بسم اللّه الرحمن الرحیم. infectious spondilodiscitis
TRANSCRIPT

ه الرحمن ه الرحمن بسم الّل بسم الّلالرحیمالرحیم
INFECTIOUSINFECTIOUSSPONDILODISCISPONDILODISCI
TISTIS

DefinitionDefinition
Infection of Infection of intervertebral intervertebral discdisc
and adjacent and adjacent vertebraevertebrae
Microbial AgentsMicrobial Agents
Pyogens (Pyogens (Staph -E coli) Staph -E coli) AcuteAcute
Brucella- Salmonella Brucella- Salmonella SubacuteSubacute
Tuberculosis Tuberculosis ChronicChronic

PATHOGENESISPATHOGENESIS

Hematogenous
Direct inoculation
Adjacent tissue
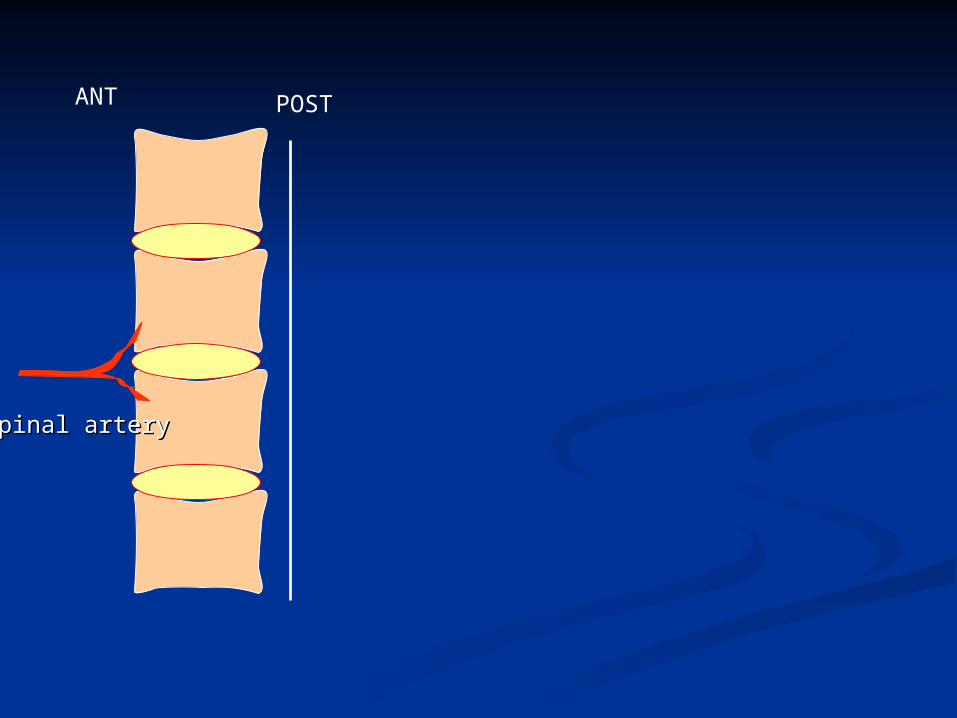
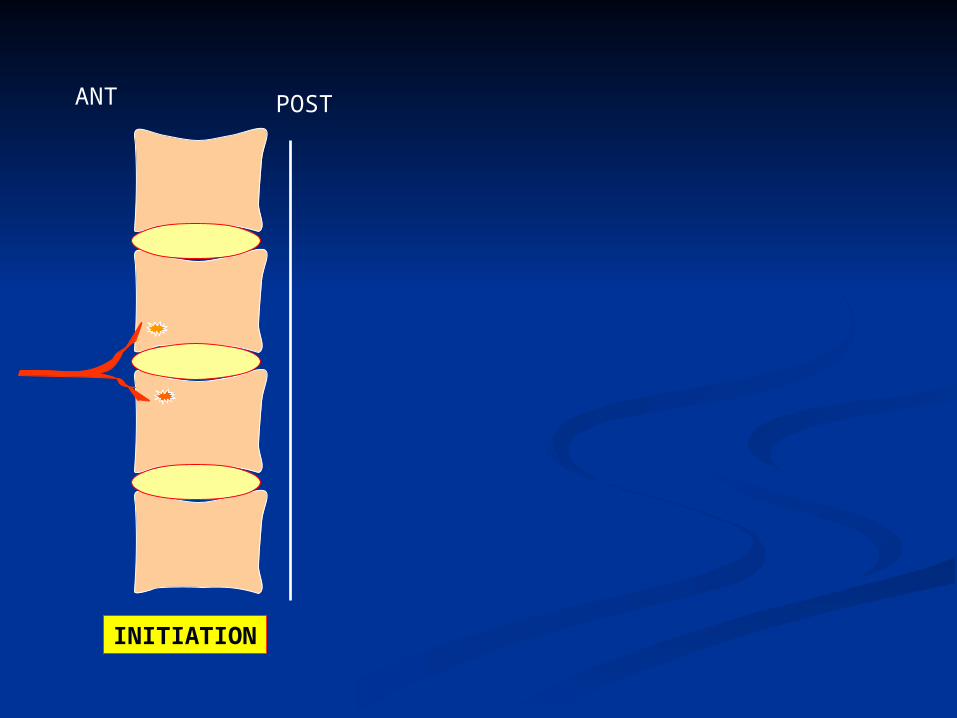
ANT POST
Spinal arterySpinal artery
ANT POST
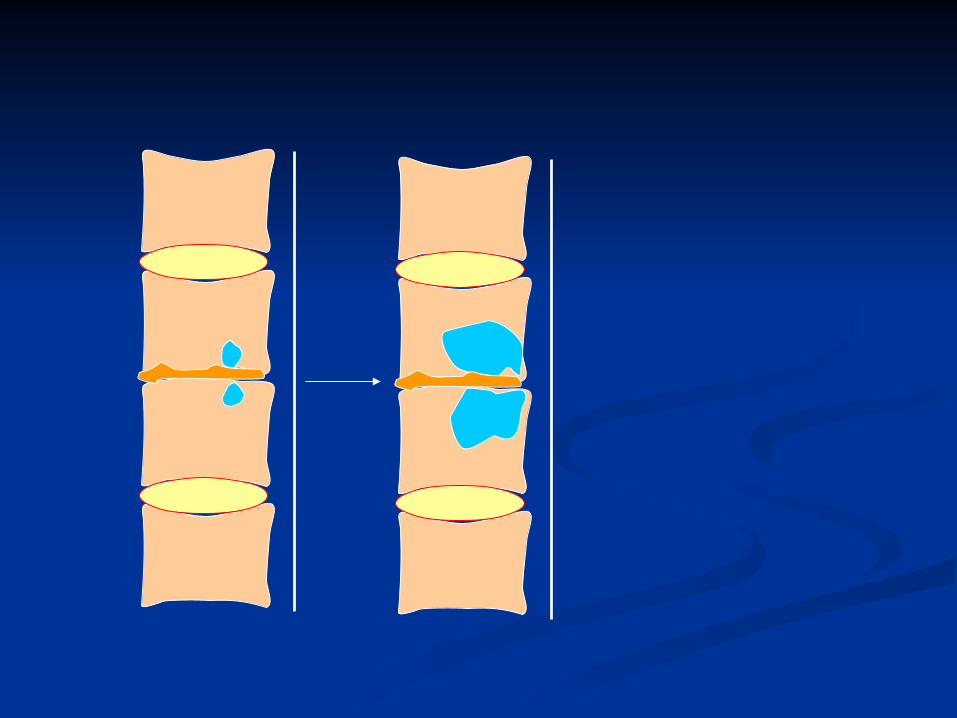
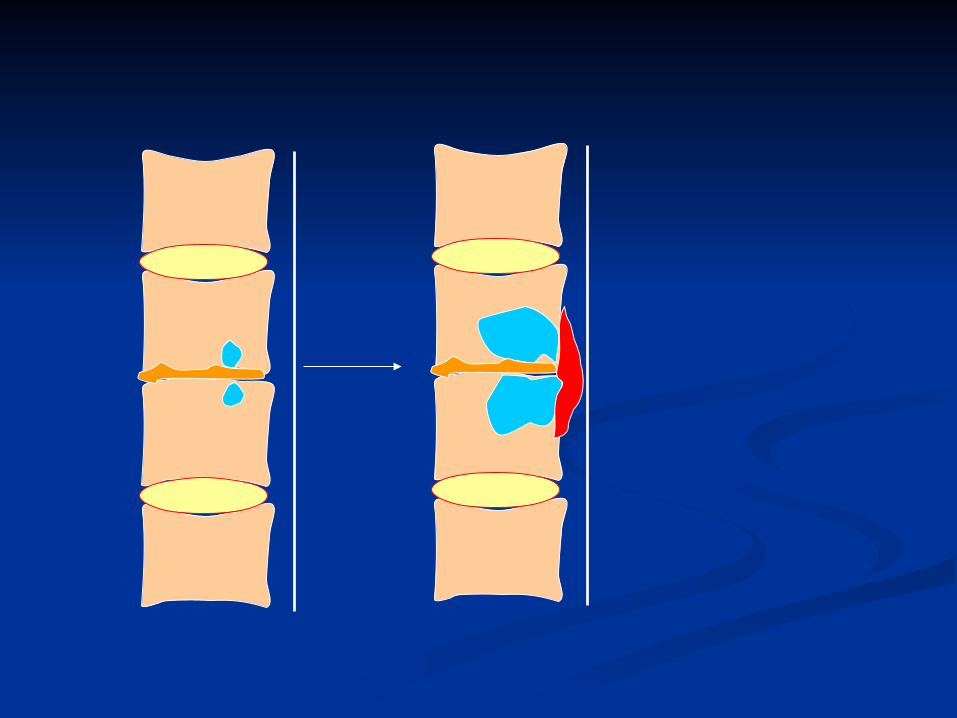
INITIATION

ANT POST
INITIATION DESTRUCTION
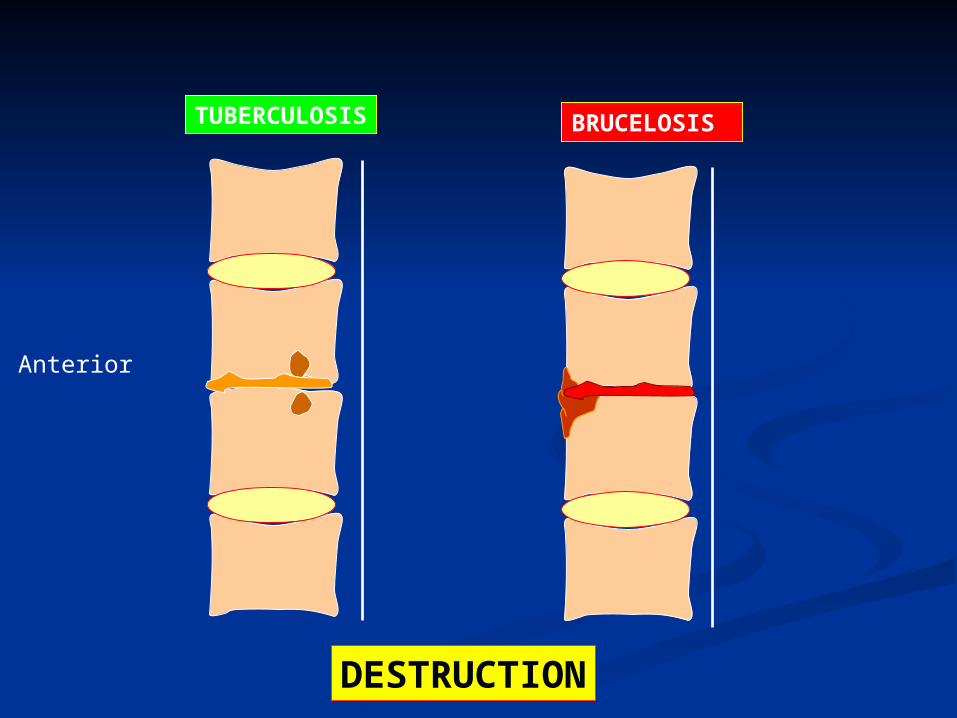
Anterior
TUBERCULOSIS
DESTRUCTION
BRUCELOSIS

Anterior
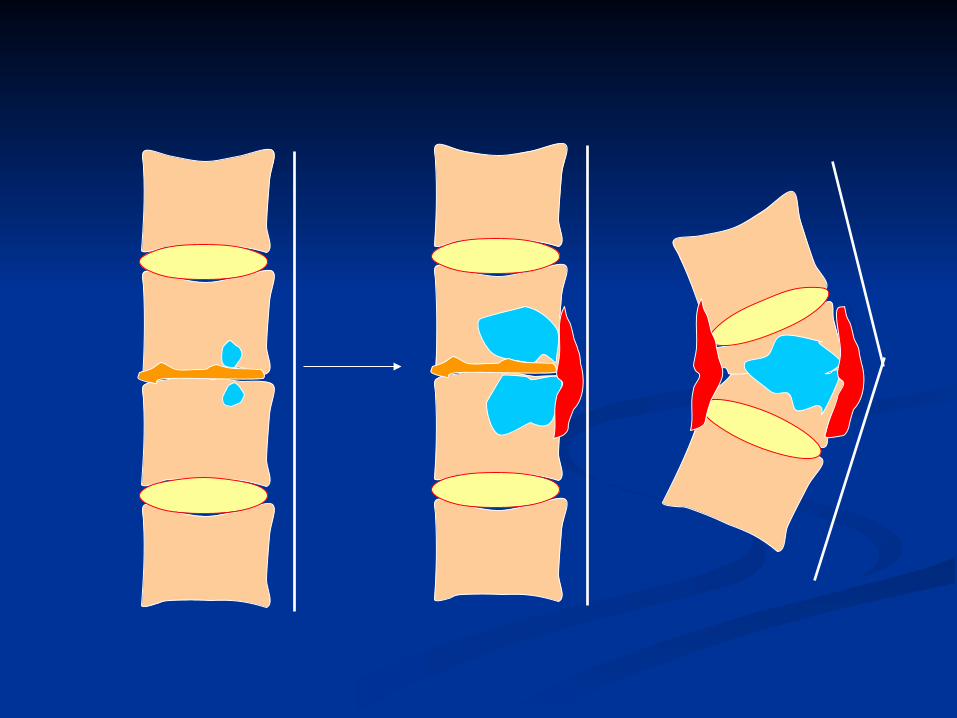
REPAIR

ANT
INITIATION REPAIR
COURSE
DESTRUCTION

SPONDYLODISCITIS SPONDYLODISCITIS OF OF
TUBERCULOSISTUBERCULOSIS
(POTT(POTT’’S disease)S disease)

EpidemiologyEpidemiology
2 % musculoskeletal2 % musculoskeletal 1% spine1% spine
Site:Site: Upper thoracic: ChildrenUpper thoracic: Children Lower thoracic: AdultLower thoracic: Adult
Lung involvement: 20-30%Lung involvement: 20-30%


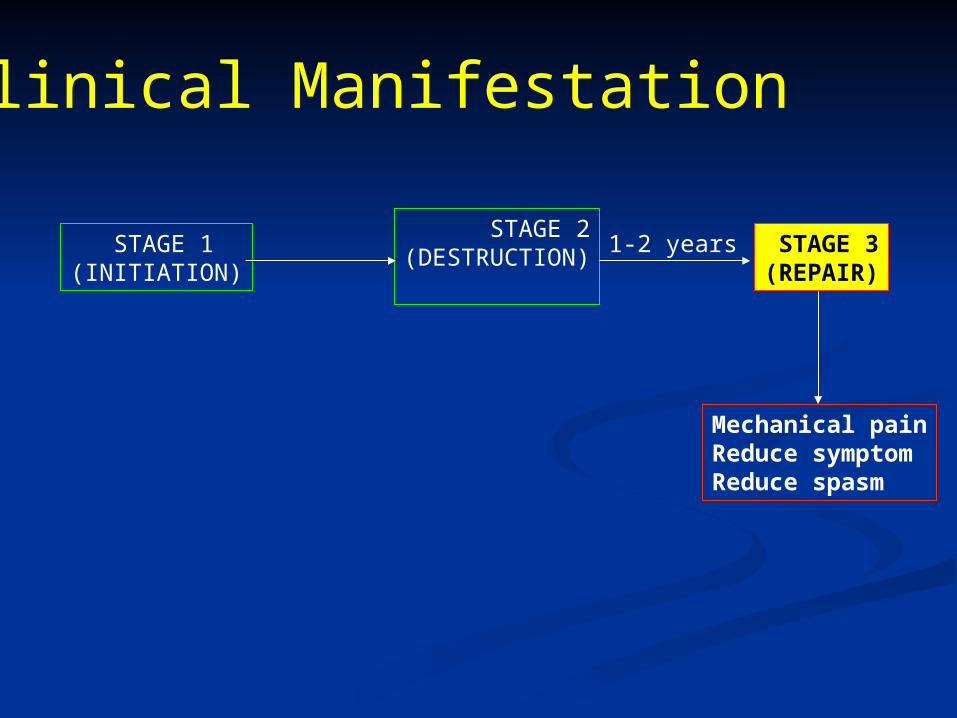
Clinical Manifestation

STAGE 1(INITIATION)
STAGE 2(DESTRUCTION) STAGE 3
(REPAIR)
Clinical Manifestation
1-2 yearsmonths

STAGE 1(INITIATION)
Mechanical painMild tenderness
Clinical Manifestation

STAGE 1(INITIATION)
STAGE 2(DESTRUCTION)
months
ConstitutionalSevere Back pain
Clinical Manifestation
Ph/Ex:Severe TendernessBlockage (erect posture)Gibbous deformityCold abscessNeurological (paraplegia)
STAGE 1(INITIATION)
STAGE 2(DESTRUCTION) STAGE 3
(REPAIR)
Mechanical painReduce symptomReduce spasm
1-2 years
Clinical Manifestation
DIAGNOSISDIAGNOSIS

IMAGINGIMAGING


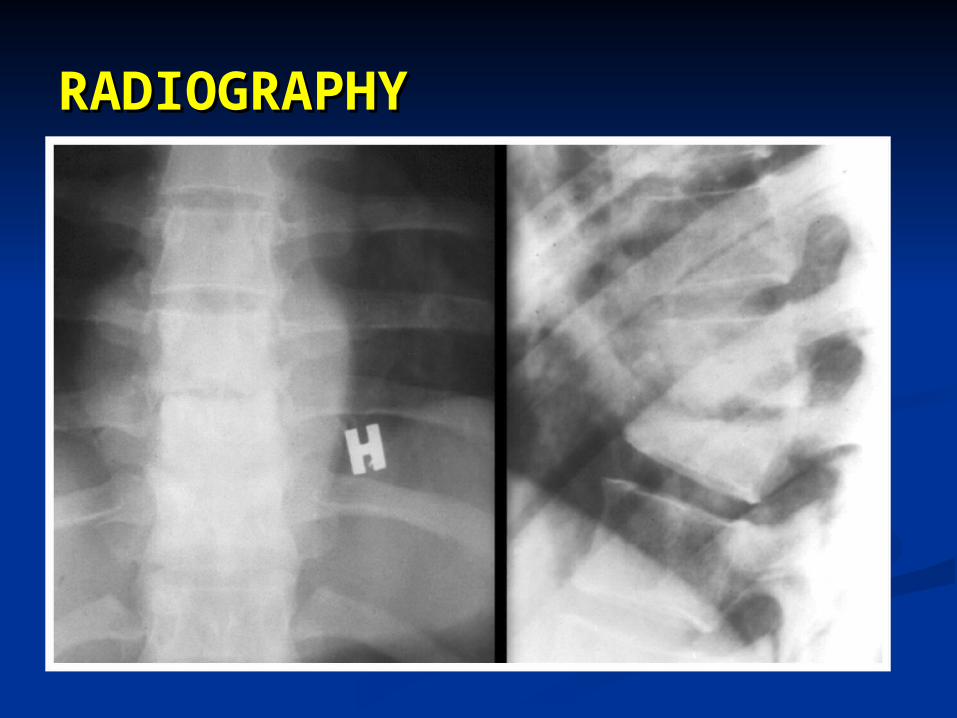
RADIOGRAPHYRADIOGRAPHY


LAB TESTSLAB TESTS

LAB TESTSLAB TESTS ESRESR PPD (+)PPD (+) Sputum smear & cultureSputum smear & culture Abscess or bone biopsy: Culture / Abscess or bone biopsy: Culture /
PathologyPathology

TREATMENTTREATMENT

TREATMENTTREATMENT Medical:Medical:
Mainstay of treatment Mainstay of treatment Alone is successful in Alone is successful in 70%70% DurationDuration: 18 m (9-12 m ?): 18 m (9-12 m ?)

TREATMENTTREATMENT Surgical:Surgical:
Advanced neurological deficitAdvanced neurological deficit Progressive Neurological deficits Progressive Neurological deficits Kyphosis > 40 degreesKyphosis > 40 degrees
MonitoringMonitoring ClinicalClinical
painpain constitutionalconstitutional mobilitymobility neurological signsneurological signs
ESR, CRPESR, CRP
RadiologyRadiology may be progress during first 6 month may be progress during first 6 month
of treatmentof treatment
BRUCELLOSISBRUCELLOSISSPONDYLODISCITISSPONDYLODISCITIS

EPIDEMIOLOGYEPIDEMIOLOGY
Spine: Spine: 7-8% of skeletal7-8% of skeletal
Site: Site: Lumbosacral (Anterior)Lumbosacral (Anterior)
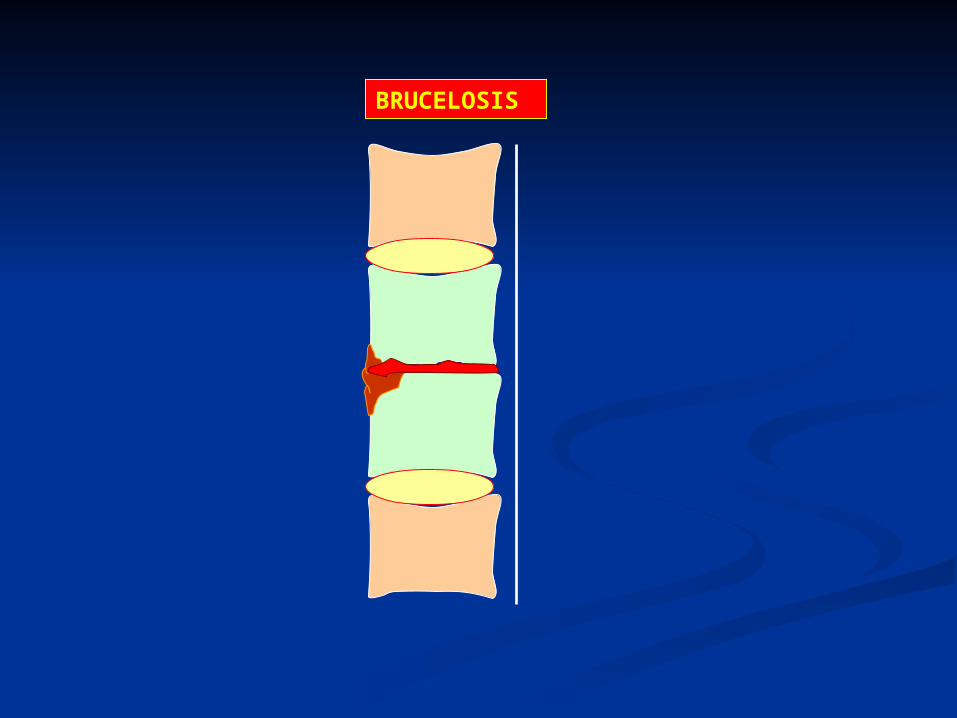
BRUCELOSIS

CLINICAL CLINICAL MANIFESTATIONMANIFESTATION
CLINICAL CLINICAL MANIFESTATIONMANIFESTATION
Constitutional:Constitutional: FeverFever Night SweatNight Sweat MalaiseMalaise ArthralgiaArthralgia ApatheticApathetic
Then: Severe low back pain Then: Severe low back pain
CLINICAL CLINICAL MANIFESTATIONMANIFESTATION
CLINICAL CLINICAL MANIFESTATIONMANIFESTATION
Physical examination:Physical examination:BlockageBlockage
Severe tendernessSevere tenderness
Fever Fever
SplenomegalySplenomegaly
LymphadenopathyLymphadenopathy

DIAGNOSISDIAGNOSIS
DIAGNOSISDIAGNOSIS Clinical presentationClinical presentation RadiographyRadiography Supporting laboratory finding Supporting laboratory finding History of potential exposure:History of potential exposure:
Endemic areaEndemic area Microbiology laboratoryMicrobiology laboratory Unpasteurized milk productsUnpasteurized milk products Contact with animalsContact with animals History of similar illness in the family History of similar illness in the family
(documented in almost 50% of cases).(documented in almost 50% of cases).


LaboratoryLaboratoryWBC: NL or lowWBC: NL or low
ESR, CRP: NLESR, CRP: NL
Wright; Cooms WrightWright; Cooms Wright
B/C or Bone marrow culture (7-35 B/C or Bone marrow culture (7-35 d)d)
ELISAELISA

TreatmentTreatment
2 Drug:2 Drug: Rifampin 600-900 mg/dRifampin 600-900 mg/d Doxycycline 100 mg twice dailyDoxycycline 100 mg twice daily
3 months3 months

SALMONELLA SALMONELLA SPONDYLODISCITISSPONDYLODISCITIS

SALMONELLA SALMONELLA SPONDYLODISCITISSPONDYLODISCITIS
Clinical sign & radiologic future is Clinical sign & radiologic future is similar to Brucellosis.similar to Brucellosis.
Diarrhea: 60%Diarrhea: 60%
Positive S/C (most commonly)Positive S/C (most commonly)

SALMONELLA SPONDYLODISCITISSALMONELLA SPONDYLODISCITIS
Treatment:Treatment:QuinolonesQuinolones
CeftriaxoneCeftriaxone
For 4 wFor 4 w
PYOGENIC PYOGENIC SPONDYLODISCITISPONDYLODISCITI
SS

PYOGENIC SPONDYLODISCITISPYOGENIC SPONDYLODISCITIS
staphylococcus aureusstaphylococcus aureus (50 (50 –– 70%) 70%)
History of recent infection (UTI; History of recent infection (UTI;
septicemia)septicemia)
Acute severe back pain; High fever; Acute severe back pain; High fever;
ChillsChills
Patient is ill. Patient is ill.
Blockage; Severe tendernessBlockage; Severe tenderness
Lumbar spine (45%) Thoracic (35%) Lumbar spine (45%) Thoracic (35%)

PYOGENIC SPONDYLODISCITISPYOGENIC SPONDYLODISCITIS
Radiography:Radiography: severe destructivesevere destructive rapidly progressive lesionrapidly progressive lesion Large bone bridgeLarge bone bridge

PYOGENIC SPONDYLODISCITISPYOGENIC SPONDYLODISCITIS
MRI: MRI:

PYOGENIC SPONDYLODISCITISPYOGENIC SPONDYLODISCITIS
Laboratory:Laboratory:LeucocytosisLeucocytosis
ESR (useful in fallow up)ESR (useful in fallow up)
CultureCultureB/C: 50% - B/C: 50% -
70%70%
Biopsy: 70% - Biopsy: 70% - 90%90% UTD UTD
19.319.3
PYOGENIC SPONDYLODISCITISPYOGENIC SPONDYLODISCITIS
Diagnosis:Diagnosis:Clinical presentationClinical presentation
RadiologyRadiology
laboratorylaboratory

PYOGENIC SPONDYLODISCITISPYOGENIC SPONDYLODISCITIS
Treatment: Treatment: Two drugs (Staph & gram negative Two drugs (Staph & gram negative organisms)organisms)
Six weeksSix weeks
Surgery:Surgery:
-- progressive progressive
-- cord compression cord compression

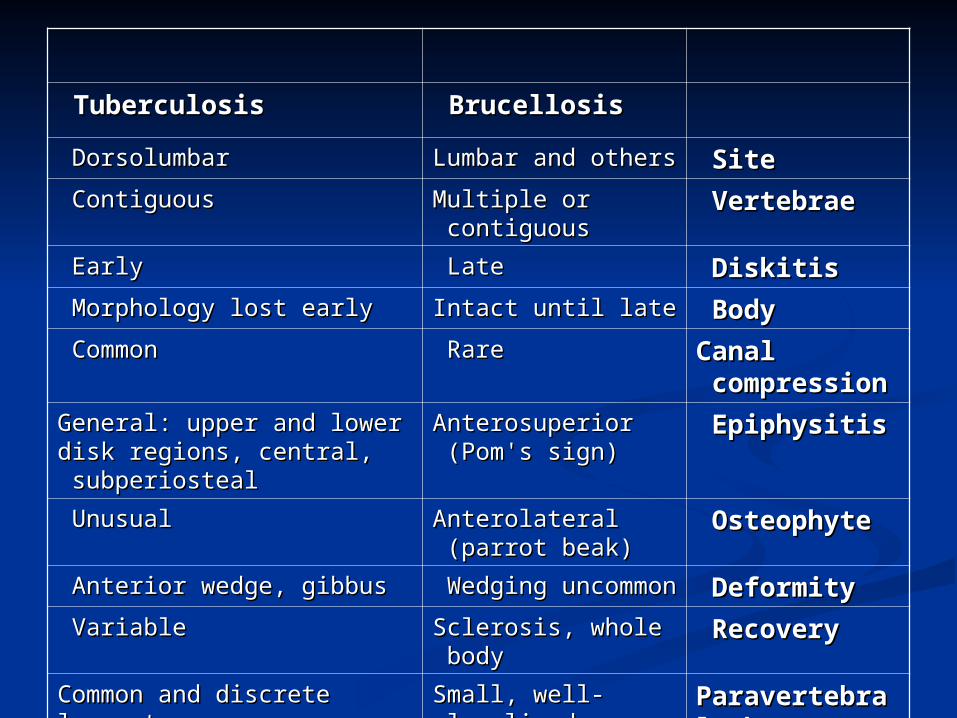
BrucellosisBrucellosis TuberculosisTuberculosis
SiteSite Lumbar and othersLumbar and others DorsolumbarDorsolumbar
VertebraeVertebrae Multiple or Multiple or contiguouscontiguous
ContiguousContiguous
DiskitisDiskitis LateLate EarlyEarly
BodyBody Intact until lateIntact until late Morphology lost earlyMorphology lost early
Canal Canal compressioncompression
RareRare CommonCommon
EpiphysitisEpiphysitis Anterosuperior Anterosuperior (Pom's sign)(Pom's sign)
General: upper and lower General: upper and lower disk regions, central, disk regions, central, subperiostealsubperiosteal
OsteophyteOsteophyte Anterolateral Anterolateral (parrot beak)(parrot beak)
UnusualUnusual
DeformityDeformity Wedging Wedging uncommonuncommon
Anterior wedge, gibbusAnterior wedge, gibbus
RecoveryRecovery Sclerosis, whole Sclerosis, whole bodybody
VariableVariable
Paravertebral Paravertebral abscessabscess
Small, well-Small, well-localizedlocalized
Common and discrete loss, Common and discrete loss, transverse processtransverse process
Psoas Psoas abscessabscess
RareRare More likelyMore likely