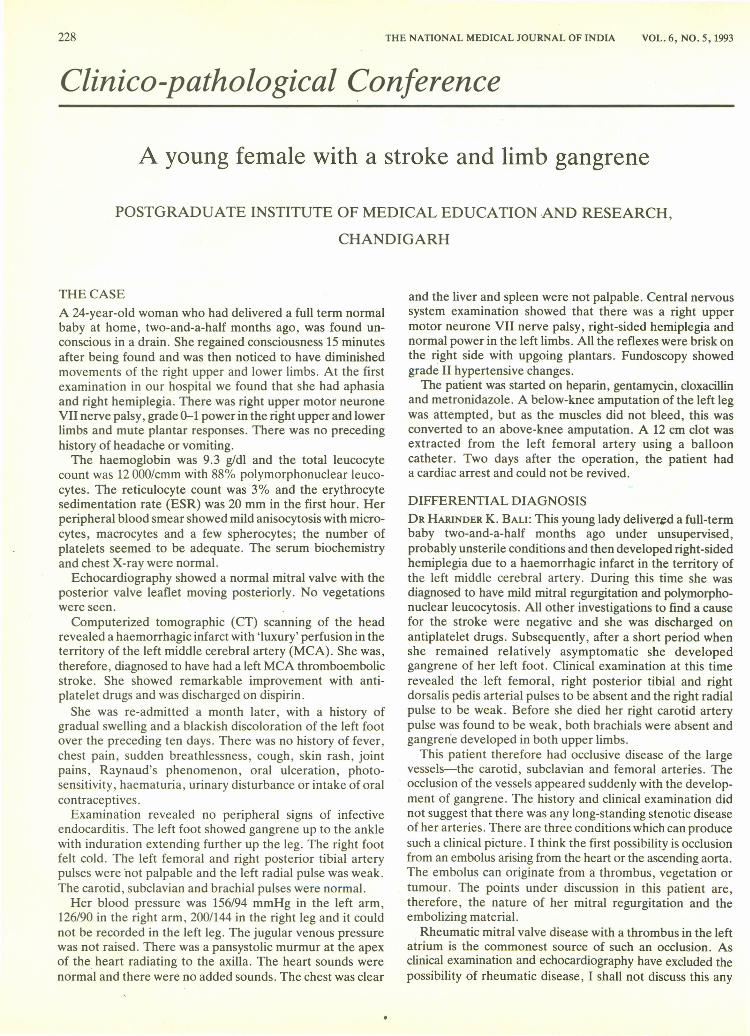
The heart weighed 240 g. There were large friable vegeta-tions along the line of closure of a normal mitral valve.The vegetations did not extend to the undersurface of thevalve and there was no destruction of the valve cusp. Thecommissures and chordae tendineae were normal (Fig. 1).Microscopically, the vegetations were bland and fibrinous.There were no bacteria or fungi. These are all features ofnon-bacterial thrombotic endocarditis. The lungs together
230
FiG 1. Gross photograph of the heart showing largepolypoidal vegetation on the mitral valve. Note the normalcommissures and chordae tendineae
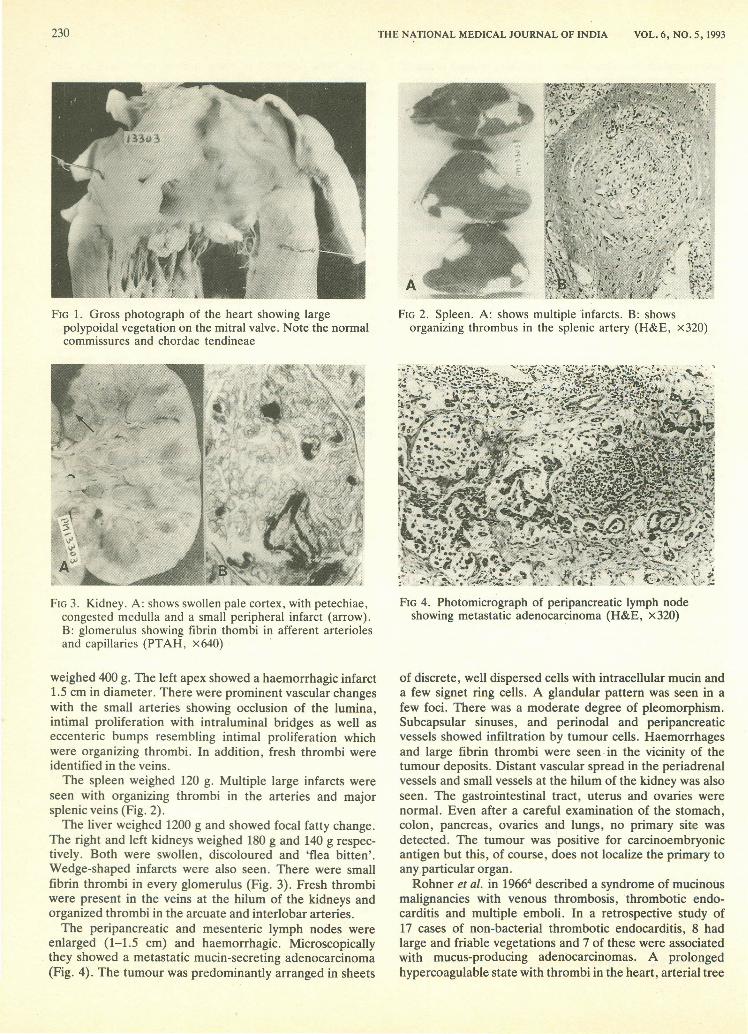
FIG3. Kidney. A: shows swollen pale cortex, with petechiae,congested medulla and a small peripheral infarct (arrow).B: glomerulus showing fibrin thombi in afferent arteriolesand capillaries (PTAH, x640) .
weighed 400 g. The left apex showed a haemorrhagic infarct1.5 em in diameter. There were prominent vascular changeswith the small arteries showing occlusion of the lumina,intimal proliferation with intraluminal bridges as well aseccenteric bumps resembling intimal proliferation whichwere organizing thrombi. In addition, fresh thrombi wereidentified in the veins.
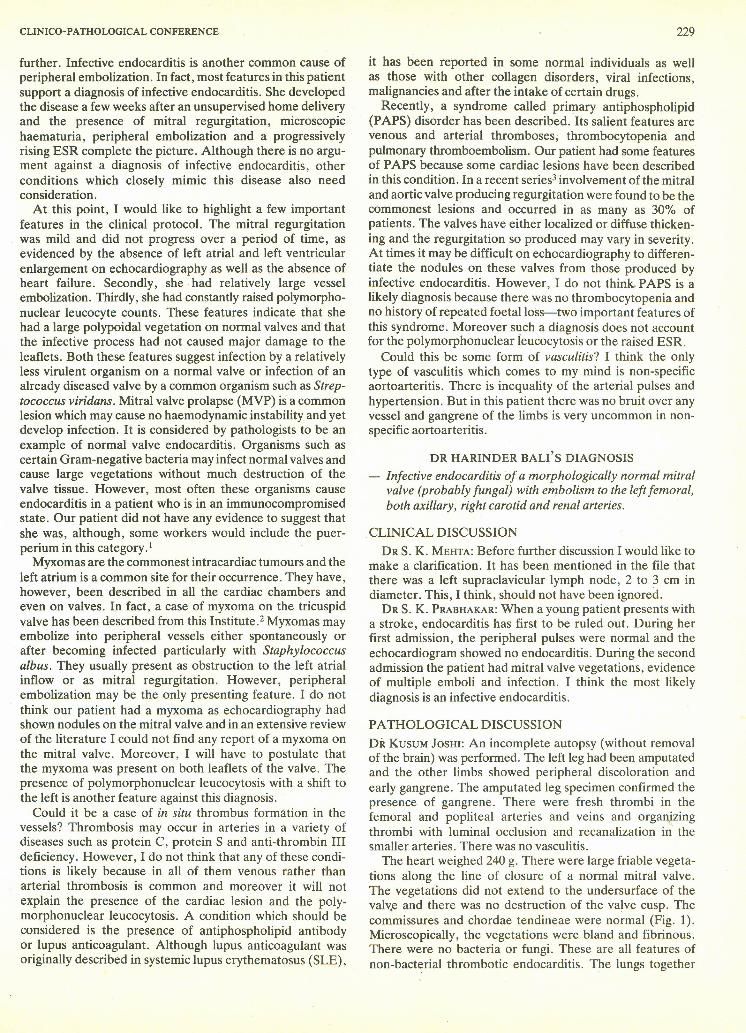
The spleen weighed 120 g. Multiple large infarcts wereseen with organizing thrombi in the arteries and majorsplenic veins (Fig. 2).
The liver weighed 1200 g and showed focal fatty change.The right and left kidneys weighed 180 g and 140 g respec-tively. Both were swollen, discoloured and 'flea bitten'.Wedge-shaped infarcts were also seen. There were smallfibrin thrombi in every glomerulus (Fig. 3). Fresh thrombiwere present in the veins at the hilum of the kidneys andorganized thrombi in the arcuate and interlobar arteries.
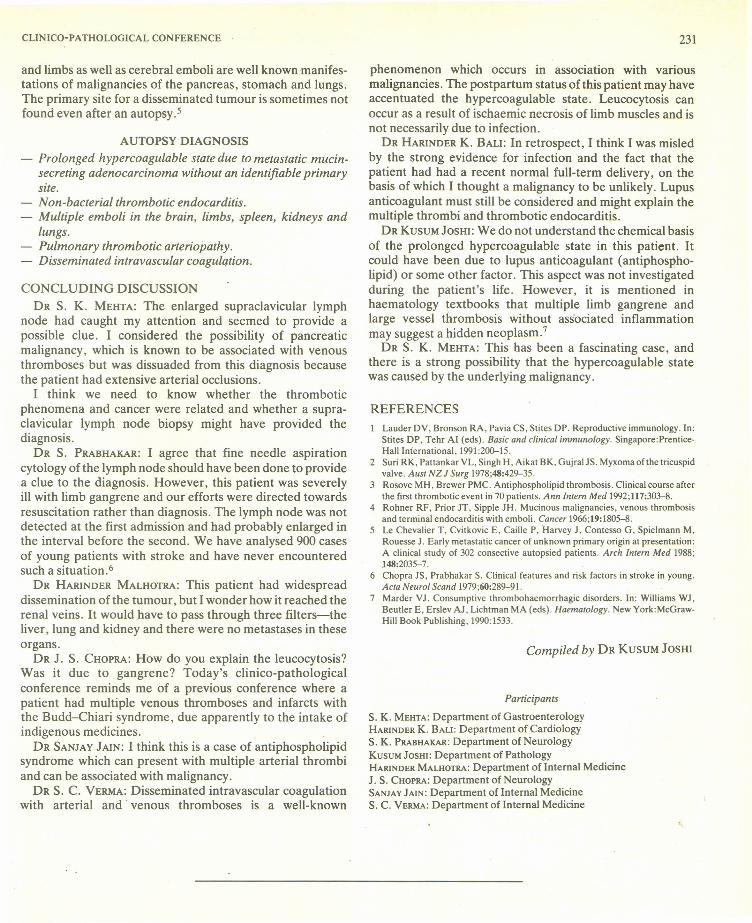
The peri pancreatic and mesenteric lymph nodes wereenlarged (1-1.5 ern) and haemorrhagic. Microscopicallythey showed a metastatic mucin-secreting adenocarcinoma(Fig. 4). The tumour was predominantly arranged in sheets
THE NATIONAL MEDICAL JOURNAL OF INDIA VOL. 6, NO.5, 1993
FiG 2. Spleen. A: shows multiple Infarcts, B: showsorganizing thrombus in the splenic artery (H&E, x320)
FIG 4. Photomicrograph of peripancreatic lymph nodeshowing metastatic adenocarcinoma (H&E, x320)
of discrete, well dispersed cells with intracellular mucin anda few signet ring cells. A glandular pattern was seen in afew foci. There was a moderate degree of pleomorphism.Subcapsular sinuses, and perinodal and peripancreaticvessels showed infiltration by tumour cells. Haemorrhagesand large fibrin thrombi were seen· in the vicinity of thetumour deposits. Distant vascular spread in the peri adrenalvessels and small vessels at the hilum of the kidney was alsoseen. The gastrointestinal tract, uterus and ovaries werenormal. Even after a careful examination of the stomach,colon, pancreas, ovaries and lungs, no primary site wasdetected. The tumour was positive for carcinoembryonicantigen but this, of course, does not localize the primary toany particular organ.
Rohner et al. in 19664 described a syndrome of mucinousmalignancies with venous thrombosis,thrombotic endo-carditis and multiple emboli. In a retrospective study of17 cases of non-bacterial thrombotic endocarditis, 8 hadlarge and friable vegetations and 7 of these were associatedwith mucus-producing adenocarcinomas. A prolongedhypercoagulable state with thrombi in the heart, arterial tree
CLINICO-PATHOLOGICALCONFERENCE
and limbs as well as cerebral emboli are well known manifes-tations of malignancies of the pancreas, stomach and lungs.The primary site for a disseminated tumour is sometimes notfound even after an autopsy. 5
AUTOPSY DIAGNOSIS- Prolonged hypercoagulable state due to metastatic mucin-
secreting adenocarcinoma without an identifiable primarysite.
- Non-bacterial thrombotic endocarditis.- Multiple emboli in the brain, limbs, spleen, kidneys and
lungs.- Pulmonary thrombotic arteriopathy,- Disseminated intravascular coagulation.
CONCLUDING DISCUSSIONDR S. K. MEHTA: The enlarged supraclavicular lymph
node had caught my attention and seemed to provide apossible clue. I considered the possibility of pancreaticmalignancy, which is known to be associated with venousthromboses but was dissuaded from this diagnosis becausethe patient had extensive arterial occlusions.
I think we need to know whether the thromboticphenomena and cancer were related and whether a supra-clavicular lymph node biopsy might have provided thediagnosis.
DR S. PRABHAKAR:I agree that fine needle aspirationcytology of the lymph node should have been done to providea clue to the diagnosis. However, this patient was severelyill with limb gangrene and our efforts were directed towardsresuscitation rather than diagnosis. The lymph node was notdetected at the first admission and had probably enlarged inthe interval before the second. We have ana lysed 900 casesof young patients with stroke and have never encounteredsuch a situation. 6
DR HARINDERMALHOTRA:This patient had widespreaddissemination of the tumour, but I wonder how it reached therenal veins. It would have to pass through three filters-theliver, lung and kidney and there were no metastases in theseorgans.
DR J. S. CHOPRA:How do you explain the leucocytosis?Was it due to gangrene? Today's clinico-pathologicalconference reminds me of a previous conference where apatient had multiple venous thromboses and infarcts withthe Budd-Chiari syndrome, due apparently to the intake ofindigenous medicines.
DR SANJAYJAIN: I think this is a case of antiphospholipidsyndrome which can present with multiple arterial thrombiand can be associated with malignancy.
DR S. C. VERMA:Disseminated intravascular coagulationwith arterial and venous thromboses is a well-known
231
phenomenon which occurs in association with variousmalignancies. The postpartum status of this patient may haveaccentuated the hypercoagulable state. Leucocytosis canoccur as a result of ischaemic necrosis of limb muscles and isnot necessarily due to infection.
DR HARINDERK. BALI: In retrospect, I think I was misledby the strong evidence for infection and the fact that thepatient had had a recent normal full-term delivery, on thebasis of which I thought a malignancy to be unlikely. Lupusanticoagulant must still be considered and might explain themultiple thrombi and thrombotic endocarditis.
DR KUSUMJOSHI:We do not understand the chemical basisof the prolonged hypercoagulable state in this patient. Itcould have been due to lupus anticoagulant (antiphospho-lipid) or some other factor. This aspect was not investigatedduring the patient's life. However, it is mentioned inhaematology textbooks that multiple limb gangrene andlarge vessel thrombosis without associated inflammationmay suggest a hidden neoplasm."
DR S. K. MEHTA:This has been a fascinating case, andthere is a strong possibility that the hypercoagulable statewas caused by the underlying malignancy.
REFERENCESLauder DV, Bronson RA, Pavia CS, Stites OP. Reproductive immunology. In:Stites OP, Tehr AI (eds). Basic and clinical immunology. Singapore.Prentice-Hall International, 1991:200-15.
2 Suri RK, Pattankar VL, Singh H, Aikat BK, GujralJS. Myxoma of the tricuspidvalve. AU5tNZ J Surg 1978;48:429-35.
3 Rosove MH, Brewer PMC. Antiphospholipid thrombosis. Clinical course afterthe first thrombotic event in 70 patients. Ann Intern Med 1992;117:303-8.
4 Rohner RF, Prior JT, Sipple JH. Mucinous malignancies, venous thrombosisand terminal endocarditis with emboli. Cancer 1966;19:1805-8.
5 Le Chevalier T, Cvitkovic E, Caille P, Harvey J, Contesso G, Spielmann M,Rouesse J. Early metastatic cancer of unknown primary origin at presentation:A clinical study of 302 consective autopsied patients. Arch Intern Med 1988;148:2035-7.
6 Chopra JS, Prabhakar S. Clinical features and risk factors in stroke in young.Acta Neurol Scand 1979;60:289-91.
7 Marder VJ. Consumptive thrombohaemorrhagic disorders. In: Williams WJ,Beutler E, Erslev AJ, Lichtman MA (eds). Haematology. New York:McGraw-Hill Book Publishing, 1990: 1533.
Compiled by DR KUSUMJOSHI
Participants
S. K. MEHTA: Department of GastroenterologyHARINDERK. BALI: Department of CardiologyS. K. PRABHAKAR:Department of NeurologyKUSUMJOSHI: Department of PathologyHARINDERMALHOTRA:Department of Internal MedicineJ. S. CHOPRA:Department of NeurologySANJAYJAIN: Department of Internal MedicineS. C. VERMA:Department of Internal Medicine