14th annual healthworld conference does health matter?. ahmad ha… · of nhpas included...
TRANSCRIPT

MOVING ONTO A SUSTAINABLE HEALTHCARE MODEL:
Evidence-based Health Care Reform
October 20th, 2015
Haseeb Ahmad
President of the Pharmaceutical
Companies Committee
Managing Director Greece, Cyprus, Malta
14th Annual Healthworld Conference
Does Health Matter?

The Greek health care maze is delivering suboptimal
outcomes
Primary Care Doctors Specialists Diagnostic Imaging
PayersPharmaciesHospitals
Limited access to relevant
information at point of care
Operate in silos Overuse/Underuse/Misuse
Mired in administrative
complexity
Not integrated in to care
delivery system
Rewarded for
volume not value
Patients experience a highly fragmented system
fraught with challenges
Patients do not receive best available care

The Greek Healthcare System
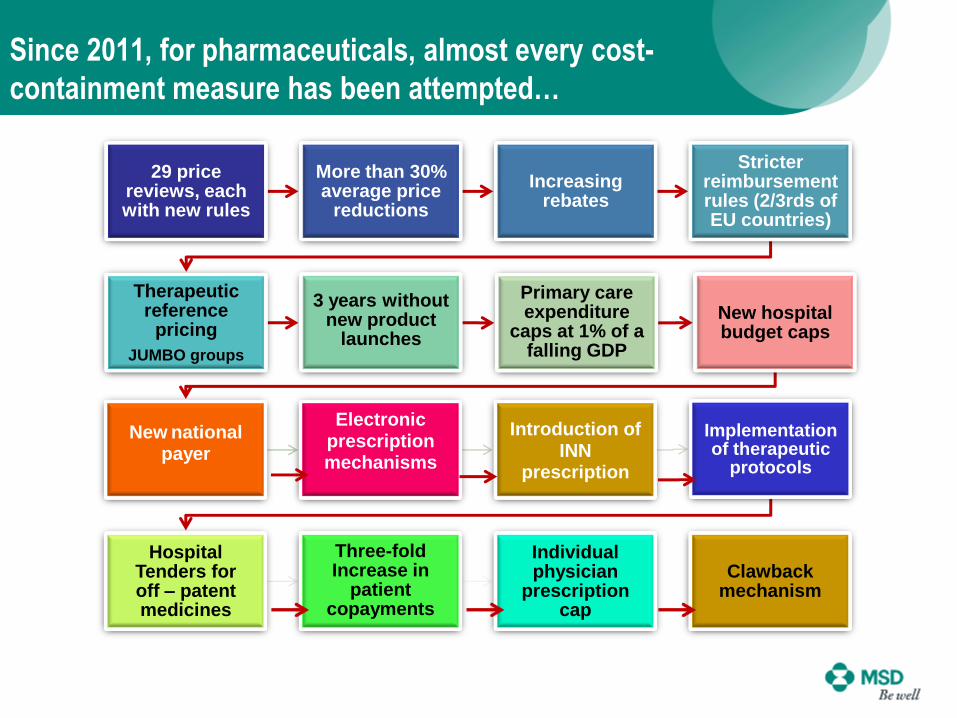
Since 2011, for pharmaceuticals, almost every cost-
containment measure has been attempted…
29 price reviews, each with new rules
More than 30% average price
reductions
Increasing rebates
Stricter reimbursement rules (2/3rds of EU countries)
Therapeutic reference
pricing
JUMBO groups
3 years without new product
launches
Primary care expenditure
caps at 1% of a falling GDP
New hospital budget caps
New nationalpayer
Electronic prescription mechanisms
Introduction of INN
prescription
Implementation of therapeutic
protocols
Hospital Tenders for off – patent medicines
Three-fold Increase in
patient copayments
Individual physician
prescription cap
Clawback mechanism

We need a Vision & Roadmap to an efficient and sustainable
health care system
Patient centric system
Focus on health outcomes
Financial sustainability
Silo based
Expenditure focused
Horizontal measures

MSD Vision: Combine and Prevention, Quality and Efficiency
Prevention &
Primary Care
Efficiency through
Funding Choices
Quality &
Innovation
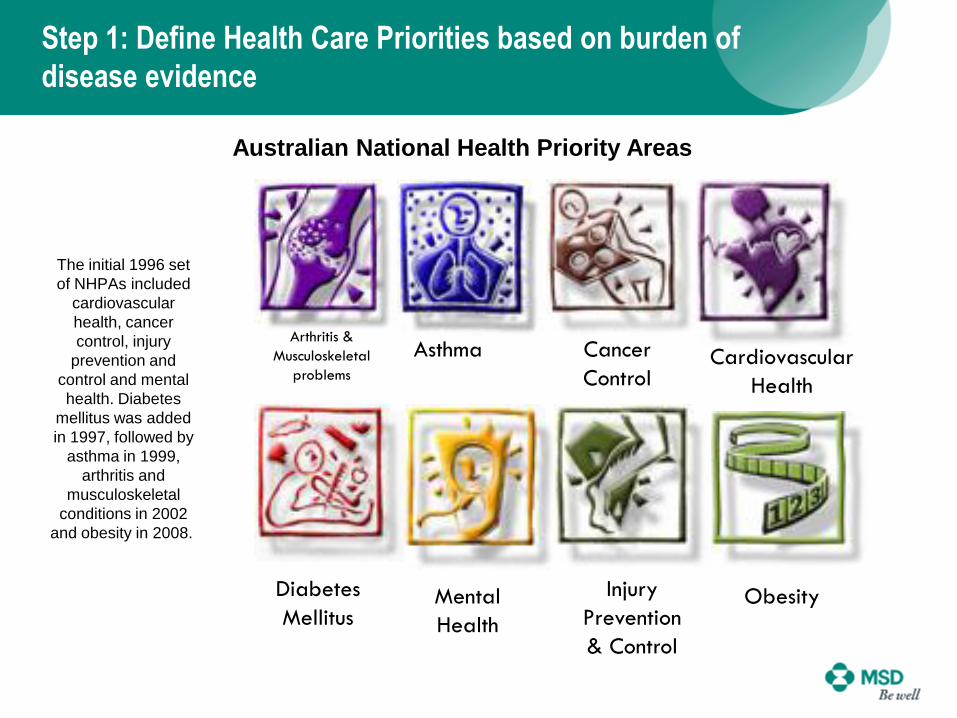
Step 1: Define Health Care Priorities based on burden of
disease evidence
The initial 1996 set
of NHPAs included
cardiovascular
health, cancer
control, injury
prevention and
control and mental
health. Diabetes
mellitus was added
in 1997, followed by
asthma in 1999,
arthritis and
musculoskeletal
conditions in 2002
and obesity in 2008.
AsthmaArthritis &
Musculoskeletal
problems
Diabetes
Mellitus
Cardiovascular
Health
Cancer
Control
Mental
Health
Injury
Prevention
& Control
Obesity
Australian National Health Priority Areas
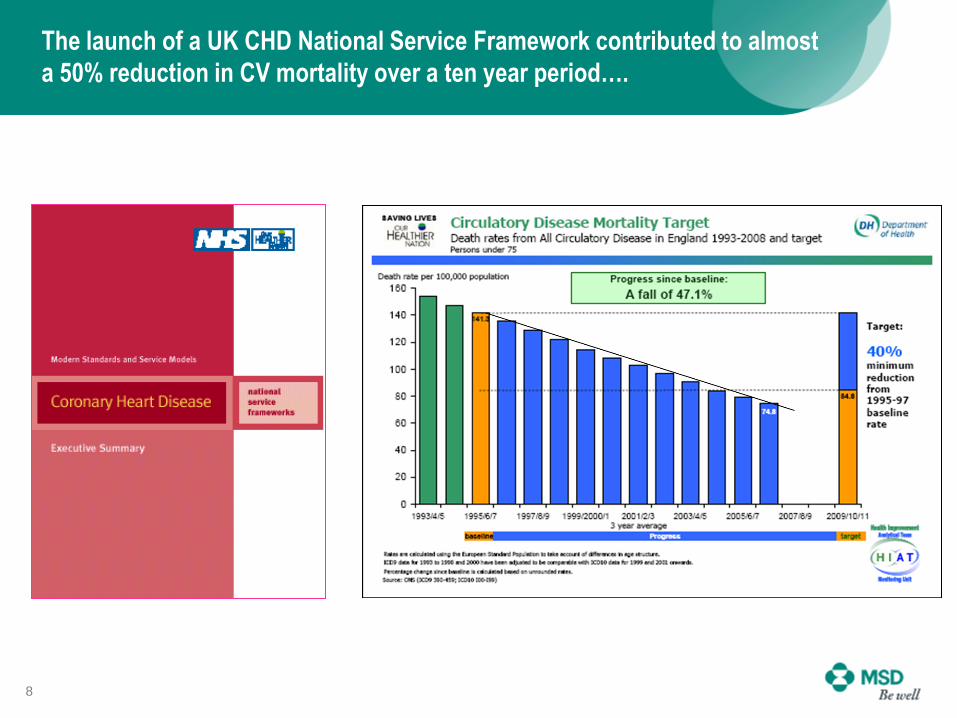
The launch of a UK CHD National Service Framework contributed to almost
a 50% reduction in CV mortality over a ten year period….
8

Step 2: Focus on Prevention and Primary Care
As severity increases amongst patients with chronic conditions,
hospitalisation costs escalate, driven by admissions and referrals

Step 2: Focus on Prevention and Primary Care
Primary Health Care Networks
Patient Literacy
Self Monitoring/Management
Care in the Community
Obesity
Unhealthy lifestyles
Smoking
Alcohol and drug use
Accidents
Exp
an
d
Fig
ht
10
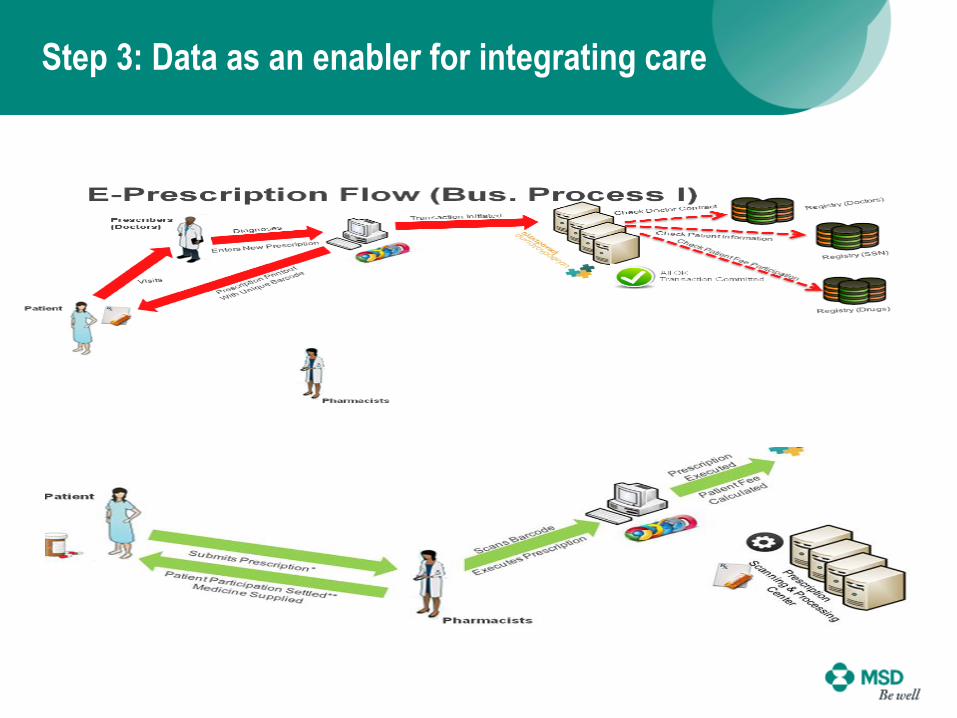
Step 3: Data as an enabler for integrating care
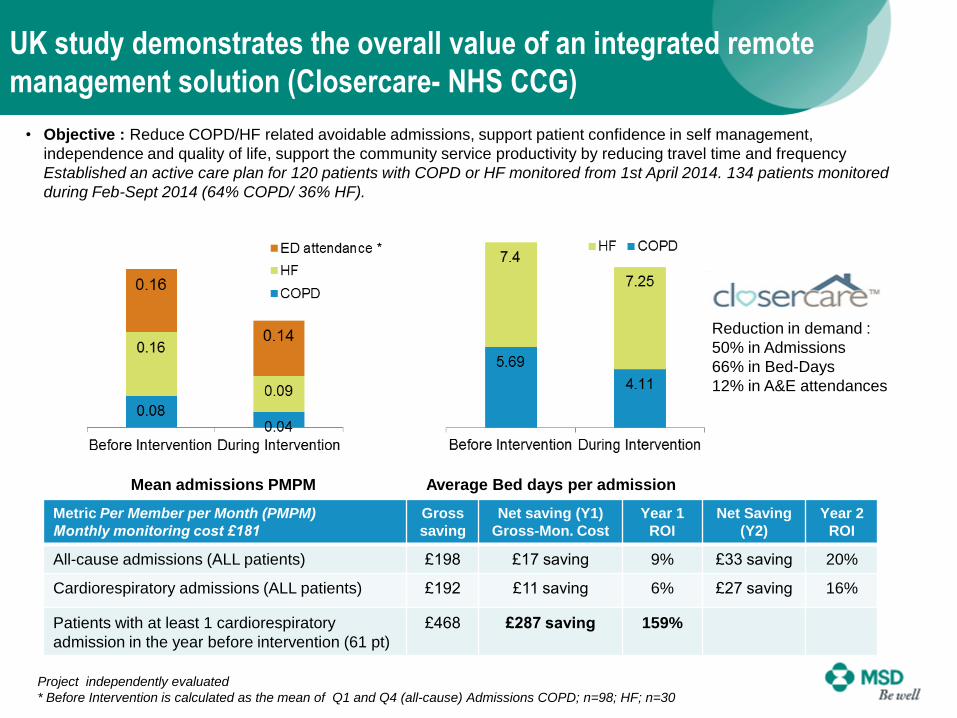
UK study demonstrates the overall value of an integrated remote
management solution (Closercare- NHS CCG)
Project independently evaluated
* Before Intervention is calculated as the mean of Q1 and Q4 (all-cause) Admissions COPD; n=98; HF; n=30
• Objective : Reduce COPD/HF related avoidable admissions, support patient confidence in self management,
independence and quality of life, support the community service productivity by reducing travel time and frequency
Established an active care plan for 120 patients with COPD or HF monitored from 1st April 2014. 134 patients monitored
during Feb-Sept 2014 (64% COPD/ 36% HF).
Mean admissions PMPM Average Bed days per admission
Metric Per Member per Month (PMPM)
Monthly monitoring cost £181
Gross
saving
Net saving (Y1)
Gross-Mon. Cost
Year 1
ROI
Net Saving
(Y2)
Year 2
ROI
All-cause admissions (ALL patients) £198 £17 saving 9% £33 saving 20%
Cardiorespiratory admissions (ALL patients) £192 £11 saving 6% £27 saving 16%
Patients with at least 1 cardiorespiratory
admission in the year before intervention (61 pt)
£468 £287 saving 159%
Reduction in demand :
50% in Admissions
66% in Bed-Days
12% in A&E attendances

Step 4: Establish Greece as a World Class Excellence Center for Real World Evidence
RWE Strategy
Analyze
Healthcare
Utilization &
Expenditure
data
Attract
Healthcare
Services
Research &
Clinical Studies
Assess
Value of
different
treatment
options via
RWE
Align
Among different
stakeholders (e.g.,
Patients, Payers,
Providers, Gvt.
Officials)

Step 5. Establish and Review Quality Indicators
14
NHS Quality Framework
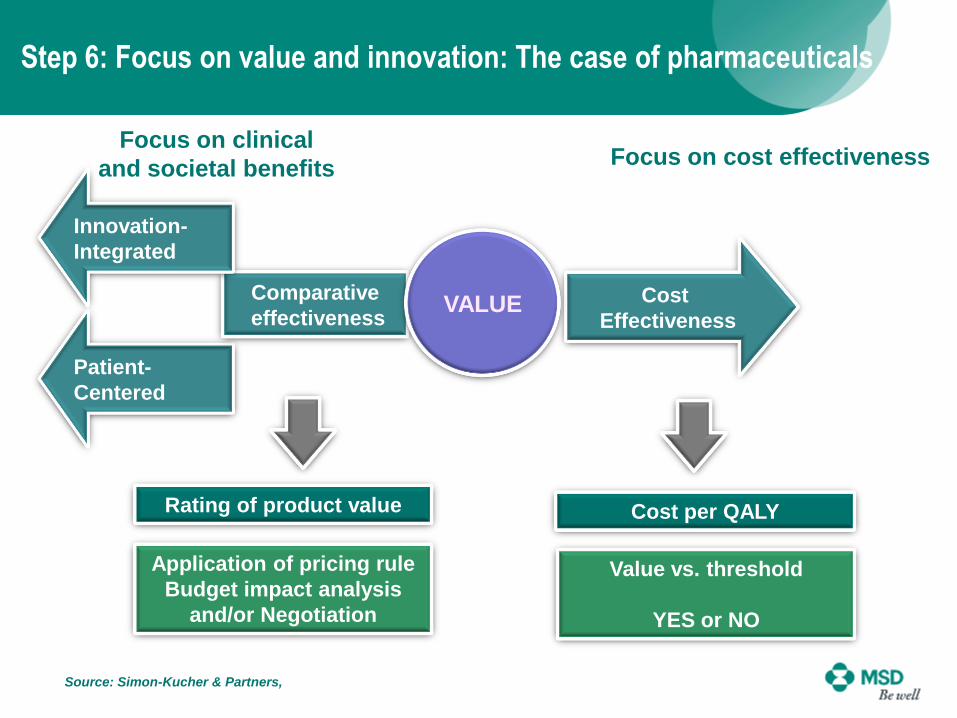
Step 6: Focus on value and innovation: The case of pharmaceuticals
Source: Simon-Kucher & Partners,
Focus on clinical
and societal benefitsFocus on cost effectiveness
Rating of product value Cost per QALY
Application of pricing rule
Budget impact analysis
and/or Negotiation
Value vs. threshold
YES or NO
Cost
Effectiveness
Patient-
Centered
Comparative
effectiveness
Innovation-
Integrated
VALUE

Towards a sustainable pharmaceutical pricing and
reimbursement system
Delayed Access
Low Innovation
External Ref.
Pricing
Narrow Use
of HTA
Parallel
Trade
Therapeutic
Ref Pricing Clawbacks
Price Cuts
Sound Value
Assessment
Transparent and
Predictable Decision
Making Process
Generic Price
Competition
Access, Innovation and
Affordability
Differential
Pricing
16
Short-sighted and
arbitrary decisions
Sustainable and
Sound P&R Policy

NEW WORLDOLD WORLD
Physician-centric
Relying on subject matter experts
Emphasis on highly specialized care
Payments largely based on fee-for-
service model with no alignment
among healthcare participants
Focus on innovation, blockbuster,
quantity and convenience of care
delivery
Patient-centric
Leveraging information technologies
Emphasis on coordination/ integration
Payment systems focusing on outcomes,
with alignment of incentives for relevant
stakeholders (patients, payors, providers)
Focus on risk stratification, case
management, real-world evidence
Innovation = Push Boundaries Innovation = Better Care at Lower Cost
Overall : Lead the change to a patient centric system

`