wsi--2017 benefits book---py eff 1.1.17 (v10.31.16)t @ work ... page 22 fsa—flexible ... refrain...
TRANSCRIPT

1
Benefits Book
Plan Year: January 1, 2017—December 31, 2017
Employer‐sponsored benefits: Health Insurance (2 Cigna plans to choose from) 1) OAPin High Deduc ble with HRA 2) OAP Low Deduc ble with HRA Dental Insurance Vision Insurance 403(b) Re rement Plan
100% Employee paid (voluntary) benefits: Flexible Spending Account (for Health care and/or Dependent care) Voluntary Life Insurance/ AD&D for Employee, Spouse and/or Children Voluntary Short Term Disability Voluntary Accident Insurance Voluntary Cri cal Illness/ Cancer Insurance
100% Company paid benefits: Life Insurance/ Accidental Death & Dismemberment (AD&D) Long Term Disability Insurance Employee Assistance Program (EAP) Worldwide Travel Assistance Paid Time Off Other Company Benefits (Substan a on Services, Direct Deposit) BB&T @ Work
v.10/31/16
Benefits Available to eligible employees:
All Full Time Employees are auto enrolled a er wai ng period is sa sfied.
2
TABLE OF CONTENTS
Employer‐Sponsored Benefits: Employee Costs per pay .………………………………………………….…………….…………. Page 3 Important Notes (eligibility, wai ng period, etc) ……………….…………………..…. Page 4 Cigna Health Plan op ons ……………………………………......………………………….…... Page 5 MyCigna Mobile App……………………………………………………………………………...…. Page 6‐7 Register on MyCigna…………….….……………………………………………………………….. Page 8 Cigna Home Delivery Pharmacy………………………………………………………………… Page 9 Cigna Help Informa on Line…………...………………………………………………………... Page 10 Healthy Incen ves Program………………………………………………………………………. Page 11 Healthy Incen ves opportuni es and requirements………………………………….. Page 12 What is an FBA? HRA? FSA?........................................................................... Page 13 Health Reimbursement Account……………………………………………………………….. Page 14‐15 Dental Plan Op on 1 (High Plan)……………………………..…………….……….…….…... Page 16 Dental Plan Op on 2 (Low Plan)……………………………………………………..…….…... Page 17 Vision Plan…………………………………...………………………………..…………………….…... Page 18‐20 403b Re rement …………….…………………………………………………………..……...……. Page 21 100% Employee paid (Voluntary) Benefits: FSA—Flexible Spending Account info (for Health care)………………………….…... Page 22 FSA—Flexible Spending Account info (for Dependent care)…………………….…. Page 23 Voluntary (Supplemental) Life/ AD&D insurance …………..………..….……….……. Page 24 Voluntary Short Term Disability insurance …………………....………..….……….……. Page 24 Voluntary Accident insurance ……….……..….……………………………………...….……. Page 25 Voluntary Cri cal illness/Cancer insurance ……….………………..…..….……….……. Page 26 100% Company paid Benefits: Life/AD&D insurance………………………………..………….………………………………..…. Page 27 Long Term Disability insurance………………………………...……….…………………..…. Page 27 Ability Assist Counseling Services (EAP)……………………………………………………… Page 28‐29 Funeral Planning & Concierge Services ……………………………………………………... Page 30‐31 Travel Assistance and ID The Protec on Services….…………………………………. Page 32‐33 Estate Guidance Services…………………………………………………………………………… Page 34‐35 Paid Time Off (PTO) .………….……………………………………...…………………………..…. Page 36 Tui on Reimbursement …………………………………………………………….……………... Page 36 State Employee’s Credit Union …………………………………………………………………. Page 36 BB&T@Work (personal banking benefits)……………………...…………………...……. Page 37‐38 Important Contact Informa on…………………………………………………….………...…. Page 39

3
Way Sta on, Inc. Semi‐Monthly Employee Contribu on Rates Per Pay Period
for Plan Year 1/1/17—12/31/17 This a brief overview created to help compare the cost of the available plans.
Health—Cigna:
OAPin High Deduc ble OAP Low Deduc ble
Hours p/wk 40+
hrs/wk 30‐39 hrs/wk
40+ hrs/wk
30‐39 hrs/wk
Individual $29.60 $78.92 $49.31 $98.63
Employee/Child(ren) $131.12 $243.54 $168.61 $281.02
Employee/Spouse $181.44 $294.87 $226.84 $340.27
Family $236.51 $384.36 $295.70 $443.55
*Employees can reduce their Health plan rate by $5 per pay by earning (5) “Healthy Incen ves”
Dental—MetLife:
HIGH PLAN LOW PLAN
With
Health Plan Without Health Plan With
Health Plan Without Health Plan
Hours p/wk All 30+ hrs/wk
40+ hrs/wk
30‐39 hrs/wk
All 30+ hrs/wk
40+ hrs/wk
30‐39 hrs/wk
Individual $16.71 $0.00 $4.19 $8.18 $0.00 $2.04
Employee/Child(ren) $42.12 $25.41 $29.60 $27.24 $19.07 $21.11
Employee/Spouse $36.07 $19.36 $23.54 $17.72 $9.55 $11.60
Family $61.23 $44.52 $48.71 $36.72 $28.55 $30.59
Vision—Cigna: Individual $3.39
Employee/Child(ren) $6.75
Employee/Spouse $6.45
Family $10.39
Life/AD&D and Long Term Disability Insurance
Company paid
Voluntary (Supplemental) Life/ AD&D Insurance (for Employee, Spouse and Dependents)
Employee paid. Amounts depend on age, tobacco status and coverage amounts elected.
Voluntary Short Term Disability Insurance
Employee paid. Amounts depend on age and income.
Voluntary Accident Insurance (for Employee, Spouse and Dependents)
Employee paid. Amounts depend on age and coverage elected.
Voluntary Cri cal Illness/ Cancer Insurance (for Employee, Spouse and Dependents)
Employee paid. Amounts depend on age, tobacco status and coverage amounts elected.

4
ENROLLMENT NOTE: If you choose not to enroll yourself and/or your Dependents because you have other (health, dental, vision) group in‐surance, you may be able to enroll yourself or your Dependents in this plan if you or your Dependents lose eligibility for that other coverage (or if the employer stops contribu ng toward your or your Dependents’ coverage). However, you must request enrollment within 31 days a er your or your Dependents’ coverage ends. In addi on, if you have a new dependent as a result of marriage, birth, adop on, or placement for adop on, you may be able to enroll yourself and your Dependents. However, you must request enrollment within 31 days a er marriage, birth, adop on, or placement for adop on.
TERMINATION NOTE: Employees who terminate employment are eligible to con nue Health, Dental and Vision coverage temporarily, under Federal COBRA guidelines. Upon termina on, if you were receiving coverage, you will receive a le er outlining your con nua on op ons.
PRE‐TAX PREMIUM NOTE: Employee premiums for Health, Dental and Vision are done through pre‐tax payroll deduc on. Should an employee wish to pay for their premiums on a post‐tax basis, please contact Human Resources.
IMPORTANT NOTES:
WAITING PERIOD (for Health, Dental, Vision, FSA, Life/AD&D and Disability Insurance): Employees are ini ally eligible on the 1st of the month following 30 days of employment, assuming the employee meets the hours per week eligibility requirements stated below. Employees who have previously completed the wai ng period and have par cipated in Way Sta on’s Benefits Program do not have to complete another 30 day eligibility period if they have been a con nuous employee who has experi‐enced a status change from full‐ me to part‐ me to full‐ me or if they have been re‐hired within 6 months of lay‐off.
DOMESTIC PARTNER NOTE (for Health, Dental, Vision, FSA, Vol Life/AD&D, Accident, Cri cal illness) Domes c Partners are eligible to par cipate on an eligible employee’s plan.
# of Hours p/week
Health Plan
Dental Plan
Vision Plan
Voluntary Life/AD&D Insurance
Voluntary Short Term
Disability
Flexible Spending Account
Dependent Care
Spending Account
40+ √ √ √ √ √ √ √
30‐39 √ √ √ √ √ √ √
20‐29
Life/AD&D
Insurance (Paid by WSI)
√
√
Long Term
Disability (Paid by WSI)
√
√
Voluntary Cri cal illness/ Cancer
Insurance
√
√
Voluntary Accident Insurance
√
√
ELIGIBILITY NOTE: Employees hired on a PRN or temporary basis or regularly scheduled to work less than 30 hours per week are not eligible for benefits.
PAYROLL DEDUCTION NOTE: Deduc ons for all Benefit plans will only come out of 24 of the total 26 payrolls per year. No Benefits deduc ons will be taken from the third paycheck of the month in which three payrolls fall.
HOURS PER WEEK REQUIRED FOR ELIGBILITY:

5
HEALTH INSURANCE OPTIONS
Carrier Cigna
Provider Network Open Access Plus or “OAP” (Na onal network)
Provider Search online www.cigna.com (or register and use MyCigna.com)
Plan Name OAPin High Deduc ble OAP Low Deduc ble
In‐Network Benefits: You pay... You pay...
Deduc ble (Individual/Family) $4,000/ $8,000 $2,000/ $4,000
Preven ve Services (ie rou ne physical) $0 (no Deduc ble) $0 (no Deduc ble)
Office Visit 5% a er Deduc ble 5% a er Deduc ble
Hospital 5% a er Deduc ble 5% a er Deduc ble
Outpa ent Surgery 5% a er Deduc ble 5% a er Deduc ble
Urgent Care 5% a er Deduc ble 5% a er Deduc ble
Emergency Room 5% a er Deduc ble 5% a er Deduc ble
RX, Deduc ble Combined with Medical Deduc ble Combined with Medical Deduc ble
RX, costs a er Deduc ble $10 / $25 / $45 $5 / $25 / $45
Maximum Out of Pocket/ Yr $6,550 (Indiv)
$7,150 (Indiv –in a Family) $13,100 (Family)
$4,500 (Indiv) $6,550 (Family)
Out‐of‐Network Benefits:
Deduc ble (Individual/Family) n/a $4,500/ $9,000
Coinsurance n/a 25%
Emergency Paid as in‐network Paid as in‐network
Maximum Out of Pocket/ Yr n/a $6,000/ $12,000
Employee's Semi‐Monthly Payroll Deduc on (24x yr)
40 hours 30‐39 hours 40 hours 30‐39 hours
Employee $29.60 $78.92 $49.31 $98.63
Employee/Child(ren) $131.12 $243.54 $168.61 $281.02
Employee/Spouse $181.44 $294.87 $226.84 $340.27
Family $236.51 $384.36 $295.70 $443.55
Deduc ble sharing:
Way Sta on HRA pays... Remaining
$2,750 (Individual) / $5,500 (Family) of Deduc ble expenses
Remaining $1,300 (Individual) / $2,600 (Family)
of Deduc ble expenses
Employee pays... First $1,250 (Individual) / $2,500 (Family)
of Deduc ble expenses First $700 (Individual) / $1,400 (Family)
of Deduc ble expenses
Total Deduc ble... $4,000 (Individual)/ $8,000 (Family) $2,000 (Individual) / $4,000 (Family)

6

7

8

9

10

11
Way Sta on “Healthy Incen ves” Program
$5 per pay discount on health plan premium (available to all health plan enrollees) In an effort to encourage a healthy lifestyle and manage costs for all, Way Sta on, Inc. (WSI) has developed a Healthy Incen ve Program for staff enrolled in any of the (2) Health Plans offered. This is a voluntary program offered by WSI to help control the rising costs of health coverage and to encourage healthy habits for employees and their families. We believe the Healthy Incen ve Program will enhance physical, emo onal, and intellectual health of our employees and their families through various means of awareness, educa on and healthy programs. In addi on over the long term, this will assist us in decreasing health care costs. The goals of the Healthy Incen ve Program are to:
increase employee par cipa on in wellness ac vi es change par cipant behavior to more healthy lifestyles; ul mately improve the health status of par cipants; and to manage rising costs of health benefits
The program is designed to provide every employee enrolled in the health plan an opportunity to earn an Incen‐ve of an addi onal $5 per pay discount on their health plan premium contribu on.
Employees who meet designated “Healthy Incen ves” are eligible to receive this discount. Details are below:
Employees must earn five (5) “Healthy Incen ves” in order to receive the $5 per pay incen ve. See a ached chart for the list of “Healthy Incen ves” you can chose from. Employees need to provide proof to WSI HR in order to receive the incen ves. See chart below for
details. Due to HIPPA privacy regula ons and confiden ality, proof submi ed to earn incen ves should just verify enrollment and/or comple on. Refrain from submi ng any documenta on that shows a diagnosis.
Incen ve amounts earned will then be processed by Payroll at the beginning of the month following confirma on of your “incen ves” earned.
Upon enrolling in one of the health insurance plans listed above, an employee has up to (6) months to earn “Healthy Incen ves” in a given plan year. Plan year begins January 1 through December 31.

12
Healthy Incen ve Descrip on of Requirement Verifica on Required for WSI HR Dept
Sign‐up for “My Account” (This incen ve is allowed one‐ me only)
1) Go to www.myCigna.com 2) Register Now
Print the web page showing registra on.
Health Assessment (This incen ve is allowed one‐ me only)
1) Go to www.myCigna.com 2) Create an account 3) Click on the tap called My Health 4) Complete Health Assessment
Print the web page showing you completed
Adult Physical exam 1) Go to your Primary Care Physician 2) Get (annual) exam (at no charge for In Network Providers!)
Completed & signed “Verifica on Sheet” (located on WSI intranet)
Age/gender specific test (i.e. cancer screening)
1) Go to your Primary Care Physician or Spe‐cialist 2) Get (annual) exam (at no charge if “Preven ve“ & In Network)
Completed & signed “Verifica on Sheet” (located on WSI intranet)
Diagnos c Lab Work 1) Go to a Par cipa ng Lab 2) Get Lab test done
Completed & signed “Verifica on Sheet” (located on WSI intranet) or Copy of Lab Slip or Copy of EOB
Engaging with a Health Coordinator, Pre‐Natal Care Coordinator, Weight Management Program/Coordinator, Case Management and/or Disease Management (inside or outside Cigna)
Completed & signed “Verifica on Sheet” (located on WSI intranet)
Smoking Cessa on program Proof or par cipa on in a Smoking Cessa on program an/or tools to qui ng tobacco use
Receipt of A endance or Receipt for qualified expense such as Nicore e, Patch, etc
Gym or Fitness Center Proof of membership and at least 3‐month’s par cipa on/ visits
Gym A endance Log (print‐out)
“Personal Workout” Proof of 3‐month’s par cipa on in a “personal workout” program. Examples in‐clude Walk, Run, Swim, Bike, Home Gym, Workout videos, etc
Personal Exercise Log w/ verifica on signature (a log sheet is on WSI intranet)
“Essen al Learning Classes” Comple on of WSI “Essen al Learning Clas‐ses” online: Defensive Driving; Stress Man‐agement for Mental Health Professionals; and/or any health related course that isn’t already a requirement for you job.
Verifica on is automa c when class is com‐pleted online
WSI Blood Drive Par cipa on A endance will be taken and turned in to WSI HR
WSI Flu Shot Par cipa on A endance will be taken and turned in to WSI HR
Yoga, Medita on, Massage, Acupuncture, Alterna ve Therapy (Sol Yoga is available at discount for WSI)
Proof or par cipa on in a Yoga, Medita on, Massage, Acupuncture or Alterna ve Thera‐py Program
Completed & signed “Verifica on Sheet” (located on WSI intranet)
Stress Management Program Proof of par cipa on in a Stress Manage‐ment Program
Completed & signed “Verifica on Sheet” (located on WSI intranet)
EAP Program Proof or par cipa on in a EAP Program Documented Confirma on
WSI Safety Program Proof of Level 3 Cer fica on in WSI’s Safety Program
A endance will be taken and turned in to WSI HR
Weight Watchers Par cipa on in program with Goals See WSI HR for details.
Eligible “Healthy Incen ves” opportuni es and requirements:

13
What is an FBA? HRA? FSA?
FBA = a (limited) Flexible Benefit Account that allows you to pay for the “first” por on of your qualified Medical and RX Deduc ble expenses by using money funded through pre‐tax payroll deduc ons. HRA = a Health Reimbursement Account that provides you Employer (WSI) money for the “second” por on of your qualified Medical and RX Deduc ble expenses. FSA = a (unlimited) Flexible Spending Account that allows you to pay for ALL of your qualified IRS 213d ex‐penses (i.e. qualified health, dental, orthodon a, vision, over‐the‐counter expenses, etc) by using money funded through pre‐tax payroll deduc ons. *Choice‐Strategies administers the FBA, HRA and FSA for Way Sta on. Eligible Combina ons of FBA, HRA and FSA:
Health Plan: OAPin High Deduc ble OAP Low Deduc ble
Employee pays… First $1,250 (Individual) / $2,500 (Family)
of Deduc ble expenses
First $700 (Individual) / $1,400 (Family)
of Deduc ble expenses
Way Sta on HRA pays…
(using CHOICE Card)
Remaining $2,750 (Individual) / $5,500 (Family)
of Deduc ble expenses
Remaining $1,300 (Individual) / $2,600 (Family)
of Deduc ble expenses
How can I pay for the “first” amount of my Deduc ble?
1) Pay with Cash, or 2) Using your FBA (limited Flexible Benefit Account used to pay for Deduc ble) *Pay with Choice‐Strategies MasterCard
How much $ can I allocate in my FBA?
Only the “first” amounts noted above.
How does $ get put in my FBA?
Money is put in an Employee’s FBA through (pre‐tax) payroll deduc ons. The annual FBA elec on amount is available on Day 1.
What if I do NOT use my FBA $?
FBA money is “use it or lose it” per plan year. All money that goes “unused” at the end of the plan year can be used for all eligible IRS 213d expenses (i.e. qualified health, den‐tal, vision, over‐the‐counter expenses, etc). You will have 75 days a er the plan year to use this money, or it’s forfeited.
Paying for your Health Plan Deduc ble
HRA only FBA & HRA FBA,HRA & FSA FSA only
WSI Health plan needed to enroll? YES YES YES NO
Minimum EE $ p/year n/a $700/1400 (OAP) or $1250/2500 (OAPin)
$700/1400 (OAP) or 1250/2500 (OAPin)
+$100 (FSA)
$100 (FSA)
Maximum EE $ p/year n/a Same as minimum (FBA)
The total FBA+FSA cannot exceed $2,600
$2,600 (FSA)

14
Health Reimbursement Account (HRA) ...Did you know? Our company offers employees high‐deduc ble health insurance plans that allow employees to u lize an HRA. An HRA is a Health Reimbursement Account that allows you to pay for/ be reimbursed for qualified Medical and RX expenses that are subject to Deduc ble. Choice‐Strategies (“CHOICE”) administers this HRA plan for us. 1) How much am I allowed to be reimbursed?
Refer to our Health Insurance Op on chart for HRA amounts
2) How will I be able to access HRA funds? Via Healthcare payment card: Members can pay for eligible expenses using a CHOICE payment card (i.e. Debit Card) Via Reimbursement:
Members can pay for eligible expenses with any form of payment and request reimbursement (using appropriate reimbursement forms sent to CHOICE). Reimbursements are made by check or direct deposit.
3) What happens if I use my account for a non‐eligible expense?
If you file a manual request for reimbursement, your request will be denied. If you use your healthcare payment card and the expense is deemed ineligible, you will be required to reimburse your account for that transac on. 4) How will I know if I need to submit a receipt to CHOICE for substan a on?
You can review if your claim requires receipt by logging into your account online. You need to submit receipts if you see a no ce. If a receipt is needed, you will also be no fied by email or le er within a week of your payment card swipe.
5) What if I don’t submit my receipts?
You must provide the receipts within the me requested, or the transac on will be deemed ineligible and you will be required to refund the amount of the transac on. If you fail to submit receipts within 45 days, your card will be deac vated. If you fail to reimburse the account, the amount of eligible expenses may be added to your W‐2 or withheld from your pay.
6) Where can I use my healthcare payment card?
Your healthcare payment card can be used na onwide at qualified merchants (such as Pharmacies, Doctor’s offices and hospitals). Your card should only be used to pay for qualified medical and RX De‐duc ble expenses under your plan. YOU SHOULD ALWAYS SAVE YOUR RECEIPTS!

15
At the Doctor's Office Give them your Cigna card
Pay your copay (if requested) with your CHOICE MasterCard
See your doctor
The doctor's office will send a claim to Cigna
Cigna will send you an EOB (Explana on of Bene‐fits) outlining the approved cost of the service, how much you paid already, and how much you s ll owe
Pay the provider with your CHOICE MasterCard ‐the “first” amount will be pulled from the Employee FBA ‐the “remaining” amount will be paid by Way Sta on HRA
At the Doctor's Office Give them your Cigna card
Pay your copay (if requested) with Cash
See your doctor
The doctor's office will send a claim to Cigna
Cigna will send you an EOB (Explana on of Benefits) out‐lining the approved cost of the service, how much you paid already, and how much you s ll owe
The Employee is responsible for the “first” Deduc ble amount (see chart for your plan’s Deduc ble).
Once the “first” Deduc ble amount has been met, the Employee provides proof to CHOICE MasterCard (via the last page of an EOB indica ng accrued Deduc ble amount YTD and Choice‐Strategies Claim Form).
Employees can begin paying provider’s with their CHOICE MasterCard (or be reimbursed via CHOICE MasterCard for any amounts over the “first” Deduc ble).
At the Pharmacy Give them your Cigna card
They'll tell you the cost of your prescrip on
Pay with your CHOICE MasterCard
At the Pharmacy Give them your Cigna card
They'll tell you the cost of your prescrip on
The Employee is responsible for the “first” Deduc ble amount (see chart for your plan’s Deduc ble).
Once the “first” Deduc ble amount has been met, the Employee provides proof to CHOICE MasterCard (via the last page of an EOB indica ng accrued Deduc ble amount YTD and Choice‐Strategies Claim Form).
Employees can begin paying provider’s with their CHOICE MasterCard (or be reimbursed via CHOICE MasterCard for any amounts over the “first” Deduc ble).
Using your Health Reimbursement Account (HRA) How does this work while I am in the "deduc ble phase" of my Health plan? For those with an FBA For those without an FBA
*All Flexible Claims are subject to audit. SAVE YOUR RECEIPTS!*

16
DENTAL PLAN 1: High Plan
In Network (PDP Den st) Out of Network (non‐PDP)
The Fee is: $700 Your Plan Pays: (50% x $700 Fee) ‐$350 Your Out of Pocket Cost: $350
The Den st’s Usual Fee is: $1,000 Your Plan Pays: (50% x $900 R&C Fee) ‐$450 Your Out of Pocket Cost: $550
Dental Benefits In‐Network Out‐of‐Network
Annual Deduc ble Individual (Waived for Preven ve) Family (Waived for Preven ve)
$50 $150
$50 $150
Annual Maximum p/person (p/calendar yr) $1,500 $1,000
Orthodon a (children up to age 19) 50% to $1,000 Life me Max p/Child
Preven ve Services (Cleanings, Fluoride treatments, oral exams, etc)
Basic Services (Fillings, Root canal, periodontal surgery, Oral Surgery, etc) Major Services (Inlays, Crowns, Fixed Bridges, etc)
Insurance pays 100% of PDP fee
Insurance pays 80% of PDP fee
Insurance pays 50% of PDP fee
Insurance pays 100% of R&C Fee**
Insurance pays 80% of R&C Fee**
Insurance pays 50% of R&C Fee**
Par cipa ng Dental Provider (PDP) Network Search
An example of Savings when you visit a Par cipa ng Dental Provider (PDP):
This is an example only. Actual fees may differ.
Your Den st says you need a Crown, a Major Service
Den st’s Usual Fee: $1,000 **R&C (Reasonable & Customary) Fee: $900 Par cipa ng Dental Provider (PDP) Fee: $700
www.metlife.com/dental Select “Find a Par cipa ng Den st”
(Network = PDP Plus)
**R&C Fee: Out‐of‐network benefits are payable for services rendered by a den st who is not a par cipa ng provider. The Reasonable and Customary charge is based on the lowest of: • the den st’s actual charge (the 'Actual Charge'), • the den st’s usual charge for the same or similar services (the 'Usual Charge') or • the usual charge of most den sts in the same geographic area for the same or similar services as determined by MetLife (the 'Customary

17
DENTAL PLAN 2: Low Plan
In Network (PDP Den st) Out of Network (non‐PDP)
The Fee is: $700 Your Plan Pays: (25% x $700 Fee) ‐$175 Your Out of Pocket Cost: $525
The Den st’s Usual Fee is: $1,000 Your Plan Pays: (20% x $900 R&C Fee) ‐$180 Your Out of Pocket Cost: $820
Dental Benefits In‐Network Out‐of‐Network
Annual Deduc ble Individual (Waived for Preven ve) Family (Waived for Preven ve)
$50 $150
$75 $225
Annual Maximum p/person (p/calendar yr) $1,000 $1,000
Orthodon a (children up to age 19) 50% to $1,000 Life me Max p/Child
Preven ve Services (Cleanings, Fluoride treatments, oral exams, etc)
Basic Services (Fillings, Oral Surgery, etc)
Major Services (Inlays, Crowns, Fixed Bridges, Root canal, periodontal surgery, etc)
Insurance pays 100% of PDP fee
Insurance pays 50% of PDP fee
Insurance pays 25% of PDP fee
Insurance pays 80% of R&C Fee**
Insurance pays 40% of R&C Fee**
Insurance pays 20% of R&C Fee**
Par cipa ng Dental Provider (PDP) Network Search
An example of Savings when you visit a Par cipa ng Dental Provider (PDP):
This is an example only. Actual fees may differ.
Your Den st says you need a Crown, a Major Service
Den st’s Usual Fee: $1,000 **R&C (Reasonable & Customary) Fee: $900 Par cipa ng Dental Provider (PDP) Fee: $700
www.metlife.com/dental Select “Find a Par cipa ng Den st”
(Network = PDP Plus)
**R&C Fee: Out‐of‐network benefits are payable for services rendered by a den st who is not a par cipa ng provider. The Reasonable and Customary charge is based on the lowest of: • the den st’s actual charge (the 'Actual Charge'), • the den st’s usual charge for the same or similar services (the 'Usual Charge') or • the usual charge of most den sts in the same geographic area for the same or similar services as determined by MetLife (the 'Customary

18

19
20

21
403b Re rement Plan
Maximum Contribu on:
The maximum contribu on of eligible pre‐tax pay is up to $18,000/ year (2017). The maximum catch‐up provision (for those age 50 and over) is an addi onal $6,000/year.
Company Match: If profitable, WSI will match 25% of the employee’s contribu on.
Ves ng schedule:
Years of Service Ves ng % Less than 1 0 1 20% 2 40% 3 60% 4 80% 5 100%
Eligibility:
FTE’s (over 21) are eligible on the 1st day of the month 30 Days a er Hire. Employee’s must work 1,000 or more hours in the plan year.
Investment info: Refer to www.principal.com for all addi onal informa on and resources.
Account number: Way Sta on’s account number is 809673

22
Flexible Spending Account (FSA) ...Did you know? Our company offers employees a Flexible Spending Account for healthcare related expenses. Choice‐Strategies (“CHOICE”) administers this plan for us. Features of an FSA:
Allow employees to set aside money on a pretax basis that can be used to pay for out‐of‐pocket 213(d) IRS eligible medical expenses
Employees save money by paying for these goods and services with pre‐tax dollars
Pre‐funded account ‐ employees have their full annual elec on available at the start of their plan
Advantages of a Choice Strategies FSA:
Employees can determine their tax savings through our: FSA Savings Calculator
Mul ple plans on one convenient Choice Strategies debit card
Member Service Representa ves can be reached by phone, email or live chat
Answers to frequently asked ques ons about FSAs can be found easily on the website
Members create their own online account to view balance and account informa on Eligible Expenses:
Health plan expenses (copay, coinsurance and/or deduc ble)
Dental
Vision
Orthodon a
Limited over‐the‐counter items (some items require DR note)
Alterna ve treatments
A full list of FSA eligible expenses can be found on the Choice Strategies website Using your Debit Card for your FSA expenses:
Process the transac ons as “credit”
Please understand that you may be required to send in receipts and/or EOB’s to validate your expense. Failure to comply may result in your card being turned off.
ALWAYS SAVE YOUR RECEIPTS! Maximum Annual Employee Contribu on: FSA = $2,600/yr Funds Forfeiture: Unused amounts at year‐end are NOT rolled over to the next plan year (i.e. funds are “use it or lose it”) **Refer to the www.Choice‐Strategies.com for claim forms and more details

23
Dependent Care Account (DCA) ...Did you know? Our company offers employees a Flexible Spending Account for Dependent Care. Choice‐Strategies (“CHOICE”) administers this plan for us. Features of a DCA:
Pre‐tax money for dependent care expenses can be set aside to pay for childcare for children through age 12 and adult day care.
Employees significantly reduce their tax liability, thereby saving money:
Consider an employee who elects to place $5000 into a Dependent Care Account. The employee’s gross salary is reduced by $5000. If the total tax rate for this employee is 20%, the employee saves $1000.
Advantages of a Choice Strategies DCA:
As DCA funds accumulate in the account as they are deducted from the employees’ salary, the funds needed to reimburse the en re claim amount may not be available
Choice Strategies has taken the extra step to provide “on‐hold claims”
Reimbursement for the claim requested is provided directly a er the funds accumulate Eligible Expenses:
Eligible expenses include day care provided by a day care facility or in‐home dependent care, before/a er school care programs, pre‐school and summer day camp.
Dependent care expenses must be for care while the employee is at work
Must be for custodial care only
Custodial care does not include expenses for food, clothing, or educa on
If a daycare provides meals in addi on to childcare and couldn’t be separated from the cost of care, it is considered an eligible expense
How do Employees Save? By using pre‐tax dollars to pay for certain benefits, employees reduce their taxable income, resul ng in more spending dollars. Contribu ons are not subject to Federal, State*, Social Security and Medicare taxes. Maximum Annual Employee Contribu ons (per IRS): Dependent Care FSA = $5,000/yr Funds Forfeiture: Unused amounts at year‐end are NOT rolled over to the next plan year (i.e. funds are “use it or lose it”) **Refer to the www.Choice‐Strategies.com for claim forms and more details.

24
Voluntary (Supplemental) Life Insurance/ Accidental Death & Dismemberment (AD&D)
Minimum $10,000
Maximum $500,000
Guarantee Issue Amount
(no underwri ng; at ini al eligibility only)
Up to $100,000
Notes: This benefit is 100% EMPLOYEE paid.
$5,000
$250,000
Up to $25,000
Increments of $2,000 to a maximum of $10,000 for
each child– no medical infor‐ma on required
(*26 years if FT student)
$10,000 per child
Up to full amount
Employee Spouse Child(ren)
Voluntary Short Term Disability
Benefit % of Weekly Earnings: 50%
Maximum Benefit Amount/ week: $500
Guarantee Issue: YES (no medical underwri ng; at ini al eligibility only)
Maximum Benefit Dura on: 12 weeks
Elimina on Period: 8th Day a er Accidental Injury
8th Days a er Illness
Notes: This benefit is 100% EMPLOYEE paid. Benefit payments are tax free.

25
Voluntary Accident Insurance
Covered Treatments/ Services: (a er Accident)
Examples of items that would receive a benefit payment: Ambulance, Appliance, Blood, Chiroprac c care, Emergency Room, Hospitaliza on, Medical Imaging Test, Outpa ent Surgery, Pain Mngmt, Physician follow up visits, Rehab, Therapy, Travel (due to covered Accident), etc
Covered Injuries & Surgical Procedures: (a er Accident)
Examples of items that would receive a benefit payment: Burns, Skin Gra s, Coma, Concussion, Dental (emergency), Dislo‐ca on, Eye injury, Fracture, Knee car lage, Lacera on, Prosthe c device, Ruptured Disc with Surgical repair, Surgery, Tendon/Ligament/Rotator Cuff, etc
Guarantee Issue: YES
Notes: This benefit is 100% EMPLOYEE paid. Payroll Deduc ons are post tax. Benefit payments are tax‐free. .
Accidental Death &/or Dismemberment: Covered
Wellness Benefit: $50 per insured per calendar year
Portable: Yes (you can con nue this policy is you leave employment/ re re)
Accident insurance cost per semi‐monthly pay
Available only at 1/1 Annual Open Enrollment
only
Employee only $8.48
Employee/ Child(ren) $15.32
Employee/ Spouse $13.95
Employee/ Spouse + Child(ren) $20.80
Spouse issue ages 17 through 64 years. Dependent Children issue ages are newborn up to their 26th birthday or through the maximum coverage age defined in the policy.
You can obtain a copy of your policy by: Visi ng www.unum.com/employees and registering under “First Time User”, or Call 800‐635‐5597 x1

26
Available only at 1/1 Annual Open Enrollment
only
Voluntary Cri cal Illness/ Cancer Insurance
Covered Condi ons:
For Cri cal Illness with Cancer: Cancer, Carcinoma in Situ (25%), Heart A ack, Coronary Artery, Bypass Surgery (25%), Stroke, End Stage Renal (Kidney) Failure, Major Organ Failure, Permanent Pa‐ralysis as the result of a Covered Accident, Coma as the result of Severe Trauma c Brain Injury, Blindness, Benign Brain Tumor, Occupa onal HIV. Addi onal Covered Condi ons for Dependent Children: ‐Cerebral Palsy ‐Cle Lip or Palate ‐Cys c Fibrosis ‐Down Syndrome
Pre‐exis ng Condi on:
This plan will not pay benefits for a claim that is caused by, contributed to by or occurs as a result of a pre‐exis ng condi on. Under this 12/12 plan, a pre‐exis ng condi on: Includes a Sickness or Injury or symptoms of a Sickness or Injury, whether diagnosed or not
for which the insured received medical treatment, consulta on, care or services including diagnos c measures, took prescribed drugs or medicines, or had been prescribed drugs or medicines in the 12 months just prior to his or her effec ve date of coverage; and
Applies if the date of diagnosis is in the first 12 months a er the effec ve date of coverage.
Portable: Yes (you can con nue this policy is you leave employment/ re re)
Purchase Amounts: Employee ‐ $5,000, $10,000 or $15,000 Spouse ‐ $5,000 or $10,000 Child ‐ 25% of Employee Coverage Amount (auto enrolled with Employee)
Guarantee Issue: Up to the Full amount (for Employee, Spouse and Children)
Notes: This benefit is 100% EMPLOYEE paid. Payroll Deduc ons are post tax. Benefit payments are tax‐free.
Cost per pay informa on is available at Open Enrollment
You can obtain a copy of your policy by: Visi ng www.unum.com/employees and registering under “First Time User”, or Call 800‐635‐5597 x1

27
Life Insurance/ Accidental Death & Dismemberment (AD&D)
Benefit Amount for eligible Employee: 1.5x employee annual earnings,
up to $200,000
Guarantee Issue: YES (no medical underwri ng)
Age Based Benefit Reduc on: ‐At age 65, par cipants receive 65% of the benefit value ‐At age 70, par cipants receive 50% of the benefit value
Notes: This benefit is 100% EMPLOYER paid.
All Full Time
Employees receive this benefit at no cost!
Long Term Disability
Benefit % of Monthly Earnings: 50%
Maximum Benefit Amount/ month: $4,000
Guarantee Issue: YES (no medical underwri ng)
Maximum Benefit Dura on: 5 years
Elimina on Period: 90 days
Notes: This benefit is 100% EMPLOYER paid. Benefit payments are subject to applicable taxes.

28
29

30

31

32

33

34

35
36
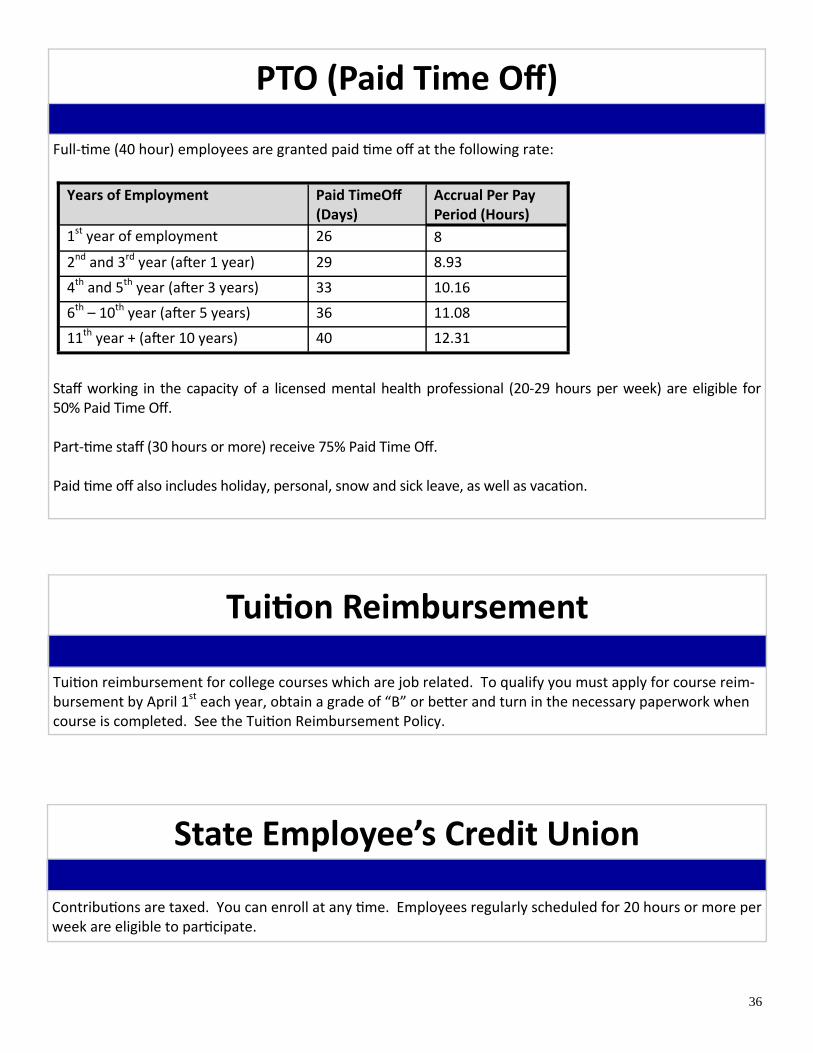
Tui on Reimbursement
Tui on reimbursement for college courses which are job related. To qualify you must apply for course reim‐bursement by April 1st each year, obtain a grade of “B” or be er and turn in the necessary paperwork when course is completed. See the Tui on Reimbursement Policy.
State Employee’s Credit Union
Contribu ons are taxed. You can enroll at any me. Employees regularly scheduled for 20 hours or more per week are eligible to par cipate.
PTO (Paid Time Off)
Full‐ me (40 hour) employees are granted paid me off at the following rate:
Staff working in the capacity of a licensed mental health professional (20‐29 hours per week) are eligible for 50% Paid Time Off. Part‐ me staff (30 hours or more) receive 75% Paid Time Off. Paid me off also includes holiday, personal, snow and sick leave, as well as vaca on.
Years of Employment Paid TimeOff (Days)
Accrual Per Pay Period (Hours)
1st year of employment 26 8
2nd and 3rd year (a er 1 year) 29 8.93
4th and 5th year (a er 3 years) 33 10.16
6th – 10th year (a er 5 years) 36 11.08
11th year + (a er 10 years) 40 12.31
37
38

39
IMPORTANT CONTACT INFORMATION
Benefit Provider Group # Phone #/ web/ email
Health Cigna 3340342 800‐244‐6224 www.mycigna.com
Dental MetLife 5548141 800‐275‐4638 www.metlife.com
Vision Cigna 3340342 877‐478‐7557 www.mycigna.com
HRA—Health Reim‐bursement Account
Choice‐Strategies Way Sta on Inc 888‐278‐2555 x2 www.Choice‐Strategies.com
FBA—Limited Flexible Spending Account (Health plan Ded only)
FSA—Flexible Spend‐ing Accts (FSA & DCA)
403b Re rement Plan Principal Way Sta on—809673 www.principal.com
Life Insurance/AD&D The Har ord 879445 www.thehar ord.com
Disability
Accident/ Cri cal illness UNUM 800‐635‐5597 x1 www.UNUM.com/employees
Ability Assist Counsel‐ing Services
The Har ord HLF902 800‐964‐3577 www.Guidanceresourcescom
Funeral Planning and Concierge Services
The Har ord HFEVLC 866‐854‐5429 www.everes uneral.com/har ord
Estate Guidance The Har ord WILLHLF www.estateguidance.com/wills
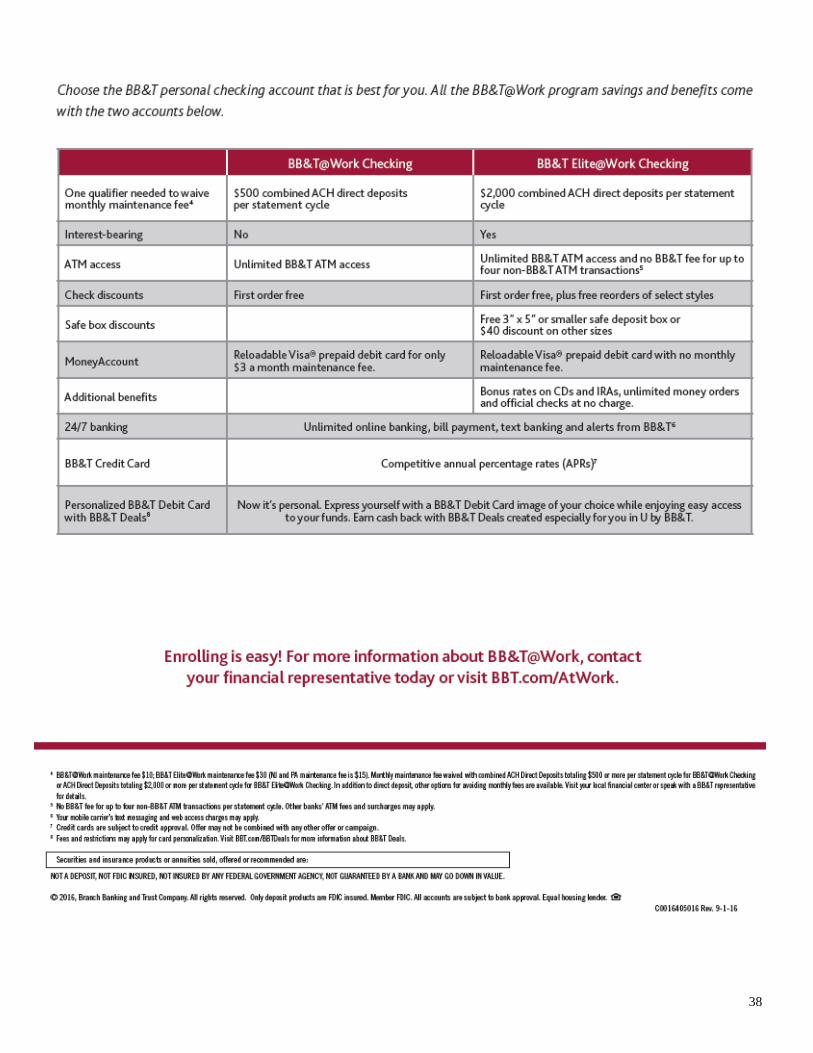
BB&T @ Work BB&T Jessica Tennant 301‐644‐6354 [email protected]
Way Sta on Inc, HR Contacts:
Frederick Co. Dawn Murphy PH: 301‐662‐0099 x4505 Fax: 301‐620‐2925 DMur‐phy@waysta oninc.org
Washington Co. Teresa Jainniney PH: 301‐733‐6063 x249 Fax: 301‐733‐6220 TJain‐niney@waysta oninc.org
Howard Co. Bev Foster PH: 410‐740‐1901 x7730 Fax: 443‐766‐7757 BFoster@waysta oninc.org
Travel Assistance and ID The Services
The Har ord GLD‐09012 800‐243‐6108 Thehar ord.com/employeebenefits
This Guide is only intended to offer an outline of benefits. All details and contract obliga ons of plans are stated in the actual summary plan descrip on.
Please contact your Human Resources Department for further informa on and contractual obliga ons.
40
Mandatory Disclosures
Notices to employees of Way Station, Inc. regarding health and welfare plans
I. Notices generally applicable to group health plans A. Special enrollment notice If you are declining enrollment for yourself or your dependents (including your spouse) because of other health insurance or group health plan coverage, you may be able to enroll yourself and your dependents in this plan if you or your dependents lose eligibility for that other coverage (or if the employer stops contributing toward your or your dependents’ other coverage). However, you must request enrollment within 30 days after your or your dependents’ other coverage ends (or after the employer stops contributing to-ward the other coverage). In addition, if you have a new dependent as a result of marriage, birth, adoption, or placement for adoption, you may be able to enroll yourself and your dependents. However, you must request enrollment within 30 days after the marriage, birth, adoption, or placement for adoption. Finally, if you or an eligible dependent has coverage under a state Medicaid or child health insurance program and that coverage is terminated due to a loss of eligibility, or if you or an eligible dependent become eligible for state premium assistance under one of these programs, you may be able to enroll yourself and your eligible family members in the Plan. However, you must request enroll-ment no later than 60 days after the date the state Medicaid or child health insurance program coverage is terminated or the date you or an eligible dependent is determined to be eligible for state premium assistance. To request special enrollment or obtain more information, contact the plan administrator identified at the end of these notices. B. CHIPRA premium assistance notice
Premium Assistance under Medicaid and the Children’s Health Insurance Program (CHIP)
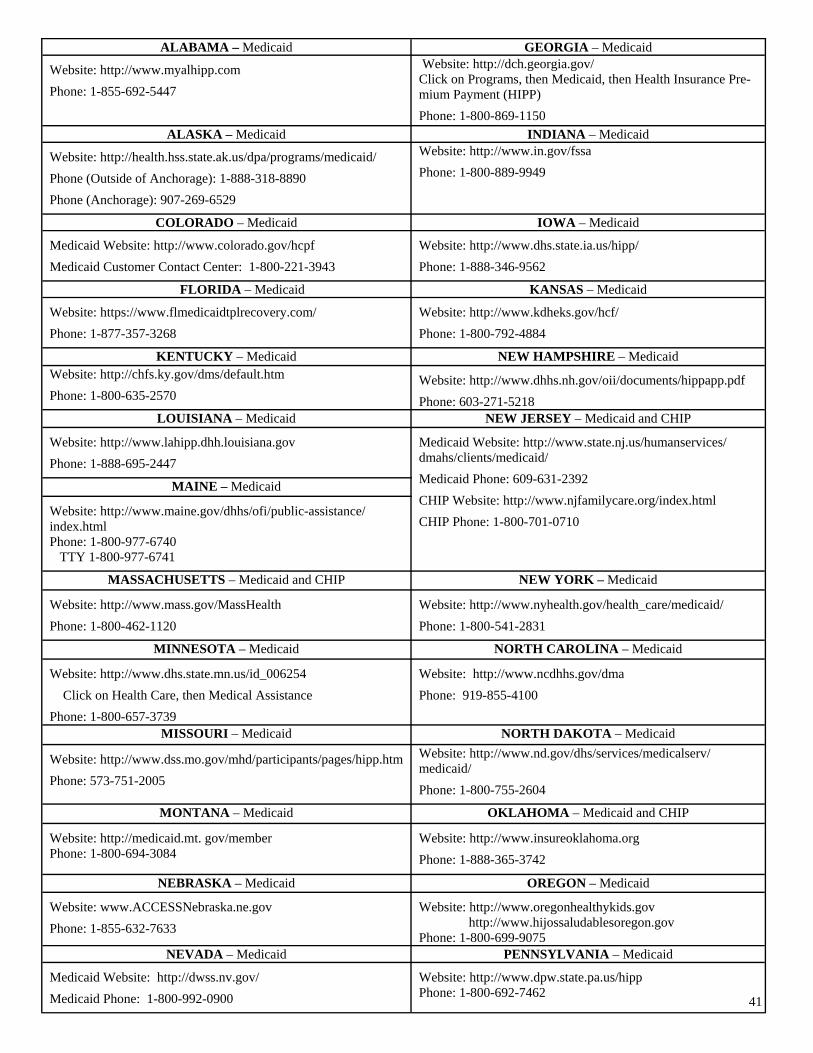
If you or your children are eligible for Medicaid or CHIP and you’re eligible for health coverage from your employer, your State may have a premium assistance program that can help pay for coverage, using funds from their Medicaid or CHIP programs. If you or your children aren’t eligible for Medicaid or CHIP, you won’t be eligible for these premium assistance programs but you may be able to buy individual insurance coverage through the Health Insurance Marketplace. For more information, visit www.healthcare.gov. If you or your dependents are already enrolled in Medicaid or CHIP and you live in a State listed below, contact your State Medicaid or CHIP office to find out if premium assistance is available. If you or your dependents are NOT currently enrolled in Medicaid or CHIP, and you think you or any of your dependents might be eligible for either of these programs, contact your State Medicaid or CHIP office or dial 1-877-KIDS NOW or www.insurekidsnow.gov to find out how to apply. If you qualify, ask your State if it has a program that might help you pay the premiums for an employer-sponsored plan. If you or your dependents are eligible for premium assistance under Medicaid or CHIP, as well as eligible under your employer plan, your employer must allow you to enroll in your employer plan if you aren’t already enrolled. This is called a “special enrollment” opportunity, and you must request coverage within 60 days of being determined eligible for premium assistance. If you have questions about enrolling in your employer plan, contact the Department of Labor at www.askebsa.dol.gov or call 1-866-444-EBSA (3272). If you live in one of the following States, you may be eligible for assistance paying your employer health plan premiums. The following list of States is current as of January 31, 2015. Contact your State for more information on eligibility –
41
ALABAMA – Medicaid GEORGIA – Medicaid Website: http://www.myalhipp.com Phone: 1-855-692-5447
Website: http://dch.georgia.gov/ Click on Programs, then Medicaid, then Health Insurance Pre-mium Payment (HIPP) Phone: 1-800-869-1150
ALASKA – Medicaid INDIANA – Medicaid Website: http://health.hss.state.ak.us/dpa/programs/medicaid/ Phone (Outside of Anchorage): 1-888-318-8890 Phone (Anchorage): 907-269-6529
Website: http://www.in.gov/fssa Phone: 1-800-889-9949
COLORADO – Medicaid IOWA – Medicaid Medicaid Website: http://www.colorado.gov/hcpf Medicaid Customer Contact Center: 1-800-221-3943
Website: http://www.dhs.state.ia.us/hipp/ Phone: 1-888-346-9562
FLORIDA – Medicaid KANSAS – Medicaid Website: https://www.flmedicaidtplrecovery.com/ Phone: 1-877-357-3268
Website: http://www.kdheks.gov/hcf/ Phone: 1-800-792-4884
KENTUCKY – Medicaid NEW HAMPSHIRE – Medicaid Website: http://chfs.ky.gov/dms/default.htm Phone: 1-800-635-2570
Website: http://www.dhhs.nh.gov/oii/documents/hippapp.pdf Phone: 603-271-5218
LOUISIANA – Medicaid NEW JERSEY – Medicaid and CHIP Website: http://www.lahipp.dhh.louisiana.gov Phone: 1-888-695-2447
Medicaid Website: http://www.state.nj.us/humanservices/ dmahs/clients/medicaid/ Medicaid Phone: 609-631-2392 CHIP Website: http://www.njfamilycare.org/index.html CHIP Phone: 1-800-701-0710
MAINE – Medicaid Website: http://www.maine.gov/dhhs/ofi/public-assistance/index.html Phone: 1-800-977-6740 TTY 1-800-977-6741
MASSACHUSETTS – Medicaid and CHIP NEW YORK – Medicaid Website: http://www.mass.gov/MassHealth Phone: 1-800-462-1120
Website: http://www.nyhealth.gov/health_care/medicaid/ Phone: 1-800-541-2831
MINNESOTA – Medicaid NORTH CAROLINA – Medicaid Website: http://www.dhs.state.mn.us/id_006254 Click on Health Care, then Medical Assistance Phone: 1-800-657-3739
Website: http://www.ncdhhs.gov/dma Phone: 919-855-4100
MISSOURI – Medicaid NORTH DAKOTA – Medicaid Website: http://www.dss.mo.gov/mhd/participants/pages/hipp.htm Phone: 573-751-2005
Website: http://www.nd.gov/dhs/services/medicalserv/medicaid/ Phone: 1-800-755-2604
MONTANA – Medicaid OKLAHOMA – Medicaid and CHIP Website: http://medicaid.mt. gov/member Phone: 1-800-694-3084
Website: http://www.insureoklahoma.org Phone: 1-888-365-3742
NEBRASKA – Medicaid OREGON – Medicaid Website: www.ACCESSNebraska.ne.gov Phone: 1-855-632-7633
Website: http://www.oregonhealthykids.gov http://www.hijossaludablesoregon.gov Phone: 1-800-699-9075
NEVADA – Medicaid PENNSYLVANIA – Medicaid Medicaid Website: http://dwss.nv.gov/ Medicaid Phone: 1-800-992-0900
Website: http://www.dpw.state.pa.us/hipp Phone: 1-800-692-7462

42
To see if any more States have added a premium assistance program since January 31, 2015, or for more information on special enrollment rights, you can contact either: U.S. Department of Labor U.S. Department of Health and Human Employee Benefits Security Administration Services www.dol.gov/ebsa Centers for Medicare & Medicaid 1-866-444-EBSA (3272) Services www.cms.hhs.gov 1-877-267-2323, Menu Option 4 Ext. 61565
RHODE ISLAND – Medicaid VIRGINIA – Medicaid and CHIP
Website: www.ohhs.ri.gov Phone: 401-462-5300
Medicaid Website: http://www.coverva.org/programs_premium_assistance.cfm Medicaid Phone: 1-800-432-5924 CHIP Website: http://www.coverva.org/programs_premium_assistance.cfm CHIP Phone: 1-855-242-8282
SOUTH CAROLINA – Medicaid
Website: http://www.scdhhs.gov Phone: 1-888-549-0820
SOUTH DAKOTA - Medicaid WASHINGTON – Medicaid
Website: http://dss.sd.gov Phone: 1-888-828-0059
Website: http://www.hca.wa.gov/medicaid/premiumpymt/pages/ index.aspx Phone: 1-800-562-3022 ext. 15473
TEXAS – Medicaid WEST VIRGINIA – Medicaid
Website: https://www.gethipptexas.com/ Phone: 1-800-440-0493
Website: www.dhhr.wv.gov/bms/ Phone: 1-877-598-5820, HMS Third Party Liability
UTAH – Medicaid and CHIP WISCONSIN – Medicaid
Website: Medicaid: http://health.utah.gov/medicaid CHIP: http://health.utah.gov/chip Phone: 1-866-435-7414
Website: https://www.dhs.wisconsin.gov/badgercareplus/p-10095.htm Phone: 1-800-362-3002
VERMONT– Medicaid WYOMING – Medicaid
Website: http://www.greenmountaincare.org/ Phone: 1-800-250-8427
Website: http://health.wyo.gov/healthcarefin/equalitycare Phone: 307-777-7531
43
C. Notice of Exchange Health Insurance Marketplace Coverage Options and Your Health Coverage Beginning in 2014, there is a new way to buy health insurance: the Health Insurance Marketplace. To assist you as you evaluate options for you and your family, this notice provides some basic information about the new Marketplace.
What is the Health Insurance Marketplace?
The Marketplace is designed to help you find health insurance that meets your needs and fits your budget. The Marketplace offers "one-stop shopping" to find and compare private health insurance options. You may also be eligible for a new kind of tax credit that lowers your monthly premium right away.
The 2017 open enrollment period for health insurance coverage through the Marketplace runs from Nov. 1, 2016, through Jan. 31, 2017. Individuals must enroll or change plans prior to Dec. 15, 2016, for coverage starting as early as Jan. 1, 2017. After Jan. 31, 2017, you can get coverage through the Marketplace for 2017 only if you qualify for a special enrollment period or are applying for Medicaid or the Children’s Health Insurance Program (CHIP).
Can I Save Money on my Health Insurance Premiums in the Marketplace?
You may qualify to save money and lower your monthly premium, but only if your employer does not offer coverage, or offers cov-erage that doesn't meet certain standards. The savings on your premium that you're eligible for depends on your household income.
Does Employer Health Coverage Affect Eligibility for Premium Savings through the Marketplace?
Yes. If you have an offer of health coverage from your employer that meets certain standards, you will not be eligible for a tax credit through the Marketplace and may wish to enroll in your employer's health plan. However, you may be eligible for a tax credit that lowers your monthly premium or a reduction in certain cost-sharing if your employer does not offer coverage to you at all or does not offer coverage that meets certain standards.
If the cost of a plan from your employer that would cover you (and not any other members of your family) is more than 9.5 percent of your household income for the year (9.56 percent for 2015), or if the coverage your employer provides does not meet the "minimum value" standard set by the Affordable Care Act, you may be eligible for a tax credit. (An employer-sponsored health plan meets the “minimum value standard” if the plan’s share of the total allowed benefit costs covered by the plan is no less than 60 per-cent of such costs.)
Note: If you purchase a health plan through the Marketplace instead of accepting health coverage offered by your employer, then you may lose the employer contribution (if any) to the employer-offered coverage. Also, this employer contribution—as well as your employee contribution to employer-offered coverage—is often excluded from income for federal and state income tax purposes. Your payments for coverage through the Marketplace are made on an after-tax basis.
How Can I Get More Information?
For more information about your coverage offered by your employer, please check your summary plan description or contact:
Kimberly Lundy, Chief of Human Resources, at 301-662-0099 or [email protected]
The Marketplace can help you evaluate your coverage options, including your eligibility for coverage through the Marketplace and its cost. Please visit HealthCare.gov for more information, as well as an online application for health insurance coverage and con-tact information for a Health Insurance Marketplace in your area.

44
II. Notices applicable to group health plans with certain benefit designs A. Wellness program disclosure If it is unreasonably difficult due to a medical condition for you to achieve the standards for the reward under this program, or if it is medically inadvisable for you to attempt to achieve the standards for the reward under this program, call the plan administrator identi-fied at the end of these notices and we will work with you to develop another way to qualify for the reward. B. Newborns’ act disclosure Group health plans and health insurance issuers generally may not, under Federal law, restrict benefits for any hospital length of stay in connection with childbirth for the mother or newborn child to less than 48 hours following a vaginal delivery, or less than 96 hours following a cesarean section. However, Federal law generally does not prohibit the mother’s or newborn’s attending provider, after consulting with the mother, from discharging the mother or her newborn earlier than 48 hours (or 96 hours as applicable). In any case, plans and issuers may not, under Federal law, require that a provider obtain authorization from the plan or the insurance issuer for prescribing a length of stay not in excess of 48 hours (or 96 hours). C. WHCRA enrollment/annual notice If you have had or are going to have a mastectomy, you may be entitled to certain benefits under the Women’s Health and Cancer Rights Act of 1998 (WHCRA). For individuals receiving mastectomy-related benefits, coverage will be provided in a manner deter-mined in consultation with the attending physician and the patient, for:
All stages of reconstruction of the breast on which the mastectomy was performed;
Surgery and reconstruction of the other breast to produce a symmetrical appearance;
Prostheses; and Treatment of physical complications of the mastectomy, including lymphedema. These benefits will be provided subject to the same deductibles and coinsurance applicable to other medical and surgical benefits pro-vided under this plan. If you would like more information on WHCRA benefits, call your plan administrator as identified at the end of these notices. For purposes of this notice, the plan administrator is: Kimberly Lundy Chief of Human Resources 301-662-0099 D. Notice for Patient Protections The following notice is provided for all plans that require or allow for the designation of primary care providers by participants or beneficiaries:
You have the right to designate any primary care provider who participates in our network and who is available to accept you or your family members. For information on how to select a primary care provider, and for a list of the participating primary care providers, contact the insurance carrier or the plan administrator identified below.
For children, you may designate a pediatrician as the primary care provider.
You do not need prior authorization from your insurance carrier or from any other person (including a primary care provider) in order to obtain access to obstetrical or gynecological care from a health care professional in our network who specializes in obstetrics or gynecology. The health care professional, however, may be required to comply with certain procedures, including obtaining prior authorization for certain services, following a pre-approved treatment plan, or procedures for making referrals. For a list of participat-ing health care professionals who specialize in obstetrics or gynecology, you may contact the insurance carrier or the plan administra-tor, Kimberly Lundy at 301-662-0099.

45
III. Notice for group health plans that provide prescription drug coverage to Medicare Part D eligible individuals Medicare Part D Creditable Coverage Notice - CIGNA OAP Low Deductible
Important Notice from Way Station, Inc. About Your Prescription Drug Coverage and Medicare
Please read this notice carefully and keep it where you can find it. This notice has information about your current prescrip-tion drug coverage offered by the group health plan through Way Station, Inc. and about your options under Medicare’s prescription drug coverage. This information can help you decide whether or not you want to join a Medicare drug plan. If you are considering joining, you should compare your current coverage, including which drugs are covered at what cost, with the coverage and costs of the plans offering Medicare prescription drug coverage in your area. Information about where you can get help to make decisions about your prescription drug coverage is at the end of this notice. There are two important things you need to know about your current coverage and Medicare’s prescription drug coverage:
1. Medicare prescription drug coverage became available in 2006 to everyone with Medicare. You can get this coverage if you join a Medicare Prescription Drug Plan or join a Medicare Advantage Plan (like an HMO or PPO) that offers prescription drug coverage. All Medicare drug plans provide at least a standard level of coverage set by Medicare. Some plans may also offer more coverage for a higher monthly premium. 2. Way Station, Inc. has determined that the prescription drug coverage offered by the group health plan through Way Station, Inc. is, on average for all plan participants, expected to pay out as much as standard Medicare prescription drug coverage pays and is therefore considered Creditable Coverage. Because your existing coverage is Creditable Coverage, you can keep this coverage and not pay a higher premium (a penalty) if you later decide to join a Medicare drug plan.
__________________________________________________________________________ When Can You Join A Medicare Drug Plan? You can join a Medicare drug plan when you first become eligible for Medicare and each year from October 15th through December 7th. However, if you lose your current creditable prescription drug coverage, through no fault of your own, you will also be eligible for a two (2) month Special Enrollment Period (SEP) to join a Medicare drug plan.

46
What Happens To Your Current Coverage If You Decide to Join A Medicare Drug Plan? If you decide to join a Medicare drug plan, your current coverage through Way Station, Inc. will not be affected. For more infor-mation on the current prescription drug option, please see the certificate of coverage. See pages 7- 9 of the CMS Disclosure of Cred-itable Coverage To Medicare Part D Eligible Individuals Guidance (available at http://www.cms.hhs.gov/CreditableCoverage/), which outlines the prescription drug plan provisions/options that Medicare eligible individuals may have available to them when they become eligible for Medicare Part D. If you do decide to join a Medicare drug plan and drop your current group health coverage through Way Station, Inc. , be aware that you and your dependents will be able to get this coverage back, subject to the terms and requirements of such group medical plan. When Will You Pay A Higher Premium (Penalty) To Join A Medicare Drug Plan? You should also know that if you drop or lose your current group health coverage through Way Station, Inc. and don’t join a Medi-care drug plan within 63 continuous days after your current coverage ends, you may pay a higher premium (a penalty) to join a Medi-care drug plan later. If you go 63 continuous days or longer without creditable prescription drug coverage, your monthly premium may go up by at least 1% of the Medicare base beneficiary premium per month for every month that you did not have that coverage. For example, if you go nineteen months without creditable coverage, your premium may consistently be at least 19% higher than the Medicare base benefi-ciary premium. You may have to pay this higher premium (a penalty) as long as you have Medicare prescription drug coverage. In addition, you may have to wait until the following October to join. For More Information About This Notice Or Your Current Prescription Drug Coverage… Contact the person listed below for further information. NOTE: You’ll get this notice each year. You will also get it before the next period you can join a Medicare drug plan, and if this coverage through Way Station, Inc. changes. You also may request a copy of this notice at any time. For More Information About Your Options Under Medicare Prescription Drug Coverage… More detailed information about Medicare plans that offer prescription drug coverage is in the “Medicare & You” handbook. You’ll get a copy of the handbook in the mail every year from Medicare. You may also be contacted directly by Medicare drug plans. For more information about Medicare prescription drug coverage:
Visit www.medicare.gov Call your State Health Insurance Assistance Program (see the inside back cover of your copy of the “Medicare & You” hand-
book for their telephone number) for personalized help Call 1-800-MEDICARE (1-800-633-4227). TTY users should call 1-877-486-2048.
If you have limited income and resources, extra help paying for Medicare prescription drug coverage is available. For information about this extra help, visit Social Security on the web at www.socialsecurity.gov, or call them at 1-800-772-1213 (TTY 1-800-325-0778).
For purposes of this notice, the plan administrator is: Kimberly Lundy Chief of Human Resources 301-622-0099
Remember: Keep this Creditable Coverage notice. If you decide to join one of the Medicare drug plans, you may be required to provcopy of this notice when you join to show whether or not you have maintained creditable coverage and, therefore, whether or not you quired to pay a higher premium (a penalty).
47
B. Medicare Part D Non-Creditable Coverage Notice - CIGNA OAPin High Deductible
Important Notice From Way Station, Inc. About Your Prescription Drug Coverage and Medicare
Please read this notice carefully and keep it where you can find it. This notice has information about your current prescrip-tion drug coverage with Way Station, Inc. and about your options under Medicare’s prescription drug coverage. This infor-mation can help you decide whether or not you want to join a Medicare drug plan. Information about where you can get help to make decisions about your prescription drug coverage is at the end of this notice. There are three important things you need to know about your current coverage and Medicare’s prescription drug cover-age:
1. Medicare prescription drug coverage became available in 2006 to everyone with Medicare. You can get this cov-erage if you join a Medicare Prescription Drug Plan or join a Medicare Advantage Plan (like an HMO or PPO) that offers prescription drug coverage. All Medicare drug plans provide at least a standard level of coverage set by Medicare. Some plans may also offer more coverage for a higher monthly premium. 2.Way Station, Inc. has determined that the prescription drug coverage offered by the CIGNA OAPin High deductible plan is, on average for all plan participants, NOT expected to pay out as much as standard Medicare pre-scription drug coverage pays. Therefore, your coverage is considered Non-Creditable Coverage. This is important because, most likely, you will get more help with your drug costs if you join a Medicare drug plan, than if you only have prescription drug coverage from the CIGNA OAPin High Deductible plan. This also is important because it may mean that you may pay a higher premium (a penalty) if you do not join a Medicare drug plan when you first become eligible. 3. You can keep your current coverage from CIGNA OAPin High Deductible plan. However, because your cover-age is non-creditable, you have decisions to make about Medicare prescription drug coverage that may affect how much you pay for that coverage, depending on if and when you join a drug plan. When you make your decision, you should compare your current coverage, including what drugs are covered, with the coverage and cost of the plans offering Medicare prescription drug coverage in your area. Read this notice carefully - it explains your options.
When Can You Join A Medicare Drug Plan? You can join a Medicare drug plan when you first become eligible for Medicare and each year from October 15th through December 7th. Since you are losing creditable prescription drug coverage under the CIGNA OAPin High Deductible plan, you are also eligible for a two (2) month Special Enrollment Period (SEP) to join a Medicare drug plan. When Will You Pay A Higher Premium (Penalty) To Join A Medicare Drug Plan? Since the coverage under the CIGNA OAPin High Deductible plan is not creditable, depending on how long you go without credita-ble prescription drug coverage you may pay a penalty to join a Medicare drug plan. Starting with the end of the last month that you were first eligible to join a Medicare drug plan but didn’t join, if you go 63 continuous days or longer without prescription drug cov-erage that’s creditable, your monthly premium may go up by at least 1% of the Medicare base beneficiary premium per month for every month that you did not have that coverage. For example, if you go nineteen months without creditable coverage, your premium may consistently be at least 19% higher than the Medicare base beneficiary premium. You may have to pay this higher premium (penalty) as long as you have Medicare prescription drug coverage. In addition, you may have to wait until the following October to join.

48
What Happens To Your Current Coverage If You Decide to Join A Medicare Drug Plan? If you decide to join a Medicare drug plan, your current Way Station, Inc. coverage will not be affected. For additional information on the prescription drug option, please see the certificate of coverage. See pages 9 - 11 of the CMS Disclosure of Creditable Cover-age To Medicare Part D Eligible Individuals Guidance (available at http://www.cms.hhs.gov/CreditableCoverage/), which outlines the prescription drug plan provisions/options that Medicare eligible individuals may have available to them when they become eligi-ble for Medicare Part D.] If you do decide to join a Medicare drug plan and drop your current Way Station, Inc. coverage, be aware that you and your depend-ents will be able to get this coverage back. For More Information About This Notice Or Your Current Prescription Drug Coverage…
Contact the person listed below for further information. NOTE: You’ll get this notice each year. You will also get it before the next period you can join a Medicare drug plan and if this coverage through Way Station, Inc. changes. You also may request a copy of this notice at any time. For More Information About Your Options Under Medicare Prescription Drug Coverage… More detailed information about Medicare plans that offer prescription drug coverage is in the “Medicare & You” handbook. You’ll get a copy of the handbook in the mail every year from Medicare. You may also be contacted directly by Medicare drug plans. For more information about Medicare prescription drug coverage:
Visit www.medicare.gov Call your State Health Insurance Assistance Program (see the inside back cover of your copy of the “Medicare & You” hand-
book for their telephone number) for personalized help Call 1-800-MEDICARE (1-800-633-4227). TTY users should call 1-877-486-2048.
If you have limited income and resources, extra help paying for Medicare prescription drug coverage is available. For information about this extra help, visit Social Security on the web at www.socialsecurity.gov, or call them at 1-800-772-1213 (TTY 1-800-325-0778).
For purposes of this notice, the plan administrator is: Kimberly Lundy Chief of Human Resources 301-622-0099