www.cambridgehaematology.com haematology in primary care: the full blood count charles crawley...
TRANSCRIPT

www.cambridgehaematology.comwww.cambridgehaematology.com
Haematology in Primary Care:Haematology in Primary Care:The Full Blood CountThe Full Blood Count
Charles CrawleyCharles Crawley
George FollowsGeorge Follows
CCambridge ambridge HHaematology aematology PPartnersartners

www.cambridgehaematology.comwww.cambridgehaematology.com
The FBCThe FBC

www.cambridgehaematology.comwww.cambridgehaematology.com
HaemoglobinHaemoglobin Low haemoglobin defines anaemiaLow haemoglobin defines anaemia
– Males 13-18g/lMales 13-18g/l– Females 11.5-16g/lFemales 11.5-16g/l– Variations:Variations:
ChildrenChildren– Neonates – 14-24g/lNeonates – 14-24g/l– 2 months – 8.9-13.2g/l2 months – 8.9-13.2g/l– 9-12ys9-12ys - 11.5-15.4g/l - 11.5-15.4g/l
PregnancyPregnancy– 33rdrd Trimester – 9.8-13.7g/l Trimester – 9.8-13.7g/l
AgeAge– 5-75-7thth decade – falls in men rises in women decade – falls in men rises in women
ExerciseExercise– Increases HbIncreases Hb
AltitudeAltitude SmokingSmoking

www.cambridgehaematology.comwww.cambridgehaematology.com
MCVMCV Mean Cell VolumeMean Cell Volume: average size of RBC : average size of RBC
– Normal adult : 76 (80) - 100 fLNormal adult : 76 (80) - 100 fL MCV < 76 fLMCV < 76 fL (microcytic) (microcytic)
MCV > 100 fLMCV > 100 fL (macrocytic) (macrocytic)
MCV 80 - 100fLMCV 80 - 100fL (normocytic) (normocytic)

www.cambridgehaematology.comwww.cambridgehaematology.com
Practical Classification of AnaemiaPractical Classification of Anaemia
Microcytic Microcytic (<76fL)(<76fL) NormocyticNormocytic Macrocytic Macrocytic (>100)(>100)
Iron deficiencyIron deficiency
ThalassaemiaThalassaemia
HaemoglobinopathiesHaemoglobinopathies
Anaemia of chronic Anaemia of chronic diseasedisease
LeadLead
HyperthyroidismHyperthyroidism
Blood lossBlood loss
Haemolytic Haemolytic
- RBC membrane- RBC membrane
- Enzyme defects- Enzyme defects
- Extrinsic- Extrinsic
Stem cell defectsStem cell defects
MegaloblasticMegaloblastic
Excess alcoholExcess alcohol
HypothyroidHypothyroid
Liver diseaseLiver disease
ReticulocytosisReticulocytosis
Drug therapyDrug therapy
Marrow failureMarrow failure
Reticulocyte count: In the investigation of anaemia• Reduced: Failure of erythropoiesis
• Increased: Appropriate BM erythroid response

www.cambridgehaematology.comwww.cambridgehaematology.com
35 year Male35 year Male Hx:Hx: Lethargy, SOBLethargy, SOB Sx:Sx: PalePale FBC:FBC: HbHb 6.4 g/dL6.4 g/dL
MCV MCV 71 fL71 fL
RDWRDW 0.190.19
WCCWCC 5.25.2
PlateletsPlatelets 375375 Film: Severe hypochromasia and Film: Severe hypochromasia and
microcytosismicrocytosis

www.cambridgehaematology.comwww.cambridgehaematology.com
Commonest Causes Iron Commonest Causes Iron DeficiencyDeficiency
FemaleFemale MaleMale1 – 5 yr1 – 5 yr NutritionNutrition NutritionNutrition
5 – 15 yr5 – 15 yr Increased Increased utilisation/ utilisation/ growthgrowth
Increased Increased utilisation/ utilisation/ growthgrowth
15 – 40 yr15 – 40 yr MenstruationMenstruation
PregnancyPregnancyCoeliac disease Coeliac disease (Malabsorption)(Malabsorption)
> 40 yr> 40 yr Gastrointestinal Gastrointestinal Blood lossBlood loss
Gastrointestinal Gastrointestinal Blood lossBlood loss

www.cambridgehaematology.comwww.cambridgehaematology.com
Blood FilmBlood Film
www.cambridgehaematology.comwww.cambridgehaematology.com
Differential DiagnosisDifferential Diagnosis
Causes of microcytic hypochromic Causes of microcytic hypochromic anaemiaanaemia– Iron deficiencyIron deficiency
Blood lossBlood lossMalabsorption - Coeliac disease; gastrectomyMalabsorption - Coeliac disease; gastrectomy Increased utilisation - parasitesIncreased utilisation - parasitesDietary deficiency - rareDietary deficiency - rare
– HaemoglobinopathyHaemoglobinopathy– Anaemia of chronic diseaseAnaemia of chronic disease

www.cambridgehaematology.comwww.cambridgehaematology.com
Fe Deficiency vs Anaemia of Fe Deficiency vs Anaemia of Chronic DiseaseChronic Disease
VariableVariable Fe Fe deficiencydeficiency
Chronic Chronic diseasedisease
Serum IronSerum Iron
TransferrinTransferrin or Normalor Normal
Transferrin SaturationTransferrin Saturation
FerritinFerritin or Normalor Normal or normalor normal
CRPCRP NormalNormal
GIT studies: endoscopy etcGIT studies: endoscopy etc

www.cambridgehaematology.comwww.cambridgehaematology.com
26 year Female26 year Female Hx:Hx: Antenatal visit; Antenatal visit; First First
trimestertrimester FBC:FBC: HbHb 11.0 g/dL11.0 g/dL
MCVMCV 73 fL73 fL
MCHMCH 27 pg27 pg
RDWRDW 0.140.14
WCCWCC 8.5 x 108.5 x 1099/L/L
Platelets Platelets 164 x 10164 x 1099/L/L Film:Film: Microcytic RBCMicrocytic RBC

www.cambridgehaematology.comwww.cambridgehaematology.com
Fe Deficiency vs HbinopathyFe Deficiency vs Hbinopathy Check iron status: FerritinCheck iron status: Ferritin Family history / ethnicity:Family history / ethnicity:
– Thalassaemia / haemoglobinopathyThalassaemia / haemoglobinopathy– Need to determine risk to fetus of severe Need to determine risk to fetus of severe
thalassaemic syndrome (in 1thalassaemic syndrome (in 1stst rimester): rimester):Homozygous thalassaemia (Homozygous thalassaemia (αα or or ββ))Homozygous Hb S (sickle cell disease)Homozygous Hb S (sickle cell disease)Severe compound heterozygous states Severe compound heterozygous states
– E.g.: HbS/E.g.: HbS/ββ; HbE/; HbE/ββ; HbSC; HbSC
– Determine need to check partnerDetermine need to check partner

www.cambridgehaematology.comwww.cambridgehaematology.com
Red Cell Distribution Width Red Cell Distribution Width (RDW)(RDW)
The degree of variation in size of RBC: N <14The degree of variation in size of RBC: N <14 Increased RDW corresponds with Increased RDW corresponds with anisocytosisanisocytosis::
– Iron deficiency (increased RDW is the earliest lab feature: Iron deficiency (increased RDW is the earliest lab feature: anisocytosis precedes the anaemia)anisocytosis precedes the anaemia)
– Megaloblastic anaemia (can be very high >20)Megaloblastic anaemia (can be very high >20)– Anaemia with bone marrow erythroid response (i.e. Anaemia with bone marrow erythroid response (i.e.
reticulocytosis)reticulocytosis) RDW useful in DDx of microcytic anaemias. RDW useful in DDx of microcytic anaemias.
– Most cases of iron deficiency: raised RDW Most cases of iron deficiency: raised RDW – Most cases thalassaemia trait: normal RDWMost cases thalassaemia trait: normal RDW

www.cambridgehaematology.comwww.cambridgehaematology.com
MCHMCH Mean Cell HaemoglobinMean Cell Haemoglobin (27-32 pg) (27-32 pg)
– The mean haemoglobin per red blood cell The mean haemoglobin per red blood cell
MCH usually rises or falls as the MCV is MCH usually rises or falls as the MCV is increased or decreased.increased or decreased.
MCH < 25 pg used as a guide to the MCH < 25 pg used as a guide to the presence of thalassaemia or presence of thalassaemia or haemoglobinopathy.haemoglobinopathy.– MCH usually markedly reduced in MCH usually markedly reduced in
thalassaemia (e.g. beta thalassaemia trait thalassaemia (e.g. beta thalassaemia trait MCH 19 pg)MCH 19 pg)
www.cambridgehaematology.comwww.cambridgehaematology.com
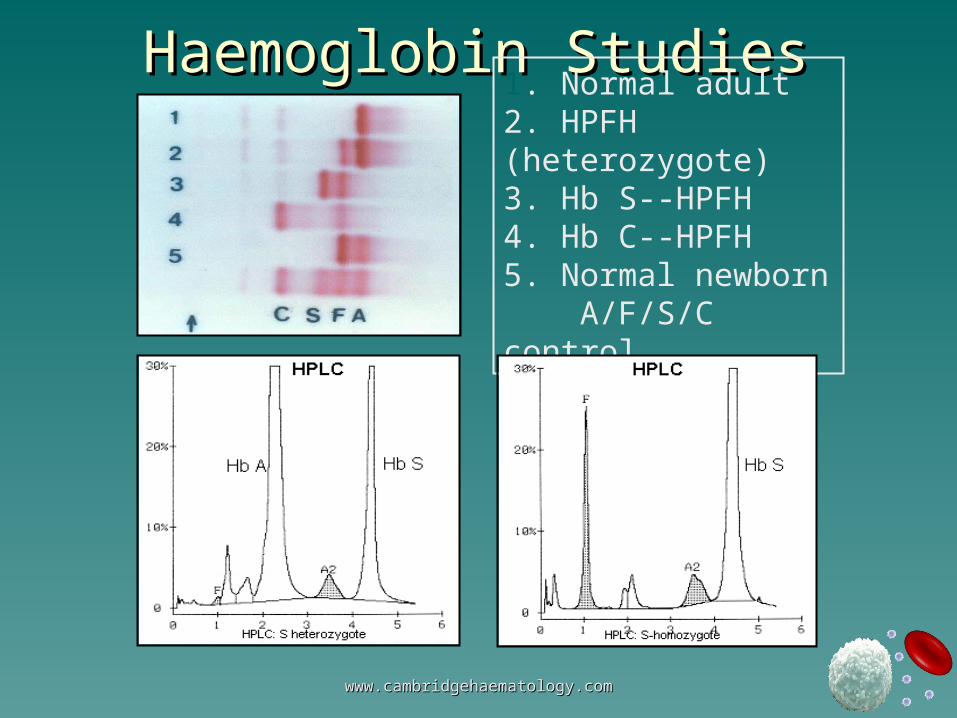
Haemoglobin StudiesHaemoglobin Studies1. Normal adult 2. HPFH (heterozygote)3. Hb S--HPFH 4. Hb C--HPFH 5. Normal newborn A/F/S/C control

www.cambridgehaematology.comwww.cambridgehaematology.com
73 year male73 year male
Hx:Hx: TirednessTiredness
FBC:FBC: HbHb 4.0 g/dL4.0 g/dLMCVMCV 102 fL102 fLRDWRDW 0.240.24WCC / PltWCC / Plt NormalNormal
Film:Film: Macrocytes, fragmented red Macrocytes, fragmented red cells, occasional NRBCcells, occasional NRBC

www.cambridgehaematology.comwww.cambridgehaematology.com
Blood FilmBlood Film73 yr old male73 yr old male

www.cambridgehaematology.comwww.cambridgehaematology.com
Severe Macrocytic AnaemiaSevere Macrocytic Anaemia
Megaloblastic anaemiaMegaloblastic anaemia Liver disease: end-stage failureLiver disease: end-stage failure Red cell aplasia:Red cell aplasia:
– Parvovirus; thymoma, other malignancyParvovirus; thymoma, other malignancy Bone marrow failure or infiltration:Bone marrow failure or infiltration:
– MyelodysplasiMyelodysplasi– Multiple myelomaMultiple myeloma

www.cambridgehaematology.comwww.cambridgehaematology.com
InvestigationsInvestigations
1.1. Serum vitamin B12Serum vitamin B12
Red cell folate (serum folate)Red cell folate (serum folate)2.2. Reticulocyte count Reticulocyte count (BM (BM
erythroid function)erythroid function)
3.3. Liver functionLiver function
4.4. Parvovirus serologyParvovirus serology
5.5. Bone marrow examinationBone marrow examination

www.cambridgehaematology.comwww.cambridgehaematology.com
Don’t Forget the AlcoholDon’t Forget the Alcohol

www.cambridgehaematology.comwww.cambridgehaematology.com
Other Causes of Macrocytic Other Causes of Macrocytic AnaemiaAnaemia
Severe liver diseaseSevere liver disease Excess alcoholExcess alcohol Haemorrhage / haemolysis: Haemorrhage / haemolysis:
reticulocytosisreticulocytosis Drug therapy: esp. cytotoxicsDrug therapy: esp. cytotoxics HypothyroidismHypothyroidism MyelodysplasiaMyelodysplasia Marrow infiltrationMarrow infiltration
– Bone marrow examination may be indicatedBone marrow examination may be indicated

www.cambridgehaematology.comwww.cambridgehaematology.com
Myelodysplasia (MDS)Myelodysplasia (MDS)
Clonal disorderClonal disorder Ineffective haematopoiesisIneffective haematopoiesis Incidence increases with ageIncidence increases with age
– Age 50yrs - 1 per 100,000Age 50yrs - 1 per 100,000– Age 70yrs – 25 per 100,000Age 70yrs – 25 per 100,000
RBC, WCC, and platelets affectedRBC, WCC, and platelets affected

www.cambridgehaematology.comwww.cambridgehaematology.com
MyelodysplasiaMyelodysplasia
Bone MarrowPeripheral Blood

www.cambridgehaematology.comwww.cambridgehaematology.com
MyelodysplasiaMyelodysplasia PrognosisPrognosis
– Number of cytopeniasNumber of cytopenias– BM Blast percentageBM Blast percentage– CytogeneticsCytogenetics– AgeAge
SurvivalSurvival– Varies 11.7 yrs – 0.4yrsVaries 11.7 yrs – 0.4yrs
ManagementManagement– SupportiveSupportive– Stem cell transplantationStem cell transplantation– New drugsNew drugs
www.cambridgehaematology.comwww.cambridgehaematology.com
Normocytic AnaemiaNormocytic Anaemia Multiple aetiologiesMultiple aetiologies Primary marrow production defectPrimary marrow production defect
– MyelodysplasiaMyelodysplasia– Marrow infiltrationMarrow infiltration– Haematinic deficienciesHaematinic deficiencies
Reduced red cell survivalReduced red cell survival– Blood lossBlood loss– Intrinsic defects (eg. Enzyme; membrane)Intrinsic defects (eg. Enzyme; membrane)– Extrinsic defects (eg. Plasma problems)Extrinsic defects (eg. Plasma problems)

www.cambridgehaematology.comwww.cambridgehaematology.com
Approach to Normocytic AnaemiaApproach to Normocytic Anaemia
History:History:– Acute blood loss ; jaundice; dark urineAcute blood loss ; jaundice; dark urine
Exclude treatable causes:Exclude treatable causes:– Check ferritin, folate, vitamin B12Check ferritin, folate, vitamin B12– Renal and hepatic functionRenal and hepatic function– Acute phase reactantsAcute phase reactants
Consider haemolysisConsider haemolysis
The blood film may have the answer !The blood film may have the answer !

www.cambridgehaematology.comwww.cambridgehaematology.com
78 year male78 year male Hx:Hx: Chest painChest pain PMHx:PMHx: Myocardial infarctMyocardial infarct FBC:FBC: HbHb 7.2 g/dL7.2 g/dL
MCVMCV 97 fL97 fL
WCCWCC 4.5 x 104.5 x 1099/L/L
PlateletsPlatelets 320 x 10320 x 1099/L/L
Reticulocytes: 320 (10-100)Reticulocytes: 320 (10-100)

www.cambridgehaematology.comwww.cambridgehaematology.com
Blood FilmBlood Film

www.cambridgehaematology.comwww.cambridgehaematology.com
Blood FilmBlood Film
RBC:RBC: SpherocytesSpherocytes
PolychromasiaPolychromasia
Nucleated red cellsNucleated red cells
Spherocytic haemolytic anaemia:Spherocytic haemolytic anaemia:
Auto-immune haemolytic anaemiaAuto-immune haemolytic anaemia
Hereditary spherocytosisHereditary spherocytosis

www.cambridgehaematology.comwww.cambridgehaematology.com
Other InvestigationsOther Investigations Biochemistry:Biochemistry:
– BilirubinBilirubin 100 100 μμmol/L (<20)mol/L (<20)– Other LFTOther LFT NormalNormal– LDHLDH 1,500 U/L1,500 U/L (120-240) (120-240)– HaptoglobinHaptoglobin <0.1<0.1
HaematologyHaematology::– Reticulocyte countReticulocyte count– Direct anti-globulin (Coombs) test: PositiveDirect anti-globulin (Coombs) test: Positive
Enzymes, Enzymes, Hereditary spherocytosis screenHereditary spherocytosis screen

www.cambridgehaematology.comwww.cambridgehaematology.com
Haemolytic AnaemiaHaemolytic Anaemia Primary Red Cell Problem:Primary Red Cell Problem:
– Red cell membrane: Hereditary Red cell membrane: Hereditary spherocytosisspherocytosis
– Enzyme defect: G6PD deficiencyEnzyme defect: G6PD deficiency– Haemoglobin defect: thalassaemiaHaemoglobin defect: thalassaemia– Abnormal red cells: dyserythropoiesis (MDS)Abnormal red cells: dyserythropoiesis (MDS)
Secondary Red Cell DestructionSecondary Red Cell Destruction– AutoimmuneAutoimmune– Severe hepatic dysfunctionSevere hepatic dysfunction– Red cell fragmentation: DIC; HUS; TTPRed cell fragmentation: DIC; HUS; TTP– Infections: malaria; clostridiumInfections: malaria; clostridium

www.cambridgehaematology.comwww.cambridgehaematology.com
Blood FilmBlood Film
Glucose-6-phosphate dehydrogenase deficiency
blister or helmet cells
www.cambridgehaematology.comwww.cambridgehaematology.com
Normocytic AnaemiaNormocytic Anaemia Blood film may have the answer:Blood film may have the answer:
– Normal red cell morphologyNormal red cell morphology– Dimorphic (high RDW): 2x RBC populationsDimorphic (high RDW): 2x RBC populations– Marked anisocytosis: marrow dysfunction/MDSMarked anisocytosis: marrow dysfunction/MDS– Is there polychromasia?Is there polychromasia?
Yes: Anaemia with marrow responseYes: Anaemia with marrow responseNo:No: Impaired marrow response Impaired marrow response
– Anaemia of Chronic Disease Anaemia of Chronic Disease – BM failureBM failure– Red cell aplasia: Parvovirus; aplastic anaemiaRed cell aplasia: Parvovirus; aplastic anaemia

www.cambridgehaematology.comwww.cambridgehaematology.com
PolycythaemiaPolycythaemia PseudopolycythaemiaPseudopolycythaemia PrimaryPrimary
– Polycythemia veraPolycythemia vera SecondarySecondary
– HypoxiaHypoxia AltitudeAltitude Cardiac/Pulmonary diseaseCardiac/Pulmonary disease CirrhosisCirrhosis Abnormal HaemoglobinsAbnormal Haemoglobins Chronic CO exposureChronic CO exposure
– Inappropriate erythropoietinInappropriate erythropoietin Renal lesionsRenal lesions TumoursTumours DrugDrug
www.cambridgehaematology.comwww.cambridgehaematology.com
Clinical FeaturesClinical Features HyperviscosityHyperviscosity
– HeadachesHeadaches– Blurred visionBlurred vision– BreathlessnessBreathlessness– ConfusionConfusion– (Plethora)(Plethora)
ThrombosisThrombosis– Venous + arterialVenous + arterial– BleedingBleeding
OtherOther– PruritisPruritis– GoutGout

www.cambridgehaematology.comwww.cambridgehaematology.com
Polycythaemia investigationsPolycythaemia investigations
FBC + FilmFBC + Film CXRCXR Cardiac assessmentCardiac assessment Red Cell massRed Cell mass Blood gassesBlood gasses
Major advance – JAK 2 mutation Major advance – JAK 2 mutation screensscreens

www.cambridgehaematology.comwww.cambridgehaematology.com
JAK2JAK2 Presence of the V617F mutationPresence of the V617F mutation indicates indicates
that the patient has an acquired, clonal that the patient has an acquired, clonal hematological disorder and not a reactive hematological disorder and not a reactive or secondary process. or secondary process.
Absence of the Absence of the JAK2JAK2 V617F mutation V617F mutation does does not exclude a MPD as up to 50% of not exclude a MPD as up to 50% of patients with ET and IMF will have wildtype patients with ET and IMF will have wildtype JAK2JAK2. .
The V617F mutation does The V617F mutation does notnot help in sub- help in sub-classifying the type of MPD of a given classifying the type of MPD of a given patient patient

www.cambridgehaematology.comwww.cambridgehaematology.com
Pathogenesis: Pathogenesis: Deregulated Tyrosine Kinases in MPDDeregulated Tyrosine Kinases in MPD
CML BCR-ABL
CMML TEL-PDGFRB
CEL FIP1L1-PDGFRA
SM KIT D816V
PV JAK2 V617F
ET JAK2 V617F
IMF JAK2 V617F

www.cambridgehaematology.comwww.cambridgehaematology.com
Questions so far?
www.cambridgehaematology.comwww.cambridgehaematology.com
PlateletsPlatelets
Too many (thrombocytosis)Too many (thrombocytosis) Too few (thrombocytopenia)Too few (thrombocytopenia) DysfunctionalDysfunctional
– When should we worry?When should we worry?

www.cambridgehaematology.comwww.cambridgehaematology.com
ThrombocytosisThrombocytosis
> 450 x 10> 450 x 1099/l/l
CausesCauses– Reactive (almost anything!)Reactive (almost anything!)
Common – bleeding, infection, malignancyCommon – bleeding, infection, malignancyTend to be less than 1000 x 10Tend to be less than 1000 x 1099/l/l
– Primary bone marrow disorderPrimary bone marrow disorderMyeloproliferative disorders (up to 3000+)Myeloproliferative disorders (up to 3000+)
(essential thrombocythaemia, myelofibrosis, (essential thrombocythaemia, myelofibrosis, polycythaemia, chronic myeloid leukaemia)polycythaemia, chronic myeloid leukaemia)

www.cambridgehaematology.comwww.cambridgehaematology.com
History, examination should guide History, examination should guide investigations and referralsinvestigations and referrals
Should the patient be on aspirin?Should the patient be on aspirin?– Only firm evidence is MPDsOnly firm evidence is MPDs– Reactive often given if > 1000, but little Reactive often given if > 1000, but little
evidence for thisevidence for this
ThrombocytosisThrombocytosis

www.cambridgehaematology.comwww.cambridgehaematology.com
Essential Thrombocythaemia (ET)Essential Thrombocythaemia (ET)– Long term management balancing Long term management balancing
thrombotic vs bleeding riskthrombotic vs bleeding risk– Aspirin for intermediate riskAspirin for intermediate risk– Cytoreduction + aspirin for higher riskCytoreduction + aspirin for higher risk
(beware the pseudohyperkalaemia!!)(beware the pseudohyperkalaemia!!)
ThrombocytosisThrombocytosis
www.cambridgehaematology.comwww.cambridgehaematology.com
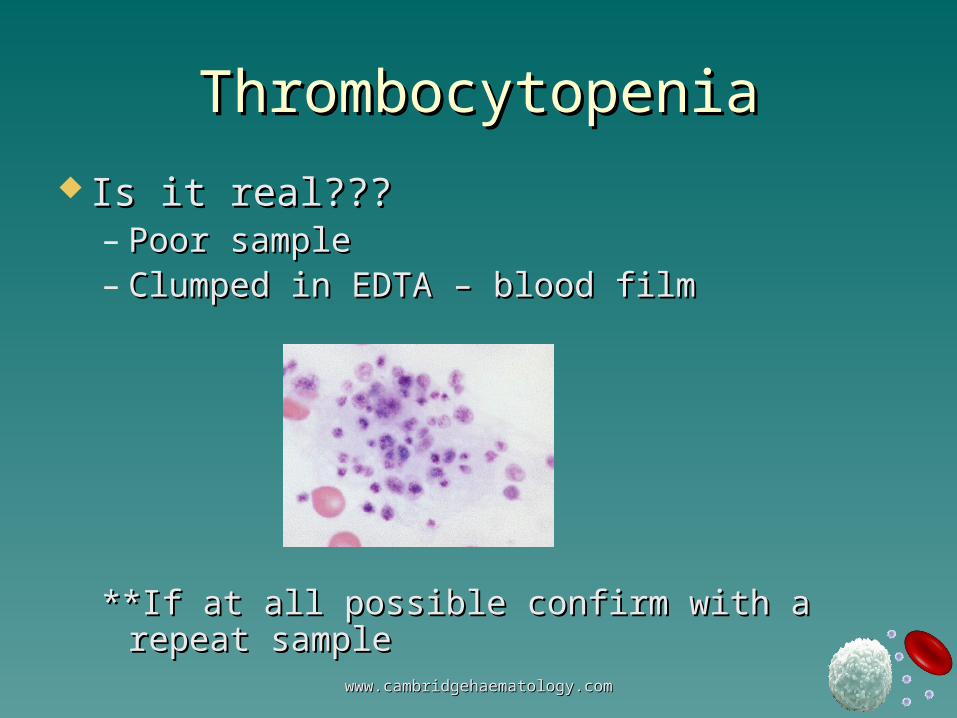
ThrombocytopeniaThrombocytopenia
Is it real???Is it real???– Poor samplePoor sample– Clumped in EDTA – blood filmClumped in EDTA – blood film
**If at all possible confirm with a repeat **If at all possible confirm with a repeat samplesample
www.cambridgehaematology.comwww.cambridgehaematology.com
PancytopeniaPancytopenia
vsvs
Isolated low plateletsIsolated low platelets
Pancytopenia – Pancytopenia – – always serious (marrow failure)always serious (marrow failure)
Isolated Isolated – may be relatively unimportantmay be relatively unimportant
ThrombocytopeniaThrombocytopenia

www.cambridgehaematology.comwww.cambridgehaematology.com
Decreased productionDecreased production– Rare in isolationRare in isolation– Viral infectionsViral infections
Increased consumptionIncreased consumption– Autoimmune – ITPAutoimmune – ITP– DrugsDrugs– PregnancyPregnancy– Large spleen / portal hypertensionLarge spleen / portal hypertension– Infections (HIV)Infections (HIV)– RARE but serious TTP – HUS - DICRARE but serious TTP – HUS - DIC
ThrombocytopeniaThrombocytopenia

www.cambridgehaematology.comwww.cambridgehaematology.com
Investigations depend on clinical Investigations depend on clinical suspicionsuspicion– Platelet volume may be helpful Platelet volume may be helpful
(small - think marrow)(small - think marrow)<8.0 and >10.5<8.0 and >10.5
– BM often not requiredBM often not required
ThrombocytopeniaThrombocytopenia

www.cambridgehaematology.comwww.cambridgehaematology.com
ThrombocytopeniaThrombocytopenia
(not joint bleeds!)

www.cambridgehaematology.comwww.cambridgehaematology.com
How real is the bleeding risk?How real is the bleeding risk?– Cause of low plateletsCause of low platelets– Wet vs dry purpuraWet vs dry purpura– Platelet transfusions often not usefulPlatelet transfusions often not useful
ThrombocytopeniaThrombocytopenia

www.cambridgehaematology.comwww.cambridgehaematology.com
ITP – a few useful remindersITP – a few useful reminders
ChildrenChildren– Acute, post viral, Acute, post viral, – spontaneous resolution (often no therapy)spontaneous resolution (often no therapy)
AdultAdult– More insidious onsetMore insidious onset– Chronic = commonChronic = common– Many (not all!) cases do require treatmentMany (not all!) cases do require treatment– Steroids – splenectomySteroids – splenectomy– Novel therapiesNovel therapies
www.cambridgehaematology.comwww.cambridgehaematology.com
Platelet DysfunctionPlatelet Dysfunction
Range of rare inherited causesRange of rare inherited causes– Family historyFamily history– Refer the child that bleeds abnormally!Refer the child that bleeds abnormally!
Don’t forget the acquired dysfunctionDon’t forget the acquired dysfunction– Renal failureRenal failure– Liver diseaseLiver disease– ASPIRINASPIRIN

www.cambridgehaematology.comwww.cambridgehaematology.com
Questions and break!

www.cambridgehaematology.comwww.cambridgehaematology.com
White CellsWhite Cells

www.cambridgehaematology.comwww.cambridgehaematology.com
White CellsWhite Cells

www.cambridgehaematology.comwww.cambridgehaematology.com
White CellsWhite Cells
Important (and commonly problematic!)Important (and commonly problematic!)– NeutrophilsNeutrophils– LymphocytesLymphocytes
Important (less commonly problematic)Important (less commonly problematic)– MonocytesMonocytes– eosinophilseosinophils
Less importantLess important– basophilsbasophils

www.cambridgehaematology.comwww.cambridgehaematology.com
NeutrophilsNeutrophils

www.cambridgehaematology.comwww.cambridgehaematology.com
NeutrophiliaNeutrophilia
Often result ‘expected’Often result ‘expected’– HistoryHistory– ExaminationExamination– primary haematological cause NOT primary haematological cause NOT
commoncommon

www.cambridgehaematology.comwww.cambridgehaematology.com
NeutrophiliaNeutrophilia
InfectionInfection Inflammation / necrosisInflammation / necrosis Cancer – any sort reportedCancer – any sort reported Bone marrow disease (MPDs, CML)Bone marrow disease (MPDs, CML) Drugs (steroids!!, growth factors)Drugs (steroids!!, growth factors)
Not always pathologicalNot always pathologicalPregnancy, smoking, normal variant!Pregnancy, smoking, normal variant!

www.cambridgehaematology.comwww.cambridgehaematology.com
NeutropeniaNeutropenia (<1.5 x 10 (<1.5 x 1099/l)/l)
Isolated neutropeniaIsolated neutropenia
vsvs
PancytopeniaPancytopenia

www.cambridgehaematology.comwww.cambridgehaematology.com
How worried should I be?How worried should I be?
Pancytopenia is ALWAYS worryingPancytopenia is ALWAYS worrying Many cases of isolated neutropenia Many cases of isolated neutropenia
are less seriousare less serious
What should I do with a neutropenic What should I do with a neutropenic patient?patient?
How common is neutropenic sepsis?How common is neutropenic sepsis?

www.cambridgehaematology.comwww.cambridgehaematology.com
PancytopeniaPancytopenia
Marrow FailureMarrow Failure– Drugs (chemotherapy)Drugs (chemotherapy)– Infiltration (cancer, MF,lymphoma etc.)Infiltration (cancer, MF,lymphoma etc.)– Myelodysplasia / leukaemia / myelomaMyelodysplasia / leukaemia / myeloma– Aplastic anaemia / PNHAplastic anaemia / PNH– Don’t forget B12 / folate (anorexia)Don’t forget B12 / folate (anorexia)
Peripheral consumptionPeripheral consumption– hypersplenismhypersplenism

www.cambridgehaematology.comwww.cambridgehaematology.com
PancytopeniaPancytopenia
Referral usually requiredReferral usually required Bone marrow biopsy usually requiredBone marrow biopsy usually required
www.cambridgehaematology.comwww.cambridgehaematology.com
Isolated NeutropeniaIsolated Neutropenia Not always easy to identify a cause!Not always easy to identify a cause! Always think drugs (idiopathic vs dose)Always think drugs (idiopathic vs dose) Viral infectionViral infection Auto-immune diseaseAuto-immune disease Marrow causesMarrow causes
(sepsis / very ill elderly)(sepsis / very ill elderly)
Don’t forget Don’t forget – Racial variationRacial variation– cyclical neutropenia (clinical and lab details)cyclical neutropenia (clinical and lab details)– If child, think congenitalIf child, think congenital

www.cambridgehaematology.comwww.cambridgehaematology.com
Investigations will depend on clinical Investigations will depend on clinical presentationpresentation– Chance finding vs ill patientChance finding vs ill patient– Viral serology may be indicated Viral serology may be indicated
(hepatitis, EBV etc – Think HIV!)(hepatitis, EBV etc – Think HIV!)– Autoimmune (SLE, sjorgrens, RA – Autoimmune (SLE, sjorgrens, RA –
Felty’s)Felty’s)– Serial blood countsSerial blood counts– Referral may be requiredReferral may be required
Isolated NeutropeniaIsolated Neutropenia

www.cambridgehaematology.comwww.cambridgehaematology.com
When to refer urgentlyWhen to refer urgently– Cause of neutropeniaCause of neutropenia
– Is the patient acutely ill?Is the patient acutely ill?
Neutropenic fever vs sepsisNeutropenic fever vs sepsis– Incidence etcIncidence etc– Antibiotic policies etc.Antibiotic policies etc.– Prophylactic antibiotics - controversialProphylactic antibiotics - controversial
Isolated NeutropeniaIsolated Neutropenia

www.cambridgehaematology.comwww.cambridgehaematology.com
LymphocytesLymphocytes
Lineage B vs T vs NKLineage B vs T vs NKOriginOriginRoleRole

www.cambridgehaematology.comwww.cambridgehaematology.com
CausesCauses– ReactiveReactive
(CMV, EBV, hepatitis, toxo, adenov)(CMV, EBV, hepatitis, toxo, adenov)
PertussissPertussiss
Inflammatory reaction (not common)Inflammatory reaction (not common)– Lymphoproliferative disorderLymphoproliferative disorder
Acute and chronic leukaemiasAcute and chronic leukaemias
lymphomaslymphomas
LymphocytosisLymphocytosis

www.cambridgehaematology.comwww.cambridgehaematology.com
Priorities for investigationPriorities for investigation– Clinical pictureClinical picture– If other FBC abnormalities, speak to a If other FBC abnormalities, speak to a
haematologisthaematologist– If in doubt, ask for an opinion on a blood If in doubt, ask for an opinion on a blood
filmfilm– Monospot test vs viral serologyMonospot test vs viral serology– Flow cytometryFlow cytometry– Molecular testsMolecular tests
LymphocytosisLymphocytosis

www.cambridgehaematology.comwww.cambridgehaematology.com
Lymphocytosis (>4 x 10Lymphocytosis (>4 x 1099/l)/l)
Blasts vs more mature cellsBlasts vs more mature cells
Clinical picture very importantClinical picture very important– Young sick child vs older well patientYoung sick child vs older well patient
vs vs

www.cambridgehaematology.comwww.cambridgehaematology.com
Young patient with clinical picture of Young patient with clinical picture of infectious mononucleosisinfectious mononucleosis– Monospot usefulMonospot useful– Film useful (rule out ALL) Film useful (rule out ALL) – Flow cytometry less helpfulFlow cytometry less helpful– Serology as second line investigationSerology as second line investigation– ID referral occasionally requiredID referral occasionally required– (worth thinking about acute HIV)(worth thinking about acute HIV)
LymphocytosisLymphocytosis

www.cambridgehaematology.comwww.cambridgehaematology.com
Acute lymphoblastic leukaemiaAcute lymphoblastic leukaemia– Children >> adultsChildren >> adults– Often presents very acutelyOften presents very acutely– Range of clinical featuresRange of clinical features– Laboratory features typicalLaboratory features typical– Referral mandatoryReferral mandatory
LymphocytosisLymphocytosis

www.cambridgehaematology.comwww.cambridgehaematology.com
Older patient with lymphocytosisOlder patient with lymphocytosis– Blood film required (CLL vs LGL)Blood film required (CLL vs LGL)– Flow cytometry usually requiredFlow cytometry usually required– ? Refer? Refer
Clinical picture Clinical picture Underlying diagnosisUnderlying diagnosis
LymphocytosisLymphocytosis

www.cambridgehaematology.comwww.cambridgehaematology.com
CLLCLL– Relatively common (300 + / year)Relatively common (300 + / year)– New entity of Monoclonal B New entity of Monoclonal B
Lymphocytosis (MBL)Lymphocytosis (MBL)– AgeAge– Clinical presentationClinical presentation
Asymptomatic stage AAsymptomatic stage A
VSVS
Symptomatic stage CSymptomatic stage C
LymphocytosisLymphocytosis

www.cambridgehaematology.comwww.cambridgehaematology.com
CLLCLL– HistoryHistory
Night sweats, weight loss, INFECTIONSNight sweats, weight loss, INFECTIONS
– ExaminationExaminationLymphadenopathy, hepato-splenomegalyLymphadenopathy, hepato-splenomegaly
– InvestigationInvestigationFlow cytometryFlow cytometry
LymphocytosisLymphocytosis

www.cambridgehaematology.comwww.cambridgehaematology.com
Flow cytometryFlow cytometry
LymphocytosisLymphocytosis
T cells
LeukaemicB cells

www.cambridgehaematology.comwww.cambridgehaematology.com
LymphocytosisLymphocytosis
Should I refer CLL?Should I refer CLL?– Long stage A phase in many patientsLong stage A phase in many patients– Patients and the ‘leukaemia’ word!Patients and the ‘leukaemia’ word!– Rough guideRough guide
SymptomaticSymptomatic Unusual / lymphoma phenotypeUnusual / lymphoma phenotype Lymphadenopathy / splenomegalyLymphadenopathy / splenomegaly Lymphocyte doubling time < 12 monthsLymphocyte doubling time < 12 months
with lymphocytes > 30 x 10with lymphocytes > 30 x 1099/l/l Hb < 10 g/dl (or haemolysing)Hb < 10 g/dl (or haemolysing) Platelets < 100x 10Platelets < 100x 1099/l/l

www.cambridgehaematology.comwww.cambridgehaematology.com
CLL – bewareCLL – beware– Not always benignNot always benign– Infections (hypogamma)Infections (hypogamma)– HaemolysisHaemolysis– ITPITP
LymphocytosisLymphocytosis

www.cambridgehaematology.comwww.cambridgehaematology.com
Rarer lymphoproliferative disordersRarer lymphoproliferative disorders– LGLLGL– PLLPLL– Leukaemic phase of most lymphomasLeukaemic phase of most lymphomas– Hairy cell leukaemiaHairy cell leukaemia
LymphocytosisLymphocytosis

www.cambridgehaematology.comwww.cambridgehaematology.com
Lymphopenia (<1.0 x 10Lymphopenia (<1.0 x 1099/l)/l)
Many cases reflect normal variantsMany cases reflect normal variants
How hard should you chase a cause?How hard should you chase a cause?
More common causesMore common causes– HIV / hepatitis / Hodgkin’s (steroids)HIV / hepatitis / Hodgkin’s (steroids)
Rarer causesRarer causes– Autoimmune disease / sarcoidosisAutoimmune disease / sarcoidosis

www.cambridgehaematology.comwww.cambridgehaematology.com
InvestigationsInvestigations– Clinical pictureClinical picture– Lymphocyte subset analysisLymphocyte subset analysis– RARE – bone marrowRARE – bone marrow
LymphopeniaLymphopenia

www.cambridgehaematology.comwww.cambridgehaematology.com
Enlarged LN ? causeEnlarged LN ? cause Clinical context is critical Clinical context is critical
– ? Symptom profile? Symptom profile– (?spleen)(?spleen)
Please do first line investigationsPlease do first line investigations– FBC may save a LN biopsyFBC may save a LN biopsy
Neck nodes – ENT fast track referralNeck nodes – ENT fast track referral Axillary and groin nodesAxillary and groin nodes
– Much depends on the clinical contextMuch depends on the clinical context– Haematology review first?Haematology review first?– Biopsy first?Biopsy first?– CT first?CT first?

www.cambridgehaematology.comwww.cambridgehaematology.com
EosinophilsEosinophils
HighHigh– Allergic disordersAllergic disorders– Drug HypersensitivityDrug Hypersensitivity– Skin DiseasesSkin Diseases– Parasitic infectionsParasitic infections– Myeloproliferative disordersMyeloproliferative disorders– Connective tissue disordersConnective tissue disorders
Churg StraussChurg Strauss

www.cambridgehaematology.comwww.cambridgehaematology.com
MonocytesMonocytes
HighHigh– Range of infectious and inflammatory stimuliRange of infectious and inflammatory stimuli– Primary BM conditionsPrimary BM conditions
CMML (overlap between myelodysplasia and CMML (overlap between myelodysplasia and myeloproliferative disorder)myeloproliferative disorder)
CMLCML
Clinical picture and blood film importantClinical picture and blood film important
If no clear cause consider haematology referralIf no clear cause consider haematology referral

Questions?
CCambridge ambridge HHaematology aematology PPartnersartners
www.cambridgehaematology.com