1 blood pressure, blood pressure agents and blood pressure guidelines ty j. gluckman, andrew p....
TRANSCRIPT
1
Blood Pressure, Blood Pressure Agents Blood Pressure, Blood Pressure Agents and Blood Pressure Guidelinesand Blood Pressure Guidelines
Ty J. Gluckman, Andrew P. DeFilippis, James Mudd, Catherine Campbell, Gregg Fonarow,
& Roger S. Blumenthal

2
Provides information on response to Rx. May help improve adherence to Rx and evaluate “white-coat” HTN
Self-measurement
Indicated for evaluation of “white-coat” HTN. Absence of 10–20% BP decrease during sleep indicates increased CVD riskAmbulatory BP monitoring
Two readings, 5 minutes apart, sitting in chair
Confirm elevated reading in contralateral arm
In-office
Brief Description Method
JNC VII Guidelines for Measurement of BPJNC VII Guidelines for Measurement of BP
BP=Blood pressure, CVD=Cardiovascular disease, HTN=Hypertension, Rx=Treatment
Chobanian AV et al. JAMA 2003;289:2560-2572

3
JNC VII Causes of Secondary HypertensionJNC VII Causes of Secondary Hypertension
Medical Conditions
Chronic kidney disease
Primary hyperaldosteronism
Renovascular disease
Chronic steroid therapy
Cushing’s syndrome
Pheochromocytoma
Aortic coarctation
Thyroid or parathyroid disease
Sleep apnea
Drugs
NSAIDS
Oral contraceptives
Adrenal steroids
Sympathomimetics
Cyclosporine or tacrolimus
Erythropoietin
Ephedra, mu huang, bitter orange
Cocaine or amphetamines
Alcohol
Chobanian AV et al. JAMA 2003;289:2560-2572
NSAIDS=Non-steroidal anti-inflammatory drugs

4Fields LE et al. Hypertension 2004;44:398-404
All
0
Pre
vale
nce
of H
yper
tens
ion
45
30
20
15
10
25
40
5
35
Mexican-American
Non-Hispanic White
Non-Hispanic Black
FM FM FM
National Health and Nutrition Examination Survey (NHANES)
Blood Pressure: Risk in U.S. AdultsBlood Pressure: Risk in U.S. Adults
1999-20001988-1994
F=Female, M=Male
Hypertension defined as blood pressure >140/90 mmHg or treatment

5
0
20
40
60
80
Hyp
erte
nsio
n P
reva
len
ce (
%)
18-29
National Health and Nutrition Examination Survey (NHANES) III
30-39 40-49 50-59 60-69 70-79 80+
Age
3%9%
18%
JNC-VI. Arch Intern Med 1997;157:2413-2446
Blood Pressure: Risk Increases with AgeBlood Pressure: Risk Increases with Age
51%
66%72%
38%
Hypertension defined as blood pressure >140/90 mmHg or treatment

6
Prospective Studies Collaboration. Lancet 2002;360:1903-1913
Usual Diastolic BP (mm Hg)Usual Systolic BP (mm Hg)
Isch
emic
Hea
rt D
isea
se M
orta
lity
(Flo
atin
g ab
solu
te r
isk)
50-59
60-69
70-79
80-89Age at Risk (Y)
40-49
256
128
64
32
16
8
4
2
1
0120 140 160 180
50-59
60-69
70-79
80-89
Age at Risk (Y)
40-49
256
128
64
32
16
8
4
2
1
080 90 100 11070
Blood Pressure: Lower is BetterBlood Pressure: Lower is Better
Isch
emic
Hea
rt D
isea
se M
orta
lity
(Flo
atin
g ab
solu
te r
isk)
Ischemic Heart Disease Mortality and Blood Pressure
BP=Blood pressure

7
Veterans Administration, 1967
Veterans Administration, 1970
Hypertension Stroke Study, 1974
USPHS Study, 1977
EWPHE Study, 1985
Coope and Warrender, 1986
SHEP Study, 1991
STOP-Hypertension Study, 1991
MRC Study, 1992
Syst-Eur Study, 1997
Total
0 0.5 1.0 1.5 2.0
0.79 (0.69 to 0.90)
He J et al. Am Heart J 1999;138:211-219
Better than placebo Worse than placebo
Blood Pressure: Risk of CHD with Active TreatmentBlood Pressure: Risk of CHD with Active Treatment
CHD=Coronary heart disease

8Abbott K et al. J Clin Pharmacology 2004;44:431-438
Trial (SBP Achieved)
1 1.5 2 2.5 3 3.5 4
AASK (127 mm Hg)
HOT (138 mm Hg)
MDRD (132 mm Hg)
ABCD (127 mm Hg)
UKPDS (144 mm Hg)
Number of BP Meds
UKPDS=UK Prospective Diabetes Study; ABCD=Appropriate Blood Pressure Control in Diabetes; MDRD=Modification of Dietary Protein in Renal Disease; HOT=Hypertension Optimal Treatment; AASK=African American Study of Kidney Disease and Hypertension
Blood Pressure: Number of Medications NeededBlood Pressure: Number of Medications Needed
9
Blood Pressure Evidence: Primary PreventionBlood Pressure Evidence: Primary Prevention
0 1 2 3 4 5 6 70
.04
.08
.12
.16
.20
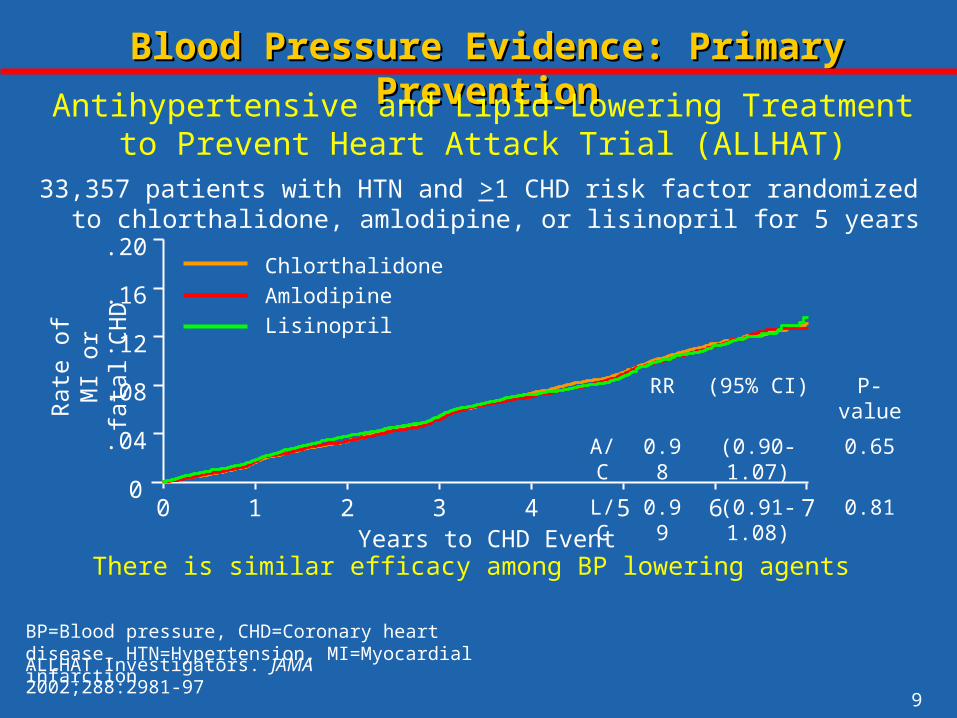
RR (95% CI) P-value
A/C 0.98 (0.90-1.07) 0.65
L/C 0.99 (0.91-1.08) 0.81
Rat
e of
MI
or
fata
l CH
DAntihypertensive and Lipid-Lowering Treatment to Prevent
Heart Attack Trial (ALLHAT)
ALLHAT Investigators. JAMA 2002;288:2981-97
Years to CHD Event
BP=Blood pressure, CHD=Coronary heart disease, HTN=Hypertension, MI=Myocardial infarction
Chlorthalidone
Amlodipine
Lisinopril
33,357 patients with HTN and >1 CHD risk factor randomized to chlorthalidone, amlodipine, or lisinopril for 5 years
There is similar efficacy among BP lowering agents

10
0 6 12 18 24 30 36 42 48 54 60 66
Study Month
4
8
12
16
0Pro
port
ion
with
CV
de
ath,
MI,
or s
trok
e (%
)
Blood Pressure Evidence: Primary PreventionBlood Pressure Evidence: Primary Prevention
Losartan Intervention for Endpoint (LIFE) Reduction in Hypertension Study
Dahlöf B et al. Lancet 2002;359:995-1003
AtenololLosartan
13% RRR, P=0.021
ARB=Angiotensin receptor blocker, CV=Cardiovascular, DBP=Diastolic blood pressure, LVH=Left ventricular hypertrophy, MI=Myocardial infarction, SBP=Systolic blood pressure
*Defined by SBP=160-200 mmHg or DBP=95-115 mmHg
9,193 high-risk hypertensive* patients with LVH randomized to losartan (100 mg) or atenolol (100 mg) for 5 years
An ARB provides greater efficacy in patients with LVH
11
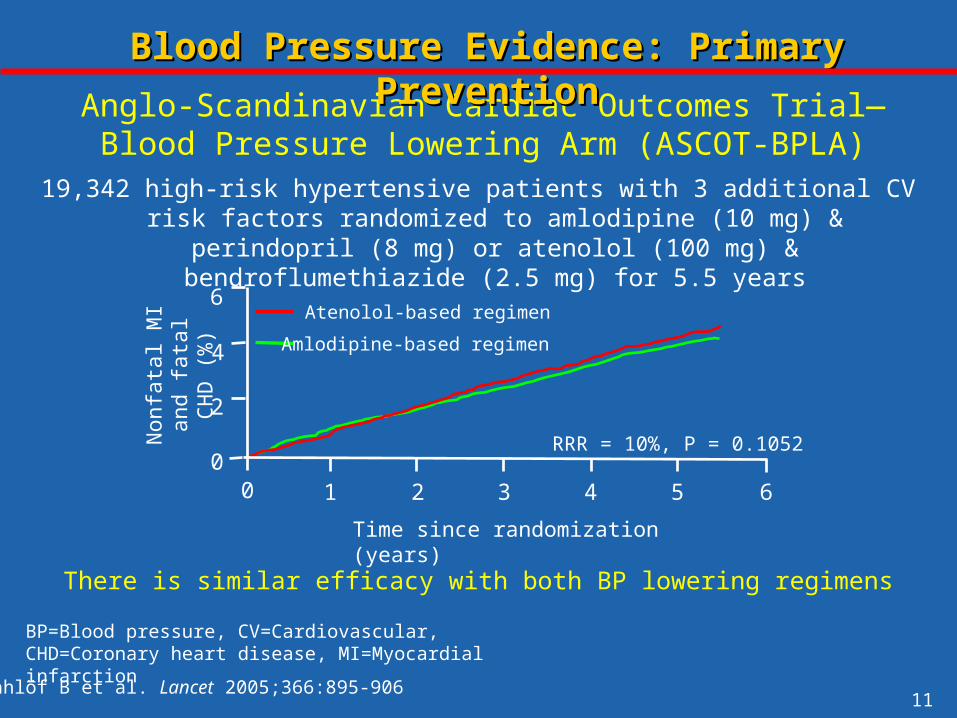
Anglo-Scandinavian Cardiac Outcomes Trial—Blood Pressure Lowering Arm (ASCOT-BPLA)
Blood Pressure Evidence: Primary PreventionBlood Pressure Evidence: Primary Prevention
Non
fata
l MI a
nd
fata
l CH
D (
%) 6
2
4
01 2 3 4 5 60
Time since randomization (years)
RRR = 10%, P = 0.1052
Atenolol-based regimen
Amlodipine-based regimen
Dahlöf B et al. Lancet 2005;366:895-906
BP=Blood pressure, CV=Cardiovascular, CHD=Coronary heart disease, MI=Myocardial infarction
19,342 high-risk hypertensive patients with 3 additional CV risk factors randomized to amlodipine (10 mg) & perindopril (8 mg) or atenolol (100
mg) & bendroflumethiazide (2.5 mg) for 5.5 years
There is similar efficacy with both BP lowering regimens

12
22,576 patients with HTN and CAD randomized to a BP lowering strategy with verapamil SR (240 mg) or atenolol (50 mg) for 2.7 years
There is comparable efficacy with a CAS or NCAS
0
5
10
15
20
25
0 6 12 18 24 36 48 5442 6030
Blood Pressure Evidence: Secondary PreventionBlood Pressure Evidence: Secondary Prevention
International Verapamil-Trandolapril Study (INVEST)
Months
RR=0.98, P=0.57
Calcium antagonist strategy (CAS)*Non-calcium antagonist strategy (NCAS)*
Pepine CJ et al. JAMA 2003;290:2805-2816
*Trandolapril (up to 4 mg) was added in those with DM, chronic kidney disease, or heart failure.
Inci
denc
e of
dea
th, M
I, or
str
oke
BP=Blood pressure, DM=Diabetes mellitus, HTN=Hypertension, MI=Myocardial infarction

13
Favors valsartan Favors amlodipine
Primary cardiac composite endpointCardiac mortalityCardiac morbidity
All myocardial infarctionAll congestive heart failureAll strokeAll-cause deathNew-onset diabetes
0.5 1 2
Blood Pressure Evidence: Secondary PreventionBlood Pressure Evidence: Secondary Prevention
Valsartan Antihypertensive Long-Term Use Evaluation (VALUE) Trial
Julius S et al. Lancet 2004;363:2022-2031
ARBS=Angiotensin receptor blocker, CCB=Calcium channel blocker, CV=Cardiovascular
15,245 patients with untreated HTN and high CV risk randomized to a BP lowering strategy with valsartan (160 mg) or amlodipine (10 mg) for 4.2 years
There is similar efficacy with an ARB and CCB
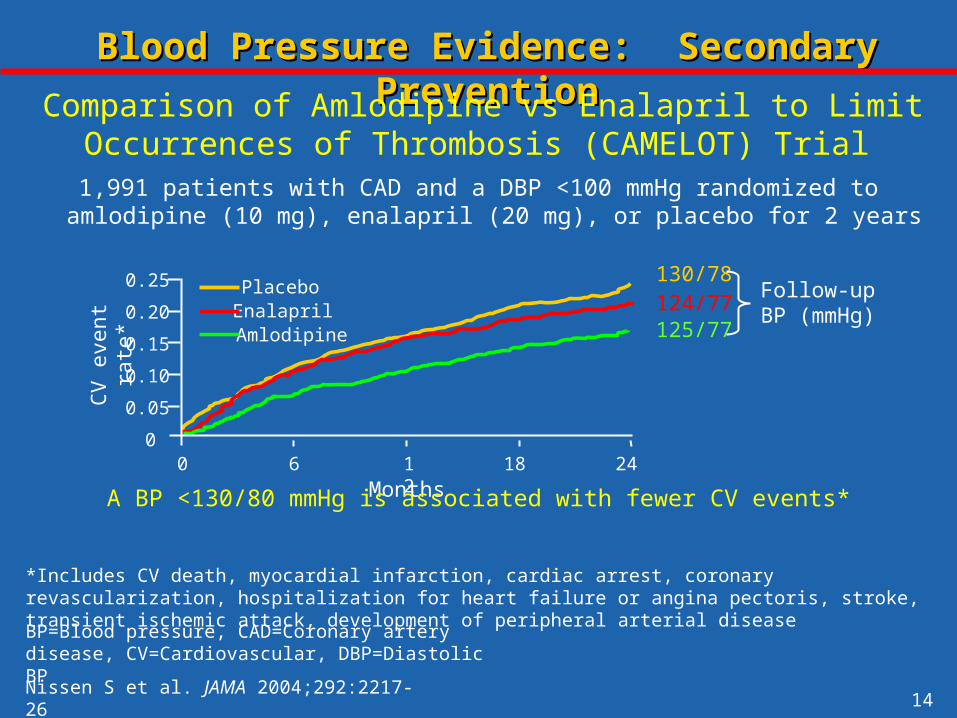
14Nissen S et al. JAMA 2004;292:2217-26
Blood Pressure Evidence: Secondary PreventionBlood Pressure Evidence: Secondary Prevention
Comparison of Amlodipine vs Enalapril to Limit Occurrences of Thrombosis (CAMELOT) Trial
*Includes CV death, myocardial infarction, cardiac arrest, coronary revascularization, hospitalization for heart failure or angina pectoris, stroke, transient ischemic attack, development of peripheral arterial disease
CV
eve
nt r
ate*
0
0.25
0.20
0.10
0.05
6 12 18 24
0.15
0
Placebo
AmlodipineEnalapril
Months
Follow-up BP (mmHg)
125/77124/77130/78
BP=Blood pressure, CAD=Coronary artery disease, CV=Cardiovascular, DBP=Diastolic BP
1,991 patients with CAD and a DBP <100 mmHg randomized to amlodipine (10 mg), enalapril (20 mg), or placebo for 2 years
A BP <130/80 mmHg is associated with fewer CV events*
15
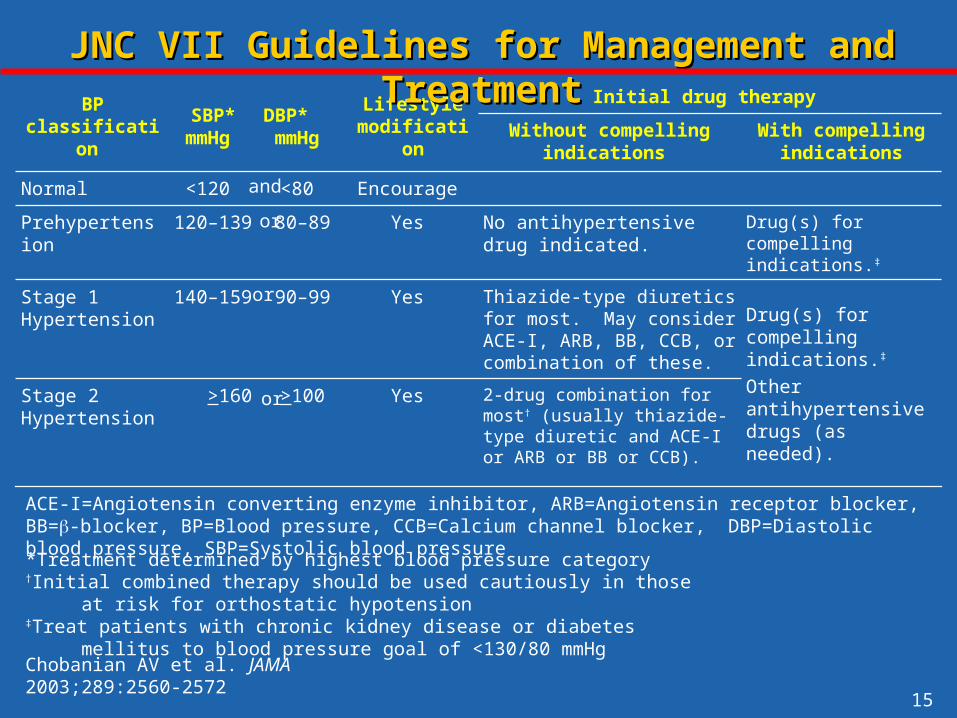
2-drug combination for most† (usually thiazide-type diuretic and ACE-I or ARB or BB or CCB).
Yes >100 >160 Stage 2 Hypertension
Drug(s) for compelling indications.‡
Other antihypertensive drugs (as needed).
Thiazide-type diuretics for most. May consider ACE-I, ARB, BB, CCB, or combination of these.
Yes 90–99 140–159 Stage 1 Hypertension
Drug(s) for compelling indications.‡
No antihypertensive drug indicated.
Yes 80–89 120–139 Prehypertension
Encourage <80 <120 Normal
With compelling indications
Without compelling indications
Initial drug therapy Lifestyle
modificationDBP* mmHg
SBP* mmHg
BP classification
JNC VII Guidelines for Management and TreatmentJNC VII Guidelines for Management and Treatment
and
or
or
or
Chobanian AV et al. JAMA 2003;289:2560-2572
ACE-I=Angiotensin converting enzyme inhibitor, ARB=Angiotensin receptor blocker, BB=-blocker, BP=Blood pressure, CCB=Calcium channel blocker, DBP=Diastolic blood pressure, SBP=Systolic blood pressure
*Treatment determined by highest blood pressure category†Initial combined therapy should be used cautiously in those at risk for orthostatic hypotension‡Treat patients with chronic kidney disease or diabetes mellitus to blood pressure goal of <130/80 mmHg

16
Modification Recommendation Approximate SBP Reduction Range
Weight reduction Maintain normal body weight (BMI=18.5-25)
5-20 mmHg/10 kg weight lost
DASH eating plan
Diet rich in fruits, vegetables, low fat dairy and reduced in fat
8-14 mmHg
Restrict sodium intake
<2.4 grams of sodium per day 2-8 mmHg
Physical activity Regular aerobic exercise for at least 30 minutes most days of the week
4-10 mmHg
Moderate alcohol <2 drinks/day for men and <1 drink/day for women
2-4 mmHg
JNC VII Lifestyle Modifications for BP ControlJNC VII Lifestyle Modifications for BP Control
Chobanian AV et al. JAMA 2003;289:2560-2572
BMI=Body mass index, SBP=Systolic blood pressure
17
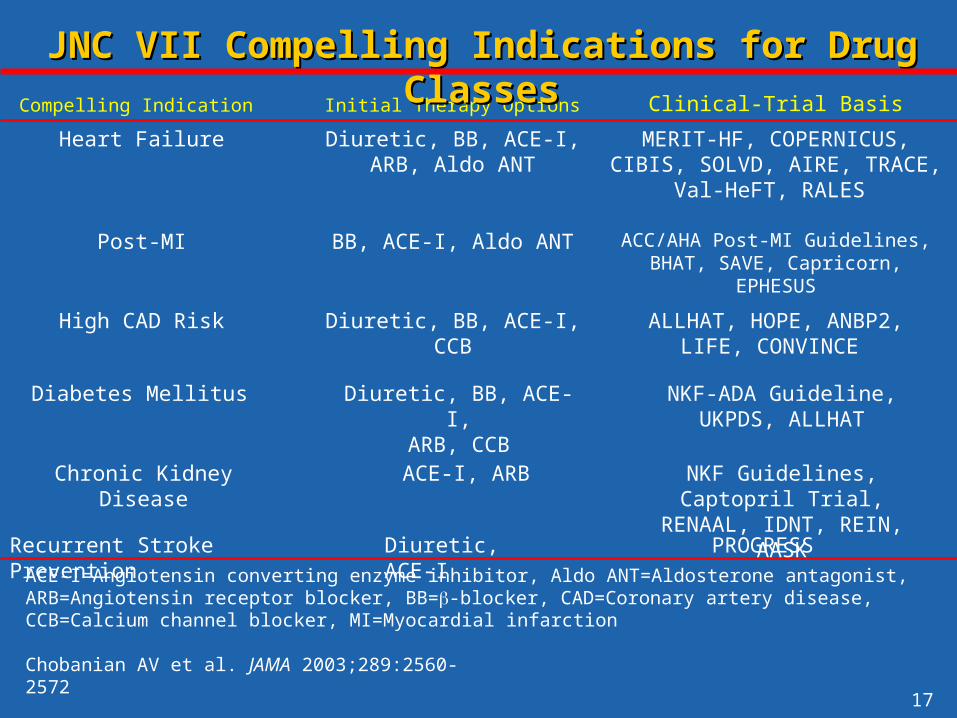
Clinical-Trial BasisCompelling Indication
ALLHAT, HOPE, ANBP2,LIFE, CONVINCE
High CAD Risk
ACC/AHA Post-MI Guidelines, BHAT, SAVE, Capricorn, EPHESUS
Post-MI
MERIT-HF, COPERNICUS, CIBIS, SOLVD, AIRE, TRACE, Val-HeFT,
RALES
Initial Therapy Options
Diuretic, BB, ACE-I, CCB
BB, ACE-I, Aldo ANT
Diuretic, BB, ACE-I,ARB, Aldo ANT
Heart Failure
JNC VII Compelling Indications for Drug ClassesJNC VII Compelling Indications for Drug Classes
Recurrent Stroke Prevention PROGRESSDiuretic, ACE-I
NKF-ADA Guideline,UKPDS, ALLHAT
NKF Guidelines, Captopril Trial, RENAAL, IDNT, REIN, AASK
Diuretic, BB, ACE-I,ARB, CCB
ACE-I, ARB
Diabetes Mellitus
Chronic Kidney Disease
Chobanian AV et al. JAMA 2003;289:2560-2572
ACE-I=Angiotensin converting enzyme inhibitor, Aldo ANT=Aldosterone antagonist, ARB=Angiotensin receptor blocker, BB=-blocker, CAD=Coronary artery disease, CCB=Calcium channel blocker, MI=Myocardial infarction

18
Optimize dosages or add additional drugs until goal BP is achieved.Consider consultation with hypertension specialist.
Lifestyle modifications
Initial drug choices
Not at goal BP
Not at goal BP (<140/90 mm Hg)(<130/80 mm Hg for those with diabetes mellitus
or chronic kidney disease)
WITH compelling indicationsWITHOUT compelling indications
Stage 1 hypertension(SBP 140–159 mm Hg or DBP 90–99 mm Hg):
Thiazide-type diuretic for most.May consider ACEI, ARB, BB, CCB, or combo.
Stage 2 hypertension(SBP 160 or DBP 100 mm Hg):
Two-drug combination for most (usually thiazide-type diuretic and
ACEI or ARB or BB or CCB).
Drugs for compelling indications:Other antihypertensive drugs
(diuretic, ACEI, ARB, BB, CCB)as needed.
JNC VII Blood Pressure Treatment AlgorithmJNC VII Blood Pressure Treatment Algorithm
Chobanian AV et al. JAMA 2003;289:2560-2572
BP=Blood pressure, DBP=Diastolic blood pressure, SBP=Systolic blood pressure

19
Blood Pressure RecommendationsBlood Pressure Recommendations
Initiation or maintenance of lifestyle modification in those with BP >120/80 mmHg.
A target BP of <130/80mmHg for individuals with any of the following: DM, chronic renal disease, CAD or CAD risk equivalents, carotid artery disease, peripheral artery disease, abdominal aortic aneurysm, those with a Framingham risk score >10% and a goal of <140/90mmHg for individuals with none of the above.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
*A BP >130/80 mmHg should be used for individuals with CKD or DM
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII

20
Blood Pressure RecommendationsBlood Pressure Recommendations
ACE-I, ARB, CCB or thiazide diuretic as first line therapy, supplement with a second agent if BP goal is not achieved with monotherapy. A beta blocker is a more appropriate choice for post-MI or angina pectoris patients.
ACE=Angiotensin converting enzyme, BP=Blood pressure, CKD=Chronic kidney disease, DM=Diabetes mellitus
*A BP >130/80 mmHg should be used for individuals with CKD or DM
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII

21
Angiotensin Converting Enzyme Inhibitor Angiotensin Converting Enzyme Inhibitor Evidence and GuidelinesEvidence and Guidelines

22
ACE Inhibitor: Mechanism of ActionACE Inhibitor: Mechanism of Action
Angiotensin II
Kininase II
Angiotensin I
Angiotensinogen
InhibitorACE
ReninBradykinin
Inactive Fragments
SympatheticVasopressin
AldosteroneVasoconstriction
ACE=Angiotensin converting enzyme
Kininogen
Kallikrein
VasodilationProstaglandins
tPA

23
Days of Follow-Up
CV
dea
th, M
I, or
st
roke
(%
)
22% RRR, P<0.0010.00
0.05
0.10
0.15
0.20
0 500 1000 1500
ACE Inhibitor Evidence: Secondary PreventionACE Inhibitor Evidence: Secondary Prevention
Placebo
Ramipril
HOPE Investigators. NEJM 2000;342:145-153
Heart Outcomes Prevention and Evaluation (HOPE) Study
ACE-I=Angiotensin converting enzyme inhibitors, DM=Diabetes mellitus, CV=Cardiovascular, HF=Heart failure, LVSD=Left ventricular systolic dysfunction, MI=Myocardial infarction
9,297 patients with DM or vascular disease plus an additional CV risk factor, but without HF or known LVSD randomized to ramipril (10 mg) or placebo
for 5 years
ACE-I reduce CV events in high-risk individuals
24
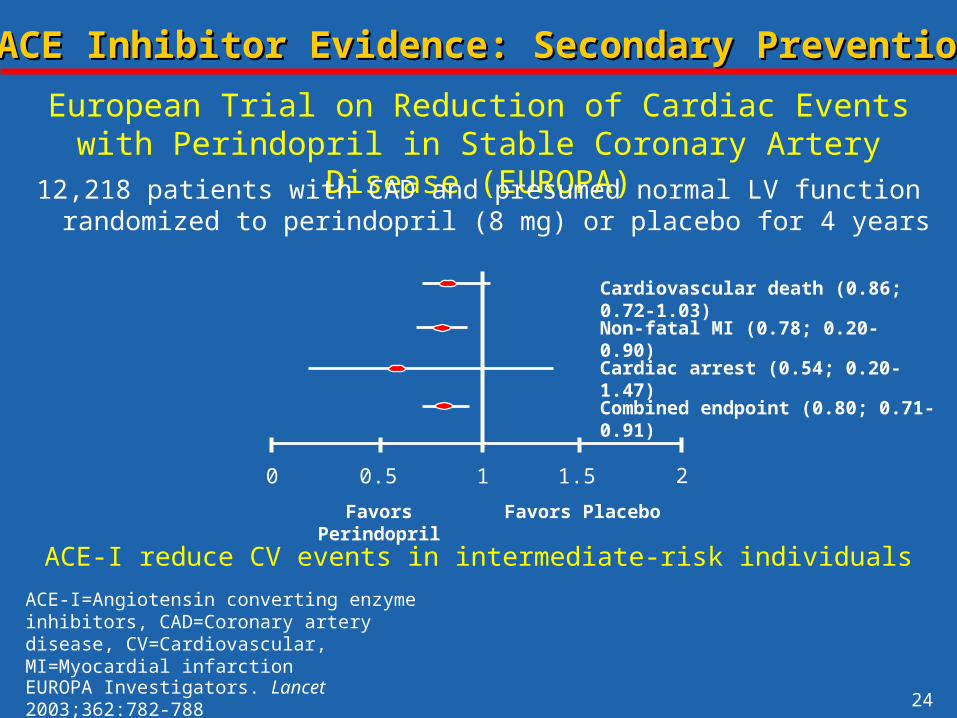
0 0.5 1 1.5 2
Cardiovascular death (0.86; 0.72-1.03)Non-fatal MI (0.78; 0.20-0.90)
Cardiac arrest (0.54; 0.20-1.47)
Combined endpoint (0.80; 0.71-0.91)
ACE Inhibitor Evidence: Secondary PreventionACE Inhibitor Evidence: Secondary Prevention
European Trial on Reduction of Cardiac Events with Perindopril in Stable Coronary Artery Disease (EUROPA)
Favors Perindopril Favors Placebo
EUROPA Investigators. Lancet 2003;362:782-788
12,218 patients with CAD and presumed normal LV function randomized to perindopril (8 mg) or placebo for 4 years
ACE-I reduce CV events in intermediate-risk individualsACE-I=Angiotensin converting enzyme inhibitors, CAD=Coronary artery disease, CV=Cardiovascular, MI=Myocardial infarction
25
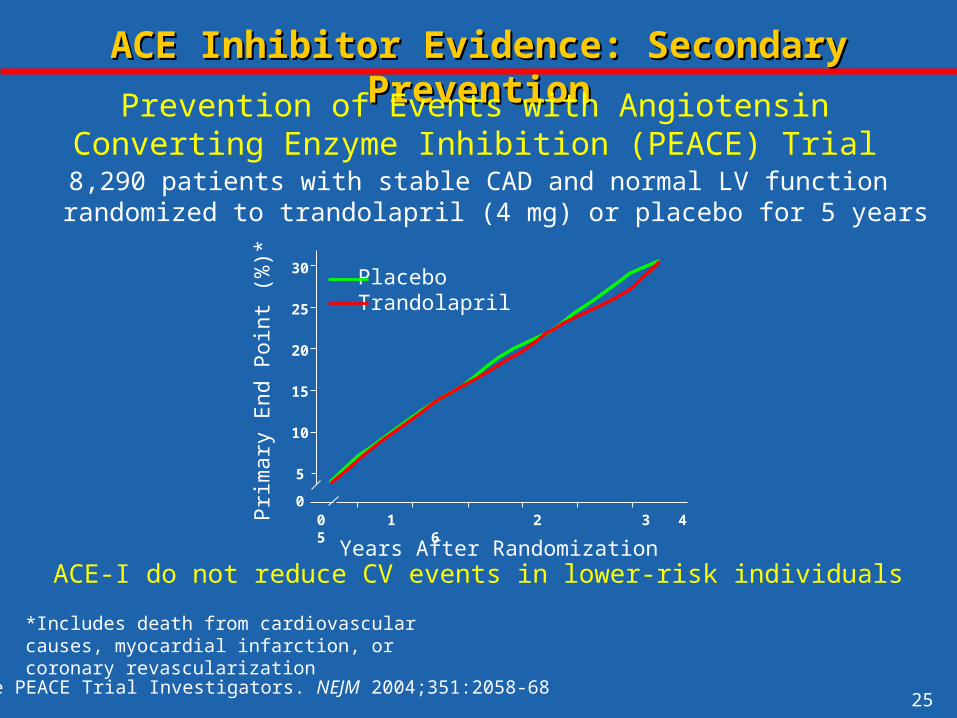
ACE Inhibitor Evidence: Secondary PreventionACE Inhibitor Evidence: Secondary Prevention
Prevention of Events with Angiotensin Converting Enzyme Inhibition (PEACE) Trial
Prim
ary
End
Poi
nt (
%)*
30
25
20
15
10
5
00 1 2 3 4 5 6
Years After Randomization
PlaceboTrandolapril
The PEACE Trial Investigators. NEJM 2004;351:2058-68
*Includes death from cardiovascular causes, myocardial infarction, or coronary revascularization
8,290 patients with stable CAD and normal LV function randomized to trandolapril (4 mg) or placebo for 5 years
ACE-I do not reduce CV events in lower-risk individuals
26
0
5
10
15
20
0 1 2 3 4 5
HOPE, placebo
HOPE, active drug (ramipril)
PEACE, placebo
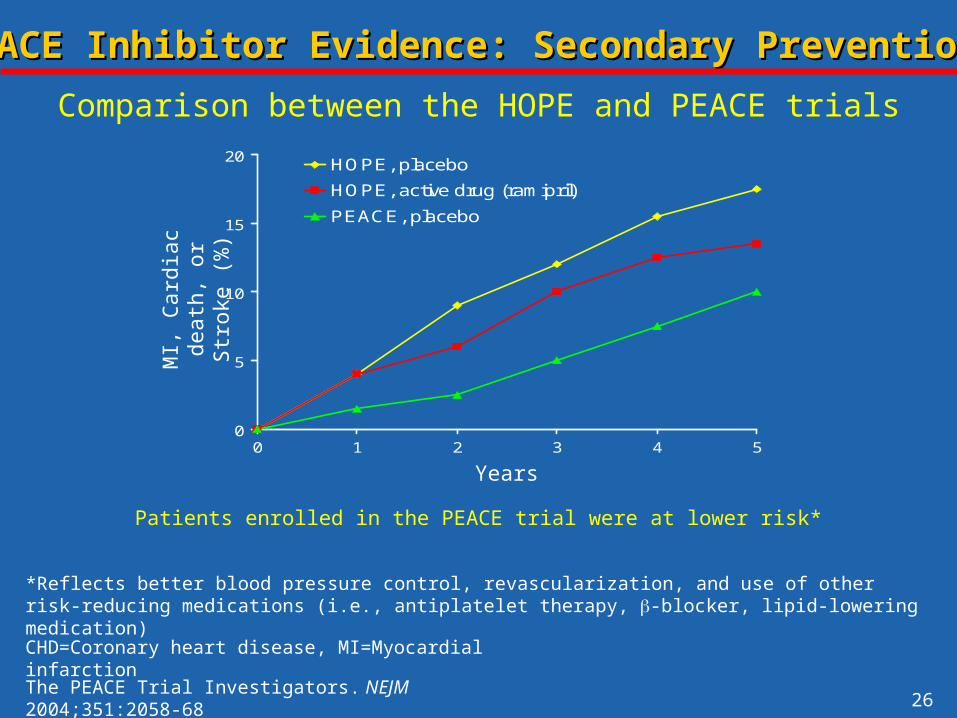
ACE Inhibitor Evidence: Secondary PreventionACE Inhibitor Evidence: Secondary Prevention
Comparison between the HOPE and PEACE trials
Patients enrolled in the PEACE trial were at lower risk*
MI,
Car
diac
dea
th,
or S
trok
e (%
)
The PEACE Trial Investigators. NEJM 2004;351:2058-68
CHD=Coronary heart disease, MI=Myocardial infarction
*Reflects better blood pressure control, revascularization, and use of other risk-reducing medications (i.e., antiplatelet therapy, -blocker, lipid-lowering medication)
Years
27
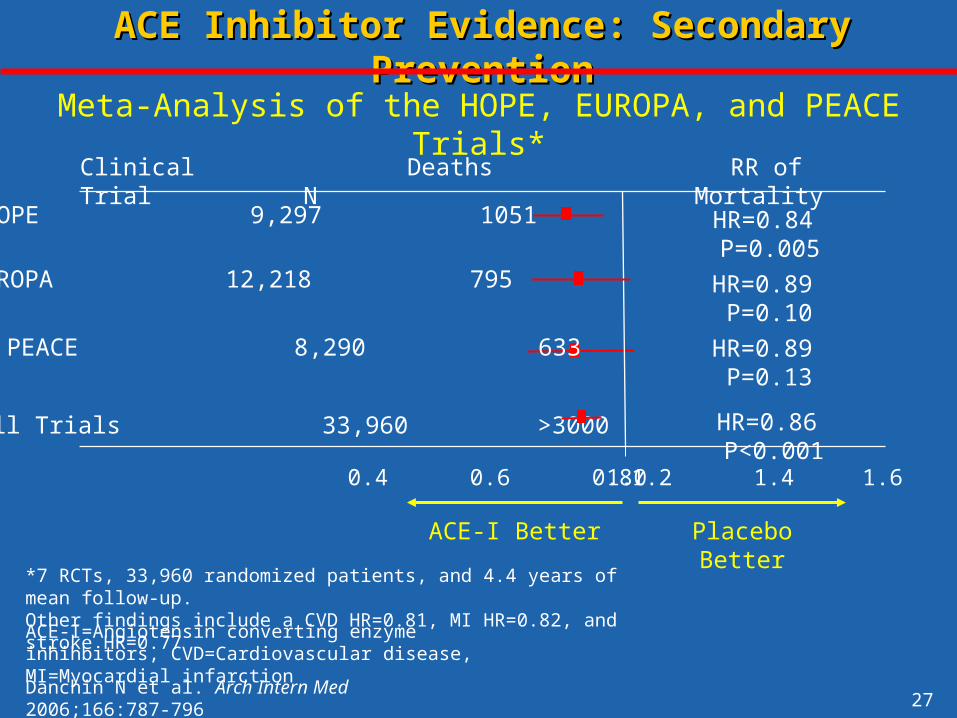
Clinical Trial
HOPE 9,297 1051
0.4 0.6 0.8 1.0 1.2 1.4 1.6
N
ACE-I Better Placebo Better
ACE Inhibitor Evidence: Secondary PreventionACE Inhibitor Evidence: Secondary Prevention
EUROPA 12,218 795
PEACE 8,290 633 HR=0.89 P=0.13
HR=0.89 P=0.10
HR=0.84 P=0.005
Deaths
All Trials 33,960 >3000 HR=0.86 P<0.001
Danchin N et al. Arch Intern Med 2006;166:787-796
Meta-Analysis of the HOPE, EUROPA, and PEACE Trials*
RR of Mortality
*7 RCTs, 33,960 randomized patients, and 4.4 years of mean follow-up. Other findings include a CVD HR=0.81, MI HR=0.82, and stroke HR=0.77
ACE-I=Angiotensin converting enzyme inhihbitors, CVD=Cardiovascular disease, MI=Myocardial infarction

28
Years
Pro
babi
lity
of E
vent
0
0.05
0.15
0.2
0.25
0.3
0 1 2 3
0.35
0.4
4
ACE-I
Placebo
OR 0.74 (0.66–0.83)OR 0.74 (0.66–0.83)0.1
Flather MD et al. Lancet 2000;355:1575–1581
SAVERadionuclid
eEF <40%
AIREClinical and/or radiographic signs of HF
TRACEEchocardiogram
EF <35%
ACE Inhibitor Evidence: Secondary PreventionACE Inhibitor Evidence: Secondary Prevention
ACE-I=Angiotensin converting enzyme inhibitors, EF=Ejection fraction, LVSD=Left ventricular systolic dysfunction, MI=Myocardial infarction, OR=Odds ratio
ACE-I provide substantial benefit in post-MI LVSD

29
ACE Inhibitor RecommendationsACE Inhibitor Recommendations
An ACE inhibitor in those following a MI, regardless of EF or in those with CAD* along with hypertension (SBP >120 mmHg), LVSD (EF <0.40), heart failure, DM, or CKD
Optional use of an ACE inhibitor in those with low risk CAD*, well controlled risk factors, normal EF, and successful revascularization
Secondary Prevention
*Defined by previous MI or angiographically significant CAD
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
ACE=Angiotensin converting enzyme, CAD=Coronary artery disease, CKD=Chronic kidney disease, CV=Cardiovascular, DM=Diabetes mellitus, EF=Ejection fraction, LVSD=Left ventricular systolic dysfunction, MI=Myocardial infarction, SBP=Systolic blood pressure

30
Angiotensin Receptor Blocker Evidence Angiotensin Receptor Blocker Evidence and Guidelinesand Guidelines

31
Receptors
Angiotensin Receptor Blocker: Mechanism of ActionAngiotensin Receptor Blocker: Mechanism of Action
AT II Receptor Blocker
Antiproliferative Action
VasodilationProliferative Action
Vasoconstriction
ATIIATI
Angiotensinogen
Other Pathways
Renin
AT I Receptor
Blocker
Angiotensin I
Angiotensin IIACE

32
2,028 patients with symptomatic HF, LVSD (EF <40%), and intolerance to ACE-I randomized to candesartan (32 mg) or placebo for 34 months
ARB reduce CV events in those intolerant of ACE-I
0 1 2 3Years
50
HR 0.77 p=0.00040
40
30
20
10
Candesartan
Placebo
ARB Evidence: Secondary PreventionARB Evidence: Secondary Prevention
Candesartan in Heart Failure Assessment of Reduction in Mortality and Morbidity (CHARM) Alternative Trial
Granger CB et al. Lancet 2003;362:772-777
ACE-I=Angiotensin converting enzyme inhibitors, ARB=Angiotensin receptor blockers, EF=Ejection fraction, HF=Heart failure, LVSD=Left ventricular systolic dysfunction
CV
Dea
th o
r H
ospi
taliz
atio
n fo
r H
F

33
ARB Evidence: Secondary PreventionARB Evidence: Secondary Prevention
Pfeffer M et al. NEJM 2003;349:1893-1906
Valsartan in Acute Myocardial Infarction Trial (VALIANT)
0.0
0.1
0.2
0.3
0.4
0 6 12 18 24 30 36
Valsartan
Valsartan and Captopril
Captopril
All
Cau
se M
orta
lity
Months
Valsartan vs. Captopril: HR = 1.00; P = 0.982
Valsartan + Captopril vs. Captopril: HR = 0.98; P = 0.726
ACE-I=Angiotensin converting enzyme inhibitors, ARB=Angiotensin receptor blockers, EF=Ejection fraction, LVSD=Left ventricular systolic dysfunction
14,703 patients with post-MI HF or LVSD (EF <0.40) randomized to captopril (50 mg tid), valsartan (160 mg bid), or captopril (50 mg tid) plus valsartan
(80 mg bid) for 2 years
ARB provide similar efficacy to ACE-I in Post-MI LVSD

34
0 1 2 3
0
10
20
30
40
50
ARB Evidence: Secondary PreventionARB Evidence: Secondary Prevention
HR 0.85, p=0.011
Candesartan
Placebo
CV
Dea
th o
r H
ospi
taliz
atio
n fo
r H
F
Years
Candesartan in Heart Failure Assessment of Reduction in Mortality and Morbidity (CHARM) Added Trial
ACE-I=Angiotensin converting enzyme inhibitors, ARB=Angiotensin receptor blockers, EF=Ejection fraction, HF=Heart failure, LVSD=Left ventricular systolic dysfunction, RAS=Renin angiotensin system
McMurray JJ et al. Lancet 2003;362:767-71
2,548 patients with symptomatic HF and LVSD (EF <40%) randomized to candesartan (32 mg) or placebo in addition to an ACE-I for 34 months
Chronic dual RAS blockade provides additional benefit
35
Angiotensin Receptor Blocker RecommendationsAngiotensin Receptor Blocker Recommendations
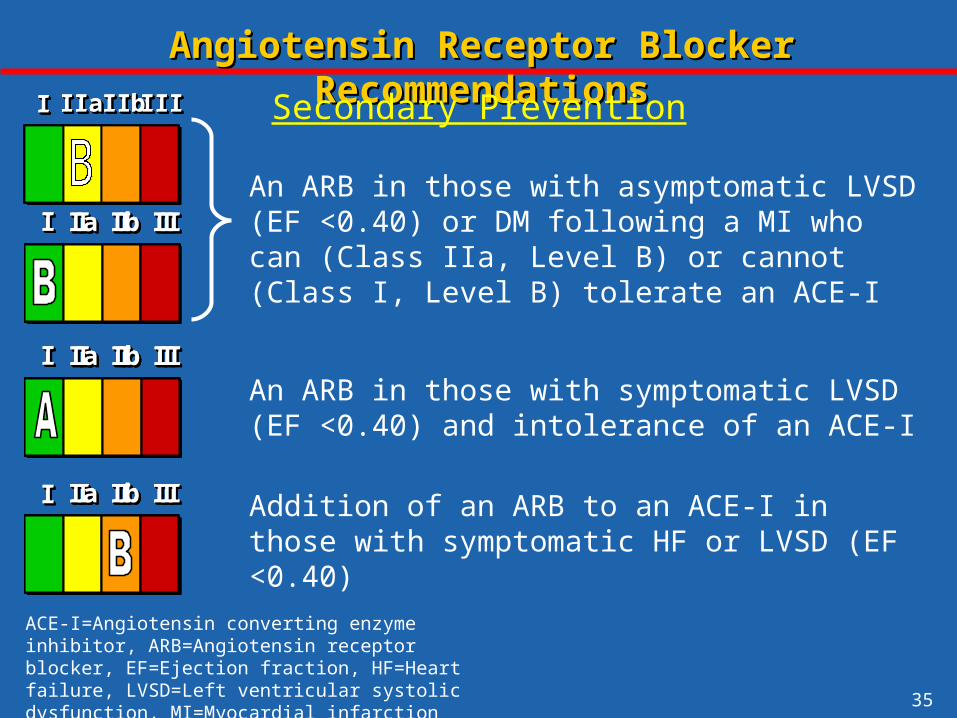
Secondary Prevention
An ARB in those with asymptomatic LVSD (EF <0.40) or DM following a MI who can (Class IIa, Level B) or cannot (Class I, Level B) tolerate an ACE-I
An ARB in those with symptomatic LVSD (EF <0.40) and intolerance of an ACE-I
Addition of an ARB to an ACE-I in those with symptomatic HF or LVSD (EF <0.40)
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
ACE-I=Angiotensin converting enzyme inhibitor, ARB=Angiotensin receptor blocker, EF=Ejection fraction, HF=Heart failure, LVSD=Left ventricular systolic dysfunction, MI=Myocardial infarction
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII

36
-blocker Evidence and Guidelines-blocker Evidence and Guidelines

37
Parasympathetic Nerve Terminal
Sympathetic Cholinergic Nerve Terminal
1
M2
M2
M2
1 2
2
2
1 2
2 2
NE
ACh
-blocker: Targets and Receptor Selectivity-blocker: Targets and Receptor Selectivity
Sympathetic Nerve Terminal
+++
_
NE NE_ +
_ _
Heart Blood Vessel
Inotropy
Chronotropy
Dromotropy
Vasoconstriction
Vasoconstriction
Vasodilation
Vasodilation
1 selective blocker
non-selective blocker
non-selective blocker with 1 blocking activity
=Alpha receptor, Ach=Acetylcholine, =Beta receptor, M=Muscarinic receptor, NE=Norepinephrine
Klabunde, RE (ed) Cardiovascular Physiology Concepts LWW 2001
38
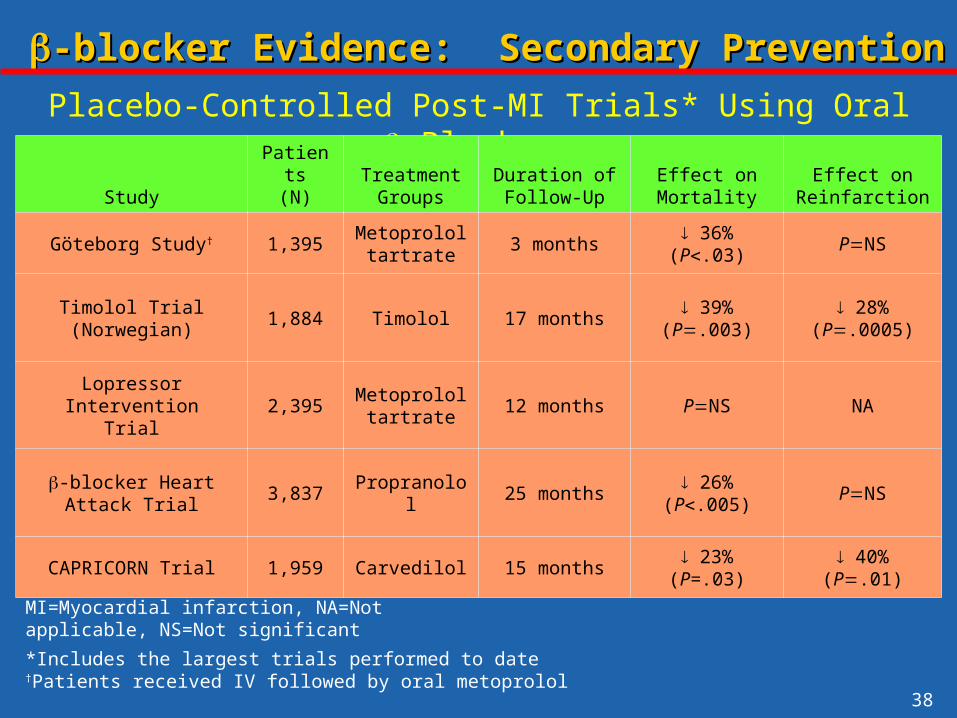
-blocker Evidence: Secondary Prevention-blocker Evidence: Secondary Prevention
Placebo-Controlled Post-MI Trials* Using Oral -Blockers
StudyPatients
(N)Treatment
GroupsDuration of Follow-Up
Effect on Mortality
Effect on Reinfarction
Göteborg Study† 1,395Metoprolol
tartrate3 months
36%(P.03)
PNS
Timolol Trial(Norwegian)
1,884 Timolol 17 months 39%
(P.003) 28%
(P.0005)
Lopressor InterventionTrial
2,395Metoprolol
tartrate12 months PNS NA
-blocker Heart Attack Trial
3,837 Propranolol 25 months 26%
(P.005)PNS
CAPRICORN Trial 1,959 Carvedilol 15 months 23%
(P=.03) 40%
(P.01)
*Includes the largest trials performed to date†Patients received IV followed by oral metoprolol
MI=Myocardial infarction, NA=Not applicable, NS=Not significant

39
Study DrugHF
SeverityPatients
(n)Follow-up
(years)Mean
Dosage Effects on Outcomes
CIBIS Bisoprolol* Moderate-Severe
641 1.9 3.8 mg/day
All cause mortality (p=NS)
CIBIS-II Bisoprolol* Moderate-Severe
2,647 1.3 7.5mg/day
All cause mortality34% (P<0.0001)
BEST Bucindolol* Moderate-Severe
2,708 2.0 152mg/day
All cause mortality (p=NS)
MERIT-HF Metoprolol succinate#
Mild-Moderate
3,991 1.0 159mg/day
All cause mortality34% (P=0.0062)
MDC Metoprolol tartrate*
Mild-Moderate
383 1.0 108mg/day
Death or Need for TX (P=NS)
CAPRICORN Carvedilol Mild 1,989 1.3 40mg/day
All cause mortality 23% (P =0.03)
US Carvedilol Carvedilol Mild-Moderate
1,094 0.5 45mg/day
All-cause mortality†65% (P=.0001)
COPERNICUS Carvedilol Severe 2,289 0.9 37mg/day
All-cause mortality35% (P =0.0014)
-blocker Evidence: Benefit in HF and/or LVSD-blocker Evidence: Benefit in HF and/or LVSD
*Not an approved indication†Not a planned end point. #Not approved for severe HF or mortality reduction alone
HF=Heart failure, LVSD=Left ventricular systolic dysfunction, NS=Not significant, TX=Transplant

40
Phase of Treatment
Acute treatment
Secondaryprevention
Overall
Total #Patients
28,970
24,298
53,268
0.5 1.0 2.0RR of death
-blockerbetter
RR (95% CI)
Placebobetter
0.87 (0.77-0.98)
0.77 (0.70-0.84)
0.81 (0.75-0.87)
-blocker Evidence: Secondary Prevention-blocker Evidence: Secondary Prevention
Antman E, Braunwald E. Acute Myocardial Infarction. In: Braunwald E, Zipes DP, Libby P, eds. Heart Disease: A textbook of Cardiovascular Medicine, 6th ed., Philadelphia, PA: W.B. Sanders, 2001, 1168.
Summary of Secondary Prevention Trials of -blocker Therapy
CI=Confidence interval, RR=Relative risk

41
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII -blocker in all patients following MI or ACS
-blocker in all patients with LVSD
-blocker in those with other forms of CV disease or DM, unless contraindicated
*Relative contraindications include asthma, chronic obstructive pulmonary disease, insulin dependent diabetes mellitus, severe peripheral arterial disease, and a PR interval >0.24 seconds
ACS=Acute coronary syndrome, CV=Cardiovascular, DM=Diabetes mellitus, LVSD=Left ventricular systolic dysfunction, MI=Myocardial infarction
-blocker Recommendations*-blocker Recommendations*
Secondary Prevention
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII