wound management formulary and clinical pathways 2017 wound... · wound management formulary and...
TRANSCRIPT

Wound Management Formulary and Clinical Pathways 2017
Written by The Tissue Viability Team GCS.
Formulary complied by Tissue Viability Team and agreed by the CCG.

2
Gloucestershire Countywide Primary Care Wound Management Formulary Contents Page 4 Introduction 5 Important & Further Information 6-7 Debridement Pathway 8-9 Exudate Pathway 10 Fungating Wound Pathway 11 Leg Ulcer Pathway 12-13 Over Granulation Pathway 14 Pressure Ulcer Grading Pathway 15-16 Skin Tear Pathway 17 Preventing Wound Infection Pathway 18 Wound Pain Evaluation 19 Wound formulary – Barrier Creams 20 Wound formulary – Contact Layers 21 Wound formulary – Basic Adhesive Dressings 22 Wound formulary – Hydrocolloid Dressings 23 Wound formulary – Gelling Fibre Dressings 24 Wound formulary – Foam Dressings with Silicone Adhesive 25 Wound formulary – Non-Adhesive Foam Dressings 26 Wound formulary – Super Absorbent Dressings 27 Wound formulary – Hydrogel Dressings / Charcoal Dressings 28 Wound formulary – Burns Dressings 29-34 Wound formulary – Antimicrobial Dressings 35 Wound formulary – Debridement Pads / Adhesive Tapes / Dressing Packs 36 Wound formulary – Swabs / Lightweight Conforming Bandages 37 Wound formulary – Elasticated Tubular Bandages

3
38 Wound formulary – Compression Bandaging 39 Wound formulary – Layer / Multi-layer Compression Bandaging 40 Wound formulary – Therapeutic Off-loading Footwear / Medicated Bandages 41 Wound formulary – Adhesive Remover / Saline / Topical Corticosteroids 42 Wound formulary – Pressure Reducing Pads 43 Wound formulary – Protease Modulating Matrix Dressings / Acrylic Dressings 44 Wound formulary – Wound Fillers / Regenerating Matrix Therapy 45 Wound formulary – Topical Pain Management / Non Adhesive Foams 46 Wound formulary – Compression Bandaging 47 Wound formulary – Topical Negative Pressure 48 Wound formulary – Larvae 49 Wound formulary – Podiatry & MIU 50-51 Appendix 1 – Exception Reporting Forms 52 Notes

4
Reviewed Nov 2016 Printed Jan 2017 Next routine review Jan 2018
INTRODUCTION This formulary is a revised edition for 2017. It is based on the previous formulary, which was developed by The County Wide Tissue Viability Steering Group comprising of representatives from Gloucestershire Care Services (GCS) and Gloucester Hospitals NHS Foundation Trust. This formulary has been reviewed by NHS Gloucestershire Medicines Management Team, with the support of GCS Lead Tissue Viability Nurse, and other nurses with an interest in dressings within the county. Our aims are towards: • Promoting evidence based practice by providing a framework within which it is safe to practice. • Promoting continuity of care. • Promoting rational prescribing. • Supporting the practical application of nurse prescribing. • Encouraging safe, effective and appropriate use of dressings. • Cost effectiveness. These formulary choices are based on performance and stability of both the item and the manufacturing / supplying company, as well as consideration of price. Please order the exact amount of dressings required, and not necessarily the listed pack size. Supplier details and contact numbers can also be obtained from the BNF. Multi Compression bandaging should be ordered following your current protocol.

5
Other Trust and external policies and procedures that are relevant to this Formulary include: • NHS Gloucestershire Care Services’ POPAM (Policy on ordering, Prescribing and Administering Medicines) • Nursing Procedures – The Royal Marsden Manual of Clinical nursing Procedure 8th edition.
A Nurse Order form is available to use when requesting FP10 supply. If a non-formulary product is used, a Non-Formulary Exception Reporting Form (available as Appendix 1) must be completed and returned to: The Lead Tissue Viability Nurse, Gloucestershire Care Services, Edward Jenner Court, Pioneer Avenue, Gloucester Business Park, Brockworth, Gloucester, GL3 4AW. Where non-formulary products are identified repeatedly, we can consider revising the formulary. Your feedback is important. Always follow manufacturer’s guidelines when applying products. This formulary contains clinical pathways designed to guide you in your clinical decisions and to ensure quality in healthcare and the standardisation of care processes.
It is fundamental that dressings with active pharmacies are not mixed, i.e. iodine and honey.
This will alter the pharmacy and the practitioner will not know the exact pharmacy they are putting on the wound bed.

.
T
DEBRIDE if not contraindicated
When not to debride
If patient has any of the following: Mummified digits, diabetic toes (some areas such as exposed
tendons may need to be kept moist) or necrotic palliative wounds. Any foot necrosis including
heels and digits: assess circulation first
Tissue type present
Non-viable? Slough necrosis or haematoma
Diabetic foot wounds should be referred to diabetic podiatry - consider high risk of infection.
Non-specialist debridement methods as
per formulary
If debridement is required promptly for example to prepare wound for VAC
therapy refer to TV team for specialist advice
Formulary dressings to aid autolytic debridement:
KerraLite Cool, ActivHeal Hydrogel.
Antimicrobial cover: Activon Honey / Algivon
Flaminal Hydro / Forte
Consider Debrisoft for superficial slough management and removal of hyperkeratosis
Two week challenge
Use your selected dressing for two weeks. If no progress use alternative
product.
If debridement is delayed after four weeks refer to tissue viability
If No?
Consult with TV if further advice needed: Consider Inadine dressings to manage dry
necrosis
Assess the wound using TIMES Underlying cause? site,
measurements
Assess the patient holistically including past medical history, medication and
nutritional status
How?
Autolytic (Using dressings), Mechanical (Debrisoft), Larval, Sharp (competent
practitioner ) Surgical ( surgeon )
Wound bed preparation using TIMES-
Tissue- type? viable
Infection
Moisture
Edges
Skin
The removal of non-viable tissue from the wound bed until healthy tissue exposed is an essential part of chronic wound healing. Follow suggested pathway to inform debridement method:
DEBRIDEMENT PATHWAY
Types of Non Viable Tissue.
May be yellow, grey, blue, brown or black. Have a slimy consistency
or form a hard eschar.
Forms of non viable tissue are: necrotic, slough, fibrous and
compromised tissue .

7
Why debride? Chronic wounds often contain necrotic or sloughy tissue, which can harbor bacteria and act as a barrier to healing. The availability of nutrients and oxygen and presence of ischemic tissue make this an ideal environment in which both aerobic and anaerobic bacteria can multiply (White and Cutting, 2008), increasing the risk of malodour and infection. Debridement of sloughy/necrotic tissue is one of the cornerstones of good wound practice and vital when reducing the bacterial burden within the wound (Vowden and Vowden 1999a; Vowden and Vowden 1999b).
When is referral necessary?
If any doubt exists as to the diagnosis or treatment pathway referral should be made to specialist services, tissue viabilty, diabetic podiatry, vascular specialists.
References:
Vowden,K. Vowden,P. Debridement made easy Wounds UK 2011:7(4)
8
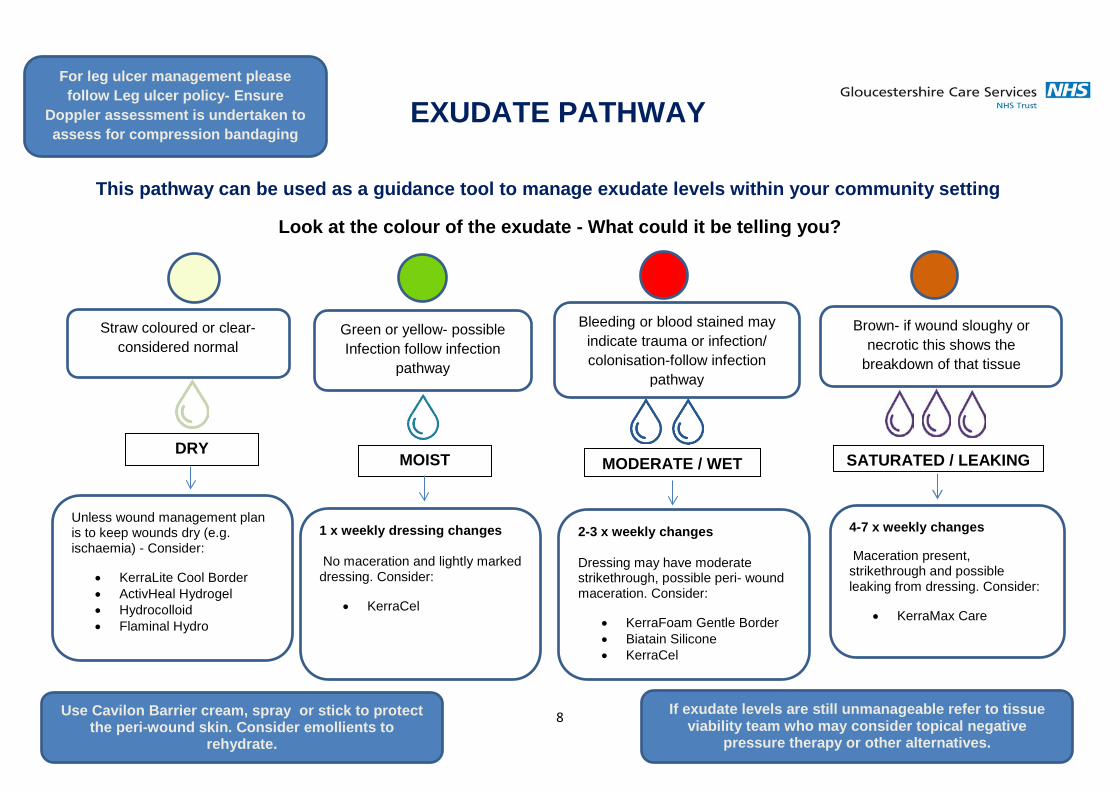
EXUDATE PATHWAY This pathway can be used as a guidance tool to manage exudate levels within your community setting
Look at the colour of the exudate - What could it be telling you?
DRY MOIST MODERATE / WET SATURATED / LEAKING
For leg ulcer management please follow Leg ulcer policy- Ensure
Doppler assessment is undertaken to assess for compression bandaging
If exudate levels are still unmanageable refer to tissue viability team who may consider topical negative
pressure therapy or other alternatives.
Straw coloured or clear- considered normal
Green or yellow- possible Infection follow infection
pathway
Bleeding or blood stained may indicate trauma or infection/ colonisation-follow infection
pathway
Brown- if wound sloughy or necrotic this shows the
breakdown of that tissue
Unless wound management plan is to keep wounds dry (e.g. ischaemia) - Consider:
• KerraLite Cool Border • ActivHeal Hydrogel • Hydrocolloid • Flaminal Hydro
1 x weekly dressing changes
No maceration and lightly marked dressing. Consider:
• KerraCel
2-3 x weekly changes
Dressing may have moderate strikethrough, possible peri- wound maceration. Consider:
• KerraFoam Gentle Border • Biatain Silicone • KerraCel
4-7 x weekly changes
Maceration present, strikethrough and possible leaking from dressing. Consider:
• KerraMax Care
Use Cavilon Barrier cream, spray or stick to protect the peri-wound skin. Consider emollients to
rehydrate.
9
Supporting information
Exudate supports healing by providing a moist wound environment. The main role of exudate is in facilitating the diffusion of vital healing factors such as immune defence by removing bacteria and the migration of cells across the wound bed. It also promotes cell proliferation, provides nutrients for cell metabolism and aids autolysis of necrotic or damaged tissue (Romanelli, et al 2010).
Although a moist wound environment is necessary for optimal wound healing, over- or under-production of exudate may adversely affect healing. Factors such as bacterial colonisation can contribute to excess exudate production; therefore it is important when assessing a wound that a holistic approach is taken to explore why exudate levels are high so appropriate treatment can be commenced.
High exudate levels can cause peri-wound maceration therefore it is important to use skin barrier products to protect your patient. Also consider the impact of exudate on a patients day to day life, such as soiled clothing and odour control, this may lead to social isolation and therefore it is vital that we manage exudate as efficiently as possible (Beldon 2016).
References
Beldon P. (2016). How to recognise, assess and control wound exudate. JCN wound care. 30 (2), 32-38.
Davies, P. (2012). Exudate assessment and management. Wound Care. S (1), 18-24.
M Romanelli, K Vowden, D Weir. Exudate Management Made Easy. Wounds International 2010; 1(2):
Available from http://www.woundsinternational.comVowden K, Vowden P. Understanding exudate management and the role of exudate in the healing process. Br JCommunity Nurse 2003; 8(11 Suppl): 4-13.

Fungating wounds are complex and therefore management should be individualised for each patient.
The below pathway is categorised with different issues that can occur with this wound type giving suggestions to support care.
Pain and discomfort Assess pain levels using wound pain assessment.
Consider breakthrough
analgesia and give prior to dressing changes.
If still unmanageable topical
morphine may be considered --Refer to GCS managing
Fungating Wound Guidelines for further information.
Exudate High absorbent
dressings may be indicated to manage
exudate- Follow exudate Pathway.
Infection Refer to GCS preventing
infection pathway. Consider if antimicrobial dressing
required.
Necrosis and slough Consider ActivHeal Hydrogel to aid in
debridement of non-viable tissue
Use honey dressings with caution as they may
cause bleeding.
Bleeding Consider alginate dressing-
In severe cases kaltostat alginate, topical adrenalin or tranexamic acid may be
required.
hMalodour Use charcoal dressings to absorb odour - Clinisorb.
Topical metronidazole may also be indicated in severe cases. Consider alternative
antimicrobial dressings.
Itching Apply KerraLite Cool.
Oral antihistamines Menthol in aqueous Consider Polymem
dressing.
Check if patient is under care of specialist
palliative care or oncology services-
Follow advised management plan from
specialist area and liaise with them prior to changing wound
care regime
If pathway followed and wound
management advice still indicated refer to tissue viability
team for specialist advice
FUNGATING WOUND PATHWAY

LEG ULCER PATHWAY
Patients presenting with a leg ulcer require a full holistic assessment including a Doppler to obtain a current ABPI or TBPI to ascertain whether there is venous or arterial impairment.
ABPI 0.8 -1.3 TBPI 0.7-1.5
Compression bandaging to be applied as per manufacturer’s instructions eg. ankle size. Toe bandaging to be applied if toes swollen. Compression Hosiery kit if minimal exudate or patient wishes to self- care with dressings. (Jobst, Medi, Activa) Wrap around device can be used if wounds are not below malleolus If wound still present re-Doppler every 12 weeks.
Full Compression
Once the ulcer has healed continue with compression wrap system or hosiery. Re- Doppler every 6 months.
ABPI 0.7 - 0.5 TBPI 0.64-0.69
Reduced Compression
Reduced Compression bandaging to be applied as per manufacturer’s instructions eg ankle size. Wrap around device can be used setting at the appropriate level mmHg if there is no wound below the malleolus. This allows patients to self-care with dressings. (Medi, Jobst, Activa) If wound still present re-Doppler every 12 weeks.
Once the ulcer has healed continue with reduced compression and either use a wrap system or hosiery. Re-Doppler every 6 months.
ABPI <0.5 or >1.3 TBPI <0.64 or >1.5
Refer for Vascular Assessment
Urgent referral for vascular assessment if ABPI is less than 0.5 or TBPI 0.64. Non Urgent referral to vascular if ABPI greater than 1.3 or TBPI greater than 1.5
Do not apply compression. If wound present dress conservatively.
Urgo K- Two Compri2 Coban2 Actico
Urgo K-Two reduced Compri2 lite Coban2 Lite
Always protect the periwound skin with a barrier cream

OVER-GRANULATION PATHWAY Over-granulation is a soft tissue that is ‘proud’ of the wound (Peduncle) and minus the granules that represent granulation tissue. It will not progress towards healing. Common causes of over-granulation are:
• Granuloma Pyogenicium- associated with post-op surgery • Friction • Internal feeding devices such as PEG • Excess moisture • Infection
Follow this pathway to support the management of over granulation tissue within your community setting:
Over granulation tissue first noticed- Cover Biatain no adhesive for two weeks
Improvement? Continue
Are there any signs of wound infection/colonisation? If yes commence infection prevention pathway, in a lightly exuding wound continue to dress with Inadine for a further two weeks.
Improvement? If resolved consider returning to conservative dressing. If some over-granulation remains consider a further 2 weeks of antimicrobial dressings.
Deterioration or no change? Dress with Inadine. If exudate levels unmanaged follow exudate pathway.
Deterioration or no change? If wound dry consider Fludroxycortide tape.
Over-granulation still present? Refer to tissue viability (referral form available on intranet) for specialist advice, a GP referral may also be indicated if dermatology advice required.

13
Consider the cause: Overgranulation is defined as an excess of granulation tissue which is in excess. Overgranulation is also known as hypergranulation, exuberant granulation tissue, or proud flesh and usually presents in wounds healing by secondary intention. It is clinically recognised by its’ friable red, often shiny and soft appearance that is above the level of the surrounding skin (Johnson & Lea 2007) and can be healthy or unhealthy tissue (Harris & Rolstad 1994) Consider differential diagnosis: Granuloma Pyogenicium: – common cause associated with post-op surgery. Presents as small erythematous papules, which may exude heavily and bleed. This may need a referral back to surgeon. Other causes include: Friction eg from PEG tube, excess moisture, infection Remember: Healthy granulation tissue - treat with pressure or steroid Unhealthy granulation tissue – may be extremely friable and require antibiotics due to infection. Malignancies: May resemble over granulation tissue References : Achieving effective outcomes in patients with over-granulation WCA UK (2011)

14
Equipment
PRESSURE ULCER GRADING
Diagnosis and contributing factors:
• Areas over bony prominence • Assess if secondary to medical equipment • Is moisture a contributing factor- assess if moisture lesion, consider continence assessment • Has a risk assessment been undertaken previously if patient already under your care, what can be learnt
from this reflect and assess why pressure damage has occurred.
Mirrored appearance superficial skin loss consider barrier cream
Actions to take • Datix • Braden • Must • Assess equipment
needs • Inform management
plan how often repositioning is required
• Appropriate wound care
• Tissue viability referral for grade 3/4- form available on intranet
Blanching/ Non blanching erythema
Press red area to
skin for 5 seconds if
unchanged this is a grade 1
Grade 2
May present as blister or superficial skin loss but not full thickness
skin loss
Grade 3
Full thickness skin loss damage to
subcutaneous tissue only and not to
underlying structures
Grade 4
Deep tissue injury which extends down
to underlying structures including
Use Kerrapro on unbroken skin to help redistribute
pressure.
Equipment
Ensure when selecting pressure reliving equipment that it does not restrict patients mobility further.
Ensure a good seated positon when selecting a cushion to promote pressure redistribution.
Refer to ICES for further equipment support
Ungradable
Where the depth of pressure damage cannot be seen secondary to the presence of non-
viable tissue

SKIN TEAR PATHWAY
rfdsssssssssssssssssssssssssssssssssssssss
Follow this pathway to inform your assessment and management of skin tears within your community setting
SKIN TEAR IDENTIFIED
ASSESS
CLEANSE
Cleanse with normal saline
REALIGN WOUND EDGES (If possible)
CONTROL BLEEDING
Elevate limb if possible, apply pressure using
gauze
CLASSIFY (MEASURE AND
DOCUMENT) Refer to GCS Guidelines on
management of acute traumatic wounds – see
pictures
Use gloved moistened finger to encourage
flap to realign
Avoid fixator strips, do not stretch wound
edges
See supporting information for additional descriptions
Category 1a
Category 1b
Category 2a
Category 2b
Category 3
DRESSING
Dress with Biatain Lite or KerraLite Cool.
Mark with arrow and date to show direction of removal.

16
Stephen-Haynes J, Carville K. Skin tears Made Easy. Wounds International 2011; 2(4): Available from
http://www.woundsinternational.com
Skin Tear Audit Research (STAR). Silver Chain Nursing Association and School of Nursing and Midwifery,
Curtin University of Technology. Revised 4/2/2010.
Category 1a A skin tear where the edges can be realigned to the normal anatomical position (without undue stretching) and the skin or flap colour is not pale, dusky or darkened. Category 1b A skin tear where the edges can be realigned to the normal anatomical position (without undue stretching) and the skin or flap colour is pale, dusky or darkened. Category 2a A skin tear where the edges cannot be realigned to the normal anatomical position and the skin or flap colour is not pale, dusky or darkened. Category 2b A skin tear where the edges cannot be realigned to the normal anatomical position and the skin or flap colour is pale, dusky or darkened. Category 3 A skin tear where the skin flap is completely absent.

WOUND INFECTIONDo you consider the wound to be infected?
Treatment plan Commence an antimicrobial dressing
For patients with a host response consider swabbing the wound and commencing antibiotics
No Improvement in clinical symptoms If no improvement has been noticed and two or more
symptoms still present refer to tissue viability team
Document a clear rationale for the new treatment plan
CRITICAL COLONISATIONDo you consider the wound to be critically colonised?
Treatment plan Cleanse the wound with Prontosan TM solution
Commence Cutimed ® Sorbact ® to manage the increasing bacterial bioburden and prevent wound infection from occurring
Review ProcessReview the wound after 2 weeks of treatment, include the following:
Wound management -TIMES Framework Compression therapy regime
Holistic assessment of the patient
PROPHYLACTIC TREATMENTDo you consider your patient to be high risk of developing or a wound Infection?
Treatment plan Cleanse the wound with Prontosan TM solution
Commence Cutimed ® Sorbact ® to prevent increase of bacterial bioburden within the wound, preventing wound infection
Review Process Review the wound every 4 weeks, this should
include the following:Wound management - TIMES Framework
Compression therapy regime (if appropriate)Holistic assessment of the patient
REVIEW OF TREATMENT REGIME Is this pathway still the most suitable treatment option for your patient?
Based on the your recent clinical assessment are the signs and symptoms of increased bacterial bioburden reducing?
Is the wound now showing signs of progression? This would include the following:Reduced wound margins? Reduced exudate levels? Signs and symptoms of increased bacterial bioburden are or have reduced?
(Refer to when to discontinue treatment or when to seek further specialist advice for next steps)
Yes - Improved Clinical Signs and SymptomsIs your patient still or considered to be high risk of developing further wound infections?
Yes - Continue treating using the prophylactic pathway regime, reviewing every 4 weeks or until healing has occurred No - Consider discontinuing the pathway and assess the wound for a more appropriate dressing selection
Document a clear rationale for the new treatment plan
PREVENTING WOUND INFECTION PATHWAY
Mellissa Beer - Tissue Viability Nurse, Gloucestershire Care Services NHS TrustSally Irving - Tissue Viability Nurse, Gloucestershire Care Services NHS TrustDawn Stevens - Clinical Nurse Manager, BSN medical Limited
Assess your wound using the TIMES frameworkAre there any signs and symptoms of a host response? (Yes, refer patient to infected pathway)
Exudate management: is your current product selection suitable for the level and type of exudate presenting? (Refer to the exudate management pathway for guidance) Is it a non-healing chronic wound? (If yes consider any underlying causes)For cellulitis please follow local pathway (refer to fl ow diagram for celllultis)
Following assessment, decide on appropriate treatment option below
160005045 - Preventing Wound Infection Pathway Amends-v3.indd 1 06/01/2017 09:56
17
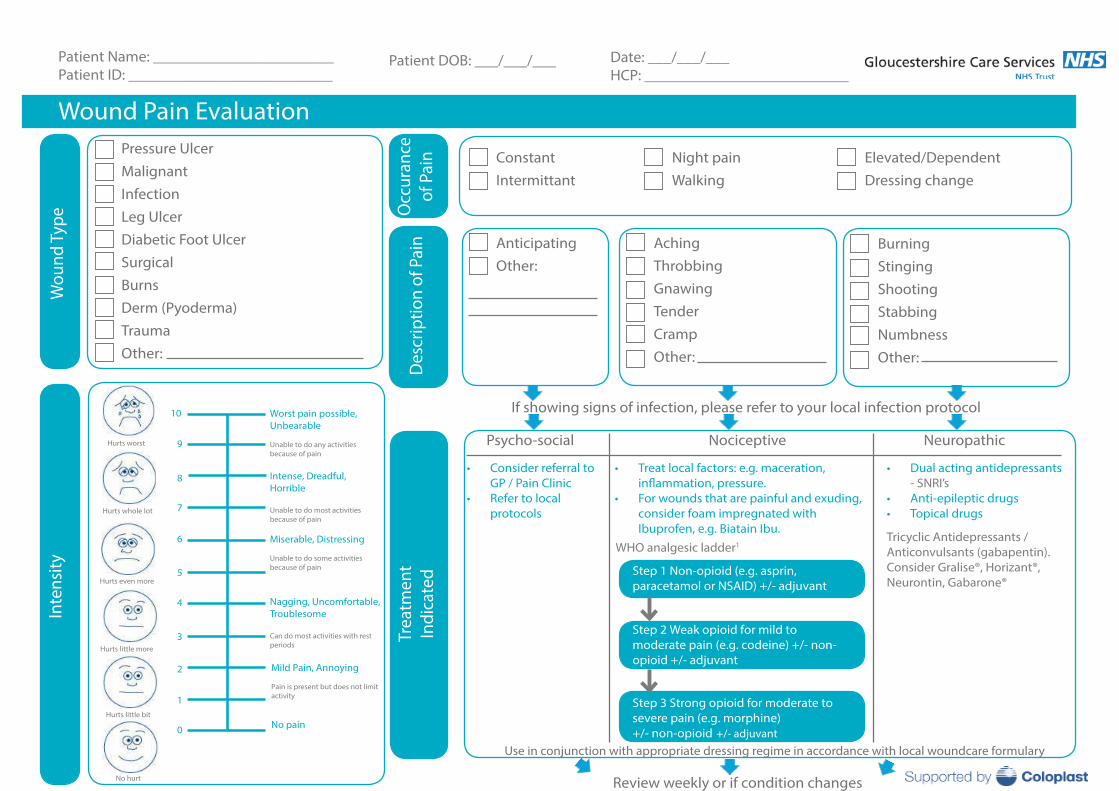
Wound Pain Evaluation
Wou
nd T
ype
Pressure Ulcer Malignant Infection Leg Ulcer Diabetic Foot Ulcer SurgicalBurns Derm (Pyoderma)TraumaOther:
Occ
uran
ce
of P
ain
Psycho-social Nociceptive Neuropathic
Trea
tmen
t In
dica
ted
Review weekly or if condition changes
Des
crip
tion
of P
ain
Inte
nsity
Tricyclic Antidepressants /Anticonvulsants (gabapentin).Consider Gralise®, Horizant®, Neurontin, Gabarone®
Patient Name: _______________________Patient ID: __________________________
Step 1 Non-opioid (e.g. asprin, paracetamol or NSAID) +/- adjuvant
WHO analgesic ladder1
Patient DOB: ___/___/___
ConstantIntermittant
Night painWalking
Elevated/DependentDressing change
AnticipatingOther:
AchingThrobbingGnawingTenderCrampOther:
BurningStingingShootingStabbingNumbnessOther:
If showing signs of infection, please refer to your local infection protocol
• Consider referral toGP / Pain Clinic
• Refer to localprotocols
• Treat local factors: e.g. maceration,
• For wounds that are painful and exuding,consider foam impregnated withIbuprofen, e.g. Biatain Ibu.
Step 2 Weak opioid for mild to moderate pain (e.g. codeine) +/- non-opioid +/- adjuvant
Step 3 Strong opioid for moderate to severe pain (e.g. morphine)+/- non-opioid +/- adjuvant
• Dual acting antidepressants- SNRI’s
• Anti-epileptic drugs• Topical drugs
Worst pain possible, Unbearable
Unable to do any activities because of pain
Intense, Dreadful, Horrible
Unable to do most activities because of pain
Miserable, Distressing
Unable to do some activities because of pain
Nagging, Uncomfortable, Troublesome
Can do most activities with rest periods
Mild Pain, Annoying
Pain is present but does not limit activity
No pain
10
9
8
7
6
5
4
3
2
1
0
Hurts worst
Hurts whole lot
Hurts even more
Hurts little more
Hurts little bit
No hurt
Date: ___/___/___HCP: __________________________
Use in conjunction with appropriate dressing regime in accordance with local woundcare formulary

19
Wound Care Formulary: Barrier Creams: Barrier cream/films are a topical formulation used to place a physical barrier between the skin and contaminants that may irritate the skin, such as exudate, this helps to prevent skin damage caused by moisture exposure. Product Manufacturer Size Tips Cavilon Barrier Film Foam Applicator
3M 1ml 3ml
Lasts for 72 hours
Cavilon Barrier Film Spray
3M 28ml
Cavilon Durable Barrier Cream
3M 2g sachet x 20 28g 92g
Lasts for 72 hours. If skin feels oily then there may be too much cream
Proshield Plus Protective Cream
H&R Healthcare 115g Can be used with highly exuding leg ulcers as well as for incontinence
Proshield Foam & Spray Cleanser
H&R Healthcare 235ml

20
Contact Layer: Wound contact layers comprise a single layer of non-adherent mesh-like material designed as protection for fragile tissue on the wound bed. They are usually used in the early, proliferative stages of healing to promote granulation and epithelialisation. Product Manufacturer Size Tips N A Ultra (Silicone coated)
Acelity 19cm x 9.5cm 9.5cm x 9.5cm
Atrauman (knitted polyester impregnated with neutral triglycerides)
Hartmann 5cm x 5cm 7.5cm x 10cm 10cm x 20cm 20cm x 30cm
ActivHeal Silicone Wound contact
Advanced Medical Solutions
5cm x 7.5cm 10cm x 10cm 10cm x 20cm 15cm x 15cm
Can be used under TNP therapy Can be left in place for 14 days

21
Basic Adhesive Dressings:
Simple dressings used for dry or lightly exuding, non-infected wounds.
Product Manufacturer Size Tips Softpore Richardson 6cm x 7cm
10cm x 10cm 10cm x 15cm 10cm x 20cm 10cm x 25cm 10cm x 30cm 10cm x 35cm
Non-woven fabric dressing with an absorbent pad for low/moderately exuding wounds
Hydrofilm Hartmann 6cm x 7cm 10cm x 12.5cm 10cm x 15cm 10cm x 25cm 12cm x 25cm 15cm x 20cm 20cm x 30cm
Film dressing which is waterproof

22
Hydrocolloid Dressings:
The gel formed when exudate is absorbed by a hydrocolloid maintains a moist wound–dressing environment while preventing fluid accumulation on the wound surface. Hydrocolloids are therefore also of value in the management of clean shallow granulating pressure ulcers.
Product Manufacturer Size Tips Comfeel Plus Transparent
Coloplast 5cm x 7cm 5cm x 15cm 5cm x 25cm 9cm x 14 cm 9cm x 25cm 10cm x 10cm 15cm x 15cm 15cm x 20cm 20cm x 20 cm
Can be used to protect the periwound area with TNP

23
Gelling Fibre Dressings:
Caboxmethyl celluose primary dressing for use on a variety of exuding wounds. Designed to lock in exudate to protect peri-wound skin from maceration, whilst helping maintain a moist healing environment.
Product Manufacturer Size Tips KerraCel Crawford Healthcare 5x 5cm
10 x 10cm 15 x 15cm 2.5 x 45cm Ribbon
UrgoClean Urgo 6cm x 6cm 10cm x 10cm 15cm x 20cm 2.5cm x 40cm 5cm x 40cm
Designed to deslough wounds but offers poly-absorbent fibres which help to manage exudate. This is not a true gelling fiber dressing.

24
Foams with Silicone Adhesive:
Silicone Foams offer superior absorption with soft adhesion; they can be used on a broad range of exuding wounds. When using foams, Silicones foams should be considered first in order to protect the peri-wound skin.
Product Manufacturer Size Tips KerraFoam Gentle Border
Crawford Healthcare 7.5cm x 7.5cm 10cm x 10cm 10cm x 20cm 12.5cm x 12.5cm 17cm x 17.5cm Sacrum 23cm x 26cm Sacrum 23cm x 25cm Heel
Biatain Silicone Lite Coloplast 7.5cm x 7.5cm 10cm x 10cm 12.5cm x 12.5cm 15cm x 15cm 17.5cm x 17.5cm
Use on non-to-low exuding wounds and skin tears.
Biatain Silicone Biatain adhesive foam
Coloplast 7.5cm x 7.5cm 10cm x 10cm 12.5cm x 12.5cm 15cm x 15cm 17.5cm x 17.5cm Sacrum Heel

25
Non Adhesive Foams:
For use when a foam dressing is required under a secondary dressing such as compression.
Product Manufacturer Size Tips Biatain Non Adhesive Coloplast 5cm x 7cm
10cm x 10cm 10cm x 20cm 15cm x 15cm 20cm x 20cm
Safe to use under compression
Foams with Adhesive:
For use when adhesive foam is required but silicone is not appropriate.
Product Manufacturer Size Tips Tegaderm Foam Adhesive (adhesive film) Oval Mini Wrap
3M 10cm x 11cm 14cm x 15cm 19cm x 22cm 6.9cm x 7.6cm 6.9cm x 6.9cm

26
Super Absorbent Dressings:
Superabsorbent dressings have extra fluid-handling capacity. They are designed to be used on wounds of varying aetiologies that produce moderate to high volumes of exudate.
Product Manufacturer Size Tips KerraMax Care Crawford Healthcare 5cm x 5cm
10cm x 10cm 10cm x 22cm 20cm x 22cm 20cm x 30cm 20cm x 50cm 21cm x 23cm Multisite
Safe to use under compression
Zetuvit E Non-Sterile Hartmann 10cm x 10cm 10cm x 20cm 20cm x 20cm 20cm x 40cm
Zetuvit E Sterile Hartmann 10cm x 10cm 10cm x 20cm 20cm x 20cm 20cm x 40cm

27
Hydrogel Dressings:
Hydrogel dressings are used in a variety of wound types and they are designed to hold moisture at the wound surface, providing the ideal environment for wound cleansing and autolytic debridement, where the body’s own enzymes debride dead tissue. The moisture donated by hydrogel dressings can help to soothe the wound and reduce pain. They can also provide a barrier to microorganisms and help to prevent infection
Product Manufacturer Size Tips KerraLite Cool Border and Non Border
Crawford Healthcare 6cm x 6cm 12cm x 8.5cm 18cm x 12.5cm 8cm x 8cm bordered 11cm x 11cm bordered 15cm x 15cm bordered
The new bordered version prevents the need for a secondary dressing
ActivHeal Hydrogel Advanced Medical Solutions
8g 15g
Charcoal Odour Dressings:
Odour–combating dressing specifically designed to target odour in a range of wounds
Product Manufacturer Size Tips Clinisorb Clinimed 10cm x 10cm
10cm x 20cm 15cm x 25cm
Both sides of the dressing are identical, not intended to be the primary dressing

28
Burns Dressings:
Please follow burns pathway for dressing selection. The dressings below are only for the use in burns as per the pathway.
Product Manufacturer Size Tips Polymem Tube Aspen 7cm x 7 cm
9cm x 9 cm
Polymem Finger & Toe Size 1, 2 or 3 Polymem 8cm x 8cm
10cm x 10cm 13cm x 13cm 17cm x 19cm
Polymem MAX 11cm x 11cm 20cm x 20cm
Polymem Roll 10cm x 61cm 20cm x 60cm

29
Antimicrobial Dressings:
An antimicrobial is an agent that kills micro-organisms or inhibits their growth. There are several types of anitimicrobial.
DACC-Coated Antimicrobial Dressings:
The physical principle of hydrophobic interaction means that bacteria and fungi become physically and irreversibly bound to the DACC dressing. This means that these dressings can be used prophylactically to prevent infection.
Product Manufacturer Size Tips Cutimed Sorbact (swabs)
BSN 4cm × 6cm 7cm × 9cm
Do not use in combination with ointments and creams as the binding effect is impaired
Cutimed Sorbact 5 Pad Pack (round)
3cm
Cutimed Sorbact (ribbon)
2cm × 50cm
Cutimed Sorbact
5cm × 2m

30
Silver Dressings:
Silver has antimicrobial activity against many antibiotic-resistant strains of bacteria. Silver may be incorporated into dressings in a number of different forms, most notably as elemental silver or in the ionic state.
Silver products should be used with caution due to their toxicity, follow the 2 week challenge.
Product Manufacturer Size Tips Askina Calgitrol Paste
BBraun
15g Supplied sterile in a tube with a long cannula to aid application of the paste into tunnels, sinuses and awkward wound shapes
Askina Calgitrol Thin 5cm x 5cm 10cm x 10cm 15 cm x 15 cm
Silver alginate matrix wound contact layer
Askina Calitrol AG 10cm x 10cm 15cm x 15cm 20cm x 20cm
The primary wound contact layer is a silver alginate that is laminated to a foam layer

31
Silver Sulphadiazine:
Usually found in a cream preparation (Flamazine®) an antibacterial contact layer with TLC-Ag Technology (polyester mesh impregnated with hydrocolloid, petroleum jelly and silver sulphadiazine particles).
Product Manufacturer Size Tips Urgotul SSD Urgo 10cm × 12cm
15cm × 20cm
Cadexomer Iodine:
Cadexomer iodine based products absorb fluids, removing exudate, pus and debris. As they swell, iodine is slowly released killing micro-organisms and forming a protective gel over the wound surface.
Product Manufacturer Size Tips Iodoflex Smith and Nephew 1 x 5g units (5)
1 x 10g units (3) 1 x 17 g units (2)

32
Povidine Iodine:
Povidone Iodine dressings deposit their iodine immediately upon application, designed to manage infection by bacterial, protozal, and fungal organisms.
Product Manufacturer Size Tips Inadine Acelity
5cm x 5cm 9.5cm x 9.5cm
Enzyme Alginogel:
Enzyme Alginogel combine the benefits of hydrogels and alginates in one product. They also incorporate unique broad spectrum antibacterial enzymes that are effective against a range of bacteria, including MRSA and can be used throughout the duration of the wound not just when infection is present.
Product Manufacturer Size Tips Flaminal Hydro Flen Pharma 15g
50g For low to moderately exuding wounds (3.5% alginate). Can be recapped as self-cleaning
Flaminal Forte 15g 50g
For moderate to heavy exuding wounds (5.5% alginate). Can be recapped as self-cleaning

33
Manuka Honey:
Manuka honey kills harmful bacteria, eliminates odours without masking them, and maintains the ideal moist wound healing environment. The osmotic effect draws harmful tissue away from the wound bed but this can cause a drawing pain.
Product Manufacturer Size Tips Activon Tulle Advancis 5cm x 5cm
10cm x 10cm
For granulating or shallow wounds, debriding or de-sloughing
Actilite 10cm x 10cm 10cm x 20cm
Designed to protect a wound, promote healing and allow the passage of exudate
Activon Tube 25g
Ideal for debriding necrotic tissue, or for topping up dressings. Good for cavities, just wash away with saline solution
Algivon 5cm x 5cm 10cm x 10cm
Ideal for wetter wounds as the alginate has a capacity to absorb

34
PHMB:
Polyhexamethylene biguanide hydrochloride (PHMB) has been used for over 60 years as an antimicrobial agent due to its broad spectrum of antimicrobial activity.
PMHB is a broad-spectrum antimicrobial and is fast and effective in killing bacteria, fungi and yeasts that reduce bioburden in critically colonised and infected wounds. There is no known resistance, systemic absorption or toxicity.
It selectively acts on bacteria without affecting healthy cells therefore suitable for long term use.
Product Manufacturer Size Tips Suprasorb X+PHMB Activa
14cm x 20 cm 2cm x 21cm rope 5cm x 5cm 9cm x 9cm
Its HydroBalance technology means it is able to absorb exudate and donate fluid at the same time Reduces pain and has soothing properties
Prontosan Wound Irrigation Solution
BBraun 350mls 40mls
Has a powerful antimicrobial agent that can reduce bioburden whilst the Betaine surfactant penetrates to clean and remove wound debris and biofilm

35
Debridement Pads:
Patented monofilament fibre technology lifts, binds and removes superficial slough and debris including biofilm quickly and easily.
Product Manufacturer Size Tips Debrisoft Activa
10cm x 10cm pads 5cm x 2cm lolly
Moisten with water or saline, do not use any cream or emollient
Adhesive Tapes:
Product Manufacturer Size Tips Clinipore
Clinisupplies 5m x 1.25cm 5m x 2.5cm 5m x 5cm 10m x 2.5cm
Hypafix
BSN 4m x 5cm 4m x 10cm 4m x 15cm
Dressing Packs:
Product Manufacturer Size Tips Nurse It Dressing Pack Medicareplus Small
Medium Large
Do not apply the gauze to a wound

36
Swabs:
Product Manufacturer Size Tips Soft Swabs Non-woven fabric swab 4ply non-sterile
Premier - Sherwood 10cm x 10cm x 100
Soft Swabs Non-woven fabric swab 4ply sterile
7.5cm x 7.5cm x 5
Light Weight Conforming Bandages:
Product Manufacturer Size Tips Hospicecrepe 239
Hartmann 4.5m x 5cm 4.5m x 7.5cm 4.5m x 10cm
K Band Bandage
Urgo 5cm x 4m 7cm x 4m 10cm x 4m 15cm x 4m
Mollelast Activa 4cm x 4cm Suitable for digit bandaging with compression bandaging

37
Elasticated Tubular Bandages:
Product Manufacturer Size Tips Comfifast Synergy Health 3.5cm (red) 1m
5cm (green) 1m 5cm (green) 3m 5cm (green) 5m 7.5cm (blue) 1m 7.5cm (blue) 3m 7.5cm (blue) 5m 10.75cm (yellow) 1m 10.75cm (yellow) 3m 10.75cm (yellow) 5m 17.5cm (beige) 1m

38
Compression Bandaging:
Compression bandages are usually 10cm wide unless specifically advised by vascular, lymphoedema, tissue viability or the complex leg wound service. Not to be carried out without the completion of the appropriate competency.
Short Stretch:
These bandages are defined as having low elasticity (or non-elastic). Short-stretch bandages deliver a low resting pressure and a high working pressure (high SSI), producing a significant massage effect on the calf-muscle when the patient is active.
Product Manufacturer Size Tips JOBST Compri2 (40mmHg)
BSN 18-25cm ankle size 25-32 cm ankle size
Has a visual indication to ensure correct pressures are achieved
JOBST Compri2 lite (20mmHg)
18-25cm ankle size 25-32 cm ankle size
Has a visual indication to ensure correct pressures are achieved
Actico (40mgHg)
Activa 5cm x 6m 6cm x 6m 8cm x 6m 10cm x 6m 12cm x 6m
39
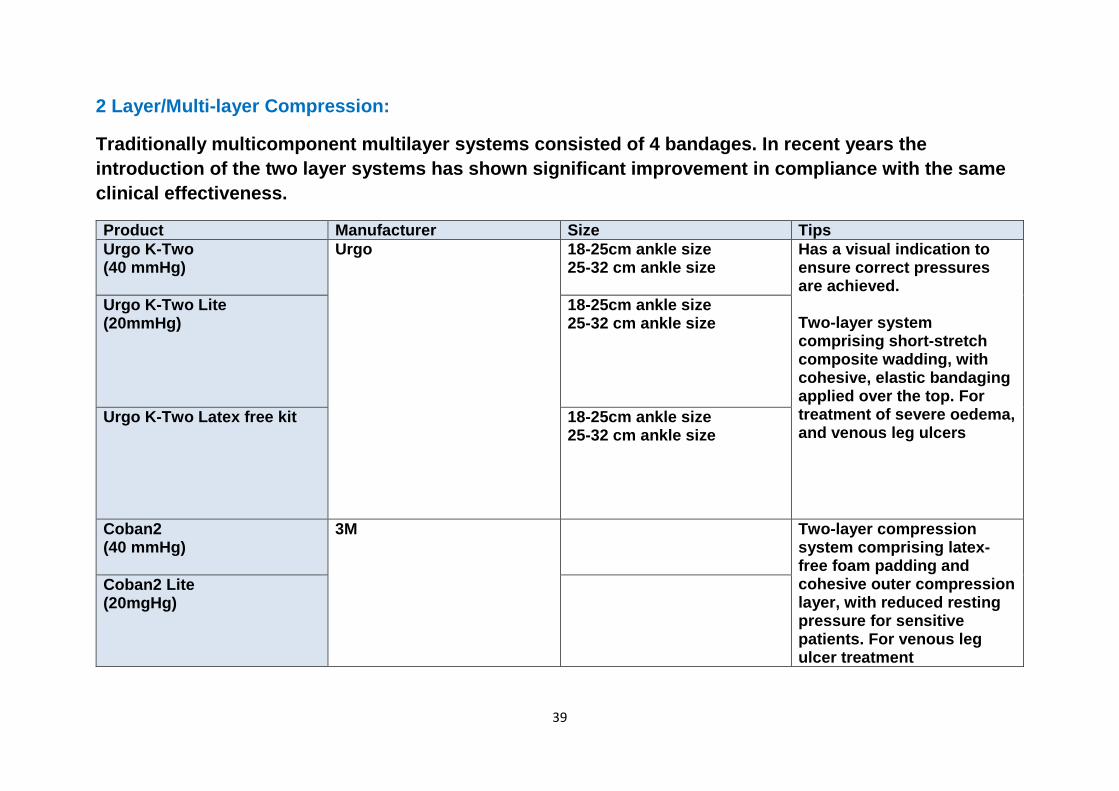
2 Layer/Multi-layer Compression:
Traditionally multicomponent multilayer systems consisted of 4 bandages. In recent years the introduction of the two layer systems has shown significant improvement in compliance with the same clinical effectiveness.
Product Manufacturer Size Tips Urgo K-Two (40 mmHg)
Urgo 18-25cm ankle size 25-32 cm ankle size
Has a visual indication to ensure correct pressures are achieved. Two-layer system comprising short-stretch composite wadding, with cohesive, elastic bandaging applied over the top. For treatment of severe oedema, and venous leg ulcers
Urgo K-Two Lite (20mmHg)
18-25cm ankle size 25-32 cm ankle size
Urgo K-Two Latex free kit 18-25cm ankle size 25-32 cm ankle size
Coban2 (40 mmHg)
3M Two-layer compression system comprising latex-free foam padding and cohesive outer compression layer, with reduced resting pressure for sensitive patients. For venous leg ulcer treatment
Coban2 Lite (20mgHg)

40
Compression: Therapeutic Off-Loading Footwear
To help prevent foot ulcers by off-loading up to 30% of pressure, from the most vulnerable parts of the foot.
Product Manufacturer Size Tips Kerraped Crawford Healthcare Small
Medium Large Extra Large
Can also be used for patients in compression bandaging
Medicated Bandages:
Designed for the wet ulcers that are surrounded by an area of sensitive skin, zinc paste bandages contain Ichthammol which soothes the skin and helps ulcers to heal.
Product Manufacturer Size Tips Zinc Paste and Ichthammol Bandage
Smith and Nephew 6m × 7.5cm

41
Adhesive Remover and Saline:
Product Manufacturer Size Tips Irripods (Sterile saline)
CD Medical 20ml (box of 25)
Peel-easy (Silicone based adhesive remover)
CD Medical 50ml aerosol
Peel-easy (Silicone based adhesive remover) wipes
Pack of 30
Topical Corticosteroids:
Topical corticosteroid therapy in an occlusive, transparent, self-adhesive and waterproof tape
Product Manufacturer Size Tips Fludroxycortide tape (Haelan Tape)
Typharma For use on over granulation- the cream can be used if the tape is unavailable
42
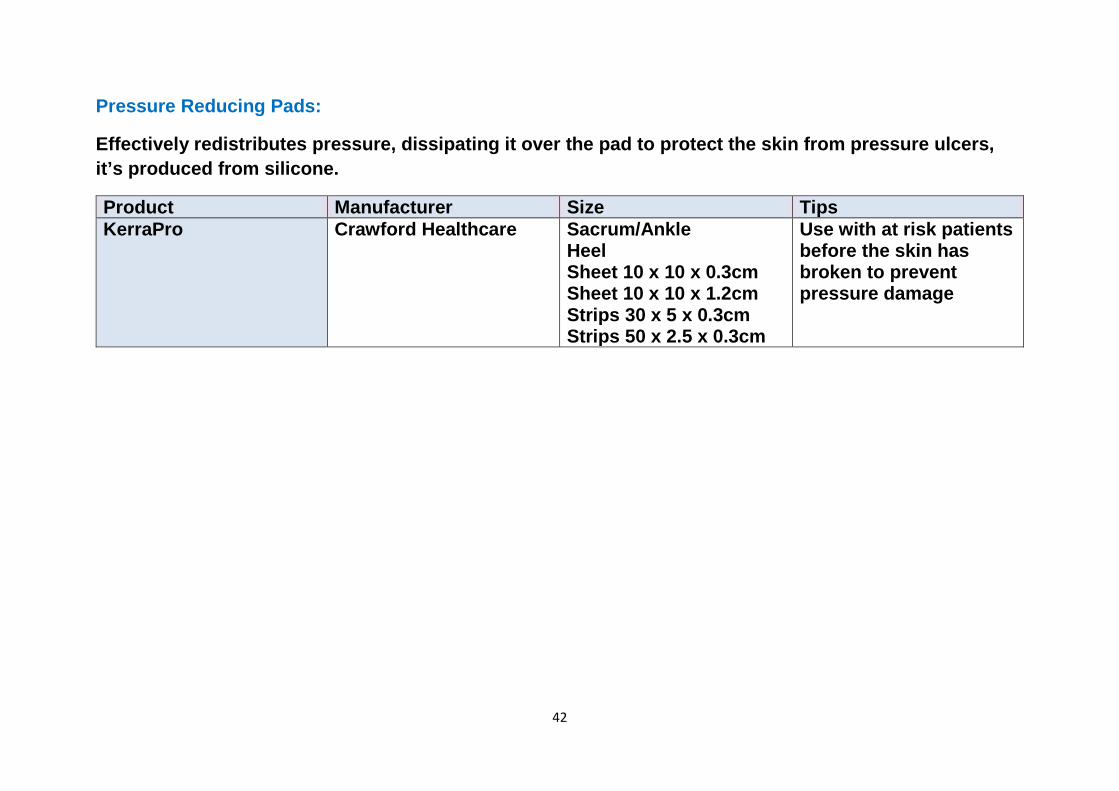
Pressure Reducing Pads:
Effectively redistributes pressure, dissipating it over the pad to protect the skin from pressure ulcers, it’s produced from silicone.
Product Manufacturer Size Tips KerraPro Crawford Healthcare Sacrum/Ankle
Heel Sheet 10 x 10 x 0.3cm Sheet 10 x 10 x 1.2cm Strips 30 x 5 x 0.3cm Strips 50 x 2.5 x 0.3cm
Use with at risk patients before the skin has broken to prevent pressure damage
43
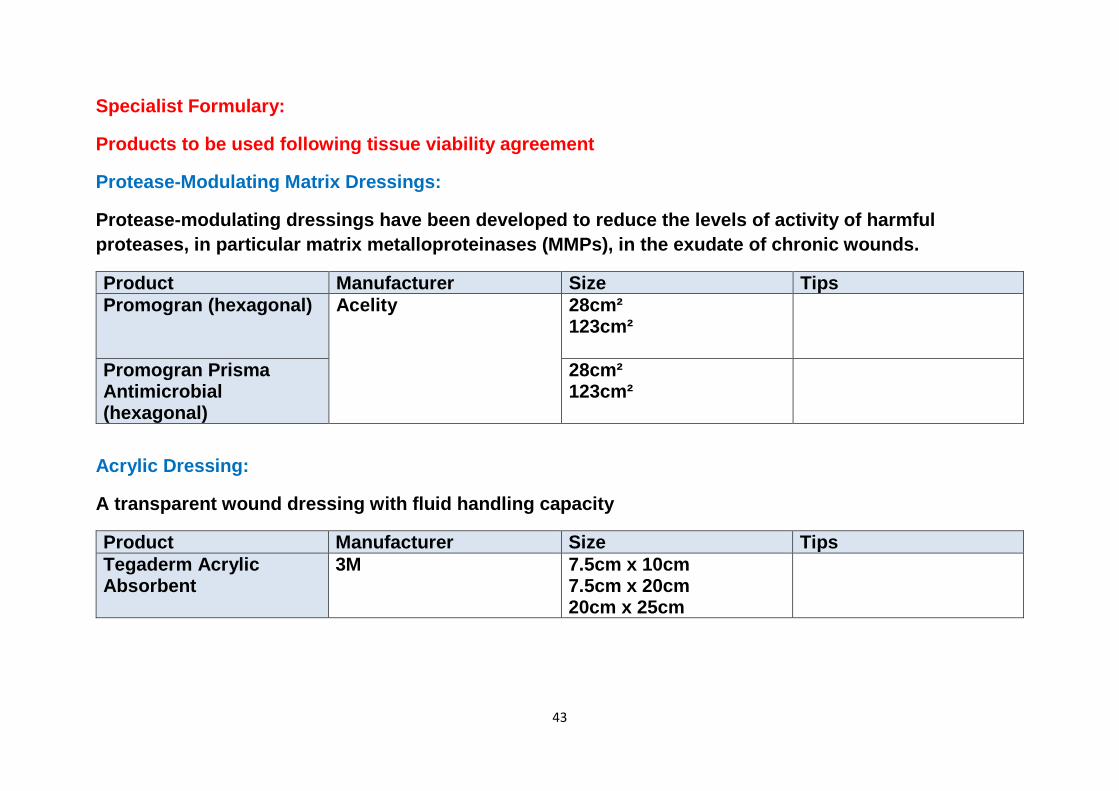
Specialist Formulary:
Products to be used following tissue viability agreement
Protease-Modulating Matrix Dressings:
Protease-modulating dressings have been developed to reduce the levels of activity of harmful proteases, in particular matrix metalloproteinases (MMPs), in the exudate of chronic wounds.
Product Manufacturer Size Tips Promogran (hexagonal) Acelity 28cm²
123cm²
Promogran Prisma Antimicrobial (hexagonal)
28cm² 123cm²
Acrylic Dressing:
A transparent wound dressing with fluid handling capacity
Product Manufacturer Size Tips Tegaderm Acrylic Absorbent
3M 7.5cm x 10cm 7.5cm x 20cm 20cm x 25cm

44
Wound Fillers:
Allevyn Cavity provides hydrocellular technology in a unique 3 dimensional structure for effective management of deep wounds.
Product Manufacturer Size Tips Allevyn Cavity Circular
Smith and Nephew 5cm 10cm
Allevyn Cavity Tubular 9cm × 2.5cm Allevyn Cavity 12cm × 4cm Allevyn Cavity Plus 5cm x 6cm
10cm x 10cm 15cm x 20cm
Regenerating Matrix Therapy:
ReGeneraTing Agents (RGTA) are engineered biodegradeable sugar based polymers that preserve the cellular microenviroment needed for tissue regeneration:
Product Manufacturer Size Tips Cacipliq20 Innocell Medical 1.5ml
5ml

45
Topical Pain Management:
See wound Pain Pathway for appropriate use
Product Manufacturer Size Tips Biatain IBU soft hold Coloplast 15cm x 15cm
10cm x 22.5cm 10cm x 12cm
A soft and flexible absorbent foam dressing containing ibuprofen which is not systemically absorbed by the body
Non Adhesive Foams:
For use when a foam dressing is required under a secondary dressing such as compression.
Product Manufacturer Size Tips Tegaderm Foams Non- Adhesive
3M 10cm x 10cm 10cm x 20cm 20cm x 20 cm
For use when formulary non adhesive foam is not sutiable
46
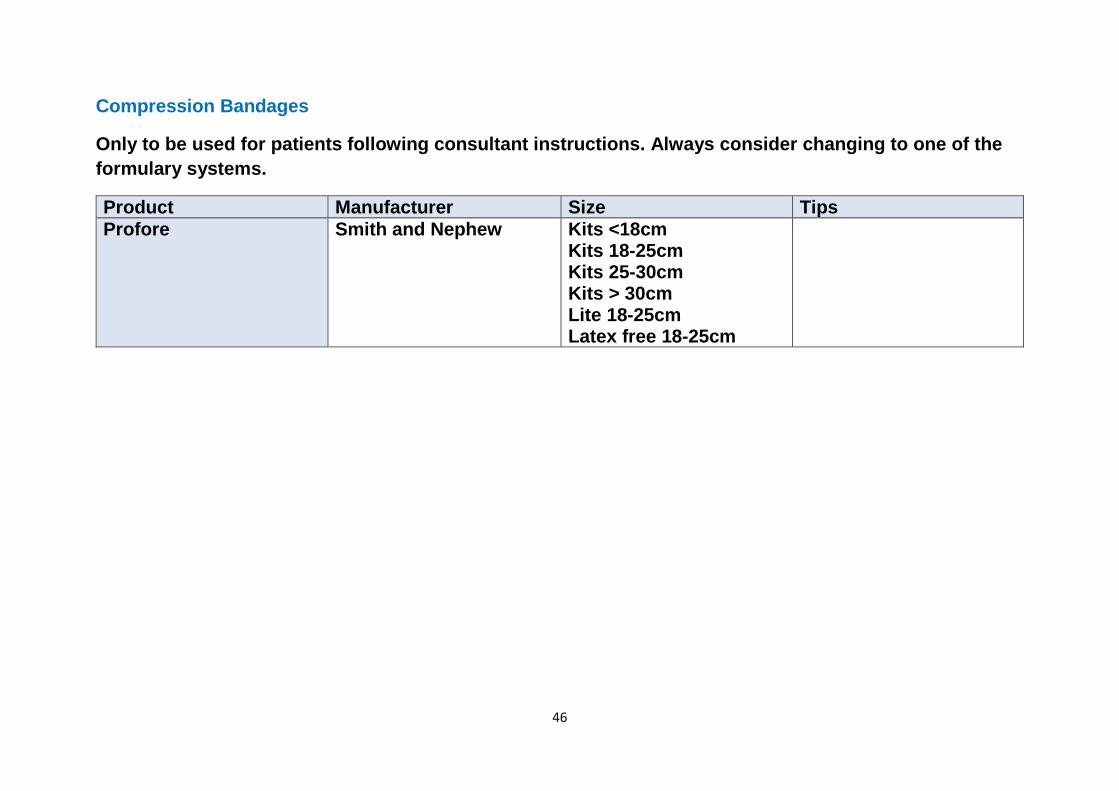
Compression Bandages
Only to be used for patients following consultant instructions. Always consider changing to one of the formulary systems.
Product Manufacturer Size Tips Profore Smith and Nephew Kits <18cm
Kits 18-25cm Kits 25-30cm Kits > 30cm Lite 18-25cm Latex free 18-25cm

47
Topical Negative Pressure (TNP)
Promotes wound healing through Topical Negative Pressure (TNP). Delivering negative pressure (a vacuum) at the wound site through a unique, proprietary dressing which helps draw wound edges together, removes infectious materials and actively promotes formation of the granulation tissue.
Not to be carried out without the completion of the appropriate competency.
Product Manufacturer Size Tips VAC Therapy Acelity (KCI) This MUST be agreed
with the Tissue Viability Team before treatment is commenced or patient accepted from the Acute Trust
PICO Smith and Nephew Canister-free and disposable This is a step up/down version of TNP and MUST be agreed by the Tissue Viability team before treatment is commenced or patient accepted from the Acute Trust

48
Larvae (Maggots) for wound debridement:
This product should not be used without consultation with the tissue viability team and completion of the appropriate competency.
Product Manufacturer Size Tips BioBag Biomonde 2.5cm x 4cm
4cm x 5cm 5cm x 6cm 6cm x 12cm 10cm x 10cm
Free Range Larvae Retention kit 30x30 cm kit with 1 vial Retention kit 30x30 cm kit with 2 vial Retention kit 30x30 cm kit with 3 vial Boot retention kit and 1 vial Boot retention kit and 2 vial Boot retention kit and 3 vial
49
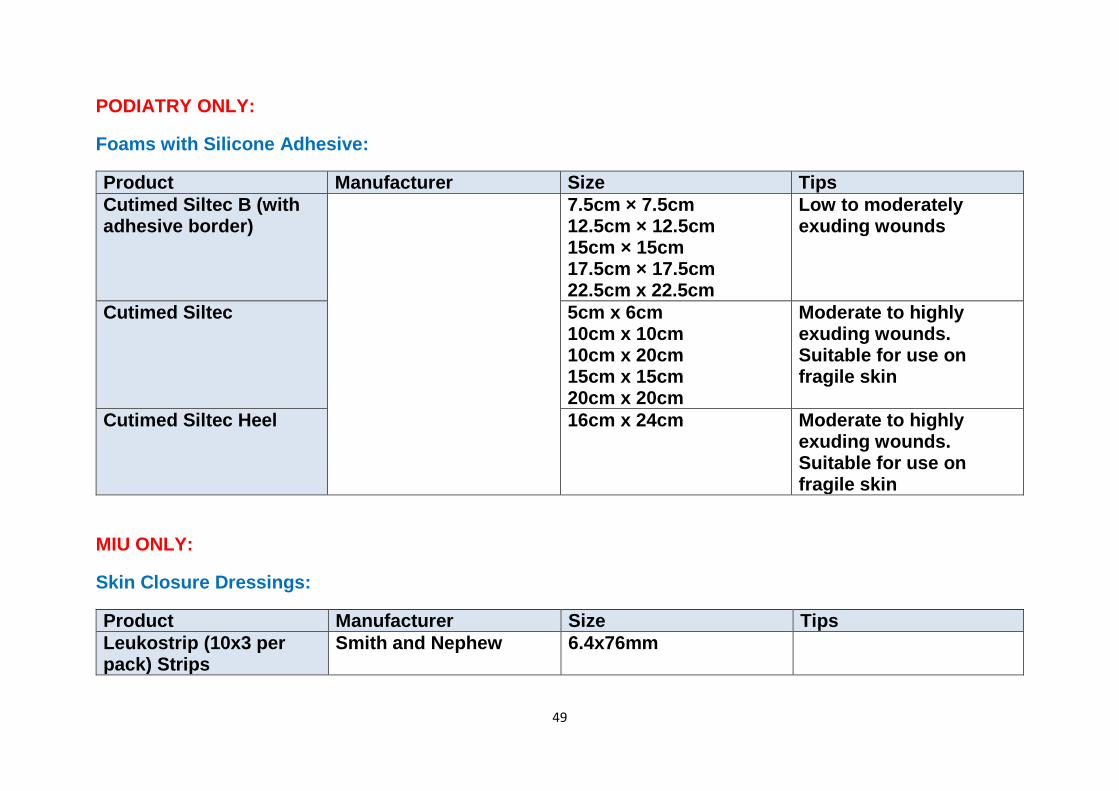
PODIATRY ONLY:
Foams with Silicone Adhesive:
Product Manufacturer Size Tips Cutimed Siltec B (with adhesive border)
7.5cm × 7.5cm 12.5cm × 12.5cm 15cm × 15cm 17.5cm × 17.5cm 22.5cm x 22.5cm
Low to moderately exuding wounds
Cutimed Siltec 5cm x 6cm 10cm x 10cm 10cm x 20cm 15cm x 15cm 20cm x 20cm
Moderate to highly exuding wounds. Suitable for use on fragile skin
Cutimed Siltec Heel 16cm x 24cm Moderate to highly exuding wounds. Suitable for use on fragile skin
MIU ONLY:
Skin Closure Dressings:
Product Manufacturer Size Tips Leukostrip (10x3 per pack) Strips
Smith and Nephew 6.4x76mm
50
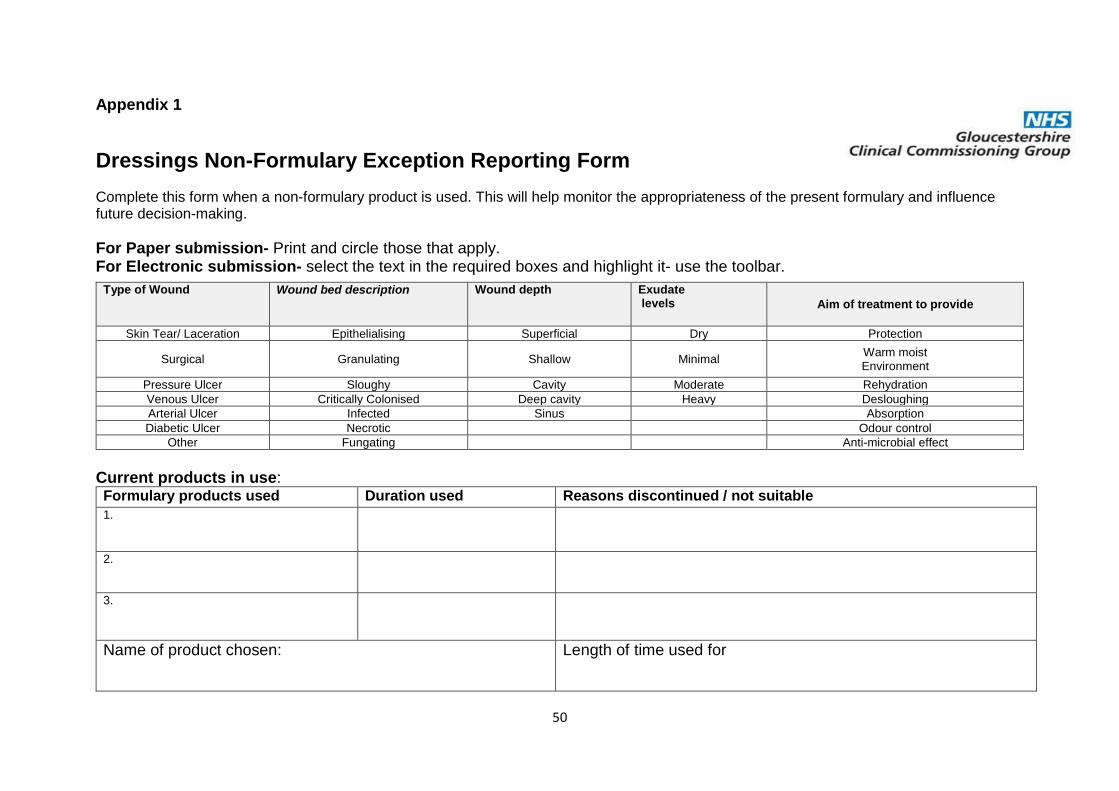
Appendix 1
Dressings Non-Formulary Exception Reporting Form Complete this form when a non-formulary product is used. This will help monitor the appropriateness of the present formulary and influence future decision-making.
For Paper submission- Print and circle those that apply. For Electronic submission- select the text in the required boxes and highlight it- use the toolbar.
Current products in use: Formulary products used Duration used Reasons discontinued / not suitable 1.
2.
3.
Name of product chosen: Length of time used for
Type of Wound Wound bed description Wound depth Exudate levels Aim of treatment to provide
Skin Tear/ Laceration Epithelialising Superficial Dry Protection
Surgical Granulating Shallow Minimal Warm moist Environment
Pressure Ulcer Sloughy Cavity Moderate Rehydration Venous Ulcer Critically Colonised Deep cavity Heavy Desloughing Arterial Ulcer Infected Sinus Absorption Diabetic Ulcer Necrotic Odour control
Other Fungating Anti-microbial effect

51
Rationale for choice
Did the product achieve the aims that were highlighted in the rationale: yes/no
If no, please give reason
Name of person submitting report Date
Contact address Telephone number
Please return completed forms to the Tissue Viability Nurses using [email protected], Gloucestershire Care Services. Edward Jenner Court. Pioneer Avenue. Gloucester Business Park, Brockworth, GL3 4AW.
52
Notes:
