wrist Αrthroscopy review: from clinical Εxam to complex repair ioannina 2014
DESCRIPTION
Review of the clinical exam, radiologic findings and operative treatment of common wrist conditions treated with wrist arthroscopy Ομιλία στο Σεμινάριο Χειρουργικής του Χεριού, Ιωάννινα 30 Οκτ- 1 Νοε, 2014. "Ανασκόπηση της Αρθροσκόπησης στο Χέρι".TRANSCRIPT


Wrist ArthroscopyClinical applications
Nickolaos A. Darlis, MD, PhD
To access this presentation on the web:

1.Diagnostic
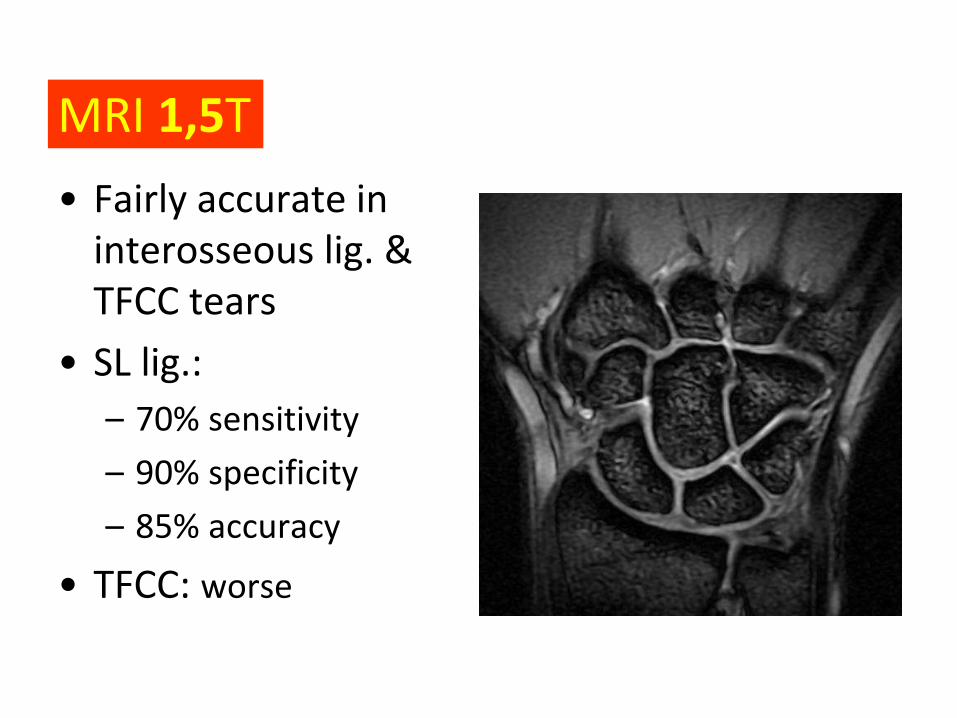
MRI 1,5T
• Fairly accurate in interosseous lig. & TFCC tears
• SL lig.:
– 70% sensitivity
– 90% specificity
– 85% accuracy
• TFCC: worse

MRI 3,0Τ
• Accuracy improved but far from excellent

1.Diagnostic

2.TFCC Lesions –DRUJ instability

3. Wrist Instability-SL LT lesions
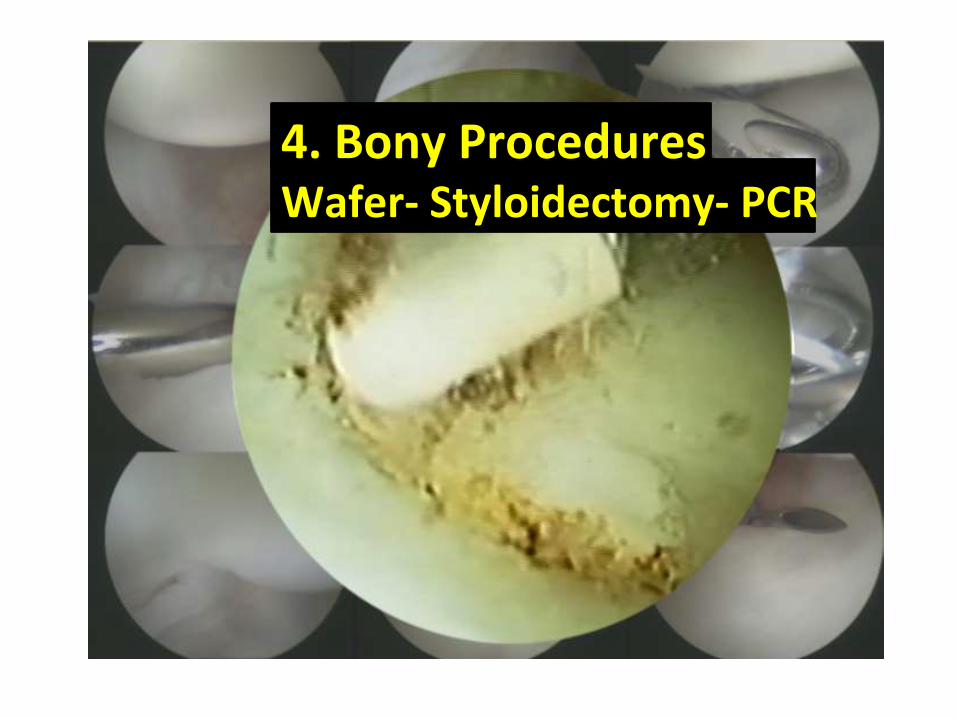
4. Bony ProceduresWafer- Styloidectomy- PCR

5.Dorsal Ganglion Resection

6.Synovectomy-Washout - Arthrolysis

7. FracturesDistal Radius- Scaphoid

#1. Radial-sided wrist pain

Radial-sided pain DD
Scaphoid fracture
SL lig. tear
Kienbock’s
AVN Scaphoid/ Preiser’s
CMC arthritis
Occult ganglion cyst
Metacarpal boss
Radiocarpal impingement

ScaphoLunate instability
Scapholunate ballottment test
Watson’s test Wrist flexion- finger extension maneuver
Anatomic snuffbox synovial irritation

Anatomic snuffbox= synovial irritation

Dorsal SL- lunate pain

Watson’s test

X-rays 1: True PA view
900 -900 position

X-rays 1: True PA view
• SL gap> 2-3mm (static instability)
• “Shortened” scaphoid
• Cortical ring sing

X-rays 2: Pronated grip view
1. Dynamic SL diastasis
2. Ulnocarpal Impingement
3. Ulnar Variance measurements

X-rays 2: Pronated grip view
NEUTRAL GRIP
Dynamic SL instability

X-rays 3: Comparative
Dynamic SL instability


Radiocarpal Arthroscopy• Always Probe the SL lig.

Geissler classification
Type I
L S

Geissler classification
Type II
L S

Geissler classification
Type III
L S

Geissler classification
Type IV
SL
C

Geissler classificationType IV

Mid-carpal Arthroscopy• Essential for accurate staging
Mid-carpal Arthroscopy• Essential for accurate staging

SL lig. lesions
• Staging
• Management •Δυναμική Αστάθεια
•Στατική Αστάθεια
•Αρθρίτιδα (SLAC)
3mo
ACUTEGood Healing Potential
CHRONICPoor Healing Potential

Acute, Geissler II, III
• Arthroscopic reduction, K-wire stabilization
L S L S

Acute, Geissler III, IV
• Open reduction, Repair
L S SL
C
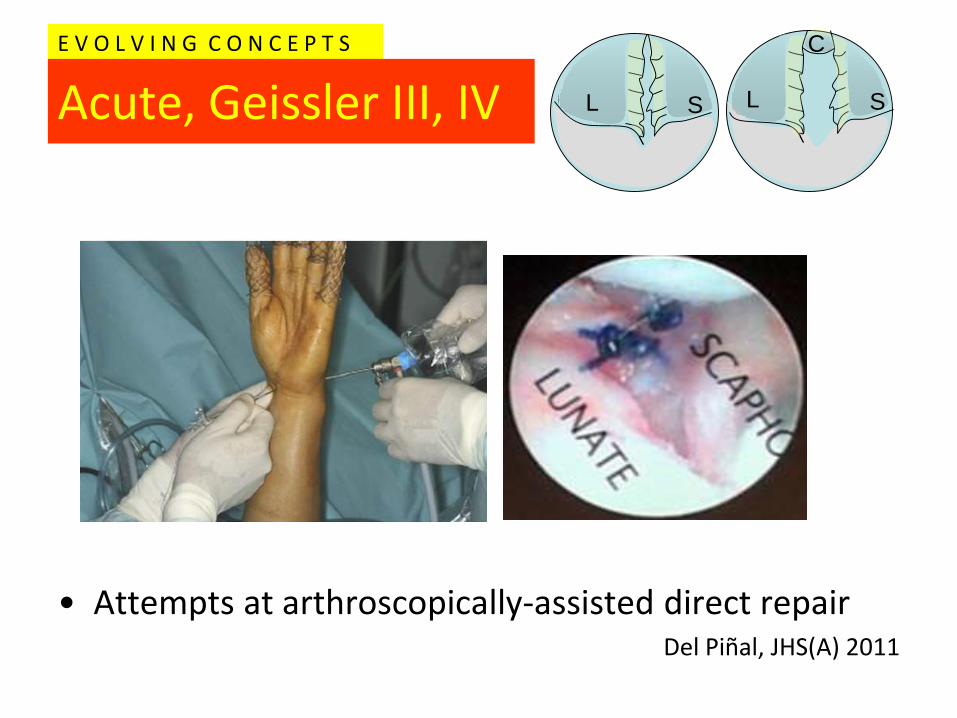
E V O L V I N G C O N C E P T S
Acute, Geissler III, IV
• Attempts at arthroscopically-assisted direct repairDel Piñal, JHS(A) 2011
L S SL
C

Chronic, Geissler I, II
• Arthroscopic debridement & pinning
L SL S

Chronic, Geissler I, II
• Thermal shrinkage & pinningDarlis & Sotereanos, JHS(A), 2005
L SL S

Chronic, Geissler III, IVDynamic Instability
• Open treatment: Capsulodesis, partial wrist arthrodesis, tendodesis, ligament reconstruction
L S SL
C

Chronic, Geissler III, IVDynamic Instability
• Aggressive arthroscopic debridement,
percutaneous pinningDarlis & Sotereanos, JHS(A), 2006
L S SL
C

Chronic, Geissler III, IVStatic Instability/Arthritis
• Open treatment: Capsulodesis, partial wrist arthrodesis, tendodesis, wrist arthrodesis
L S SL
C

Chronic, Geissler III, IVStatic Instability
• Arthroscopic Reduction and Association of the Scaphoid and Lunate (RASL) Aviles et al, Arthroscopy, 2007
L S SL
C

#2. Ulnar-sided wrist pain

Ulnar-sided pain DD
TFCC tear
LT lig. tear
DRUJ arthritis
Fracture/ Non-union Ulnar styloid
Ulnocarpal Impaction Syndrome
ECU tendinitis/ instability
Fracture hamate
Pisiform arthritis
Unlar artery thrombosis
Ulnar n. compression Guyon’s
Superficial Ulnar n. neuritis

Fovea sign
TFCC lesion

TFCC impaction
test
Nakamura/ ulnocarpal stress test
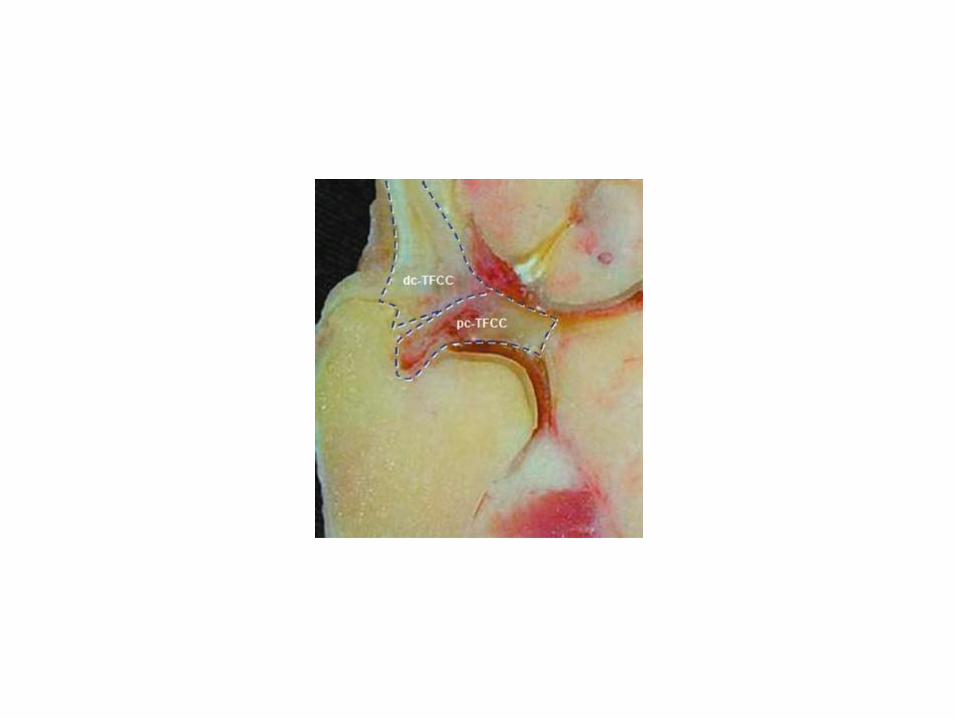
TFCC lesion

Volar & Dorsal RU lig.- Foveal attachment
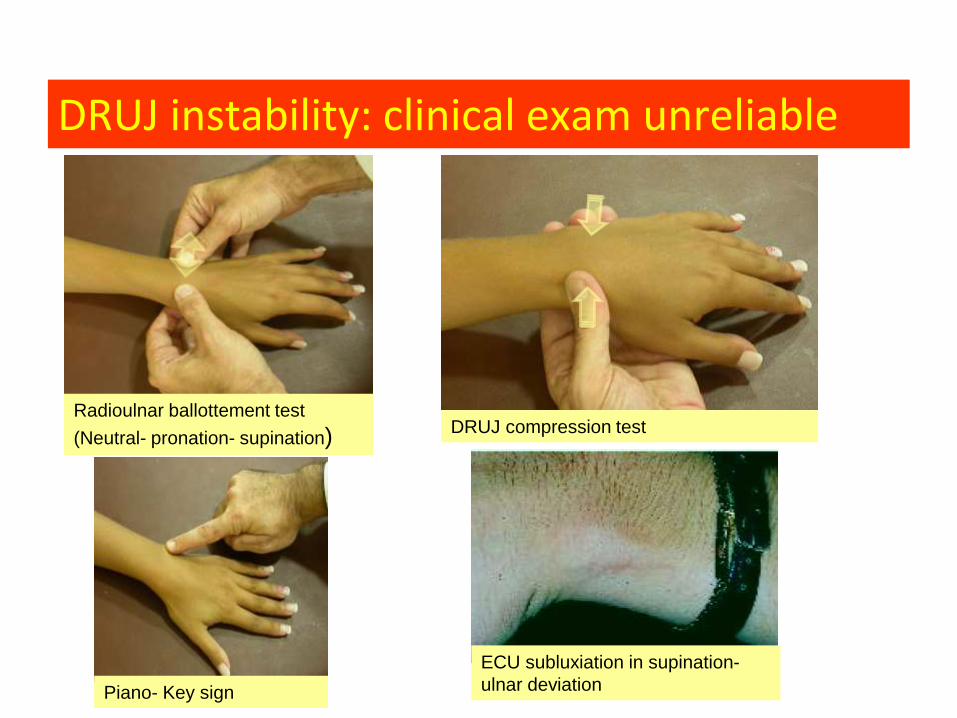
DRUJ instability: clinical exam unreliable
Radioulnar ballottement test
(Neutral- pronation- supination) DRUJ compression test
Piano- Key sign
ECU subluxiation in supination-
ulnar deviation

LT instability
LT ballottement/ Reagan’s test Kleinman’s shear test (LT)

X-rays : Pronated grip view

•Unlocarpal impaction syndrome
•Ulnar variance measurements
X-rays : Pronated grip view

Central tear
Peripheral tear)
Radial tear
Tear location
Deep bundle of TFCC
Volar radioulnar lig.radius
ulna

1. Central TFCC lesions
• Poorly vascularized- healing potential minimal
• Arthroscopic debridement up to 2/3 of articular disc
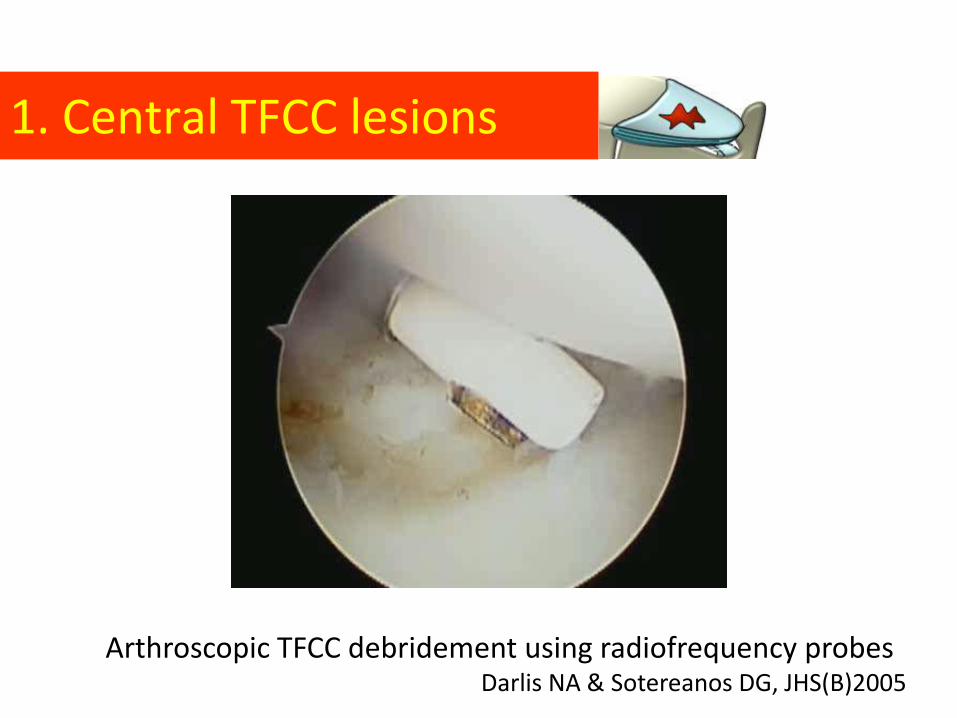
Arthroscopic TFCC debridement using radiofrequency probes Darlis NA & Sotereanos DG, JHS(B)2005
1. Central TFCC lesions

1. Central TFCC lesions
• Often degenerative and associated with ulnocarpal impaction syndrome
• Ulnar recession procedure to prevent symptom recurrence

Ulnocarpal Impaction Syndrome
Clinical features:
• Ulnar sided wrist pain
• Associated degenerative changes:
– Ulnar side of the lunate
– Radial side of the ulnar dome
– TFCC central tear
– Triquetrum- LunoTriquetrum lig.
• Usually positive or neutral ulnar variance

MRI

Arthroscopic Wafer procedure
• Preferred when modest shortening needed
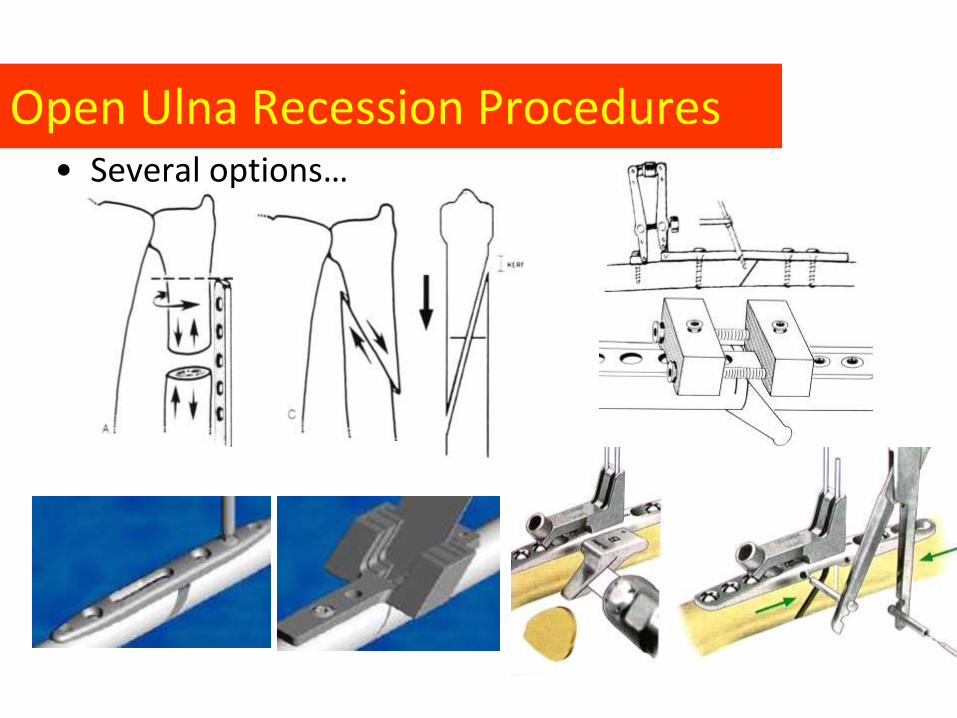
Open Ulna Recession Procedures• Several options…
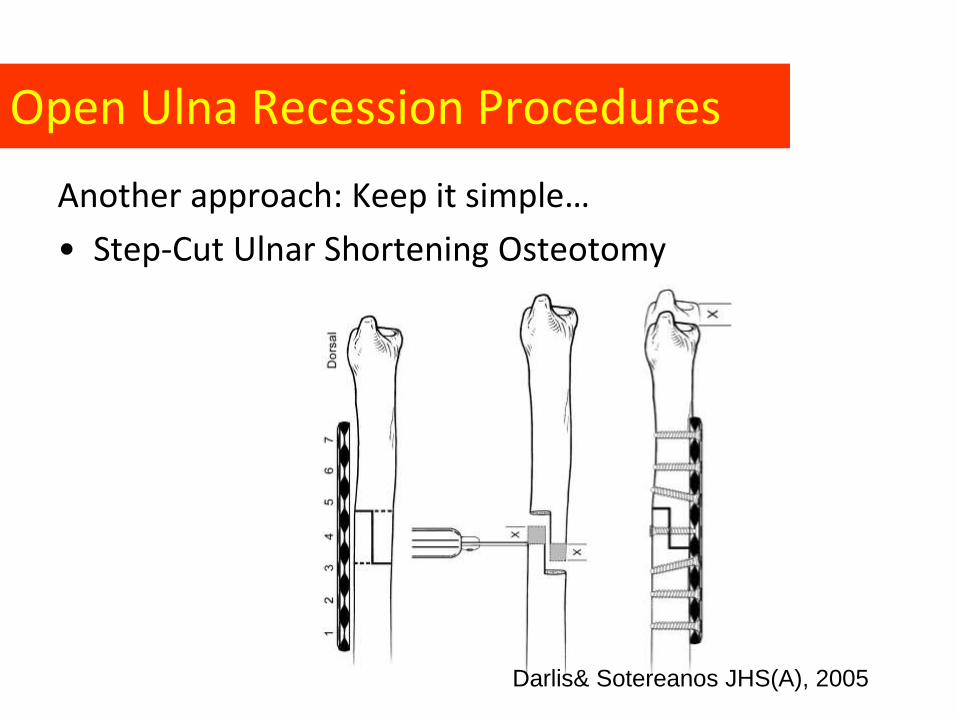
Open Ulna Recession Procedures
Another approach: Keep it simple…
• Step-Cut Ulnar Shortening Osteotomy
Darlis& Sotereanos JHS(A), 2005

2. Peripheral (ulnar) TFCC tears
• Well vascularized
• Repairable

Timing of the repair
ACUTEGood Healing Potential
SUBACUTEUnpredictable
CHRONICPoor Healing Potential
0 6 months 1 year
3mo 6mo

Usual location of peripheral tears
Dorsal

Usual location of peripheral tears

The Iceberg Concept Atzei &Lucetti 2011

REPAIR TO CAPSULE REATTACH TO FOVEAOR
TFCC TFCC
3. Peripheral (ulnar) TFCC tears

• Clinical DRUJ instability
• Fracture through the fovea
• MRI findings
• Arthroscopic findings
– Positive Hook Test
– Direct Foveal Portal Arthroscopy
Foveal attachment involvement

Hook test

REPAIR TO CAPSULE
REATTACH TO FOVEA
3. Peripheral (ulnar) TFCC tears

REPAIR TO CAPSULE

REPAIR TO CAPSULE
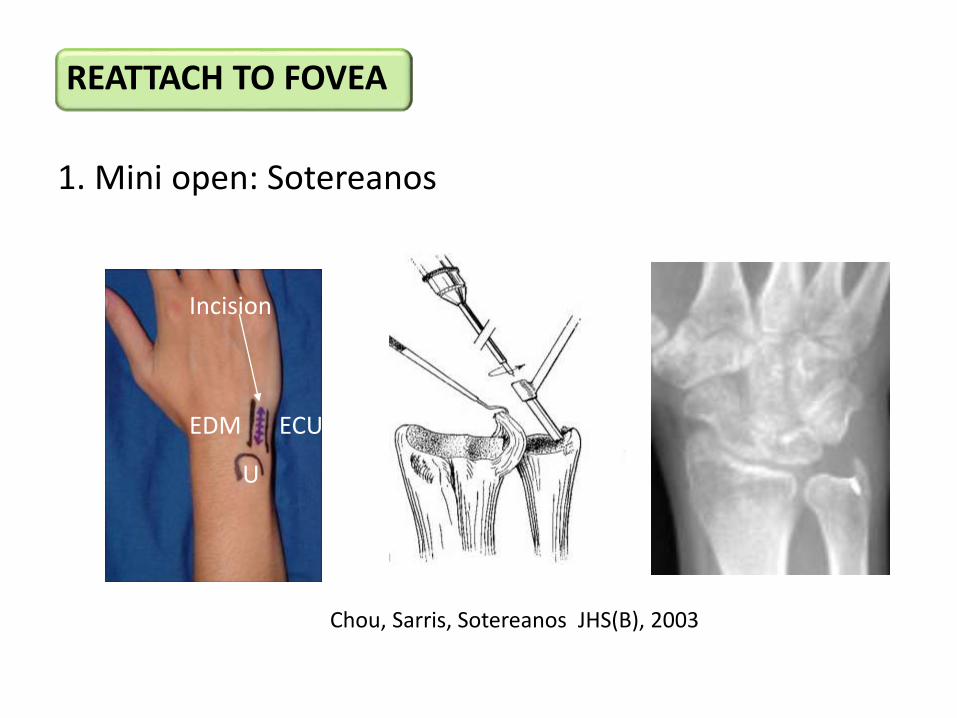
1. Mini open: Sotereanos
Chou, Sarris, Sotereanos, JHS(B), 2003
U
EDM ECU
Incision
Chou, Sarris, Sotereanos JHS(B), 2003
REATTACH TO FOVEA
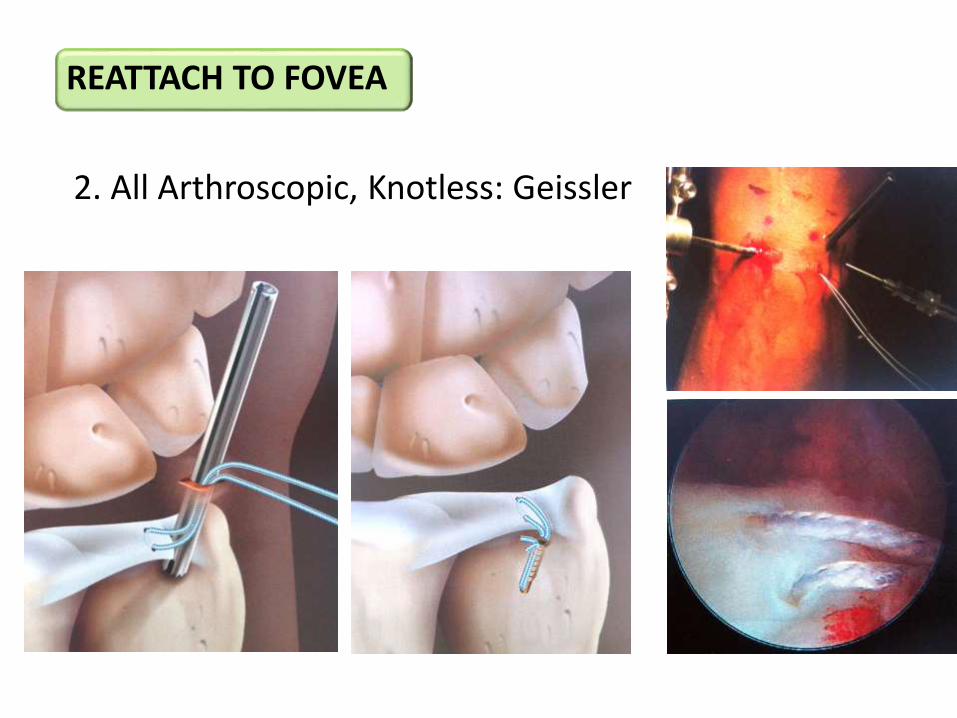
2. All Arthroscopic, Knotless: Geissler
REATTACH TO FOVEA


TFCC
6R
ACC 6R

TFCC
6R
ACC 6R

TFCC
6R
ACC 6R


TFCC
6R
ACC 6R

TFCC
6R
ACC 6R


3. Distal Radius Fracture

• Consider in young, high demand patients
• Currently indicated in selected injuries:
– Radial styloid Fx
– Die Punch Fx
– Three & Four part Fx
– DRUJ instability or interosseous lig tear
• No metaphyseal comminution
Arthroscopically assisted reduction

1. Radial styloid

1. Radial styloid

1. Radial styloid

1. Radial styloid

1. Radial styloid

1. Radial styloid

2. die punch2. Die punch

3. Three & Four part fractures

3. Three & Four part fractures3. Three & Four part fractures

3. Three & Four part fractures3. Three & Four part fractures

3. Three & Four part fractures3. Three & Four part fractures

3. Three & Four part fractures3. Three & Four part fractures

3. Three & Four part fractures3. Three & Four part fractures

3. Three & Four part fractures3. Three & Four part fractures

3. Three & Four part fractures3. Three & Four part fractures

2008, Caroline Leclercq, MD & the European Wrist Arthroscopy Society
Wrist Arthroscopy complications
Inability to complete procedure(ganglion excision, TFCC repair)
20%
Nerve Lesions(Radial and Ulnar n. sensory branches)
10%
Chondral lesions 9%
CRPS 8.5%
Traction- Potitioning(oedema, neurapraxia, stiffness)
8.5%
Loose bodies 5%
6% in 9185 procedures

European Wrist Arthroscopy Society

www.geap.org

Thank You
To access this presentation on the web: