world bank documentdocuments.worldbank.org/curated/en/163371468051882704/pdf/mul… · tamil nadu...
TRANSCRIPT

Document of
The World Bank
FOR OFFICIAL USE ONLY
Report No. 9259
PROJECT COMPLETION REPORT
INDIA
TAMIL NADU INTEGRATED NUTRITION PROJECT(CREDIT 1003-IN)
DECEMBER 28, 1990
Population, Human Resources, Urban & Water Operations DivisionCountry Department IVAsia Regional Office
This document has a restricted distribution and may be used by recipients only in the performance oftheir official duties. Its contents may not otherwise be disclosed without World Bank authorization.
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized

ABBREVIATIONS
CHC - Community Health CenterCNC - Community Nutrition CenterCNI - Community Nutrition InstructressCNS - Community Nutrition SupervisorCNW - Community Nutrition WorkerDEAR - Department of Evaluation and Applied
ResearchFST - Ferrous sulphate tabletsFY - Fiscal yearHSC - Health Sub-CenterICDS - Integrated Child Development SevicesIAS - Indian Administrative ServiceMCH - Maternal and Child HealthNMP - Noon Meals ProgramOED - Operations Evaluation DepartmentPCR - Project Completion ReportPHC - Primary Health CenterPHR - Population, Human ResourcesPPAR - Project Performance Audit ReportSAR - Staff Appraisal ReportSDR - Special Drawing RightsTINP - Tamil Nadu Integrated Nutrition ProjectUSAID - US Agency for International Development
FISCAL YEAR
January 1st to December 31st

FOR OFFICIAL USE ONLYTHE WORLD BANK
Washington. D.C 20433USA.
Office of O,fectocGeneralOpVWatmns EvaluMtrn
December 28, 1990
MEMORANDUM TO THE EXECUTIVE DIRECTORS AND THE PRESIDENT
SUBJECT: Project Completion Report: India - Tamil Nadu IntegratedNutrition Proiect (Credit 1003-IN)
Attached, for information, is a copy of a report entitled"Project Completion Report: India - Tamil Nadu Integrated NutritionProject (Credit 1003-IN)" prepared by the Asia Regional Office. Noaudit of this project has been made by the Operations EvaluationDepartment by this time.
Attachment
This document has a restricted distribution and may be used by recipients only in the perfotmanceof their official duties. Its contents may not otherwise be disclosed without World Bank authorization.

FOR OMCIAL USE ONLY
PROJECT COMPLETION REPORT
INDIA
TAMIL NADU INTEGRATED NUTRITION PROJECT(Credit 1003-IN)
Table of Contents
Paae No.
Preface . . . . . . . . . . . . . . . . . . . . . . . . iEvaluation Summary . . .......... iii
I. PROJECT REVIEW FROM BANK'S PERSPECTIVE
A. Introduction.. . . . .1
B. Prolect DescriRtion . . . . . . . . . . . . . . . . . 1Project Identity . . . . . . . . . . . . . . . . . . . 1Background .. 2Project Objectives and Strategy . . . . . . . . . . . 3Project Components . . . . . . . . . . . . . . . . . . 4
C. Proiect Results .... . . . . . . . . . . . . . . . 5Physical progress .... . . . . .. 5Nutrition .... . . . . . . .. 5... . . . . . . . SHealth ..... . . . . . . .. 6Cost-effectiveness .... . . . . . . 7
D. Proiect Strengths and Weaknesses: Lessons Learned . . 8The Project Design and Implementation Process . . . . 8
The project design process . . . . . . . . . . . 8The implementation process . . . . . . . . . . . 9
The Nutrition Component . . . . . . . . . . . . . . . 10The worker: recruitment, tasks & routines . . . . 10Growth monitoring .. 10Supplementation . . . . . . . . . . . . . . . . . 11Food processing and distribution . . . . . . . . 11Problems experienced in nutrition component . . . 12Possible responses . . . . . . . . . . . . . . . 12
The Health Component . . . . . . . . . . . . . . . . . 14Training and Supervision . . . . . . . . . . . . . . . 17The Communications and Community ParticipationComponent .. 18Monitoring and Evaluation . . . .19Conclusions: Summary of Lessons Learned . .22
This document has a restricted distribution and may be used by recipients only in the performanceof their official duties. Its contents may not otherwise be disclosed without World Bank authorization.
Pate No.
II. PROJECT REVIEW FROM THE BORROWER'SPERSPECTIVE . . . . . . . . . . . . . . . . . . . . . . . 23
III. STATISTICAL INFORMATION. ... 24
1. Related Bank Loans and/or Credits . . . . . . . . . . 24
2. Project Timetable . . . . . . . . . . . . . . . . . . 24
3. Credit Disbursements .. 25
4. Project Results .. 26
5. Project Costs and Financing .. 27
6. Status of Covenants .. 28
7. Use of Bank Resources .. 29
ANNEXES
1. TINP'S Community Nutrition CenterSummary Performance Chart . . . . . . . . . . . . . . . . 31
2. Thresholds Indicating Poor Performance . . . . . . . . . . 32
References ........................ 33

PROJECT COMPLETION REPORT
INDIA
TAMIL NADU INTEGRATED NUTRITION PROJECT(CREDIT 1003-IN)
PREFACE
This is the Project Completion Report (PCR) for the Tamil NaduIntegrated Nutrition Project ia India, for which Loan 1003-IN in the amount ofUS$ 32.0 million was approved on 15 April, 1980. The loan was closed on 31March, 1989, two years behind schedule. It was almost fully disbursed, and thelast disbursement was on October 17, 1989.
The PCR was prepared by the Population and Human Resources, Urban andWater Operations Division of the Asia Regional Office (Preface, EvaluationSummary, Parts I and III). The Borrower was requested by the Bank to preparePart II, but a reply has not been received.
Preparation of this PCR was started after a national level workshop toevaluate the project, which was organized by the Government of Tamil Nadu inAugust, 1989. It is based, inter alia, on the Staff Appraisal Report; the Loan,Guarantee and Project Agreements; supervision reports; correspondence between theBank and the Borrower; and independent evaluation studies of the project (seeReferences).

- iii -
PROJECT COMPLETION REPORT
INDIA
TAMIL NADU INTEGRATED NUTRITION PROJECT(CREDIT 1003-IN)
E.VALUATION SUMMARY
Proiect Obiectives
1. The main project objectives (para 2.07) were: (a) to halve malnutritionamong children under four years of age; (b) to reduce infant mortality by 25%;(c) to reduce vi.--in A deficiency in the under fives from about 27% to about 5%;and (d) to raduce anaemia in pregnant and nursing women from about 55% to about20%.
Implementation Exy,;irience
2. Implementation experience was good. Village nutrition centers staffedby community workers were set up in about 9,000 villages of Tamil Nadu. Workers'skills and motivation were evaluated as very high. About 2,000 new Health Sub-Centers were constructed. Implementatic.. delays were not significant. The twoyear extension of the project was required to expend savings generated by Rupeedevaluation, rather than to complete originally planned project activities (para2.11).
3. Factors responsible for smooth implementation included the state'sstrong political commitment to the nutrition sector; the high quality of themanagers assigned by the state to the project; the attention given by bothBorrower and IDA staff to the design of project software systems duringpreparation; and the use of the first project year for field testing of thesesystems in a small area, before rapid subsequent expansion (paras 3.02-3.06).
Results
4. With regard to the project's nutrition goals, it is estimated that TINPcon'ributed to a reduction of a third or more in severe malnutrition among 6-24month old, and contributed, together with another nutrition programsimultaneously implemented by the state, to a reduction of about half among 6-60month old. These achievements surpass those of most other nutrition programs.On the other hand, the project did not achieve its ambitious goal of reducingmalnutrition as a whole by 50%. Even in the parts of Tamil Nadu benefitinglongest from the project, severe plus moderate malnutrition together fell by 28%(from 53% to 38%) for under six children, and by only 10% for 6-36 monthchildren; results were poorer elsewhere (paras 2.13-2.18). The main problem wasfailure to substantially reduce moderate malnutrition.

- iv -
5. The project's health goals were not satisfactorily met. Infantmortality went down by 12%-26Z in different areas of the project; but it is notclear how far these declines were caused by the project. Reductions in vitaminA deficiency and anaemia were not directly measured, but the targets were clearlynot achieved. Process evaluation indicated that less than a third of under sixchildren and pregnant and lactating women had been covered by the related projectinterventions. The main problem was lack of effective collaboration betweenhealth and nutrition workers in the field (paras 2.19-2.21 and 3.26-3.27).
Sustainability
6. TINP is sustainable both institutionally and financially. By the closeof the project, the state had created from scratch a nutrition infrastructurewith excellent outreach through a skilled and motivated field staff and a groupof managers with the commitment and capacity to objectively assess the strengthsand weaknesses of their own program, and take corrective action. On thefinancial side, Tamil Nadu decided to continue to fund the project from its ownresources after project closing, and at the time of writing has requested asecond IDA credit to expand it state-wide (para 2.06). TINP's financialsustainability is indicated by the fact that its recurrent cost of about US$4.7mrepresented less than five percent of the state's spending on nutrition in1989/90.
Findings and Lessons Learned
7. During implementation, TINP attracted a great deal of interest from theinternational nutrition community. Despite the fact that it did not achieve allof its goals, the project has an unusual number of lessons for the design andimplementation of other programs, some of which are already being applied. Theselessons are partly technical ones related to nutrition and health. But perhapsthe most important ones stem from the design of the project's software, which hasa number of features which could be adapted to improve the coverage and qualityof services in any of the 'people-oriented' sectors.
8. On the nutrition side, TINP showed that part time village workers, ifproperly trained and suppo.ted, can substantially improve their community'snutritional status. Second, the project demonstrated unambiguously that growthmonitoring is an effective and feasible intervention in large scale nutritionprograms. Third, the project showed that targeted supplementation based ongrowth faltering plus feeding of all severely malnourished children cansignificantly reduce severe malnutrition; but that a move to feeding allmoderately malnourished children plus greater attention to maternal nutritionseems necessary to make a substantial impact on moderate malnutrition (paras3.10-3.24).
9. On the health side, the main finding was that large scale investmentin health infrastructure and supplies is not sufficient to improve performance.Complementary measures are needed on the software side which will maximize healthand nutrition workers' incentive to cooperate, and make them more accountable fordoing so (para 3.36). TIN's experience sug;ested six or seven such measures

-v-
(paras 3.28-3.35), for experimentation in the proposed follow-on project.
10. TINP's most significant lessons lie in the design of the project'ssoftware on the nutrition side. Key features for replication include carefullydefined recruitment criteria for local workers (para 3.07); limitation of fieldworker tasks to what is manageable and high priority (para 3.08); specificationof daily and monthly work routines (para 3.09); the innovative decentralizedtraining systet (para 3.37); supervisory ratios which facilitate on the jobtraining (para 3.39); the use of local women's groups to support projectactivities (paras 3.06 and 3.42-4); the display of performance information toclients and workers at the village nutrition center (para 3.46); and a managementinfo-mation system which could rapidly detect performers falling belowestablished norms (para 3.48).
11. Overall, TINP can be viewed as an innovative and successful project,showing that large scale, community level interventions in the social sectors canwork. The lessons from the project are significant ones, and can help tostrengthen other outreach programs in India and elsewhere.

PROJECT COMPLETION REPORT
INDIA
TAMIL NADU INTEGRATED NUTRITION PROJECT(CREDIT 1003-IN)
I. PROJECT REVIEW FROM BANK'S PERSPECTIVE
A. Introduction
1.01 The Tamil Nadu Integrated Nutrition Project (TINP) is of specialinterest to the Bank and to the Indian and international nutrition community forseveral reasons. It is one of the first free-standing nutrition projectssupported by IDA to be evaluated. Second, it is one of the largest nutritioneducation/targeted supplementary feeding programs in the world. Third, althoughthe project did not achieve all of its planned goals, independent evaluationindicates that it has been one of the more successful efforts to date to reducesevere malnutrition. Fourth, the innovative design of TINP's software componentsoffers many lessons for other projects and programs.
1.02 For the above reasons, this Project Completion Report is longer thanthe norm, and focuses particularly on the software and process aspects of theproject. Part B of the report describes the sectoral environment in which theproject was formulated, and the object' 's, content and results of the project.Part C focuses selectively on key design and implementation features which appearto have contributed to the project's achievements, and which may contain lessonsfor the design of other programs. It also focuses on aspects of the projectwhich were less successful than planned, and the lessons from this experience.
B. Project Description
Proiect Identity
Project Name Tamil Nadu Integrated Nutrition ProjectCredit No. 1003-INDate of Credit Effectiveness August 5, 1980Completion Date March 31, 1989Closing Date March 31, 1989Total Project Cost US$81.0 million equivalentOriginal Project Cost US$66.4 million equivalentForeign Exchange Component(Appraisal Estimate) US$7.29 million equivalent
IDA Credit US$32.0 millionIDA Credit, Total Disbursed US$31.977 millionIDA Credit, Total Canceled US$0.023 millionRVP Unit AsiaCountry IndiaSector PHRSubsector Nutrition

-2-
Background
2.01 India's concern about malnutrition dates from independence in 1947,and intensified as a result of the famine in the state of Bihar in 1966/7.Beginning witi the Fourth Plan (1968-73), the Government began to expand existingfeeding programs as a way to help bridge the nutrition gap, while longer-termfood production and income-generating meanures took hold. In 1975, it launchedthe Integrated Child Development Services Scheme on an experimental basis. Thishas now become the main child nutrition program, operating in about 40% of thecountry; however, in the late 19709, when TINP was developed, it covered onlyabout six million people. By that time, public feeding programs of various typeshad expanded to reach an estimated 20 million beneficiaries.
2.02 While concern about malnutrition was reflected to greater or lesserdegree in the policies and programs of all Indian states, Tamil Nadu's commitmentto the nutrition sector has been particularly strong. The state commissionedstudies in the mid and late 1970s, which showed that only one out of 16 majorstates was worse than Tamil Nadu in terms of average daily food intake; that 85%of under six children in the state were less than 90% of the recommended weightfor their age; and that malnutrition was a leading or associated cause of morethan 75% of the dea'hs of 0-3 year old children. By the early 1980s, Tamil Naduhad decided to substantially increase spending on nutrition, and expected thisinvestment to make a significant contribution to the achievement of its SixthPlan goals, which were to reduce economic and social inequalities; to raiseincomes and employment; and to reduce the poverty and improve the quality of lifeof the weaker sections of the population.
2.03 By the late 1970s, about 25 nutrition programs were operating inTamil Nadu, mostly under government auspices. The state was spending about US$8.8m. per annum on the sector, three quarters of which was accounted for by aschool meals program reaching around two million children. However, all of thestates's nutrition programs combined reached less than 10% of pre-schoolchildren, the group that studies had shown to be most affected by malnutrition.And various evaluation studies had shown that the existing nutrition programswere of limited success for the following reasons:
(a) they did not reach intended beneficiaries because they failed to setor adhere to nutritional criteria with respect to target groups;
(b) on-site feeding tended to substitute for food which beneficiarieswould otherwise have consumed at home;
(c) food taken home was shared with other family members, and thusdiluted the impact on the beneficiary;
(d) the supplement given was too coarse and bulky for very youngchildren to eat;
(e) feeding was mainly confined to children who came to centers on a

-3-
drop-in basis, rather than through active efforts to identify thosemost at nutritional risk;
(f) insufficient emphasis was given to nutrition education for mothers;and
(g) food and education alone could not adequately improve nutritionalstatus in the absence of complementary health care interventions.
2.04 A strong commitment to nutrition was thus combined with doubts aboutthe appropriateness of the design of existing nutrition programs. In particular,there was increasing awareness in the State of the need to improve the targetingand lower the unit cost of its interventionn; to promote better nutrition andhealth practices within families; and to strengthen maternal and child health(MCH) services. This situation led to the request for IDA assistance to developa nutrition project focusing on children in the first three years of life, thenutritionally most vulnerable group. This was only the fourth request for afree-standing nutrition project that the World Bank had at that time received.
2.05 IDA's program in India in the late 1970s focussed on the power andagriculture sectors. Of a total of US$7,206m. of IDA resources committed toIndia at the time TINP was appraised, only US$33m. had gone to the socialsectors, for two credits for education and population which went to the Board in1972. The latter credit, which closed in 1980 and was evaluated in a PPAR datedJanuary 1982 (No. 3748), was implemented in selected districts of Uttar Pradeshand Karnataka. It included a small nutrition component, which was evaluated asnot very successful. This was mainly because food was given on a take-homebasis, and it was not clear how much was eaten by the malnourished child asopposed to shared with other family members. Nutrition components have not beenincorporated in subsequent Bank-assisted projects in India.
2.K'5 In 1982, the Tamil Nadu Government initiated a second major nutritioninitiative, the Chief Minister's Noon Meals Program, which supplies a daily rice-based meal to all children from three years and up. This had achieved state-widecoverage by the time the TINP credit closed ir. 1989, while TINP was operating inabout half the state. At this point the state government decided to continue theoperation of TINP using its own funds, and to approach IDA for a second creditwhich would expand TINP services to pre-school children in the rest of the state,and add several new features to the program to strengthen its impact in existingareas. Discussions on the design of the proposed follow-on project were takingplace at the time of writing this report.
Project Obiectives and StrategV
2.07 TINP's overall goal was to imDrove the nutrition and healthconditions of pre-school children, with emphasis on those aged 6-36 months, andof pregnant and nursing women. The main project target was a 50% reduction inthe incidence of protein-energy malnutrition from a level at appraisal of about60% among children under three years of age. Additionally, the project aimed to

- 4 -
contribute to the Government's goal of achieving the following objectives in theproject area: a) a 252 reduction in the infant mortality rate, then about 125per 1,000; b) reduction in the incidence of Vitamin A deficiency in childrenunder five, from about 27% to about 5%; c) reduction in the incidence ofnutritional anaemia in pregnant and nursing women, from about 55% to about 20%.
2.08 The main project strategies were to provide nutrition education andprimary health care to pregnant and lactating women and children 6-36 months; tomonitor the growth of children in this age group through monthly weighing andgrowth charting; and to provide supplementary feeding and health checks to thosechildren whose growth was found to be faltering, as well as intensive counsellingto their mothers. This was to be managed primarily through a new cadre of parttime, paraprofessional Community Nutrition Workers. These were to be assistedby local women's groups created under the project, together with the existinghealth outreach and referral serviceo, which would be strengthened under theproject. Monitoring and evaluation were to have an important role, since theGovernment wished to see whether, through the project, it would be possible toincrease the effectiveness and reduce the unit costs of its nutrition programs.
2.09 The project was planned to take place in the rural areas of sixdistricts of the state (later to become ten districts as a result ofadministrative bifurcation), chosen for having the worst nutritional status.Geographically, these districts covered about half the state, and a ruralpopulation of about nine million people. The project was to be implemented overfive years, with a phased expansion on a block by block basis (the block is anIndian administrative unit covering about 100,000 people).
Proiect ComRonents
2.10 The total project cost at appraisal of US $66.4m. was allocated amongfive components as follows: Nutrition Service Delivery (47%), Health ServiceDelivery (43%), Communications (6%), Monitoring and Evaluation (2%), and ProjectCoordination (2%). Project costs by category were distributed as follows:Salaries and Allowances (24Z), Civil Works (19%), Vehicles, Equipment andFurniture (14%), Food Supplement (13%), Drugs and Supplies (12%), Training (6Z),Vehicle and Other Operating Costs (6%), Contract Services (5%) and ProjectManagement Fund (1%). The following main items and activities were financedunder the different components:
(a) Nutrition. Staff, rent, furniture and equipment for 9,000 newlycreated Community Nutrition Centers (CNCs); supervisory staff,accommodation and transport; running costs of supervisors' officesand CNCs, including therapeutic food for beneficiaries;
(b) Health. Construction, furniture, equipment, salary and runningcosts for 1,600 Health Sub-Centers (HSCs), for ten institutions forclassroom training of Multi-Purpose Health Workers and theirsupervisors, and for field training wings at 39 Primary HealthCenters; bicycles, motorcycles and vehicles for health staff andsupervisors; drugs, vaccines and supplies;

- 5 -
(c) Communications. Costs of designing, producing and disseminatingfilms, filmstrips, radio broadcasts, folk plays and writtenmaterials for nutrition and health education campaigns and fortraining neighborhood leaders.
(d) Monitorinz and Evaluation. Monitoring and evaluation offices ineach project district, and costs of baseline and special studies,data processing and routine monitoring activities.
(e) Project Coordination. Rent, furniture, equipment, staffing andother operating costs of the project coordination office; funds forinnovative activities.
2.11 During project implementation, the Dollar and SDR appreciatedsubstantially against the Rupee, with the result that the IDA credit was able togenerate significantly more Rupee funds than had been expected at appraisal. TheGovernment therefore proposed the following additional investments to utilizethese 'savings': Construction of two food supplement production plants;construction, equipping and staffing of 410 additional Health Sub-Centers;development of a Communications Center in Madras to serve as a state levelresource for the planning, monitoring and evaluation of educational work in thenutrition sector. Later economic analysis led to questions about the viabilityof the food production plants, and these were not constructed; the remainingadditional investments were implemented.
C. Project Results
2.12 Physical progress. The project's closing date was extended fromMarch 1987 to March 1989 in order to fully utilize the additional project fundsgenerated by currency fluctuations. This extension--which was also the cause ofthe project's Rupee cost overrun--did not reflect delays in implementation, sincethe activities originally included in the project were completed more or lessaccording to the original schedule.
2.13 Nutrition. An independent evaluation by the Tamil Nadu Government'sDepartment of Evaluation and Applied Research (Chidambaram, 1989) comparedresults in four areas coming on stream in different phases of the project'sdevelopment against the situation at the start of the project. This evaluation,referred to henceforth in this report as the DEAR evaluation, showed reductionsin severe malnutrition (grades III and IV, i.e. less than 60Z of normal weightfor age) varying from 402 to 552 among children 6-60 months old (Vol II, table4). However, it is not clear how much of this reduction was caused by theproject, how much by secular trends, and how much by benefits from the daily mealsupplied to 25-60 month children by the IMP (para 2.06). Neither of the latterimportant influences was addressed by the DEAR evaluation.
2.14 It is very difficult to disentangle the independent effects of TINPwith the data available. With regard to the effects of TINP as opposed to theNMP, DEAR data indicate (Vol II, table 2) that among 6-36 month children severe

- 6 -
malnutrition fell by between 26Z and 42% in different project areas. While thesedata suggest a strong independent impact of TINP, they cannot be conclusive,because they still contain the 25-36 month age group also fed by the NMP. Anindependent assessment by Shekar (1989) made a direct comparison, and concludedthat reduction in severe malnutrition was greater among 6-24 month than 25-36month children; but this study was limited to one block. With regard to theimpact of TINP as opprsed to developments in general in the state, the DEARcomparison of pilot and control blocks suggests a strong project impact over andabove secular trends. But weaknesses in the evaluation design (para 3.52) makeit impossible to quantify this with any confidence.
2.15 Further uncertainty is introduced by some evidence (Shekar, 1989)that the DEAR evaluation may underestimate the reduction in malnutrition achievedin the project area (para 3.53). Serious account should also therefore be takenof the project's own service statistics, which evaluators agree to be ofunusually high quality. They may be a more relevant measure of project impactsince they focus on nutrition status in villages covered by project services,rather than in larger population taken as the denominator by the DEAR evaluation.The monitoring data indicate a larger reduction of severe malnutrition in the 6-36 month group, of between 36% and 66%. Again, of course, these figures includethe 25-36 month age group fed by the NMP, and as with the DEAR data also reflectan unknown influence from secular trends.
2.16 Overall, it is probably fair to conclude that TINP, independently ofthe NMP but not independently of secular trends, achieved a reduction of a thirdto a half in severe malnutrition among 6-24 month children; and that the projectcontributed, together with the NMP and secular trends, to a reduction of abouthalf among 6-60 month children.
2.17 There was less success in reducing moderate malnutrition (defined asbetween 70% and 60% of normal weight for age). In the second and last phases ofthe project, the DEAR evaluation indicates that second degree malnutrition washigher at project end than at the beginning. But this is inevitable, since atemporary rise in second degree malnutrition naturally follows improvement inthird and fourth grade children. More significantly, however, by the end of theproject grade two malnutrition in children under five had only come down by 14%in the first block to be developed, and still affected about 30% of children(DEAR, Vol. II, table 1).
2.18 TINP's overall nutrition objective was to reduce malnutrition in 6-36month children by 50% during the project period; the appraisal report did notspecify which grades, but it may be assumed that this meant moderate and severemalnutrition. According to the DEAR evaluation (Vol. II, tables 1 and 2), in theinitial block to be developed moderate and severe malnutrition together fell only10% in the 6-36 month age group, and by 28% in the 6-60 month group. Thereduction was much less in later phases of the project, where the grade twopopulation had--presumably temporarily--increased.
2.19 Health. As against the target of 25%, the DEAR evaluation indicatedthat infant mortality had declined by 26 to 29% in the blocks first developed,

and by 12 to 13% in the later phases of the projectl a rate for the project areaas a whole was not calculated. The project therefore can be said to havecontributed to meeting the state's mortality reduction target (this was how theproject target was expressed), but it is not clear how far the project wasactually responsible for achieving the above declines, since declines of the sameaverage magnitude occurred in the non-project districts of the state; on theother hand, the TINP project districts were chosen because they were relativelydisadvantaged, so that average mortality reduction figures may reflect more thanaverage achievement.
2.20 Success in achieving the project's two other formal healthobjectives--reduction from 27% to 5% in Vitamin A deficiency in under fivechildren, and reduction in anaemia from 55Z to 20% of pregnant and nursing women--was not evaluated directly. Nevertheless, inferences can be drawn from coveragelevels achieved in related interventions, which, according to the DEARevaluation, had risen very significantly, but were nevertheless well short ofwhat would have been needed to achieve the proje,zt targets. 55% of childrenreceived half or more of the due doses. 28% of children had not received asingle dose. While at least half of all eligible pregnant women had receivedFerrous Sulphate Tables (FST) against anaemia, only 18.5% had received the rightquantity of FST. There is no data to indicate what percentage of women gettingFST actually took the tables.
2.21 Unsatisfactory performance with these two interventions can partiallybe explained by periodic national shortages of Vitamin A, and quality problemswith the FST, leading to their withdrawal at one point by health componentmanagers. But similar performance was found at evaluation with other healthinterventions emphasized under the project (although not given formal targets).For example, 56% of antenatal cases were being registered by the end of theproject; 45Z of eligible women received full anti-tetanus immunization; only 37%of children received regular health check-ups; and only 60% of children hadreceived three DPT immunizations. These coverage rates are good by averageIndian standards, and considerable better than in the non-project areas. Butthey were well below the rather ambitious, informal project targets of 80-90% foreach of these services.
2.22 Cost-effectiveness. DEAR's evaluation deals with project impact, butnot explicitly with the issue of cost-effectiveness, although this was a primaryconcern of the state government (para 2.04) at appraisal. One study (Dapice,1988), commissioned during project implementation, attempted to compare the cost-effectiveness of TINP with the major national child development program, theIntegrated Child Development Services (ICDS). The study concludedthat TINP hadachieved roughly twice the reduction in severe malnutrition of ICDS for a smallercost (about US$9.1 per direct beneficiary). However, this study needs to betreated with some caution, for three reasons. First, it compared only one TINPand one ICDS block. Second, it looked at effectiveness only in terms of reducingsevere malnutrition, when the goals of both programs were to reduce malnutritionin general. Third, it is not clear that a comp&rison with ICDS is a fair one,because TINP was a nutrition/health program only, while ICDS is a childdevelopment program with broader goals, including pre-school education.

- 8 -
2.23 TINP nevertheless demonstrated that highly targeted feeding programs,complementing effective nutrition education, can have a substantial impact onsevere malnutrition for far less money than universal feedings in an establishedTINP block, monitoring data show that no more than 251 of 6-36 month childrenwere in feeding at any one time, with a corresponding saving in food supplementcosts. The project does not, however, demonstrate that the TINP targeting modelis a cost-effective formula for dealing with moderate as well as severemalnutrition, in view of the project's limited effects on the former.Experiments are currently going on in Tamil Nadu to determine the effects onmoderate malnutrition of broadening the target group for supplementation (seealso paras 3.22-3.24). The results should have important implications for thedesign of nutrition programs in the proposed follow-on project and in othercountries.
D. Proiect Strengths and Weaknesses: Lessons Learned
3.01 The third part of this report begins by reviewing the general designand implementation approaches that were important to TINP's achievements, andthen analyses lessons learned component by component. Because of its importance,the training and supervision system is discussed as a separate component, eventhough it was not treated as such in the original project appraisal report.
The Proiect Design and Implementation Process
3.02 The groiect design process. Project design was facilitated by anunusually strong nutrition information base, in the form of the USAID-financedTamil Nadu Nutrition Study, completed in 1973 by a multi-disciplinary team ofnutritionists, economists, biologists, food technologists, behavioral scientists,engineers and systems specialists. The study was apparently at the time the mostsystematic effort undertaken in a developing country to analyze the nutritionaspects of food production, distribution and consumption, with a particular focuson identifying interventions to improve child survival. The project also drewfrom experience with IDA-financed nutrition project then under implementationin Indonesia. Features incorporated from this project into TINP included thefocus on the 0-3 age group, the use of part time community nutrition workers asthe main change agents, and the calorie-dense food supplement. Finally, thedesign # oroject software was also influenced by the Bank-developed Training andVisit tem of agricultural extension, most notably with regard to highlydefined work routines for field staff; frequent, decentralized in-servicetraining; and reasonable spans of control for supervisory staff.
3.03 The final project design was the result of sixteen months ofintensive dialogue between the Government and IDA teams, which resulted insubstantial ref ineme- and simplification of the original project proposal. Thishad originally interaed the project to cover four states, which was felt by IDAto be too ambitious for % first operation in the sector. It had alsoincorporated village water supply and food production, processing and storageinterventions, which vere later excluded from the project because it was feltthat these would complicate project management and could better be tackledthrough sector-specific programs. Another result of the dialogue during

- 9 -
preparation was the innovative food supplementation system, which focused onfeeding very young children for relatively brief periods for growth recoverypurposes, in contrast to existing programs which tended to provide prolongedfeeding for older children.
3.04 The implementation process. Implementation was guided on a day today basis by a newly created project coordination unit, headed by an IndianAdministrative Service (IAS) officer who was also designated Additional DirectorSocial Welfare. The IAS status and the rank of this officer in the Directoratewere important factors in facilitating implementation; at the same time, thecreation of a separate unit for managing the project meant that attention to itwas not diffused in the press of managing existing departmental programs. TheProject Coordinator reported to an Empowered Committee chaired by the State'sChief Secretary and consisting of the relevant Development Secretaries, which metperiodically to review proL:ess and take major decisions. The high level andinter-departmental nature of this committee were important factors in achievingcoordination and getting things done.
3.05 Project expansion was carefully planned. The project was confinedto one administrative block in its first year, during which the implementationstrategy was tested and refined. IDA's role was particularly important duringthis period, as it was during preparation, with three or four visits byinterdisciplinary teams in a year, as against the six monthly reviews that becamethe routine in subsequent years. Project expansion after the first year wasrapid. An important contribution to flexibility and innovation in projectmanagement both in the pilot block and the expansion phase was made by theProject Management Fund, from which small amounts could be committed for studiesand operations research at the discretion of the project coordinator withoutbureaucratic clearance. This fund financed no less than 63 small studies whichhelped identify problems during implementation, and also financed an innovativeprogram for food supplement production by village women's groups (see para.3.14).
3.06 Project expansion was also carefully planned at the micro level, withspecial attention to preparing the local community whenever the project movedinto a new village. After recruitment and training of the Community NutritionWorker (CNW), but prior to the offering of any project services, a women's groupwas formed consisting of about 20 people with a particular interest in health andnutrition. This group was briefed on the aims of the project, and played animportant part in explaining them in turn to the community. Two key elements ofthe program's philosophy were communicated at this stage, before services wereeven delivered. First, that the feeding program was to be purely rehabilitativein nature, with only needy children getting supplemented; the primaryresponsibility for child care and nutrition was to remain with the family.Second, that the project was the community's, and project staff accountable tolocal people. The CNW's supervisor made it clear at the initial briefing of thewomen's group that the community should approach her and complain if any of thepromised services were not in fact delivered.

- 10 -
The Nutrition Component
3.07 The worker: recruitment. tasks and routines. The criteria forrecruitment of the CNWs were important to the project's success. They had to bewomcn from the village (one was chosen for every 1,500 people), with an interestin health and nutrition; and where possible they were women who were poorer thanaverage, but who had well nourished childt en. In addition to having good accessto mothers and high motivation, such women tended to be credible sources ofadvice because they could demonstrate from their own experience that poorfamilies could provide better nutrition for their children even with existingresources. These qualities were given higher weight in selecting workers thantheir educational levels.
3.08 The project design consciously limited CNWs' tasks to a small numberwhich were manageable and likely to have a high impact on nutrition. These weregrowth monitoring; nutrition education; supplementary feeding; education in oralrehydration for diarrhea cases; twice yearly Vitamin A supplementation; andquarterly deworming. The growth monitoring, supplementation and dewormingprograms were limited to the under four age group both because these were thenutritionally most vulnerable, and because this group was small enough forworkers to pay them and their mothers individual attention.
3.09 Workers' daily and monthly routines were clearly defined. In themornings, they ran the supplementary feeding program. In the afternoons, theycarried out home visits to families with problem children. Three predetermineddays a month were set aside for child weighing, which on the first two days tookplace at specified locations in the village which were convenient to mothers.The third day was set aside for following up on mothers who had failed to bringtheir children for weighing. This outreach approach resulted in a highproportion of children being weighed every month--normally 85-90% of children inmain villages, although substantial numbers of children in outlying hamlets werenot reached (see para. 3.15).
3.10 Growth monitoring. A good deal of controversy persists about whethergrowth monitoring is a necessary and feasible intervention for large scalenutrition programs. TINP managers are convinced that regular growth monitoringwas the core intervention in the program, for three reasons. First, the growthchart could detect faltering growth and incipient malnutrition long before it wasvisible to either mother or worker, allowing action to be taken before theproblem became serious and hence more difficult to treat. Second, weighing andgrowth charting with the participation of mothers provided the central focus fornutrition education. Third, the child's charted growth path provided the basisfor deciding whether supplementary feeding was necessary. On the question offeasibility, studies during project implementation consistently reported a highdegree of accuracy in both taking weights and recording them. TINP hasdemonstrated unambiguously that growth monitoring is a feasible intervention forparaprofessional workers in large scale nutrition programs, providing thattraining and supervision are carefully planned (see paras 3.37 to 3.39).

- 11 -
3.11 Supplementation. After much debate during project preparation, acombination of nutrition grade and weight gain was used as the criterion forentry into the supplementary feeding program. All children with severe (grade3 or 4) malnutrition were fed, as also all children who failed to gain weight intwo successive monthly weighing, even if such children were in the normalcategory by grade. Children in the first category were graduated from feedingwhen they reached grade two and were on a normal growth path, children in thesecond category after three months, providing they were gaining weight normally.Attendance in the feeding program was evaluated as high, averaging about 95% ofthose eligible.
3.12 The weight gain method had three general advantages. First, theconcept was educational in itself, demonstrating to mothers the importance offeeding more to maintair. growth momentum. Second, feeding growth falteringchildren early, even when they were in grade normal, could prevent thedevelopment of moderate and severe malnutrition. The fact that no less than 85%of children in the average TINP village suffered a growth setback and entered thefeeding proeram at some time suggests that this preventive role may have beenquite significant. Third, it was thought that this selection method would becheaper, in terms of numbers in the feeding program, than supplementing allmoderately malnourished children. With no more than 25% of children in thefeeding program in the final year of the project, this was clearly the case.However, as noted above (para. 2.17), the project failed to achieve a substantialimpact on moderate malnutrition, and it appears that this was in part because itwas supplementing too few children.
3.13 The TINP food supplement was a ready-to-eat mix of wheat, gram,groundnut cake, sugar, maize and vitamin and mineral mix, delivering 380 caloriesa ration. It was served in the form of 'laddus', or small ball-shaped snacks.This type of supplement had three advantages. The use of locally consumed foodsensured that it was acceptable. Because the food was ready to eat, cooking costsand workers' time were saved. And, most importantly, because the food was servedin the form of a snack, mothers tended to think of it as a supplement to the dietrather than as a meal which might substitute for existing consumption. Thisperception was reinforced by the timing of feeding at the Community NutritionCenter, which was in the first half of the morning, i.e. between meals.
3.14 Food processinR and distribution. Three quarters of the project'sfood requirement was supplied by a government-owned factory in Karnataka, anothersouthern Indian state. The remainder was produced by 322 of the women's groupsset up under the project (para. 3.06). Breaks in food supply from either sourcewere not experienced during the project. The cost per kilo of food produced byvillage groups was similar to that of factory produced food (about Rs.7, orUS$0.5). Village level production had the advantage of contributing also toincome and empluyment opportunities for local women, as well as a significanteducational spin-off; women in villages where the supplement was produced learnedthe recipe and began to make it for normal home consumption. On the other hand,problems were becoming apparent by the end of the project with quality control,and with accountability of project funds, and it is unlikely that this form ofproduction will be expanded.

- 12 -
3.15 Problems experienced in nutrition component. Four main weaknessesin the nutrition component have been identified by various evaluators. First,it appears that up to 30% of eligible children in the project districts did notreceive project services, especially regular weighing. This is a seriousproblem, because the excluded group will inevitably include cases of severemalnutrition which have not been detected. A recently conducted study on thecharacteristics of excluded beneficiaries concludes that the majority ofexclusion is for geographical reasons--they live outside the current catchmentarea of the project--rather than self-exclusion by dropping out of the program.This probably explains why project monitoring data show 85-90% weighing rates(for villages covered by the project), while the DEAR evaluation (which sampledthe entire rural population in the project districts) reports closer to 70%.
3.16 Second, just over four per cent of children failed to respond toproject inputs, and remain in feeding. While this group of 'hard coremalnourished' is small, it is very important, because it consists mainly ofchildren who are severely malnourished and hence at high risk of dying. At thetime of writing, a study was also being conducted to determine thecharacteristics of non-responders. The evidence available to date suggests thatthese are children with medical problems which have not been resolved and/orchildren from very poor families whose food resources are inadequate for thefamily even with the supplement provided by the project.
3.17 Third, as already discussed, the project did not achieve a rapidreduction in moderate malnutrition. Fourth, an unacceptably large number ofchildren who graduated from feeding relapsed into supplemeL.tation within sixmonths. A project financed study on relapse rates (Rajivan, undated) found that42Z of the children that graduated relapsed once; 6% relapsed twice; less than1% a third time. Thus, while the project succeeded in helping these children,they might have recovered sooner to a normal growth path had they received alonger, unbroken period of supplementary feeding.
3.18 Possible responses. At the time of writing, six possible responsesto the above problems had been proposed for implementation in the next project.First, it was accepted that TINP's interventions were focused on the 6-36 monthold child, and paid too little attention to children's nutrition in the womb andin the first six months of life. Due to poor maternal nutrition, about 302 ofbabies are born under weight, and hence at higher risk of mortality, morbidityand persistent malnutrition. A better focus on maternal nutrition and on childcare during the first six months would produce bigger, stronger infants lessprone to malnutrition in general, and in particular to the problems of non-response, relapse and failure to move out of grade two.
3.19 Under the TINP project design, the female Health Worker was givenresponsibility for growth monitoring and general care of the 0-6 month child, andfor deciding which pregnant women should receive supplementation. Although thispart of the program has not been specifically evaluated since 1982, it appearsthat this did not work well, largely because of the numbers and distancesinvolved for a worker covering a population of 5,000. It is now proposed to makethe CNW responsible for both these groups, and also for birth weight recording,

- 13 -
which was very incomplete under the project. Particular emphasis would be givento increasing the percentage of antenatal cases registered; to giving a broaderrange of antenatal care services; and to bringing all malnourished pregnant andlactating women into supplementation.
3.20 Second, changes in the ration size and the type of food supplementare being discussed, so that supplementation has a greater effect on nutrition.This should have consequences for all of the weight gain problems mentionedabove, but particularly for -hildren who are non-responders because theirfamilies are too poor to feed them adequately at home. Bigger rations may bedifficult for children to finish, so consideration is also being given toreducing the bulk or viscosity of the normal ration, and in addition to enrichingthe supplement being given to seriously malnourished children.
3.21 Third, it is proposed to improve the frequency and quality of medicalattention that malnourished children receive. This should be of particularbenefit to non-responders with health problems which make it difficult for themto absorb adequate nutrients. This issue is discussed in the following sectionon health. Fourth, children failing to thrive may be admitted into the feedingprogram on the basis of a check weighing a fortnight rather than a month afterinadequate weight gain is first detected, thus preventing some further declinein nutritional status. (Children are not admitted into feeding immediately whengrowth faltering is detected, because brief growth interruptions due toinfections are common and usually self-correcting; responding to such cases withthree months of supplementation is unnecessary, and wasteful of resources).
3.22 Fifth, and most significantly in financial terms, it is proposed tosupplement all children with moderate malnutrition instead of only those withfaltering growth as at present. This is a recognition that the existingselection criteria did not make a big enough and fast enough impact on this typeof malnutrition. The growth faltering entry criterion would however be retainedfor grade one and normal children, because of its apparently important role inpreventing moderate and severe malnutrition. Such a decision would initiallydouble the number of children in feeding, but it is hoped that the numbers ofmoderately malnourished children would subsequently come down to half the presentlevels. If that were the case, the food costs of the program in its maintenancephase would not substantially increase from the present, even taking into accountthe increased unit cost of the ration, and increased numbers of pregnant womenin feeding.
3.23 The impact of this move to grade two feeding is hard to predict. Itcould be less than hoped to the degree that moderately malnourished children arestunted as well as low weight for age, since such cases are harder torehabilitate (a study of the incidence of stunting is now being conducted). Buteven if stunting is now common, the measures proposed to increase birth weightsand sustain normal growth in the first year of life should help to prevent it inthe future. Moreover, initial results of a small scale experiment with universalfeeding of grade twos in two blocks of the TINP area show a fairly rapid decreasein the incidence of moderate malnutrition, even without the introduction ofcomplementary measures to improve maternal and 0-6 month infant nutrition. This

- 14 -
experiment is now being expanded to additional blocks to confirm its findings.
3.24 In addition to reducing moderate malnutrition, the move tosupplementing all grade two children should significantly reduce the relapserate. Many of those currently relapsing are children graduating from grade threeinto grade two, who would now stay in feeding for a much longer period; a TINP-financed study of relapse cases indicated that while 45Z of those fed for 90 daysrelapse, less than 30% of those fed for 180 days do. Related to the question ofthe relapse rate is whether the proposed follow-on project should graduatechildren immediately they reach grade one or give them an additional period of'protective' feeding to reduce the chances of subsequent relapse.
3.25 Finally, three kinds of responses are planned to the problem ofexclusion. First, in the existing project areas it is planned to develop anadditional 20% of CNCs to cover villages left out of the original project becauseof insufficient funds at the time of appraisal. Second, a mapping exercise willbe undertaken to see whether a different distribution of hamlets between CNCvillages will improve access. Third, experiments will be c'rried out withdifferent approaches to service delivery in the hamlets--for eximple, employingan additional helper to deliver the food supplement to the hamlet, or creatinga special Women's Working Group in the hamlet to help in education and serviceprovision.
The Health Component
3.26 TINP' s nutrition component has received more attention from observersand evaluators than its health component, despite the fact that the latterabsorbed almost 50% of project costs, spent primarily on establishment of newhealth sub-centers, and on additional drug supplies. As noted in paras 2.19-2.21, these investments did not have a satisfactorily return in terms ofachieving targets levels of service coverage. The problem was that despite moreclinics and more supplies being available, cooperation between health workers andCNWs in the field never really developed, and hence full advantage was not takenof the potential for increased health service outreach offered by the newlycreated network of CNCs.
3.27 Yet the software side of the health system was not neglected duringproject preparation. Work routines were designed for health workers to regularlyvisit the CNCs in their areas to provide support to CNWs. However, these visitsdid not in general take place as planned; one indicator of this was the DEARevaluation's finding that only 28% of pregnant women knew the name of theirhealth worker, as against 69% for CNWs. The failure of health workers and CNWsto work as a team in large measure explains low rates of ante-natal registrationand lower than anticipated coverage of interventions such as FST, vitamin A andimmunization. A weak health/nutrition coordination was partly the consequenceof poor relationships between staff in the state's departments of health andsocial welfare in the early years of the project. But it is also a more generalproblem, not unique to TINP or to Tamil Nadu and remaining equally unresolved inthe case of the ICDS program. The remainder of this section reviews seven lessonssuggested by the TINP experience for improving coordination.

- 15 -
3.28 First, the state government proposed a structural reform of itsdepartments of public health and social welfare to improve cooperation betweenhealth and nutrition staff. Under the new structure being discussed at the timeof writing, all female staff in the field (CNWe and health workers, and theirrespective supervisors) would be responsible to one officer at the districtlevel, reporting via the Community Health Nurse, who would act as project officerat the block level. While separate departments of Public Health, Family Welfareand Social Welfare would be retained at the state level, instructions to fieldstaff would be issued under the joint names of the three directors.
3.29 Second, it was recognized that the number of pregnant and lactatingwomen per health worker (about 125 in her population of 5,000) made it difficultfor her to provide adequate service to all. It was therefore suggested thattasks might be reallocated to give the CNW a greater role in the following areas:
* registration of antenatal cases* iron supplementation* maternal growth monitoring and supplementation* birth spacing motivation* identification of likely cases for birth spacing? taking birth weights and referral of LBWA* growth monitoring 0-6 month child and weaning education* vitamin A supplementation* identification of children for immunization• follow-up of immunized children* treatment of moderate and referral of severe ARI cases
3.30 The experience of the first project suggested that those tasks wouldbe within the competence of the CNW, and manageable given that each CNW would bedealing with only about 30 pregnant and lactating women. It was hoped that theincreased asistance provided to the health worker--especially in her priorityareas of immunization and family planning--might encourage in return greatercooperation from the health worker in providing the more complicated services forwhich CNWs are not trained, for example:
* antenatal check-ups, identification of high risk pregnancies* prescription of temporary contraceptive methods* check-up of LBW babies, education for mothers* immunization* referrals of malnourished children with health problems* referrals of severe ARI cases
3.31 Third, it was recognized that work routines needed to be redesignedso as to provide a minimum, set (and hence monitorable) number of days * monthon which the health worker would visit the CNC to work jointly with the CWM. Inaddition to the existing monthly immunization day, possibilities included settingup a monthly 'mothers' day', on which ante- and post-natal cases could meet withthe health worker; or for the health worker to take advantage of thQ existingmonthly weighing days to do antenatal care and family planning work, andproviding health check-ups to children identified as malnourished. Healthworkers' regularity in making the minimum scheduled visits could be monitored byboth health and nutrition supervisors, and reviewed at monthly staff meetings.

- 16 _
3.32 Fourth, it might be desirable to decentralize the MCH record-keepingsystem from the health center to the CNC, and to treat the CNC as a sort ofsatellite health center, since this is where the majority of MCH services vouldactually be provided. This might both improve the accuracy of record-keeping,and give the health worker an added incentive to visit the CNC.
3.33 Fifth, it was felt that a spirit of collaboration between health andnutrition could be better built up by ioint training of the workers, than simplyby the issuance of new guidelines or instructions. This is discussed in moredetail below (paras 3.37 to 3.39). Fifth, just as joint work routines would bedeveloped for front line workers, it was felt that performance would be improvedif loint sunervision routines were developed for their immediate supervisors.A minimum number of days a month, say eight, would be set aside for health andnutrition supervisors to spend together with front line workers on days when thefront line workers from the two departments were themselves working together.
3.34 Sixth, new incentives and Drocedures for referrals needed to bedeveloped. Problems encountered in this area during the project included thefailure of mothers to take their referred children to the Primary Health Center(PHC--the referral facility for each 30,000 population), and the absence of asystem for communicating doctors' diagnoses to health workers and CNWs so thatthey could take appropriate follow-up action. Ideas put forward forexperimentation during the second project included offering mothers a transportallowance as an incentive to complete their and their children's referrals, anddevelopment of a new referral slip with a detachable portion for the doctor'sdiagnosis and treatment recommendations, which would be given to the mother toshow to the health worker and CNW.
3.35 Seventh, it was proposed to experiment in the second project withstrengthening the capacitv of PHCs and Community Health Centers (CHCs) to dealwith referral cases. At the PHC level it was proposed to supply additionalequipment and laboratory facilities, plus training in diagnosis and treatment fordoctors dealing with routine referrals. But it was recognized that the CHC (thereferral facility for every 100,000 population) was the lowest level in thehealth system equipped to deal with cases of obstetrical risk and rehabilitationof non-responding malnutrition cases, and that these were not set up for therelatively long stays these cases typically require. It was therefore proposedto experiment with the creation of 'MCH annexes', simple 10 or 12 bedded non-hospital facilities where women could stay with a family member while waiting fordelivery, or while rehabilitating a severely malnourished child under thesupervision of a specialist.
3.36 In summary, therefore, the lesson from TINP was that large scaleinvestment in health infrastructure and supplies was not sufficient to improveperformance in the field, and maybe not necessary. The strategy suggested forthe follow-on project was to reduce investment in civil works in the healthsector, and to limit additional drug supplies to those needed to dealspecifically with the referral needs of the project's key target groups. At thes:-me time, the aim would be to develop a package of mutually reinforcing measureson the software side, which would both maximize health and nutrition workers'

- 17 -
incentive to cooperate, and make them more accountable for doing so.
Training and Supervision
3.37 TINP's training system for nutrition workers was innovative, cheap
and highly effective. Both pre- and in-service training of CNWe were carried outat the block level, by a Community Nutrition Instructress (CNI), who was a fulltime trainer/supervisor for that block. This system had a number of advantagesover training carried out in regional training centers, the pattern for most
field worker training in India:
(a) the trainee was not disoriented by being taken out of her ownenvironment;
(b) because training took place in a borrowed room at the blockheadquarters, with the trainees sitting on the floor, the learningsituation paralleled the situation in which workers would later betraining mothers;
(c) trainees could be trained with other workers from the local area,giving them the chance to share and solve local problems;
(d) the trainer had the chance to build up a long term relationship withthe workers, and hence could tailor training to local needs andindividual problems;
(e) evaluation of effectiveness of training was automatic and immediate,since the trainer later helped supervise the workers;
(f) training was cheap because there was no overhead of traininginstitutions, and minimal costs for transporting trainees to theplace of training; and
(g) because training was local and cheap, in-service training could bearranged quickly and as often as the needs of workers required.Instead of each worker getting a standard amount of training, groupsof poorer performers could be singled out for special support.
3.38 This system contrasted with that for health worker training under
TINP, which relied on regional training institutions for in-service training.Such training was infrequent. Joint training of CNWs and health workers was
carried out under TINP for the last ten days of the CNW's are-service training.It is proposed under the follow-on project to expand the concept of block level
training to include joint in-service training for nutrition and health workersfor one week each six months. In addition to imparting technical skills, this
would be an important intervention to encourage teamwork (para 3.33).
3.39 TINP's field supervision structure was one Community NutritionSupervisor (CNS) for every ten CNWs. This ratio was chosen to allow the
supervisor to spend a full day a fortnight with each worker, in line with the

- 18 -
project's philosophy that supervision presented an opportunity for on the jobtraining rather than simply inspection. Just as the Community NutritionInstructress was also a supervisor, so the Community Nutrition Supervisor wasalso a trainer. The high level of support to the workers arising from thisoverlapping of the training and supervision function contrasts strongly with thesituation in India's ICDS and Family Welfare programs, and was a primary reasonfor the high level of competence and motivation of CNWs.
The Communications and Community Participation ComDonent
3.40 TINP's communications component was managed by a small staffreporting to a Joint Director in the Project Coordination Office. The same staffhandled the preparation of materials for training under the project. Outsidethis unit, no department or institution existed in the state government tooversee communications in the nutrition sector. For this reason, it was agreedthat a priority use for savings under TINP (see para 2.11) was to develop aCommunications Center, which would plan, monitor and evaluate information,education and communication activities in the nutrition sector. As discussionsbegan on the formulation of the follow-on project, it was also agraed that asTINP became a statewide program and staff training loads increased, there was aneed for a similar apex function for the planning, monitoring and evaluation oftraining in the sector. It was therefore decided to broaden the function ofthis institution to become .? Communications and Training Center.
3.41 A very wide range of mass media materials was produced under thecommunications components, including films, posters, wall paintings, hoarding,pamphlets, folders, village theater scripts and folk tale stories. DEAR'sproject evaluation and an iadependent consultant st ly of the communicationscompoaent (Ferguson, 1989' evaluated the reach of these various media andconcluded that posters and wail paintings had the greatest reach, while films hadthe least because they were not so widely distributed. The evaluations alsoconcluded that more use could be made of TV as a medium, in view of its rapidlyincreasing reach in the stat67; rural areas. Neither study, however, attemptedto evaluate the effectivenesi. of the various media and messages developed interms of changing the knowledge, attitude or practice of project clients; thiswork remains to be done before a detailed communications strategy for the follow-on project can be produced.
3.42 The project placed great emphasis on interpersonal communication,both through the CNWs and through the Women's Working Groups created in everyproject village (see para 3.06). That the interpersonal communications effortwas in genera' successful is indicated by the DEAR evaluation's finding from itsclient survey that there was a near universal understanding of the project'sobjectives aznd the services it was supposed to provide, a high participation ratein feeding (in most cases across caste barriers) for those eligible, and awidespread understanding and acceptance of the concept of selective supplementaryfeeding.
3.43 The WWGs had an important role in encouraging initial acceptance ofthe project (para 3.06), and were extremaly active in participating in health and

- 19 -
nutrition education sessions, in carrying out cooking demonstrations and inassisting at monthly weighing sessions. The large numbers, the active nature andthe sustained interest of these groups in the project all contrast strongly withefforts to develop community involvement in other government-run health andnutrition outreach programs in India. Part of the explanation for this successmay be attributed to differences between the status and education of women inTamil Nadu as compared to some northern states. But it seems clear that the highdegree of motivation of CNWs and the quality of their training in communicationwere also key factors.
3.44 On the other hand, it appears that the outreach of the communicationeffort was greater from the CNWs themselves than from the WWGs. Both evaluationsof the communications component concluded that the WWGs had a relatively smallimpact in terms of passing on educational messages to mothers outside the group.The same was true of the Children's Working Groups formed by many WWGs in theproject area. While the children in these groups quickly absorbed the key healthand nutrition messages they were taught, and many became adept participants indance, song and theater emphasizing these themes, there was little spin-off ofknowledge to children outside the group. Greater emphasis would therefore needto be laid in the second project on training workers to train Working Groupmembers to be better educators of those outside their groups.
Monitoring and Evaluation
3.45 Monitoring. TINP's nutrition monitoring system was based on thechild cards, including growth charts, updated monthly by the CNWs. One of TINP'sachievements, noted both by the DEAR evaluation and a second independentevaluation of the monitoring system (Rajagopalan and Vaidyanathan, 1989), was thecompleteness of these records, and the accuracy of the information in them. Thisis a further reflection of the effectiveness of the decentralized trainingsystem, and the regularity of field supervision; one of the jobs of the CNS wasto carry out regular spot checks of the accuracy of a sample of children'srecords at her CNCs. By the end of the project, Tamil Nadu's CNCs contained whatwas probably the largest collection of high quality longitudinal child growthdata in the world. The State intends to collect a large sample of these data andmake them available to Indian and international researchers.
3.46 Two aspects of record-keeping at the CNC level may be particularlyuseful for replication elsewhere, as a means of focussing worker attention onpriority clients and on performance. First, child cards/growth charts werestored not in registers but on shelves, with a pigeonhole for each grade ofmalnutrition. Thus, for example, it was possible to pull out immediately allrecords for severely malnourished children, and to keep track of grade shiftssimply by transfers of records from pigeonhole to pigeonhole. Second, monthlyperformance at each CNC was publicly displayed on a standard chart on the CNCwall (see annex one). At a glance, each worker, supervisor and Women's WorkingGroup member could see how the key nutrition indicators for the village weremoving, and how well the CNW was doing in getting services to the scheduledcastes as opposed to the general population.

- 20 -
3.47 The common weakness of the nutrition and health record-keepingsystems at the field level was that workers had to fill in too many reports andregisters. At the time of writing, a state level committee was considering howthe system could be simplified for the follow-on project. In addition, thehealth monitoring system suffered from shortages of registers, so that healthworkers spent unnecessary time making their own; and from a combination of highstaff turnover and infrequent in-service training, which meant that healthrecords were not always of consistent quality. The proposed expansion of blocklevel in-service training to the health workers should help to remedy the latterproblem.
3.48 Performance information was transmitted monthly via the CommunityNutrition Instructress and a monitoring cell at the district level to themonitoring and evaluation unit in the project coordination office, headed by anAssistant Director. The processing of information was rapid; block-wiseperformance statistics were available to the project coordinator with a lag ofonly one month. Each block's performance was compared to norms (see annex two),and low-performing blocks were singled out for corrective measures. However,according to the evaluation of the monitoring component, feedback to the fieldconsisted more of routine indications of failures to meet norms, than ofsystematic efforts to find and deal with underlying causes of poor performance,or to revise the norm if it was not applicable to a particular block. This isan area that would require attention in the follow-on project.
3.49 Evaluation. The project evaluation process was carefully designed.A baseline survey was carried out in each project district before implementationbegan. A first round evaluation of the initial project block was done in 1982;a midterm evaluation covering the first project district was undertaken in 1984;and the terminal evaluation was completed in early 1987. It is interesting tonote that midterm evaluations, now a routine part of the project cycle, were arelatively new feature at the time TINP was designed. both for reasons ofcaution in committing resources to a new sector, and in order to allow rapidfeedback, IDA's Board of Directors had required midterm evaluations in the caseof all of the early nutrition projects, and after these midterm evaluations heldBoard discussions of the first three projects.
3.50 In addition to these periodic evaluations, DEAR also carried outnutrition surveillance continuously in the initial project block, and in acontrol block. Soon after the project ended, a three day workshop, including afield trip to the project area, was held in Tamil Nadu to review the project'sresults and design; about a hundred representatives of the Indian nutritioncommunity participated. In addition to the terminal evaluation, six backgroundpaper were commissioned for the workshop from local consultants (see Capoor andNaik; Chatterjee; Ferguson; Ghosh; Joseph; Rajagopalan and Vaidyanathan).
3.51 DEAR's independent sample surveys in general confirmed the accuracyof the data collected by CNWs on the clients they served. But, because theevaluations sampled the entire rural population and not just TINP's clients, theyalso came up with critically important and hitherto unknown information about theextent of exclusion (see para 3.15). Partly because the midterm evaluation

- 21 -
findings were not ready until 1986, these findings were not acted on by projectmanagement until work began on the design of the proposed follow-on project.Nevertheless, many of the other major evaluation findings--for example, theproject's relative failure to reach pregnant women and deal with moderatemalnutrition--were clear both to project management and to IDA staff long beforethe evaluations took place, because of the high quality of the project monitoringdata.
3.52 With hindsight, it appears that both implementing and fundingagencies could have taken much earlier action to respond to these problems byexperimenting immediately with changes in project design, rather than waitinguntil completion and the design of a follow-on project. It seems that TINP,having taken a 'learning process' approach in its initial year in the pilotproject block, then largely froze its design during the expansion to the rest ofthe state. The project's monitoring and evaluation system was not used to thefull for mid-course correction.
3.53 The DEAR data are of reasonably high quality, with the result thatmore is known about the impact of TINP than of most nutrition projects around theworld. Nevertheless, the design and execution of the evaluation were weak inseveral respects (Shekar, 1989), most importarzly with regard to measuring whatwas happening to nutrition conditions in the rest of the state. This is becausethe control area for the evaluation was only one block, which was merged into theproject after 40 months of implementation, during which a drought occurred.Moreover, the pilot block had both substantially higher levels of initialmalnutrition and somewhat higher rainfall, irrigation, literacy rates anddependency ratios; under these circumstances, steeper rates of decline ofmalnutrition in the pilot block might have been expected.
3.54 Second, baseline and evaluation surveys were carried out at differentseasons. This is in particular likely to invalidate the evaluation's findingswith regard to declines in diarrhea incidence, which are probably overestimated.Third, the surveys in pilot and control blocks were carried out by differentagencies using different sampling strategies. It also appears that while thebaseline and final surveys oversampled several population groups of particularinterest (households with maternal and infant deaths; pregnant and lactatingwomen; scheduled castes), no adjustment for this was made in the final analysis.This no doubt helps to explain the less favorable results shown by the sampleevaluation data as compared to the project monitoring data.
3.55 Finally, the terminal evaluation focused mainly on impact, less onproject cost-effectiveness and the design of the project's software. Twoadditional studies would therefore be useful for the design of future nutritionoperations. First, a comparative study of TINP's cost-effectiveness vis-a-visnutrition education/supplementary feeding programs in other countries. Second,a thorough documentation of those project software features with lessons forother programs, in particular of CNW recruitment, ob design and work routines;the nutrition training and supervision systems; the processes used to preparecommunities for the project and form and sustain women's groups; and theorganization of community-based supplementary food production.

- 22 -
Conclusion: Summary of Lessons Learned
3.56 Although TINP did not achieve all its goals, much good came of theproject, not least in terms of the unusual number of lessons it offer for thedesign and implementation of other programs. Some of these lessons are technicalones relating to the nutrition and health sectors. But perhaps the mostimportant ones relate to the design of the project's software, and many of thesecould be adapted and applied to the design of outreach programs in any of the'people-oriented' sectors.
3.57 In the nutrition side, TINP showed that part time village workers,if properly trained and supported, can substantially improve their community'snutritional status. Second, the project demonstrated unambiguously that growthmonitoring is an effective and feasible intervention in large scale nutritionprograms. Third, the project showed that targeted supplementation based ongrowth faltering plus feeding of all severely malnourished children cansignificantly reduce severe malnutrition; but that a move to feeding allmoderately malnourished children plus greater attention to maternal nutritionseems necessary to make a substantial impact on moderate malnutrition.
3.58 On the health side, the main finding was that large scale investmentin health infrastructure and supplies is not sufficient to improve performance.Complementary measures are needed on the software side which will maximize healthand nutrition workers' incentives to cooperate, and make them more accountablefor doing so. TINP's experience suggested six or seven such measures forexperimentation in the proposed follow-on project.
3.59 TINP's most significant lessons for other outreach programs lie int.e design of the project's software on the nutrition side. Key features forreplication include carefully defined recruitment criteria for local workers;limitation of field worker tasks to what is manageable and high priority;specification of daily and monthly work routines; the innovative decentralizedtraining system; supervisory ratios which facilitate on the job training; the useof local women's groups to support project activities; the display of performanceinformation to clients and workers at the village nutrition center; and amanagement information system which could rapidly detect performers falling belowestablished norms.
3.60 Overall, TINP can be viewed as an innovative and successful project,showing that large scale, community level interventions in the social sectors canwork. The lessons from the project are significant ones, and can help tostrengthen other outreach programs in India and elsewhere.

- 23 -
II. PROJECT REVIEW FROM THE BORROWER'S PERSPECTIVE
The Bank sent the Borrower Parts I and III of the draft PCR withrequest to prepare Part II. A reply has not been received.
a

- 24 -
III. STATISTICAL INFORMATION
1. Related Bank Loans or Credits
Credit No. : 312-IN
Title : First Population Project
Year of Approval : 1972
Purpose : The project would: (a) support an urban programconcentrating upon motivation and family planningservices to recently delivered mothers in urban areas;(b) implement an optimal GOI program by providing allthe staff and facilities which the national familyplanning program would provide if it had sufficientresources; (c) support an intensive rural programconcentrating on recently delivered mothers in ruralareas; and (d) support nutrition component to determinethe effect that improved nutrition for infants andmothers will have on the acceptance of family planningservices, and to test the best means of providingnutrition.
Status : The credit was closed on May 21, 1980. Physicalcomponents of the project were completed in March 1980.
Comments : A Project Performance Audit Report (Report No. 3748dated August 1981) is available from the AsiaInformation Center.
2. Project Timetable
Planned Revised Actual
Identification May 1978Preparation Mission September 1978 October 1978Appraisal Mission March 1979 July 30, 1979Credit Negotiations August 1979 February 27, 1980Board Approval September 1979 April 15, 1980Credit Signing May 12, 1980Credit Effectiveness Aug. 5, 1980Credit Closing March 31, 1987 March 31, 1989 March 31, 1989Project Completion June 30, 1986 March 31, 1989 March 31, 1989

- 25 -
3. Credit Disbursements
---- (US$ million) ---- Actual as XIDA FY Quarter Ending SAR Estimate Actual of Estimate
1981 September 1980 0.50December 1980 1.20March 1981 2.00June 1981 2.90 1.13 38.97
1982 September 1981 3.80 1.56 41.05December 1981 4.75 2.28 48.00March 19821 5.73 2.67 46.64June 1982 6.80 4.63 68.09
1983 September 1982 7.90 4.93 62.41December 1982 9.15 5.10 55.74March 1983 10.70 6.05 56.54June 1983 12.45 7.91 63.53
1984 September 1983 14.35 8.03 55.96December 1983 16.35 8.42 51.50March 1984 18.55 10.81 58.27June 1984 20.95 10.99 52.46
1985 September 1984 23.50 12.52 53.28December 1984 26.20 12.97 49.50March 1985 29.05 15.19 52.29June 1985 32.00 16.74 52.31
1986 September 1985 32.00 17.14 53.56December 1985 32.00 17.52 54.75March 1986 32.00 20.37 63.66June 1986 32.00 22.66 70.81
1987 September 1986 32.00 22.82 71.31December 1986 32.00 23.25 72.66March 1987 32.00 25.81 80.66June 1987 32.00 26.14 81.69
1988 September 1987 32.00 26.31 82.22December 1987 32.00 26.49 82.78March 1988 32.00- 27.66 86.44June 1988 32.00 28.41 88.78
1989 September 1988 32.00 28.41 88.78December 1988 32.00 28.63 89.47March 1989 32.00 29.49 92.16June 1989 32.00 30.16 94.25
1990 September 1989 32.00 30.31 94.72December 1989 32.00 31.98 99.94
Date of Final Disbursement: October 17, 1989

- 26 -
4. Proiect Results
Appraisal Targets Actual Achievements
Improve the nutrition and health Reductions in severe malnutritionconditions of preschool children, varying from 24% to 37% amongwith emphasis on those aged 6-36 children 6 to 36 months old.months. In the later phase of the project,
reduction of severe malnutritionwas higher, at about 55%.
Achieve a 25% reduction in the Infant mortality declined by 26%infant mortality rate, estimated to 29% in the blocks developedat appraisal at 28 per 1,000. earlier, and by 12% to 13% inAchieve a 25% reduction in the later phases of the project.mortality rate of children betweenthe ages of one and four years,estimated at appraisal at 28 per1,000 children.
Reduce to 5Z the incidence of This was not evaluated directly.Vitamin A deficiency in children Less than 25% of all eligibleunder five years of age, estimated children received all due dosesat appraisal at up to 27%. of Vitamin A syrup, while 28% of
children had not received evenone dose. This poor performancecan partly be explained byperiodic shortages of Vitamin A.
Reduce to 20% the incidence of This was not evaluated directly.nutritional anemia in pregnant and Half of all eligible pregnantnursing women, estimated at 55% women had not received Ferrousduring appraisal. Sulfate tablets (FST) against
anemia, while only 18.5% hadreceived the right quantity ofFST. This poor performance canpartly be explained by qualityproblems with the FST, leadingto their withdrawal at one pointby health component managers.

- 27 -
5. Proiect Costs and Financing
A. Proiect Costs (USS million)
AppraisalItems Estimate Actual
Civil Works 13.24 16.73Vehicles, Equipment & Furniture 9.52 5.59Training 4.14 2.89Contract Services & Technical Assistance 3.26 0.59Food Supplements 8.88 12.04Project Management Fund 0.67 2.36Drugs and Supplies 7.93 11.80Salaries and Allowances 15.12 23.77Vehicle Operating Costs 0.82 0.26Other Operating Costs 2.82 4.97Total Project Costs 66.40 81.00
B. Prolect Financing (USS million)
Source Expenditure Categories Planned Actual
IDA Civil Works 10.6 13.39Vehicles, Equipment &Furnitur. 7.5 4.47Training 3.3 2.31Contract Services & Technical Assistance 2.6 0.47Project Management Fund 0.5 1.89Drugs and Supplies 6.3 9.44Unallocated 1.2 0.00
32.0 31.97
DOMESTIC Subtotal 34.4 49.03
TOTAL 66.4 81.00

- 28 -
6. Status of Covenants
ProjectAgreementSection Subject Status
2.05 (a) Tamil Nadu shall promptly furnish to IDA the plans, specifications, reports, contract OKdocuments and construction and procurement schedules for the Project.
2.05 (b) Tamil Nadu shall:(i) maintain records and procedures adequate to record and monitor Project progress; OK(ii) enable IDA's representatives to examine Project facilities and construction OKsites and any relevant records and documents; and(iii) furnish to IDA regularly all such information as IDA shall reasonably request OKconcerning the Project, its cost and benefits, and expenditures from the Creditproceeds.
2.05 (c) Not later than six months after Project Closing Date or such later date as may be OKagreed for this purpose with IDA, Tamil Nadu shadl prepare and furnish to IDA aproject execution report.
2.08 Tamil Nadu shall:(a) carry out review of Project execution (i) one year after Project services have OKbeen introduced in Kottampatti block; and (ii) after Project services have beenintroduced in about 70 blocks, but not later than March 31, 1983, such reviews to beunder TORs satisfactory to Tamil Nadu and IDA, and shall furnish IDA with the reviewresults.(b) take into account in the review to be carried out under paragraph (a)(ii) above OKthe evaluation of mobile medical teams in Tamil Nadu being undertaken by the NationalInstitute of Health and Family Welfare and the results of other pilot projects andstudies with respect to ways to introduce community health and nutrition services inTamil Nadu.
2.10 Tamil Nadu shall, not later than December 31, 1980. establish an Advisory Panel on OK. PanelEvaluation in order to review and conment on the evaluation of the Project. est 2/81
2.11 Tamil Nadu shall, not later than August 31, 1980, prepare and furnish to IDA for its OKcomments curricula for training of staff, and shall thereafter carry out said trainingin accordance with such curricula, taking into account IDA's comments.
2.12 Tamil Nadu shall, not later than June 30, 1981. carry out and furnish to IDA for its OK.comments, a study designed to identify ways of improving selection, procurement and Completrddelivery of drugs and medicines for primary health centers and health sub-centers. 4/9/82
2.13 Tamil Nadu shall, not later than August 31. 1980, establish within the Directorate of OK.Public Health, a post of Deputy Director (Training), and appoint thereto an officer Compliancewith suitable qualifications and experience. 9/30/81
2.14 Tamil Nadu will seek and obtain IDA's approval for each expenditure in excess of OK$50,000 equivalent to be made out of the proceeds of the Project Management Fund.
2.15 Tamil Nadu to apply selection criteria satisfactorv to Tamil Nadu and IDA for OKbeneficiaries of the food supplement program under Part A of the Project.
2.16 Tamil Nadu to carry out the final evaluation study under Part D of the Project under OKterns of reference satisfactory to Tamil Nadu and IDA.
3.01 Tamil Nadu to maintain adequate accounting records in respect of the Project, of the OKdepartments or agencies responsible for carrying out the Project or any part thereof.
3.02 Tamil Nadu shall have its accounts and financial statements in respect of the Project OKaudited each fiscal year by auditors acceptable to IDA. and furnish to IDA not laterthan nine months after the end of fiscal year certified copies of said audit reports.

- 29 -
7. Use of Bank Resources
A. Staff and Consultant Inputs
Stage of Prolect Cycle Actual No. of Staffweeks
Through Appraisal .......................................... 103.0Appraisal through Board Approval .30.0Board Approval through Effectiveness .14.0Supervision .208.3
B. Missions
No. of Days Specialization Performance Rating Types of10nth/Year Persons in Field Regresented j/ Status Problems 3/
Through Appraisal:
May 1978 9 21 NTR,AGR,ECN,ARCAugust 1978 1 19 NTROctober 1978 6 28 NTR,AGR.ECN.HLT,COHMarch 1979 8 21 NTR,ECN.HLTJuly 1979 7 21 NTR.ECN.HLT.ARC
Appraisal throughBoard Approval:
January 1980 2 7 NTR
Supervision:
May 1930 4 15 NTR.MSP,ARC 1 M,PNovember 1980 4 15 NTR.HLT.COM 2 MJuly 1981 4 15 NTR,H&E,HLT 2 M,PApril 1982 4 14 NTR,HLT,M&E 2 MOctober 1982 2 13 NTR,M&E 2 T,MJune 1983 5 16 NTR,COM,ARC,M&E 2 T.MOctober 1983 4 11 NTR,COM,ARC,M&E 2 MMay 1984 5 15 NTR.M&E,ARC.HLT I T,MMarch 1985 5 15 HLT,M&E.ARC 2 MSeptember 1985 4 13 HLT,ARC,NTR 2 MJune 1986 4 14 HLT,NTR.ARC,ECN 2December 1986 3 10 HLT.ECN.ARC 2 MMay 1987 3 14 NTR,HLT 2 MFebruary 1988 2 10 NTR,ECN 2
1/ NTR - Nutrition Specialist; AGR - Agriculturist; ECN - Economist; ARC - Architect; HLT - Health SpecialistCOM - Communications Specialist; MSP - Management Specialist; M&E - Monitoring & Evaluation Specialist
2/ 1 - Problem-free or minor problems; 2 - Moderate problems; 3 - Major problems3/ M - Management; T - Technical
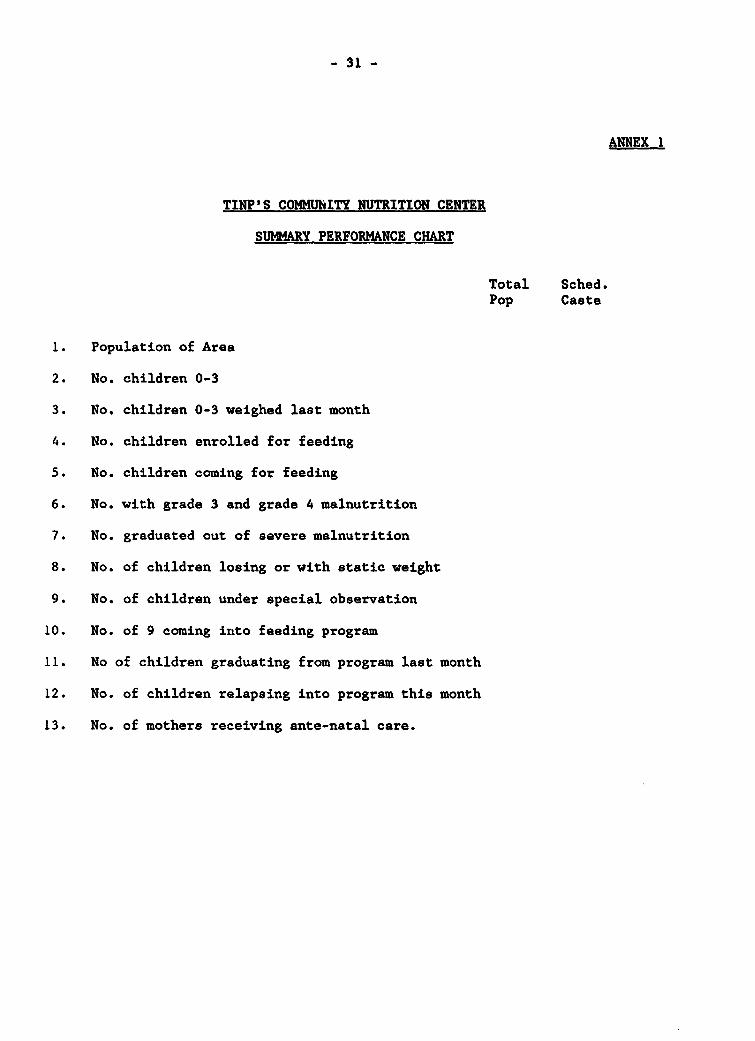
- 31 -
ANNEX 1
TINP'S COMMUhITY NUTRITION CENTER
SUMMARY PERFORMANCE CHART
Total Sched.Pop Caste
1. Population of Area
2. No. children 0-3
3. No. children 0-3 weighed last month
4. No. children enrolled for feeding
5. No. children coming for feeding
6. No. with grade 3 and grade 4 malnutrition
7. No. graduated out of severe malnutrition
8. No. of children losing or with static weight
9. No. of children under special observation
10. No. of 9 coming into feeding program
11. No of children graduating from program last month
12. No. of children relapsing into program this month
13. No. of mothers receiving ante-natal care.

- 32 -
ANEX 2
Thresholds Indicating Poor Performance
Percent of personsIndicator weighed
1. Coverage of children receiving supplement Less than 202
2. Coverage of number of children weighed Lose than 802
3. Coverage of Grade III & IV childrenamong weighed More than 10Z
4. Coverage of children entering the feedingprograme every month to total childrenweighed Less than 22
5. Coverage of children under feeding formore than 3 months More than 401
6. Coverage of children under feeding formore than 6 months More than 201
7. Children graduated in 90 days of feeding Less than 501
8. Total children graduated Less than 301
9. Children first relapsed during the monthto children graduated during the past6 months More than 32
10. Covera'e of pregnant women entering thefeeding programme to total pregnant andlactating women (eligible for feeding) Less than 1%
11. Coverage of pregnant and lactating womenreceiving supplement Less than 101
12. Coverage of distribution of vitamin A tochildren 6-36 months during last 6 months Less than 301
13. Coverage of administration of dewormingduring the month Less than 40Z

- 33 -
REFERENCES
Capoor, I. and Naik, P. Focus on Aspects of Training in TINP. Mimeo, 1989.
Chatterjee, M. On the Nutrition Component of TINPs Some Lessons and Issues.Mimeo, 1989.
Chidambaram, G. Tamil Nadu Integrated Nutrition Project--Terminal Evaluation (2Vols). Govt. of Tamil Nadu, 1989.
Dapice, D. A Cost Study of ICDS and TINP. Mimeo, 1988.
Evaluation and Applied Research Department, Govt. of Tamil Nadu. Mid-Term ImnactEvaluation Report of Tamil Nadu Integrated Nutrition Project. KottamDatti Block--Phase 1. TINP, 1984.
Ferguson, A. F. and Co. Study on Effectiveness of Communication Component.Mimeo, 1989.
Chosh, S. The Tamil Nadu Integrated Nutrition Project. Health Inputs. Mimeo,1989.
Joseph, A. Scope for Community Participation. Mimeo, 1989.
Rajagopalan, S. and Vaidyanathan, K.E. Management Information System of TamilNadu Integrated Nutrition Project: An Appraisal. Mimeo, 1989.
Raj ivan, A.K. Report on Pattern of Graduation in Different Feeding Durations andRelapse of Children to Feeding at Different Ages. Mimeo, undated.
Shekar, M. The Tamil Nadu Integrated Nutrition Project. A Review of the Projectwith Special Emphasis on the Monitoring and Information System. Mimeo, 1989.
World Bank. India: Staff Appraisal of a Nutrition Project in Tamil Nadu.Unpubd. 1980.