year three, quarter three malaria diagnosis and …
TRANSCRIPT
YEAR THREE, QUARTER THREE MALARIA
DIAGNOSIS AND TREATMENT PROGRESS
REPORT: April –June 2018
Private Health Sector Project
The Private Health Sector Project is a technical assistance project to support the Government of Ethiopia.
The Private Health Sector Project is managed by Abt Associates Inc. and is funded by the United States Agency for
International Development (USAID), under Contract No. AID-663-LA-16-00001.
Recommended Citation Private Health Sector Project, Year Three, Quarter Three Report (April–June 2018)
Report on Diagnosis and Treatment of Malaria in Private Facilities. 20 July 2018. Rockville, MD. Private Health Sector
Project, Abt Associates.
Submitted to: Dr. Mesfin Tilaye
Agreement Officer’s Representative
Health Network Program Advisor
USAID| Ethiopia
Addis Ababa, Ethiopia
Submitted by: Dr. Mesfin Teferi, Chief of Party
USAID| Private Health Sector Project
Abt Associates Inc. 1 6130 Executive Blvd
1 Rockville, Maryland 20852 1 T. 301.347.5000 1 F. 301.913.9061
1 www.abtassociates.com
YEAR THREE, QUARTER THREE
MALARIA DIAGNOSIS AND TREATMENT
PROGRESS REPORT
DISCLAIMER
The author’s views expressed in this publication do not necessarily reflect the views of the United States
Agency for International Development (USAID) or the United States Government

i
CONTENTS
Acronyms ................................................................................. 3
1. Program description ................................................... 4
1.1 General Overview ........................................................................... 4
1.2 Strategies ........................................................................................... 4
1.3 Objectives ......................................................................................... 4
2. Performance report .................................................... 5
2.1 Working with the Private Health Facilities ............................... 5
2.2 Working with work place facilities ............................................. 5
2.3 Clinical seminars .............................................................................. 6
2.4 Case management training ............................................................ 6
2.5 Site visit and Support ...................................................................... 7
2.5.1 Gambella region visit by central team .......................... 7
2.6 Summary of JSS findings from other regions ............................ 9
2.7 Onsite orientation to regional PHSP and PHFA program
officers ............................................................................................. 10
2.8 Malaria laboratory support ......................................................... 10
2.9 DQAs ............................................................................................... 11
2.10 Research ................................................................................... 11
2.11 Service Delivery ...................................................................... 12
2.12 Other activities ....................................................................... 16
3. Challenges .................................................................. 16
4. Major activities for year three, quarter Four ......... 16
Annex A: Malaria Program Activity Matrix, Year Three,
QUARTER THREE April –June 2018................................... 17
Annex B: List of facilities reported in Quality1mprovement
for Malaria diagnosis and treatment ................................... 19

ii
List of Tables
Figure 1: Malaria case management training for FDRE sugar corporation
workers, 7-11 May 2018 .....................................................................7
Table 1: JSS Summary (April –June 2018) .......................................................9
Table 2: Malaria Diagnosis and Treatment at Private Health Facilities
(April –June 2018) .............................................................................. 12
table 3: Malaria cases treated, admitted, and referred and malaria-
related deaths in private health facilities (January-March 2018)
................................................................................................................. 13
Table 4: Malaria cases by age and sex in PHSP-supported facilities (April
–June 2018) .......................................................................................... 14
List of Figures
Figure 1: Malaria case management training for FDRE sugar corporation
workers, 7-11 May 2018 .....................................................................7
Figure 2: Trends In Malaria Diagnosis and Treatment at Project-Assisted
Private Facilities, Jul 017_to June 2018 ......................................... 15
3
ACRONYMS
AL Artemether lumefantrine
CQ Chloroquine
EPHI
EQA
DQA
FDRE
FMOH
HMIS
Ethiopian Public Health Institute
External Quality Assurance
Data Quality Assessment
Federal Democratic Republic of Ethiopia
Federal Ministry of Health
Health Management Information System
IEC Information, Education and Communication
IG Implementation Guidelines
JSS Joint Supportive Supervision
OPD
PHEM
PFSA
PHFA
Out-patient Department
Public Health Emergency Management
Pharmaceuticals Fund and Supply Agency
Private Health Facility Association
PHSP Private Health Sector Project
PMI President’s Malaria Initiative
PPM Public-private Mix
PQ Primaquine
PT Panel Testing
RDT Rapid Diagnostic Test
RHB
RRF
Regional Health Bureau
Requesting and reporting form
RRL Regional Reference Laboratory
SNNPR Southern Nations, Nationalities, and Peoples Region
TAC Technical Advisory Committee
TB
USAID
Tuberculosis
United State Agency for International Development
4
1. PROGRAM DESCRIPTION
1.1 General Overview
The Private Health Sector Project (PHSP) is a United States Agency for International Development
(USAID)-funded project, with partial funding from the President’s Malaria Initiative (PMI). The project
provides technical assistance to enable private and workplace health facilities in Ethiopia to provide
quality malaria diagnosis and treatment. In the reporting period (April-June 2018) , the project provided
technical support to 163 facilities (15 in Afar, 28 in Amhara, 15 in Benishangul Gumuz, 14 in Dire Dawa,
12 in Gambella, 32 in Oromia, 19 in Southern Nations, Nationalities, and Peoples Region [SNNPR], and
28 in Tigray). Within the same period, these facilities tested 86,309 patients suspected for malaria,
diagnosed 14,846 patients, and treated them accordingly. During the next quarter, PHSP will continue
supporting those facilities to provide standard and quality malaria diagnosis and treatment services.
1.2 Strategies
The project pursues the following strategies to achieve its goals:
Conducting policy dialogue with Regional Health Bureaus (RHBs) to engage private facilities in
public-private mix (PPM)-based malaria case management, policy dialogue, and advocacy.
Conducting rapid assessments to map the geographic distribution of the migrant and mobile
work force.
Developing a PPM implementation guideline for malaria prevention and control through the
private health sector.
Building the capacity of health providers (case managers, laboratory and pharmacy/supply chain
professionals, ) through team training, joint supportive supervision (JSS), and mentoring.
Supporting implementation of PPM to expand the number of service sites offering malaria care.
Providing technical assistance to the Federal Ministry of Health’s (FMOH) malaria program.
Working through partnerships with other stakeholders to improve access to effective and
efficient malaria care services.
1.3 Objectives
The malaria component of the project has the following objectives:
Increase access to and uptake of malaria services in private health facilities.
Enhance capacity of local partners to ensure the sustainability of PPM partnerships.
Enhance pharmaceutical supply chain management and rational drug use at private health
facilities, including work places.
Enhance program learning and innovative ventures in malaria care and treatment.
5
Generate evidence on malaria service needs of the migrant and mobile workforce for decision
making and programming.
2. PERFORMANCE REPORT
2.1 Working with the Private Health Facilities
During the reporting period (April – June 2018), PHSP continued supporting the 163 private and work
place health facilities in all regions of the country, except Somalia, Harari, and Addis Ababa city
administrative state.
2.2 Working with work place facilities
PHSP continued supporting 12 Federal Democratic Republic of Ethiopia (FDRE) Sugar corporation
health facilities and other nine work place health facilities located in Amhara, Afar, Oromiya, SNNPR and
Tigray regions. These facilities are serving large number of permanent and seasonal migrant workers
who are at high risk of malaria as most of the places are stratified in the high risk category.
The 12 FDRE Sugar Corporation have around 21,842 permanent employees and 42,378 seasonal and
migrant workers and the health facilities with different structures in the factories are providing the
malaria diagnosis and treatment services for a total population 256,880 peoples.
The other 9 work place facilities have a total number 7,383 permanent and 78,758 seasonal workers and
the health facilities are serving for more than 100,000 total population.
Working with FMOH, RHBs, and Stakeholders
PHSP carried out the following activities with the FMOH, RHBs, and other stakeholders during the
reporting period:
Attended the Technical Advisory Committee (TAC) meeting where updates of the program
were shared and successfully advocated with the TAC about the benefits of having a PPM-
malaria IG policy document
Federal Ministry of Health established a task force to develop PPM-malaria Implementation
Guidelines document. The task force is composed of representatives from the following
partners: FMOH, USAID/PMI, ICAP, Transform PHCP, WHO, UNICEF and PHSP.
Developed the PPM-malaria Implementation Guidelines draft document and shared with the task
force to enrich their work further.
Attended the annual USAID/MOP meeting and presented the project performance and future
plans.
Facilitated the USAID/PMI PPM-malaria facility visit in Gambella by preparing brief documents,
demonstrating the performance of the project in the supported facilities, and gathered
important feedback to improve future project implementation.
Attended a workshop of “Annual review meeting on TB, HIV and Malaria external quality
6
assurance (EQA)” organized by EPHI. During the workshop, PHSP emphasized the significance
of integrating the malaria EQA with the well-established TB EQA in all private health facilities.
During the workshop participants reached the following consensuses:
1. Improve the EQA system of malaria.
2. Implement the malaria EQA in all government and private health facilities.
3. Strengthen the capacity and competency of regional laboratories and EQA centers
through Panel Testing (PT) and international trainings.
4. Revise and prepare standard training materials on malaria laboratory.
5. Revise the curricular structure on malaria and tuberculosis (TB) microscopy.
2.3 Clinical seminars
The project conducted five sessions of a one day clinical seminar in Hawassa, Humera, Awash, Assosa
and Gambella to 121 physicians and health officers working in the out-patient departments (OPDs). The
aim of the seminar was to update targeted clinicians with the new malaria diagnosis and management
process and to share with the providers the important parameters that can be used to monitor the
malaria program in their facilities.
2.4 Case management training
In collaboration with the FMOH and FDRE Sugar Corporation, the project organized a training to build
the capacity of clinicians and laboratory workers and provided one round of the recent malaria case
management training in Adama.
Objectives of the training:
Build the capacity of the clinicians to provide quality and standard clinical care for patients with
malaria, and update the other staff with a one day orientation session within the facility.
Build the capacity of laboratory professionals from the same facilities to improve their skills in
malaria microscopy and synchronize with the standards.
The outcome of the training:
A total of 30 clinicians (27 males and three females) and 12 laboratory professionals from the 12
FDRE Sugar Corporation health facilities attended and completed the training.
The full packages of the training materials and a one day update orientation document were
given in hard and soft copies.
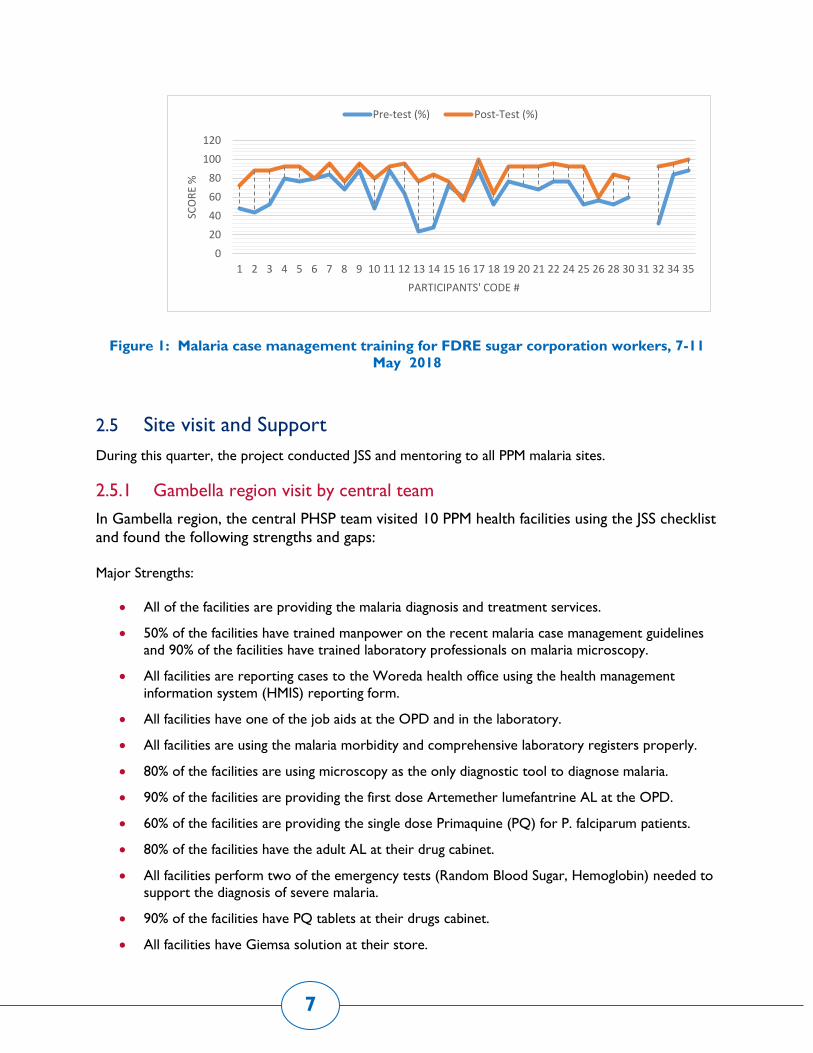
All trainees received post- test and 27 (90%) of them scored the minimum requirement for
certification.
After receiving the training, the trainees provided a one day update orientation session to 256
professionals within their facility.
7
Figure 1: Malaria case management training for FDRE sugar corporation workers, 7-11
May 2018
2.5 Site visit and Support
During this quarter, the project conducted JSS and mentoring to all PPM malaria sites.
2.5.1 Gambella region visit by central team
In Gambella region, the central PHSP team visited 10 PPM health facilities using the JSS checklist
and found the following strengths and gaps:
Major Strengths:
All of the facilities are providing the malaria diagnosis and treatment services.
50% of the facilities have trained manpower on the recent malaria case management guidelines
and 90% of the facilities have trained laboratory professionals on malaria microscopy.
All facilities are reporting cases to the Woreda health office using the health management
information system (HMIS) reporting form.
All facilities have one of the job aids at the OPD and in the laboratory.
All facilities are using the malaria morbidity and comprehensive laboratory registers properly.
80% of the facilities are using microscopy as the only diagnostic tool to diagnose malaria.
90% of the facilities are providing the first dose Artemether lumefantrine AL at the OPD.
60% of the facilities are providing the single dose Primaquine (PQ) for P. falciparum patients.
80% of the facilities have the adult AL at their drug cabinet.
All facilities perform two of the emergency tests (Random Blood Sugar, Hemoglobin) needed to
support the diagnosis of severe malaria.
90% of the facilities have PQ tablets at their drugs cabinet.
All facilities have Giemsa solution at their store.
0
20
40
60
80
100
120
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 24 25 26 28 30 31 32 34 35
SCO
RE
%
PARTICIPANTS' CODE #
Pre-test (%) Post-Test (%)

8
All facilities have slides box and started to store slides for rechecking.
100% of the facilities were involved during the first malaria laboratory EQA in the region.
Major gaps:
None of the facilities are reporting using the public health emergency management (PHEM)
reporting system.
Two facilities (20%) are using both rapid diagnosis test (RDT) and microscopy to diagnose
malaria.
Two facilities are using PQ for the radical cure purposes.
Five facilities (50%) are giving treatment clinically for slide negative uncomplicated cases.
Not all facilities are determining parasite load.
70% of the facilities do not have the paediatric AL formulations.
Data discrepancy between the two registers and the monthly HMIS reports.
Only 40% of the facilities had the Artesunate injection during the supervision time.
Only 30% of the facilities had methanol, and none of them are performing thin smear.
Some facilities are not storing the anti-malaria drugs in a lockable cabinet, and only one facility is
storing the prescription of the anti-malaria drugs for auditing.
Facilities were using Artesunate injection for non- complicated cases.
Actions taken:
Clinical seminar, onsite orientation and support given to the clinicians, focal persons and the
laboratory professionals based on the identified technical and other gaps.
Discussed with the regional staffs and agreed on the following action points:
o Distribute methanol solution once the regional laboratory receives it.
o Provide the important anti-malaria drugs without any bureaucratic issues to the PPM
facilities based on the requesting and reporting form (RRF).
o Provide the EQA feedback to each facility.
o Continue doing the EQA every quarter.
o Accommodate the PPM facilities during the regional JSS.
o Disaggregate the data of the private facilities’ contribution during the HMIS report to the
FMOH.
o Facilitate the referral linkage between the PPM facilities and Gambella Hospital.
o Recruit a potential temporary mentor who will assist the project in close follow up of the
program activities.
o Identify new private facilities in the city and nearby cities who will be assessed for
enrolment by the project.
9
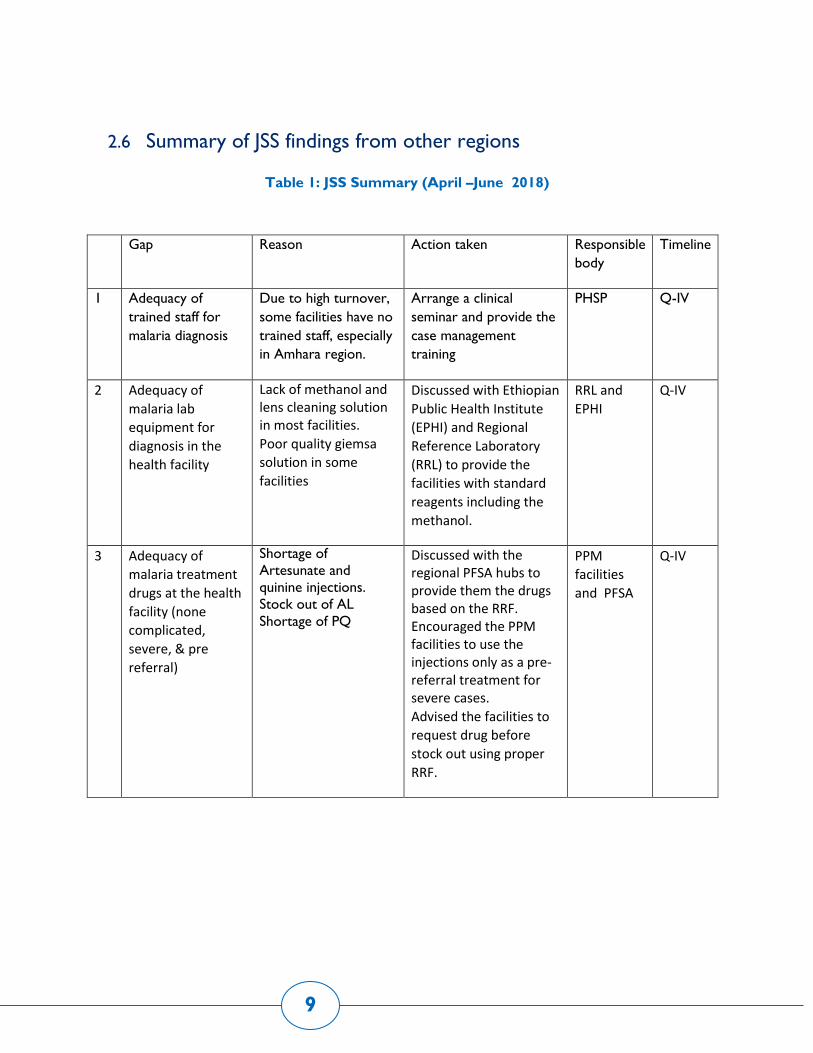
2.6 Summary of JSS findings from other regions
Table 1: JSS Summary (April –June 2018)
Gap Reason Action taken Responsible
body
Timeline
1 Adequacy of
trained staff for
malaria diagnosis
Due to high turnover,
some facilities have no
trained staff, especially
in Amhara region.
Arrange a clinical
seminar and provide the
case management
training
PHSP Q-IV
2 Adequacy of
malaria lab
equipment for
diagnosis in the
health facility
Lack of methanol and lens cleaning solution in most facilities.
Poor quality giemsa
solution in some
facilities
Discussed with Ethiopian
Public Health Institute
(EPHI) and Regional
Reference Laboratory
(RRL) to provide the
facilities with standard
reagents including the
methanol.
RRL and
EPHI
Q-IV
3 Adequacy of
malaria treatment
drugs at the health
facility (none
complicated,
severe, & pre
referral)
Shortage of
Artesunate and
quinine injections.
Stock out of AL
Shortage of PQ
Discussed with the regional PFSA hubs to provide them the drugs based on the RRF. Encouraged the PPM facilities to use the injections only as a pre-referral treatment for severe cases.
Advised the facilities to
request drug before
stock out using proper
RRF.
PPM
facilities
and PFSA
Q-IV

10
2.7 Onsite orientation to regional PHSP and PHFA program officers
The Central PHSP team provided onsite orientation on the major clinical updates, newly developed
supportive supervision and mentoring checklists, and onsite demonstrations on how to utilize the
checklists to PHSP regional program officers and PHFAs in SNNPR region.
The aim of the orientation was:
To update their knowledge with the recently revised malaria case management guidelines.
To start utilizing the checklists for the upcoming supervisions and mentoring.
Refresh on the basics of supervision and mentoring activities.
2.8 Malaria laboratory support
Training on Malaria Microscopy:
Provided malaria microscopy training for 30 laboratory professionals (M=26, F=4) selected from
Afar, Amhara, Oromia, Tigray, & SNNPR private and work place health facilities.
Provision of Job aids
Malaria Microscopy Job aids, WHO bench aids and SOPs were provided to Gambella and
Benishangul Gumuz PPM malaria sites.
Supportive supervision findings of the malaria laboratory diagnosis
Supportive supervision was conducted in 71 private health facilities in Amhara Oromia and SNNP
regions.
The comprehensive laboratory register is available in 80% of the health facilities.
WHO bench aid, SOPs and other provider support tools are available in 50% of the private
facilities.
All facilities are not doing thin film..
Very low malaria microscopy EQA coverage/participation..
Shortage of microscope cleaning solution and methanol/ethanol in most facilities.
Many health facilities are not performing IQC with known positive and negative slides.

11
Malaria EQA
PHSP supported Gambella and Benishangul Gumuz regional laboratories to run the first malaria
microscopy EQA in the regions. A total of 27 PPM-malaria facilities (15 in Benishangul Gumuz &
12 in Gambella regions) have received onsite evaluation and random slide rechecking.(Detailed
findings presented in The following figure)
Figure: malaria microscopy service onsite evaluation EQA result at Private health clinics
in Gambella town May, 2010 E.C.
Afar RHB has already integrated the EQA system into the private sector and 15 PPM malaria
facilities received random slide rechecking and corresponding feedback.
The project attended the annual EQA meeting and reflected on the gap of EQA in the private
sector and a final strong direction by FMOH and EPHI to accommodate all the PPM malaria sites
during the regional laboratory quarterly EQA program.
2.9 DQAs
PHSP reviewed the data quality of Year Three Quarter One and Two by crosschecking the reported
findings with the recount findings in 11 facilities from Amhara, Oromiya and SNNPR regions. During the
process there was no disparity between the reported and recounted number of identified and treated
number of malaria cases in the facilities.
2.10 Research
In close collaboration with PMI, PHSP completed the first draft report of the research on “Monitoring of
human and mosquito behavior and attitudes towards malaria prevention and treatment in agricultural
development areas in Ethiopia”, and shared with all responsible personnel to comment on the report
before submitting for publications. Per PMI’s feedback, PHSP is expanding the research to include
implementation strategies and preparing a manuscript for publication. The project will also disseminate
the study findings to all stakeholders.
0102030405060708090
100
100
91.7
95
0 50.0
0
75.0
0
8.3
100
100
10075.0
91.7
0
91.7
85.7
78.5
83.5
91.7
0
8.3
5
100
50.0
100
25.0
100
91.7
0 0 025.0
8.3
100
8.3 14.3
21.5
17.5
8.3
Per
form
an
ce i
n %
Items/Practices
Ye…

12
2.11 Service Delivery
As mentioned above, PHSP provided technical support to facilities through training, site-level support, and linkage to anti-malarial commodity
supplies. During the quarter, 163 project-supported facilities reported and the performance is summarized in the following tables and figures.
Table 2: Malaria Diagnosis and Treatment at Private Health Facilities (April –June 2018)
Region
All
malaria
suspected
cases
Total
cases
Microscopy RDT Percent
confirmation
Dx TBF Pos % PF PV Mixed TRDT Pos % PF PV Mixed
Afar 6672 789 6515 739 11.3 457 251 13 157 50 31.8 33 17 0 100%
Amhara 17732 1140 17225 1057 6.1 576 422 59 507 83 16.4 42 36 5 100%
Beneshangul
Gumuz 11518 3558 11518 3558 30.9 1687 1866 5 0 0 0 0 0 0
100%
Dire Dawa 933 52 933 52 5.6 34 18 0 0 0 0 0 0 0 100%
Gambella 8054 4766 8054 4766 59.2 4124 498 144 0 0 0 0 0 0 100%
Oromia 17686 440 16983 409 2.4 168 230 11 703 31 4.4 20 11 0 100%
SNNPR 17501 2982 17265 2903 16.8 1683 1031 189 236 79 33.5 53 26 0 100%
Tigray 6213 1119 5585 853 15.3 426 419 8 628 266 42.4 224 33 9 100%
Total 86309 14846 84078 14337 17.1 9173 4735 429 2231 509 22.8 372 123 14 100%
NB: TBF=total blood film, pos=positive , Dx=diagnosis, PF=plasmodium falciparum, PV=plasmodium vivax, TRDT=total rapid diagnostic tests

13
Table 3: Malaria cases treated, admitted, and referred and malaria-related deaths in private health facilities (January-March
2018)
NB: CQ=chloroquine, AL=artemether lumefantrine, AM=artemether
Region Total Cases Total
treated
Treated Number of Malaria cases
AL CQ Quinine AM Artesunate Admitted Referred Deaths
Afar 789 789 482 268 0 32 7 0 0 0
Amhara 1140 1140 610 456 0 73 1 0 0 0
Beneshangul Gumuz 3558 3558 1687 1852 0 19 0 0 0 0
Dire Dawa 52 52 31 18 0 0 3 0 1 0
Gambella 4766 4766 4268 498 0 0 0 0 0 0
Oromia 440 440 183 235 5 8 9 0 1 0
SNNPR 2982 2982 1761 1061 52 24 84 0 9 0
Tigray 1119 1119 577 452 0 84 6 0 0 0
Total 14846 14846 9599 4840 57 240 110 0 11 0

14
Table 4: Malaria cases by age and sex in PHSP-supported facilities (April –June 2018)
Region Total Cases
treated
Age in Years and Sex Disaggregation
< 5 5 - 14 >=15 PW*
Total
Male Female Male Female Male Female Male Female
Afar 789 39 29 66 27 421 207 0 526 263
Amhara 1140 76 63 96 67 520 318 1 692 448
Beneshangul Gumuz 3558 574 441 287 298 969 989 20 1830 1728
Dire Dawa 52 1 1 2 1 31 16 0 34 18
Gambella 4766 452 338 303 259 1686 1728 3 2441 2325
Oromia 440 25 10 35 27 218 125 0 278 162
SNNPR 2982 103 160 463 502 1063 691 1 1629 1353
Tigrai 1119 51 30 99 69 614 256 0 764 355
All Regions 14846 1321 1072 1351 1250 5522 4330 25 8194 6652

15
Figure 2: Trends In Malaria Diagnosis and Treatment at Project-Assisted Private Facilities, Jul 017_to June 2018
10771
21914 2255021202
11103
14846
10113
20,738
2255021185
11103
14846
75.0%
80.0%
85.0%
90.0%
95.0%
100.0%
105.0%
0
5000
10000
15000
20000
25000
Jan_Mar17 Apr_Jun17 Jul_Spet17 Oct_dec17 Jan_March18 Apr_Jun18
% C
on
firm
ed
# o
f M
alar
ia C
ase
Diagnosed Malaria Treated Malaria % Confirmed Malaria

16
2.12 Other activities
Prepared a poster presentation slides for the East African private health sector forum.
3. CHALLENGES
A few PPM facilities in Gambella Region lack commitment and motivation.
Difficulty in accessing methanol and lens cleaning solutions by most of the PPM facilities.
Difficulty in getting all febrile cases from the registers.
Interrupted supplies of the anti-malaria drugs from PFSA.
Irrational use of the injectable Arthesunate.
Poor EQA coverage to the PPM facilities.
None
4. MAJOR ACTIVITIES FOR YEAR THREE, QUARTER
FOUR
Continue supporting the FMOH in the development of PPM Malaria Implementation Guidelines,
provision of training of trainer trainings.
Continue supporting the 163 health facilities to provide quality malaria services.
Provide two rounds of malaria case management trainings.
Provide clinical mentoring to the high yielding facilities.
Provide targeted and integrated supportive supervision to sample facilities in all regions.
Conduct a clinical seminar in Amhara region.
Strengthen the malaria EQA system by supporting the regional laboratories in high malaria
yielding facilities.
Disseminate the findings of the study on “Monitoring of human and mosquito behavior and
attitudes towards malaria prevention and treatment in agricultural development areas in
Ethiopia” and prepare the study report for dissemination.
Develop a pocket reference book for clinicians.
Assure the data quality by performing DQAs.
Organize a clinical seminar for clinicians working in Addis Ababa.
Discuss in the TAC meeting the development a standard supportive supervision and mentoring
checklist that also addresses the private sector.
Finalize the development and dissemination of the PPM malaria implementation guideline

17
ANNEX A: MALARIA PROGRAM ACTIVITY MATRIX, YEAR THREE,
QUARTER THREE APRIL –JUNE 2018
Indicator Indicator /output Planned
Achieved
1 Support the FMOH in the development of PPM
Malaria implementation guidelines
PPM-malaria
Implementation guideline 1 1
2 Conduct dissemination workshop on PPM- Malaria
Program IG
# of workshops organized 0
3 Participate in the National High Impact countries
Global Fund proposal development
# of workshops
organized attended
cancelled
4 Participate in and sponsor the national celebration
of World Malaria Day 2018
# of events/ proceedings 1 1
5 Provide parasitological diagnostic services to 98%
(393,310) of patients suspected (401,337) for
malaria in 214 supported health facilities
Proportion of
parasitological identified
malaria cases
>98% 100 %
6 Provide malaria treatment for 100% (62,929) of
malaria patients in the 168 facilities
% of patients who
received the malaria
treatment
100% 100 %
7 Provide two rounds of malaria case management
training for doctors, health officers and nurses.
# of training participants 60 30
8 Provide four rounds of four-day training on malaria
diagnosis to 140 Lab professionals # of training participants 60 30
9 Print and distribute different sets of job aids and
treatment guidelines to 214 private health facilities
(Lab Bench aids/guidelines/ clinical standard
operating procedures distributed)
# of facilities who
received and are using the
job aids
214 163
10 Conduct JSS # of facilities that received
JSS 2 1
11 Conduct clinical mentoring for the new regions # of facilities that received
mentoring 2 1
18
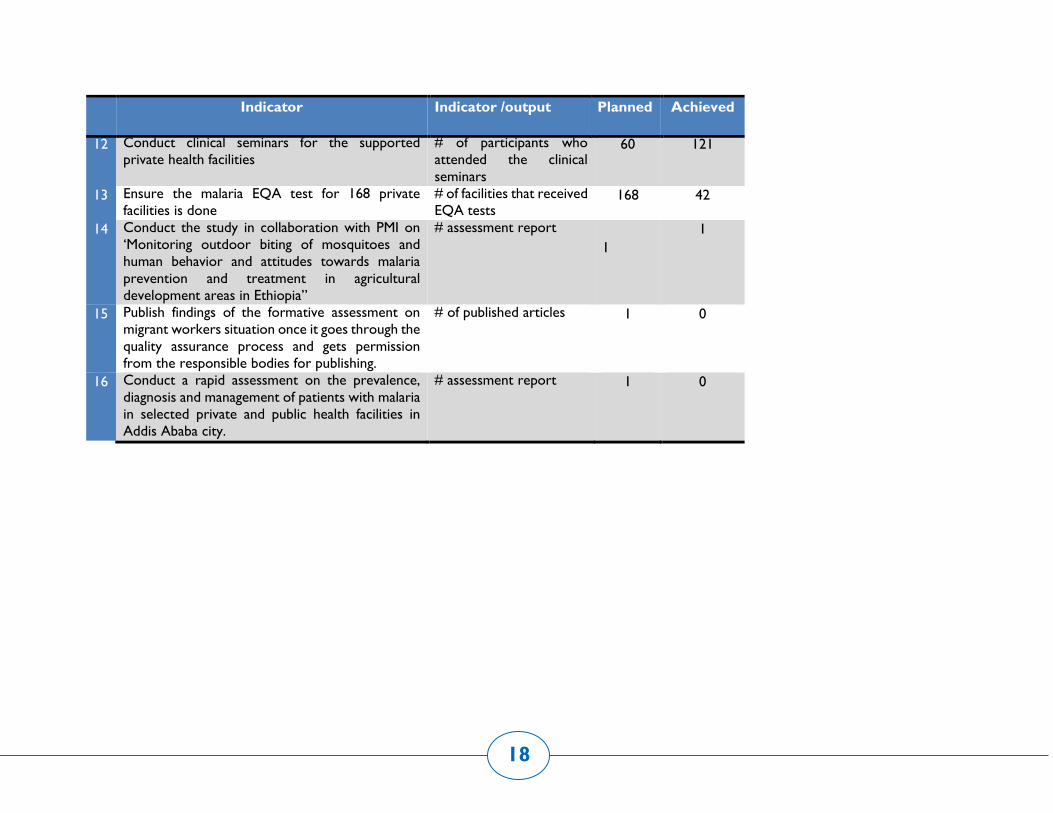
Indicator Indicator /output Planned
Achieved
12 Conduct clinical seminars for the supported
private health facilities
# of participants who
attended the clinical
seminars
60 121
13 Ensure the malaria EQA test for 168 private
facilities is done
# of facilities that received
EQA tests 168 42
14 Conduct the study in collaboration with PMI on
‘Monitoring outdoor biting of mosquitoes and
human behavior and attitudes towards malaria
prevention and treatment in agricultural
development areas in Ethiopia”
# assessment report
1
1
15 Publish findings of the formative assessment on
migrant workers situation once it goes through the
quality assurance process and gets permission
from the responsible bodies for publishing.
# of published articles
1 0
16 Conduct a rapid assessment on the prevalence,
diagnosis and management of patients with malaria
in selected private and public health facilities in
Addis Ababa city.
# assessment report
1 0

19
ANNEX B: LIST OF FACILITIES REPORTED IN QUALITY1MPROVEMENT FOR
MALARIA DIAGNOSIS AND TREATMENT
During the reporting period 100% supported facilities reported malaria data to town/woreda office based on the national requirements through
HMIS.
Region Malaria sites
supported
Malaria site reported (April
–June 2018)
Addis Ababa 0 0
Afar 15 15
Amhara 29 29
Beneshangul Gumuz 15 15
Dire Dawa 14 14
Gambella 12 12
Harari 0 0
Oromia 32 32
SNNPR 18 18
Tigray 28 28
Total 163 163
