pharmacotherapy gi disorders
TRANSCRIPT
Clinical Use of Drugs :Pharmacotherapy GI Disorders

Upper GI Disorders
GI Anatomic region
Gastric Acid Secretion⇨ Neuronal
– sight, smell, taste → cholinergic pathway⇨ Physical
– strecth → ↑acetylcholine & ↑gastrin⇨ Hormonal
● Stimulate parietal cells to secrete gastric acid
⇨ Gastrin⇨ Acetylcholine⇨ Histamine
Proton pump (H+/K+- ATPase)
Acid Secretion
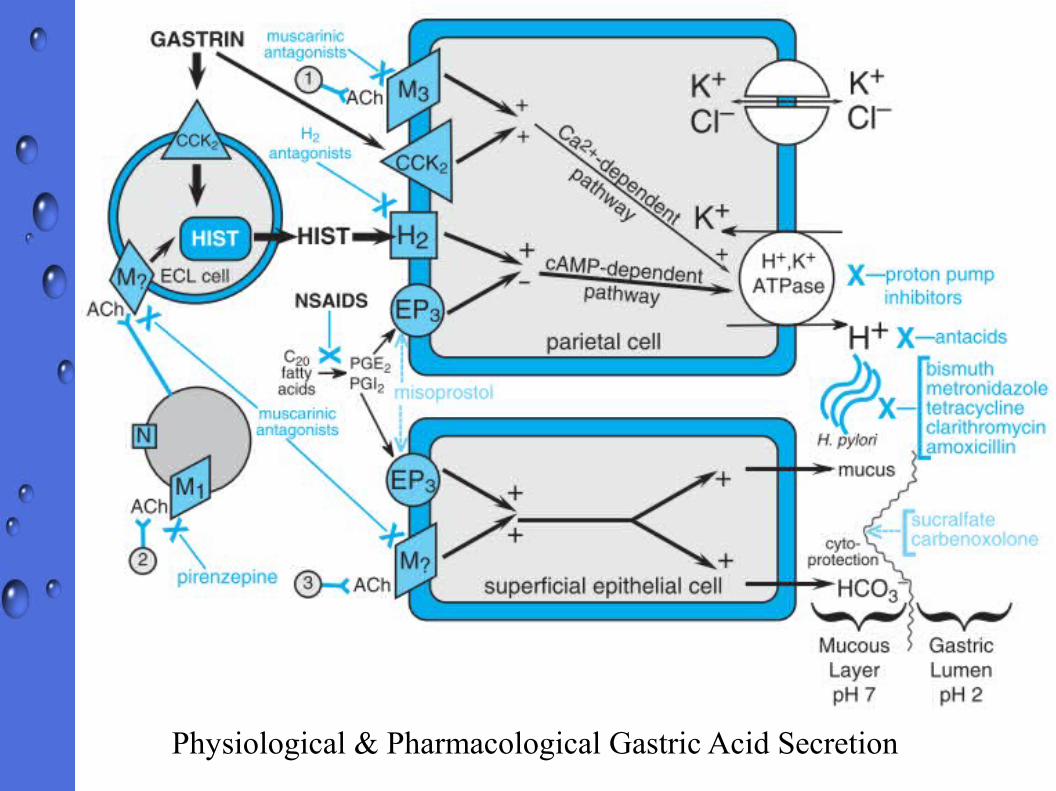
Physiological & Pharmacological Gastric Acid Secretion

Pharmacotherapy of Acid – Related Disorders
Acid-suppressing drugsProton-pump Inhibitors (PPIs)Proton-pump Inhibitors (PPIs)⇨ Five PPIs available in clinical use : Omeprazole,
Esomeprazole, Lansoprazole, Rabeprazole, & Pantoprazole
– Similar in their pharmacological properties⇨ All PPIs have equivalent efficacy at comparable
doses⇨ PPIs diminish daily production of acid by 80 –
95% → most potent gastric suppressorsmost potent gastric suppressors
⇨ PPIs → prodrugsprodrugs, require activation in acid environment → tetracyclic sulfenamide → unable to diffuse back to canalicular membrane
⇨ Activated form of PPIs covalently bound to H+/K+-ATPase → Acid secretion resume after newly formed H+/K+-ATPase molecules → Prolong acid suppression (24 – 48 hours)
⇨ PPIs block final steps of acid secretionPPIs block final steps of acid secretion ⇨ Effective in acid suppression regardless of other
stimulating factors⇨ Dosage form : Enteric – coated drugs, enteric – coated
granules, enteric – coated tablets, powdered in combination with bicarbonate → to prevent degradation by acid in the stomach

Pharmacokinetics :⇨ Rapidly absorbed, highly protein – bound,
extensively metabolized by hepatic CYPs● CYP2C19 & CYP3A4
– CYP2C19 genotype● Asian vs Caucasian or African American (23% vs (23% vs
3%)3%)⇨ Chronic renal failure does not lead to
accumulation of PPIs with once-a-day dosing⇨ Hepatic impairment substantially reduce
clearence of esomeprazole and lansoprazole

⇨ Most common : nausea, abdominal pain, flatulence, & diarrhea
● Subacute myopathy, arthralgia, headache, & rash
⇨ Inhibition of CYP2C19, slower the clearence of phenytoin, disulfiram, & other drugs metabolized the same enzymes)
⇨ Increase expression of CYP1A2 (increase clearence of imipramine, antipsychotic drugs, tacrin, & theophylline)
⇨ Loss of gastric acidity → affect bioavailability of ketoconazole, ampicillin esters, & iron salts
⇨ Chronic use ≈ hip fracture, possibly decreasing Ca2+ absorption
Adverse Effects & Drug Interactions
⇨ Most common : nausea, abdominal pain, flatulence, & diarrhea
● Subacute myopathy, arthralgia, headache, & rash
⇨ Inhibition of CYP2C19, slower the clearence of phenytoin, disulfiram, & other drugs metabolized the same enzymes)
⇨ Increase expression of CYP1A2 (increase clearence of imipramine, antipsychotic drugs, tacrin, & theophylline)
⇨ Loss of gastric acidity → affect bioavailability of ketoconazole, ampicillin esters, & iron salts
⇨ Chronic use ≈ hip fracture, possibly decreasing Ca2+ absorption
Adverse Effects & Drug Interactions
Therapeutic Use⇨ Promote healing of gastric & duodenal
ulcers⇨ Gastroesophageal reflux disease (GERD)⇨ Hypersecretory conditions : Zolinger-
Ellison syndrome⇨ Prevention of recurrence of NSAID –
associated gastric ulcers
H2 Receptor Antagonists
⇨ H2RAs → competitive inhibitors of H2 receptor on basolateral membrane of parietal cells
⇨ Available drugs : Cimetidine, Ranitidine, Famotidine, Nizatidine
● Differ in pharmacokinetics & propensity to cause drug interations
⇨ H2RAs predominantly inhibit basal acid secretion → suppressing nocturnal acid secretion
⇨
Pharmacokinetics
⇨ Rapidly absorbed, peak serum concentration achieved within 1 – 3 hours
⇨ Small percentage of H2RAs are protein-bound⇨ Liver disease per se is not indication for dose
adjustment⇨ Excreted by kidneys through filtration & tubular
secretion → reduce dose on patients with reduced creatinine clearence
Adverse Effects & Interactions⇨ H2RAs generally well-tolerated
⇨ Low incidence of AEs : diarrhea, headache, fatigue, muscular pain, & constipation
⇨ Neurologic : headache, dizziness, drowsiness, lethargy, hallucination, psychosis)
⇨ Long-term use :– Cimetidine at high doses → inhibit testosterone binding to
androgen receptors & inhibition of CYP reduce hydroxylation of estradiol
– Galactorrhea in women, and gynecomastia, reduced Galactorrhea in women, and gynecomastia, reduced sperm counts & impotence in mensperm counts & impotence in men
⇨ Blood dyscrasia including thrombocytopenia have been reported
⇨ H2RAs cross the placenta & excreted in breast milk
Therapeutic Uses⇨ Promote healing of gastric & duodenal ulcers⇨ Treat uncomplicated GERD⇨ Prevent occurrence of stress ulcers
Agents that Enhance Mucosal Defences
Prostaglandin Analog : Misoprostol⇨ Synthetic analog of PGE1⇨ Gastric acid secretion inhibition – Dose related
⇨ 100 – 200 ug significantly inhibit basal secretion ( up to 95%) or food – stimulated secretion ( 85% inhibition)
⇨ Cytoprotective role of prostaglandin toward gastric acidity⇨ Stimulate Gi pathway → decreasing cAMP & gastric acid
secretion⇨ Stimulate mucin & bicarbonate secretion⇨ Increase blood flow
⇨ Recommended dose for ulcer prophylaxis : 200 ug four times a day
● Frequent dosing limited its use → inconvenience⇨
⇨ Misoprostol can cause exacerbation of inflammatory bowel disease
⇨ Contraindicated in pregnancy → increase uterine contractility
Therapeutic Use⇨ To prevent NSAID-induced mucosal injury
Sucralfate⇨ Sulfated polysaccaride → Octasulfate of sucrose
⇨ Inhibit pepsin-mediated hydrolisis of mucosal proteins contributes to mucosal erosion & ulceration
⇨In acid environment (pH<4), sucralfate → cross-linking → viscous & sticky polymer that adhere to epithelial cells & ulcer crater up to 6 hours after single dose
⇨Stimulating secretion of PGs & growth factors
Therapeutic Use⇨ In critically patients, sucralfate may offer advantage
over PPIs & H2RAs in preventing stress ulcers⇨ Condition associated with mucosal inflammation /
ulceration which is not responsive to acid suppression such as oral mucositis (radiation & aphtous ulcer), bile reflux gastropathy
Bismuth Salts⇨ Binding to and protecting mucosal lesion⇨ Enhancing cellular protective mechanims⇨ Antimicrobial effects, primarily againts
H.pylori⇨ Frequently use in combination with other
antibiotics to eradicate H.pylori
Prokinetic agentsProkinetic agentsMetoclopramide & Betanechol⇨ Stimulate motility of upper GI & increase LES
(lower esophageal sphincter)⇨ Patients with delayed gastric emptying or refractory to
other available treatment options

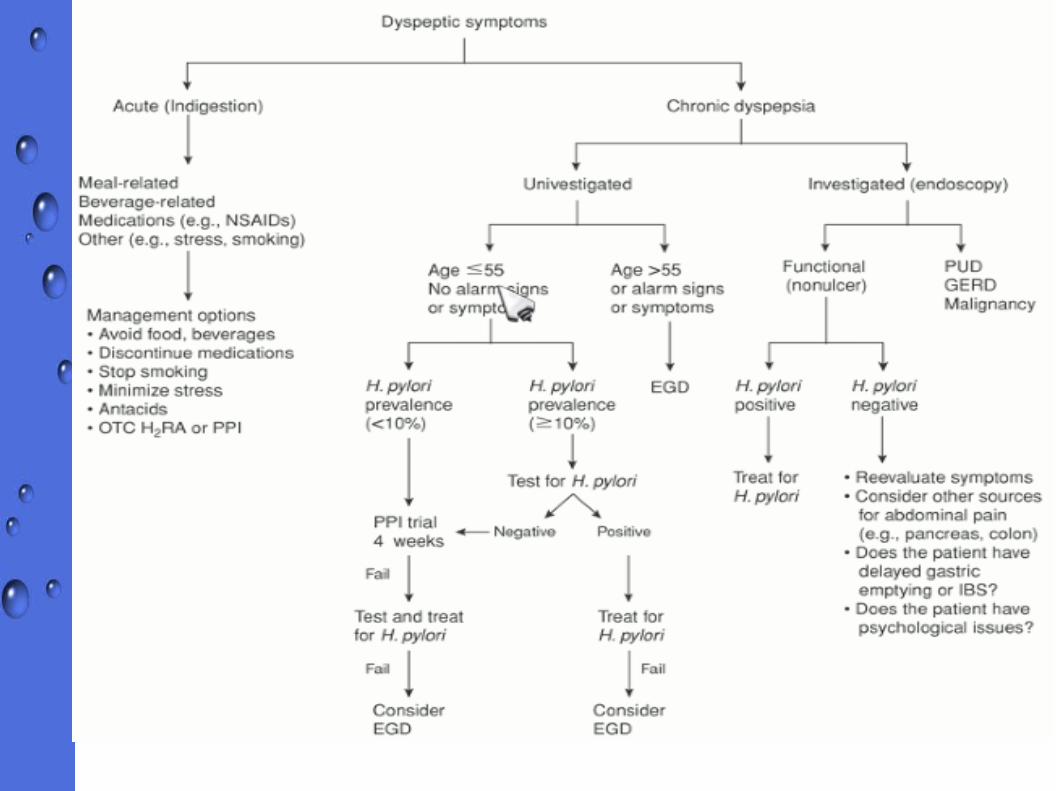
General Guidelines of medical management of Gastroesophageal Reflux Disease (GERD)
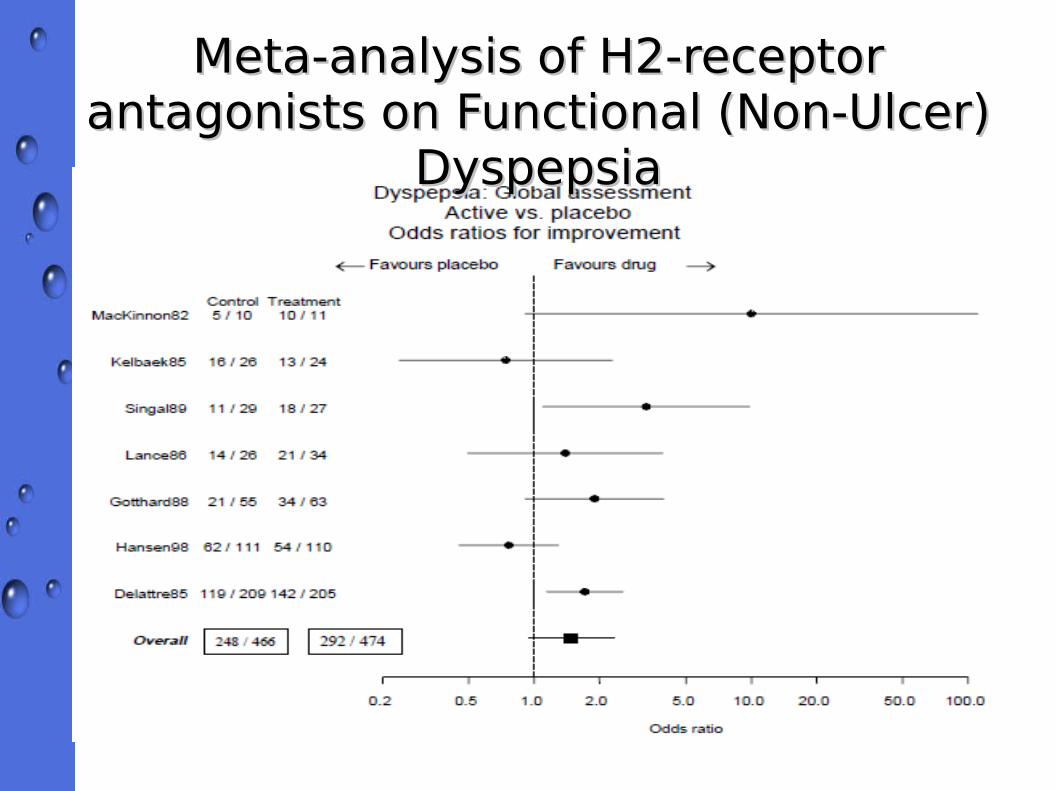
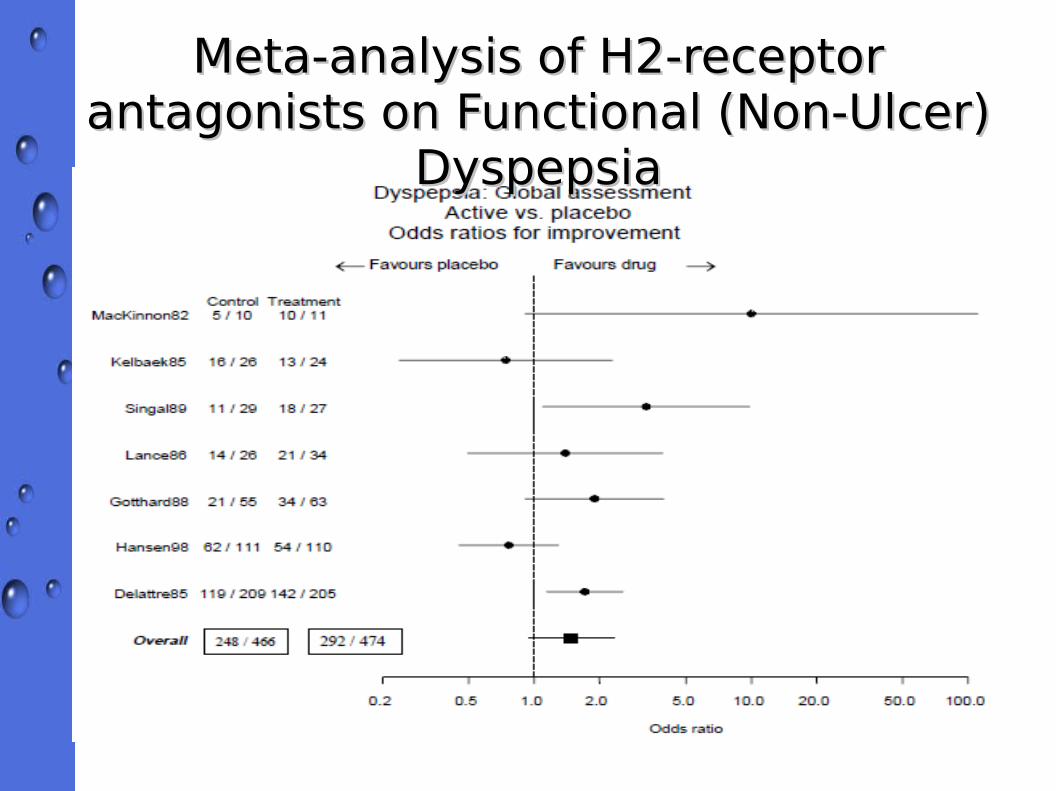
Meta-analysis of H2-receptor Meta-analysis of H2-receptor antagonists on Functional (Non-Ulcer) antagonists on Functional (Non-Ulcer)
DyspepsiaDyspepsia
Meta-analysis of H2-receptor Meta-analysis of H2-receptor antagonists on Functional (Non-Ulcer) antagonists on Functional (Non-Ulcer)
DyspepsiaDyspepsia

Comparison of Prokinetic, Acid Suppression, Comparison of Prokinetic, Acid Suppression, and Antianxiety Therapies in Functional and Antianxiety Therapies in Functional
DyspepsiaDyspepsia
Both Mosapride and Famotidine significantly improved the symptoms of Functional Dyspepsia within 2 weeks and the improvement was maintained for 8 weeks after the beginning of the study (p < 0.001)

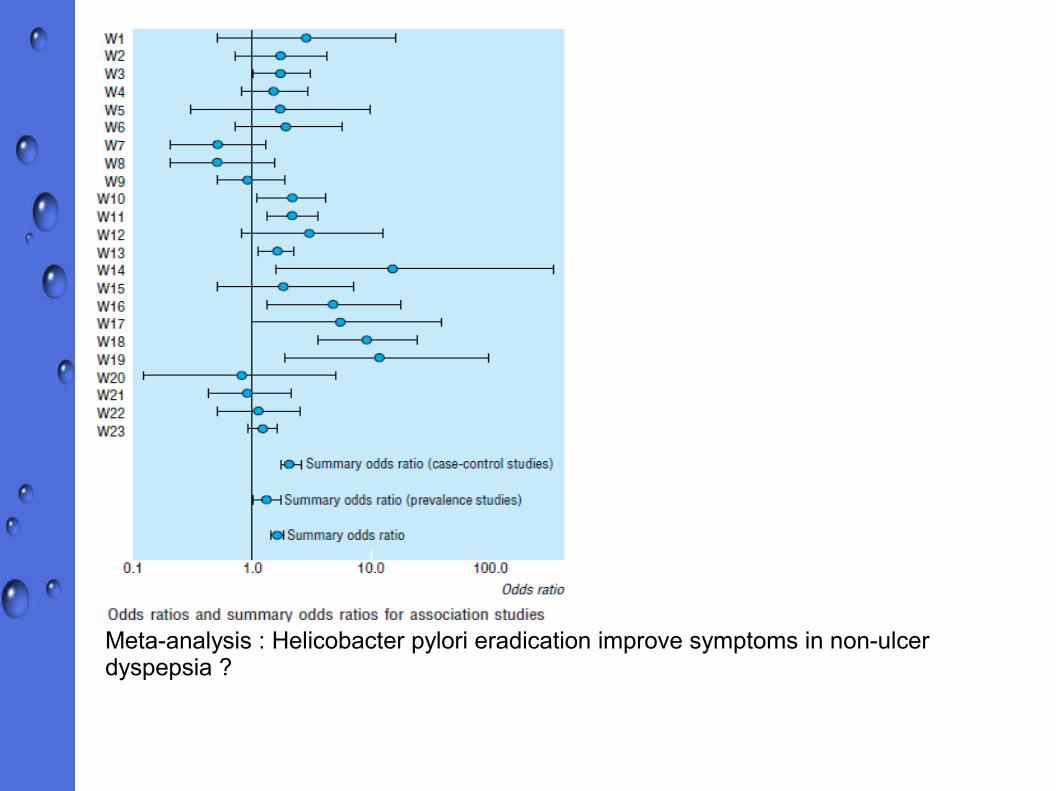
Meta-analysis : Helicobacter pylori eradication improve symptoms in non-ulcer dyspepsia ?

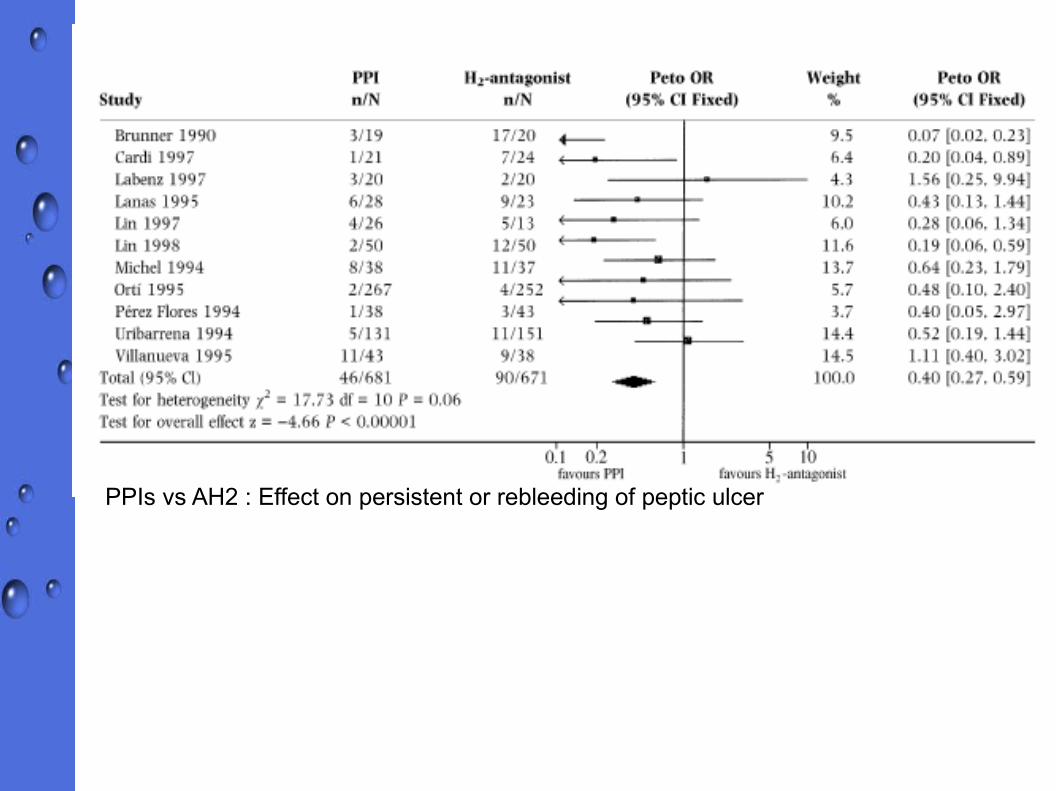
PPIs vs AH2 : Effect on persistent or rebleeding of peptic ulcer
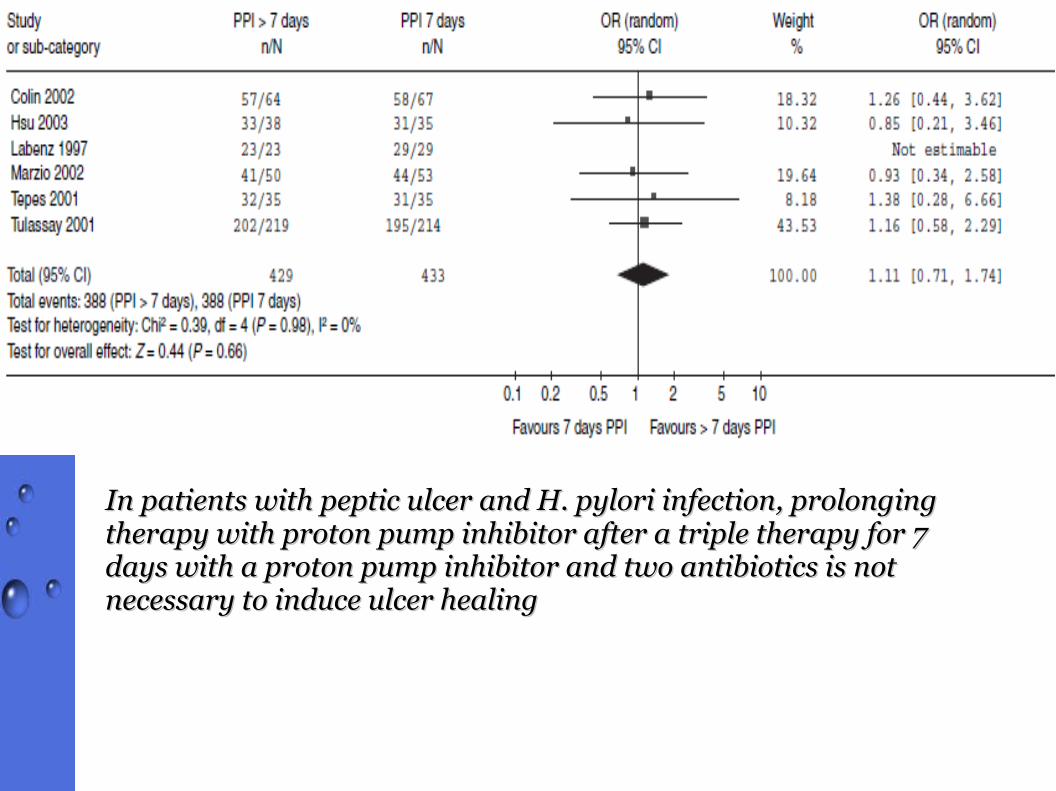
In patients with peptic ulcer and H. pylori infection, prolonging In patients with peptic ulcer and H. pylori infection, prolonging therapy with proton pump inhibitor after a triple therapy for 7 therapy with proton pump inhibitor after a triple therapy for 7 days with a proton pump inhibitor and two antibiotics is not days with a proton pump inhibitor and two antibiotics is not necessary to induce ulcer healingnecessary to induce ulcer healing
Step-Up vs Step-Down Therapy in New-Onset Dyspepsia
⇨ Double-blind, randomized controlled trial● Step-up therapy : started with antacids, switched to
H2-receptor antagonists, and then ended with proton pump inhibitors (PPIs)
● Step-Down therapy : reversed order
– Step-Up therapy somewhat more Step-Up therapy somewhat more cost effectivecost effective than a than a step-down approach, but effectiveness of treatment step-down approach, but effectiveness of treatment and adverse events are similar.and adverse events are similar.

Nausea & VomitingPatophysiology of Emesis⇨ Nausea, the imminent need to vomit
● Associated with gastric stasis⇨ Retching,
⇨ Labored movement of thoracic & abdominal muscles before vomiting
⇨ Vomit● Forceful of GI contents caused by GI retroperistalsis
⇨ Act of vomiting require coordinated contraction of abdominal muscles, pylorus, antrum, raised gastric cardia, diminished lower esophageal sphincter, & esophageal dilatation
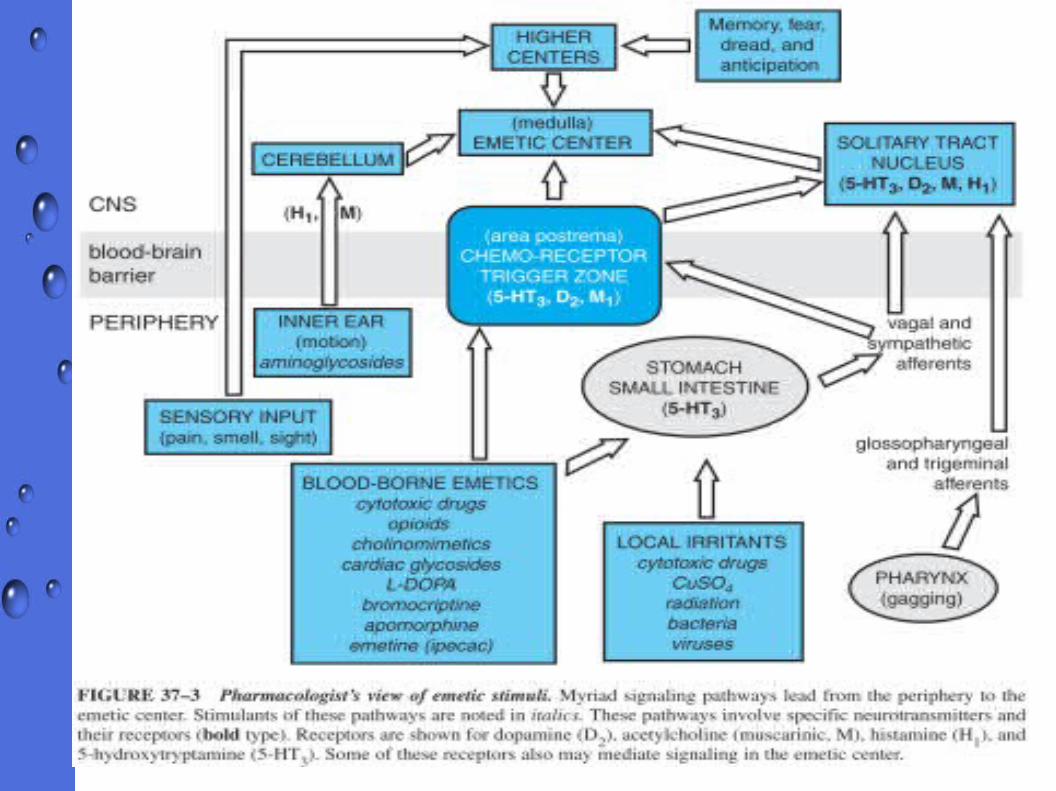
⇨ Chemoreceptor trigger zone (CTZ)⇨ Neurotransmitter receptor : cholinergic, histaminic,
serotonergic, dopaminergic, opiate, neurokinin, & benzodiazepin receptors
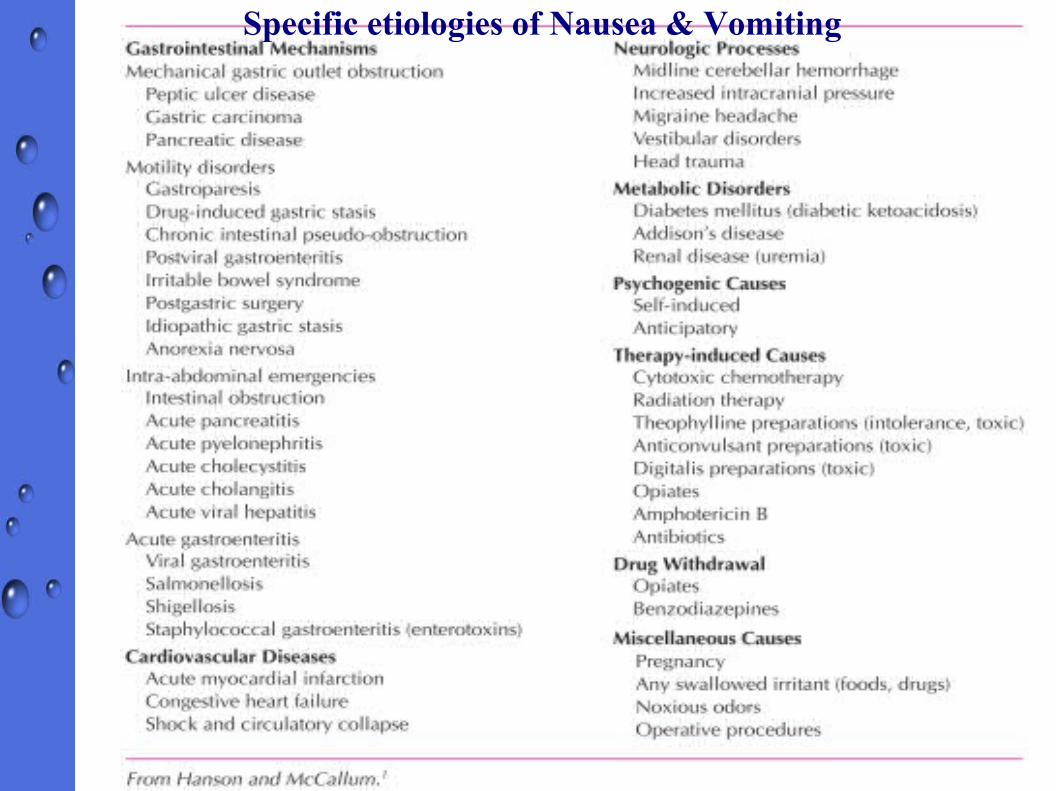
Specific etiologies of Nausea & Vomiting
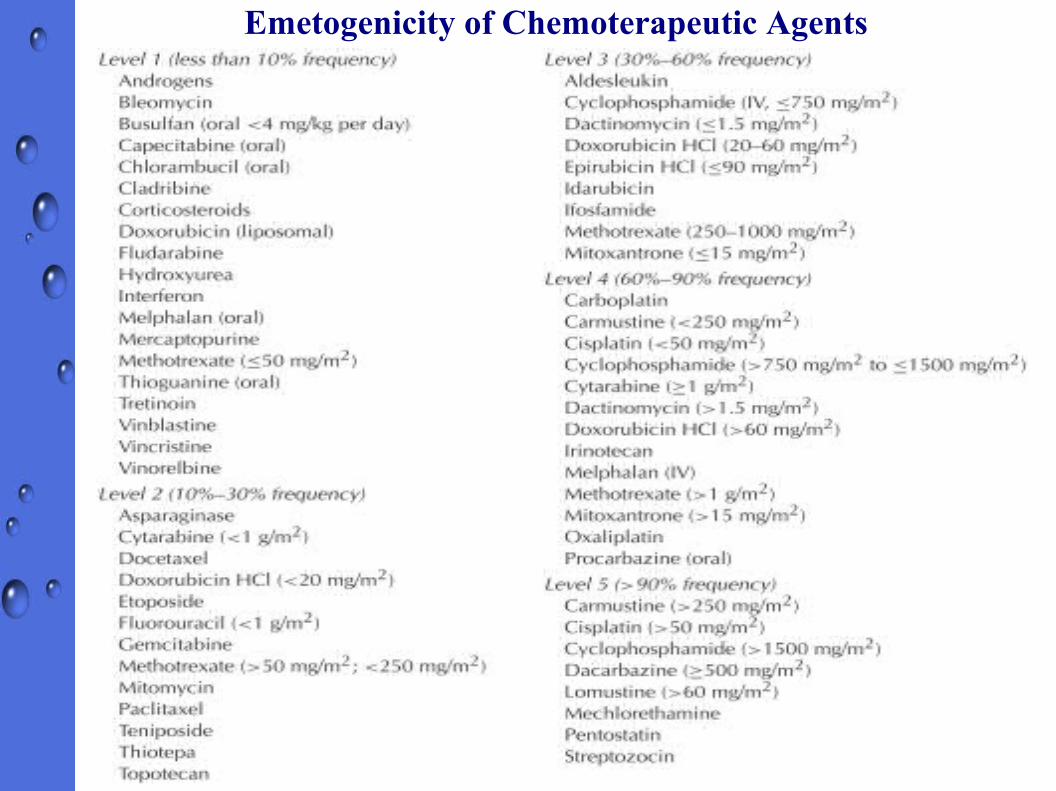
Emetogenicity of Chemoterapeutic Agents
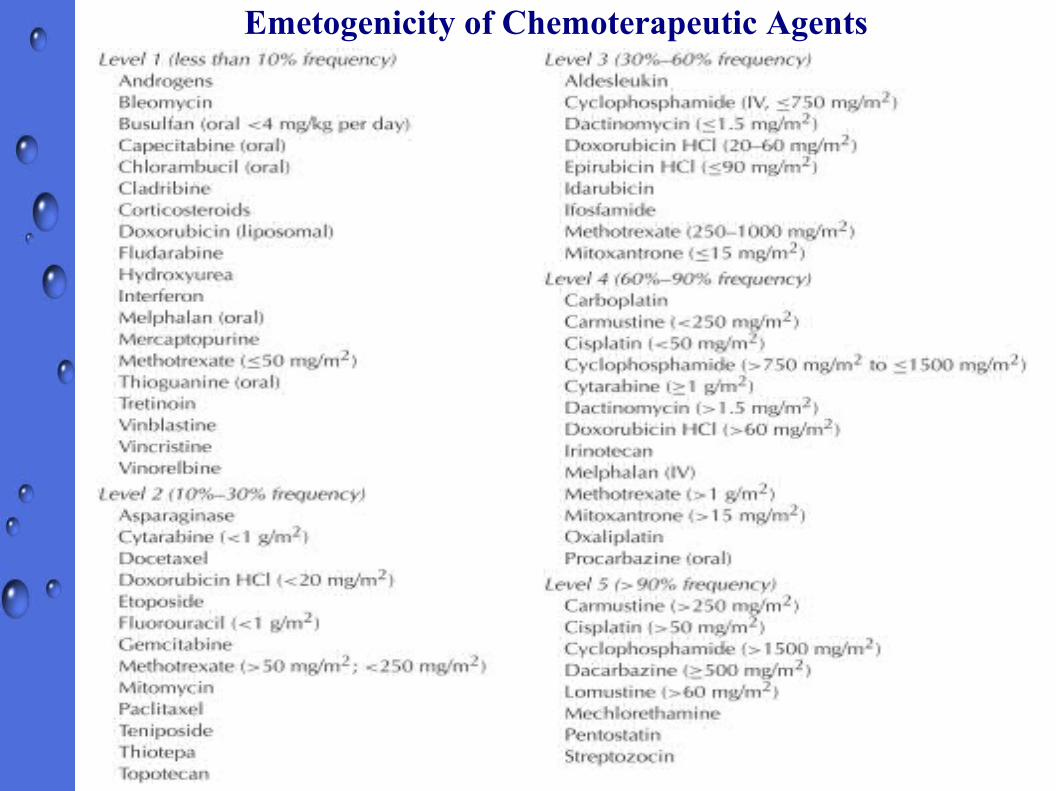
Emetogenicity of Chemoterapeutic Agents
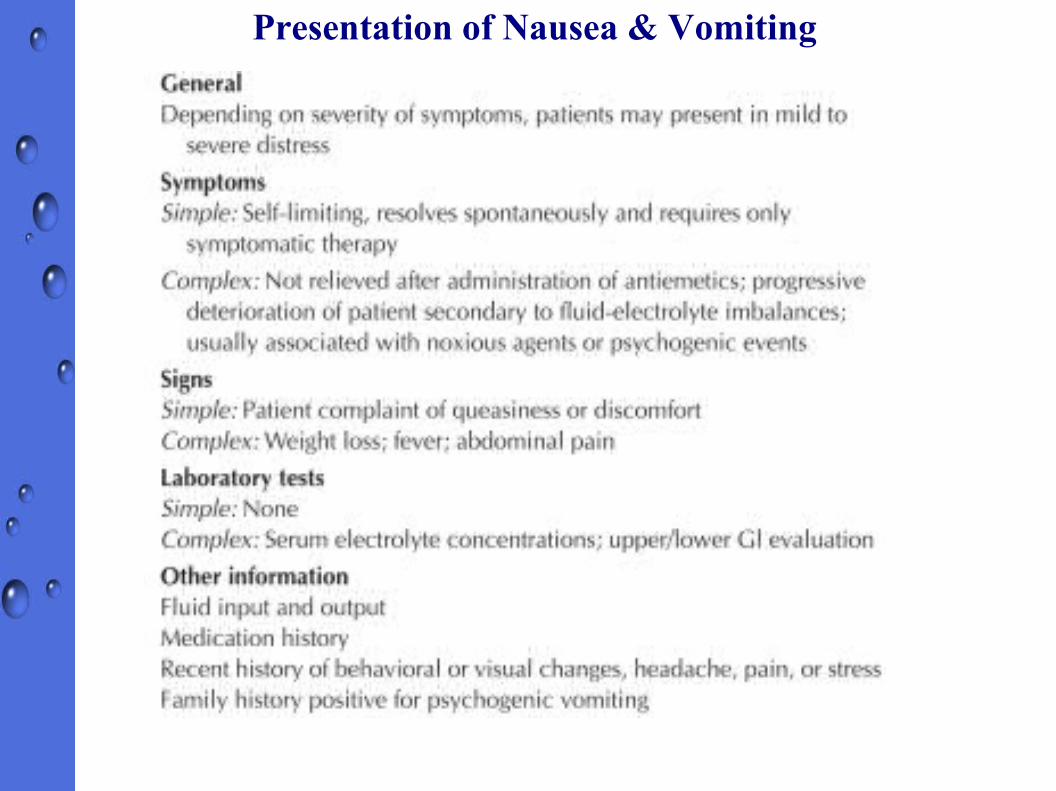
Presentation of Nausea & Vomiting

TreatmentNon pharmacologic⇨ Dietary restriction if appropiate⇨ Stable physical position⇨ Psychological & behavioral intervention
● Relaxation● Bio-feedback● Self-hypnosis● Cognitive distraction● Guided imagery● Systematic desentization
⇨ Etc
Pharmacological intervention
Pharmacological Intervention
Factors that enable clinician to discriminate the choices of antiemetic must be recognized, :⇨ The suspected etiology of symptoms⇨ Frequency, duration, & severity of the episodes⇨ The ability of patients to use oral, rectal,
injectable or transdermal medication⇨ The success of previous antiemetic medication



Laxative, Cathartics, & Therapy of Constipation
⇨ Fluid content is principal determinant of stool content (70 – 85% contain water)
⇨ 8 – 9 L of fluid enter small intestine ⇒ 1 – 1.5 L crossing ileocaecal valve, colon extracts most of remaining fluid ⇒ ∽ 100 ml of fecal water daily
⇨ Secretory changes, bowel movement, transit time, extent of absorption determine the consistency of stool⇨ Neurohormonal mechanisms, pathogens, drugs might alter
processes above⇨ Up to 60% of patients with constipation have normal
colonic transit⇨ Predominant factors underlying constipation often not
obvious ⇒ therapy remain empiric & non specific
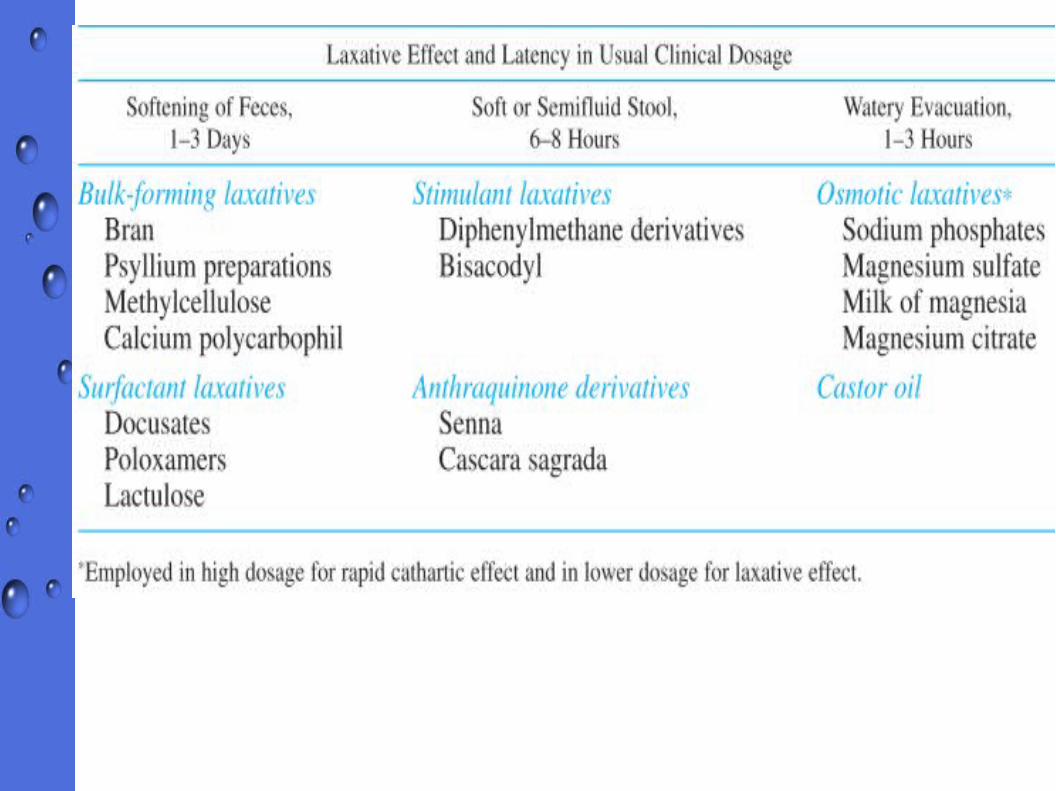
⇨ Laxation : evacuation of formed fecal material from rectum)
⇨ Catharsis : evacuation of unformed, usually watery fecal material from the entire colon– The terms frequently used interchangebly
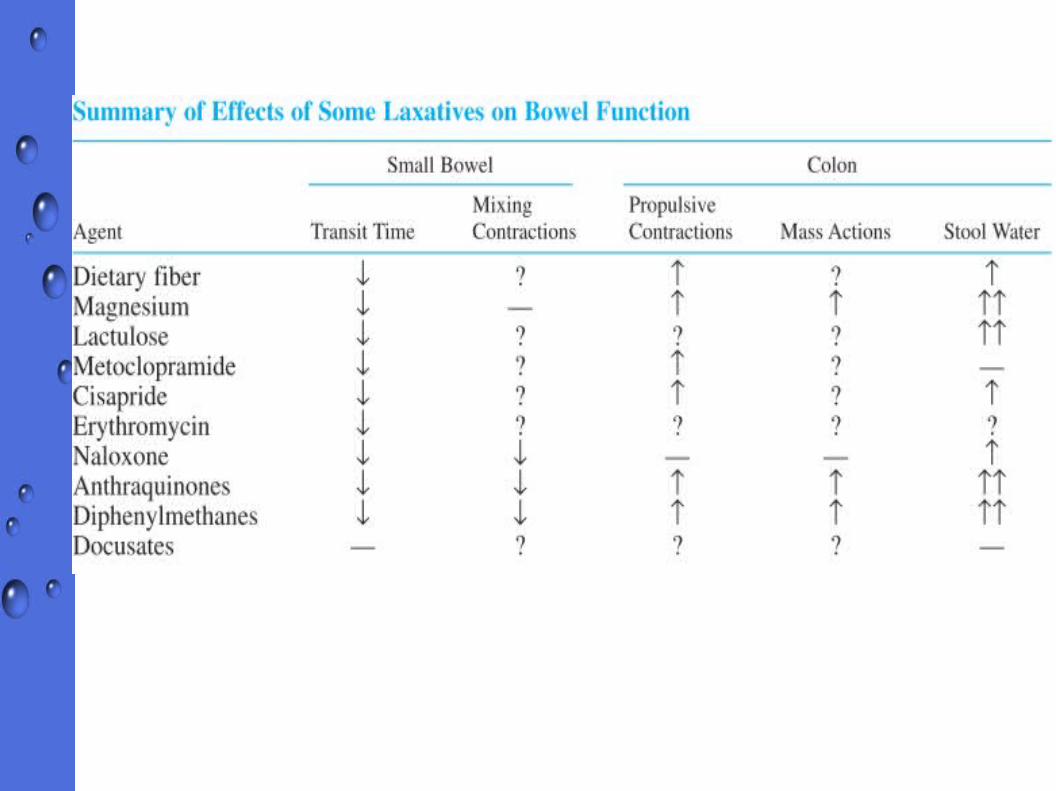
⇨ Mode of Action of Laxative :– Enhancing retention of intraluminal fluid by
hydrophilic or osmotic mechanims– Decreasing the net absorption of fluid by effects on
small- and large-bowel fluid & electrolyte transport– Altering motility by either inhibiting segmenting
(nonpropulsive) contractions or stimulating propulsive contractions


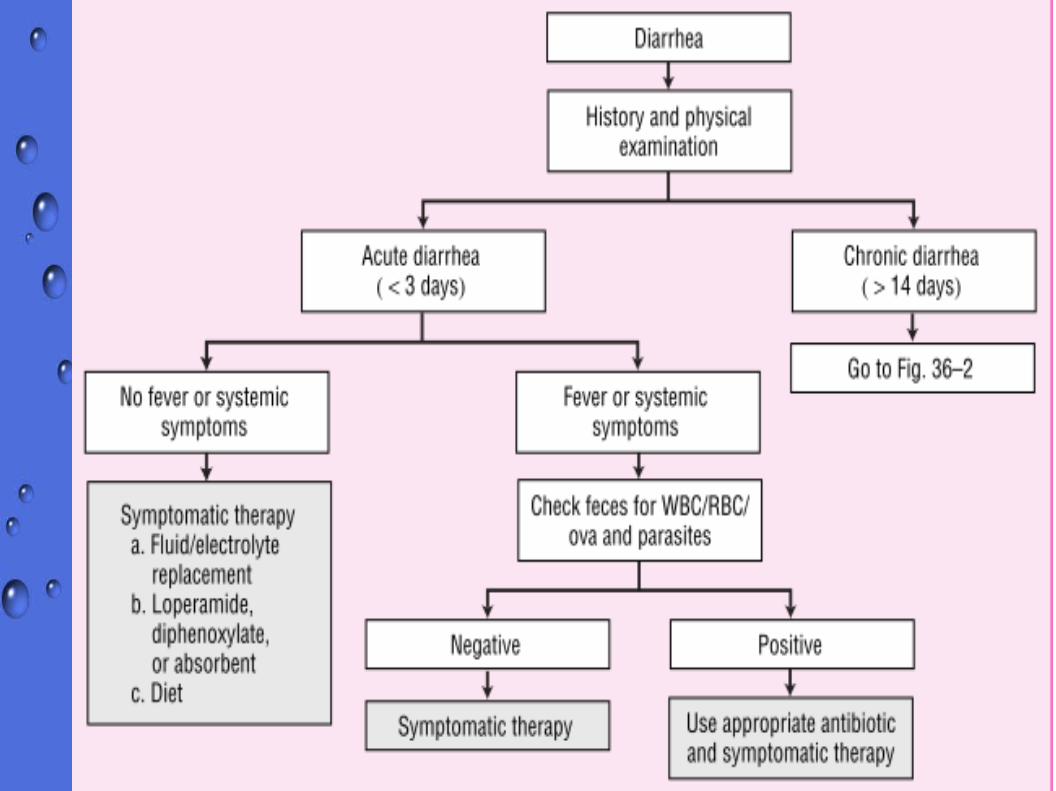
Antidiarrheal agents⇨ Oral rehydration solution is the cornerstone of
therapy for patient with acute illness resulting significant diarrhea
⇨ Pharmacotherapy should be reserved for patients with persistence symptoms
⇨
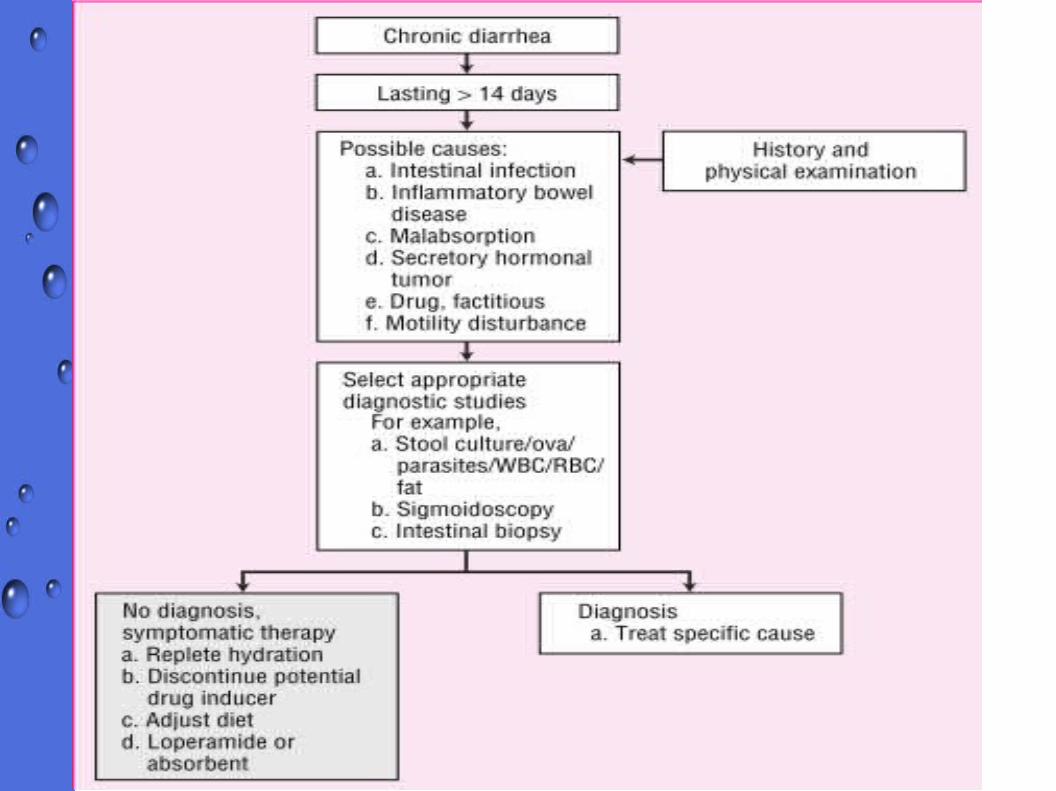
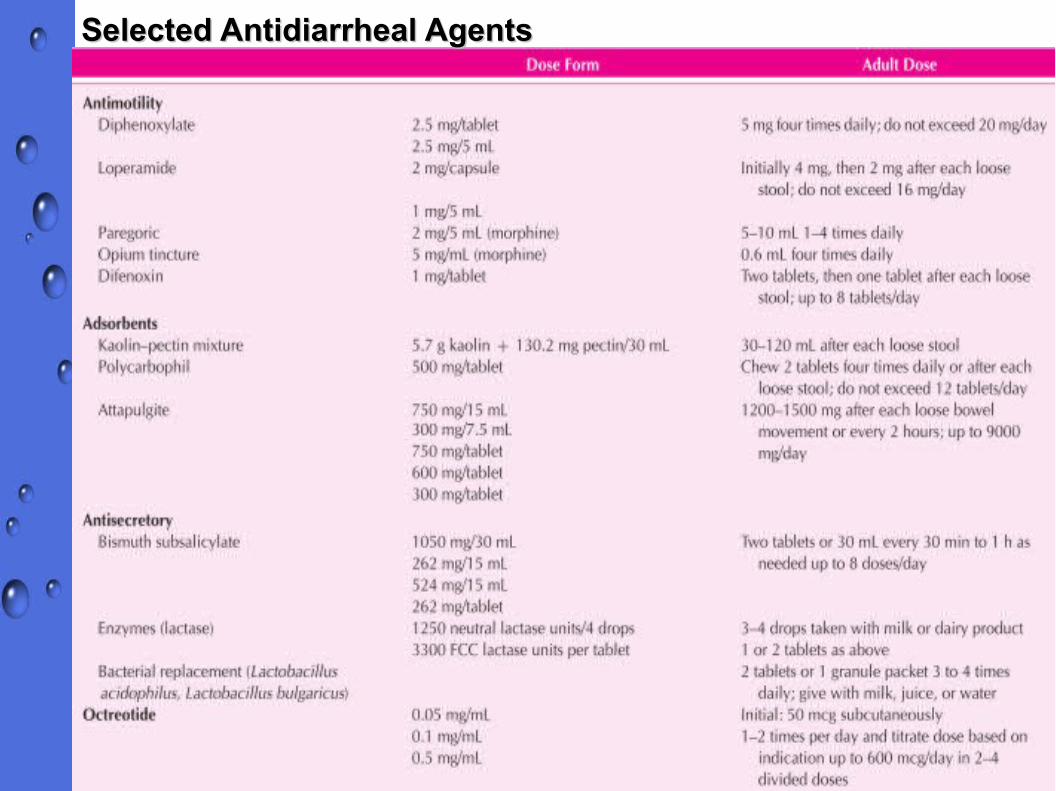
Selected Antidiarrheal AgentsSelected Antidiarrheal Agents