109734756 module 14 pharmacotherapy for onocologic disorders
TRANSCRIPT

Geriatric Pharmacy Review
Module 14: Pharmacotherapy for Oncologic Disorders

Copyright 2011 American Society of Consultant Pharmacists
Accreditation Information
ASCP is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education.
This home study web activity has been assigned 3.5 credit hours.
ACPE UPN: 0203-0000-10-041-H-01-P
Release Date: 3/15/2010
Expiration Date: 3/15/2013
To receive continuing education credit for this course, participants must complete an on-line evaluation form and pass the on-line assessment with a score of 70% or better. If you do not receive a minimum score of 70% or better on the assessment, you are permitted 4 retakes. After passing the assessment, you can print and track your continuing education statements of credit online.
Geriatric Pharmacy Review courses have not yet been approved for Florida consultant pharmacy continuing education.

Copyright 2011 American Society of Consultant Pharmacists
Content Experts
Trinh Pham, PharmD, BCOP Assistant Clinical Professor University of Connecticut School of Pharmacy Yale New Haven Hospital
Disclosure:
Trinh Pham has no relevant financial relationships to disclose.

Copyright 2011 American Society of Consultant Pharmacists
Aging and Cancer
Learning Objectives:
By the end of this Review Concept you should be able to:
• Describe the incidence and mortality trends associated with oncological disorders among the elderly
• Describe the process of malignant transformation and the development of a clinically significant tumor
• Cite some of the current theories regarding the relationship between age and the incidence of cancer
• Describe primary strategies for the prevention and treatment of cancer
• Explain the importance of early cancer screening and reasons why early detection is difficult
• Understand the importance of a comprehensive geriatric assessment and its role in determining the appropriate therapy for
the elderly cancer patient
• List the patient and disease related factors that influence the choice of cancer treatment
• Describe the complications that can occur as a result of cancer treatment and how they are managed

Copyright 2011 American Society of Consultant Pharmacists
Cancer in the Elderly: Incidence and Mortality
Cancer is the second leading cause of death in the United States and it is a major problem for the elderly. The most common cancers include breast, lung, colon, and prostate.
The incidence of cancer increases with age and it is estimated that by the year 2030 approximately 20% of the United States population will be 65 years of age or older, compared to 12.4% at the present time. Since over 60% of all newly diagnosed cancers and 71% of all cancer deaths occur in persons over the age of 65, it may be expected that the burden of cancer care will rise dramatically in the United States in the future.This shift in the population demographics is due to the aging of the “baby boomers” and has created an increased interest in developing programs and fostering research focusing on the optimal care of geriatric cancer patients.This module will focus on the management of cancer in the geriatric patient population and the following specific areas will be addressed:the biology of cancer in the older person; the goals of cancer prevention in the elderly; the determination of the fitness of the elderly patient using the comprehensive geriatric assessment; the pharmacologic, pharmacodynamic and pharmacokinetic changes involved with the process of aging, their impact on therapy selection and consequences on toxicity outcomes; the evidence based guidelines for the treatment of cancer; and, lastly, the evidence based guidelines for the management of toxicities related to the treatment of cancer.
Incidence (%) in persons > 65 years Mortality (%) in persons > 65 years
Lung Cancer ~70 ~70
Colon & Rectum ~70 -‐
Prostate Cancer 68 91.8
Breast Cancer 48 58.6

Copyright 2011 American Society of Consultant Pharmacists
The Process of Malignant Transformation and Tumor Proliferation
• Genetic alteration • Failure of normal control mechanisms • Proliferation and metastases
Malignant transformation or carcinogenesis involves a number of different genetic alterations that occur sequentially in a cell. These alterations include deletion of tumor suppressor genes, the mutation of proto-oncogenes, and other chromosomal aberrations. These genetic changes may be caused by exposure to carcinogens, viruses or occur as a result of hereditary predisposition.
The result is the generation of cells that lack the specific appearance and function of the normal cells. Under normal conditions, hormones and growth factors tightly control the proliferation of cells; however, these control mechanisms have failed in the process of carcinogenesis and the result is an uncontrolled proliferation of malignant cells that eventually may invade and metastasize to other tissues in the body.

Copyright 2011 American Society of Consultant Pharmacists
Theories Associating Aging and Cancer
• Longer duration of carcinogenic exposure • Increased susceptibility of cells to carcinogens • Decreased ability to repair DNA • Activation of oncogene/loss of tumor suppression gene • Decreased immune surveillance
Effect of Aging on Neoplastic Behavior
Rate of tumor growth • Logarithmic growth of some tumors with age
Carcinogen Exposure • Older individuals are at greater risk of developing cancer compared to younger individuals when exposed to the same carcinogen
Tissue Aging • Molecular alterations in the aged tissue is similar to those that occur in carcinogenesis
Proliferative Senescence • Loss of ability of cell to proliferate with aging • Involves molecular changes that predispose to increased risk of malignant changes • Senescent cells are resistant to apoptosis

Copyright 2011 American Society of Consultant Pharmacists
Theories Associating Aging and Cancer
Biology of Cancer and Aging • Changes intrinsic to the neoplastic cell (“seed” effect)
• i.e., expression of multi drug resistance (MDR) gene in AML • Changes in tumor host (“soil” effect)
• i.e. increased circulating level of interleukin-6 (IL- 6) in NHL which increases proliferation rate
More Aggressive Cancers in Older Adults • Non-Hodgkin’s Lymphoma • Acute Myelogenous Leukemia • Malignant Melanoma • Thyroid Cancer
Less Aggressive Cancers in Older Adults • Lung Cancer • Breast Cancer • Colon Cancer • Prostate Cancer • Renal Cancer
As a person ages, the potential for malignant transformation of cells increases.Why is there this increased risk with age?Several theories have been proposed to explain the increased susceptibility of cells to neoplastic alteration in older adults.
First, older persons have less resistance and longer exposure to carcinogens. They also have a decline in their immune function, changes in defense mechanisms against tumors, and furthermore, they have defects in tumor suppressor genes and a decreased ability to repair DNA.

Copyright 2011 American Society of Consultant Pharmacists
Theories Associating Aging and Cancer
Second, the epidemiology of squamous cell carcinoma of the skin in humans have documented that there is a logarithmic growth of the tumor with age.Studies of lung cancer have also demonstrated that when older and younger individuals were exposed to the same carcinogen, the incidence of lung cancer was higher among the aged as compared to the young.
And lastly, a new and promising theory for the correlation between cancer and aging is based upon the concept of proliferative senescence. This theory hypothesizes that molecular changes that occur in aging organisms to slow down cellular proliferation rate may actually render the cells more susceptible to environmental carcinogens.
In summary, the process in which aging affects the development of cancer is dependent on many factors. Furthermore, the clinical course of the cancer is also dependent upon the biologic behavior of the neoplasm in addition to the age of the person. The prognosis of the cancer may be either worse or better depending on the biology of the tumor cells, the “seed”, and changes in the ability of the older tumor host to sustain and stimulate tumor growth, the “soil” effect.
For most cancers, there is no consistent difference in clinical presentation for different age groups. While the five-year survival rate for many cancers is lower in the elderly, there are some cancers that behave less aggressively in older adults and sorting out the biologic factors that differentially affect neoplastic behavior in elderly patients is complex.
Copyright 2011 American Society of Consultant Pharmacists
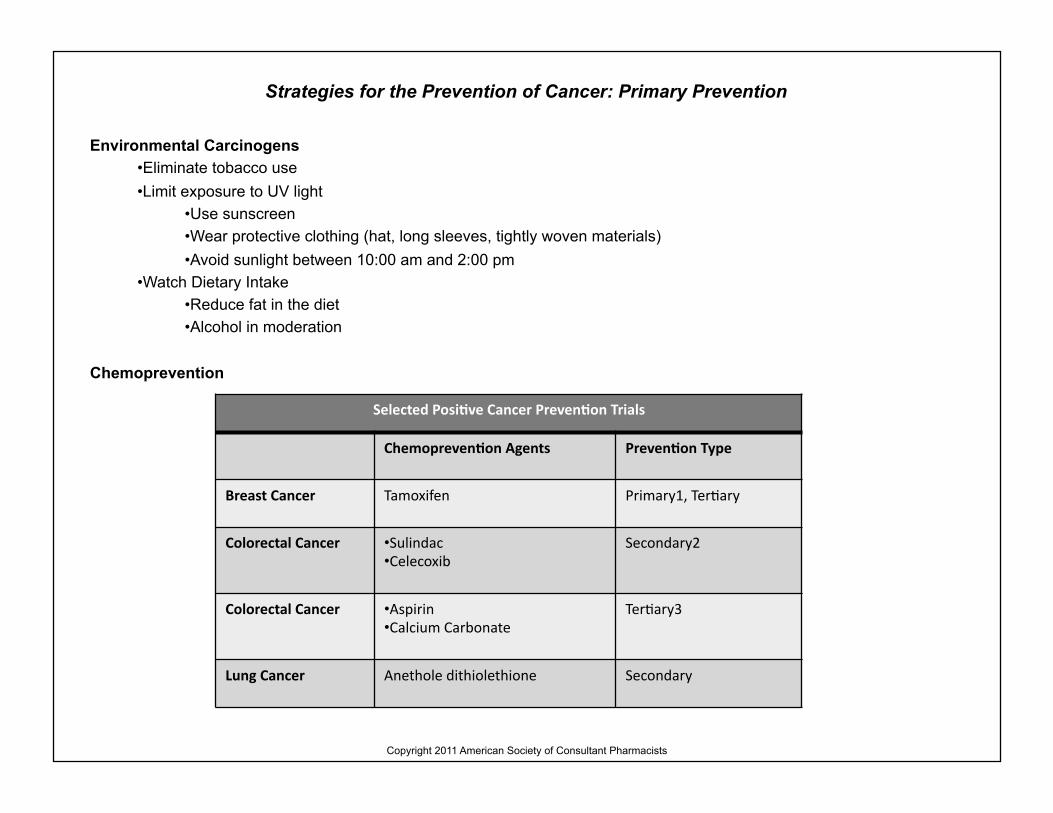
Strategies for the Prevention of Cancer: Primary Prevention
Environmental Carcinogens • Eliminate tobacco use • Limit exposure to UV light
• Use sunscreen • Wear protective clothing (hat, long sleeves, tightly woven materials) • Avoid sunlight between 10:00 am and 2:00 pm
• Watch Dietary Intake • Reduce fat in the diet • Alcohol in moderation
Chemoprevention
Selected PosiAve Cancer PrevenAon Trials
ChemoprevenAon Agents PrevenAon Type
Breast Cancer Tamoxifen Primary1, Ter:ary
Colorectal Cancer • Sulindac • Celecoxib
Secondary2
Colorectal Cancer • Aspirin • Calcium Carbonate
Ter:ary3
Lung Cancer Anethole dithiolethione Secondary

Copyright 2011 American Society of Consultant Pharmacists
Strategies for the Prevention of Cancer: Primary Prevention
Selected PosiAve Cancer PrevenAon Trials
ChemoprevenAon Agents PrevenAon Type
Lung Cancer Re:nyl palmitate Ter:ary
Prostate Cancer Finasteride Primary
Prostate Cancer • Doxazosin • Finasteride
Secondary
Head & Neck Cancer • Isotre:noin • Vitamin A • Beta Carotene • Interferon-‐a
Secondary
Isotre:noin Interferon-‐a
Ter:ary
1-Prevent de novo malignancies in otherwise healthy person 2- Prevent the progression of pre-malignant lesions to cancers 3- Preventing second primary tumor in patients cured of initial cancer

Copyright 2011 American Society of Consultant Pharmacists
Strategies for the Prevention of Cancer: Primary Prevention
Ongoing Chemoprevention Trials
Breast Cancer Tamoxifen, Raloxifene
Lung Cancer COX-2 Inhibitors Selenium Gefitinib
An encouraging area of research in oncology is in the field of cancer prevention. This is an enticing concept because the proactive approach of cancer prevention may eliminate or decrease the chance of being diagnosed with cancer, preserve life, and avert the complications associated with a malignancy or its treatment.
However, when cancer prevention is being considered in the elderly, it is essential to consider that due to the limited life expectancy of this population, the benefit of survival gain may be reduced. Thus, the value of chemoprevention should be assessed in terms of its potential in averting cancer-related morbidity and preserving quality of life in addition to the outcome of possible gain in survival time.
Cancer prevention may be either primary or secondary. Primary prevention involves the elimination of exposure to carcinogens and environmental factors that are associated with the growth of some cancers.Chemoprevention, defined as the administration of natural, synthetic, or biologic chemical agents to suppress, reverse, or prevent the development of cancer, is also considered to be primary prevention.
Colorectal Cancer COX-2 Inhibitors
Prostate Cancer Selenium Vitamin E

Copyright 2011 American Society of Consultant Pharmacists
Strategies for the Prevention of Cancer: Primary Prevention
Examples of agents that have demonstrated in clinical trials to be effective in reducing the risk of developing newly diagnosed cancers, the occurrence of second cancers, or the progression of premalignant cancer to overt cancer include the selective estrogen receptor modulators, examples of which are tamoxifen and raloxifene, the 5-alpha reductase inhibitor and example of which is finasteride, the non-steroidal anti-inflammatory agents, and vitamin A derivatives. The tables provide summary data on agents that are effective for the prevention of specific cancers and ongoing trials that are evaluating the efficacy other agents.
The critical questions that have not been answered in the use of these chemoprevention agents and need to be addressed in the future are: At what age should these agents be administered and for how long?Will the elderly, who have presumed pre-cancer, benefit from chemoprevention? Does chemoprevention reduce the number of cancer deaths? What are the side effects associated with these chemopreventive agents and what is the acceptable risk versus benefit ratio? Do these chemopreventive agents improve quality of life? And lastly, what are the costs associated with the administration of these agents?

Copyright 2011 American Society of Consultant Pharmacists
Strategies for the Prevention of Cancer: Secondary Prevention
Screening Recommendations
Breast Cancer
• Mammography • ACS- Annually after age 40 • USPSTF –Every 1 to 2 years ages 50-69 • AMA – Every 1-2 years 40-49, annually at age 50
• Clinical Breast Examination • ACS- Every 3 years 20-39, yearly after 40, monthly self breast examination starting at 20 years. • USPSTF –Insufficient data to recommend for or against
Cervical Cancer
• Pap Test • ACS-Annually at 18 years or when sexually active, after 2-3 negative tests continue at discretion of physician • USPSTF- every 3 years if ever had sexual intercourse, discontinue after 65 years of age with consistently negative results • AGS- Every 3 years until 70
Colorectal Cancer
• ACS- after 50, yearly FOBT PLUS flexible sigmoidoscopy and DRE every 5 years or colonoscopy and DRE every 10 years or double contrast enema and DRE every 5 to 10 years • AMA- Annual FOBT & DRE starting at age 50 and flexible sigmoidoscopy every 3 to 5 years

Copyright 2011 American Society of Consultant Pharmacists
Strategies for the Prevention of Cancer: Secondary Prevention
Prostate Cancer
ACS and AUA- Offer annual DRE and PSA starting at age 50 to men with at least 10 -year life expectancy and to younger men at high risk
Skin Cancer
ACS- Skin examination every 3 years between 20-40 years, every year at age 40 and older
ACS-American Cancer Society, USPSTF-U.S. Preventive Services Task Force, AMA-American Medical Association, AGS-American Geriatrics Society, AUA-American Urologic Society. DRE- Digital Rectal Exam, FOBT-Fecal Occult Blood Test, PSA-Prostate Specific Antigen
Secondary prevention involves diagnosing cancer at an earlier stage by screening individuals at high risk of developing cancer.The assumptions are that the cancer may be diagnosed during the pre-clinical phase and that early diagnosis is associated with increased curability due to early treatment initiation.The effectiveness of secondary prevention is measured by the reduction in cancer-related deaths.
Presently, guidelines are available for the early screening of cancers from medical organizations such as the United States Preventive Services Task Force, the American Cancer Society, the American Geriatric Society, the American Urological Association, and the American Medical Association.Unfortunately, the recommendations from these organizations sometimes conflict with each other and the primary care physician and health care providers working in the field of oncology must synthesize the data and determine the best course of action for his patient.

Copyright 2011 American Society of Consultant Pharmacists
Strategies for the Prevention of Cancer: Secondary Prevention
In general, a clinical breast examination and mammography is recommended every 1 to 2 years for women between 50 to 70 years of age for breast cancer screening. Most organizations recommend a PAP smear and pelvic examination at least every 3 years for women between 20 and 65 years of age for cervical cancer screening.
For colorectal cancer screening, the standard recommendation is an annual fecal occult blood test and flexible sigmoidoscopy every 5 to 10 years starting at age 50.The recommendation for prostate cancer screening is controversial. Some organizations recommend an annual digital rectal exam and serum prostate specific antigen test starting at 50 years of age and some organizations such as the U.S. Preventive Services Task forces have no recommendations for prostate cancer screening citing insufficient evidence to support such practice.
Cancer screening guidelines in the elderly patient is uncertain. The recommendations for this population should not be based exclusively on age-specific guidelines but rather accompanying factors such as life expectancy, the risk of cancer related deaths, the potential for harm due to psychological stress, the possibility of false positives, and the possibility of treating clinically insignificant cancers should be taken into consideration.

Copyright 2011 American Society of Consultant Pharmacists
Cancer Symptoms in the Elderly
Signs/Symptoms Possible Malignancy Confused with
Increased Skin Pigment Melanoma
Age Spots Squamous Cell Carcinoma
Rectal Bleeding Cons:pa:on
Colorectal Rectal
Hemorrhoids, Aging
Dyspnea Lung Aging, Out of Shape
Decreased Urinary Stream Prostate “Dribbling”, BPH
Breast Change Breast Normal Atrophy
Fa:gue Metasta:c or Hematologic Cancer
Aging, Out of Shape
Bone Pain Metasta:c Cancer, Mul:ple Myeloma
Arthri:s, Aging

Copyright 2011 American Society of Consultant Pharmacists
Cancer Symptoms in the Elderly
Cancer screening and routine follow up visits with a primary care physician is beneficial for the early identification of cancers in the elderly patient population. Most types of cancer can only be cured if they are diagnosed before they metastasize. As is well known, a delay in the diagnosis of cancer results in more advanced stage presentation which portends a poorer prognosis overall. Therefore early detection of cancer increases an individual’s chance of survival.
This is especially imperative in light of the fact that the early symptoms of cancer in the elderly are sometimes more difficult to recognize compared to younger, healthier patients. Despite well publicized warning signs, elderly individuals often do not present for early detection. The explanation for this is due to the tendency to confuse specific cancer symptoms with normal changes of the aging process.
For example, early symptoms such as pain may be confused with exacerbation of preexisting chronic pain and may be ignored by the patient, or the coexistence of other diseases such as anemia can mask the early symptoms of cancers. There is no easy solution to this dilemma other than educating the elderly on the importance of routine physician check up visits and emphasizing to physicians the need of being more attuned to their patient population and the possibility of cancer in their work up differential.

Copyright 2011 American Society of Consultant Pharmacists
Assessment of Aging
Category of Aging Age Range ClassificaAon
Young-‐Old 70-‐75 years Beginning of senescence
Old-‐Old 76-‐84 years
Oldest-‐ Old > 85 years Beginning of frailty
Comprehensive Geriatric Assessment (CGA)
Domain Instrument
Health • Number of comorbid condi:ons • Charlson’s Comorbidity Scale • Chronic Illness Ra:ng Scale-‐Geriatric
(CIRS-‐G) FuncAon • Performance Status • Instrumental Ac:vi:es of Daily Living (IADL)-‐ (shopping, use of transporta:on, cooking, cleaning, managing money, taking medica:ons) • Ac:vi:es of Daily of Living (ADL)-‐ (bathing, grooming, toile:ng, dressing, feeding, appropriate behavior)

Copyright 2011 American Society of Consultant Pharmacists
Assessment of Aging
Comprehensive Geriatric Assessment (CGA)
Domain Instrument
CogniAon • Folstein Mini Mental Status (MMS) • Demen:a Ra:ng Scale (DRS)
EmoAons Geriatric Depression Scale (GDS)
Social • Living condi:ons, marital adjustment, • caregiver adequacy, caregiver stress, income, transporta:on
NutriAon Mini Nutri:onal Assessment (MNA)
Pharmacy Drug list and interac:on
Defining the Frail Elderly
• Age > 85 • Dependence in 1 or more activities of daily living (ADLs) • 3 or more comorbid conditions • 1 or more geriatric syndromes

Copyright 2011 American Society of Consultant Pharmacists
Assessment of Aging
Originating from Medicare and Social Security regulations, the arbitrary definition of “geriatric” or “elderly” is a person who is 65 years of age or older. This population, however, is heterogeneous and the definition does not reflect the underlying health status of the individuals in this group.
Although aging is associated with a progressive decline in a person’s functional reserve, this is an individualized process and different people develop disease, functional restrictions and physiologic limitations at varying rates that are not reflective of chronologic age. It is significant, however, to note that starting at the age of 70 years, the incidence of age related changes increases steeply and starting at the age of 85 years the functional reserve is almost exhausted and an individual may be categorized as frail elderly.
Given this diversity of functional status in the elderly population, the process of assessing the fitness of these individuals is challenging. The comprehensive geriatric assessment is a multidisciplinary tool, which assesses the domains of health, functional status, nutrition, cognition, socio-economic aspects, and emotional aspects that are likely to change with aging. This multidimensional, interdisciplinary patient evaluation instrument is effective in identifying unsuspected comorbid conditions, physical or emotional dysfunction, and incompetence in daily functional activities. These factors have been shown to be independent predictors of survival and are vital in determining the ability of the patient to undergo and withstand surgery, cytotoxic therapy or other types of treatment.
The National Comprehensive Cancer Network (NCCN) has developed guidelines for the treatment of older patients with cancer to ensure that therapy is adequate, toxicities are avoided, and quality of life is maintained. Performing a comprehensive geriatric assessment is one of their recommendations for the initial evaluation of elderly patients diagnosed with cancer.
Copyright 2011 American Society of Consultant Pharmacists
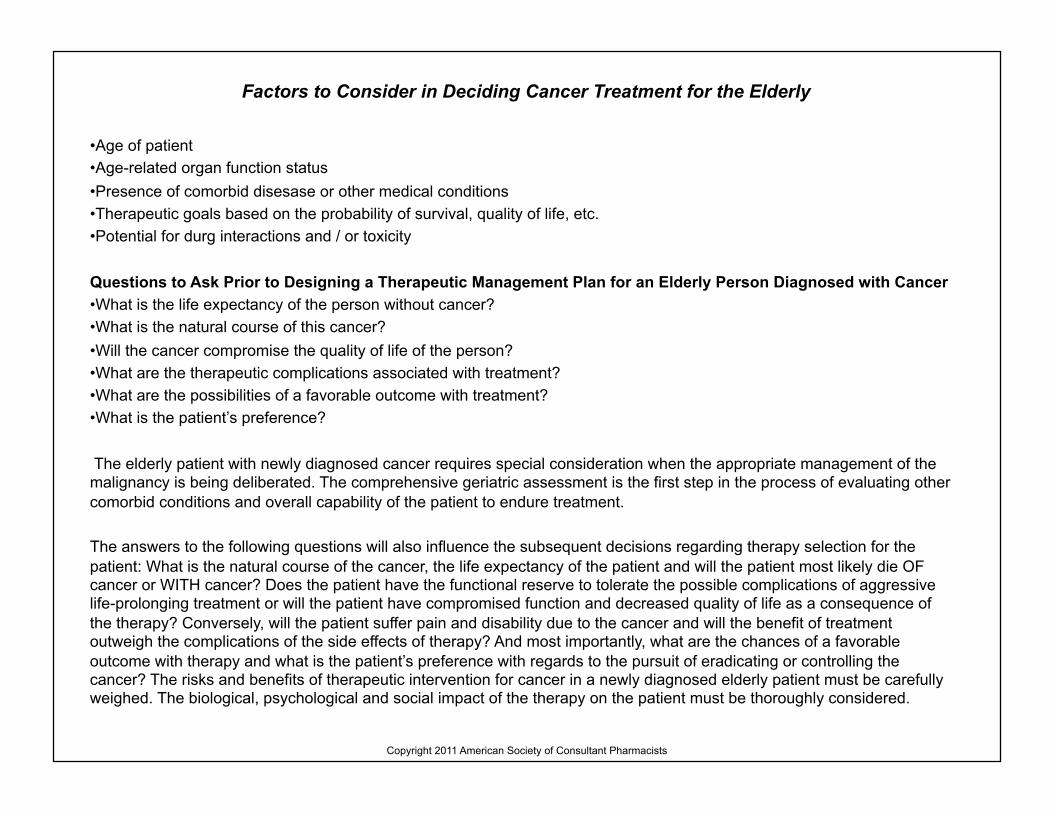
Factors to Consider in Deciding Cancer Treatment for the Elderly
• Age of patient • Age-related organ function status • Presence of comorbid disesase or other medical conditions • Therapeutic goals based on the probability of survival, quality of life, etc. • Potential for durg interactions and / or toxicity
Questions to Ask Prior to Designing a Therapeutic Management Plan for an Elderly Person Diagnosed with Cancer • What is the life expectancy of the person without cancer? • What is the natural course of this cancer? • Will the cancer compromise the quality of life of the person? • What are the therapeutic complications associated with treatment? • What are the possibilities of a favorable outcome with treatment? • What is the patient’s preference?
The elderly patient with newly diagnosed cancer requires special consideration when the appropriate management of the malignancy is being deliberated. The comprehensive geriatric assessment is the first step in the process of evaluating other comorbid conditions and overall capability of the patient to endure treatment.
The answers to the following questions will also influence the subsequent decisions regarding therapy selection for the patient: What is the natural course of the cancer, the life expectancy of the patient and will the patient most likely die OF cancer or WITH cancer? Does the patient have the functional reserve to tolerate the possible complications of aggressive life-prolonging treatment or will the patient have compromised function and decreased quality of life as a consequence of the therapy? Conversely, will the patient suffer pain and disability due to the cancer and will the benefit of treatment outweigh the complications of the side effects of therapy? And most importantly, what are the chances of a favorable outcome with therapy and what is the patient’s preference with regards to the pursuit of eradicating or controlling the cancer? The risks and benefits of therapeutic intervention for cancer in a newly diagnosed elderly patient must be carefully weighed. The biological, psychological and social impact of the therapy on the patient must be thoroughly considered.

Copyright 2011 American Society of Consultant Pharmacists
Cancer Treatment Options
• Surgery • Chemotherapy and Hormonal Therapy • Radiation Therapy
Aggressive surgery, radiation therapy, and standard chemotherapy are viable treatment options for the elderly patient diagnosed with cancer.Elective cancer surgery and standard doses of radiation therapy is tolerated well by patients even in their 80’s.Therefore, the arbitrary implementation of less aggressive therapy for cancer patients based upon chronologic age is not acceptable as there are no data to support this practice.

Copyright 2011 American Society of Consultant Pharmacists
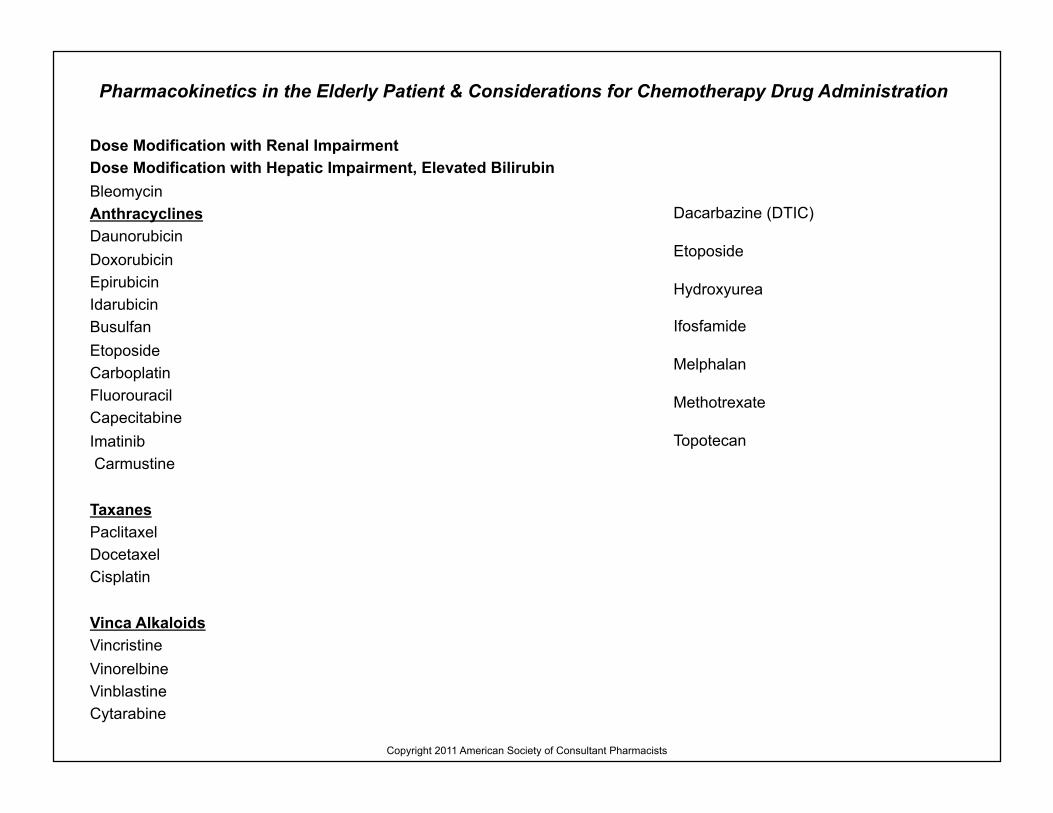
Pharmacokinetics in the Elderly Patient & Considerations for Chemotherapy Drug Administration
Absorption • Decreased gastrointestinal motility • Decreased splanchnic blood flow • Decreased secretion of digestive enzymes • Mucosal atrophy
Distribution • Increased body fat • Decreased intracellular water content • Decreased plasma albumin • Decreased red blood cell concentration
Metabolsim • Decreased liver size and liver blood flow • Decreased Phase I metabolism
• CYP450 1A2:20 – 30% decrease in clearance
Excretion • Decreased renal mass • Decline in renal function and glomerular filtration rate (GFR)
Copyright 2011 American Society of Consultant Pharmacists
Pharmacokinetics in the Elderly Patient & Considerations for Chemotherapy Drug Administration
Dose Modification with Renal Impairment Dose Modification with Hepatic Impairment, Elevated Bilirubin Bleomycin Anthracyclines Daunorubicin Doxorubicin Epirubicin Idarubicin Busulfan Etoposide Carboplatin Fluorouracil Capecitabine Imatinib Carmustine
Taxanes Paclitaxel Docetaxel Cisplatin
Vinca Alkaloids Vincristine Vinorelbine Vinblastine Cytarabine
Dacarbazine (DTIC)
Etoposide
Hydroxyurea
Ifosfamide
Melphalan
Methotrexate
Topotecan

Copyright 2011 American Society of Consultant Pharmacists
Pharmacokinetics in the Elderly Patient & Considerations for Chemotherapy Drug Administration
It is reasonable to anticipate that an elderly person may have reduced functional reserve of many organ systems and that the pharmacologic, pharmacodynamic and pharmacokinetic aspects of drug therapy will be altered. The absorption of oral chemotherapy agents may be reduced due to mucosal atrophy, decreased splanchnic blood flow or secretion of digestive enzymes. As a person ages, their body fat content doubles and intracellular water decreases which results in decreased volume of distribution of polar drugs and increase in volume of distribution of lipid soluble drugs.
Furthermore, the reduction in serum albumin and red blood cell concentration associated with aging may increase the toxicities of chemotherapy agents that have high binding affinity with these compounds due to the increase in free drug concentrations. Chemotherapy drugs that are metabolized by the cytochrome P450 system may be affected since it has been demonstrated that there is a decrease in clearance of CYP1A2 by 20-25% in healthy elderly patients as compared to younger patients. And lastly, the decline in renal function as manifested by the decrease in glomerular filtration rate may result in elevation in serum concentrations and toxicity of drugs that are mainly renally eliminated.
In spite of all of these anticipated changes in organ function in the elderly, the key message however, is that chemotherapy should be tailored for the individual patient and the doses of the drug should be adjusted based upon the patient’s calculated glomerular filtration rate and liver function status as assessed by liver enzymes and bilirubin levels. There is no data to corroborate an empiric dose decrease based on chronological age alone.

Copyright 2011 American Society of Consultant Pharmacists
Considerations in the Use of Oral Chemotherapy Agents
• Cost • Patient preference • Quality of life • Compliance • Polypharmacy • Complementary / Alternative medicine • Drug interactions
Commonly Prescribed Oral Chemotherapy Agents Common Cancer Type
Capecitabine Breast, Colorectal
GefiAnib Lung
ImaAnib Chronic Myelogenous Leukemia, Gastrointes:nal Stromal Tumor
Temozolomide Anaplas:c Astrocytoma, Melanoma
Etoposide Lung
Chlorambucil Chronic Lymphocy:c Leukemia, Lymphomas

Copyright 2011 American Society of Consultant Pharmacists
Considerations in the Use of Oral Chemotherapy Agents
In the last 20 years the availability of oral chemotherapy agents for the treatment of various malignancies has increased. Factors such as patient preference, improved quality of life, and cost of therapy have been influential in the development of these agents. On the other hand, the issue of compliance can be a major obstacle in the implementation of an oral chemotherapy regimen.
Some factors associated with higher rates of noncompliance include lower socioeconomic status, treatment in a community based setting, female gender, poor recall of the medication regimen, and the complexity of the medication regimen. The implication is that the effectiveness of the medication will be diminished and the chance of disease free survival is affected if the patient is not taking their medication as directed.
Commonly Prescribed Oral Chemotherapy Agents Common Cancer Type
Melphalan Lymphoma, Mul:ple Myeloma
Cyclophosphamide Breast, Leukemia, Lymphoma
CarmusAne (CCNU)
Brain Tumor
Thalidomide Mul:ple Myeloma

Copyright 2011 American Society of Consultant Pharmacists
Considerations in the Use of Oral Chemotherapy Agents
Another facet to consider in the use of oral chemotherapy is the issue of polypharmacy and drug interactions.On average, the older patient takes at least four medications and self-medication with alternative herbal therapies is increasing. The consequence is an increase in the probability of drug interactions and toxicities.
The dilemmas that may limit the use of oral chemotherapy agents can be minimized by prescribing simple dosage regimens, suggesting the use of devices that helps with compliance, and educating patients on the importance of adhering to the dosing schedule and the necessity of consulting with a pharmacist or other health care providers prior to self initiation of alternative therapies.
On the whole, the expanding role of oral chemotherapy in the treatment of malignancies is a positive step forward in providing cancer patients with more options, convenience, and control in the management of their disease.

Copyright 2011 American Society of Consultant Pharmacists
Managing the Complications of Cancer Therapy: Neutropenia
Consequences of Neutropenia • Increased risk of infection • Febrile neutropenia • Hospital admission • Antibiotic administration
Consequences of Older Age and Chemotherapy Administration • Increased neutropenic complications • Increased risk of febrile neutropenia (FN) • Increased risk of death from FN • Reduced dose intensity of chemotherapy • Increased risk of 1st cycle hematologic toxicity
Role of Colony Stimulating Factors in Elderly Patients:
• Should be administered in patients older than 70 years of age receiving moderately toxic chemotherapy:
• i.e., CHOP (Cyclophosphamide, doxorubicin, vincristine, prednisone) • Or regimens with toxicity level of CHOP
• Consider adding colony stimulating factor early in the course of treatment i.e. 1st or2nd cycle of chemotherapy

Copyright 2011 American Society of Consultant Pharmacists
Managing the Complications of Cancer Therapy: Neutropenia
Colony Stimulating Factor 1
Dosing Recommendation • G-CSF (Granulocyte colony stimulating factor, filgrastim, NeupogenÒ )
• 5 mcg/kg/day SC/IV once daily • GM-CSF (Granulocyte macrophage colony stimulating factor, Sargramostim, LeukineÒ)
• 250 mcg/kg/day SC/IV once daily • Peg-Filgrastim (NeulastaÒ)
• 6 mg SC once per cycle of chemotherapy
1- The colony stimulating factor should be initiated 24 hours after the end of chemotherapy.
One of the most common dose-limiting side effects of chemotherapy is myelosuppression.The spectrum of myelosuppression includes neutropenia, anemia, and thrombocytopenia, which leads to the clinical manifestations of increased infection risk, fatigue, and bleeding episodes.
It is observed that the concentration of pluripotent hematopoietic stem cells decline with age yet normal basal hematopoiesis is maintained and preserved. It is only under stress conditions that the blunted response of the hematopoetic stem cells is evident. A review of clinical trials involving breast cancer and non-hodgkin’s lymphoma patients older than 65 years demonstrate that the incidence of myelosuppression and the risk of complications from neutropenia and mortality from febrile neutropenia increase with increasing age.The use ofcolony stimulating factors (CSF) such as granulocyte-CSF (G-CSF) or granulocyte-macrophage –CSF(GM-CSF) have been proven to shorten the duration of neutropenia and the risk of hospitalization for neutropenic fever after induction chemotherapy administration.
From evidence-based data, the American Society of Clinical Oncology and the National Comprehensive Cancer Network recommend primary prophylactic administration of colony stimulating factors in patients aged 70 and older receiving moderately toxic chemotherapy such as CHOP or CHOP-like regimens.

Copyright 2011 American Society of Consultant Pharmacists
Managing the Complications of Cancer Therapy: Anemia
Potential Causes of Anemia • Iron Deficiency • Vitamin B12 Deficiency • Renal Insufficiency • Anemia of Chronic Disease • Anemia of Unknown Causes • Chemotherapy or Radiation Therapy
Consequences of Anemia • Decline in energy level, fatigue • Decline in quality of life • Loss of independence • Increased risk of heart failure, myocardial infarction • Decreased cognition • Enhanced toxicity of chemotherapy • Reduced survival
Anemia Toxicity Scale
Grade Severity NCI1 Scale (Hemoglobin in g/dl)
WHO2 scale (Hemoglobin in g/dl)
1 Mild 10-‐normal* 9.5 – 10
2 Moderate 8 – 10 8 – 9.4
3 Severe 6.5 – 7.9 6.5 -‐ 7.9
4 Life-‐Threatening < 6.5 < 6.5

Copyright 2011 American Society of Consultant Pharmacists
Managing the Complications of Cancer Therapy: Anemia
National Cancer Institute Definition of Anemia • Male: Normal Hemoglobin =14 - 18 g/dl • Female: Normal Hemoglobin =12-16 g/dl
World Health Organization Definition of Anemia
• Male: Hemoglobin < 13 g/dl • Female: Hemoglobin < 12 g/dl
Risk Factors for Developing Symptomatic Anemia • Transfusion in past 6 months • History of prior myelosuppressive therapy • History of radiation therapy to > 20% of skeleton • Myelosuppression potential of current therapy • Age • Hemoglobin level
Anemia is one of the most common symptoms experienced by patients diagnosed with cancer.The causes may be the underlying cancer disease, nutritional deficiencies, anemia of chronic disease, the toxic effect of therapy such as chemotherapy or radiation, or a combination of these factors.
According to the World Health Organization, the definition of anemia is a hemoglobin level less than 13 g/dl in males and less than 12 g/dl in female.There is a minor discrepancy in the definition for mild and moderate anemia between the National Cancer Institute and the World Health Organization; however, they are identical in their classification of more severe anemia.

Copyright 2011 American Society of Consultant Pharmacists
Managing the Complications of Cancer Therapy: Anemia
As a person ages the risk of anemia is high due to concomitant comorbid factors. The prevalence and incidence of anemia starts to increase at the age of 65 years and the increase is even steeper after age 80.Patients with anemia experience fatigue, decreased quality of life, increased risk for cardiovascular complications, decreased cognition, increased toxicity with chemotherapy agents, increased need for blood transfusions, and lastly decreased survival.
In general the treatment of anemia should be individualized and based upon the underlying cause. There should be correction of nutritional deficiencies and treatment of the infection or inflammatory processes, hemolytic diseases and occult blood loss. Red blood cell transfusions or crystalloid replacement should be administered to symptomatic patients with transient anemia.

Copyright 2011 American Society of Consultant Pharmacists
Managing the Complications of Cancer Therapy: Anemia (cont.)
Indications for Erythropoietin • Asymptomatic with risk factors of developing anemia • Symptomatic - Consider when Hgb = 10 – 11 g/dl
• Strongly consider when Hgb < 10 g/dl
Package Insert Recommendation
Epoetin alfa 150 units/kg or 10,000 units;
administered SC 3x a week – dose to 300 units/kg or 20,000 units;
administered SC 3x a week
Darbepoetin 2.25 mcg/kg/week SC – up to 4.5 mcg/kg/week SC
Common Clinically Used Regimens
Epoetin alfa 40,000 units weekly SC –dose to 60,000 units weekly SC
Darbepoetin 3 mcg/kg every 2 weeks SC – to 5 mcg/kg every 2 weeks SC
Darbepoetin 200 mcg every 2 weeks SC – up to 300 mcg fixed dose every 2 weeks SC
• Reduce dose by 25% if Hgb – by > 1 g/dl in 2 week period
• Hold Therapy if Hgb > 12 g/dl, reinitiate 75% of dose when Hgb < 12 g/dl
* All patients should have iron panel studies with serum iron, total iron binding capacity, and serum ferritin and add iron supplementation if ferritin is < 100 and transferrin saturation is < 20%

Copyright 2011 American Society of Consultant Pharmacists
Managing the Complications of Cancer Therapy: Anemia (cont.)
The hematologic growth factor erythropoietin regulates proliferation, maturation, and differentiation of red blood cells. It is indicated in patients who have symptomatic anemia or who are asymptomatic but have risk factors for development of anemia after other treatable causes of anemia have been ruled out.
The initial dosing recommendations, dose adjustments and monitoring parameters for the administration of the different erythropoietin formulations are provided in the accompanying table.
It is important to ensure that patients have adequate iron stores and that iron supplementation is provided as needed. The patient should be reassessed 4 weeks after initiation of therapy to ensure adequate response. If the patient is not responding, the dose should be increased as recommended. If there is still no response after the dose increase 4 weeks later, then the therapy should be discontinued to prevent the administration of an expensive drug without clinical benefit. If the patient has responded as indicated by a hemoglobin increase of at least 1 g/dl, then the therapy may be continued until it is deemed that the patient’s hematopoeitic system has recovered completely.

Copyright 2011 American Society of Consultant Pharmacists
Managing the Complications of Cancer Therapy: Nausea & Vomiting
Types of Nausea and Vomiting
• Acute – Nausea/vomiting occurring 0 to 24 hours after chemotherapy administration and usually resolves within the first 24 hours • Delayed – Nausea/vomiting occurring > 24 hours after chemotherapy administration • Breakthrough – Nausea/vomiting occurring despite prophylactic antiemetics • Anticipatory – Nausea/vomiting occurring before receiving chemotherapy
• Usually occurs in patients who had poor control of acute or delayed emesis with prior chemotherapy
Principles of Antiemetic Therapy
• The goal is to PREVENT nausea and vomiting • The emetogenicity potential of the chemotherapy regimen should be determined to facilitate the appropriate choice of antiemetic regimen • Patient should receive antiemetic therapy throughout the full period of emesis risk. • For moderately and highly emetogenic chemotherapy regimens, the risk of emesis is at least 4 days. • For chemothepray regimens with a high potential of causing delayed emesis, patient should have around the clock antiemetic to cover the delayed emesis phase. • A benzodiaepine should be considered for patients who are at risk for anticipatory emesis • The lowest, efficacious dose should be used • Oral and IV antiemetic formulations are equally effective • Consider the toxicity of the antiemetics based upon patient specific characteristics such as age

Copyright 2011 American Society of Consultant Pharmacists
Managing the Complications of Cancer Therapy: Nausea & Vomiting
Management of Breakthrough Emesis • Administer multiple concurrent antiemetics from different classes • Rectal or intravenous may be routes of administration of choice • Administer antiemetics around the clock with alternating schedules or routes with the different classes of antiemetics
Non Pharmacologic Measures • Hydration, electrolyte replacement • Multiple small meals. Bland, non-spicy, non-oily foods
Nausea and vomiting is a frequent complication of chemotherapy. It is classified as acute onset, delayed, breakthrough, and anticipatory. The principles for controlling emesis and the types of antiemetic agents used for each of these phases of nausea vomiting may differ slightly.
Prevention of nausea and vomiting is the primary goal in the management of chemotherapy induced emesis. The first step in the management of chemotherapy induced emesis is to assess the emetogenic potential of the chemotherapy because the choice of antiemetic regimen is based upon this classification. The patient should receive antiemetics around the clock to control both acute and delayed emesis. For patients who are at risk for anticipatory emesis, a benzodiazepine such as lorazepam should also be prescribed. There is no difference in efficacy between the oral or intravenous route of administration of the antiemetics; however, if the patient has ongoing emesis, the intravenous or rectal route is preferable. The side effect profile of the different classes of antiemetics is also an important factor to consider. Elderly patients are especially susceptible to the side effects of some antiemetic drugs, for example, the phenothiazines, butyrophenones, and high dose metoclopramide may cause excessive sedation, hypertension, and extrapyramidal reactions. The steroids may cause hyperglycemia, agitation, insomnia, and irritability. On the other hand, the serotonin antagonists are not associated with significant side effects.
The non-pharmacologic measures used to treat chemotherapy induced emesis include hydration and electrolyte repletion as needed. Patients should be advised to eat multiple small meals consisting of bland foods that are not spicy or oily.

Copyright 2011 American Society of Consultant Pharmacists
Pharmacologic Agents for Control of Chemotherapy-Induced Nausea & Vomiting
• Serotonin (5-HT3) Antagonists – ondansetron, granisetron, dolasetron, palonosetron • NK-1 Antagonist – aprepitant • Steroids – dexamethasone, prednisone • Phenothiazines – prochlorperazine, promethazine, chlorpromazine • Butyrophenones – haloperidol, droperidol • Benzamides – metoclopramide, trimethobenzamide • Benzodiazepines – lorazepam, alprazolam • Cannabinoids – dronabinol • Anticholinergic – scopolamine • Antihistamine – diphenhydramine, dimenhydrinate, meclizine, cyclizine
Emetogenecity of the Chemotherapy Regimen
(Risk of Emesis) Recommended AnAemeAc Regimen for Acute Emesis
High (>90%) • 5HT3 Antagonist + Cor:costeroid
• +/-‐ NK-‐1 antagonist
Moderate (30-‐90%) 5HT3 Antagonist + Cor:costeroid
Low (10-‐30%) Single agent cor:costeroid or dopamine antagonist or phenothiazines or butyrophenones
Minimal (< 10%) NONE

Copyright 2011 American Society of Consultant Pharmacists
Pharmacologic Agents for Control of Chemotherapy-Induced Nausea & Vomiting
Emetogenicity
Options for Delayed Emesis
High • Dexamethasone Plus 5-HT3 antagonist or metoclopramide
Moderate • Dexamethasone • OR Dexamethasone + 5HT3 OR5HT3 • OR metoclopramide + 5HT3 ORmetocopramide
Low / Minimal • NONE
There are many pharmacologic options for the treatment of chemotherapy induced nausea and vomiting and they include the serotonin antagonists, corticosteroids, phenothiazines, anticholinergics, and the newly approved neurokinin antagonists.
The administration of the serotonin antagonist in conjuntion with a corticosteroid has been proven to be effective in the management of acute-onset nausea and vomiting and should be considered as first line therapy for highly to moderately emetogenic chemotherapy regimens. The NK-1 antagonist, aprepitant, should be added for multi-day chemotherapy regimens that are highly emetogenic and is associated with significant risk for delayed nausea and vomiting.

Copyright 2011 American Society of Consultant Pharmacists
Pharmacologic Agents for Control of Chemotherapy-Induced Nausea & Vomiting
For patients receiving low emetogenicity chemotherapy regimens, single agent antiemetic is effective in preventing nausea and vomiting and the options include a corticosteroid, phenothiazine, or butyrophenone.
For anticipatory nausea and vomiting, a benzodiazepine such as lorazepam is effective.
In general, all 5-HT3 antagonists are considered to be equally efficacious and the oral route is as effective as the intravenous route. The distinguishing characteristic is that palonosetron has a 100-fold higher binding affinity for the 5-HT3 receptor and a longer half life compared to the other serotonin antagonists. Palonosetron has equivalent efficacy for control of acute emesis as compared to the other 5HT3 antagonists. However, for delayed emesis palonosetron may be better. Palonosetron’s role in the treatment of chemotherapy induce emesis is not well defined yet at this point, but as we have more data available, it may the agent of choice for highly emetogenic chemotherapy regimens that have a high potential of causing delayed nausea and vomiting.

Copyright 2011 American Society of Consultant Pharmacists
Minimizing Chemotherapy-Associated Toxicities
Recommendations for Minimizing Toxicities Associated with Chemotherapy
• Initial patient evaluation with the comprehensive geriatric assessment • Exclude frail patients from aggressive treatment • Institute nutrition support, social support • Control underlying diseases and disabilities • Adjust chemotherapy doses according to patient’s creatinine clearance, liver function, and bilirubin level • Maintain hemoglobin levels above 12 g/dl • Administer granulocyte hemopoietic growth factors prophylactically in patients > 70 years of age receiving CHOP or similar
regimens • For patients > 60 years administer granulocyte hemopoietic growth factors prophylactically for induction or consolidation
therapy for acute myelogenous leukemia • Provide aggressive fluid resuscitation for mucositis and diarrhea • Consider less toxic alternatives to doxorubicin where there is data demonstrating equal effectiveness in patients > 70 years • Provide antiemetics to prevent nausea and vomiting • Counsel patient to take laxative and stimulant agents to prevent constipation associated chemotherapy agents that causes
autonomic neuropathy
Copyright 2011 American Society of Consultant Pharmacists
Minimizing Chemotherapy-Associated Toxicities
There are many factors to consider in the treatment of the elderly patient diagnosed with cancer.A comprehensive geriatric assessment is an essential first step to determine the patient’s overall health, functional status and support network.The decision to treat the patient should not be from preconceived perceptions that elderly patients are automatically not able to tolerate chemotherapy, surgery, or radiation therapy.Instead, therapy should be individualized based upon the patient’s specific organ status function, performance status, comorbid conditions, predicted life expectancy, and desire outcome of treatment.
If chemotherapy is deemed appropriate for the patient, aggressive measures should be taken prevent toxicities.Appropriate adjustment of chemotherapy dose based upon kidney, heart, lung, or liver function should be explored.The administrations of colony stimulating factors to facilitate hematopoetic recovery should be considered.Close patient monitoring for side effects such as mucositis, diarrhea or constipation should be performed in order to institute appropriate supportive care as soon as possible.
As our population ages and the number of elderly people is predicted to almost double by the year 2030, it is crucial that clinicians become familiar with the common health issues faced by this patient population.Therapy should not be withheld due to discrimination based on age and lack of understanding of the physiologic status of this group of patients.Systematic evaluation of each patient and individualized therapy is the key to ensuring appropriate therapeutic outcome and treatment of the elderly patient population diagnosed with cancer.

Copyright 2011 American Society of Consultant Pharmacists
References
For additional information, see:
Balducci L. Anemia, Cancer, Aging. Cancer Control 2003 Nov/Dec; 10(6); 478-484.
Balducci L. Evidence-based management of cancer in the elderly. Cancer Control 2000 Jul/Aug; 7(4); 368-374.
Balducci L, Beghe C. Prevention of cancer in the older person. Clin Geriatr Med 2002 Aug; 18(3); 505-528.
Balducci L, Beghe C. Cancer and age in the USA. Crit Rev Oncol Hematol 2001;37;137-145.
Balducci L, Beghe C. The application of the principles of geriatrics to the management of the older person with cancer. Crit Rev Oncol Hematol 2000;35;147-154.
Balducci L, Extermann M. Cancer and aging. An evolving panorama. Hematol Oncol Clin North Am 2000 Feb;14(1);1-16.
Balducci L, Hardy CL, Lyman GH. Hemopoietic reserce in the older cancer patient: clinical and economic considerations. Cancer Control 2000 Nov/Dec; 7(6); 539-546.
Balducci L, Lyman G, Ozer H. Patients aged > 70 are at high risk for neutropenic infection and should receive hemopoietic growth factors when treated with moderately toxic chemotherapy. J Clin Oncol 2000; 19; 1583-1585.
Balmer C., Valley A. W.(1996).Basic Principles of cancer treatment and cancer chemotherapy. In: Dipiro JT, Talbert RL, Yee GC, et al. (Eds). Pharmacotherapy: A Pathophysiologic Approach. Samford: Appleton and Lange, 2403-2466.
Carbone PP. Advances in the systemic treatment of cancers in the elderly. Crit Rev Oncol Hematol 2000;35;201-218.

Copyright 2011 American Society of Consultant Pharmacists
References
Cohen, H. J.(1994).Oncology and aging:Generaly principles of cancer in the elderly.In Hazzard, W. R., Bierman, E.L., Blass, J. P., Ettinger, W. H. & Halter, J. B. (Eds.). Geriatric Medicine and Gerontology, 3rd ed.New York:McGraw-Hill: 77-90.
Ettinger, D. S. (1995).Preventing chemotherapy-induced nausea and vomiting: An update and a review of emesis. Semin Oncol; 22(4) Suppl 10:6-18.
Groopman JE, Itri L. Chemotherapy-Induced Anemia in Adults: Incidence and Treatment. J Natl Cancer Inst 1999 Oct; 9(19); 1616-1634.
Grunberg,S. M., HeskethP. J. (1993). Control of chemotherapy-induced emesis. N Engl J Med; 329(24):1790-97.
Jacox, A. K., Carr, D. B, Payne, R, et al. (1994). Management of cancer pain. Clinical practice guideline no. 9. Rockville, MD: Agency for Health Care Policy and Research (AHCPR publication no. 94-0592).
Kennedy BJ. Aging and cancer. Oncology (Huntingt)2000 December; 14(12);1731-1740.
Levy, M. H. (1996). Pharmacologic treatment of cancer pain. N Engl J Med; 335(15):1124-32.
Lichtman, SM. Chemotherapy in the elderly. Semin Oncol 2004 April; 31(2);160-174.
Lichtman, SM. Guidelines for the treatment of elderly cancer patients. Cancer Control 2003 Nov/Dec; 10(6); 445-452.
Lichtman, S. M. (1995). Physiological aspects of aging Implications for the treatment of cancer. Drugs-Aging;7(3):212-21.

Copyright 2011 American Society of Consultant Pharmacists
References
National Cancer Institute http://www.nci.nih.gov/
National Comprehensive Cancer Network. Practice Guidelines in Oncology. Version.1.2004. Antiemesis
National Comprehensive Cancer Network. Practice Guidelines in Oncology. Version.2.2004. Cancer and Treatment Related Anemia.
Pharmaceutical Information Network: Cancer Information Center http://pharminfo.com/disease/cancer_db.html
Pizzo, P. A. (1993). Management of fever in patients with cancer and treatment-induced neutropenia. N Engl J Med; 328(18):1323-1332.
Portenoy, R. K. (1993). Cancer pain management. Semin Oncol;20(2) Suppl 1:19-35.
Repetto L, Biganzoli L, Koehne CH, Luebe AS, Soubeyran P, Tjan-Heijnen VCG, Aapro MS. EORTC Cancer in the elderly tsk force guidelines for the use of colony-stimulating factors in elderly patients with cancer. Eur J Cancer 2003; 39; 2264-2272.
Repetto L, Balducci L. A case for geriatric oncology. Lancet Oncol May 2002; 3; 289-297.
Repetto Lazzaro, Comandini D. Cancer in the elderly: assessing patients for fitness. Crit Rev Oncol Hematol 2000;35;155-160.
Rosti G, Kopf B, Cariello A, Monti M, Dazzi C, Papiani G, et al. Prevention and therapy of neutropenia in elderly patients. Crit Rev Oncol Hematol 2003; 46; 247-253.

Copyright 2011 American Society of Consultant Pharmacists
References
Schwartz R. N. (1995). Cancer in the Elderly. In: Delafuente J. C., Stewart,R. B., (Eds.) Therapeutics in the elderly. Cincinnati: Harvey Whitney Books, 500-12.
Tsao AS, Kim ES, Hong WK. Chemoprevention ofCancer. CA Cancer J Clin 2004 May/June; 54; 150-180.
University of Pennsylvania Cancer Center: OncoLink http://cancer.med.upenn.edu/
Yancik R, Ries L Aging and cancer in America. Demographic and epidemiologic perspectives. Hematol Oncol Clin North Am 2000 Feb;14(1);17-23
Yancik R, Ries L.Cancer in older persons: An international issue in an aging world. Semin Oncol 2004 Apr;31(2):128-136
Zagonel V, Fratino L, Sacco C, et al. (1996). Reducing chemotherapy-associated toxicity in elderly cancer patients. Cancer Treat Rev; 22:223-244.
Zoorob R, Anderson R, Cefalu C, Sidani M. Cancer screening guidelines. Am Fam Physicians 2001; 63: 1101-1112.
Zulian GB. Health care delivery in the older person with cancer. Crit Rev Oncol Hematol 2000;35;227-232.

Copyright 2011 American Society of Consultant Pharmacists
Cancer of the Breast, Lung, and Brain
Learning Objectives:
By the end of this review concept, you should be able to:
• Cite the epidemiologic trends associated with lung, breast and brain cancers.
• Differentiate the signs and symptoms of presentation and diagnosis of lung, breast and brain tumors.
• Analyze the various treatment regimens and related effects for lung, breast and brain cancers.
• List common sites for metastases for lung, breast and brain cancers.

Copyright 2011 American Society of Consultant Pharmacists
Lung Cancer
Incidence • Estimated 219,440 new cases in 2009
• Male: 116,090 cases • Female: 103,350 cases
Mortality • Estimated 159,390 deaths in 2009
• Male: 88,900 deaths • Female: 70,490 deaths
• Overall 5 year survival rate is 15% • 88% mortality rate
• More than 2/3 of patients are over 65 years of age
Epidemiology in Elderly Patients • Median age at diagnosis is 69 years
• More than 50% are over 65 years of age • More 30% are over 70 years of age
Lung cancer is the most common cause of cancer-related death in both men and women in the United States. It accounts for 15% of all cancer diagnosis and 29% of all cancer related deaths. The risk of developing lung cancer rises with age. During the last decade, the incidence and mortality from lung cancer has decreased among individuals who are 50 years of age or younger; on the other hand, the incidence has increased among those 70 years of age and older. In considering gender, the incidence rate of lung cancer declined significantly in men and the death rate declined at 2% per year from 1994 to 2004. In women, there was a sharp rise in lung cancer incidence in the 1960s and since 1987, more women have died from lung cancer than breast cancer. After increasing for many decades in women, the lung cancer death rates are finally approaching a plateau

Copyright 2011 American Society of Consultant Pharmacists
Classification of Lung Cancers
Lung cancer is divided into 2 major histologic types: non-small cell lung cancer and small cell lung cancer. Non-small cell lung cancer is the more common subtype and accounts for more than 85% of all lung cancer cases. Small cell lung cancer accounts for only 15% of all lung cancer cases. Non- small cell lung cancer is often diagnosed in the advanced stage of the disease and is generally considered to be chemotherapy resistant. Small cell lung cancer is rarely cured and it is characterized by a rapid doubling time, high growth fraction, and early development of metastasis.
Non-small cell lung cancer is further classified as adenocarcinoma, squamous cell carcinoma and large cell carcinoma. Adenocarcinoma is the most common subtype and is most frequently observed in patients who never smoked, women, and is rising in incidence in younger adults. Adenocarcinoma may also metastasize rapidly to other sites such as liver, bones, brain, and adrenal glands. Squamous cell carcinoma is the second most common subtype of non-small cell lung cancer and tends to be more indolent.
Subtypes
Non Small Cell Lung Cancer (85%) Adenocarcinoma (40%)
Women
Non-‐Smokers
Squamous Cell Carcinoma (20%) Large Cell Carcinoma (5%)
Small Cell Lung Cancer (15%) Small Cell or Oat Cell

Copyright 2011 American Society of Consultant Pharmacists
Risk Factors for Developing Lung Cancer
Tobacco • 20 fold increase in lung cancer risk • cause of 90% of lung cancers in men • cause of 75-85% of lung cancers in women • Exposed non-smokers (second-hand smoke)
• 25-35% increased risk compared to non-smokers
Genetic predisposition • Family history • Germ-line mutation in:
• DNA repair genes • Epidermal growth factor receptor gene • p53 tumor suppressor gene
Occupational and chemical exposure • Radon, ionizing radiation • Asbestos • Arsenic • Chromium • Nickel
Cigarette smoking is the most important risk factor for lung cancer. Smoking causes all types of lung cancer but it is most strongly linked with small cell lung cancer and squamous cell lung cancer. There is a dose-response relationship in the development of lung cancer where the risk increases with increased duration of smoking and the number of cigarettes smoked per day. The risk of developing lung cancer decreases after smoking cessation and quitting smoking can benefit at any age no matter how long a person has smoked. The decrease in risk, however, will not be equal to that of a non-smoker.
Reports of familial clustering of lung cancer suggest that there is a hereditary basis to the development of lung cancer. Lung cancer susceptibility and risks are increased in germ line mutations p53 tumor suppressor genes, epidermal growth factor receptor genes or DNA repair genes.
Other less common causes of lung cancer include exposure to radon gas, asbestos, and carcinogenic chemicals such as organic arsenic compounds, nickel, and chromium.

Copyright 2011 American Society of Consultant Pharmacists
Screening and Diagnosis for Lung Cancer
Screening • No recommendation for routine screening for early detection of lung cancer • National Lung Cancer Screening Trial
• Compares low dose CT vs. chest x-ray for early detection of lung cancer • Enrolled current and former smokers • Designed to detect improvement in mortality with CT screening • Results are pending and expected to be available around 2012
Work-Up and Diagnosis of Lung Cancer • History and Physical Exam
• Biopsy and pathological review for classification of lung cancer histology • Chest X-Ray • Chest, liver CT scans • MRI or CT scan of head for small cell lung cancer • Bone Scan • Baseline CBC, serum chemistries, liver function tests, LDH
At the present time, there are no standard screening recommendations for the early diagnosis of lung cancer. This is because neither chest x-ray nor sputum cytology has been shown to reduce mortality. Ongoing clinical trials are evaluating the efficacy of different screening and early detection methods for lung cancer and its role in possibly decreasing mortality. The National Comprehensive Cancer Network encourages high-risk individuals to participate in these trials.
For the diagnostic work up of lung cancer, a biopsy and an analysis of the tumor by a pathologist is necessary for a definitive diagnosis. Other additional tests include a chest x-ray and CT scan of the chest, liver, and brain, and a bone scan for evaluation of metastasis. Baseline complete blood count, serum chemistries and liver function tests are also essential to evaluate potential toxicity from chemotherapy.

Copyright 2011 American Society of Consultant Pharmacists
Clinical Manifestations of Lung Cancer
Clinical Manifestations of Lung Cancer • Persistent cough • Sputum streaked with blood • Chest pain • Voice change • Recurrent pneumonia or bronchitis • Pleural effusion • Superior vena caval obstruction • Bone Pain • Neurologic symptoms • Spinal cord compression
A new or changing cough that is sometimes associated with blood is the most common presenting symptom of lung cancer. Frequently, patients may also manifest dyspnea, hoarseness, anorexia, weight loss and fatigue. Patients with metastatic disease to the brain can present with neurologic symptoms such as severe headaches and double vision. Other extrapulmonary symptoms include bone pain or pathologic fractures secondary to bone metastasis or liver dysfunction due to spread of the cancer to the liver. Compression of the superior vena cava by the lung cancer may cause patients to develop shortness of breath and swelling of the face and arms because blood is not able to return to the heart.
Patients with small cell lung cancer may present with a paraneoplastic syndrome, which are a collection of symptoms that result from the production of biologically active substances by the tumor. These signs and symptoms occur remotely from the primary tumor site or the metastatic site and may be endocrine, neuromuscular or musculoskeletal in nature. Eaton Lambert myasthenic syndrome presenting with proximal leg weakness is an example of a neurologic manifestation. SIADH due to the production of vasopressin or Cushing’s syndrome due to the production of adrenocorticotropic hormone by the cancer cells is a another common manifestation of the paraneoplastic syndrome.
Paraneoplastic Syndrome • Weight loss/cachexia • Syndrome of Inappropriate Anti-Diuretic Hormone (SIADH) • Cushing’s Syndrome • Hypercalcemia • Eaton Lambert myasthenic syndrome

Copyright 2011 American Society of Consultant Pharmacists
Staging of Lung Cancer
Non Small Cell Lung Cancer
TNM Staging System Tumor size; Lymph node involvement; Metastasis
Stage I - confined to the lung without lymphatic spread Stage II - large tumor with lymph node involvement in the same side of the chest where the tumor originated. Stage III- includes lymph node and other regional involvement near the lung Stage IV - includes any tumor with distant metastasis to sites such as the liver, bone or brain
Small Cell Lung Cancer
Limited Disease - tumor is confined to the side of the chest where it originated (ipsilateral hemithorax): the mediastinum and the supraclavicular lymph nodes. Can be safely encompassed within a tolerable radiation field.
Extensive Disease – disease beyond ipsilateral hemithorax. Metastasis to liver, bone, brain or may include malignant pleural or pericardial effusion or hematogenous metastasis
Non-Small Cell Lung cancer is classified by the TNM staging system according to the American Joint Commission on Cancer. T is for tumor size, N evaluates the presence of lymph node involvement and M assesses for metastasis. These staging procedures are useful in determining if the tumor is surgically resectable and the prognosis for the patient.
Small cell lung cancer is usually advanced at the time of diagnosis; therefore; it is classified as either Limited Disease or Extensive Disease.

Copyright 2011 American Society of Consultant Pharmacists
Lung Cancer Prognosis
Non-‐Small Cell Lung Cancer
Stage Incidence 5-‐year survival rate
Stage I 10% 57-‐67%
Stage II 20% 40-‐55%
Stage IIIA 15% 23-‐25%
Stage IIIB 15% 3-‐7%
Stage IV 40% 1%
Small Cell Lung Cancer
Stage 2 year survival rate Median overall survival
Limited Disease 40% 14-‐20 months
Extensive Disease Less than 5% 9-‐11 months

Copyright 2011 American Society of Consultant Pharmacists
14.02.07 Lung Cancer Prognosis
Good Prognostic Factors
• Early stage of the disease at diagnosis • Good performance status • Weight loss not more than 5% • Female gender
Poor Prognostic Factors
• Mutation of p53 tumor suppressor gene • Activation of k-ras oncogenes • Elevated LDH • Endocrine paraneoplastic syndrome • Poor performance status
Factors that predict good prognosis include early stage at diagnosis, good performance status, weight loss of less than 5%, and female gender. Unfortunately, only about 30% of non-small cell lung cancer patients are diagnosed with stage I or II of the disease, the remaining 70% are diagnosed with advanced stage III or IV. For small cell lung cancer, about one-third of patients present with limited disease and two thirds present with extensive disease.
As can be seen from the table, 5-year survival rate is highest for patients diagnosed with stage I or II non small cell lung cancer. Survival is poorest in patients diagnosed with extensive stage small cell lung cancer where the 2-year survival rate is less than 5%.

Copyright 2011 American Society of Consultant Pharmacists
Non-Small Cell Lung Cancer Treatment Options
Surgery
• Localized disease • Potentially curative for stage I and II • Lobectomy is the standard surgical procedure • Rarely indicated for stage IV except for: • Solitary lesion brain metastasis
Radiotherapy
• Unresectable cancers (stage I through IIIB) • Radiation alone or in combination with chemotherapy • Adjuvant radiation therapy with chemotherapy after surgery • Stage III
Surgical resection is the cornerstone of therapy for patients with stage I through IIIA non-small cell lung cancer. For stage I and II disease, it is the best option for cure if the cancer can be completely resected and the patient is able to tolerate the surgical procedure.
Radiation with curative intent is a viable alternative for patients who are not able to tolerate surgery because of other comorbid conditions. It also indicated for non-resectable stage IIIB non-small cell lung cancer. For these situations, radiation is usually administered in combination with chemotherapy to optimize outcome.
Radiation in combination with chemotherapy is also indicated as adjuvant therapy after surgical resection in patients with stage IIIA disease.

Copyright 2011 American Society of Consultant Pharmacists
Non-Small Cell Lung Cancer Treatment Options
Chemotherapy
• Resectable stage I through III • Adjuvant therapy after surgery • Cisplatin based chemotherapy offers survival advantage • Carboplatin + paclitaxel if patient is not able to tolerate cisplatin
Unresectable stage IIIA and IIIB • Concurrent chemotherapy with radiation • Cisplatin based therapy in combination with:
• Etoposide or vinblastine or gemcitabine or paclitaxel or vinorelbine • Carboplatin + Paclitaxel if patient is not able to tolerate cisplatin
Metastatic or recurrent disease
First-line therapy • 2 drug regimens (doublet) preferred • Platinum (cisplatin or carboplatin) based with any of the following:
• Docetaxel • Paclitaxel • Gemcitabine • Vinorelbine

Copyright 2011 American Society of Consultant Pharmacists
Non-Small Cell Lung Cancer Treatment Options
Second line therapy • Disease progression during or after 1st line therapy • May use single agent:
• Docetaxel (Taxotere®) or • Pemetrexed (Alimta®)
Targeted Therapy • Bevacizumab (Avastin®) – inhibits angiogenesis
• Non-squamous cell carcinoma • No history of hemoptysis • No untreated CNS metastasis
Erlotinib (Tarceva®) • First-line therapy with or without chemotherapy
• Advanced or metastatic disease • Never smoked • Active epidermal growth factor receptor (EGFR) mutation
• Second line therapy • Disease progression during or after 1st line chemotherapy
• Third line therapy

Copyright 2011 American Society of Consultant Pharmacists
Non-Small Cell Lung Cancer Treatment Options
Administering adjuvant chemotherapy after surgical resection of stage I, II or III non-small cell lung cancer has been shown to improve survival.
In patients with unresectable disease, concurrent chemotherapy with radiation is the treatment of choice. Median survival for patients is about 16 to 17 months.
Chemotherapy is primarily palliative for patients with metastatic lung cancer. It has been shown that combination chemotherapy with 2 agents produce 30-40% one-year survival rate and is superior to single agent as first line therapy.
If chemotherapy is used, a platinum-based combination chemotherapy regimen is the preferred choice. The platinum is usually cisplatin. Combination chemotherapy prolongs survival, improves symptoms and quality of life. All the different platinum-based doublets are considered equally efficacious and the response rate and survival did not differ between the regimens.
If a patient fails first line therapy, single agent chemotherapy with activity against non-small cell lung cancer is the next step. Docetaxel, pemetrexed and erlotinib are indicated as single agent second line therapy. Pemetrexed is a multi-targeted antifolate agent.
Bevacizumab is a monoclonal antibody that blocks vascular endothelial growth factors and inhibits angiogenesis. In 2006, it received FDA approval for unresectable, locally advanced, recurrent or metastatic non-small cell lung cancer. It is administered in conjunction with the carboplatin plus paclitaxel chemotherapy regimen. To be eligible for this therapy the patient has to be diagnosed with adenocarcinoma or large cell carcinoma. Patients with squamous cell subtype, hemoptysis at baseline or brain metastasis are not eligible because it was found that they are at higher risk of bleeding in phase II studies.
Erlotinib is a small molecule inhibitor of the epidermal growth factor receptor tyrosine kinase and inhibits cell proliferation. It was approved by the FDA in 2004 for locally advanced or metastatic non-small cell lung cancer after failure of at least one prior chemotherapy regimen. It may be given as first line therapy for patients who have known active epidermal growth factor receptor mutation and never smoked. Diarrhea and acne like rash are the dose limiting toxicities for this therapy.

Copyright 2011 American Society of Consultant Pharmacists
Small Cell Lung Cancer Treatment Options
Surgery • Limited role in small cell lung cancer
• Indicated for early stage, limited disease
Radiation • Combination with chemotherapy in limited stage disease
• Local failure reduced by 25-30% • 2 year survival improved by 5-7%
Chemotherapy
• Limited stage • Concurrent chemotherapy and radiation • Cisplatin + Etoposide x 4-6 cycles
Extensive stage • Cisplatin + etoposide • Carboplatin + irinotecan
Extensive stage with brain metastasis • Chemotherapy before or after whole brain radiation therapy

Copyright 2011 American Society of Consultant Pharmacists
Small Cell Lung Cancer Treatment Options
Failure during or after first line therapy • Second Line Therapy
• Taxanes (paclitaxel or docetaxel) • Ifosfamide • Gemcitabine • Camptothecin (irinotecan, topotecan) • Vinorelbine • Oral etoposide • CAV (Cyclophosphamide, doxorubicin, vincristine)
Prophylactic Cranial Irradiation (PCI) for Small Cell Lung Cancer • Recommended for:
• Limited or extensive stage disease with: • Complete or near complete response to therapy • Partial response to initial therapy
• NOT recommended for patients with: • Multiple comorbidities • Poor performance status • Impaired mental function
Limited stage small cell lung cancer is diagnosed in approximately 30% of patients and early stage limited disease is diagnosed in less than 5% of patients; the other two-thirds of small cell lung cancer patients present with hematogenous spread at the time of diagnosis.
Surgery is indicated only for patients with early limited stage disease, which, in general, is defined as a tumor that is 3 cm or less in size. This means that only 2 to 5% of patients diagnosed with small cell lung cancer are candidates for surgical resection. Surgery offers no benefit for tumors larger 3 cm.

Copyright 2011 American Society of Consultant Pharmacists
Lung Cancer and Older Patients
NON-SMALL CELL LUNG CANCER
• Stage IB – II • Restrospective Study: Surgery followed by combination cisplatin + vinorelbine vs.
surgery followed by observation • Patients 65 years or older receive less chemotherapy than younger counterparts • Elderly patients receiving chemotherapy have improved survival with tolerable toxicity
• Locally Advanced Disease (Stage III) • Selected fit elderly patients may receive combined chemotherapy and radiation; preferably in a clinical trial
Advanced Disease • Single agent third-line chemotherapy such as vinorelbine is recommended as standard of care instead of best
supportive care alone • Select fit elderly patients may be eligible for cisplatin based doublet therapy
• Prospective trials with attenuated cisplatin dose in combination with gemcitabine or vinorelbine show activity against the cancer with good toxicity profile in elderly patients
• Need large clinical trials specifically designed for elderly patients to confirm these results. • Bevacizumab is not well tolerated in elderly patients in combination with chemotherapy and is not recommended
SMALL CELL LUNG CANCER
• Limited Stage Disease • Concurrent chemotherapy and radiation
• similar response rate as younger patients with potential for cure • significantly more toxicity compared to younger patients

Copyright 2011 American Society of Consultant Pharmacists
Lung Cancer and Older Patients
Extensive Stage Disease • Elderly patients experience more toxicity compared to younger patients • Should not a priori exclude chemotherapy in the elderly since small cell lung cancer is very responsive to chemotherapy
Elderly cancer patients often present with multiple comorbidities and physiological limitations such as decreased organ function that makes it challenging to select optimal treatment options for them. Furthermore, in lung cancer, if the patient underwent surgical resection, they may also be at higher risk for experiencing chemotherapy induced toxicity.
There are few prospective studies evaluating the tolerability of chemotherapy in elderly patients with lung cancer. Available data are usually from retrospective analysis and is not ideal for basing treatment decisions. More clinical trials that are specific for the elderly patient population are needed in order to better define optimal therapy for elderly patients.
For many stages of lung cancer, cisplatin based chemotherapy with or without radiation is the standard of care. Some elderly patients may be able to tolerate the toxicity of these regimens and derive survival benefit; therefore, dose reduction of chemotherapy or withholding chemotherapy should not be a priori planned strategy for elderly patients diagnosed with lung cancer. There are phase III trials that support the use of single agent chemotherapy in place of best supportive care for patients with metastatic disease who are not able to tolerate combination chemotherapy. Patients with good performance status, adequate organ function and minimal comorbid conditions should be carefully selected for chemotherapy or combination therapy with radiation. If the data is available, the decision should be supported by data from clinical trials that are specifically designed to evaluate the effect of therapy in elderly patients.

Copyright 2011 American Society of Consultant Pharmacists
Symptom Management in Lung Cancer
Symptom Recommendations
SIADH Fluid restriction, saline for symptomatic patients, demeclocycline, treat the cancer
Cushing’s Syndrome Consider ketoconazole
Cough
Cough suppressants: opioid and non-opioid (e.g. dextromethorphan). Consider steroid therapy if coughing is secondary to radiation pneumonitis
Dyspnea
Short acting opioids, oxygen, relieve anxiety (benzodiazepine), relaxation techniques, cool air or fan
Hypercalcemia Hydration, furosemide, bisphosphonate
Superior Vena Caval (SVC) Obstruction Radiation to shrink tumor and relieve symptoms of SVC obstruction

Copyright 2011 American Society of Consultant Pharmacists
Symptom Management in Lung Cancer
Symptom Recommendations
Side effects from bevacizumab Wound healing complications – Do not administer bevacizumab within 28 days of any major surgery
Nephrotic syndrome- monitor proteinuria by dipstick urinalysis. If urine dipstick is 2+ or greater, obtain 24 hour urine collection. Adminster bevacizumab only if proteinuria is less than 2gm/24 hours
Hypertension- monitor blood pressure every 2 to 3 weeks during treatment with bevacizumab. Initiate appropriate anti hypertensive medication if hypertension develops
Hemorrhage- do not administer to patients with serious hemorrhage or recent hemoptysis. If bleeding occurs discontinue bevacizumab
GI perforation – discontinue bevacizumab if this occurs

Copyright 2011 American Society of Consultant Pharmacists
Symptom Management in Lung Cancer
Surveillance After Lung Cancer Treatment
After recovery from primary therapy Non-Small Cell Lung Cancer Small Cell Lung Cancer
• History and Physical Exam • CT scan
• History and Physical Exam • Chest imaging • Blood work as necessary
Year One Every 4 to 6 months
Every 2-3 months
Year Two Every 3 to 4 months
Year Three
Annually
Year Four Every 4 to 6 months
Year Five
Year 6 and beyond Annually

Copyright 2011 American Society of Consultant Pharmacists
Breast Cancer
• 60 years of age and older • 70% of breast cancer patients • 70 years of age and older • 46% of breast cancer patients
• Breast cancer incidence is 6-fold higher in elderly women
• Breast cancer mortality rate is 8-fold higher in elderly women
New Cases (Invasive Breast Cancer) New Cases (in situ)
Deaths
Total 194,280 62,280 40,610
Female 192,370 40,170
Male 1,910 440

Copyright 2011 American Society of Consultant Pharmacists
Breast Cancer
Breast cancer is the most commonly diagnosed cancer in American women and accounts for thirty two percent of all malignancies. It is the second leading cause of cancer death among women, trailing only after lung cancer. From 2001 to 2004, the incidence of breast cancer started to decline by 3.5% per year, after continuously increasing in incidence for more than 2 decades. This is attributed to the reduced use of hormone replacement therapy after publication of results that linked hormone replacement therapy use to increased risk of heart disease and breast cancer from the Women’s Health Initiative study in 2002. The National Health Interview survey showed that the rate of mammography screening in women 40 years of age and older dropped from 70% in 2000 to 66% in 2005 and this maybe another contributing factor to the decline of breast cancer incidence rates.
Breast cancer mortality has steadily decreased since 1990, with larger decreases in women younger than 50 years of age compared to women who are 50 years of age or older. The reason may be due to breast cancer screening, which detects the disease earlier, and the availability of improved treatment options.
Breast cancer is a disease of aging and more than 50% of breast cancer cases occur in women 60 years and older. As the elderly population in the United States is increasing due to the aging of the “baby boomers”, the number of older patients diagnosed with cancer will also increase accordingly. By the year 2030 an estimated 70.2 million people will be over the age of 65 and the number of women diagnosed with breast cancer will increase by 72%.This escalating number of elderly women who will be diagnosed with breast cancer stresses the need for more research focusing in this patient population for the best evidence to prevent and treat the disease.

Copyright 2011 American Society of Consultant Pharmacists
Risk Factors for Developing Breast Cancer
Age:
• Lifetime risk is 1 in 7 based on life expectancy of 85 years • Family history (1st degree relative) • Previous breast cancer diagnosis • Diagnosis of lobular carcinoma in situ or benign breast disease • High breast tissue density • Irradiation of the breast • Genetic mutations in the BRCA1 and BRCA2 genes
Estrogen Exposure History • Early age at menarche (14 years of age or younger) • Late onset of menopause (55 years of age or older) • Age of birth of first child (>30 years) • Nulliparity
Modifiable risk factors • Obesity • Post menopausal obesity • Post menopausal hormone replacement therapy • Physical inactivity • Alcohol consumption
Estimated Risk of Developing Breast Cancer
Age (years)
1 in 14 60-79
1 in 24 40-59
1 in 228 < 39
Copyright 2011 American Society of Consultant Pharmacists
Risk Factors for Developing Breast Cancer
Modified Gail Model of Breast Cancer Risk Assessment: • A model to determine the relative risk of developing breast cancer • Analyzes the combination of the following factors:
• History of ductal or lobular carcinoma in situ • Age (> 35 years) • First degree relatives with breast cancer • Prior breast biopsies and presence of atypical ductal hyperplasia • Age at menarche • Age at first live birth • Ethnicity
Many risk factors are associated with the development of breast cancer; however, it should be noted that 60% of women with breast cancer have no identifiable major risk factors, emphasizing that the actual cause of breast cancer is largely unknown. Aside from being female, age is the most significant risk factor for the development of breast cancer. A positive family history of breast cancer, a previous diagnosis of breast cancer or benign breast disease such as hyperplasia, or high dose radiation to the chest are additional risk factors.
Mutations of the breast cancer 1 or 2 gene, otherwise known as BRCA1 or BRCA2 gene, predisposes the woman to an 80% lifetime risk of developing breast cancer. BRCA1 or BRCA2 gene mutation accounts for 5 to 10% of all breast cancer cases and only 1% of the general population has a mutation in either of these genes.

Copyright 2011 American Society of Consultant Pharmacists
Risk Factors for Developing Breast Cancer
Evaluation of reproductive factors that increase breast cancer risk include obtaining the patient’s menstrual history, where a history of early menarche defined as 14 years of age or younger and late menopause defined as 55 years of age or older, increases the risk. Never having children or having children after age 30 also increases the risk of developing breast cancer.
The risk of a woman developing breast cancer may be predicted mathematically by various models. The modified Gail Model is one such tool. Seven different factors are analyzed in this model and the composite score of relative risk for each factor is utilized to calculate the overall risk of developing breast cancer. The instrument does have its limitations and it is only one of many models that predict the risk of developing breast cancer.
Accurate assessment of a woman’s risk of developing breast cancer is important and may have ramifications for therapy decisions. A woman should undergo counseling and thorough discussion with her physician prior to initiating the risk assessment process.

Copyright 2011 American Society of Consultant Pharmacists
Prevention of Breast Cancer
Intervention Benefits Indications Side Effects
Tamoxifen
• ~ 50% ↓ risk of developing breast cancer
* Limited data for women with BRCA 1/2 mutation
• Premenopausal
• Postmenopausal
* 35 years or older with Gail model 5 year breast cancer risk greater than 1.7
• Endometrial cancer
• Thromboembolism
• Stroke
• Cataract
* Hot Flashes
Raloxifene Equivalent to tamoxifen
• Postmenopausal
* 35 years or older with Gail model 5 year breast cancer risk greater than 1.7
• Endometrial cancer
• Thromboembolism
• Hot flashes
All the side effects are less compared to tamoxifen

Copyright 2011 American Society of Consultant Pharmacists
Prevention of Breast Cancer
Intervention Benefits Indications Side Effects
Prophylactic Bilateral Oophorectomy
• 50% ↓ risk of breast cancer
• 85% ↓ risk ovarian cancer
* Protects women with BRCA 1 or 2 mutation
• BRCA 1 or 2 mutation
* After a woman is done with childbearing
• Osteoporosis
• Cardiovascular disease
* Cognitive changes
Effective means for preventing breast cancer are limited. The antiestrogen tamoxifen is approved by the FDA for reduction of breast cancer in high-risk women. This is based upon results from the NSABP Breast Cancer Prevention Trial that showed a 49% decrease in the short-term risk of developing breast cancer when tamoxifen is initiated in a woman with high risk of developing breast cancer based upon the Gail Model of breast cancer risk assessment.
.Raloxifene was originally evaluated to determine fracture risks in postmenopausal women with osteoporosis. Secondary analysis in this study showed that breast cancer risk was reduced in patients receiving raloxifene compared to patients receiving placebo. Thus, this lead to the STAR trial, which is a Study of Tamoxifen and Raloxifene in postmenopausal women at risk of developing breast cancer. Raloxifene was found to be equivalent to tamoxifen in decreasing the risk of developing breast cancer and is FDA approved for post-menopausal women.

Copyright 2011 American Society of Consultant Pharmacists
Breast Cancer Early Detection Guidelines from the American Cancer Society
Women at increased risk due to family history, past breast cancer history, previous radiation therapy to chest wall, or other risk factors. should consult their physician regarding earlier mammogram screening, more frequent exams or additional tests such as ultrasound or MRI. http://www.komen.org/bse website has video instructions on performing BSE
Mammography Screening Recommendations for Elderly
American Cancer Society and American College of Preventive Medicine No recommendation of when to stop screening based upon age. Should take into consideration patient’s comorbid conditions
American Geriatric Society Mammography every 3 years after 75 years of age if life expectancy is > 4 years
United States Preventative Services Task Force • No evidence of benefit for women over 75 years of age • Mammography screening for women over 70 years with reasonable life expectancy
Screening Recommendations
Breast Self Exam (BSE) Monthly starting at 20 years
Clinical Breast Exam (CBE) Every 3 years in 20’s and 30’s Annually starting at 40 years
Mammogram3 Annually starting at age 40 years
Copyright 2011 American Society of Consultant Pharmacists
Breast Cancer Early Detection Guidelines from the American Cancer Society
The aim of breast cancer screening is to detect the cancer early in its asymptomatic phase with the specific goal of reducing breast cancer mortality.
Breast self examination is considered optional in all age and breast cancer risk groups based upon a large, randomized trial in Shanghai, China that showed instructions in breast self examination has no effect on reducing breast cancer mortality. If a woman chooses to perform periodic breast self-examination, she may review technique instructions at the Susan G. Komen website for breast cancer.
A clinical breast examination performed by a physician during a woman’s periodic health exam provides an opportunity to discuss with the patient the importance of early breast cancer detection. It is also a chance to emphasize to the patient the importance of an awareness of a family history of breast and ovarian cancers in first and second-degree relatives on both maternal and paternal sides.
Breast mammography has been proven consistently in randomized trials to reduce breast cancer mortality by up to 30% although a Cochran Review concluded that it might decrease it by only 15%. There is no consensus on when to start mammography screening and how often. Established guidelines from different countries and medical organizations recommend yearly to biennial mammograms starting at 40 to 50 years of age. The American Cancer Society specifically recommends annual mammogram starting at the age of 40.
Screening mammography for women up to 70 years of age is widely recommended. There is insufficient data to recommend for or against routine mammography screening in women over 70 years of age because no patients older than 74 years and few patients between 70 and 74 years were enrolled in randomized trials of mammography screening. When deciding on routine mammography screening for women over 70 years of age, factors such as the woman’s comorbid conditions, functional status, bone mineral density, interest in preventive care and willingness to accept the potential harm of screening, such as false positives, should be considered.

Copyright 2011 American Society of Consultant Pharmacists
Signs, Symptoms and Workup for Breast Cancer Diagnosis
Signs and Symptoms of Breast Cancer
• Development of lump or swelling in the breast • Skin irritation or dimpling • Nipple pain or retraction • Redness/scaliness of nipple or skin • Discharge other than breast milk
Workup for Breast Cancer
• History and physical exam • Diagnostic bilateral mammogram or ultrasound • Biopsy of tumor
• Fine Needle aspiration • Needle guided biopsy • Open surgical biopsy
• Complete Blood Count • Chest X-Ray • Liver function tests • Determination of hormone receptor status (estrogen and progesterone) • Bone scan if patient has elevated alkaline phosphatase • Abdominal CT scan or ultrasound or MRI if patient has elevated alkaline phosphatase or abnormal liver function

Copyright 2011 American Society of Consultant Pharmacists
Signs, Symptoms and Workup for Breast Cancer Diagnosis
Palpation of a breast lump is the most common sign in most patients diagnosed with breast cancer. On the other hand, sometimes the lump is seen only on mammography and no mass was felt by the woman or health care professional.
The breast lump is often hard, irregular and feels different from the rest of the breast. Patients may also feel a persistent lump in the axilla or under the arm which is a manifestation of enlarged lymph nodes. Irregularity or retraction of the breast skin or nipple may also occur.
Pain in the breast and discharge from the nipple may indicate breast cancer although some benign conditions also manifest these symptoms. Therefore, a medical evaluation by a physician is recommended to differentiate between breast cancer and other benign conditions.
In more advanced breast cancer cases there may be swelling or distortion of the skin and patients may experience symptoms related to other organ involvement such as pain in the area of bone metastasis or lung nodules on chest x-ray from lung metastasis.
In the presence of any of these signs and symptoms a prompt evaluation and diagnosis by a physician is imperative.
The workup of a diagnosis for breast cancer involves obtaining a thorough patient medical history in addition to a physical examination. Necessary laboratory tests that are useful include a complete blood count and chemistries to determine organ function and to detect possible metastasis. A mammogram is indicated to evaluate the suspicious mass and an ultrasound is helpful in determining if the mass is cystic or solid.
The suspicious mass should be biopsied for microscopic examination of the tissue by a pathologist for a definitive diagnosis.
A chest x-ray, bone scan, or abdominal CT scan may also be performed if there is suspicion of metastasis to other sites such as the lungs, bone, or liver.

Copyright 2011 American Society of Consultant Pharmacists
Staging of Breast Cancer
American Joint Commission on Cancer TNM Staging System
In situ • Stage 0 - cancer is confined to within the duct or lobules of the breast and has not broken through the basement membrane • Lobular carcinoma in situ • Ductal carcinoma in situ
Local or Early Disease • Stage I – the cancer is confined to the breast • Stage II – the cancer has spread to lymph nodes on the same side (ipsilateral) of the breast
Locally Advanced Disease • Stage III – the cancer has spread to superficial structures of the chest wall or there is involvement of ipsilateral internal mammary lymph nodes (near the breast bone)
Advanced Disease • Stage IV – metastasis to the liver, lung, bone, brain

Copyright 2011 American Society of Consultant Pharmacists
Staging of Breast Cancer
The TNM staging system is used to stage breast cancer.
The information about the tumor size, lymph node involvement, and metastasis are combined to determine the clinical stage of the breast cancer, which ranges from Stage 0 to Stage IV.
The stage of the breast cancer is directly related to the prognosis and the higher the stage the poorer the prognosis.
The goal of therapy for patients diagnosed with carcinoma in situ or stage 0 breast cancer is to prevent the occurrence of invasive breast disease and to diagnose and treat the cancer early while it is still confined to the ducts within the breast.
The main option for a patient diagnosed with lobular carcinoma in situ is observation because the risk of developing invasive breast cancer is low. Prophylactic bilateral mastectomy or prophylactic tamoxifen therapy may be considered to reduce the risk of developing invasive breast cancer.
Stage I and II breast cancer are potentially curable with surgery, radiation, chemotherapy and hormonal therapy. The goals of therapy for Stage III and IV disease are to prolong survival, control symptoms and maintain quality of life since it is difficult to cure patients at these higher stages of the disease. With improvements in the available treatment options for breast cancer in the past couple of decades, treatment resembles that for chronic disease since sequential use of different chemotherapy agents, hormonal therapy and targeted therapy are able to maintain disease remission.

Copyright 2011 American Society of Consultant Pharmacists
Treatment Options for Breast Cancer
Surgery • Breast conserving surgery followed by radiation • Modified radical mastectomy • Sentinel lymph node biopsy
Complications from surgery • Lymphedema (10 – 30% in women undergoing axillary dissection) • Numbness • Reduced shoulder mobility • Psychological sequelae of mastectomy • Phantom breast sensations
There are 2 types of treatment options for breast cancer, local therapy and systemic therapy. Surgery and radiation therapy are for local control of the cancer. Chemotherapy, hormonal therapy and targeted therapy are considered to be systemic therapy.
Surgery is one of the main treatment options for non-metastatic breast cancer. The type and extent of the surgery depends on the tumor size and the stage of the breast cancer. Breast conserving surgery or modified radical mastectomy are appropriate treatment options for patients diagnosed ductal carcinoma in situ. If the patient received breast-conserving surgery, adjuvant radiation should be administered to prevent the risk of recurrence or local failure. For patients with small size breast cancer, it has been shown that breast conserving surgery such as lumpectomy or segmental resection followed by radiotherapy is equivalent to modified radical mastectomy.
Radical mastectomy, other wise known as Halsted mastectomy, involves removal of the muscles of the chest wall along with the breast and axillary lymph nodes.This procedure is rarely performed in present day practice because it is not any more effective than less radical procedures. Instead, breast conserving surgery and modified or simple radical mastectomy are the more commonly performed surgical procedures.

Copyright 2011 American Society of Consultant Pharmacists
Treatment Options for Breast Cancer
Evaluation of the lymph nodes by axillary dissection is standard for all surgeries to assess the extent of spread of the cancer. Cancer cells found in the lymph nodes indicates possible metastases outside the breast and axillary area to the lungs, liver or bones and signifies that adjuvant chemotherapy or hormonal therapy is required. A sentinel lymph node is the first lymph node that drains and receives fluid from the breast tumor. It is detected by injecting a dye and radioactive isotope around the breast tumor, and then the first lymph node that the dye reaches is removed and examined to determine if there are cancer cells present. If there are cancer cells present, the entire lymph node chain is removed. If there are no cancer cells present, the patient is spared from total removal of the lymph node chain and the morbidities associated with it such as lymphedema.
Side effects associated with breast cancer surgery include reduced shoulder mobility, stiffness, and lymphedema. These side effects may be prevented by a gradual exercise program of the affected arm postoperatively. Phantom breast sensations after a modified radical mastectomy are reported as pain, itching, or the vague sensation that the breast is still present.
Copyright 2011 American Society of Consultant Pharmacists
Treatment Options for Breast Cancer
Radiotherapy
• Localized disease control • Decrease recurrence rate as adjuvant therapy after breast conserving surgery • Relieves pain in patients with metastatic disease to the bone • Side Effects:
• Acute skin erythema (<20% of patients) • Acute pneumonitis (2% of patients) • Fibrosis to skin (rarely seen) • Arm edema (depends on extent of axillary surgery)
The purpose of radiation therapy is to optimize local control of the breast cancer after breast conserving surgery. It is often administered in early stage breast cancer because it reduces the risk of local recurrence from 26% to only 7% and it improves overall survival. Radiation is also administered to patients with metastatic breast cancer. The purpose in this case is to control the spread of the disease and relieve symptoms such as bone pain in the case of bone metastasis.

Copyright 2011 American Society of Consultant Pharmacists
Treatment Options for Breast Cancer
Hormonal Therapy
Indications for Hormonal Therapy in Treating Breast Cancer
• As adjuvant therapy for early disease or advanced breast cancer in women with positive estrogen and/or progesterone receptor hormonal status
• As primary therapy for women with metastatic breast cancer with positive estrogen and/or progesterone receptor hormonal status
• Duration is usually for 5 years for prevention of breast cancer and as adjuvant therapy for early or advanced breast cancer • For metastatic breast cancer, the duration of hormonal therapy is until patient develops progression of the breast cancer • Hormonal therapy should be administered after completion of chemotherapy because it is thought that concurrent
administration decreases the beneficial effect of chemotherapy.
Hormonal Therapy for TreaAng Breast Cancer
IndicaAons Side Effects/ConsideraAons
AnAestrogens (SelecAve Estrogen Recepor Modifiers (SERMs) Blocks estrogen receptor
Tamoxifen
Toremifene
Premenopausal and Postmenopausal ER/PR + Breast Cancer
* No advantage of toremifene over tamoxifen. Complete cross tolerance between tamoxifen and toremifene
• Hot flushes • Thromboembolic events • Endometrial cancer • Cataract • Vaginal dryness
Tamoxifen is metabolized by CYP2D6 to its acAve metabolite
* avoid drugs that are CYP450 inhibitors

Copyright 2011 American Society of Consultant Pharmacists
Treatment Options for Breast Cancer
Hormonal Therapy for TreaAng Breast Cancer
IndicaAons Side Effects/ConsideraAons
Aromatase Inhibitors Inhibits estrogen synthesis
• Anastrozole • Letrozole • Exemestane (steroidal)
Postmenopausal ER/PR + breast cancer
Exemestane is indicated as second line therapy amer tamoxifen failure
Headache, hot flushes, vaginal dryness -‐ occurs less frequent than tamoxifen
• Myalgias/arthralgias, • Osteoporosis • Fractures
Baseline Bone Mineral Density (BMD) measurement: -‐ consider calcium + vitamin D and bisphosphonate if BMD is low
Estrogen Receptor Antagonist Down regula:on of estrogen receptors
Fulvestrant
Second line therapy amer failure with tamoxifen or aromatase inhibitors
Available as intramuscular injec:on
Headaches, nausea, vomi:ng, backache, injec:on site reac:on
Patients diagnosed with primary invasive breast cancer should have their estrogen and progesterone receptor status determined. About 70% of breast cancers are estrogen and/ or progesterone receptor positive and the frequency rises with increasing age.
All patients with positive hormonal receptor status should receive adjuvant hormonal therapy regardless of their age, menopausal status, HER-2 receptor status, or whether or not the patient will be receiving adjuvant chemotherapy.
Copyright 2011 American Society of Consultant Pharmacists
Treatment Options for Breast Cancer
Tamoxifen is the most established adjuvant hormonal therapy for breast cancer in both premenopausal and postmenopausal women. It is generally the first line hormonal therapy used. It has been shown to decrease breast cancer recurrence by 40% and breast cancer death by 31%. Most women tolerate tamoxifen reasonably well. Some may experience mild nausea, menopausal symptoms, hot flushes, headaches, depression, and dizziness. There is also an increased risk of endometrial cancer, retinopathy and thromboembolic events. Women receiving tamoxifen therapy should have regular follow up visits with their physician for monitoring and management of these side effects.
In postmenopausal women, their estrogen is derived from peripheral conversion of circulating androgens by the aromatase enzyme. Aromatase inhibitors are effective in improving disease free survival in postmenopausal women and are indicated for this patient population. They should not be used in premenopausal women because they do not affect ovarian production of estrogens. Aromatase inhibitors have a better side effects profile compared to tamoxifen in terms of blood clots, stroke or endometrial cancer as well as hot flushes and vaginal dryness. On the other hand, more women experience fractures or joint pain on an aromatase inhibitor such as anastrozole compared to tamoxifen.
Hormonal therapy should not be administered concurrently with chemotherapy because chemotherapy inhibits DNA synthesis causing tumor cell death and hormonal therapy has a static effect on tumor cells. The concern is that the growth inhibitory effect of hormonal therapy may diminish the cytotoxic effect of chemotherapy.
Other hormonal agents such as exemestane and fulvestrant are indicated as second line therapy after a patient has failed tamoxifen therapy for the treatment of metastatic breast cancer.
Hormone ablation may also be achieved with surgical procedures such as oophorectomy or administration of leutenizing hormone-releasing hormone analogs. These procedures have not been shown to be more effective than tamoxifen in preventing breast cancer recurrence.

Copyright 2011 American Society of Consultant Pharmacists
Chemotherapy for Breast Cancer
Indications for Chemotherapy • Adjuvant therapy after surgery/radiation for stage II to III disease • As first line therapy for metastatic breast cancer • As neoadjuvant therapy to shrink tumor prior to surgery • As second line therapy after disease recurrence or progression
Chemotherapy Agents • Prefer anthracycline containing combination chemotherapy regimen (doxorubicin or epirubicin) • AND/OR taxane containing combination regimen (paclitaxel or docetaxel) • Single agent chemotherapy may be given for metastatic disease • Oral capecitabine may be given as second line therapy after failure with first line treatment option
Systemic chemotherapy is indicated as adjuvant therapy for high-risk breast cancer patients after surgery or for the treatment of metastatic breast cancer. The administration of adjuvant polychemotherapy and tamoxifen reduces the odds of breast cancer recurrence and death in all age groups younger than 70 years of age.
There are many available chemotherapy regimen options for the treatment of breast cancer. An anthracycline-based regimen has been shown to decrease mortality by 38% in women younger than 50 years of age and 20% in women between 50 and 69 years of age. The addition of a taxane to an anthracycline regimen decreases the mortality rate by another 1.5%. The choice of a chemotherapy regimen depends on the side effects profile of the specific regimen and patient tolerability based upon their comorbid conditions.

Copyright 2011 American Society of Consultant Pharmacists
Chemotherapy for Breast Cancer
Combination chemotherapy for breast cancer is associated with moderate to severe nausea and vomiting, myelosuppression and other organ specific toxicities related to the individual drugs. Congestive heart failure may occur with doxorubicin although the risk depends on the total cumulative dose of the drug the patient is receiving. Neuropathies and hypersensitivity have been associated with the administration of paclitaxel, while pulmonary edema is a side effect of docetaxel.
The oral chemotherapy agent capecitabine, a prodrug of fluorouracil, is currently indicated as either combination therapy with a taxane for metastatic breast cancer that is resistant to an anthracycline or as single agent therapy for metastatic breast cancer that is resistant to both an anthracycline and taxane. The most common side effect associated with capecitabine is hand foot syndrome. Capecitabine should be taken within 30 minutes of a meal.

Copyright 2011 American Society of Consultant Pharmacists
HER-2 Positive and Epidermal Growth Factor (EGFR) Over Expressing Breast Cancer
Characteristics of HER-2 Positive Breast Cancer
• More aggressive clinical course • Increased risk of metastasis • Reduced response to chemotherapy • Higher probability of disease recurrence • Shortened overall survival (median survival time halved compared to HER-2 negative patients ( 3 years
versus 6 to 7 years) • Poorer prognosis
Trastuzumab • Humanized monoclonal antibody that binds selectively to the extracellular domain of HER2
• Degrades HER2 receptor • Promotes antibody dependent cellular toxicity • Induces apoptosis • Inhibits angiogenesis • Affect tumor growth • Additive or synergistic effect with various chemotherapy agents
• Indications: • Adjuvant therapy in early stage breast cancer and metastatic breast cancer that demonstrates HER2 over expression
• Side Effects: • Infusion related reactions; fever and chills
• Premedicate with acetaminophen and diphenhydramine
Copyright 2011 American Society of Consultant Pharmacists
HER-2 Positive and Epidermal Growth Factor (EGFR) Over Expressing Breast Cancer
• Nausea, vomiting, diarrhea • Arthralgia, myalgia • Abdominal pain, chest pain, • Increased risk of cardiotoxicity in conjunction with doxorubicin
• Monitor cardiac ejection fraction
Lapatinib • Oral dual tyrosine kinase inhibitor targeting both HER1 and HER2 receptors • Indications:
• Administered in combination with capecitabine for advanced or metastatic breast cancer that over expresses HER2 after failure with other therapies
• Side Effects: • Nausea, vomiting, diarrhea • Hand foot syndrome
• Administration – do not take with food. Take 1 hour before or after a meal. Do not eat grapefruit or drink grapefruit juice when taking this drug.
The EGFR, or otherwise known as the epidermal growth factor receptor, family of receptors includes four receptors: HER1 (also known as EGFR), HER2, HER3, and HER4.
In 20% to 30% of breast cancers, the HER2 gene is amplified meaning there are excess copies of the gene and the HER2 protein is over expressed meaning there is excess production of the protein. Amplification of HER2 signifies a more aggressive clinical course with poorer prognosis and shortened survival. EGFR or HER1 is over expressed in 27% to 30% of breast cancers.

Copyright 2011 American Society of Consultant Pharmacists
HER-2 Positive and Epidermal Growth Factor (EGFR) Over Expressing Breast Cancer
Trastuzumab is a humanized monoclonal antibody that binds selectively and with high affinity to the extracellular domain of HER2. The mechanism of trastuzmab is not well understood but it is thought that it decreases expression of HER2 from the cell surface, induces antibody dependent cellular cytotoxicity, inhibits angiogenesis, and induces apoptosis.
In metastatic breast cancer with overexpression of HER2, trastuzumab single agent produces 26% response rates and response rates increases to 63 to 79% when it is combined with other chemotherapy agents such as paclitaxel or doxorubicin.
Trastuzumab has been shown to improve disease free survival and overall survival when it is administered with chemotherapy as adjuvant therapy for early stage breast cancer.
The most common toxicity associated with trastuzumab is an infusion related reaction that manifests as fever and chills which occurs with the first dose and improves with subsequent doses.
Congestive heart failure can develop with trastuzumab alone or in combination with paclitaxel or docetaxel and especially with an anthracycline. Patients should be monitored for signs and symptoms of cardiac dysfunction while on trastuzumab therapy.
Lapatinib is available as an oral tablet. It is a dual tyrosine kinase inhibitor that targets both EGFR and HER2 receptors. Lapatinib is indicated to be administered with capecitabine after a patient has failed first line therapy for both advanced and metastatic breast cancer that over expresses HER2. The most common side effects are due to both lapatinib and capecitabine and include nausea, vomiting, diarrhea and hand foot syndrome.

Copyright 2011 American Society of Consultant Pharmacists
Symptom Management in Breast Cancer
Symptom Comments and Recommendations
Hot Flushes Non-pharmacologic therapy: cooling strategies such as using air conditioning and fans, wearing open weave cotton clothing to allow circulation.
Avoid hot, spicy foods, drinking warm liquids or alcohol.
Pharmacologic therapy: venlafaxine, paroxetine, gabapentin or clonidine. If the patient is on tamoxifen, avoid antidpressants that inhibits CYP2D6 such as paroxetine since tamoxifen needs CYP2D6 for metabolism to its active metabolite.
Vaginal Changes Dryness, pruritus, increased risk of urinary tract infections, dyspareunia (difficult or painful sexual intercourse).
Non-estrogenic vaginal lubricants are recommended to relieve symptoms of dryness and dyspareunia.
Systemic estrogen or topical estrogens are not recommended for women with hormone positive breast cancer.

Copyright 2011 American Society of Consultant Pharmacists
Symptom Management in Breast Cancer
Symptom Comments and Recommendations
Osteoporosis • Associated with aromatase inhibitor hormonal therapy. • Obtain baseline bone mineral density (BMD). • Consider vitamin D, calcium and bisphosphonates if the BMD is low. • Counsel patient to perform weight-bearing exercise.
Congestive Heart Failure • Consequence of anthraycline chemotherapy or trastuzmab. • Obtain ejection fraction at baseline and periodically while on therapy. • Monitor for signs of congestive heart failure such as dyspnea, orthopnea, increased cough, peripheral edema
Hand Foot Syndrome • Possibly due to capecitabine. • Monitor for numbness, tingling, swelling, erythema, pain, blistering, or desquamation of palms of hands and soles of feet. • Counsel patient to contact his/her oncologist at the first sign of these symptoms. • May need dose reduction of capecitabine if side effect interferes with activities of daily living or is intolerable
Non Pharmacogic Intervention: avoid immersion in hot water, avoid activities that increase pressure in the affected areas, use topical emollients that contain urea or lanolin. Pharmacologic intervention: pyridoxine
Lymphedema • Avoid strenuous exercise. • Do not carry heavy bag on affected arm. • Avoid infection in affected arm, for example be careful shaving armpits, cutting fingernails, wear gloves when working in the garden. • Elevate the arm when possible, wear compression hosiery made to measure for lymphedema
Bony metastasis • Monthly bisphosphonates with either pamidronate or zoledronic acid has been shown to decrease the incidence of developing a skeletal related event and decreases pain score

Copyright 2011 American Society of Consultant Pharmacists
Symptom Management in Breast Cancer
Women with breast cancer experience many adverse symptoms that may be due to the cancer, surgery, hormonal therapy or chemotherapy. The most common symptoms include hot flushes, osteoporosis and vaginal changes due to hormonal therapy. Congestive heart failure and hand foot syndrome are due to chemotherapy or targeted HER2 therapy. Lymphedema is a consequence of surgical dissection of the axilliary lymph nodes and bone fractures or pain can be due to bone metastasis.
Optimal management of these symptoms can significantly improve the patient’s quality of life. Pharmacists have a role in providing both pharmacologic and non-pharmacologic recommendations in preventing or treating these symptoms.

Copyright 2011 American Society of Consultant Pharmacists
Treatment of Breast Cancer in the Elderly Patient Population
Factors Influencing Therapy Decisions in the Elderly • Age • Presence and Degree of Comorbid Conditions • Life Expectancy • Estimated benefit from treatment • Natural History of the Breast Cancer • Stage of the Breast Cancer • Lack of clinical trials data in the elderly patient population
Characteristics of Breast Cancer in the Elderly • High frequency of positive hormone receptor status • Higher percentage with lymph node negative disease compared to younger women
When treatment of breast cancer is being considered for elderly women, the patient’s anticipated life expectancy, co-morbid conditions, functional status and risk for recurrence should be determined before systemic therapy is offered.
It is observed that breast cancer in the elderly population has more favorable characteristics. This is evidenced by the cancer expressing either estrogen or progesterone receptor status, having a lower proliferative rate and no expression of the epidermal growth factor receptor or HER2 receptor. About 85% of women who are 65 or older are estrogen receptor positive and more than 63% are progesterone receptor positive. Adjuvant hormonal therapy with either tamoxifen or an aromatase inhibitor should be considered for older women with either positive estrogen or progesterone receptors.

Copyright 2011 American Society of Consultant Pharmacists
Treatment of Breast Cancer in the Elderly Patient Population
It is not recommended that chemotherapy should be added to hormonal therapy if the elderly woman is hormonal status positive and lymph node negative because it has not been shown to provide improved benefit.
Chemotherapy may be considered in an elderly woman who is hormonal status positive and lymph node positive or in hormonal status negative patients. Since chemotherapy is associated with greater toxicities and more frequent clinical visits, it should only be considered in the elderly patient that is in reasonably good health who can tolerate chemotherapy.

Copyright 2011 American Society of Consultant Pharmacists
Conclusion for Breast Cancer
• Breast cancer incidence is increasing, mortality is decreasing
• Tamoxifen can be taken to prevent breast cancer in both pre and post menopausal women
• Raloxifen can be taken to prevent breast cancer only in postmenopausal women
• An aromatase inhibitor is more effective than tamoxifen as adjuvant therapy for treating postmenopausal hormonal receptor
positive breast cancer patients
• Trastuzumab is indicated as adjuvant therapy for early stage cancer and as first line therapy for metastatic breast cancer in
women with over expression of HER2
• Lapatinib is a dual tyrosine kinase inhibitor that targets both HER1 (EGFR) and HER2 and offers additional drug options in
the treatment of breast cancer
• Surgical and radiation techniques are improving and advancing towards less aggressive procedures in the treatment of
breast cancer
In the last 20 years, the treatment of breast cancer has advanced significantly. Breast cancer mortality is decreasing in the
Western world because of advances in treatment options. Pharmacists have an opportunity to be more involved in the care
of patients with breast cancer and provide medication counseling due to the availability of oral chemotherapy agents and the
need for supportive care issues such as hot flushes, osteoporosis and side effects of chemotherapy

Copyright 2011 American Society of Consultant Pharmacists
Brain Tumors in Adults: Gliomas and Primary CNS Lymphoma
Brain and Other Nervous System Tumors Incidence • An estimated 20,070 newly diagnosed cases in 2009
• 12,010 cases in males • 10,060 cases in females • Incidence is higher in whites than in blacks
Mortality • An estimated 12,920 deaths in 2009
• 7,200 in males • 5,490 in females • Mortality is higher in males than females
It is estimated that about twenty two thousand new cases of primary tumors of the brain and other nervous systems will be diagnosed and about thirteen thousand deaths will occur in the United States in 2009. Brain tumors account for 85 to 90% of all primary central nervous system tumors. In children, it is the second most common form of cancer after leukemia. In adults, primary brain tumors commonly occur in the fifth and sixth decades of life. The incidence of primary brain tumors is higher in whites than blacks and mortality rate is higher in males than females.
Brain tumors may be classified as primary or secondary tumors. Primary brain tumors are cancers that originate in brain tissues and are named for type of cells or the location of the brain in which they begin. Secondary brain tumors, or otherwise known as metastatic brain tumors, are cancers that originated from another part of the body and have spread to one or more parts of the brain. The cells from metastatic tumors are the same as the cells from which the cancer originated originated, for example, metastatic breast or lung cancer. Secondary brain tumors occur more frequently than primary brain tumors.

Copyright 2011 American Society of Consultant Pharmacists
Brain Tumors in Adults: Astrocytoma and Primary CNS Lymphoma
World Health Organization (WHO) Grading of Brain Tumors
Grade I • The tumor is differentiated and looks
like normal cells • Grows very slowly and rarely spreads
into nearby tissues • Entire tumor may be removed by surgery
Grade II • Tumor grows slowly but may spread
into nearby tissues • May transform to higher grade tumor • Has potential for recurrence
Grade III • High growth rate and is very likely to
spread into nearby tissues • Cells are not well differentiated,
looks very different from normal cells Grade IV
• High growth rate and spreads very quickly into nearby tissues
• Cells are not differentiated • Contains areas of necrosis (dead cells) in the tumor • More difficult to cure than low grade tumors
Types of Malignant Brain Tumors in Adults
Astrocytoma (most common type of glioma)
• Arise from astrocytes (star-shaped glial cells) • Most often arise in cerebrum in adults
• Grade I or II (low grade) • Median survival is 6 to 8 years
• Grade III • High grade: anaplastic astrocytoma • Median age of diagnosis is 45 years
• Grade IV • High grade: glioblastoma multiforme or malignant astrocytic glioma • Average age of diagnosis is 55 years

Copyright 2011 American Society of Consultant Pharmacists
Brain Tumors in Adults: Astrocytoma and Primary CNS Lymphoma
Primary CNS Lymphoma (PCNSL) • A variant of extra-nodal non-Hodgkin’s Lymphoma without evidence of systemic disease • Involves the brain, leptomeninges, eyes or spinal cord • Fifty percent of all PCNSL occur in patients over 60 years of age • Twenty five percent of all PCNSL occur in patients over 70 years of age • Male predominance in AIDS-associated PCNSL (male:female ratio, 7.38:1) • Most are diffuse large B-cell lymphomas • T-cell lymphomas are rare
There are many different types of brain and central nervous system tumors. These tumors are named based on the cell type from which they are derived and the location where the tumor first formed in the brain or central nervous system.
The classification of brain tumors is based on the World Health Organization classification of nervous system tumors, which establishes a malignancy scale based on the histologic features of the tumor. The histologic grade is from a scale of one to four. The lower grade one and two tumors are slow growing and less aggressive compared to the higher grade three or four tumors, which have a high growth rate, are less differentiated and are more likely to spread into nearby tissues.
The most common primary brain tumors are gliomas which are cancers derived from glial cells. An astrocytoma is a type of glioma. A grade 3 astrocytoma is known as an anaplastic astrocytoma and a grade 4 astrocytoma is known as a glioblastoma multiforme or malignant astrocytic glioma. These two subtypes of astrocytomas account for approximately 38% of all primary brain tumors.
Primary CNS lymphoma is defined as a lymphoma that is limited to the brain and central nervous system without systemic disease. It does not include systemic lymphoma that has spread to the central nervous system. It accounts for 2.7% of all malignant cancers of the CNS. The median age of occurrence for primary CNS lymphoma is older for immunocompetent patients at 53 to 57 years of age. For immunocompomised patients the median age of occurrence is much younger at 32 to 35 years of age. The sex distribution of the disease is equal in immunocompetent patients but in immunocompromised patients there is a clear male predominance.

Copyright 2011 American Society of Consultant Pharmacists
Brain Tumors in Adults: Astrocytoma and Primary CNS Lymphoma
Risk Factors for Developing Astrocytoma • Age • Family History • Radiation • Exposure to chemicals
• Formaldehyde (pathologists and embalmers) • Vinyl chloride (workers who make plastics) • Acrylonitrile (textiles and plastics)
Risk Factors for Developing Primary CNS Lymphoma • Immunodeficiency • AIDS (acquired immunodeficiency syndrome) • Immunosuppression from transplant procedures • Congenital immune deficiency • Ataxia telangiectasia • Wiskott-Aldrich syndrome • Severe combined immunodeficiency • Autoimmune conditions
• Rheumatoid arthritis • Systemic lupus erythematosis • Myesthenia gravis • Sjogren’s syndrome • Sarcoidosis • Vasculitis
• Epstein-Barr virus infection
There are few definitive observations of environmental or occupational causes of brain tumors, most causes of adult brain tumors is unknown. In general, brain tumors are more common in males than females and more common among whites than among people of other races. Most brain tumors are detected in people over 70 years of age.
People with a family history of brain tumors are more likely to develop the cancer. Exposure to radiation and certain chemicals such as vinyl chloride or formaldehyde may also increase the risk of developing brain cancers.
For patients diagnosed with primary CNS lymphoma, risk factors include previous infections with the Epstein-Barr virus, having a diagnosis of AIDS or exposure to immunosuppressant drugs after a solid organ transplant. Having a congenital deficiency or certain types of autoimmune diseases may also increase the risk of developing primary CNS lymphoma.
Copyright 2011 American Society of Consultant Pharmacists
Clinical Signs and Symptoms of Brain Tumors
• Headaches (more severe in the morning) • Drowsiness during the day and extended night sleep • Nausea or vomiting • Speech, vision or hearing abnormalities • Problems balancing or walking • Cognitive dysfunction
• Difficulty concentrating • Memory deficits
• Changes in mood or personality • Partial or generalized seizures • Elevated intracranial pressure • Numbness or tingling in the arms or legs
Diagnosis of Brain Tumors • Physical exam • Neurologic exam • Lumbar puncture – CSF examination • MRI • CT scan • Biopsy sample
The signs and symptoms from brain tumors depend on the location, size and the type of the brain tumor. Headaches are common and occur in approximately 35% of patients. Headaches associated with nausea, vomiting or focal neurologic deficits in a patient without a previous history of headaches are characteristic symptoms. In a patient with a history of headaches, there is a change in the characteristic, frequency and intensity of the headaches. In patients with gliomas, seizures occur in one-third of patients and altered mental status develops in 15 to 20% of patients. The type of localized neurologic deficit depends on the location of the tumor. Motor dysfunction and cognitive deficits include numbness or weakness of an arm or leg, loss of vision, difficulties with speech, and impaired memory and judgment.
In primary CNS lymphoma, focal neurologic deficits such as hemiparesis or dysphasia are the most common presentation in more than 50% of patients. Thirty three percent of patients experience headaches, nausea and vomiting due to increased intracranial pressure and ocular symptoms such as blurred vision or floaters develop in 50% of patients. Seizure is less common and develops in about 10% of patients.
The diagnostic work up of a primary brain tumor includes a lumbar puncture to analyze the cerebral spinal fluid. An MRI or CT scan is performed to find the location of the mass, measure its size, and to assess the degree of edema. The diagnosis is confirmed with a biopsy of the tumor.

Copyright 2011 American Society of Consultant Pharmacists
Prognostic Factors
Astrocytomas • Favorable Prognostic Factors
• The grade of the tumor • Age less than 50 years • Good performance status • Intact neurological function • Resectability of the tumor
CNS Lymphoma • Favorable Prognostic Factors
• Age less than 60 years • Single, well-circumscribed tumor • Absence of immunodeficiency • Absence of meningeal or peri-ventricular tumor • Diffuse mixed and small noncleaved cell lymphoma
In determining prognosis for patients diagnosed with gliomas, good prognostic factors include younger age, good performance status, low grade tumors, intact neurological function and complete resection of the tumor. Glioblastoma, which is a grade 4 aggressive astrocytoma, carries the worst prognosis of all the different types of gliomas.
Good prognostic factors for primary CNS lymphoma include single, solitary tumors, age less than 60 years and absence of immunodeficiency. The subtype of CNS lymphoma that does well is diffuse mixed and small noncleaved cell lymphomas. Patients with large immunoblastic and large noncleaved or cleaved lymphomas have worse prognosis.

Copyright 2011 American Society of Consultant Pharmacists
Treatment Options
Astrocytoma
• Low-Grade (Grade I and II) • Surgery
• Patients with large lesions and mass effect • Radiation
• Adjuvant therapy after surgery • Chemotherapy
• Role of adjuvant chemotherapy is under investigation • Temozolomide is an option
• High Grade (Grade III and IV; anaplastic astrocytoma and glioblastoma multiforme or malignant astrocytic glioma)
• Surgery • Maximal debulking while minimizing neurologic deficits
• Radiation • Adjuvant therapy after surgery • Prolongs survival compared to supportive care alone after surgery
• Chemotherapy • Temozolomide
• Oral alkylating agent • Good CNS penetration • Good option for patients older than 70 years who may not tolerate radiation therapy
• Carmustine (BCNU) • Biodegradable polymer (Gliadel® wafer)
• PCV (procarbazine, CCNU (lomustine), vincristine)

Copyright 2011 American Society of Consultant Pharmacists
Treatment Options
Treatment options for astrocytomas include surgery, radiation and chemotherapy. Surgical resection of the brain tumor is recommended for both low grade and high grade astrocytomas. The goal of therapy is to completely remove as much of the tumor as possible while striving to preserve neurologic function at the same time.
Radiation has a major role in the treatment of astrocytomas. In low-grade tumors, radiation has been shown to extend the time to recurrence but it has not been shown to improve overall survival. On the other hand, in anaplastic astrocytoma, adjuvant radiation therapy after surgery has been shown to prolong survival. In patients with glioblastomas, the addition of radiation to surgery increases survival from 3 to 4 months to 7 to 12 months.
The role of chemotherapy for low-grade astrocytomas and anaplastic astrocytoma is still under investigation. Currently, temozolomide is an option for low-grade astrocytomas over the combination PCV chemotherapy regimen because it is associated with less toxicity.
In patients with anaplastic astrocytomas there is no standard treatment after surgery. The role of chemotherapy after surgery is controversial because study results in this patient population are conflicting with some studies demonstrating survival benefit and others do not. Radiation with concomitant and adjuvant temozolomide or adjuvant temozolomide alone are acceptable options in patients with anaplastic astrocytoma.
For glioblastomas, adjuvant temozolomide with radiation has convincingly shown benefit with median survival increased by 2 and a half months and 2-year survival by 16.1%. Temozolomide is considered to be the standard of care for glioblastoma multiforme based upon this data. Temozolomide is an oral alkylating agent that has good CNS penetration. It is a viable alternative for patients who are older than 70 years of age in whom radiation has shown little survival benefit with much toxicity.
Another chemotherapy approach for glioblastoma involves the implantation of biodegradable polymers containing carmustine, known as Gliadel® wafers, into the tumor bed after surgical resection with radiation therapy. The carmustine is released slowly over several weeks to kill any residual tumor cells.
The combination PCV chemotherapy regimen is an option for patients with recurrent anaplastic astrocytoma or glioblastoma multiforme.

Copyright 2011 American Society of Consultant Pharmacists
Treatment Options
Primary CNS Lymphoma • High-dose methotrexate prior to radiation therapy
• Dose is > 3.5 gm/m2 • Median survival to 23-42 months • Currently is the standard therapy
• Whole Brain Irradiation • Steroids
• 40% response rate • Transient effect on the tumor and recurrence commonly occurs • Avoid administration prior to biopsy due to difficulty in histology interpretation of the tumor after the steroid
The main treatment for primary CNS lymphoma involves the combination of high-dose methotrexate chemotherapy followed by radiotherapy. Chemotherapy has been shown to prolong time to tumor progression and prolong median survival compared to radiation alone. Whole brain radiation may be offered after systemic chemotherapy. When CNS lymphoma is being considered in the differential diagnosis of a brain tumor, administration of a corticosteroid should be avoided because it may eradicate the lymphoma lesion and makes it difficult to diagnose the disease.

Copyright 2011 American Society of Consultant Pharmacists
Symptom Management in Brain Tumors
Symptom Comments and Recommendations
Seizures Initiate antiepileptic drugs in patients who presents with seizures.
Avoid seizures medications that induce CYP450 enzymes if possible to prevent drug interaction with chemotherapy.
No evidence to recommend initiation of prophylactic seizure medication in gliomas if a patient has not had a seizure
Peri-tumor edema Initiate corticosteroids.
Monitor for steroid side effects.
Cushing’s syndrome and steroid induced myopathy may occur if a patient is on prolonged high doses of corticosteroid therapy.
Consider prophylactic antibiotics for pneumocystis jiroveci.
Prevent osteoporosis and compression fracture from long term steroid therapy with vitamin D, calcium supplements and bisphosphonates.
Furosemide and mannitol may also be used to treat edema

Copyright 2011 American Society of Consultant Pharmacists
Symptom Management in Brain Tumors
Symptom Comments and Recommendations
Venous thromboembolism
Venous thromboembolism may occur in patients with malignant gliomas in the leg and pelvic veins. The cumulative incidence is 20 to 30%.
Anticoagulation therapy with low molecular weight heparin is indicated unless a patient has intracerebral hemorrhage or other contraindications.
Fatigue May initiate modafinil or methylphenidate
Methotrexate Side Effects
Renal toxicity – maintain good hydration, alkalinize the urine to maintain pH above 7.
Discontinue NSAIDS, avoid ascorbic acid or drinking orange juice or grapefruit juice which may acidify the urine.
Myelosuppression and mucositis - administer leucovorin rescue Nausea and vomiting - provide anti-emetics
Temozolomide Side Effects
Myelosuppression, monitor for neutropenic fever.
Initiate Pneumocystis carinii pneumonia prophylaxis for patients receiving therapy for glioblastoma multiforme.
Provide antiemetics if needed.

Copyright 2011 American Society of Consultant Pharmacists
Symptom Management in Brain Tumors
Supportive care in patients with brain tumors is indicated to prevent or control problems such as the side effects of chemotherapy or symptoms from the tumors. Seizure is a common symptom for patients with high-grade gliomas such anaplastic astrocytoma or glioblastoma multiforme. At this time, there is no evidence to recommend starting prophylactic anti-seizure medications. Anti-seizure medication is indicated only once a patient has experienced a seizure. Edema of the brain may occur in patients with brain tumor due to mass effect and therapy with a corticosteroid, mannitol or furosemide is necessary to relieve the swelling of the brain.
Twenty to thirty percent of patients with malignant gliomas are at risk for developing venous thromboembolism. Fortunately, the risk of intra-tumoral hemorrhage associated with anticoagulation therapy in glioma patients with venous thromboembolism is low. Therefore, anticoagulation therapy with a low molecular weight heparin is appropriate for a patient with venous thromboembolism unless they have contraindications such existing intracerebral hemorrhage. Administration of CNS stimulants such modafinil or methylphenidate may help fatigue in some patients.
Lastly, the side effects of specific chemotherapy agents should be monitored and appropriate measures should be taken to avoid toxicity when available.
In summary, primary brain tumors account for 2% of all cancer malignancies. Treatment options for brain tumors include surgery, radiation therapy, chemotherapy or a combination of these modalities. The specific type of therapy for each type of tumor varies due to different sensitivities and response rate of the tumors. The role of a pharmacist in the treatment of these tumors is to be knowledgeable with the management of side effects and symptoms related to either drug therapy or the disease state.

Copyright 2011 American Society of Consultant Pharmacists
References
For additional information, see:
Cancer Statistics Jemal A SR, Siegel R. et al. Cancer Statistics, 2009. CA Cancer J Clin 2009, July/August
Lung Cancer
Gridelli C, Rossi A, Maione P. Challenges in treating older non-small lung cancer patients. Ann of Oncol 2008;19 (Suppl 7):vii100-vii113
Gridelli C, Langer C, Maione P, et al. Lung cancer in the elderly. J Clin Oncol 2007;25:1898-1907
Herbst RS, Heymach JV, Lippman SM. Lung Cancer. NEJM 2008; 359: 1367-80
Herbst RS, Sandler RA. Bevacizumab and erlotinib: A promising new approach to the treatment of NSCLC. Oncologist 2008;13:1166-1176
Molina JR, Yang P, Cassivi SD, et al. Non-small cell lung cancer: Epidemiology, Risk Factors, Treatment, and Survivorship. Mayo Clin Proc 2008;83(5):584-594
NCCN. Lung Cancer. Practice Guidelines in Oncology. V.2.2009. Accessed at www.NCCN.org
Sher T, Dy GK, Adjei AA. Small cell lung cancer. Mayo Clin Proc 2008;83(3):355-367

Copyright 2011 American Society of Consultant Pharmacists
References
Smith RA, Cokkinides V, Brawley OW. Cancer Screening in the United States 2009: A review of current American Cancer Society guidelines and issues in cancer screening. CA Cancer J Clin 2009,59:27-41
Walker S. Updates in non-small cell lung cancer. Clin J Onco Nurs 2008;12(4):587-596
Breast Cancer Balducci L. Treating elderly patients with hormone sensitive breast cancer: What do the data show? Cancer Treatment Reviews 2009;35:47-56
Harmer V. Breast cancer-related lymphedema: risk factors and treatment. Br J of Nurs 2009;18(3):166-172
Loprinzi CL, Wolf SL, Barton DL, Laack NN. Symptom management in premenopausal patients with breast cancer. Lancet Oncol 2008;9:993-1001
NCCN. Breast Cancer. Practice Guidelines in Oncology. V.1.2009. Accessed at www.NCCN.org
Muss HB. Adjuvant treatment of elderly breast cancer patients. The Breast 2007;16:S159-165
Nielsen DL, Andersson M, Kamby C. HER2 targeted therapy in breast cancer. Monoclonal antibodies and tyrosine kinase inhibitors. Cancer Treatment Reviews 2009;35:121-136
Smith RA, Cokkinides V, Brawley OW. Cancer screening in the United States 2009: A review of current American Cancer Society guidelines and issues in cancer screening. CA Cancer J Clin 2009,59:27-41
Thomsen A, Kolesar JM. Chemoprevention of breast cancer. Am J Health-System Pharm 2008;65:2221-8

Copyright 2011 American Society of Consultant Pharmacists
References
Brain Tumors Bhagavathi S, Wilson JD. Primary Central Nervous Lymphoma. Arch Pathol Lab Med 2008;132:1830-1834
Buckner JC, Brown PD, O’neill BP, et al. Central Nervous System Tumors. Mayo Clin Proc 2007;82(10):1271-1286
NCCN. Central Nervous System Cancers: Practice Guidelines in Oncology. V.1.2009. Accessed at www.NCCN.org
Wen PY, Kesari S. Malignant Gliomas in Adults. NEJM 2008;359:492-507
Web Resources:
http://www.nci.nih.gov/
http://www.NCCN.org
http://www.cancer.org

Copyright 2011 American Society of Consultant Pharmacists
Colorectal, Pancreatic, and Prostate Cancer
Learning Objective:
By the end of this Review Concept you should be able to:
• Cite the epidemiology for colorectal cancer.
• Identify the risk factors for colorectal cancer.
• Describe the recommended screening procedures for colorectal cancer.
• List the most common symptoms associated with colorectal cancer and describe how they may differ depending on the location of the primary tumor.
• Describe the role of surgery and chemotherapy in managing colorectal cancer.
• Describe the epidemiology and manifestations of prostate cancer.
• Describe options for the early and late treatment of prostate cancer.
• Describe the epidemiology for pancreatic cancer.
• Describe the signs and symptoms and complications associated with pancreatic cancer.
• Describe the treatment options for pancreatic cancer.

Copyright 2011 American Society of Consultant Pharmacists
Colorectal Cancer
Epidemiology
• Third most frequently diagnosed cancer in men and women
• Estimated 146,940 new cases of colorectal cancer in 2004
• 106,370 colon cancer cases
• 40,570 rectal cancer cases
• Estimated 56,730 colorectal deaths in 2004
• Mortality decreased over past 30 years
Cancers of the rectum and colon account for eleven percent of all cancers and ten percent of all cancer related deaths in men and women. It is the third leading cause of cancer-related deaths after lung and breast cancer. It is estimated that in 2004 there will be approximately 147,000 cases of newly diagnosed colorectal cancer, about 106,000 of which will be colon cancer and 41,000 of which will be rectal cancer.
The good news is that the mortality rate for colorectal cancer has been decreasing during the past 30 years due in part to screening recommendations and better treatment modalities.

Copyright 2011 American Society of Consultant Pharmacists
Risk Factors for Colorectal Cancer
Age • Increases with increasing age • Median age of diagnosis 69 years • 90% > 50 years at diagnosis
Hereditary • 2 – 4 x increased risk with 1st degree
relative with colorectal cancer • Familial Adenomatous Polyposis (FAP) • Hereditary Non-Polyposis
Colorectal Cancer (HNPCC)
Inflammatory Bowel Disease (IBD) • Chronic Ulcerative Colitis • Crohn’s Disease
Previous Colorectal Cancer
Previous Pelvic Irradiation
Diet • High fat • Low fiber
Lifestyle
• Alcohol intake • Physical inactivity • Obesity • Tobacco use • Occupational exposure • Asbestos • Pesticides • Herbicides • Metal workers
Genetic Mutations
• K-ras mutations • Deleted Colon Cancer Gene (DCC gene) • Loss of chromosome 17p • Mutation mismatch repair genes • Inactivation of tumor suppressor genes

Copyright 2011 American Society of Consultant Pharmacists
Risk Factors for Colorectal Cancer
The incidence of colorectal cancer rises throughout life, almost doubling with each decade over age fifty. More than two-thirds of colorectal cancer cases occur in people sixty-five and older and more than 90% occurs in people over fifty years of age.
A family history of colorectal cancer or a genetic susceptibility to colorectal cancer due to syndromes such as hereditary nonpolyposis colon cancer (HNPCC) or familial adenomatous polyposis (FAP) predisposes a person to a greater risk of developing colorectal cancer. For a person with FAP, the lifetime risk of developing cancer approaches 100% by age 50 years and for the person with HNPCC the lifetime risk of developing colorectal cancer approaches 80%. Vigilant surveillance of these conditions has been shown to reduce the risk of developing colorectal cancer.
Patients who have symptoms of inflammatory bowel disease for more than 8 years or symptoms of left sided colitis for more than 15 years are at increased risk of developing colorectal cancer. Patients with a previous history of colorectal cancer or pelvic irradiation are also at increased risk.
Lifestyle factors that may influence the risk of developing colorectal cancer include having a diet that is high in fat and low in fiber. Alcohol consumption, tobacco use, physical inactivity, obesity and occupational exposure are also associated with the increased risk of developing colorectal cancer.
All individuals should be encouraged to decrease their fat intake and increase their fiber intake along with initiating healthy lifestyle modifications such as limiting alcohol and tobacco use and participation in more physical activities.
Genetic changes that affect the development of colorectal cancer include mutation of the K-ras proto-oncogene, deletion of the colon cancer gene, the loss of chromosome 17 p or mutation in genes that repair mismatch DNAs.

Copyright 2011 American Society of Consultant Pharmacists
Screening for Colorectal Cancer
• Digital Rectal Examination (DRE) • Fecal Occult Blood Test (FOBT) • Flexible Sigmoidoscopy • Colonoscopy • Barium enema
American Cancer Society Colorectal Cancer Screening Recommendations Average Risk Patient Starting at Age 50
DRE: Every Year FOBT: Every Year
Sigmoidoscopy: Every 5 Years Colonoscopy: Every 10 Years
Barium Enema: Every 5-10 years
Individuals at High Risk of Developing Colorectal Cancer
HNPCC Colonoscopy every 1 – 2 years Star:ng at 20 – 30 years
Colonoscopy every year Star:ng at 40 years FAP Sigmoidoscopy every year Star:ng at puberty
IBD Colonoscopy every 1 – 2 years 8 years amer onset of pancoli:s or 15 years amer onset of lem-‐sided pancoli:s
Colo-‐rectal Cancer Colonoscopy every 3 – 5 years One year amer treatment

Copyright 2011 American Society of Consultant Pharmacists
Screening for Colorectal Cancer
Patients with early tumors still confined to the mucosal layers have a much higher survival rate than patients with more advanced disease because their tumors can be completely surgically resected. Thus, screening recommendations for colorectal cancer are aimed at detecting the cancer at an earlier stage in order to optimize treatment that will cure the disease and decrease mortality.
Routine screening for the average risk individual starts at age fifty and includes annual stool testing for occult blood and digital rectal examination. A sigmoidoscopy or barium enema should be performed every 5 years, or a colonoscopy should be performed every 10 years.
Screening of high-risk patients is more frequent and begins at an earlier age. The table provides colorectal screening recommendations for the various high risk patients.

Copyright 2011 American Society of Consultant Pharmacists
Clinical Manifestations of Colorectal Cancer
• Rectal Bleeding: bright red blood with stool • Abdominal Pain • Changes in Bowel Habits • Abdominal Distention • Nausea, vomiting • Early stage tumors are often asymptomatic • Advanced or Metastatic Disease
• Hepatomegaly, jaundice • Weight loss • Leg edema from lymph node metastasis • Lung and bone metastasis
Tumors of the Transverse and Descending Colon:
Left-Sided Lesions
• Obstructive symptoms • Cramping, constipation • Diarrhea • Bowel changes • Bleeding
Tumors of the Cecum and Ascending Colon:
Right-Sided Lesions
No significant changes in bowel habits Watery diarrhea Occasional abdominal pain

Copyright 2011 American Society of Consultant Pharmacists
Clinical Manifestations of Colorectal Cancer
Tumors of the Rectosigmoid
• Hematochezia • Tenesmus • Painful defecation • Narrowing of stool caliber
The majority of colorectal cancer occurs in the distal portion ofthe colon and the rectum. Sixty percent of cancers are located in the left side of the colon.
Generally the disease is asymptomatic until it either becomes quite large or penetrates through the bowel mucosa. Two thirds of patients with colorectal cancer do not seek medical attention until the disease is more advanced when symptoms are present.
Symptoms of more advanced colorectal cancer include bleeding through the rectum, which is visible in the stool; changes in bowel habits, including constipation and occasional diarrhea. Nausea, vomiting, weight loss and pain may indicate bowel obstruction or perforation.
Left-sided colonic lesions tend to cause more obstructive symptoms, while right-sided lesions can cause abdominal discomfort and slow bleeding that later shows up as anemia.
The most common site of metastasis for colorectal cancer is the liver or the lungs. Hepatomegaly, jaundice, pruritis are associated with liver metastasis.

Copyright 2011 American Society of Consultant Pharmacists
Workup of Colorectal Cancer Diagnosis
• Past medical history and family history • Physical exam • Colonoscopy, sigmoidoscopy, or barium enema • Baseline laboratory tests (CBC, LFTs, PT, PTT, serum CEA) • Chest x-ray • CT-scan or ultrasonography • Intraluminal and hepatic MRI
Staging of Colorectal Cancer American Joint Commission on Cancer TNM Staging System and the Modified Astler-Collier (Duke’s) Staging System:
Colorectal Cancer Staging System
MAC Duke’s TNM 5-year survival 0
A / B1 A Stage I 90%
B2 B IIA 60-80% B3 B IIB
C1 C IIA 59.8%
C2/C2/C3 C IIB 42%
D - IV 8%

Copyright 2011 American Society of Consultant Pharmacists
Workup of Colorectal Cancer Diagnosis
In addition to a physical examination, the diagnosis of colorectal cancer relies on colonoscopy with a biopsy of the tumor, or excision of suspicious lesions. Additional tests are performed to determine the extent of the disease such as chest x-ray to rule out lung metastasis or abdominal CT scan to rule out liver metastasis. Baseline laboratory tests such as a CBC, serum chemistries, PT and PTT should also be performed.
Colorectal cancer staging is based upon the American Joint Commission on Cancer, the Modified Astler Collier System or the Dukes’ Staging System. The table provides a comparison of how each staging system correlates with each other.
Stage I and II disease are usually limited to the intestinal wall. Stage I penetrates only the mucosa and submucosa layers. Stage II penetrates through the muscle tissue layers and serosa.Stage III disease involves the surrounding lymph nodes, and stage IV involves distant metastasis, which commonly occurs in the liver and lungs.
Individuals with higher stage of the disease have poorer 5 years survival rate. Patients with stage I disease have a 90% 5 years survival rate. The lower 5 year survival rate of 60-80% in stage II disease is due to greater penetration of the tumor into the intestinal wall. The 5 year survival rate for stage III ranges from 27% to 60% depending on the number of positive lymph nodes found during lymph node dissection. Lastly, the 5 year survival rate for metastatic prostate cancer is about 8% reflecting the extensiveness of the disease and difficulty in treating it.

Copyright 2011 American Society of Consultant Pharmacists
General Principles of Therapy for Colorectal Cancer
Surgery • Cure for localized disease • Mainstay of therapy for stage I-III • Palliation for stage IV
Radiation • Given as adjuvant therapy and palliation for rectal cancer • Only given as palliation for colon cancer
Chemotherapy • Adjuvant therapy for advanced disease
Immunotherapy • Bevacizumab
• Monoclonal antibody targeting the vascular endothelial growth factor • Cetuximab
• Monoclonal antibody targeted at the epidermal growth factor receptor • Second line therapy for patients who are refractory to therapy with irinotecan based or FOLFOX regimen
Treatment of Stage I-III Colon Cancer
Stage I – II • Surgery and lymphadenopathy
Stage III • Surgery • Adjuvant chemotherapy

Copyright 2011 American Society of Consultant Pharmacists
General Principles of Therapy for Colorectal Cancer
• Leucovorin and Fluorouracil • Fluorouracil(5-FU)/leucovorin/Oxaliplatin (FOLFOX)
• Side effects with 5-FU/leucovorin: • diarrhea, stomatitis, nausea, vomiting • palmar-plantar erythrodysesthesia
• Side effects with the FOLFOX regimen: • above side effects with 5-FU/ leucovorin, PLUS
• acute cold induced neuropathy • delayed sensory neuropathy
Treatment of Stage I-III Rectal Cancer
Stage I • Surgery
Stage II-III • Surgery • Adjuvant radiation with 5-FU • Adjuvant chemotherapy
• Leucovorin and Fluorouracil • Fluorouracil(5-FU)/leucovorin/Oxaliplatin (FOLFOX)
Copyright 2011 American Society of Consultant Pharmacists
General Principles of Therapy for Colorectal Cancer
Excision surgery is the only potentially curative treatment for colorectal cancer.If they are small enough, any polyps found during colonoscopy can be removed with electrocautery. Larger lesions should be biopsied first to confirm malignancy, and then surgically removed. Surgery is the mainstay of therapy for Stage I to III colorectal cancer.
Radiation therapy may be administered as adjuvant therapy for patients with rectal cancer to reduce the risk of tumor recurrence. Radiation may also be administered for symptom palliation in both colon and rectal cancer.
Adjuvant chemotherapy administered in advanced disease has been shown to increase overall survival.
This next section will focus on treatment options for the different stages of colon and rectal cancer.
For patients diagnosed with localized stage I to stage III colon cancer, surgery along with lymphadenectomy is the primary treatment modality.Adjuvant chemotherapy may be considered for high risk stage II patients in the setting of clinical trials.
In stage III colon cancer, adjuvant chemotherapy clearly shows benefit in overall survival and acceptable chemotherapy regimens include 5–FU and leucovorin or the FOLFOX regimen consisting of 5-FU, leucovorin, and oxaliplatin. Nausea, vomiting, diarrhea, and palmar plantar erythrodysesthesia are common with 5-FU and leucovorin. Patients receiving oxaliplatin may experience dysesthesia in the extremities and perioral area when exposed to cold immediately after treatment.
Therefore, prior to treatment patients should be warned against drinking ice cold water and patients should avoid breathing cold air post treatment if the weather is cold.
Treatment of stage I to III rectal cancer also involves surgery. Patients with Stage II or III disease should also receive adjuvant radiation therapy with 5-FU as a radiosensitizer to minimize the risk of pelvic recurrence. Adjuvant chemotherapy with a 5-FU based regimen or FOLFOX is also recommended to reduce the risk of local recurrence and improve survival.

Copyright 2011 American Society of Consultant Pharmacists
Treatment of Stage IV Colorectal Cancer
Combination Chemotherapy Regimen
• First Line Intensive Therapy • Infusional 5-FU/ leucovorin/oxaliplatin (FOLFOX) • Infusional 5-FU/leucovorin/irinotecan (FOLFIRI ) • Bevacizumab and 5-FU containing regimen
• First Line for Patients who can not tolerate intensive therapy • Capecitabine • Bolus,infusional, or protracted 5-FU/leucovorin
• Second Line Therapy • Infusional 5-FU/leucovorin/Irinotecan (FOLFIRI ) • FOLFOX • Cetuximab and irinotecan • Irinotecan
• Radiation
• Surgery
The goals of therapy for stage IV metastatic colorectal cancer are to extend survival and improve symptoms.
The primary treatment modality for stage IV disease is chemotherapy. There are many chemotherapy regimen options available and the choice of which regimen to administer is based upon the toxicity profile of the regimen and the type and timing of prior chemotherapy the patient has received.

Copyright 2011 American Society of Consultant Pharmacists
Treatment of Stage IV Colorectal Cancer
The goals of therapy for stage IV metastatic colorectal cancer are to extend survival and improve symptoms.
The primary treatment modality for stage IV disease is chemotherapy. There are many chemotherapy regimen options available and the choice of which regimen to administer is based upon the toxicity profile of the regimen and the type and timing of prior chemotherapy the patient has received.
In general, 1st-line chemotherapy may include the FOLFOX or the FOLFIRI regimen or the use of the monoclonal antibody bevacizumab and a 5-FU containing regimen.
For patients who may not be able to tolerate intensive first line therapy, alternative chemotherapy agents such as capecitabine or 5-FU and leucovorin may be considered.
Post Treatment Surveillance for Colorectal Cancer
History and Physical ExaminaAon Every 3 months for the first 2 years Every 6 months for the next 5 years
CEA Marker Baseline
Every 3 months for 2 years Every 6 months for next 2 – 5 years
Colonoscopy Within 1 year of resec:on Annually if polyps are noted
Every 3 years if no polyps noted

Copyright 2011 American Society of Consultant Pharmacists
Treatment of Stage IV Colorectal Cancer
If the patient fails 1st-line therapy, second line therapy may include the alternative regimen that was not chosen.
Radiation therapy in metastatic colorectal cancer is used to manage symptoms associated with localized disease.
Surgery is considered for resectable liver or lung metastasis or to manage obstruction or perforation associated with the primary tumor.
Patients with a history of colorectal cancer are at increased risk of developing second cancers; therefore, surveillance post-treatment is essential to detect the cancer early if it recurs.
After a patient has received and completed treatment for colorectal cancer, it is recommended that the patient should have a history and physical exam every 3 months for the first 2 years, then increase to every 6 months for the next 5 years. A baseline CEA level should also be obtained, followed by a level every 3 months for the next 2 years, then every 6 months for the next 2 to 5 years. A colonoscopy should also be obtained within 1 year of the surgical resection the every 3 years thereafter if no polyps are noted or annually of polyps are noted.

Copyright 2011 American Society of Consultant Pharmacists
Prostate Cancer
Epidemiology • Most common cancer in males • Estimated 230,110cases in 2004 • Second most common cause of cancer related death in men • Estimated 29,900 deaths in 2004
Risk Factors • Age • Race • Family history • Diet • Occupation
Prostate Cancer Screening
Digital Rectal Exam (DRE) • Lumps, hardness, inability to move the prostate indicate further need for evaluation
Prostate Specific Antigen • Screening, determine prognosis, detect recurrence, monitor response to therapy
Factors that increase PSA • DRE • Biopsy • Benign Prostatic Hypertrophy • Prostatitis

Copyright 2011 American Society of Consultant Pharmacists
Prostate Cancer
Factors that decrease PSA • Finasteride • Saw palmetto • Surgery • Radiation • Hormonal Therapy
Following lung cancer, prostate cancer is the 2nd-leading cause of cancer death in men. It is the second most common malignancy in American men. It is estimated that 230,110 new cases of prostate cancer will be diagnosed in 2004 and an estimated 29,900 men will die ofthis disease.
The probability of developing prostate cancer increases with age. In men less than 65 years of age, about 1 in 10 will be diagnosed with prostate cancer. Between the age of 65 years to 74 years, 2 in 10 men will be diagnosed with prostate cancer. The incidence is highest in men over 75 years of age where 7 in 10 men will be diagnosed with prostate cancer.
Prostate cancer affect African Americans fifty percent more often than white Americans. The risk is lowest for Asians. Individuals with a family history of prostate cancer have a higher risk of developing prostate cancer, especially at a younger age. The correlation between prostate cancer and diet is less clear; however, it is thought that a high fat diet may increase the risk of prostate cancer. Occupational exposure to industrial chemicals may also predispose a man to greater risk of prostate cancer.
Prostate cancer screening involves 3 modalities, a digital rectal exam, a serum prostate specific antigen level, and a transrectal ultrasound. A digital rectal exam allows the physician to feel for lumps or hardness of the prostate. If these signs are present, further evaluation tests are needed. The prostate specific antigen is a glycoprotein secreted by epithelial cells of the prostate, the purpose of which is to liquify seminal secretions. The PSA is specific for prostate abnormalities but not for prostate cancer. The PSA may be used to screen for possible prostate cancer, to predict prognosis, to detect recurrence after therapy, and to monitor a patient’s response to therapy.

Copyright 2011 American Society of Consultant Pharmacists
Prostate Cancer
Besidesprostate cancer, ejaculation and prostate manipulation may increase the PSA level. Therefore this test should be performed 48 hours after these manipulations.
The 5-alpha reductase inhibitor, finasteride, and saw palmetto have been shown to decrease PSA levels; therefore, a thorough patient medication history should be obtained prior to obtaining PSA levels.

Copyright 2011 American Society of Consultant Pharmacists
Colorectal Cancer Screening: PSA
PSA velocity • Measures the change of the PSA values over time • A higher doubling time of the PSA value correlates with a high PSA velocity and a higher risk of having prostate cancer
PSA density • Used to differentiate high PSA levels in men with a large prostate with prostate cancer • PSA value divided by the prostate volume as measured by a transrectal ultrasound
Interpretation of PSA Values
0-4 ng/ml Normal, age non-specific
4-10 ng/ml Borderline
> 10 ng/ml Suspicious for malignancy
Age Specific Reference Ranges
Age Normal PSA
40-49 years 0-2.5 ng/ml
50-59 years 0-3.5 ng/ml
60-69 years 0-4.5 ng/ml
70-79 years 0-6.5 ng/ml

Copyright 2011 American Society of Consultant Pharmacists
Colorectal Cancer Screening: PSA
Screening Recommendations
DR Eand PSA • Annually for all men > 50 years • Annually starting at 40 years for men with high risk
Transrectal Ultrasound • Recommended when DRE and PSA are abnormal
Signs and Symptoms of Prostate Cancer • Poor stream • Hesitancy • Sensation of incomplete emptying • Frequency • Urgency • Urge incontinence • Hematuria • Dysuria • Pain (spine, hips, ribs) • Impotence • Incontinence • Swollen lymph nodes
The cutoff value for normal PSA levels is different for older and younger men. The value is lower in younger men and higher in older men. In order to attain more specificity of the PSA level for cancer detection, it has been shown that the rate of change of the PSA over time, known as the PSA velocity, provides useful information and increases the sensitivity of prostate cancer diagnosis. The PSA density is a ratio of the PSA level divided by the volume of the prostate as measured by a transrectal ultrasound. The purpose of this test is to distinguish men with high PSA levels due to a large prostate without prostate cancer.
Prostate cancer screening recommendations starts at age 50 with an annual digital rectal examination and PSA level. For men who are at high risk of developing prostate cancer, the recommendation is to start screening at age 40.
If the DRE or PSA level is abnormal, then follow up with a transrectal ultrasound is recommended.
Routine screening is not recommended for men with < than 10 years of life expectancy.

Copyright 2011 American Society of Consultant Pharmacists
Colorectal Cancer Screening: PSA
Ninety-five percent of prostate cancers begin as an adenocarcinoma, usually in the peripheral region of the prostate. It may invade the periurethral tissue at the site of benign hyperplastic hypertrophy, causing urethral obstruction. It may also cause urethral obstruction by direct extension into the bladder or by spreading into the seminal vesicles. As the disease metastasizes, pelvic lymph nodes and bones of the pelvic and lumbar spine may become involved. The natural progression of prostate cancer is somewhat unpredictable, with some patients succumbing to a fulminating and rapidly metastasizing course, and others doing well without treatment for years.
Signs and symptoms of prostate cancer are generally absent in the early stage of the cancer. As the disease spreads into the urethra, patients may experience symptoms similar to those of benign prostatic hyperplasia such as urinary retention and distended bladder. If the tumor has invaded the ureters, patients may present with uremia. These genitourinary problems may be accompanied by lymphadenopathy. Skeletal pain and pathological fractures are often the initial symptoms of advanced, metastatic disease.

Copyright 2011 American Society of Consultant Pharmacists
Workup of Prostate Cancer Diagnosis
• Physical Examination • PSA measurement • Transrectal ultrasound • Transrectal needle biopsy of prostate • Gleason scoring of tumor • Bone Scan • Pelvic CT Scan or MRI Scan • CBC, Serum Chemistries
Staging of Prostate Cancer
Gleason Grading of Prostate Cancer
• Grades the tumor based upon the level of differentiation of the tumor cells • A score from 1 – 5 is assigned to 2 different samples from the prostate.Then the scores are summed to yield a total score ranging from 2 to 10.
• Gleason Score of 2 – 4: • Well differentiated, slight anaplasia
• Gleason Score of 5 – 6: • Moderately differentiated, moderate anaplasia
• Gleason Score of 7 – 10: • Poorly differentiated or undifferentiated, marked anaplasia

Copyright 2011 American Society of Consultant Pharmacists
Workup of Prostate Cancer Diagnosis
A rectal examination of the patient reveals a prostate that isharder than normal. The serum Prostate Specific Antigen or PSA is elevated in most men with prostate cancer, even prior to symptoms, and is often used to assist in detectingthe disease in men who are asymptomatic. A transrectal ultrasound with a guided needle biopsy of the prostate through the rectum or perineum will confirm the diagnosis. A bone scan or CT of the abdomen is performed if the patients has signs of metastatic disease such as bone pain or jaundice.
While a digital rectal exam is sufficient to evaluate the local extent of the tumor, staging is necessary to characterize the extent of the disease and determine the most appropriate type of treatment. The first staging involves determining the degreee of differentiation of the tumor called the Gleason Score. The higher the grade or score, the less differentiated the tumor is and the poorer the prognosis for the patient.
The tumor is then staged based upon its size, lymph node involvement, and metastasis. In stage A disease the tumor is still small and is diagnosed incidentally on histologic examination. In stage B disease the tumor is palpable on digital rectal examination. In stage C the tumor has spread beyond the wall of the prostate but it is still confined to the pelvis. In stage D there is widespread dissemination of the disease.
Staging of Prostate Cancer
Stage A (I) Tumor discovered incidentally on histologic exam
Stage B (II) Tumor palpable on digital rectal exam
Stage C (III) Tumor extending beyond the prostate but confined to within the pelvis
Stage D (IV) Disseminated tumor

Copyright 2011 American Society of Consultant Pharmacists
Treatment Options for Prostate Cancer
Watchful Waiting
• Involves monitoring the prostate cancer and intervening only when the patient becomes symptomatic or the cancer progressed
• DRE and PSA should be performed every 6 months • It is an option for patients with a life expectancy of less than 10 years, the tumor is at Stage A or Stage B, the Gleason
score < 7, and PSA is less than 10 – 20 ng/ml
Advantages: • Avoids the side effects of therapy • Retains quality of life • Reduces the risk of treating small indolent cancer
Disadvantages: • Increased anxiety from the patient • Risk of progression of the cancer with uncertain long-term natural history of the prostate cancer • Therapy may be more intense • Requires frequent monitoring
Surgery • Radical Prostatectomy
Radiation Therapy

Copyright 2011 American Society of Consultant Pharmacists
Treatment Options for Prostate Cancer
Hormonal Therapy • Orchiectomy • LHRH analogs • Antiandrogens • Administered when the doubling time in the rise of the PSA is short • Administered immediately when patient experiences tumor related symptoms or has overt metastasis • LHRH analogs are as effective as orchiectomy • LHRH combined with antiandrogens provides limited benefit over LHRH analog alone • Antiandrogen therapy should precede LHRH agonists and continued in combination for one month to prevent tumor flare
Chemotherapy
Treatment options for prostate cancer include watchful waiting, surgery, radiation therapy, hormonal therapy, and chemotherapy.
The premise for watchful waiting is that prostate cancer is a benign, indolent disease and treatment is not necessary for some patients. It is generally only indicated for men with early stage prostate cancer that is at stage A or B, with a Gleason Score less than 7, and a PSA level less than 10 to 20 ng/ml, and a life expectancy of less than 10 years. The advantage to this option is that patients avoid the side effects of therapy while maintaining quality of life.
Surgery, specifically, radical prostatectomy is another primary treatment option for prostate cancer. As with other types of cancer, the only chance of curing prostate cancer is to remove the tumor while it is still localized. Complications of the surgical procedure include urinary incontinence and impotence; however, cure rates for patients with localized disease are excellent.

Copyright 2011 American Society of Consultant Pharmacists
Treatment Options for Prostate Cancer
Radiation therapy in prostate cancer is less reliable, and is recommended for patients who are not good surgical candidates.
The objective for hormonal treatment is to deprive prostatic tumors of circulating androgens and promote regression of primary and secondary tumors. Hormonal ablation is achieved either by surgical castration with an orchiectomy or medical castration with the use of LHRH agonists, or the use of agents that block binding of androgens to their receptors with the use of antiandrogens.
Hormonal therapy is the only effective treatment for patients with advanced stage or metastatic prostate cancer. In general, hormonal therapy is administered when the PSA velocity is high or if the patient experiences symptoms of metastatic prostate cancer.
Surgical castration and medical castration are both equally effective, but for psychological reasons, most patients choose medical castration. LHRH is generally effective when administered as the primary single hormonal therapy. Many men experience a “flare”—an acute worsening of their symptoms for several days after hormonal therapy is implemented. This is caused by an initial surge of testosterone, and treatment should continue unless back pain secondary to spinal cord compression worsens. In instances where the tumor flare symptoms are too severe to administer the LHRH safely, an antiandrogen can be administered prior to and in combination with the LHRH for a month to prevent complications of tumor flare.
Unfortunately, patient often relapses following hormonal therapy because prostatic cancer is composed of both hormone sensitive and hormone resistant cells. Chemotherapy agents are usually ineffective due to the slow growth of the disease and are used only when patients are no longer responding to hormonal therapy.

Copyright 2011 American Society of Consultant Pharmacists
Hormonal Therapy Options
LHRH Agonists
Leuprolide acetate • 7.5 mg IM q month • 22.5 mg IM q 3 months • 30 mg IM q 4 months • Subcutaneous implant to be delivered at
a control rate for 1 year
Common Adverse Drug Effects: • Hot flashes • Tumor flare • Impotence • Deep Vein Thrombosis /Pulmonary Embolism
Goserelin • 3.6 mg deep SC q month • 10.8 mg q 3 months • Side effects same as leuprolide
Antiandrogens
This slides provides information on the different LHRH agonists and antiandrogens that are used in practice for the treatment of prostate cancer. Common doses and side effects are also provided for your reference.
Flutamide • 250 mg PO TID • Start at 125 mg and titrate up
Adverse Drug Effects: • Rare methemoglobinemia
Bicalutamide • 50 mg PO QD
Nilutamide • 300 mg PO qd for 1 month, then 150 mg PO once daily
Adverse Drug Effects: • Disulfiram-like reaction • Decreased visual accommodation • Cconstipation • Interstitial pneumonitis
Class Adverse Drug Effects of Antiandrogens: • Gynecomastia • Hematuria, diarrhea • Impotence • Mild LFT increase
Second Line Hormonal Therapy • Antiandrogen withdrawal • Corticosteroids • Aminoglutethimide • Ketoconazole • Megesterol acetate

Copyright 2011 American Society of Consultant Pharmacists
Treatment of Different Stages of Prostate Cancer
Stages A & B of Prostate Cancer: • Radical prostatectomy • Radiation therapy • Watchful Waiting
Stage C Prostate Cancer: • Surgery is NOT an option • Radiation therapy • Adjuvant hormonal therapy
Stage D Prostate Cancer: • Hormonal therapy is first line
• Orchiectomy • LHRH agonists • Antiandrogens
• Chemotherapy for hormone refractory prostate cancer
• Estramustine • Mitoxantrone
Prostate Cancer Surveillance
Watchful WaiAng Clinical exam, DRE, & PSA every 6 months
DefiniAve Local Therapy DRE & PSA every 6 months, repeat prostate biopsy 1 year amer diagnosis
Treated with Intent to Cure
PSA every 6 months for 1st 5 years, then annually Annual DRE
Locally Advanced or MetastaAc Disease
History, physical examina:on, DRE, PSA every 3 to 6 months
Bone scan when pa:ents develop symptoms or PSA rises very quickly

Copyright 2011 American Society of Consultant Pharmacists
Treatment of Different Stages of Prostate Cancer
For patients diagnosed with Stage A or B prostate cancer the treatment options include a radical prostatectomy, radiation therapy, or watchful waiting. For a young patient with a life expectancy of more than 10 years, a radical prostatectomy is the treatment of choice. For patients who have less than 10 years of life expectancy and with a tumor that shows indolent characteristics, watchful waiting may be a reasonable option. Radiation is generally not the treatment of choice and is reserved for the patient who may not be able to tolerate surgery.
For patients with stage C prostate cancer, surgery is not an option. Radiation therapy combined with hormonal therapy is the treatment of choice for this stage of the disease and offers a chance of cure.
For patients with metastatic prostate cancer, the goal of therapy is to provide pain relief and palliate symptoms and to delay progression of the disease. Hormonal therapy is the primary treatment modality for stage IV prostate cancer.
Chemotherapy is generally used as a last resort when the patient’s prostate cancer has transformed into hormone refractory disease. Common chemotherapy agents used for this stage include estramustine, a nitrogen mustard and estradiol combination, and mitoxantrone.
After treatment is initiated, serum PSA tests are done periodically to monitor effectiveness of therapy and assess the recurrence of disease. A rising PSA in a man with a history of prostate cancer is an indication for treatment of recurrent disease.

Copyright 2011 American Society of Consultant Pharmacists
Pancreatic Cancer
Epidemiology • Estimated 31,860 new cases will be diagnosed in 2004 • Estimated 31,270 deaths will occur in 2004 • Accounts for 2% of all cancer diagnosis • Accounts for ~ 5% of all cancer related deaths • Fifth leading cause of adult deaths from cancer • Only 1 – 4% of patients will be alive 5 years after diagnosis
Risk Factors • Age (> 50 years, frequently in 7th & 8th decades) • Tobacco smoking • Family History • Race (African Americans) • Diabetes • Pancreatitis • Diet • Industrial chemical exposure
Molecular Features of Pancreatic Cancer • K-ras mutations • HER2/neu overexpression • p16, p53 mutations

Copyright 2011 American Society of Consultant Pharmacists
Pancreatic Cancer
Pancreatic cancer is the 5th most common cause of cancer related deaths in the United States. It is predicted that there will be 31,860 cases of newly diagnosed pancreatic cancer and almost the same number of deaths in 2004. Only 1 to 4% of patients diagnosed with pancreatic cancer will be alive at 5 years because the disease is very aggressive, it is very difficult to diagnose, and there are no effective systemic treatment options for this cancer.
Pancreatic cancer rarely occurs before 50 years of age. It is commonly diagnosed in the seventh and eighth decades of life. There is firm evidence linking smoking and pancreatic cancer and patients with a family history of pancreatic cancer is at high risk for developing the disease. The incidence in African-Americans has been found to be 30% higher than among white Americans.
There has been some correlation found between diabetes, pancreatitis and pancreatic cancer, although this association is a topic of great debate. There have been no clear dietary risk factors for pancreatic cancer. However, there may be a positive association between pancreatic cancer with meat and carbohydrate consumption, and dietary fat and increased body mass index has been implicated in experimental models. Exposure to chemical such as pesticides, ionizing radiation, betanaphthylamine and benzidine is also associated with an increased risk of pancreatic cancer.
Mutations of K-ras proto-oncogene occurs in about 90% of pancreatic cancers. Overexpression of the HER2/neu protein has also been found along with mutations of the p16 and p53 gene.

Copyright 2011 American Society of Consultant Pharmacists
Natural History of Pancreatic Cancer
Natural History of Pancreatic Cancer
• Spreads early to regional lymph nodes • Subclinical liver metastasis present in majority of patients • 50% of patients have metastasis at the time of diagnosis • Recurrence following curative procedures common • >80 % of patients present with disease that can
not be cured by surgical resection
Natural History of PancreaAc Cancer
Median Survival
Localized Disease 15 – 19 months 5-‐year survival ~20%
Locally Advanced Disease 6 – 10 months
MetastaAc Disease 3 – 6 months
Presenting Signs and Symptoms
• Jaundice • Pruritis • Phlebitis • Pain in the upper abdomen • Nausea, vomiting • Diarrhea, belching, bloating, hiccups • Constipation • Loss of appetite, weight loss • Mild diabetes • Depression
Diagnostic Workup
• History and Physical exam • Jaundice, abdominal masses, enlarged gallbladder, enlarged liver, ascites, enlarged lymph nodes, phlebitis
• Ultrasonagraphy or CT Scan of the abdomen to identify mass • Endoscopic Retrograde Cholangiopancreatography (ERCP) • Fine needle aspiration biopsy • CA 19-9 • CBC, serum bilirubin • Serum Alkaline Phosphatase

Copyright 2011 American Society of Consultant Pharmacists
Natural History of Pancreatic Cancer
Pancreatic cancer is aggressive and it spreads early in the disease to regional lymph nodes and the liver. Disease recurrence following potentially curative therapy is common in pancreatic cancer and patients usually relapse and die of their disease 5 years beyond the diagnosis and therapy. The most common site of metastasis is the liver and may occur in 50 – 70% of patients following potentially curative combined modality treatment.
The median survival is approximately 15 to 19 months for patients with localized disease, 6 to 10 months for patients with locally advanced disease, and the survival decreases to only 3 to 6 months if the patient has disseminated disease.
The most common symptom of pancreatic cancer is pain in the upper abdomen along with loss of appetite, nausea and vomiting, and constipation. Fifty percent of patients complain of early feeling of fullness after a meal. Other symptoms include diarrhea, bloating, phlebitis, problems with sleeping, and fatigue. Pruritis may also occur due to bile duct obstruction.
A diagnostic workup for pancreatic cancer includes an ultrasonagraphy or CT scan of the abdomen to identify any mass in the pancreas. If results from the CT scan are equivocal, then an ERCP may be performed instead. The tumor marker CA 19-9 is elevated in 70 to 80% of pancreatic cancer cases. A fine needle aspiration biopsy of the mass is necessary for histologic diagnosis of pancreatic cancer.

Copyright 2011 American Society of Consultant Pharmacists
Pancreatic Cancer
Staging • Resectable • Locally Advanced • Metastatic
Treatment Options for Pancreatic Cancer:
Surgery • Pancreaticoduodenectomy (Whipple Procedure) • Biliary Stenting
Radiation • Radiation concurrent with fluorouracil postoperatively
Chemotherapy • Fluorouracil • Gemcitabine
Resectable Disease • Surgical resection
Locally Advanced Disease • Radiotherapy and Chemotherapy • Adjuvant Chemotherapy • Fluorouracil or Gemcitabine
Metastatic Disease • Chemotherapy
• Fluorouracil • Gemcitabine

Copyright 2011 American Society of Consultant Pharmacists
Pancreatic Cancer
The most widely accepted and utilized staging system for pancreatic cancer is the Clinical Staging System based upon 3 classifications. The first classification is if the cancer is resectable or borderline resectable. The second classification is if the cancer is locally advanced, and the third is if the cancer is disseminated.
Treatment options for pancreatic cancer include surgery, radiation therapy and systemic chemotherapy.
Surgical procedure involving resection of the tumor and the surrounding pancreatic tissue. It is the only potentially curative treatment option for pancreatic cancer.
Radiation therapy concurrent with fluorouracil chemotherapy should be administered following surgical resection in all patients.
Fluorouracil has been the most widely used chemotherapy agent in the treatment of pancreatic cancer in the past few decades. Today, however, gemcitabine is the current standard of care for patients with locally advanced and metastatic pancreatic cancer.

Copyright 2011 American Society of Consultant Pharmacists
Complications from Pancreatic Cancer
Pain • Chemotherapy / Radiation Therapy • Analgesics • Anesthetic blocks • Behavioral approaches
Obstructive Jaundice • Surgical bypass • Endobiliary Stenting
Weight Loss or Cachexia • Megesterol acetate • Dexamethasone • Dronabinol
Pancreatic Insufficiency • Pancreatic enzyme replacement
Depression and Fatigue • Tricyclic antidepressants • Selective serotonin reuptake inhibitors • Methylphenidate • Recombinant human erythropoietin
The goal of therapy for most patients diagnosed with pancreatic cancer is palliation of symptoms and optimization of supportive care.
Pain is reported by 75 – 80% of patients at initial evaluation of the pancreatic cancer and it is described as a dull, fairly constant pain of visceral origin localized to the region of the middle and upper back. Optimal pain management consists of radiation therapy with or without chemotherapy to palliate the pain associated with the pancreatic cancer. Pharmacologic management involves the use of analgesic agents such as opioids or non-steroidal inflammatory agents. An anesthetic block of the celiac plexus may also offer fast and effective pain control that can last for a period of 3 to 4 months.
For patients with pancreatic cancer located in the head of the pancreas, obstructive jaundice leads to the diagnosis. Symptoms of obstructive jaundice include pruritis, jaundiced sclera and skin, discolored urine and clay colored stool. Biliary decompression by a surgical bypass or an endobiliary stenting is the technique to resolve this situation.
Cachexia and weight loss is associated with weakness, poor quality of life and contributes to depression and increased morbidity. Caloric supplementation and hydration are initial treatment along with pharmacologic intervention with the addition of appetite stimulants such as megesterol acetate and dexamethasone. The addition of pancreatic enzymes for pancreatic insufficiency will improve malabsorption, bloating, diarrhea, and prevents further weight loss in pancreatic cancer patients.

Copyright 2011 American Society of Consultant Pharmacists
Complications from Pancreatic Cancer
Forty-seven to seventy-one percent of patients with pancreatic cancer experience depression. Treatment for this symptom includes the use of tricyclic antidepressants or selective serotonin reuptake inhibitors. Furthermore, for the patient experiencing fatigue, the psychostimulant methylphenidate may be used to improve this symptom. Lastly, a recombinant erythropoietin can be used to correct the anemia if all other treatable causes of the anemia have been ruled out.
In summary, pancreatic cancer is an aggressive cancer for which a cure still remains elusive and the treatment of this disease is challenging. Palliation of the patient’s symptoms is important to maintain the best quality of life and attention must be paid to controlling the patient’s pain, improving the patient’s nutritional status and meeting their psychosocial needs.

Copyright 2011 American Society of Consultant Pharmacists
Resources
For additional information, see:
Abbruzzese JL. Past and present treatment of pancreatic adenocarcinoma: chemotherapy as a standard treatment modality. Semin in Oncol.2002;29:2-8.
Akduman B, Crawford ED. The management of high risk prostate cancer. J Urol.2003;169:1993-1998.
Balmer C, Valley AW.(1996).Basic Principles of cancer treatment and cancer chemotherapy.In: Dipiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, & Posey LM,(Eds.). Pharmacotherapy: A Pathophysiologic Approach. Samford: Appleton and Lange: 2403-2466.
Blackstock AW, Cox AD, Tepper JE. Treatment of pancreatic cancer: current limitations, future possibilities. Oncology.1996;10:301-323.
Brendler CB.(1994).Oncology and aging:Generaly principles of cancer in the elderly.In: Hazzard WR, Bierman EL, Blass JP, Ettinger WH, & Halter JB, (Eds.). Geriatric medicine and gerontology, 3rd ed.New York:McGraw-Hill:657-664.
Davise LE, Krawczeniuk MM. (1996). Colorectal Cancer. In: Dipiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, & Posey LM,(Eds.). Pharmacotherapy: A Pathophysiologic Approach. Samford: Appleton and Lange: 2513-2538.
EL Kamar FG, Grossbard ML, Kozuch PS. Metastatic pancreatic cancer: emerging strategies in chemotherapy and palliative care. Oncologist.2003;8:18-34.
Folprecht G, Kohne CH. The role of new agents in the treatment of colorectal cancer. Oncology.2004;66:1-17.

Copyright 2011 American Society of Consultant Pharmacists
Resources
Goldspiel BR, Kolesar JM, Kuhn JG. (1996). Prostate Cancer. In: Dipiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, & Posey LM,(Eds.). Pharmacotherapy: A Pathophysiologic Approach. Samford: Appleton and Lange: 2539-2558.
Jemal A, Tiwani R, Murray T, Ghafoor A, Samuels A, Ward E, et al. Cancer Statistics, 2004. CA Cancer J Clin.2004;54:8-29.
Kent EC, Hussain MHA. The rationale for adjuvant chemotherapy for high-risk prostate cancer. Curr Opin Urol.2003;13:123-131.
Konner J, O’Reilly E. Pancreatic Cancer: epidemiology, genetics, and approaches to screening. Oncology.2002;16:1615-1638.
McMurtry CT, McMurtry JM. Metastatic prostate cancer: complications and treatment. J Am Geriatr Soc.2003;51:1136-1142.
National Comprehensive Cancer Network Clinical Practice Guidelines. Colorectal Cancer. June 2004
National Comprehensive Cancer Network Clinical Practice Guidelines. Prostate Cancer. June 2004
National Comprehensive Cancer Network Clinical Practice Guidelines. Pancreatic Cancer. June 2004
Schwartz RN. (1995). Cancer in the Elderly. In:Delafuente JC, Stewart RB, (Eds.). Therapeutics in the elderly. Cincinnati: Harvey Whitney Books, 500-12. National Cancer Institute: Pharmaceutical Information Network: Cancer Information Center: University of Pennsylvania Cancer Center: OncoLink: