ykl-40expressionisassociatedwithpoorerresponsetoradiation ... · radiation resistance/sensitivity...
TRANSCRIPT

YKL-40 Expression is Associatedwith Poorer Response to Radiationand Shorter Overall Survival in GlioblastomaChristopher E. Pelloski,1AnitaMahajan,1MosheMaor,1Eric L. Chang,1ShiaoWoo,1Mark Gilbert,2
Howard Colman,2 HelenYang,3 Alicia Ledoux,3 Hilary Blair,4 Sandra Passe,4
Robert B. Jenkins,4 and Kenneth D. Aldape3
Abstract Purpose:YKL-40 is a secreted protein that has been reported to be overexpressed in epithelialcancers and gliomas, although its function is unknown. Previous data in a smaller sample setsuggested thatYKL-40 was a marker associated with a poorer clinical outcome and a geneticallydefined subgroup of glioblastoma. Here we test these findings in a larger series of patients withglioblastoma, and in particular, determine if tumorYKL-40 expression is associated with radiationresponse.Experimental Design: Patients (n = 147) with subtotal resections were studied for imaging-assessed changes in tumor size in serial studies following radiation therapy. An additional set(n = 140) of glioblastoma patients who underwent a gross-total resection was tested to validatethe survival association and extend them to patients withminimal residual disease.Results: In the subtotal resection group, higherYKL-40 expression was significantly associatedwith poorer radiation response, shorter time to progression and shorter overall survival.The asso-ciationof higherYKL-40 expressionwithpoorer survivalwas validated in the gross-total resectiongroup. Inmultivariate analysis withboth groups combined (n =287),YKL-40was an independentpredictor of survival after adjusting for patient age, performance status, and extent of resection.YKL-40 expression was also compared with genetically defined subsets of glioblastoma byassessing epidermal growth factor receptor amplification and loss at chromosome 10q, two ofthe common recurring aberrations in these tumors, using fluorescent in situ hybridization. YKL-40was significantly associatedwith10q loss.Conclusions:The findings implicateYKL-40 as an important marker of therapeutic response andgenetic subtype in glioblastomas and suggest that it may play an oncogenic role in these tumors.
Glioblastoma is an aggressive disease with median overallsurvival of 10 to 12 months after diagnosis. Despite advances insurgical techniques, postoperative supportive care, radiationdelivery, and adjuvant systemic therapy, the life expectancy ofpatients with glioblastoma has remained essentially unchangedover the last several decades. Radiation therapy, given afterprimary surgical resection, is the standard adjuvant treatmentwith proven efficacy for glioblastoma (1–3). However, thistumor is regarded as clinically radioresistant, as a relativelylarge proportion of patients experience tumor progression
during radiotherapy (4, 5). Most lesions recur/progress within 1to 2 cm from the primary surgical margin, well withinradiotherapy fields (6–8). Although factors that underlieradiation resistance/sensitivity in glioblastoma are not well-understood, older patients have been reported to exhibit apoorer response to radiation (9). With respect to molecularcorrelates of radiation response, gain in chromosome 7 andlosses in chromosomes 9p and 13q copy number have beenreported to be associated with a poorer response (10). We havepreviously found that overexpression of epidermal growthfactor receptor (EGFR) correlates with a less favorable response(11). A better understanding of the molecular factors thatconfer radioresistance in glioblastoma may lead to newapproaches to improve the radiation sensitivity of these tumors.
YKL-40 (also known as CHI3L1 or human cartilageglycoprotein-39) is located on chromosome 1q32.1 and is asecreted protein whose function is poorly understood and hashomology with glycosyl hydrolases. YKL-40 may have a role incell migration (12) and connective tissue modeling (13–15)and is involved in the inflammatory response (16, 17).Increased YKL-40 levels have been associated with diseaseactivity in rheumatoid arthritis and other autoimmune disor-ders (18–24). Additionally, it has been implicated as a serummarker for aggressive disease in colon (25), ovarian (26, 27),and breast carcinoma (28, 29). Elevated YKL-40 levels were
www.aacrjournals.orgClin Cancer Res 2005;11(9) May1, 2005 3326
Authors’Affiliations: Departments of 1Radiation Oncology, 2Neuro-Oncology,and 3Pathology, University of Texas M.D. Anderson Cancer Center, Houston,Texas, and 4Department of Pathology and Laboratory Medicine, Mayo Clinicand Foundation, Rochester, MinnesotaReceived 8/31/04; revised12/16/04; accepted1/5/05.Grant support: Grant P01CA85799 (to R.B. Jenkins and K.D. Aldape) and anM.D. Anderson Institutional Research Grant to K.D. Aldape.The costs of publication of this article were defrayed in part by the payment ofpage charges. This article must therefore be hereby marked advertisement inaccordancewith18 U.S.C. Section1734 solely to indicate this fact.Requests for reprints: Kenneth D. Aldape, Department of Pathology, Box 85,University of Texas M.D. Anderson Cancer Center, 1515 Holcombe Boulevard,Houston, TX 77030. Phone: 713-792-7935; Fax : 713-745-1105; E-mail:[email protected].
F2005 American Association for Cancer Research.
Imaging, Diagnosis, Prognosis
Research. on June 11, 2020. © 2005 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

identified in a gene expression profiling study of glioblastoma,as was the presence of YKL-40 in the serum of glioblastomapatients (30). Preliminary data from our laboratory showed theexistence of an association between higher YKL-40 expressionlevels and worse overall survival in glioblastoma. Becauseradiotherapy is a major treatment modality for glioblastomafollowing surgery, we hypothesized that YKL-40 might beassociated with response to radiation. To test this hypothesis,we identified a group of glioblastoma patients who hadundergone subtotal resections, selected in order that measur-able residual disease could be followed on serial imagingstudies. We examined the relationship between YKL-40expression, radiation response, and survival in this set. Inaddition, we tested the prognostic association between YKL-40expression and glioblastoma in an independent sample of grosstotally resected patients with glioblastoma. Finally, we examinerelationships of YKL-40 expression with EGFR amplificationand chromosome 10 status to test whether YKL-40 is associatedwith this genetic subset.
Materials andMethods
Patient characteristics. One hundred and forty-seven cases ofsubtotally resected glioblastoma were identified at the University ofTexas M.D. Anderson Cancer Center from January 1993 until June2003. Inclusion criteria required that the patient (a) had not receivedany prior therapy for the tumor, (b) underwent a preoperative andimmediate postoperative (within 48 hours) magnetic resonanceimaging (MRI) of the brain to assess the extent of resection, (c)received radiation therapy, (d) underwent at least one post-radiotherapyMRI (within 10 weeks of completion), and (e) had archival paraffin-embedded tissue available for immunohistochemical staining. Caseswere re-reviewed by a neuropathologist (K.D. Aldape) to ensure thatthey fulfilled histologic criteria for glioblastoma using current WHOguidelines, which include a high-grade astrocytic tumor with micro-vascular proliferation and/or necrosis. One hundred and thirteen ofthe 135 patients with reported radiation therapy doses (84%) receiveda radiation tumor dose of z5,400 cGy. Most of the patients whoreceived lower doses either underwent hypofractionated regimens, ordeteriorated during their treatment course and could not completeradiation therapy. One hundred and nine (78%) received systemicchemotherapy. At least one cycle of 39 unique treatment regimens(single agent or in combination), composed of 28 different agents wereused. Of these varied chemotherapeutic regimens, most (98 of 109)were either procarbazine-, lomustine-, and vincristine-based (n = 20) ortemozolamide-based (n = 68). Institutional Review Board approval wasobtained for these studies.
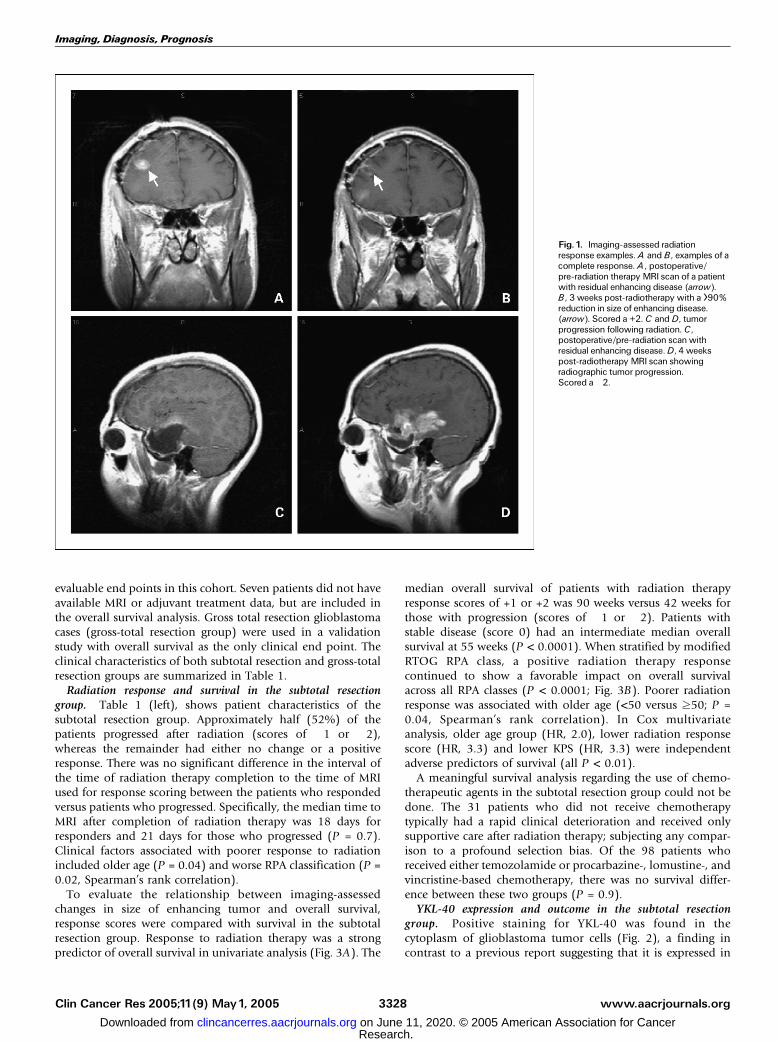
The radiation therapy response was determined by comparing thechange in enhancing tumor size between the post-surgical assessmentand first post-radiation therapy MRI in a manner previously defined byBarker and colleagues (31). The magnitude of radiation therapyresponse was assessed using a five-tiered scoring system, which rangedfrom +2 (z50% size reduction; Fig. 1A and B) to �2 (z50% tumorgrowth; Fig. 1C and D). The +1/�1 scores represented a change(reduction and increase, respectively) of <50% magnitude in size in theenhancing cross-sectional area. Post-radiation therapy MRI films wereunavailable for seven patients and although these seven patients werenot included in the response analyses, they were included in overallsurvival analyses.
A second cohort of 140 patients with gross total resections during thesame time interval represented a group for whom associations betweenYKL-40 and overall survival could be tested and used to validate thefindings in the first group. Inclusion was based on criteria a and babove, with a verified gross total (>95%) resection, along with archivalparaffin tissue available for YKL-40 staining. This patient group had
characteristics similar to that of the subtotal resection group (Table 1).Sixty out of 78 patients with reported doses (77%) received a radiationtumor dose of z5,400 cGy. In the patients with unreported doses(received radiation therapy at outside facilities), the radiation therapywas described as ‘‘conventional’’ in most cases. Six patients did notreceive adjuvant radiation therapy.
Overall survival was determined from the date of diagnosis to thedate of death or last follow-up. Time to progression was determinedfrom the date of the initial therapeutic surgery to the date ofradiographically detected (MRI) enhancing tumor progression insubtotal resection patients or the date of last radiographic follow-up.The Radiation Therapy Oncology Group (RTOG) recursive partitioninganalysis (RPA) classification system for malignant glioma (33, 34),recently modified by Shaw and colleagues (32), was used. The modifiedRTOG RPA classification for glioblastoma takes into account age,Karnofsky performance status (KPS), extent of resection, and the abilityof patients to perform activities of daily living (described as working[W+/�]).
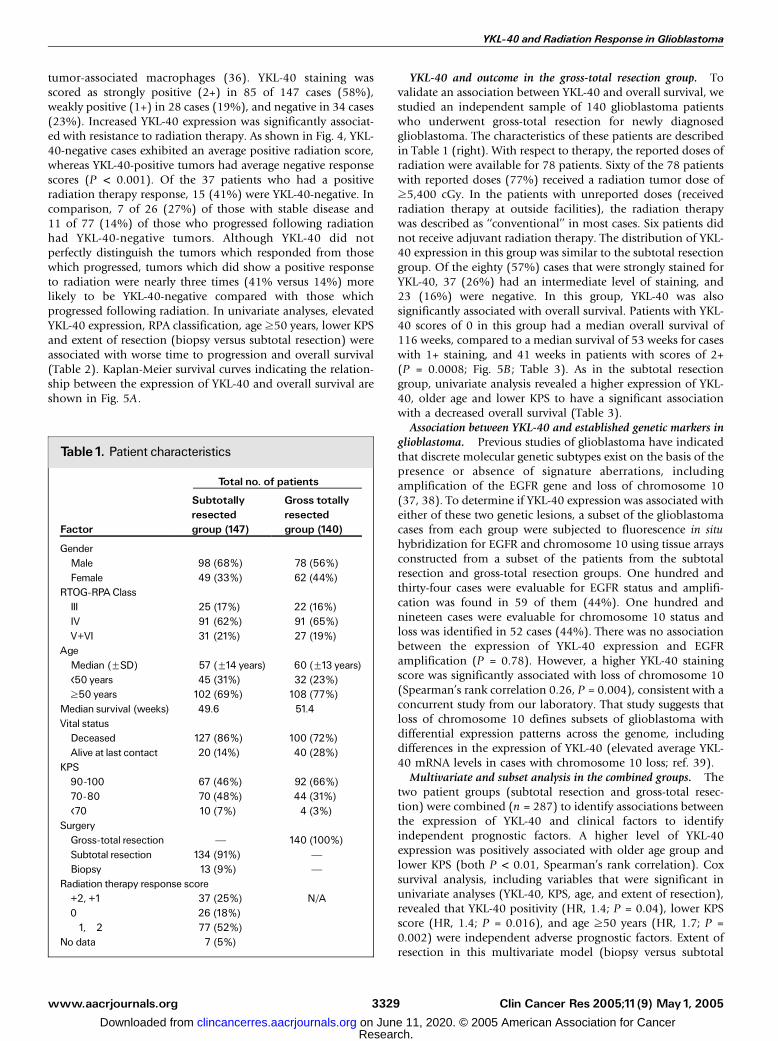
Immunohistochemistry and tissue array construction. Paraffin blockswere obtained from the Department of Pathology archives at Universityof Texas M.D. Anderson Cancer Center. Each case was reviewed by aneuropathologist (K.D. Aldape) to identify blocks with sufficient tumoravailable for analysis. A polyclonal antibody to YKL-40 was obtainedfrom Quidel Corporation (San Diego, CA). Immunohistochemistry wasdone as previously described (33) and slides were incubated in primaryantibody overnight at 4jC at an antibody dilution of 1:1,500. Stainingwas scored using a three-tiered system: 2+, strongly positive staining inthe majority of tumor cells at least 1 medium power (100�)microscopic field (2+); 1+, weak/patchy staining in tumor cells; and0, no staining (Fig. 2A-E). Staining was scored while blinded to clinicaldata. Cases known to be positive and negative were used as controls foreach batch of tumor samples.
Cases (n = 140) were randomly selected from the subtotal resectiongroup (n = 94) and gross-total resection group (n = 52) from whichtissue arrays were constructed. A Beecher (Sun Prairie, WI) manualtissue arrayer was used to generate tissue arrays. A minimum of twocores were used for each case, and most had three cores or greater.
Fluorescence in situ hybridization. EGFR amplification and chro-mosome 10 loss were assessed using fluorescence in situ hybridizationanalysis of glioma specimens distributed on tissue microarrays. A dual-probe dual-color probe set for EGFR (red fluorophore) and thecentromere of chromosome 7 (green fluorophore) was used to assessEGFR amplification. A dual-color probe set for PTEN (red) and thecentromere of chromosome 10 (green) was used to assess chromosome10 loss. Both probe sets were obtained from Vysis, Inc. (Downer’sGrove, IL). Hybridization methods and criteria for EGFR amplificationand chromosome 10 loss have been previously reported (34).
Statistical analysis. Spearman’s Rho correlation was used todetermine associations between clinicopathologic variables. Kaplan-Meier (35) survival analysis was used to compare overall survival andtime to progression between subgroups. Patients who were alive at lastfollow-up (for overall survival) or who had no documented time toprogression at last follow-up were considered to be censored. Cox-regression multivariate analysis was used for determining independentprognostic factors.
Results
Subtotal resection cases (n = 147) were accrued to evaluatethe effect of radiotherapy by observing changes in residualtumor size in serial imaging studies. With respect to therapeuticregimen, 113 of the 135 patients with reported radiationtherapy doses (84%) received a radiation tumor dose of z5,400cGy. One hundred and nine (78%) received systemic chemo-therapy at some time during the disease course. Radiationresponse, time to progression, and overall survival were
www.aacrjournals.org Clin Cancer Res 2005;11(9) May1, 20053327
YKL-40 and Radiation Response in Glioblastoma
Research. on June 11, 2020. © 2005 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
evaluable end points in this cohort. Seven patients did not haveavailable MRI or adjuvant treatment data, but are included inthe overall survival analysis. Gross total resection glioblastomacases (gross-total resection group) were used in a validationstudy with overall survival as the only clinical end point. Theclinical characteristics of both subtotal resection and gross-totalresection groups are summarized in Table 1.
Radiation response and survival in the subtotal resectiongroup. Table 1 (left), shows patient characteristics of thesubtotal resection group. Approximately half (52%) of thepatients progressed after radiation (scores of �1 or �2),whereas the remainder had either no change or a positiveresponse. There was no significant difference in the interval ofthe time of radiation therapy completion to the time of MRIused for response scoring between the patients who respondedversus patients who progressed. Specifically, the median time toMRI after completion of radiation therapy was 18 days forresponders and 21 days for those who progressed (P = 0.7).Clinical factors associated with poorer response to radiationincluded older age (P = 0.04) and worse RPA classification (P =0.02, Spearman’s rank correlation).
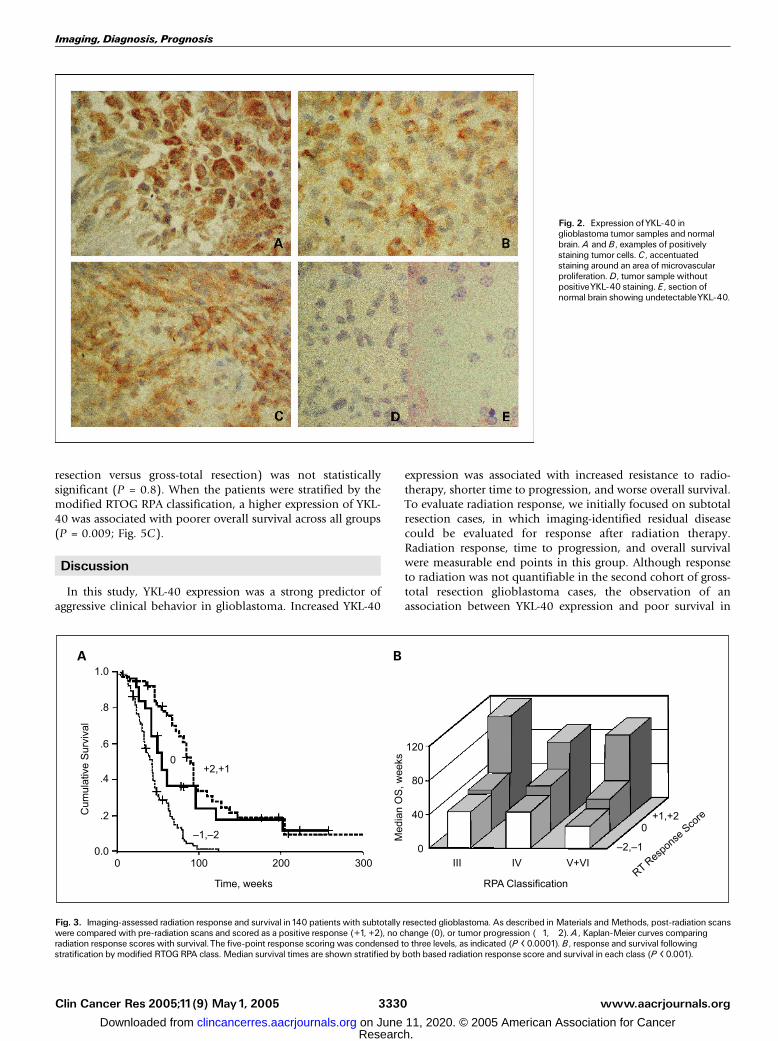
To evaluate the relationship between imaging-assessedchanges in size of enhancing tumor and overall survival,response scores were compared with survival in the subtotalresection group. Response to radiation therapy was a strongpredictor of overall survival in univariate analysis (Fig. 3A). The
median overall survival of patients with radiation therapyresponse scores of +1 or +2 was 90 weeks versus 42 weeks forthose with progression (scores of �1 or �2). Patients withstable disease (score 0) had an intermediate median overallsurvival at 55 weeks (P < 0.0001). When stratified by modifiedRTOG RPA class, a positive radiation therapy responsecontinued to show a favorable impact on overall survivalacross all RPA classes (P < 0.0001; Fig. 3B). Poorer radiationresponse was associated with older age (<50 versus z50; P =0.04, Spearman’s rank correlation). In Cox multivariateanalysis, older age group (HR, 2.0), lower radiation responsescore (HR, 3.3) and lower KPS (HR, 3.3) were independentadverse predictors of survival (all P < 0.01).
A meaningful survival analysis regarding the use of chemo-therapeutic agents in the subtotal resection group could not bedone. The 31 patients who did not receive chemotherapytypically had a rapid clinical deterioration and received onlysupportive care after radiation therapy; subjecting any compar-ison to a profound selection bias. Of the 98 patients whoreceived either temozolamide or procarbazine-, lomustine-, andvincristine-based chemotherapy, there was no survival differ-ence between these two groups (P = 0.9).
YKL-40 expression and outcome in the subtotal resectiongroup. Positive staining for YKL-40 was found in thecytoplasm of glioblastoma tumor cells (Fig. 2), a finding incontrast to a previous report suggesting that it is expressed in
www.aacrjournals.orgClin Cancer Res 2005;11(9) May1, 2005 3328
Fig. 1. Imaging-assessed radiationresponse examples.A and B, examples of acomplete response. A , postoperative/pre-radiation therapy MRI scan of a patientwith residual enhancing disease (arrow).B, 3 weeks post-radiotherapy with a >90%reduction in size of enhancing disease.(arrow). Scored a +2. C andD, tumorprogression following radiation. C,postoperative/pre-radiation scanwithresidual enhancing disease.D, 4 weekspost-radiotherapy MRI scan showingradiographic tumor progression.Scored a�2.
Imaging, Diagnosis, Prognosis
Research. on June 11, 2020. © 2005 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
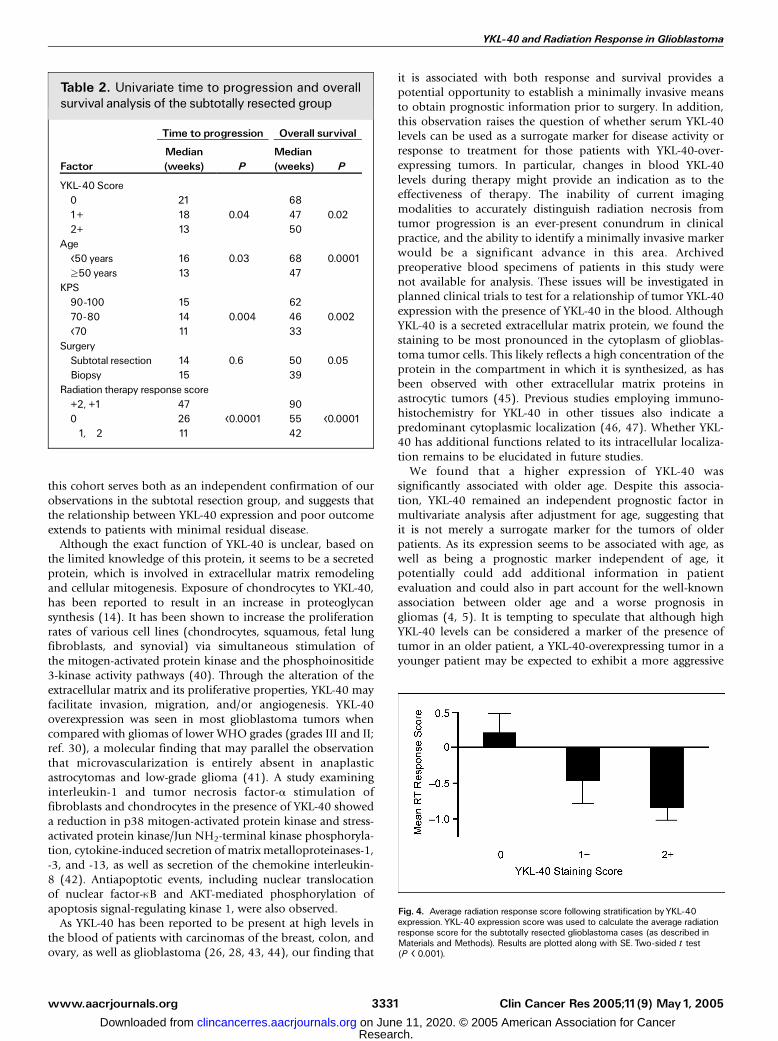
tumor-associated macrophages (36). YKL-40 staining wasscored as strongly positive (2+) in 85 of 147 cases (58%),weakly positive (1+) in 28 cases (19%), and negative in 34 cases(23%). Increased YKL-40 expression was significantly associat-ed with resistance to radiation therapy. As shown in Fig. 4, YKL-40-negative cases exhibited an average positive radiation score,whereas YKL-40-positive tumors had average negative responsescores (P < 0.001). Of the 37 patients who had a positiveradiation therapy response, 15 (41%) were YKL-40-negative. Incomparison, 7 of 26 (27%) of those with stable disease and11 of 77 (14%) of those who progressed following radiationhad YKL-40-negative tumors. Although YKL-40 did notperfectly distinguish the tumors which responded from thosewhich progressed, tumors which did show a positive responseto radiation were nearly three times (41% versus 14%) morelikely to be YKL-40-negative compared with those whichprogressed following radiation. In univariate analyses, elevatedYKL-40 expression, RPA classification, age z50 years, lower KPSand extent of resection (biopsy versus subtotal resection) wereassociated with worse time to progression and overall survival(Table 2). Kaplan-Meier survival curves indicating the relation-ship between the expression of YKL-40 and overall survival areshown in Fig. 5A.
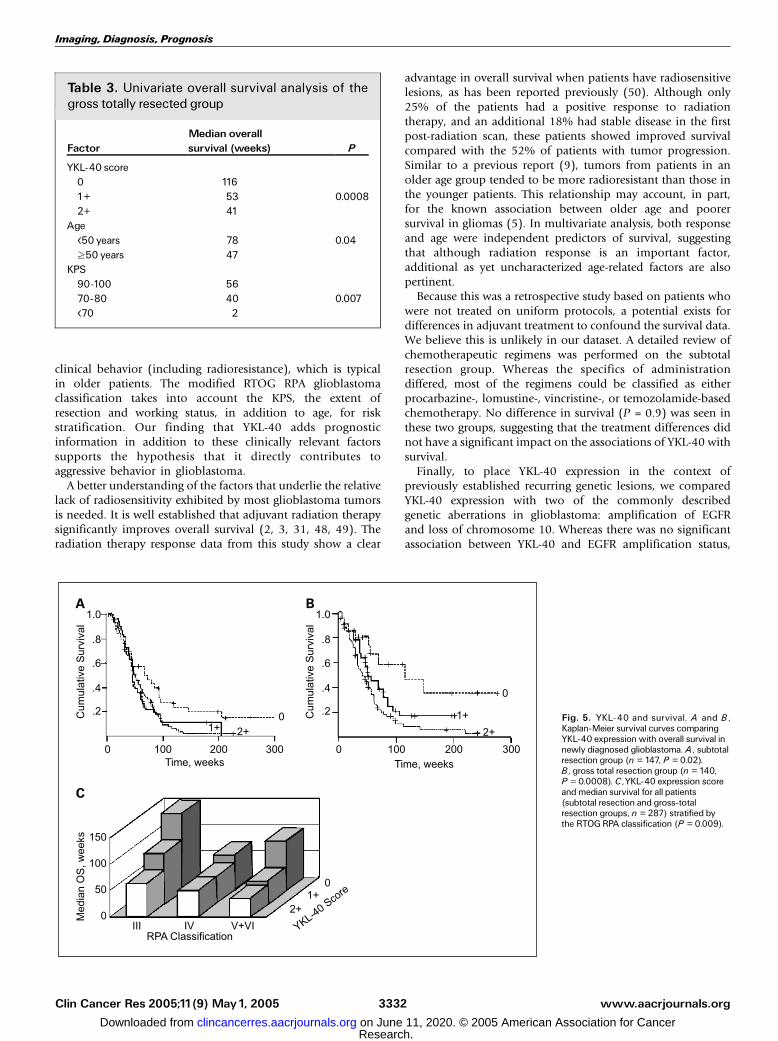
YKL-40 and outcome in the gross-total resection group. Tovalidate an association between YKL-40 and overall survival, westudied an independent sample of 140 glioblastoma patientswho underwent gross-total resection for newly diagnosedglioblastoma. The characteristics of these patients are describedin Table 1 (right). With respect to therapy, the reported doses ofradiation were available for 78 patients. Sixty of the 78 patientswith reported doses (77%) received a radiation tumor dose ofz5,400 cGy. In the patients with unreported doses (receivedradiation therapy at outside facilities), the radiation therapywas described as ‘‘conventional’’ in most cases. Six patients didnot receive adjuvant radiation therapy. The distribution of YKL-40 expression in this group was similar to the subtotal resectiongroup. Of the eighty (57%) cases that were strongly stained forYKL-40, 37 (26%) had an intermediate level of staining, and23 (16%) were negative. In this group, YKL-40 was alsosignificantly associated with overall survival. Patients with YKL-40 scores of 0 in this group had a median overall survival of116 weeks, compared to a median survival of 53 weeks for caseswith 1+ staining, and 41 weeks in patients with scores of 2+(P = 0.0008; Fig. 5B; Table 3). As in the subtotal resectiongroup, univariate analysis revealed a higher expression of YKL-40, older age and lower KPS to have a significant associationwith a decreased overall survival (Table 3).
Association between YKL-40 and established genetic markers inglioblastoma. Previous studies of glioblastoma have indicatedthat discrete molecular genetic subtypes exist on the basis of thepresence or absence of signature aberrations, includingamplification of the EGFR gene and loss of chromosome 10(37, 38). To determine if YKL-40 expression was associated witheither of these two genetic lesions, a subset of the glioblastomacases from each group were subjected to fluorescence in situhybridization for EGFR and chromosome 10 using tissue arraysconstructed from a subset of the patients from the subtotalresection and gross-total resection groups. One hundred andthirty-four cases were evaluable for EGFR status and amplifi-cation was found in 59 of them (44%). One hundred andnineteen cases were evaluable for chromosome 10 status andloss was identified in 52 cases (44%). There was no associationbetween the expression of YKL-40 expression and EGFRamplification (P = 0.78). However, a higher YKL-40 stainingscore was significantly associated with loss of chromosome 10(Spearman’s rank correlation 0.26, P = 0.004), consistent with aconcurrent study from our laboratory. That study suggests thatloss of chromosome 10 defines subsets of glioblastoma withdifferential expression patterns across the genome, includingdifferences in the expression of YKL-40 (elevated average YKL-40 mRNA levels in cases with chromosome 10 loss; ref. 39).
Multivariate and subset analysis in the combined groups. Thetwo patient groups (subtotal resection and gross-total resec-tion) were combined (n = 287) to identify associations betweenthe expression of YKL-40 and clinical factors to identifyindependent prognostic factors. A higher level of YKL-40expression was positively associated with older age group andlower KPS (both P < 0.01, Spearman’s rank correlation). Coxsurvival analysis, including variables that were significant inunivariate analyses (YKL-40, KPS, age, and extent of resection),revealed that YKL-40 positivity (HR, 1.4; P = 0.04), lower KPSscore (HR, 1.4; P = 0.016), and age z50 years (HR, 1.7; P =0.002) were independent adverse prognostic factors. Extent ofresection in this multivariate model (biopsy versus subtotal
www.aacrjournals.org Clin Cancer Res 2005;11(9) May1, 20053329
Table1. Patient characteristics
Total no. of patients
Factor
Subtotallyresectedgroup (147)
Gross totallyresectedgroup (140)
GenderMale 98 (68%) 78 (56%)Female 49 (33%) 62 (44%)
RTOG-RPAClassIII 25 (17%) 22 (16%)IV 91 (62%) 91 (65%)V+VI 31 (21%) 27 (19%)
AgeMedian (FSD) 57 (F14 years) 60 (F13 years)<50 years 45 (31%) 32 (23%)z50 years 102 (69%) 108 (77%)
Median survival (weeks) 49.6 51.4Vital statusDeceased 127 (86%) 100 (72%)Alive at last contact 20 (14%) 40 (28%)
KPS90-100 67 (46%) 92 (66%)70-80 70 (48%) 44 (31%)<70 10 (7%) 4 (3%)
SurgeryGross-total resection J 140 (100%)Subtotal resection 134 (91%) JBiopsy 13 (9%) J
Radiation therapy response score+2, +1 37 (25%) N/A0 26 (18%)�1,�2 77 (52%)
No data 7 (5%)
YKL-40 and Radiation Response in Glioblastoma
Research. on June 11, 2020. © 2005 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
resection versus gross-total resection) was not statisticallysignificant (P = 0.8). When the patients were stratified by themodified RTOG RPA classification, a higher expression of YKL-40 was associated with poorer overall survival across all groups(P = 0.009; Fig. 5C).
Discussion
In this study, YKL-40 expression was a strong predictor ofaggressive clinical behavior in glioblastoma. Increased YKL-40
expression was associated with increased resistance to radio-therapy, shorter time to progression, and worse overall survival.To evaluate radiation response, we initially focused on subtotalresection cases, in which imaging-identified residual diseasecould be evaluated for response after radiation therapy.Radiation response, time to progression, and overall survivalwere measurable end points in this group. Although responseto radiation was not quantifiable in the second cohort of gross-total resection glioblastoma cases, the observation of anassociation between YKL-40 expression and poor survival in
www.aacrjournals.orgClin Cancer Res 2005;11(9) May1, 2005 3330
Fig. 2. Expression ofYKL-40 inglioblastoma tumor samples and normalbrain. A and B, examples of positivelystaining tumor cells.C, accentuatedstaining around an area of microvascularproliferation.D, tumor sample withoutpositiveYKL-40 staining. E , section ofnormal brain showing undetectableYKL-40.
Fig. 3. Imaging-assessed radiation response and survival in140 patients with subtotally resected glioblastoma. As described in Materials andMethods, post-radiation scanswere compared with pre-radiation scans and scored as a positive response (+1, +2), no change (0), or tumor progression (�1,�2). A , Kaplan-Meier curves comparingradiation response scores with survival.The five-point response scoring was condensed to three levels, as indicated (P < 0.0001). B, response and survival followingstratification by modified RTOGRPA class. Median survival times are shown stratified by both based radiation response score and survival in each class (P < 0.001).
Imaging, Diagnosis, Prognosis
Research. on June 11, 2020. © 2005 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
this cohort serves both as an independent confirmation of ourobservations in the subtotal resection group, and suggests thatthe relationship between YKL-40 expression and poor outcomeextends to patients with minimal residual disease.
Although the exact function of YKL-40 is unclear, based onthe limited knowledge of this protein, it seems to be a secretedprotein, which is involved in extracellular matrix remodelingand cellular mitogenesis. Exposure of chondrocytes to YKL-40,has been reported to result in an increase in proteoglycansynthesis (14). It has been shown to increase the proliferationrates of various cell lines (chondrocytes, squamous, fetal lungfibroblasts, and synovial) via simultaneous stimulation ofthe mitogen-activated protein kinase and the phosphoinositide3-kinase activity pathways (40). Through the alteration of theextracellular matrix and its proliferative properties, YKL-40 mayfacilitate invasion, migration, and/or angiogenesis. YKL-40overexpression was seen in most glioblastoma tumors whencompared with gliomas of lower WHO grades (grades III and II;ref. 30), a molecular finding that may parallel the observationthat microvascularization is entirely absent in anaplasticastrocytomas and low-grade glioma (41). A study examininginterleukin-1 and tumor necrosis factor-a stimulation offibroblasts and chondrocytes in the presence of YKL-40 showeda reduction in p38 mitogen-activated protein kinase and stress-activated protein kinase/Jun NH2-terminal kinase phosphoryla-tion, cytokine-induced secretion of matrix metalloproteinases-1,-3, and -13, as well as secretion of the chemokine interleukin-8 (42). Antiapoptotic events, including nuclear translocationof nuclear factor-nB and AKT-mediated phosphorylation ofapoptosis signal-regulating kinase 1, were also observed.
As YKL-40 has been reported to be present at high levels inthe blood of patients with carcinomas of the breast, colon, andovary, as well as glioblastoma (26, 28, 43, 44), our finding that
it is associated with both response and survival provides apotential opportunity to establish a minimally invasive meansto obtain prognostic information prior to surgery. In addition,this observation raises the question of whether serum YKL-40levels can be used as a surrogate marker for disease activity orresponse to treatment for those patients with YKL-40-over-expressing tumors. In particular, changes in blood YKL-40levels during therapy might provide an indication as to theeffectiveness of therapy. The inability of current imagingmodalities to accurately distinguish radiation necrosis fromtumor progression is an ever-present conundrum in clinicalpractice, and the ability to identify a minimally invasive markerwould be a significant advance in this area. Archivedpreoperative blood specimens of patients in this study werenot available for analysis. These issues will be investigated inplanned clinical trials to test for a relationship of tumor YKL-40expression with the presence of YKL-40 in the blood. AlthoughYKL-40 is a secreted extracellular matrix protein, we found thestaining to be most pronounced in the cytoplasm of glioblas-toma tumor cells. This likely reflects a high concentration of theprotein in the compartment in which it is synthesized, as hasbeen observed with other extracellular matrix proteins inastrocytic tumors (45). Previous studies employing immuno-histochemistry for YKL-40 in other tissues also indicate apredominant cytoplasmic localization (46, 47). Whether YKL-40 has additional functions related to its intracellular localiza-tion remains to be elucidated in future studies.
We found that a higher expression of YKL-40 wassignificantly associated with older age. Despite this associa-tion, YKL-40 remained an independent prognostic factor inmultivariate analysis after adjustment for age, suggesting thatit is not merely a surrogate marker for the tumors of olderpatients. As its expression seems to be associated with age, aswell as being a prognostic marker independent of age, itpotentially could add additional information in patientevaluation and could also in part account for the well-knownassociation between older age and a worse prognosis ingliomas (4, 5). It is tempting to speculate that although highYKL-40 levels can be considered a marker of the presence oftumor in an older patient, a YKL-40-overexpressing tumor in ayounger patient may be expected to exhibit a more aggressive
www.aacrjournals.org Clin Cancer Res 2005;11(9) May1, 20053331
Table 2. Univariate time to progression and overallsurvival analysis of the subtotally resected group
Time to progression Overall survival
FactorMedian(weeks) P
Median(weeks) P
YKL-40 Score0 21 681+ 18 0.04 47 0.022+ 13 50
Age<50 years 16 0.03 68 0.0001z50 years 13 47
KPS90-100 15 6270-80 14 0.004 46 0.002<70 11 33
SurgerySubtotal resection 14 0.6 50 0.05Biopsy 15 39
Radiation therapy response score+2, +1 47 900 26 <0.0001 55 <0.0001�1,�2 11 42
Fig. 4. Average radiation response score following stratification byYKL-40expression. YKL-40 expression score was used to calculate the average radiationresponse score for the subtotally resected glioblastoma cases (as described inMaterials and Methods). Results are plotted along with SE. Two-sided t test(P < 0.001).
YKL-40 and Radiation Response in Glioblastoma
Research. on June 11, 2020. © 2005 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
clinical behavior (including radioresistance), which is typicalin older patients. The modified RTOG RPA glioblastomaclassification takes into account the KPS, the extent ofresection and working status, in addition to age, for riskstratification. Our finding that YKL-40 adds prognosticinformation in addition to these clinically relevant factorssupports the hypothesis that it directly contributes toaggressive behavior in glioblastoma.
A better understanding of the factors that underlie the relativelack of radiosensitivity exhibited by most glioblastoma tumorsis needed. It is well established that adjuvant radiation therapysignificantly improves overall survival (2, 3, 31, 48, 49). Theradiation therapy response data from this study show a clear
advantage in overall survival when patients have radiosensitivelesions, as has been reported previously (50). Although only25% of the patients had a positive response to radiationtherapy, and an additional 18% had stable disease in the firstpost-radiation scan, these patients showed improved survivalcompared with the 52% of patients with tumor progression.Similar to a previous report (9), tumors from patients in anolder age group tended to be more radioresistant than those inthe younger patients. This relationship may account, in part,for the known association between older age and poorersurvival in gliomas (5). In multivariate analysis, both responseand age were independent predictors of survival, suggestingthat although radiation response is an important factor,additional as yet uncharacterized age-related factors are alsopertinent.
Because this was a retrospective study based on patients whowere not treated on uniform protocols, a potential exists fordifferences in adjuvant treatment to confound the survival data.We believe this is unlikely in our dataset. A detailed review ofchemotherapeutic regimens was performed on the subtotalresection group. Whereas the specifics of administrationdiffered, most of the regimens could be classified as eitherprocarbazine-, lomustine-, vincristine-, or temozolamide-basedchemotherapy. No difference in survival (P = 0.9) was seen inthese two groups, suggesting that the treatment differences didnot have a significant impact on the associations of YKL-40 withsurvival.
Finally, to place YKL-40 expression in the context ofpreviously established recurring genetic lesions, we comparedYKL-40 expression with two of the commonly describedgenetic aberrations in glioblastoma: amplification of EGFRand loss of chromosome 10. Whereas there was no significantassociation between YKL-40 and EGFR amplification status,
www.aacrjournals.orgClin Cancer Res 2005;11(9) May1, 2005 3332
Table 3. Univariate overall survival analysis of thegross totally resected group
FactorMedian overallsurvival (weeks) P
YKL-40 score0 1161+ 53 0.00082+ 41
Age<50 years 78 0.04z50 years 47
KPS90-100 5670-80 40 0.007<70 2
Fig. 5. YKL-40 and survival. A and B,Kaplan-Meier survival curves comparingYKL-40 expressionwith overall survival innewly diagnosed glioblastoma. A , subtotalresection group (n = 147, P = 0.02).B, gross total resection group (n = 140,P = 0.0008). C,YKL-40 expression scoreandmedian survival for all patients(subtotal resection and gross-totalresection groups, n = 287) stratified bythe RTOGRPA classification (P = 0.009).
Imaging, Diagnosis, Prognosis
Research. on June 11, 2020. © 2005 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

we identified a correlation between higher YKL-40 stainingand loss of chromosome 10. This finding, in addition to thesurvival associations, independently confirms the results froma concurrent expression profiling/array comparative genomichybridization study, which identified YKL-40 as a potentialprognostic marker in a set of 34 glioblastomas. Thecorrelation between DNA-based and mRNA-based changesshown in that study indicated that loss of chromosome 10was associated with altered expression of a subset of genesacross the genome. YKL-40 was among the genes most highlylinked with chromosome 10 status (39). The larger study inthis article supports the hypothesis that chromosome 10 statusis a marker for a subset of glioblastomas and has genetic and
clinical implications, including YKL-40 overexpression andpotentially more aggressive behavior. The YKL-40 gene islocated on a region of chromosome 1q that is not known forfrequent DNA copy number aberrations in glioblastoma. Ourdata suggest that its primary mode of up-regulation is at thetranscriptional level. The relationships between loss ofchromosome 10 and altered expression of YKL-40, andpotentially additional important genes in glioblastoma,remains to be determined.
Acknowledgments
We thankJoann Aaron for editorial assistance.
www.aacrjournals.org Clin Cancer Res 2005;11(9) May1, 20053333
References1.Walker MD, Alexander E Jr, HuntWE, et al. Evaluationof BCNU and/or radiotherapy in the treatment of ana-plastic gliomas. A cooperative clinical trial. J Neu-rosurg1978;49:333^43.2.Walker MD, Green SB, Byar DP, et al. Randomizedcomparisons of radiotherapy and nitrosoureas for thetreatment of malignant glioma after surgery. N Engl JMed1980;303:1323^9.3.MohanDS, SuhJH, PhanJL, et al. Outcome in elderlypatients undergoing definitive surgery and radiationtherapy for supratentorial glioblastoma multiforme ata tertiary care institution. Int JRadiat Oncol Biol Phys1998;42:981^7.4. Burger PC, Green SB. Patient age, histologic features,and length of survival in patients with glioblastomamultiforme. Cancer1987;59:1617^25.5. Scanlon PW,TaylorWF. Radiotherapy of intracranialastrocytomas: analysis of 417 cases treated from1960 through1969. Neurosurgery1979;5:301^8.6.Wallner KE, Galicich JH, Krol G, Arbit E, Malkin MG.Patterns of failure following treatment for glioblastomamultiforme and anaplastic astrocytoma. Int J RadiatOncol Biol Phys1989;16:1405^9.7.Massey V, Wallner KE. Patterns of second recurrenceof malignant astrocytomas. Int J Radiat Oncol BiolPhys1990;18:395^8.8. Hochberg FH, Pruitt A. Assumptions in the radio-therapy of glioblastoma. Neurology1980;30:907^11.9. Barker FG Jr, Chang SM, Larson DA, et al. Age andradiation response in glioblastoma multiforme. Neuro-surgery 2001;49:1288^97; discussion 97^8.10. Huhn SL, Mohapatra G, Bollen A, et al. Chromo-somal abnormalities in glioblastoma multiforme bycomparative genomic hybridization: correlation withradiation treatment outcome. Clin Cancer Res 1999;5:1435^43.11. Barker FG Jr, Simmons ML, Chang SM, et al. EGFRoverexpression and radiation response in glioblasto-ma multiforme. Int J Radiat Oncol Biol Phys 2001;51:410^8.12. Boot RG, van Achterberg TA, van Aken BE, et al.Strong induction of members of the chitinase familyof proteins in atherosclerosis: chitotriosidase andhuman cartilage gp-39 expressed in lesion macro-phages. Arterioscler Thromb Vasc Biol 1999;19:687^94.13. Clancy R. Nitric oxide alters chondrocyte functionby disrupting cytoskeletal signaling complexes.Osteoarthritis Cartilage1999;7:399^400.14. De Ceuninck F, Gaufillier S, Bonnaud A, et al. YKL-40 (cartilage gp-39) induces proliferative eventsin cultured chondrocytes and synoviocytes andincreases glycosaminoglycan synthesis in chondro-cytes. Biochem Biophys Res Commun 2001;285:926^31.15. Garnero P, Piperno M, Gineyts E, et al. Crosssectional evaluation of biochemical markers of bone,cartilage, and synovial tissue metabolism in patientswith knee osteoarthritis: relationswith disease activityand joint damage. Ann RheumDis 2001;60:619^26.
16. Nordenbaek C, Johansen JS, Junker P, et al. YKL-40, a matrix protein of specific granules in neutrophils,is elevated in serum of patients with community-acquired pneumonia requiring hospitalization. J InfectDis1999;180:1722^6.17. Volck B, Price PA, Johansen JS, et al. YKL-40,a mammalian member of the chitinase family, is amatrix protein of specific granules in human neutro-phils. Proc Assoc Am Physicians1998;110:351^60.18. Bernardi D, Podswiadek M, Zaninotto M, Punzi L,Plebani M. YKL-40 as a marker of joint involvementin inflammatory bowel disease. Clin Chem 2003;49:1685^8.19. Johansen JS, Baslund B, Garbarsch C, et al. YKL-40 in giant cells and macrophages from patientswith giant cell arteritis. Arthritis Rheum 1999;42:2624^30.20. Koutroubakis IE, Petinaki E, Dimoulios P, et al.Increased serum levels of YKL-40 in patients withinflammatory bowel disease. Int J Colorectal Dis2003;18:254^9.21. La Montagna G, D’Angelo S, Valentini G. Cross-sectional evaluation of YKL-40 serum concentrationsin patients with systemic sclerosis. Relationshipwith clinical and serological aspects of disease.JRheumatol 2003;30:2147^51.22. Peltomaa R, Paimela L, Harvey S, HelveT, Leirisalo-Repo M. Increased level of YKL-40 in sera frompatients with early rheumatoid arthritis: a new markerfor disease activity. Rheumatol Int 2001;20:192^6.23.Vind I, Johansen JS, Price PA, Munkholm P. SerumYKL-40, a potential new marker of disease activity inpatients with inflammatory bowel disease. Scand JGastroenterol 2003;38:599^605.24.Volck B, Johansen JS, Stoltenberg M, et al. StudiesonYKL-40 in knee joints of patients with rheumatoidarthritis and osteoarthritis. Involvement of YKL-40 inthe joint pathology. Osteoarthritis Cartilage 2001;9:203^14.25. Cintin C, Johansen JS, Christensen IJ, et al. SerumYKL-40 and colorectal cancer. Br J Cancer 1999;79:1494^9.26. Hogdall EV, JohansenJS, Kjaer SK, et al. High plas-maYKL-40 level in patients with ovarian cancer stageIII is related to shorter survival. Oncol Rep 2003;10:1535^8.27. Dehn H, Hogdall EV, Johansen JS, et al. PlasmaYKL-40, as a prognostic tumor marker in recurrentovarian cancer. Acta Obstet Gynecol Scand 2003;82:287^93.28. Johansen JS, Christensen IJ, Riisbro R, et al. HighserumYKL-40 levels in patients with primary breastcancer is related to short recurrence free survival.Breast Cancer ResTreat 2003;80:15^21.29. Jensen BV, Johansen JS, Price PA. High levels ofserum HER-2/neu and YKL-40 independently reflectaggressiveness of metastatic breast cancer. ClinCancer Res 2003;9:4423^34.30. Tanwar MK, Gilbert MR, Holland EC. Gene expres-sion microarray analysis reveals YKL-40 to be a
potential serum marker for malignant character inhuman glioma. Cancer Res 2002;62:4364^8.31.Barker FGJr, PradosMD,ChangSM, et al. Radiationresponse and survival time in patients with glio-blastoma multiforme. JNeurosurg1996;84:442^8.32. Shaw EG, SeiferheldW, Scott C, et al. Reexaminingthe Radiation Therapy Oncology Group (RTOG)recursive partitioning analysis (RPA) for glioblastomamultiforme (GBM) patients. Int J Radiat Oncol BiolPhys 2003;57:S135^6.33. Simmons ML, Lamborn KR, Takahashi M, et al.Analysis of complex relationships between age, p53,epidermal growth factor receptor, and survival inglioblastoma patients. Cancer Res 2001;61:1122^8.34. Smith JS, Tachibana I, Passe SM, et al. PTENmutation, EGFRamplification, andoutcome inpatientswith anaplastic astrocytoma and glioblastomamultiforme. JNatl Cancer Inst 2001;93:1246^56.35. Hegi ME, Diserens AC, Godard S, et al. Clini-cal trial substantiates the predictive value of O-6-methylguanine-DNA methyltransferase promotermethylation in glioblastoma patients treated withtemozolomide.ClinCancerRes 2004;10:1871^4.36. Shostak K, Labunskyy V, Dmitrenko V, et al. HCgp-39 gene is upregulated in glioblastomas. CancerLett 2003;198:203^10.37. Mohapatra G, Bollen AW, Kim DH, et al. Geneticanalysis of glioblastomamultiforme provides evidencefor subgroups within the grade. Genes ChromosomesCancer1998;21:195^206.38. von Deimling A, von Ammon K, Schoenfeld D, et al.Subsets of glioblastomamultiforme defined bymolec-ular genetic analysis. Brain Pathol1993;3:19^26.39. Nigro JM, Misra A, Zhang L, et al. Integrated CGH-array and expression array profiles identify clinicallyrelevant molecular subtypes of glioblastoma. CancerRes 2004; In press.40. Recklies AD,White C, Ling H. The chitinase 3-likeprotein human cartilage glycoprotein 39 (HC-gp39)stimulates proliferation of human connective-tissuecells and activates both extracellular signal-regulatedkinase-andprotein kinaseB-mediated signallingpath-ways. BiochemJ 2002;365:119^26.41. Kleihues PBP, CollinsVP, Newcomb EW, Ohgaki H,CaveneeWK. Glioblastoma. In: CW Kleihues P, editor.Pathology and genetics of tumours of the nervoussystem, 1st ed.Vol.1. Lyon, France: IARCPress; 2000.p. 29^39.42. Ling H, Recklies AD. The chitinase 3-like proteinhuman cartilage glycoprotein 39 inhibits cellularresponses to the inflammatory cytokines interleukin-1and tumour necrosis factor-a. Biochem J 2004;380:651^9.43. Shapiro WR, Green SB, Burger PC, et al.Randomized trial of three chemotherapy regimensand two radiotherapy regimens and two radiotherapyregimens in postoperative treatment of malignantglioma. Brain Tumor Cooperative Group Trial 8001.JNeurosurg1989;71:1^9.44. Johansen JS, Jensen HS, Price PA. A new
YKL-40 and Radiation Response in Glioblastoma
Research. on June 11, 2020. © 2005 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

www.aacrjournals.orgClin Cancer Res 2005;11(9) May1, 2005 3334
biochemicalmarker for joint injury. Analysis ofYKL-40in serum and synovial fluid. Br J Rheumatol 1993;32:949^55.45. Oz B, Karayel FA, Gazio NL, Ozlen F, Balci K. Thedistribution of extracellular matrix proteins andCD44S expression in human astrocytomas. PatholOncol Res 2000;6:118^24.46. Johansen JS, OleeT, Price PA, et al. Regulation ofYKL-40 production by human articular chondrocytes.Arthritis Rheum 2001;44:826^37.
47. Kawasaki M, HasegawaY, Kondo S, Iwata H. Con-centration and localization of YKL-40 in hip joint dis-eases. JRheumatol 2001;28:341^5.48.Marijnen C, van der Berg S, van Duinen S,ThomeerR, Noordijk E. Radiotherapy is effective in patientswith glioblastomamultiformewith a very limitedprog-nosis and in patients above 70 years of age. Int JRadiat Oncol Biol Phys 2003;57:S328.49. Kristiansen K, Hagen S, KollevoldT, et al. Combinedmodality therapy of operated astrocytomas grade III
and IV. Confirmationof the value of postoperative irra-diation and lack of potentiation of bleomycin on sur-vival time: a prospective multicenter trial of theScandinavian Glioblastoma Study Group. Cancer1981;47:649^52.50.Wood JR, Green SB, Shapiro WR. The prognosticimportance of tumor size in malignant gliomas: acomputed tomographic scan study by the BrainTumor Cooperative Group. J Clin Oncol 1988;6:338^43.
Imaging, Diagnosis, Prognosis
Research. on June 11, 2020. © 2005 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
2005;11:3326-3334. Clin Cancer Res Christopher E. Pelloski, Anita Mahajan, Moshe Maor, et al. Radiation and Shorter Overall Survival in GlioblastomaYKL-40 Expression is Associated with Poorer Response to
Updated version
http://clincancerres.aacrjournals.org/content/11/9/3326
Access the most recent version of this article at:
Cited articles
http://clincancerres.aacrjournals.org/content/11/9/3326.full#ref-list-1
This article cites 48 articles, 12 of which you can access for free at:
Citing articles
http://clincancerres.aacrjournals.org/content/11/9/3326.full#related-urls
This article has been cited by 16 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. (CCC)Click on "Request Permissions" which will take you to the Copyright Clearance Center's
.http://clincancerres.aacrjournals.org/content/11/9/3326To request permission to re-use all or part of this article, use this link
Research. on June 11, 2020. © 2005 American Association for Cancerclincancerres.aacrjournals.org Downloaded from