world bank documentdocuments.worldbank.org/curated/en/303321468743377564/pdf/multi0... · bcsir...
TRANSCRIPT

.~~~~~~~~~~~~~~~4* ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ l
* =~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~-O
- ~~~~~~-' -t ~ ~ ~ ~ ~ ~ C
K. I~~~~~~~~-y ~~~~~~, -u~~~I.~~~~~~~~~~~~~c
.5. S %~~~~~~~~~~~~~~~~~~~~~~~~~~F
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized


ADDRESSING THE PUBLIC HEALTH CRISIS
CAUSED BY ARSENIC CONTAMINATION OF DRINKING WATER
IN BANGLADESH
Authors
Rachel Beth Kaufmann (World Bank)
Birte Holm Sorensen (World Bank)
Mahfuzur Rahman (ICDDR,B)
Kim Streatfield (ICDDR,B)
Lars Ake Persson (ICDDR,B)
Technical Editors
Sundararajan Srinivasa Gopalan (World Bank)
Rachel Beth Kaufmann (World Bank)
June 30, 2001*
South Asia Health, Nutrition, and Population Unit
World Bank
* This document is a slight revision of the June 30, 2001 version that was presented to the Government of
Bangladesh. Minor changes have been made to enhance clarity and to reflect a January, 2002 agreement that
the term "arsenicosis" will be used in official documents to refer to arsenic-related skin conditions only.

ACKNOWLEDGEMENTS
The authors gratefully acknowledge the valuable contributions made by others in the preparation of this
document.
Portions of the text were taken, by permission, from WaterAid. Arsenic, 2000: An Overview of Arsenic
Issues in Bangladesh, by Elizabeth Jones.
Reviewers of this document include Dr. Alan H. Smith, of the University of California, Berkeley (United
States); Dr. A. Mushtaque R. Chowdhury of BRAC; and Dr. Anthony Measham of WB.
Reviewers of previous drafts include Dr. Smith; Dr. Measham; Ms. Adele of the Development Association
for Self-Reliance, Communication and Health; Dr. Harry Deoraj Caussy of the World Health Organization
(WHO); and Dr. D.N. Guha Mazumder of the Institute of Post Graduate Medical Education & Research
(India).

CONTENTS
A cknow ledgem ents .................................................................... 2
Abbreviations Used .................................................................... 4
Executive Summary .................................................................... 5
1. THE PROBLEM ..................................................................... 9
2. THE RESPONSE SO FAR ................................................................ 14
3. PROPOSALS FOR AN ENHANCED RESPONSE ............................................ 18
Appendices
1. Health Problems Due to Chronic Exposure to Arsenic Contaminated Drinking Water .............. 25
2. Restructuring of Bangladesh Arsenic Mitigation and Water Supply Project (BAMWSP) ............. 31
3. Response of Partner Agencies to the Arsenic Crisis in Bangladesh .............................. 34
4. BAMWSP: Current Status and Priority Tasks for Arsenic Mitigation Efforts ...................... 37
5. Questions to be Answered Through Public Information Campaigns ............................. 47
6. Arsenic Contamination of Drinking Water in Bangladesh: Public Health Research Needs ........... 48
7. Issues Relevant to Testing of Water Samples for Arsenic ....................................... 60
References .................................................................... 62

ABBREVIATIONS USED
BAMWSP Bangladesh Arsenic Mitigation - Water Supply Project
BCSIR Bangladesh Council for Scientific and Industrial Research
BGS British Geological Survey
BINP Bangladesh Integrated Nutrition Program
BMRC Bangladesh Medical Research Council
BRAC Bangladesh Rural Advancement Committee
BUET Bangladesh University of Engineering and Technology
CDC Centers for Disease Control and Prevention (United States)
DANIDA Danish International Development Agency
DCH Dhaka Community Hospital
DFID Department for International Development (United Kingdom)
DHS Demographic and Health Survey
DOE Department of Environment
DPHE Department of Public Health Engineering
GOB Government of Bangladesh
ICDDR,B International Center for Diarrhoeal Disease Research, Bangladesh
ISDCM Integrated Services for the Development of Children and Mothers
IDA International Development Association
IEC Information, education, and communication
MLGRD Ministry of Local Government, Rural Development, and Cooperatives
MOHFW Ministry of Health and Family Welfare
NGO Non-governmental organization
NIH National Institutes of Health (Unuted States)
NIPSOM National Institute of Preventive and Social Medicine
OCETA Ontario Centre for Environmental Technology Advancement (Canada)
ppb Parts per billion
RAP Rapid Action Program
SOES School of Environmental Studies, Calcutta (India)
UNDP United Nations Development Program
UNICEF United Nations Children's Fund
WB World Bank
WHO World Health Organization

EXECUTIVE SUMMARY
Following the widespread use of tube-wells over the past decade, health problems caused by the ingestion
of arsenic through drinking water have come to light at an alarming rate in Bangladesh. This public health
calamity has been described as "the largest mass poisoning of a population in history"1 . The health effects
of arsenic exposure can be extremely deleterious, ranging from the commonest manifestation in terms of
skin changes including pigmentation on the chest, back, and arms, small hyperkeratoses ("corns" or "warts")
on the palms and soles to the much more serious effects, i.e., cancer of the skin, bladder, kidneys, and lungs,
cardiovascular effects, neurological effects, anemia, and possibly cancer of the liver and diabetes. The
seriousness of the manifestation of chronic arsenic poisoning depends on the dose and duration of exposure.
In view of the grave public health consequences of arsenic contamination of drinking water, the World Bank
(WB), at the request of Government of Bangladesh (GOB) commissioned this report to review the situation
and make recommendations for the way forward. The objectives of this document are:
o to assist the Government of Bangladesh in developing policies and strategies for addressing the arsenic-
related public health crisis in both the short term and the long term;
o to assist the development partners of Bangladesh in determining the appropriate extent and nature of
external support required in this regard;
The paper describes the problem, by summarizing the available evidence regarding exposure to arsenic-
contaminated water in Bangladesh along with the historical context, describes the response of governmental
and non-governmental agencies in relation to the arsenic problem so far, and recommends future actions,
including fostering public-private partnerships and identifying areas for operational research, especially
with regard to public health.
The paper primarily addresses the public health response and does not deal exhaustively with testing and
provision of arsenic free water. This is not intended to diminish the importance of provision of arsenic
free water - it is absolutelt essential! But many donors, government and non-government agencies are
actively involved in this aspect of the problem. Until now, little attention has been given to the health
aspects.
The paper does not seek to provide a detailed strategy, action plan, timeframe or budget for addressing
arsenic-related public health activities. The purpose of this paper is to raise the issues for discussion and
further study during subsequent preparation of an Arsenic Public Health Project. Such detailed plans are
therefore expected to be developed by the respective agencies, as a result of (rather than as a part of) this
document.
1 Smith AH et al. Contamination of drinking-water by arsenic in Bangladesh: a public health emergency. Bulletin ofthe World Health Organization, 2000, 78:1093-1103.

The Problem (Historical Context and Available Evidence)
In the 1970s and the 1980s, tube-wells were installed throughout Bangladesh as a means of providing water
that was free of the bacterial and pesticide contamination found in surface waters. It is now estimated that
97% of the rural population uses tube-well water for drinking, cooking, and irrigation. This increased use
of tube-wells has resulted in a decrease in the incidence of diarrheal diseases but an unintended consequence
has been the marked and widespread occurrence of arsenicosis (a term used to describe skin conditions
associated with chronic ingestion of arsenic), observed since 1993. Arsenic is present in tube-well water in
Bangladesh in concentrations much higher than the WHO guideline of 10 parts per billion (ppb; or
micrograms per liter) and even higher than the less stringent standard of 50 ppb set by the Government of
Bangladesh. Surveys have shown a wide range of 20% to 94% (depending on the geographical area, testing
methods and standards used in the different surveys) of water samples from tube-wells with arsenic
concentrations of above 50 ppb, one survey showing 8.4% of the wells with concentrations as high as 300
ppb. The ground water is arsenic-contaminated in at least 61 of Bangladesh's 64 districts. Based on the
above, at least 20 million people in Bangladesh (about 20% of the population) are exposed to the risk of
arsenic poisoning from contaminated drinking water, but estimates range as high as 77 million.
The Response thus far
The single largest effort mounted by Bangladesh so far to address the problems caused by arsenic
contamination of water in Bangladesh has been in through a Project called Bangladesh Arsenic Mitigation
and Water Supply Project (BAMWSP), jointly financed by the Government, the Swiss Development
Cooperation and the WB - though a credit from the International Development Association (IDA).2 The $44
million project includes activities to address the immediate problem as well as to find a long-term solution.
Apart from screening and testing (both water samples and patients), the project supports information
provision and training activities. This project has been having considerable implementation problems and is
currently being restructured; Appendix 2 describes briefly the restructuring plan.
There is an inter-sectoral National Steering Committee for Arsenic Mitigation, with representation from the
relevant line ministries and other partner agencies. Yet there is no national policy or strategy to address the
problem of arsenic contamination of drinking water. No effective mechanism exists to coordinate the
different sectors involved, particularly to bring together the interventions aimed at supplying arsenic-safe
water and those aimed at providmg health services to those affected.
The Department of Public Health Engineering (DPHE) has been testing tube-wells and conducting activities
aimed at informing the public about the problem.
The Ministry of Health and Family Welfare (MOHFW) has also carried out a few activities to address this
problem; some information, education, and communication (IEC) materials developed, treatment protocols
have been developed, some training of health professionals has been undertaken and patients have been
identified.
2 World Bank. Project Appraisal Document, Bangladesh Arsenic Mitigation and Water Supply Project, 1998

Finally, several international agencies and Non-Governmental Organizations (NGOs) have been supporting
interventions to deal with arsenic contamination of drinking water; but there is a need for better
coordination among these partner agencies and a concerted and coherent national plan. These activities have
mainly been centered around provision of arsenic free drinking water; several NGOs and the United
Nations Children's Fund (UNICEF) supported activities have included comprehensive community
responses to the arsenic problem. There is a need for coordination amongst these partner agencies and for a
coherent national plan to ensure national coverage.
Proposals for an Enhanced Response
The highest priority should undoubtedly be given to testing of water and provision of safe drinking water
solutions that are acceptable and affordable. This paper proposes an additional and immediate enhanced
response to the serious public health challenge that arsenic contamination of drinking water poses in
Bangladesh. The response needs to be multi-sectoral and nationwide. There is a critical need to link the
interventions in the water sector with those in the health sector and to ensure the full participation of other
relevant line ministries and departments. A stronger partnership between the public sector and the private
sector (including NGOs) is also required to maximize the benefits from a concerted response.
Solutions developed should be gender-sensitive and take account of implications for women in particular,
because they generally are burdened with the responsibility of fetching the water for the whole household.
Thus any solution that impose an even greater burden on women, e.g., by making them walk much longer
distances to fetch water than they already do, will not be appropriate. Finally it is absolutely vital to ensure
coordination among the various partners, both national and international.
The activities being covered already under the restructured BAMWSP are: arsenic mitigation activities at the
village, union parishad and upazila levels, deep aquifer mapping and related studies, formal Government
mechanism for the verification and certification of water-testing technologies and activities aimed at
addressing the safe disposal of arsenic and other chemical byproducts arising from the mitigation activities.
Other activities recommended to be part of the enhanced response are:
* Informing the public about the problem, its health implications, and what the communities can do
themselves to mitigate the effects;
* Nationwide training of health professionals, to detect, treat and counsel the victims of arsenic
contamination;
* Establishing an effective system of case-finding (both passive and active, and both during and apart
from water-testing activities) and surveillance (as an integral part of the overall Epidemiological
Surveillance System);

* A comprehensive research agenda (especially within the domain of public health) to better inform
future policies and strategies; (details in Appendix 6);
* Water-testing riding on case-finding efforts (i.e., by the health sector) and case-finding efforts piggy-
backed to water-testing (i.e., by the water supply sector);
* Provision of safe drinking water both from the perspective of arsenic and in terms of microbiological
pathogens.
Actions following the dissemination of this paper are likely to include:
* A review of public health responses in other countries affected by arsenic;
* A review of NGO-sponsored comprehensive, community based arsenic mitigation activities, to
determine what does and does not work;
* A review of training curricula;
* A review of public information experiences and materials;
* Creation of an international expert panel for identification and dissemination of research related to
arsenic.

1 THE PROBLEM
1.1 ARSENIC IN DRINKING WATER AROUND THE WORLD
Arsenic has been documented to be carcinogenic, i.e., cancer-causing. Inorganic compounds of arsenic are
much more toxic than organic compounds containing arsenic. Such highly toxic arsenic has been detected in
ground-water in a number of countries around the world. The WHO has provisionally determined 10 ppb
as the maximum permissible concentration in drinking water. As this guideline is provisional (in view of
technical difficulties in measuring small quantities of arsemc in water), country governments have set their
own safety standards for arsenic in drinking water; 50 ppb is the maximum permissible concentration in
Bangladesh. Table 1 shows selected results from surveys of arsenic contamination of drinking water in eight
countries around the world, as reported in the literature. While the highest reported concentration is in
India, the second highest is in Bangladesh. However, the seriousness of the problein is worse in Bangladesh
than anywhere else, in terms of the size of the population exposed to the risk. Asia has at least four of the
major problem areas in the world, in Bangladesh, West Bengal, India, Inner Mongolia, and Taiwan.
1.2 THE RECENT HISTORY OF ARSENIC CONTAMINATION OF WATER IN BANGLADESH
Until the early 1970s, most of the over 100 million inhabitants of Bangladesh obtained their drinking water
from shallow hand-dug wells, rivers and ponds-a practice that was associated with cholera, diarrheas and
dysenteries, due to microbiological contamination of such surface water. To address this problem of water-
borne intestinal disorders as well as to enhance the supply of water for agricultural purposes, the
Government, with the help of international partners and non-governmental organizations, carried out a
program of installing tube-wells with hand-pumps all over Bangladesh and mass campaigns to convince
people that the ground water was safer to drink. It is estimated that Bangladesh now has 8 to 12 million
shallow tube wells3 . Reportedly, by the 1997, 80% of the population had access to "safe" drinking water4 .
However, an unintended consequence of this successful switch from surface to underground sources of
drinking water has been the increasing discovery of arsenic contamination of drinking water, which has put
as much as 15-20% of the population at the risk of developing chronic arsenic poisoning, the effects of which
manifest themselves slowly, sometimes over decades.
The arsenic contamination in Bangladesh is of geological origin. Differences in the rate of ground-water
movement due to the location of rivers and in topography or type of sediment (clay, silt or sand) probably
account for much of the local variation in the extent of arsenic contamination. It is unknown whether the
recent heavy use of groundwater has affected the rate of release of arsenic into groundwater; so it is difficult
to predict whether the contamination will increase or decrease over time.
3 World Health Organization. Arsenic in Drinking Water Fact Sheet No. 210, Revised May, 2001 (Available athttp:I /www.who.int/inf-fs/en/fact2l0.html.)
4 UNICEE Progotir pathey, on the road to progress; achieving the goals for children in Bangladesh, October 1998.Dhaka. Bangladesh Bureau of Statistics, Ministry of Planning, Government of the People's Republic of Bangladesh withUNICEF, 1999.

Table 1. Arsenic contamination of drinking water around the world
Country Highest reported concentration Number of individuals Year first
of arsenic in drinking water (ppb) potentially exposed reported
Argentina * 3000 20,000 1938
Bangladesh 4730 > 20 million 1970
Chile *. 800 250,000 1958
China *w 2140 > 400,000 1969
India * 3880 > 1 million 1978
Mexico * 800 > 200,000 1963
Taiwan * 800 > 100,000 1961
Thailand . 800 no data 1987
Source: Modified after Mandal BK et al. 19965, Guha Mazumder DN et al. 19986, and British Geological Survey and Mott
McDonald, 19997
Source of arsenic contamination. *ground water * Industrial source into surface water u surface water
Ground water is found at different depths below the surface. Most parts of Bangladesh contain at least two
aquifers: a shallow aquifer extending from 10 to 100 meters below the surface, and a deeper aquifer starting
at about 200 meters below the ground. The tube-wells generally tap into the shallow aquifer, which is the
source of the current arsenic problem. Water from depths of less than 10 meters or more than 150-200 meters
appears to be essentially arsenic-free. It has been observed that shallow wells are usually uncontaminated
even in areas where a high proportion of tube wells show arsenic contamination. But the shallow wells are
more prone to microbiological contamination, and tube-wells deeper than 200 meters below the surface are
much more expensive to install.
A regional survey showed a correlation between the year of construction of the wells and the proportion that
was contaminated. On average, older wells were more likely to be contaminated than recently constructed
ones. Only long-term monitoring will determine whether this finding actually corresponds to increasing
5 Mandal BK et al. Arsenic in groundwater m seven districts of West Bengal, India - the biggest arsenic calamity in theworld. Current Science, 1996, 70:976-986.
6 Guha Mazumder DN et al. Arsenic levels m drinking water and the prevalence of skin lesions in West Bengal, India.International Journal of Epidemiology, 1998, 27:871-877.
7 British Geological Survey and Mott MacDonald (UK): Executive Summary of the main report of Phase I, groundwaterstudies of arsenic contamination in Bangladesh. For the Government of Bangladesh, Mirustry of Local Government, RuralDevelopment, and Cooperatives, Department of Public Health Engineering, and Department for International
9 Development (UK), 1999.

concentrations over time in individual wells. The possible effect of the water-pumping itself on arsenic
concentration could be a key policy issue for the water sector. The critical question is whether or not
pumping of groundwater is creating or exacerbating the problem of arsenic in drinking water.
1.3 STUDIES OF ARSENIC IN THE GROUND-WATER OF BANGLADESH
Arsenic contamination of groundwater was first reported in 1993 by the DPHE in Chapai Nawabganj district
(Barughuria Union, Sadar Upazila)8 . Other early data came from the Dutch-funded Eighteen District Towns
project of DPHE. The analyses carried out in the Netherlands confirmed the patchy nature of the arsenic
distribution. An international conference on arsenic in 1995 convened by Dr. Dipanker Chakraborti of the
School of Environmental Studies (SOES), Jadavpur University, Calcutta, raised the awareness about the
arsenic problem of West Bengal and made it clear that there was an urgent need for more detailed studies in
Bangladesh. Since then, several studies have been conducted on arsenic contamination of drinking water in
Bangladesh. With assistance from WHO, the DPHE zonal laboratories were equipped for arsenic analyses
and several thousand water samples have been analyzed in these laboratories. An increasing number of
studies of arsenic contamination followed from 1997 onward.
The National Institute of Preventive and Social Medicine (NIPSOM), in a survey in the Rajarampur village
of Nawabganj district in 1996-1997, found that 29% of the wells were contaminated by arsenic in
concentrations above 50 ppb9 . In 1996-97 Dhaka Community Hospital (DCH) and SOES found that 91% of
the 265 tube wells tested contained greater than 50 ppb of arsenic in the Samta village, Jessore District10; a
different study by DCH and SOES found such levels in 59% of samplesll.
In 1997, a nationwide survey of about 23,000 tube wells by DPHE with assistance from UNICEF used field-
test kits that only classified the arsenic concentration of the water as above or below 100 ppb. This survey
however demonstrated that arsenic contamination was most serious in the southeast of Bangladesh.
A British Geological Survey (BGS) study of Chapai Nawabgonj in early 1997 revealed concentrations of
arsenic up to 2400 ppb. Also in early 1997, a randomized sample survey of wells in six districts in northeast
Bangladesh by the Bangladesh University of Engineering and Technology (BUET) indicated extensive
contamination of that region. Another BGS survey of 41 districts in 1998 found arsenic levels of over 50 ppb
in 35% of the water samples; in this survey, 8.4% of the samples were above 300 ppb7 . Figure 1 shows a map
of Bangladesh, with the distribution of arsenic contamination, as found by the BGS.
8 Khan AW et al. Arsenic contamination in groundwater and its effect on human health with particular reference toBangladesh. Journal of Preventive and Social Medicine, 1997, 16. 65-73
9 Ahmad SA et al. Arsenic contamination m ground water and arsenicosis in Bangladesh International Journal ofEnvironmental Health Research, 1997, 7:271-276
10 Biswas BK et al. Detailed study report of Samta, one of the arsenic-affected villages of Jessore District,Bangladesh. Current Science, 1998, 74:134-145.
11 Chowdhury TR et al. Arsenic poisoning in the Ganges delta. Nature, 1999, 401: 545-546. 4D

A survey by the Rapid Action Program (RAP), in villages already known to have arsenic contaminated wells,
found arsenic concentrations of more than 100 ppb in 62% of the 32,651 wells 12 . The Bangladesh Rural
Advancement Committee (BRAC) surveyed all 12,000 wells in the Hajiganj Upazila of Chandpur district by
field test kits, and showed that 94% of the wells were contaminated. That survey also demonstrated the
potential of involving community workers in large-scale water testing programs.
Based on the results of water-testing, it has been estimated that more than 20 million people (or roughly 20%
of the total population) are at risk of arsenic exposure through contaminated drinking water in Bangladesh.
Estimates on the higher side range from 25-77 million. However, comprehensive studies on the incidence
and prevalence of the diseases resulting from arsenic contamination have been very few. In a study of 200
affected villages, RAP found arsenic-induced skin lesions in 1802 of 469,424 people. During the same period,
a more detailed study of four villages found skin lesions in 430 adults of the 1481 interviewed and
examined1 3 . A 3-week survey by DCH and SOES in 18 affected districts found skin lesions in 57.5% of the
1630 adults and children examined 14 . In another study, of the 7364 patients examined, approximately a third
were found to have skin lesions typical of arsenic poisoning15 . Despite very limited case-finding efforts,
more than 7000 patients with arsenicosis have been identified already. Based on cancer risk estimates made
by the U.S. National Research Council16 , and a conservative figure of 20 million population exposed, there
could be 200,000 excess cancer cases caused by arsenic contamination of drinking water, a grave public
health crisis. Obviously, the estimate of cancer risk will be even greater if one uses the higher estimates of
population exposed.
Appendix 1 lists the known health effects of ingesting inorganic arsenic in drinking water over prolonged
periods. Suffice it to say that these effects range from skin lesions to cancers and could be extremely serious.
As this document is being drafted, preliminary information is emerging regarding arsenic in food (from
irrigation of crops) and absorption of arsenic through the skin (during bathing and agricultural work in
paddies). The extent to which these may be harmful is yet to be established.
In summary, the widespread arsenic contamination of tube-well water in Bangladesh has been clearly
established, though estimates have ranged from 20% to 94% of the wells examined, depending on the
selection of wells to be surveyed, the testing methodology used, and the standards used. The extent of
arsenic poisoning among the people exposed to contaminated water also varies and needs further study;
but there is no question that the threat is serious and needs immediate attention.
12 Quamruzzaman Q et al. Rapid action programme: emergency arsenic mitigation programme in two hundredvillages in Bangladesh. In Arsenic Exposure and Health Effects. Proceedings of the Third International Conference on ArsenicExposure and Health Effects, 12-15 July 1998, San Diego, pages 363-366 Oxford, Elsevier Science, 1999
13 Tondel M et al. The relationship of arsenuc levels in drinking water and the prevalence of skn lesions inBangladesh Environmental Health Perspectives, 1999, 107:727-729
14 Dhar RK et al. Groundwater arsenic calamity in Bangladesh. Current Science, 1997, 73:48-59.
15 Biswas BK et al. Groundwater arsenic contamtnation and sufferings of people in Bangladesh, a report up to January 1999Paper presented at the International Conference, Arsenic in Bangladesh Ground Water. World's Greatest ArsenicCalamity, Staten Island, New York, USA, 27-28 February, 1999.
16 National Research Council. Arsemc m drinking water. 'Washington, DC: National Academy Press, 1999

Figure 1. Map of Bangladesh showing the distribution of arsenic contamination in groundwater
270 1 1 1 1 1
240
iu ~~~~~~Arsenic (jAg L-1)
26 *~~~~~~~~ <10
_ *~~~~~~ >50
U)~~~~~~~~~~~~~~~~~~~~1
230
220
210
(c) DPHE/BGS/DFID (2000)
20° l l l l l880 89° 900 910 920 930
Longitude
Source: British Geological Survey and Departmnent of Public Health Engineering, 200117. Used by permis-
sion of British Geological Survey.
17 British Geological Survey and Department of Public Health Engineering. Arsenic contamination of groundwaterin Bangladesh. Kinniburgh, D G and Smedley, P L (Editors). Volume 2: Final report. Britsh Geological Survey ReportWClOOs19, British Geological Survey, Keyworth, 2001 <

2 THE RESPONSE SO FAR
2.1 THE ACrORS INVOLVED
2.1.1 The Department of Public Health Engineering (DPHE)
DPHE, which is under the Ministry of Local Government, Rural Development and Cooperatives (MLGRD),
is charged with providing safe drinking water to both rural and urban areas. DPHE is thus responsible for
testing water quality.- DPHE has one staff person at the Upazila level who is responsible for water testing,
presently using Hach field kits. DPHE also has laboratories at the four zone offices where a colorimetric
method is used for testing water for arsenic. The latter test method costs 500 Taka (roughly equal to US$10)
and capacity is limited.
2.1.2 The Public Health System
The Government health services in Bangladesh are the responsibility of the MOHFW and are provided
through a network of facilities at the primary, secondary and tertiary levels of health care. Only 12% of out-
patient services are sought from the public sector. Health effects of arsenic ingestion have not, until now,
formed an important part of the pre-service or in-service training curriculum for medical or other health
professionals including field workers in Bangladesh. Nor has the management of patients with arsenic-
related diseases been receiving any priority attention from the health services so far.
2.1.3 The Non-Governmental Organizations (NGOs)
There are some 600-700 NGOs in Bangladesh offering varying levels of health services. These range in size
from BRAC, which employs 25,000 full-time staff and has activities in 50,000 villages, to very small
community groups that operate in a single village. NGOs have a comparative advantage in terms of their
ability to coordinate water supply interventions with health service interventions, because of the absence of
different line ministries vested with different responsibilities, and because of their usually smaller scope of
coverage. Most health NGOs operate community-based services and clinics with limited resources, usually
without a medical doctor on staff; however, a few well-equipped and staffed rural hospitals are also run by
NGOs.
2.1.4 The Commercial Private Sector
The commercial (for-profit) private sector includes private pharmacies, physician-managed private practices
and nursing homes, and clinics run by other health professionals and by traditional or village healers. Many
of the private care providers also hold government jobs. Little is known about the extent to which arsenic
patients currently seek medical assistance from the private sector, or about what advice they may be given.
Essentially, there has been no effort thus far to forge a partnership with the pnvate sector in dealing with the
problems caused by arsenic contamination of drinking water.

2.2 THE RESPONSE SO FAR FROM THE PUBLIC SECTOR
2.2.1 The National Steering Committee for Arsenic Mitigation
In 1996, a National Steering Committee for Arsenic Mitigation was set up and headed by the Honorable
Minister for Health and Family Welfare. Its mandate included policy formulation, endorsement of
programs, and monitoring and coordination of activities related to arsenic contamination. The committee is
inter-sectoral in its composition, with representatives from the relevant line ministries and other partner
agencies.
A comprehensive plan to ensure national coverage and coordination between water testing, training of
health staff, mass media campaigns and interpersonal communication is, however, yet to be developed.
Some reasons for the slow progress in development of a national policy and strategy are:
l lack of knowledge of the extent and serious long term effects of contamination of water sources;
e uncertainty regarding the feasibility and safety of using alternative water sources;
e concems about costs, feasibility, and safety of water treatment options and patient treatment options;
* a desire to hold back decisions until sustainable interventions can be offered;
* lack of coordination between relevant govemrnment agencies (progress has likely been hampered by the
split of responsibility for addressing issues of water contamination and its health effects between
MLGRD and MOHFW).
l lack of effective partnerships with the private sector, NGOs and international agencies; and
* concern about the political implications of an aggressive and open policy to deal with arsenic
contamination.
2.2.2 Response of the Water Sector
(a) The Bangladesh Arsenic Mitigation Water Supply Project (BAMWSP)
So far, the largest intervention mounted by Bangladesh to deal with arsenic contamination of water is the
Bangladesh Arsenic Mitigation Water Supply Project (BAMWSP), which was started in late 1998 and wasplanned to run over 4 years. The US$ 44.4 million project is financed by GOB, grant funds from Swiss
Development Corporation, and an IDA Credit. It was envisioned as the first phase of a longer-term program
to be funded by at least one additional 4-year credit from IDA. The project is currently being restructured.
Appendix 2 provides a brief description of the current ideas on the restructuring of the project.
The Project has two major components: (i) emergency screening of tube wells and arsenicosis patients alongwith provision of emergency water supply and medical interventions and (ii) identification of longer-term,
sustainable solutions to the arsenic crisis. To date, BAMWSP has moved slowly; only US$2 million of the
available funds have been disbursed and water-testing and patient identification have been conducted inonly 30 out of 463 upazilas. Along with a number of institutional flaws in the project design, the reasons for

the slow start include design issues related to institutional arrangements, lack of a clear strategic plan, and
lack of clear government leadership to motivate and coordinate arsenic related activities.
The BAMWSP Technical Advisory Group consists of an eight-member panel of experts who, at the request
of BAMWSP, advise on technical issues such as alternative drinking water sources, field test kit
specifications, and arsenic removal technologies as well as commission research on these topics. (Members
are from BAMWSP, Dhaka University, Department of Civil Engineering, BUET, International Union for
Conservation of Nature, Dhaka Community Hospital Trust, Private Rural Initiative Program, MOHFW, and
DPHE.) They are now recommending the Merck kit for water testing, the three-kolshi arsenic removal
technology and the following alternative water sources to replace or supplement shallow tube wells: deep
tube wells, rainwater harvesting, pond sand filters, and hand-dug wells.
BAMWSP is currently supporting clinician training through the Bangladesh Medical Association, targeting
2,000 physicians at the district/upazila level and 12,600 field staff at the union level. The training covers
identification, diagnosis, and management of patients with arsenic-related diseases, including referral. The
training is limited to the upazilas chosen for priority interventions by BAMWSP.
(b) Other Activities in the Water Sector
DPHE has also provided some information to the general public related to arsenic but focus has until now
been on water related issues, with less attention given to health consequences.
A number of other local organizations, bilateral and international donors, NGOs, and research institutions
have also initiated programs, most of whlch emphasize water testing and identifying sustainable water
treatment options. The larger donors supportmg DPHE for arsenic mitigation are UNICEF, WHO, the
Danish International Development Assistance (DANIDA), the Canadian International Development Agency,
the United Kingdom Department for International Development (DFID), the Japan International
Cooperation Agency, Australian Aid, the United States Agency for International Development, the United
Nations Development Program (UNDP), and Rotary International. A United Nations Foundation grant for
2.5 million dollars, approved in July 2000, will enable UNICEF and WHO to support a project to provide
clean drinking water alternatives to nearly 1.1 million people in three of the worst affected sub-districts of
Bangladesh2. Brief descriptions of projects conducted by major stakeholders are listed m Appendix 3.
Water sector agencies, especially the NGOs, have also undertaken physician traimng, case identification,
public education, and community involvement in finding solutions to the arsenic problem.
2.2.3 Response of the Health Sector
MOHFW, through a UNICEF funded project, is currently training doctors and health workers in an effort to
have at least some health professionals informed about the diagnosis of arsenic-related diseases and
alternaive options for drinking water across country. A treatment protocol and IEC materials have been
prepared.
There is some overlap between training conducted by the Bangladesh Medical Association, MOHFW, and
3 NGOs sponsored by UNICEF directly. By and large, the districts where a high proportion of tube wells are

known to be contaminated have been given priority. The Bangladesh Integrated Nutrition Project (BINP) is
training staff in their areas of operation to test water at their centers for arsenic and to diagnose skin lesions
if patients present themselves.
2.2.4 Available arsenic removal technologies
A number of arsenic removal methodologies have been developed for use in Bangladesh, some suitable for
households and some suited to serve communities. These technologies generally use one of the following
methods of arsenic removal: co-precipitation (coagulants bind arsenic and are then filtered); adsorption
(arsenic adsorbed onto surface of suitable materials); ion-exchange (arsenic ions attracted to charged
polymer resins); and membrane filtration (selectively permeable membranes remove arsenic by filtration).
Some NGOs have undertaken small-scale testing of one or more methodologies and some are distributing
technologies to their clients.
Household level arsenic removal technologies were recently (2000-2001) tested in a rapid assessment by
BAMWSP / DFID / WaterAid Bangladesh15 . Technologies were selected on the basis of previous encouraging
results, relative user-friendliness, ready availability within country and the interest of the organization
promoting the technology. Preliminary results of the tests are shown in Table 2. Testing will continue to
determine each technology's "breakthrough" point, when so much water has passed through that the
technologies can no longer filter more arsenic.
Table 2. Results of BAMWSP/DFID/WaterAid assessment of arsenic removal technologies1 5.
Technology tested Percentage of treated Average initial / User total score*
water brought below annual operating (315 highest
50 ppb arsenic cost (Taka) possible)
Alcan Enhanced 100 25,000/15,000 235
Activated Aluminium
BUET Activated Alumina Filter 100 1000/unknown 96
DPHE / DANIDA Two-Bucket System 25** 325/ unknown 200
Garnet Home-Made Filter 43 400/ unknown 149
Sono Three-Kolshi Method 100 325/ unknown 203
Stevens Institute Technology 85 500/unknown 138
Tetrahedron Ion Exchange Resin Filter 81 12,000/6000 174
* The user preference scale included variables such as overall preference, flow rate, taste, smell, ease of use, cost, ease of movement,ease of maintenance and waiting time.
** This method is not effective at reducing arsenic levels if the well water arsenic level is above 120 ppb; effective at lower arsenic
levels.

3 PROPOSALS FOR AN ENHANCED RESPONSE
This chapter proposes an immediate and enhanced response to the serious public health challenge that
arsenic contamination of drinking water poses in Bangladesh. The response needs to be multi-sectoral and
nationwide. There is a critical need to link the interventions in the water sector with those in the health
sector and to ensure the futll participation of other relevant line mimstries and departments such as the
Ministry of Information, the Ministry of Science and Technology, the Ministry of Agriculture, the
Department of Environment (DOE), the Bangladesh Council for Scientific and Industrial Research (BCSIR),
and the Bangladesh Medical Research Council (BMRC). There is also the need to develop a stronger
partnership between the public sector and the private sector (especially NGOs).
The solutions developed should be gender-sensitive and take account of implications for women in
particular, because they are generally the people who are burdened with the responsibility of fetching the
water for the whole household. Thus, any solution that impose an even greater burden on women, e.g., by
making them walk longer distances to fetch water than they already do, will not be appropnate.
Finally, it is absolutely vital to ensure coordination among the various stakeholders, both national and
international. Fortunately, there is an established and well functiomng donor coordination mechanism
through the Bangladesh Health and Population Consortium, which supports the Sector Program for health
in Bangladesh. However, coordination mechanisms across sectors - both within and between agencies -
will have to be established and strengthened.
A group of donor agencies working in the field of arsenic mitigation have prepared a comprehensive
overview of the pnority actions required. They include:
Implementation of Field Mitigation Activities
Arsenic mitigation activities should be planned at the village, union parishad, and upazila level through
community mobilization and technical assistance and financial support.
Deep Aquifer Mapping
There is a need for a comprehensive mapping of the deep aquifer water sources and a better
understanding of the impact associated with tapping the deep aquifer (in various parts of the country)
for drinking water.
Technology Verification
A formal government mechanism, possibly housed in BCSIR, is required to assess and verify the
applicability of proposed treatment technologies for removal of arsenic.
Waste Issues
The DOE should address potential environmental impacts of disposal of arsenic and other byproducts
Aft arising from mitigation activities.

Priority activities to be part of the public health response are:
* Informing the public
* Training health care workers
* Establishing an effective system of case-finding and surveillance
* Establishing and pursuing a research agenda (specifically in the field of public health)
* Water testing linked to case-finding (i.e., within the health sector)
3.1 INFORMING THE PUBLIC
Well-designed public education programs need to be carried out, both to inform people about the issues and
to educate them about risk-reduction options. The programs must make clear what arsenicosis is and what
it is not. Although no data is available to say whether or not arsenicosis victims suffer social discrimination,
there is concern that victims might be ostracized, especially if people if people incorrectly assume that skin
lesions represent contagious disease.
Public information messages must make it clear that the emergency strategy is one of risk minimization
using existing knowledge and that research is under way to provide long-term solutions. It will be essential
to use public information to create empowerment and reassurance rather than scare and panic. Additionally,
the messages should be easy to comprehend and should be translated into local languages.
As there is not a functioning system in place to test all tube wells in the country in the short run, basic
information should be available to all Bangladeshis to allow them to take precautions for obtaining arsenic-
free water. The information strategy could include the use of mass media as well as more localized group
or interpersonal communications through schools and special programs. The latter efforts should be
coordinated with tube well testing.
Public information campaigns will require good coordination between public and private sectors to ensure
high quality, broad coverage, and regular updates of the information. Considering the urgency of the
situation, all the partners need to act simultaneously to ensure the maximum impact. Appendix 5 lists a set
of core issues that need to be addressed in public information campaigns. It is noted that UNICEF has
developed a well-researched information package.
3.2 TRAINING HEALTH CARE PROVIDERS
Clinical treatment providers, be they public or private, will have to possess knowledge and skills for both
preventive and curative measures relating to arsenic. Such skills extend beyond the conventional medical
knowledge of diagnosis and treatment to include information on water testing, arsenic removal techniques,
and alternative water sources as well as basic skills in counseling to improve peoples' compliance in using
safe water alternatives.

One significant problem is the lack of proven, effective treatment options. Physicians have been advised to
provide anti-oxidant vitamins in the hope that these may be beneficial. The later sequelae of chronic arsenic
exposure, such as cancers, cardiovascular disease, and diabetes, must be treated as one ordinarily treats
these diseases. However, at local clinics, equipment and expertise to treat these diseases are not available.
Training must therefore focus on what can be done to help the patients in the absence of effective treatment,
e.g., education, counseling, and referrals.
Clearly, it is highly important that safe and effective treatments be identified. Rigorous clmical studies on
the effectiveness of potential treatments must be conducted, and the results should be speedily incorporated
into provider and public education programs. It must, however, be emphasized that priority should be given
to providing safe drinking water options since patients will gradually improve when exposure stops.
Training of health staff in relation to arsenic-related diseases has until now been provided by several
agencies. The training has largely covered diagnosis, treatment, and referral with less emphasis on
preventive measures and counseling skills.
Experience from the Health and Population Sector Program indicates that the current system of training
health workers (both pre-service and in-service) is unlikely to have the capacity to conduct the required
nationwide training for all clinical workers within a short period.
A viable immediate option may be to develop a basic training package with information required at the
community, union, upazila, and district levels and to prepare a phased plan for national traming based on
need, i.e. starting with the upazilas known to have the highest concentration of affected tube wells. This
training task could be shared between governmental and non-governmental training institutions. The
training package should then be regularly updated to incorporate new research findings.
As a long-term measure, information and skills regarding arsenic contamination of drinking water and its
health effects should be included in basic curricula for health care workers.
3.3 CASE-FINDING AND SURVEILLANCE
3.3.1 Case-finding
There are two types of case-finding, active and passive. Passive case-finding is simply allowing individuals
to present themselves for treatment. Active case-finding is going out to the field to examine individuals for
signs of arsenic-related diseases.
Some of the NGOs that perform field tests of tube well water also do related case-finding by querying or
examining the individuals who use the well in question for arsenic-related skin lesions. These active case-
finding efforts should be continued. Case-finding and medical referrals, along with public education,
should be integrated into all tube well testing efforts. Although arsenic can cause a variety of health
conditions, it is only feasible for tube well testers to look for skin lesions, which are the commonest and
earliest symptoms.

However, as field tests can be inaccurate and may not detect all the individuals exposed to arsenic, case-
finding can and should be improved by carefully training outreach workers - starting with health workers,
but eventually extending to other sectors, if needed - to recognize arsenic-related skin lesions, and including
this activity as part of their regular job descriptions. When health workers do active case-finding, they also
need to be equipped to counsel their clients.
Additionally, medical practitioners should contribute to case-finding by making a special effort to check for
skin lesions and counsel patients about arsenic. The skin check should be repeated as opportunities arise.
If patients complain of other symptoms that may be arsenic-related, the clinicians should advise, treat, and
refer as appropriate.
3.3.2 Surveillance
Passive case-finding will likely result in detecting a fraction of the actual number of cases because the initial
symptoms are mild and most people are unaware of arsenic and its hazards (although eventual public
enlightenment about arsenic poisoning and its symptoms could change this somewhat.) Active case-finding
is carried out unevenly at best. Thus, case-finding efforts by themselves are not an adequate source of data.
A national survey, using a representative sample, consistent methodology, and diagnostic criteria, would
both indicate the total prevalence of arsenicosis and provide evidence regarding whether susceptibility
varies by age, sex, or other factors; it may also provide some clues about areas hardest hit. The most efficient
way to complete such a survey is to piggy-back it onto an existing population based survey as descnbed in
appendix 6.
Following such a survey, arsenic surveillance should be integrated into the overall epidemiological
surveillance system by including chronic arsenic poisoning as a notifiable disease.
Standardized criteria for diagnosing and grading skin lesions must be developed and carefully followed.
WHO is leading an effort to develop such criteria; once finalized, they should be adopted by the MOHFW,
widely disseminated, and used uniformly by all organizations engaged in case-finding, treatment, and
surveillance.
3.4 RESEARCH NEEDS
The appropriate response to arsenic contamination of drinking water over the medium and long term will
require a considerable amount of further research.
The Ministry of Science and Technology and the BMRC, in consultation with other stakeholders, should be
instrumental in defining the research agenda for the public health response to arsenic contamnination and
assist in identifying suitable national and international research institutes to conduct such research.
This section suggests some of the important public health questions that need to be answered by research.
In some cases, the needed research is already being conducted. In other areas, however, the research has not
yet commenced. In this document the research agenda is fairly comprehensive to ensure that the discussion

in connection with this paper will cover all or most of the unknown areas. The actual research agenda of a
follow-up project is likely to be reduced at the time of detailed plannng in view of time, capacity and budget
restraints. Some of these topics may be taken up under the aegis of MOHFW through the establishment of
an international expert panel to issue requests for research proposals and make decisions about funding. As
part of the research agenda may be considered as international public goods, this would warrant
international funding.. Further, MOHFW can take an important role in ensuring that 1) the necessary
research is completed, 2) efforts are not needlessly duplicated, and 3) results are properly interpreted,
disseminated, and utilized for policy-making and planning.
The following page lists the research questions that should be addressed, categorized broadly under three
areas. Appendix 6 treats the subject of research needs more elaborately, and suggests how each question
could be studied.
Health Effects
a) How many people are now apparently affected by arsenic, and where are they living?
b) What is the incidence of skin lesions attributable to arsenic? What is the latent period?
c) What percentage of those with skin lesions will develop other arsemc-related health outcomes,
including skin cancer, internal cancers, cardiovascular disease, et cetera? What percentage of those
without skin lesions will develop these outcomes? What are the latent periods?
d) Does arsenic intake by pregnant women affect pregnancy outcomes?
e) What is the dose-response relationship (with dose expressed in terms of both arsenic concentration and
duration of exposure)?
f) How do the risks of drinking water contaminated with arsenic compare with the risks of drinking
surface water contaminated with pathogenic bacteria?
Susceptibility
g) How is susceptibility modified by factors such as nutritional status, general health status, infections, et
cetera, which have a potential for intervention?
h) How is susceptibility modified by factors such as age and sex, which don't have a potential for
intervention?
Effectiveness of Treatment
i) What is the effectveness of treatment with anti-oxidant vitamins (A, E, & C) in reversing skin lesions?
j) What is the effectiveness of selenium (and other micronutrients) in reversing skin lesions?

k) What is the effectiveness of increased protein intake in reversing skin lesions?
1) Is chelation therapy useful in long-term exposure?
m) What is the effectiveness of salicylic acid and other skin lotions in reversing skin lesions?
n) What is the impact of providing arsenic-free water in reversing skin lesions?
o) What is the impact of treating skin lesion patients on the incidence of other health outcomes?
3.5 WATER TESTING AND CASE MANAGEMENT (LINKED TO EACH OTHER)
It is important to note the close relationship required between those responsible for patient counseling and
those charged with provision of alternative water supply. Because provision of clean water is the
responsibility of DPHE, testing of water for arsenic naturally falls within their jurisdiction.
But as provision of clean water is the first line of treatment for arsenic-related diseases, the current lack of
capacity for testing and provision of arsenic-free water presents a problem for provision of appropriate
health care. Compliance with medical recommendations can be difficult to secure in the best of
circumstances. If the "treatment" prescribed, i.e. an alternative water source, is not available when required,
then good compliance cannot be achieved and institutional credibility will suffer.
Thus, although testing water is not primarily the responsibility of the health sector, health interventions
(such as case-finding, counseling and treatment) will have limited success unless they are linked to testing
water. This warrants capacity-building within the health sector to test water from individual tube wells, as
well as inter-sectoral partnerships. Health workers advising patients to test and drink only safe water would
be meaningless if neither the health workers themselves nor the community members possess the means to
do this. Therefore, MOHFW needs to work actively with relevant other organizations to ensure that its
workforce is trained in water testing (just as the water-testers from the DPHE need to be trained to recognize
skin lesions caused by arsenic) and that adequate numbers of accurate field test kits are made available to
the public. As a bare minimum, MOHFW must ensure that all water sources within their facilities are free
of arsenic.
Additionally, in order to perform robust health research as well as quality control assessments of field kit
testing, laboratories able to conduct accurate, quantitative water testing must exist. The government must
ensure that a sufficient number of laboratories throughout Bangladesh become able to perform dtis function.
There are several laboratories in Bangladesh that can perform quantitative laboratory analysis at present.
(Appendix 7 presents details related to water-testing). These laboratories should be encouraged and
supported with training and reference materials so that they can become certified reference laboratories
according to WHO standards.

3.6 PROVIDING SAFE WATER
Clearly, finding affordable water sources that are safe in terms of both arsenic and microbial organisms, as
well as acceptable to user communities, is the ultimate and permanent solution to the problem. Such sources
may include shallow tube well water that has been treated to remove arsenic by any of several technologies
as well as alternative sources such as treated surface water, rain water, dug wells, deep tube wells, et cetera.
There are pros and cons for each option. For example, shallow tube wells with hand pumps provide
pathogen-free water near individual houses, but large numbers of these - up to 80-90 % in some coastal areas
- exceed the Bangladesh arsenic standard of 50ppb. Deep tube wells are much less likely to have arsenic
contamination, but cost much more to install and are therefore unlikely to be available to individual
households. Shallow ring wells are cheaper, but provide lower quality water and may dry up mid-dry
season. Rainwater is a good alternative in the monsoon, but requires large storage capacity if the full dry
season is to be bridged. Lesser investment in storage provides up to 250-280 days of drinking water. Surface
water and ponds are contaminated with pathogens and possibly even pesticides, and also lose water in the
dry season.
It should be recognized that solutions are needed for both the short and the long term, and these solutions
may not be identical. The best alternative may vary from area to area, and local communities should be able
to choose their own solutions from among available options. Water security, i.e. the sustained availability of
sufficient quantities of safe water for drinking, washing and for other domestic uses, will remain the concern
of the women in the household. Therefore the active participation of women and sufficient consideration of
their concerns are critical to the development of best options for the communities and individual
households.
It is very important that the available arsenic removal methods be rigorously tested for effectiveness and
acceptability using clearly defined criteria. The highest priority should be given to testing treatments
already being used. The Ontario Center for Environmental Technology Advancement (OCETA) has
undertaken to test arsenic removal methodologies with rigorous evaluation criteria; the same should be
done for alternative water sources. Both laboratory and real-world trials are required. Results from these
trials should be widely disseminated and used to inform both provider and public education programs.
Ultimately, information as well as materials for arsenic removal technology and for establishing alternative
water sources must be available at an affordable price at the village level. This will likely require multiple
distribution systems including one or more government agencies, NGOs, and the private sector. The private
sector should be encouraged and provided with incentives to start production and distribution of arsenic
removal technologies. This will further require pricing policy and safeguards in place to ensure that the
poor also have access to clean water. Key issues to be addressed are private sector capacity as well as how
and where needed capacity may be developed.
0h

Appendix 1
Health Problems Due to Chronic Exposure to Arsenic contaminateddrinking water
The health effects that result from the ingestion of arsenic-contaminated drinking water manifest themselves
gradually after a long latent period (5-15 years).4 "18 A major increase in the number of cases of arsenic-
caused diseases can be projected into the future if the population continues to drink arsenic-contaminated
water. Probable future effects include skin lesions, diabetes mellitus, chronic bronchitis, hypertension,
cirrhosis of the liver, peripheral neuropathy, and cancers of the lungs, bladder, kidney, skin and possibly
liver. In fact, arsenic may have a negative impact on every organ in the body.
Non-cancerous Conditions
Skin lesions
Hyperpigmentation, depigmentation and keratosis are the commonest forms of skin lesions attributed to
arsenic poisoning. The latent period (i.e., the time from first exposure to manifestation of disease) for these
lesions, in particular keratoses, is typically on the order of 10 years. 1 The shortest latent period described in
the literature (with high exposure) is 2.5 years.19 The rapidity with which the skin lesions appear is believed
to be dose-dependent. 6
Black-foot disease
Arsenic is a major risk factor for what is called "black-foot disease", peripheral atherosclerosis resulting in
dry gangrene and spontaneous amputation of affected extremities. The disease was named for its most
striking clinical feature-black discoloration of the feet or hands. The cause of black-foot disease was not
immediately clear, and the first case report, in 1954, attributed this disease to potassium intoxication. 20 The
disease was endemic in the south-west coastal region of Taiwan, where residents had used arsenic-
contaminated water for more than 80 years. Patients with black-foot disease often had arsenic-induced skin
lesions, e.g., hyperpigmentation, hyperkeratosis, and skin cancers, and they often died of cancer of the
bladder, liver, lungs, kidney, and prostate, as well as from circulatory diseases. 21'22' 23,24' 25' 26 The male-to-
female ratio was 1.5:1, although a majority of the female patients were younger than the males.2 3
18 Smith AH, Rahman M. Arsenic in drinking water: a public health point of view. Medicine Digest, 2001.
19 Saha KC. Chronic arsenical dermatoses from tube-well water in West Bengal during 1983-87. Indian Journal ofDermatology, 1995, 40:1-12.
20 Kao TM et al. Spontaneous gangrene and chronic potassium poisoning. Presented at the 46th Annual Meeting ofthe Formosan Medical Association, Taipei, Taiwan, 1954.
21 Chen CJ et al. Malignant neoplasms among residents of a Blackfoot Disease-endemic area in Taiwan: high-arsenicartesian well water and cancers. Cancer Research, 1985, 45:5895-5899.
22 Tseng WP et al. Prevalence of skin cancer in an endemic area of chronic arsenicism in Taiwan. Journal of the NationalCancer Institute, 1968, 40:453-463
23 Ch'i IC, Blackwell RQ. A controlled retrospective study of blackfoot disease, an endemic peripheral gangrenedisease in Taiwan. American Journal of Epidemiology, 1968, 88:7-24.

Appendix 1Health Problem due to Chronic Arsenic Exposure
Other non-cancer forms of presentation
Relationships showing dose-response patterns between ingested arsenic and diabetes mellitus and
hypertension, respectively, have been reported from Taiwan, Sweden, and Bangladesh. 2 7' 2 8' 2 9'3 0 Animal
experiments and other epidemiological studies on humans have also raised the possibility that arsenic
exposure may have serious effects on reproductive outcomes.
Other clinical manifestations of chronic ingestion of arsenic-contaminated drinking water include
gastroenteritis, weakness, conjunctival congestion, edema, portal hypertension, bronchitis, and
hepatomegaly. 31 Additionally, problems such as dermatitis, bronchitis, and nasal septum perforation have
been observed among those exposed to arsenic through inhalation, rather than ingestion. 3 2
Cancerous Conditions
Skin cancer
In 1887, Hutchinson first described skin cancer in patients treated with arsenic-containung medication for
psoriasis and other skin conditions.3 3' 34 A characteristic sequence of skin effects caused by chronic arsenic
exposure seems to involve initial hyperpigmentation, followed by the pre-cancerous condition keratosis,
and, finally, skin cancer (although progression through all of these stages is not necessarily inevitable). The
knowledge base is weak regarding latent penods for arsenic exposure through drinking water and skin
cancer (as well as for other malignancies). The lifetime risk of skin cancer from the intake of just 1
microgram / kilogram body weight/ day (roughly 1 liter/ day at 50 ppb arsenic content) has been estimated
24 Tseng WP et al. A clinucal study of blackfoot disease in Taiwan, an epidemic penpheral vascular disease. Memoirs ofthe College of Medicine National Taiwan University, 1961, 7.1-17.
25 Tseng WP. Blackfoot disease in Taiwan: a 30-year follow-up study. Angiology 1989, 40:547-558.
26 Tseng WP. Effects and dose-response relationships of skin cancer and blackfoot disease with arsenic. EnvironmentalHealth Perspectives, 1977, 19:109-119.2 7 Rahman M. Nonmalignant Health Effects of Arsenic Exposure. Link6ping University Medical Dissertation. No612, Linkoping, Sweden: 1999.
28 Rahman M et al. Diabetes mellitus associated with arsenic exposure in Bangladesh. American Journal of Epidemiology,1998, 148:198-203.
29 Rahman M et al Relations between exposure to arsenic, skin lesions and glucosuria. Occupational and EnvironmentalMedicine, 1999, 56:277-281.3 0 Rahman M et al. Hypertension and arsenic exposure in Bangladesh. Hypertension, 1999, 33:74-78.
31 Guha Mazumder DN et al. Non-cancer effects of chronic arsemcosis with special reference to liver damage. In:Abernathy CO, Calderon RL, Chappel WR, editors. Arsenic: exposure and health effects, pages 112-123. London: Capman andHall, 1997.
32 Pershagen G, Vahter M. Arsenic: a toxicological and epidemiological appraisal. SNV PM 1128. The nationalSwedish Environment Protection Board, Stockholm, 1979
33 Hutchinson J. Arsenic cancer. British Medical Journal, 1887, 2 1280-1281.
34 Hutchinson J. On some examples of arsenic-keratosis of the skin and of arsenic-cancer. Transactions of the PathologicalSociety of London, 1887, 39 352-363.

Appendix 1Health Problemn due to Chronic Arsenic Exposure
to range from 1/1000 to 2/1000.35 It is noted that the actual average quantity of water ingested per person
each day in Bangladesh may be higher than 1 liter because of the hot weather.
Based on many studies in Taiwan, Chile, Argentina, and China, it is almost certain that increasing incidences
of various cancers will occur in Bangladesh. There may be susceptibility differences between the populations
of Taiwan and Bangladesh that only time and further studies will reveal. Based on present knowledge from
many different populations in the world, there is every reasons to expect large numbers of skin cancer cases
to result in Bangladesh, in particular if arsenic exposure continues.
Kidney and bladder cancer
Dose-response relationships between levels of arsenic in drinking water and mortality from bladder cancer
and, to a lesser extent, from kidney cancer and have been described extensively in a population in
Taiwan.22' 3 6 ,37 Men who consumed water with 800 ppb arsenic were 28.3 times more likely to die of bladder
cancer than unexposed men; and exposed women were 65.4 times more likely to die of bladder cancer than
unexposed women. Clear indications of urinary tract cancer associated with arsenic ingestion were also
seen in a large population exposed to arsenic in Chile, where the region experienced standardized mortality
ratios of 6.0 - 8.2% due to bladder cancer.3 8 Additional evidence comes from Argentina and Japan as well
as among the users of Fowler's solution (a medicinal, arsenic-containing solution). 39 ,40,4l142
Lung cancer
It is well known that lung cancer may be caused by the inhalation of inorganic compounds of arsenic, but
extensive evidence now shows that increased risk of lung cancer is a major consequence of ingestion of
arsenic in drinking water. This evidence comes in particular from major studies in Taiwan and Chile, but
additional support for the conclusion that lung cancer is the major fatal cancer outcome from ingestion of
arsenic comes from studies in Japan and Argentina.31 ,3 7' 38
35 United States Environmental Protection Agency. Special report on ingested inorganic arsenic: skin cancer; nutritionalessentiality. Washington, DC: EPA625/3-87/013,1988.
36 Chen CJ et al. Arsenic and cancer (letter). Lancet, 1988, 1:414-415.
37 Chen CJ et al. Cancer potential in liver, lung, bladder and kidney due to ingested morganic arsenic in drinking water.British Journal of Cancer, 1992, 66:888-892.
38 Smith AH et al. Marked increase in bladder and lung cancer mortality in a region of Northem Chile due to arsenicin drinking water. American Journal of Epidemiology, 1998, 147:660-669.
39 Hopenhayn-Rich C et al. Bladder cancer mortality associated with arsenic in drinking water m Argentma.Epidemiology, 1996, 7:117-124.
40 Hopenhayn-Rich C et al. Lung and kidney cancer mortality associated with arsenic in drinking water in Cordoba,Argentina. International Journal of Epidemiology, 1998, 27:561-569.
41 Smith AH et al. Cancer risks from arsenic in drinking water. Environmental Health Perspectives, 1992, 97:259-257.
42 Smith AH et al. Cancer risks from arsenic in drinking water: implications for drinking water standards. In:Proceedings of the Third Intemational Conference on Arsenic Exposure and Health Effects, 12-15 July 1998, San Diego,pp 191-200. Oxford: Elsevier Science, 1999.

Appendix 1Health Problem due to Chronic Arsenic Exposure
Liver cancer
Studies in Taiwan have found a connection between arsenic in water and elevated death rates due to liver
cancer. 31 However, this effect has not been reported in other major populations exposed in Chile and
Argentina. 16
Cancer mortality
The main causes of death due to chronic ingestion of arsenic in drinking water are internal cancers, as skin
cancers due to arsenic are not usually fatal if appropriate and early treatment is provided. In Taiwan, highly
exposed populations drinking water containing an average of 800 ppb of arsenic had relative risk estimates
for bladder cancer on the order of 30-60.37,43 In Chile, 5-10% of all deaths of those over the age of 30 in the
exposed population were attributable to arsemc-caused internal cancers, in particular bladder and lung
cancer. 39 In Argentina, where exposure levels were lower than in Taiwan and Chile, a mortality study in the
arsenic-exposed region of C6rdoba showed increased risks of bladder and lung cancer among both men and
women.4 0 ,41
Grading of Arsenic-Related Conditions
WHO, Southeast Asia Region, has undertaken to devise a grading scheme for arsenic-induced skin lesions
as part of standards for case definition, detection, reporting, and management. A draft scheme should be
available in late 2001, with field testing to begin in early 2002.
The various health effects associated with arsenic exposure have been categorized into a pre-climcal
(undetectable) stage, and primary, secondary and tertiary "stage" categories by physicians at NIPSOM 4 44
and this scheme has been slightly modified by the ICDDR,B (Table 3). The modification of the NIPSOM
scheme added diabetes mellitus, as studies suggested that arsenic exposure contributes as a risk factor for
diabetes and that diabetes may occur in spite of absence of skin lesions. In this scheme, the primary and
secondary conditions tend to be non-malignant, while the malignant effects manifest themselves in the
tertiary "stage". However, it is important to note that affected individuals may not necessarily have all
manifestations of a certain category, and the timing of different signs and symptoms may vary. Further, an
individual may manifest signs and symptoms of a more advanced category stage without passing through
signs and symptoms of earlier categories. Thus, while this scheme may be useful for assessing the seventy
of a patient's present condition, it does not necessarily indicate the degree of past exposure to arsenic,
medical history, or prognosis.
43 Chen CJ, Wang CJ. Ecological correlation between arsenuc levels in well water and age adjusted mortality frommalignant neoplasms Cancer Research, 1990, 50:5470-5475.
44 Khan AW, Ahmad SA. Arsenic in drinking water. Health effects and management. A training manual. Dhaka:AM Department of Occupational and Environmental Health. NIPSOM, 1997.

Appendix 1Health Problem due to Chronic Arsenic Exposure
Estimating the Burden of Arsenic-Related Conditions
Despite the very limited case-finding efforts in Bangladesh, already more than 7000 patients with symptoms
related to arsenic poisoning have been identified (some estimates indicate as many as 100,000 cases of skin
lesions in Bangladesh caused by arsenic1 . Current risk estimates in the international literature are mostly
based on data from Taiwan or other localities, where health effects of arsenic exposure through drinking
water have been studied for a long time. Some of these estimates are based on ecological comparisons, with
obvious weaknesses from a methodological point of view. Scientists have modeled cancer risks based upon
observed data from around the world. The U.S. National Research Council estimated cancer risk (for all
cancers combined) on the order of 1 in 100 for arsenic exposure levels around 50 ppb of water.16 Smith et
al. estimated that based upon the current standard of 50 ppb, the lifetime risk of dying from cancer of theliver, lung, kidney or bladder, from drinking 1 L/day of water could be as high as 13 per 1000 persons.4 2 '4 3
Using the same method, the risk estimate for 500 ppb of arsenic in drinking water would be 13 per 100
persons. Applying this risk to a conservative estimate of 20 million people in Bangladesh exposed to arsenic-
contaminated drinking water, the present generation may suffer from 200,000 - 270,000 cancer cases,
attributable arsenic poisoning. Evidently, the estimate of future cancer cases will be correspondingly far
greater if the higher exposure figures of 35-77 million are used - if they live long enough and if exposure is
not rapidly reduced.
While there may be differences in susceptibility to arsenic health effects, 36'4 5 it is remarkable that dissimilar
populations in Taiwan, Chile, Japan, and Argentina have clear increases in risks of several cancers. There is
no basis to think that the Bangladeshi people would not have similar susceptibilities. In fact, the widespread
malnutrition in the country would lead one to expect, if anything, that the risks might be higher than
elsewhere in the world.
The impact of arsenic extends beyond the immediate health effects to extensive social and economic
hardship, which affect the poorer segments of the population disproportionately. Factors such as increased
cost of health care, loss of productivity and income, and social exclusion because of visible skin lesions are
just some of the indirect effects that need to be studied more carefully to obtain a more complete picture of
the overall impact of arsenic contamination of drinking water.
45 Agency for Toxic Substances and Disease Registry. Toxicological Profile for Arsenic (Update). United StatesDepartment of Health and Human Services, 2000. o

Appendix 1Health Problem due to Chronic Arsenic Exposure
Table 3. Categories, signs, symptoms and descriptions of various arsenic-related health problems
Category Symptom /Sign /Condition Description
Primary Melanosis (spotted, diffuse) Darkening or blackening of skin color. Small black
spots or diffuse black patches particularly over
the trunk and back
Keratosis (spotted, diffuse) Skin becomes hard and rough, especially on
palms and soles
Conjunctivitis Reddening of eyes
Bronchitis Inflammation of the lower respiratory tract
Gastroenteritis Nausea, vomiting and loose motions
Diabetes mellitus Abnormal blood sugar levels, due to insulin deficiency
Secondary Leucomelanosis Black and white spots on skin
("raindrop" pigmentation)
Hyperkeratosis Rough nodules on palm and sole
Non-pitting edema Swelling of leg
Peripheral neuropathy Distal numbness, tingling, cold, weakness,
impaired sensations
Hepatomegaly Increased size of liver
Nephropathy, early Early kidney disease.
Tertiary Gangrene Necrosis of limbs leading to amputation
Nephropathy, late Acute tubular necrosis, cortical necrosis and
renal failure
Cancer Cancer of the skin, urinary bladder and lungs
Liver failure
Source: ICDDR,B modification of staging scheme proposed by NIPSOM

Appendix 2
RESTRUCTURING OF BANGLADESH ARSENIC MITIGATION ANDWATER SUPPLY PROJECT (BAMWSP)
The following is an extract from the documentation under preparation for the restructuring of BAMWSP
(IDA Credit 3124)
RECONSTRUCTION OF BAMWSP: SALIENT POINTS
* BAMWSP will be implemented following a program approach.
* Partnership will be built with relevant government agencies.
* The rural component of BAMWSP will be implemented through effective involvement of the grass-root
level local government and the community with technical support from DPHEE.
* Small/Medium/Large NGOs will be contracted in to provide specific capacity support to the local
government and community.
* The PMU of BAMWSP will be strengthened by reorganizing the project management structure in line
with the reoriented task and responsibility.
* Need for specific technical assistance will be identified and taken on a 'as and when required basis'.
* Donors may put their committed TA resource into a common pool from where the required TA inputs
will be funded.
* BAMWSP will coordinate the field/implementation level activities while the Local Government
Division will do the overall coordination including inter-ministerial and multi-sectoral coordination.
* It is expected that a transitional process of about one year will allow all interested donors and
development partners to coordinate their efforts will that of BAMWSP and all development partners
will follow a common protocol.
* The Local Government Division under the leadership of the Secretary, Local Government Division willprovide strategic guidance; inter ministerial / cross sectoral coordination and facilitation to the
implementation of over all activities of arsenic mitigation.
* The Local Government Division is aimed at entering into partnership agreement for the agreed priority
tasks by the end of August and bringing on board consultants for most critical technical assistance in an
expeditious manner.
It is expected that the interested and potential donors will coordinate their efforts with that of BAMWSP andafter a certain period of time all development partners will be following a common protocol for arsenicmitigation.

Appendix 2Restructuring of BAMWSP
* Screening of tube wells (Rural & Urban) * Primary Identification of patients * Communication
* Health Component * Hydro-geological Issues * Technology Validation * R & D * Mitigation * MIS
BAMWSP (1998-2001)
Partnership with Partnership with Partnership withGSB for BCSIR Technology Unicef/Ministry of
Hydro geological verification Information forIssues Issues communication
* Screening of tube wells * Primary Identification of patients- * Mitigation * MIS * Coordination
Partnership with Partnership with Partnership withMinistry of Health ITN Others asfor health treatment for R & D and necessary
of patient technical matters
B A M W S P (July 2001 - June 2002)
- National Arsenic Mitigation Program
July 2002
The Program Approach
Figure 1

Appendix 2Restructuring of BAMWSP
Small/ Medium NGOs National NGOs Private Firm(Providing capacity (Providing capacity (For M & E)
support to the LGIs and support to the LGIs andcommunity in screening community in screening
and mitigation) and mitigation)
* Screening of tubewelHs * Primary Identification of patients* Mitigation * MIS * Coordination
Paurashava/DPHE Local Government Local Administration(Urban Component) Institutions
BAMWSP Implementation Mechanism
(July 2001 - June 2002)
Figure: 2

Appendix 3
RESPONSE OF PARTNER AGENCIES TO THE ARSENIC CRISIS INBANGLADESH
UNICEF ACTIVITIES
UNICEF has supported a comprehensive community-based arsenic mitigation program in five upazilas in
cooperation with BRAC, Grameen Bank, DCH, and Integrated Services for Development of Children and
Mothers (ISDCM) (Table 4) and has, with DPHE, initiated several nation-wide activities and action research
projects. The national-scale activities include testing of tube wells by use of field test kits to give the first
impression of the arsenic problem as well as development and testing of a comprehensive communication
campaign through mass media. DPHE and UNICEF are currently developing the second phase of the
community based project (in 15 upazilas), with further emphasis placed on sustainability, communuty
involvement and community cost sharing. The United Nations Foundation will provide funds for three of
the upazilas in this joint undertaking with WHO, which includes a research component.
Table 4. Overview of several community based arsenic mitigation activities and identification of individuals with
arsenic-related skin lesions.
Upazila Number of Number of Number with Total Proportion with
Villages Tube wells Skin Lesions Population Skin Lesions
Jhikorgacha* 163 26,737 151 261,607 57/10,000
Sonargaon 368 25,048 252 235,607 106/10000
Kachaua 245 17,787 202 293,683 68/10,000
Bera * 170 14,407 120 284,804 42/10,000
Manikgong . 371 21,300 19 332,000 5/10,000
Activities performed by: * BRAC, v Grameen Bank, * DCH, and # ISDCM
WHO ACTIVITIES
WHO is playing an important role in the development of a technical monograph to synthesize the
knowledge on arsenic as directed by the UNACC Interagency Steering Committee on Sustainable
Development for Water Supply and Sanitation in 1998. WHO has provided technical assistance in
modifying a locally developed test kit and in framing criteria for assessing and certifying field test kits.
Finally, WHO is reviewing the scientific studies on relevant analytical techniques, environmental
contaminant levels, human exposure, toxicity, and health effects. Based on this review, WHO will update
the Environmental Health Criteria on Arsenic for the International Program on Chemical Safety 46,47 Finally,
46 World Health Organization WHO guidelines for drinking-water quality. Vol. 2, second edition, Health crmtena andother supporting information. Geneva: WHO, 1996
47 World Health Organization. Environmental health cnterna 18: Arsenic Geneva: WHO, 1981.

Appendix 3
WHO is preparing diagnostic classification for arsenic-related diseases.
ACTIVITIES CONDUCTED BY BRAC. GRAMEEN BANK, DCH, AND ISDCM.
BRAC. BRAC, one of the largest national non-governmental organizations in Bangladesh, has proven
capacities for field-level program implementation and socio-economic research, has a strong institutional
network, and has experience in training community members in testing tube well water for arsenic. In 1999,
in collaboration with UNICEF and DPHE, BRAC initiated arsenic mitigation activities in two upazilas,
Sonargaon of Narayanganj district and Jhikargacha of Jessore district. The year before, BRAC had
completed countrywide testing of tube wells that had been installed by DPHE during 1997-1998, with
assistance from UNICEF48. A total of 12,604 tube wells were tested under this project, using field kits. The
testing program in Hajiganj upazila was completed in just over a month. In Hajiganj upazila, 93% of the
11,954 tube wells tested by BRAC showed significant arsenic content. Once all tube-wells were tested, the
results were presented to communities at meetings. The communities in arsenic affected areas decided on
what alternative system to use, where the system was to be located, and committed themselves to
maintaining the system. Priority was given to villages where the arsenic problem was found to be more
widespread. When the results of field-testing by village health workers were compared with laboratory
results, 93% were consistent.
Table 5. Safe water options offered by BRAC
Option Water sources Location Families served
Pond sand filter Surface water Community 40-60
Rain water harvesting Rain water Family 1
Two chamber treated unit Surface water Community 6-10
Safi filter Ground water Family 1
Dug wells Surface water Family 1
Deep wells Ground water Community 6-10
Grameen Bank. Grameen Bank, with assistance from UNICEF and DPHE, started its testing program in 1997
in Chandpur district4 9 . The project followed an integrated approach and included four main activities:
communication about arsenic and arsenicosis; testing of all tube wells in the upazila; screening,
identification and support to arsenicosis patients; and monitoring and evaluation of alternative water
supply technologies. The technologies tested ranged from home-based solutions such as the 3-kolshi arsenic
removal filter to community-based alternatives such as the pond sand filter for treatment of surface water.
48 BRAC. Combating a deadly menace: early experiences with a community based arsenic mitigation project inBangladesh, 2000.
49 Grameen Bank. Completion report of community based arsenic mitigation project (GB-DPHE-UNICEF Project),2000.

Appendix 3
Dhaka Community Hospital. DCH completed the RAP survey financed by UNDP and WB on behalf of the
MOHFW50 . The project objective was to identify patients, test and mark all tube wells, identify and provide
the best option for arsenic free water, and follow-up on the status of patients. RAP, established in 1997, first
surveyed two hundred villages that had already been identified as having arsenic-contaminated tube wells.
These villages had a total population of 469,424. Approximately two thirds of the 32,651 tube wells had
levels of arsenic over 100 ppb. An extension of RAP was completed by June, 2000 in 300 additional villages.
Using its own resources, DCH has also completed a countrywide sampling survey of tube well water and is
presently working in collaboration with UNICEF and DPHE on arsenic mitigation activities in Bera upazila.
Integrated Servicesfor Development of Children and Mothers. ISDCM's Community Based Safe Water Supply
and Arsenic Mitigation Project was launched in 2000 with assistance from UNICEF and DPHE. Tubewells
were tested in Manikgong Sadar upazila of Manikgong district. ISDCM advocated that communities use
only safe tube well water, rainwater, and treated surface water. The project also tested technologies
including arsenic free deep tubewells, a continuous arsenic removal plant (SIDKO), rainwater harvesting,
and other household treatment units. Significant emphasis was put on women's participation and gender
equity in the project.5 1
50 Dhaka Community Hospital. Report on action research on community based arsenic mitigation project, DCH-DPHE-UNICEF Project, 2000.
51 Integrated Services for Development of Children and Mothers, Community Based Arsenic Mitigation Project m9 Manikgong Sadar Upazila, 2000.

Appendix 4BAMWSP Current Status and Priority Tasks
BAMWSP: CURRENT STATUS AND PRIORITY TASKS FOR ARSENIC MITIGATION EFFORTS
Present Status Intermediate Term Long Term
(1-2 years) (2-5 years)A Communication
A.1 Existing DPHEE/UNICEF Task Task
Communication Campaign: MoH A.1 Implementation of MoH approved A.1 Continued routine communication on
approved/ field tested; ready for communications campaign. the risks associated with arsenic
nation-wide implementation. contaminated water, accepted and
Communication campaign not yet A.2 Establish a mechanism for common approved arsenic mitigation
implemented. strategy development, implementation technologies, nutritional and behavioral
and upgrading of communication aspects.
A.3 Absence of mechanisms to share being campaigns
communication strategies & materials A.2 Regular evaluation and upgrading of
developed by various stakeholders A.3 Identify partners to implement based communication strategies reflecting
intensified communication campaign emerging knowledge and information
upon agreed strategy
Impact assessment of campaigns
Outcome
Delivery of consistent series of A.3 Outcome
messages reaching out to all affected Consistent application of sound arsenic
individuals mitigation solutions at household and
community levels.

Appendix 4
BAMWSP Current Status and Priority Tasks
Present Status Intermediate Term Long Term
(1-2 years) (2-5 years)
B Mitigation Strategy
B.1 Concept of Bangladesh Arsenic Task Task
Mitigation Trust proposed B.1 Develop/ implement an arsenic arsenic B.1 Review and refine the mandate of the
mitigation program that creates arsenic mitigation program to reflect
B.2 Government order for Upazila/Union partnerships for effective delivery of the future needs of the country
Parishad implementation focus, mitigation at community level
awaiting application Outcome
B.2 Create an atmosphere of inclusiveness, Strategically positioned entity capable
B.3 DPHE/UNICEF/WHO developed; mobilizing all resources, especially the of reacting to changes within the
implementation framework knowledge and experiences of the GOB sector.
BAMWSP, WPP and NGOs are and stakeholders, for mitigation
developing similar frameworks
B.3 Development of an entity to
B.4 Ineffective mechanisms for coordinate activities and information
disseminating arsenic mitigation associated with a sector wide approach
experiences and results for arsenic mitigation
B.5 Absence of effective coordination at B.4 Outcome
various administrative levels. Proactive program responsible for
sector wide activities associated with
arsenic in the water

Appendix 4
BAMWSP Current Status and Priority Tasks
Present Status Intermediate Term Long Term
(1-2 years) (2-5 years)
C Measurement
C.1 Ability to identify hotspots Task Task
C.1 Develop/implement a comprehensive C.1 Continued monitoring of both
C.2 Field test kits available for yes/no at strategy for determining the severity hotspot areas and the rest of
50 ppb, with high degree of of arsenic contamination in hotspot Bangladesh to determine changes in
uncertainty areas, and other potential water quality arsenic concentrations and associated
issues water quality parameters
C.3 Improved kits under development and
costly C.2 Develop/ implement a coordinated Outcome
nationwide strategy for evaluating and Creation of a database and
C.4 Limited information (gathered) reporting the overall arsenic scenario dissemination of water quality
providing incomplete contamination and general water quality issues information that can be used in the
picture and reduces proper decision decision-making process
making abilities C.3 Reliability of data generated by test
kits must be determined
Outcome
Adequate information regarding water
quality in hotspot areas for sound
interventions
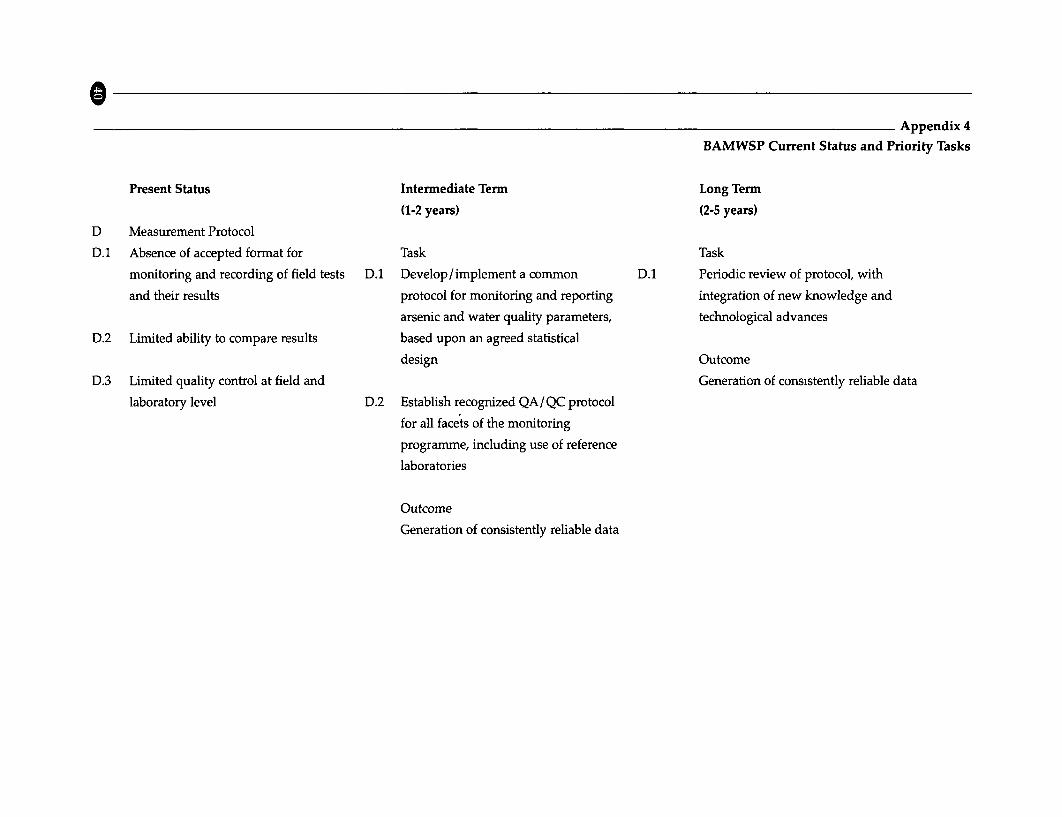
Appendix 4
BAMWSP Current Status and Priority Tasks
Present Status Intermediate Term Long Term
(1-2 years) (2-5 years)
D Measurement Protocol
D.1 Absence of accepted format for Task Task
monitoring and recording of field tests D.1 Develop/implement a common D.1 Periodic review of protocol, with
and their results protocol for monitoring and reporting integration of new knowledge and
arsenic and water quality parameters, technological advances
D.2 Limited ability to compare results based upon an agreed statistical
design Outcome
D.3 Limited quality control at field and Generation of consistently reliable data
laboratory level D.2 Establish recognized QA/QC protocol
for all facets of the monitoring
programme, including use of reference
laboratories
Outcome
Generation of consistently reliable data

Appendix 4
BAMWSP Current Status and Priority Tasks
Present Status Intermediate Term Long Term
(1-2 years) (2-5 years)
E Mitigation Options
Potential options that have been Task Task
identified as promising (with location E.1 Continue development and E.1 Monitoring and subsequent analysis
specific limitations) include (pending identification of promising mitigation of verified technologies in the field
recognized Environmental options for arsenic safe water, which
Technology Verification): will require ETV Outcome
Access to arsenic-safe drinking water
E.1 Arsenic avoidance Establish/implement a long-term
safe green wells monitoring protocol for verified
deep tube wells technologies in the field, including
surface water technologies sustained social acceptance and
(pond sand filters, dug wells) application
rain water harvesting
Outcome
E.2 Arsenic removal Access to arsenic-safe drinking water
three kolshi filter
ALCAN/BUET activated alumina
Stevens / Tetrahedron

BAppendix 4
BAMWSP Current Status and Priority Tasks
Present Status Intermediate Term Long Term
(1-2 years) (2-5 years)
F Environmental Technology Verification Protocol
Task Task
F.1 Protocols for testing and verifying F.1 Identify and mobilize GOB lead agency F.1 Functioning ETV Program within
suitable technologies are completed for registration, testing and Bangladesh, for registration, testing and
verification of arsenic mitigation verification of water treatment
F.2 Inability of current organizational set- technologies technologies
up to meet ETV requirement.
Initiate ETV Program Outcome
F.3 Many technologies in Bangladesh have ETV compliant drinking water
not been subjected to any recognized Outcome technologies that meet or exceed GOB
testing protocol Mechanism for registration, testing standards
and verification of arsenic mitigation
F.3 A properly staffed and mandated GOB technologies
agency is required to take up longer
term task
F.4 A preliminary rapid assessment has
been completed on a limited number
of technologies
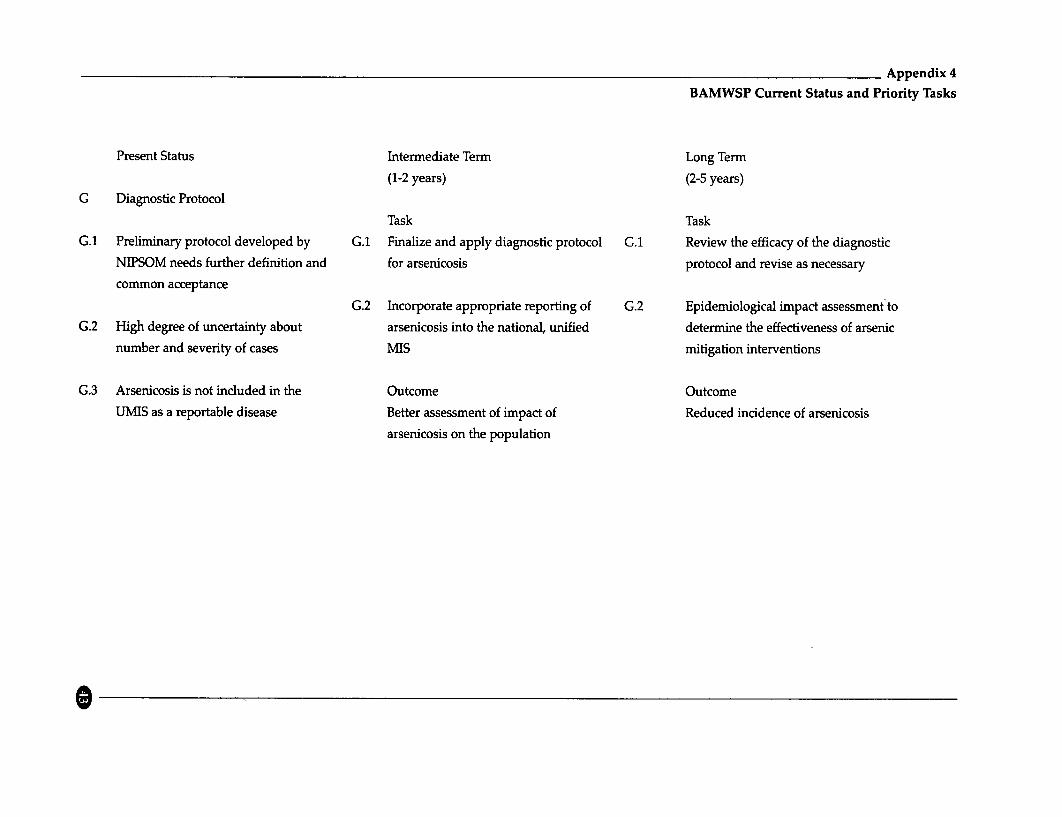
Appendix 4BAMWSP Current Status and Priority Tasks
Present Status Intermediate Term Long Term
(1-2 years) (2-5 years)
G Diagnostic Protocol
Task Task
G.1 Preliminary protocol developed by G.1 Finalize and apply diagnostic protocol G.1 Review the efficacy of the diagnostic
NIPSOM needs further definition and for arsenicosis protocol and revise as necessary
common acceptance
G.2 Incorporate appropriate reporting of G.2 Epidemiological impact assessment toG.2 High degree of uncertainty about arsenicosis into the national, unified determine the effectiveness of arsenic
number and severity of cases MIS mitigation interventions
G.3 Arsenicosis is not included in the Outcome Outcome
UMIS as a reportable disease Better assessment of impact of Reduced incidence of arsenicosis
arsenicosis on the population

Appendix 4
BAMWSP Current Status and Priority Tasks
Present Status Intermediate Term Long Term
(1-2 years) (2-5 years)
H Patient Management Protocol
Task H.1 Task
H.1 No known treatment regime for H.1 Expert consultation regarding Established protocol for treatment
arsenicosis treatment options for individuals and/or relief for individuals suffering
suffering from the effects of prolonged from the effects of prolonged exposure
H.2 Nutritional supplements such as exposure to arsenic to arsenic
Vitamins and Spirulina have been
proposed, but have no proven H.2 Develop/ implement patient H.2 Monitoring effectiveness of treatment
scientific basis. Some local research management protocol for all stages of protocol
on-going (NIPSOM-Columbia) the disease
H.3 Identify potential avenues of research
H.3 Agreed protocol for patient Identify potential avenues of research into the effective prevention and/or
management needs urgent into the effective prevention and/ or treatment of arsenicosis
development treatment of arsenicosis
Outcome
Outcome Application of recognized patient
Develop and identify tools for patient management regime for arsenicosis
management

Appendix 4
BAMWSP Current Status and Priority Tasks
Present Status Intermediate Term Long Term
(1-2 years) (2-5 years)
I Community Health Aspects
Task Task
I.1 Negative social consequences for 1.1 Develop/implement communication I.1 Review and enhance community based
patients strategy to increase understanding of initiatives focused upon addressing
the social factors associated with arsenicosis issues
I.2 Economic and social impact to arsenicosis within the family and
individuals and families community I.2 Provide support to communities
impacted by arsenicosis
1.3 Increased stress on health service 1.2 Develop / implement community based
delivery system support mechanisms for providing Outcome
relief to individuals, organizations and Programs to strengthen community
1.4 Deterioration of socio-cultural and institutions actions focused upon socio-cultural
organizational capacity of the factors impacted by arsenic
community Provide information to impacted
people regarding potential options and
I.5 Increased mental anguish due to develop/implement mechanisms
inability to act allowing for communities to act.
Outcome
Community awareness of arsenicosis
issues and greater community
involvement
Q

Appendix 4
BAMWSP Current Status and Priority Tasks
Present Status Intermediate Term Long Term
(1-2 years) (2-5 years)
J Capacity DevelopmentTask Task
J.1 Lack of program direction has J.1 Identify /develop/implement specific J.1 Develop/implement a strategy for
inhibited the effectiveness of capacity capacity development programs with maintaining level of skills and
development activities suitable Bangladesh counterpart knowledge within Bangladesh
agencies and organizations
Outcome
J.2 Coordinate activities and information Institutions and organizations with an
regarding all partner activities, enhanced skill set.
developing/ implementing mechanisms
for exchange of information and
personnel, and provide avenues
through which training of qualified
personnel can be undertaken
Outcome
Transfer of knowledge, technology and
skills to Bangladesh entities

Appendix 5
QUESTIONS TO BE ANSWERED THROUGH PUBLIC INFORMATIONCAMPAIGNS
The essential information that should be available to everyone includes:
What is arsenic and why is it important?
What are the health risks of arsenic and how can they be prevented?
Note: Skin manifestations of chronic arsenic exposure should be widely explained along with information
on what they are not (i.e. leprosy, contagious, hereditary, or a curse). People should be advised to seekmedical attention if they have signs of arsenic-related diseases, and especially if they have signs of skin
cancer.
It is vitally important that people understand that there is limited knowledge about any treatment and that
the best safety measure is to drink only uncontaminated water. They should know that there is probably a
relationship between the extent of health damage and the amount of arsenic exposure (both in terms of
length of time they have been drinking contaminated water and the level of contamination in that water),
but that the extent of health risks may also be determined by other factors and that not everyone drinkingthe same water is necessarily affected to the same degree. People should understand that the presence or
absence of skin lesions does not necessarily indicate the likelihood of developing more severe health
outcomes, but that stopping exposure will markedly reduce the risk of future disease.
If future research indicates that some groups are more likely than others to be affected (e.g. pregnant women,
children, et cetera), then education messages should be revised to include this new information. Similarly,
messages should be revised as information about effectiveness of treatments becomes available.
How can I know if my tube well is contaminated?
Note: Information on water sources that are most likely to be contaminated, where to obtain testing kits and
how to test, parts of the country that are most likely to be contaminated, and frequency of testing requiredmust be communicated nationally.
What alternatives do I have if my tube well is contaminated?
Note: The presently known effective options must be widely communicated along with the considerationsinvolved in making a choice between those options. These include both water treatment options andalternative water source options; and both of these include household-level and community-level options.
When results from the OCETA trial of water treatment methods are available, there will be updated andmore specific information to communicate in this regard.
People must also be advised that they should not revert to using surface water unless they can consistentlytreat the water to remove bacterial pathogens.
What is GOB (in partnership with other agencies) doing about the arsenic problem?

Appendix 6Public Health Research Needs
ARSENIC CONTAMINATION OF DRINKING WATER INBANGLADESH: PUBLIC HEALTH RESEARCH NEEDS
The research recommendations have been classified under three broad areas, and within each area, specific
questions are proposed and elaborated upon. At the end of this appendix, Table 6 summarizes the research
activities that should be undertaken in the near term, middle term, and long term.
1.1 Health Effects of Arsenic Contamination in Bangladesh
Importance
There is very little information available on the extent to which people are now showing health effects from
arsenic, and it is not yet possible to make sound projections regarding the sizes of the anticipated epidemics
of skin cancer and other health outcomes. Information is needed to direct current mrtigation and treatment
activities toward those who are most affected, and to put in place programs to develop health system
capacities for the future.
Virtually all case identification efforts to date have focused solely upon skin lesions (areas of hyper- and
hypo-pigmentation and hyperkeratoses) as the only outcome of interest. This focus is sensible because these
skin lesions are both characteristic of long-term arsenic exposure and relatively easy to identify, i.e. diagnosis
can be made without biopsies or other medical and laboratory tests. However, these lesions are generally
not of medical significance by themselves (although there are anecdotal reports that hyperkeratosis is a
stigmatized condition that leads to social isolation and loss of work, marriage and school opportunities.)
Although severe hyperkeratosis can be painful, it cannot be assumed that those with skin changes will
develop important health outcomes such as cancer, et cetera, only that there may be an increased risk of such
development. Similarly, it cannot be assumed that those without skm lesions will not develop important
health outcomes. Thus, pigment changes should be seen as markers of arsenic exposure that indicate - but
do not prove - the possibility of other, more severe conditions. In other words, studying the prevalence and
incidence of skin lesions is a useful place to start, but that effort alone cannot describe the full picture of
arsenic's effects on health in Bangladesh.
Specific questions addressed in this section and specific recommendations
(a) How many people are now apparently affected by arsenic, and where are they living?
The percentage and distribution of the exposed population that has developed health outcomes from arsenic
is not fully known. This is partly because case-finding activities have been extremely limited (only done in
some areas, and cases only sought in households identified as using arsenic-contaminated water based on
imperfect water testing), and partly because case-finding activities have focused exclusively on
dermatological signs (although some individuals likely develop other diseases before, or without,
dermatological signs).

Appendix 6Public Health Research Needs
Although water testing and mitigation efforts should not be held up pending the work below, estimating thepercentage and distribution of those affected would be useful for:
* determining higher and lower priority areas for mitigation and treatment efforts - ideally, thesedecisions will be based on health outcomes, for which water testing is an imperfect proxy (especiallywhen water testing is qualitative rather than quantitative).
o planning for health systems development (both physician training and siting clinics where needed).
* identifying appropriate populations for study to answer other health-related questions (below)
In the near term, a comprehensive study of the population for signs and symptoms appears infeasible dueto the need to train an enormous number of local health care providers (or others) to carry out the work.Another choice would be a population-based, stratified, cluster survey. Ideally, strata would reflectwatershed systems as well as political boundaries. Within each selected cluster, every individual would beexamined by trained individuals for arsenical skin lesions. It would not be feasible to perform thoroughexams for other health outcomes in a national survey unless mobile medical examination units containingfacilities for storing samples, performing biopsies, et cetera, could be developed. To make the survey mostworthwhile, data on nutritional status, general health status, water quality (including quantitative arsenicmeasurement), should also be collected. Developing and carrying out such a survey is a complex task. Itwould require participation by those most expert in the hydro-geological situation of Bangladesh, a surveysampling expert, epidemiologists, and interviewers fluent in Bangla and well-trained in interview methodsand the recognition of arsenical skin lesions. The survey would be costly to perform but should beconsidered in the near term because of the valuable information it would provide. If it is determined thatthe project is too expensive, it can be deferred until the middle term and prioritization decisions formitigation programs can be made upon the basis of the BGS and other results. (For operational purposes itshould be remembered that the RAP project demonstrated that, in a limited area, it was possible to identifythe most affected villages and proceed to intervention).
In the middle term, it would be cost-effective to piggy-back a survey onto another population-based studythat will occur in any case, because adding a few items to an existing survey has a low marginal cost. TheDemographic and Health Survey (DHS) would serve this purpose well. The DHS is a periodic, population-based survey of women of reproductive age. It could be expanded to include the data items recommendedabove. Ordinarily conducted every 3 years, the next iteration of this survey will occur in fall, 2002 if the 3-year schedule is adhered to.
In addition, as NGOs and government agencies visit each upazila and village in turn, prevalence figures canbe determined for localized areas by direct, active case identification. For this method to be reliable, the caseidentification must be performed much more rigorously than it has been to date. Thus far, a number oforganizations have incorporated limited case-finding into their outreach activities, typically by querying orexamining individuals whose well water tests positive by the Merck kit. These organizations will thenreport a number or percentage affected among those they examined. Similarly, some organizations haveestimated the number affected by reporting the number of people who present themselves for treatment.These estimates are flawed for several reasons, to wit:

Appendix 6Public Health Research Needs
- in outreach situations, only those using water containing arsenic >100 ppb (Merck test kit limits) have the
opportunity to be included in the numerator or denominator. However, the Merck kit cannot identify all
who have been exposed to toxic amounts of arsenic.
- further, m outreach situations, not all are willing to admit to having signs of arsenic-related diseases
- similarly, in clinical situations, only those presenting themselves for medical treatment are counted in the
numerator
- in both outreach and clinical situations, the denominator (all persons who drink water in the locality) is
usually not readily available and is not collected by the investigators
To improve estimates, it is recommended that when outreach efforts are made, all individuals in the outreach
area should be examined for skin lesions, regardless of the water test result. This should be done because
field test kits do not give precise results, as well as because their limit of detection is 100 ppb (well above the
cut point that is expected to be associated with health outcomes). This method is known as active case-
finding. Passive case-finding, i.e. counting cases who present for treatment, should not be relied upon to
make prevalence estimates because it is likely that a great number of people with signs and symptoms will
not seek clinical care.
Ideally, where feasible (based on political and social considerations, confidentiality concerns, and skills of
the outreach staff), health findings should be recorded on a standardized form that includes the individual's
name, age, sex, address, location (determined by Geographic Information System localization), water source,
time using water source, water test method, water test date, water test result, and extent and stage of skin
lesions (using internationally recognized staging criteria). Both those with and without skin lesions shpuld
have information recorded. At a minimum, age, sex, and water information should be recorded for dvery
individual so that reliable denominator information is had. DPHE is developing a scheme for uniquely
numbering each tube well in Bangladesh, and the unique number should be used in this and all resAarch
activities.
Because new cases will occur, existing cases may improve upon provision of safe water, and arsenic levels
in well water may change over time, ongoing surveillance should be instituted over the long term to monitor
the situation. The optimal schedule for repeat examinations is uncertain, but every 2 years might be
advisable to begm with. These skin examinations can take place regardless of whether the government
maintains responsibility for testing water. Locally-based health workers can be trained to identify and
measure the extent of arsenical lesions.
If records can be kept by name, and if village health workers can be trained to make accurate and objective
measurements, then rates of incidence and regression can be calculated from repeat examinations in the
same site. In addition, if records can be kept by name, it will be possible to create a registry of patients who
can be contacted in the future to collect data on long-term health outcomes, or who can be contacted to
participate in clinical trials.

Appendix 6Public Health Research Needs
Finally, the disease surveillance forms currently utilized by clinics and hospitals should be revised to include
cases of hyperkeratosis and arsenic-related skin cancer.
(b) What is the incidence of skin lesions attributable to arsenic? What is the latent period?
A measure of incidence as well as prevalence is important for projecting future treatment needs. To
determine incidence as well as prevalence from the survey described in (a), a structured interview should
contain items regarding when each household began drinking tube well water and items regarding date of
onset of signs of arsenicosis shown by all individuals who inhabited the households since that time,
including members who have since died or moved away. Excluding individuals no longer in the household
will lead to an underestimate. This information should also be collected in the cohorts described in (c).
(c) What percentage of those with skin lesions will develop other arsenic-related health outcomes,
including skin cancer, intemal cancers, cardiovascular disease, et cetera? What percentage of those
without skin lesions will develop these outcomes? What are the latent periods?
The answers to these questions are vital to health infrastructure planning. It is assumed that GOB will wish
to train adequate numbers of physicians and create adequate numbers of appropriately-sited clinics to
diagnose and treat the expected epidemic of skin cancer, because early surgical treatment of skin cancer is
relatively straightforward and highly successful. Data are needed to estimate how many cases will occur
and where and when they will occur. The other health outcomes are more difficult and expensive to
diagnose and treat. Given the presently low GOB financial allocations to the heath sector it seems unlikely
that GOB will prioritize building of infrastructure to provide the more complex and costly treatments
required by other health outcomes such as intemal cancers. It should be noted that money spent on
provision of altemative water sources will likely reduce the occurrence of skin and other cancers, but that
new arsenic-related cases may still occur because for some, the switch to safe water will come after disease
has progressed past a point of no return.
Although arsenic-exposed individuals are currently offered treatment (with vitamins, et cetera) if they have
skin lesions, it has not been shown that longer term health outcomes will occur only in those with such
lesions. To answer this question, individuals must be followed over time and given regular follow-up
examinations. Cohorts for such longitudinal studies should be developed as soon as possible. This work
will entail,relafively sophisticated medical examinations and must be carried out by epidemiologists in
conjunction with clinical research staff at local medical facilities. In these studies, all water sources must be
tested quantitatively by a certified laboratory. Arrangements must be made for securing long-term
participation of study individuals and for tracking them as they migrate, change names, et cetera. Because
conducting longitudinal studies is complex, investigators experienced in such work and investigators
familiar with Bangladeshi social patterns should lead the study. Appropriate cohorts will include those with
a range of exposures and current signs and symptoms.
The ICDDR,B field site in Matlab upazila is ideal for a cohort study because ICDDR,B has collected full
information there on population vital statistics, reproductive outcomes, health, et cetera since 1963.

Appendix 6Public Health Research Needs
ICDDR,B has received funding for a variety of studies from the United States Agency for International
Development, WHO, and Swedish Intemational Development Agency. However, ICDDR,B does not
currently have the capacity to quantitatively measure arsenic in water and this capacity would have to be
developed. Another such study was recently funded by the U.S. National Institutes of Health (NIH):
Columbia University (U.S.) will be creating a cohort of adults in Araihazar to follow for development of
cancers over the next five years. Any other promnising areas for cohorts should also be given consideration,
although it will be more efficient to improve upon existing cohorts than to develop multiple new ones.
These cohort studies will be expensive, but they are vital to furthering our understanding of the health
impact of arsenic exposure.
(d) Does arsenic intake by pregnant women affect pregnancy outcomes?
The answer to this question will be important in village situations where a limited amount of safe water is
available and decisions must be made about whlch individuals should have primary access to it. There is
no good human evidence showing that arsenic harms fetuses but animal evidence shows that doses high
enough to cause illness in pregnant females may cause low birth weight, fetal malformations (neural tube
defects and kidney maldevelopment), and fetal death. Fortunately, two rich data sources for answering this
question already exist. Since 1996, BINP has tracked all birth outcomes by name for all women in its
operational areas. The program logs are kept locally at feeding sites. Efforts should be made immediately
to mine this rich data source. Water sources for each of the women listed in program logs should be tested
for arsenic, using accurate quantitative methods if possible. Information within the logs should be entered
into computers and analyzed. It will be possible to determine if current arsenic content in drinking water is
related to recent pregnancy outcomes (miscarriage, stillbirth, birth defects, birth weight) while controlling
for mother's age, initial weight, pregnancy weight gain, and participation in supplemental feeding. This
work is relatively straightforward and could be performed quickly by epidemiology graduate students or
any epidemiological consulting firm with assistance from data entry clerks fluent and literate in Bangla.
Similarly, the data collected by ICDDR,B in Matlab can be analyzed for the same purpose. Again, the
drinking water has yet to be tested. The group from Columbia University (see c above) will also be
conducting a similar analysis in Araihazar.
(e) What is the dose-response relationship (with dose expressed in terms of both arsenic concentration
and duration of exposure)?
For the moment, this question matters most to Bangladesh in making projections of future cases and health
infrastructure needs, as discussed in (c). However, if the findings cause GOB to change its drinking water
standard from 50 ppb to something else, there will be obvious implications for criteria for water treatments
and test kits, as well as provision of health surveillance and other health services.
This question is also of enormous importance to the world. Global data on the dose-response relationship
are the basis on which WHO, GOB, and other national governments set standards for allowable amounts of
arsenic in drinking water. Often these standards are based on insufficient data. The United States, for

Appendix 6Public Health Research Needs
example, is considering lowering its standard based on projections from Taiwan data - where arsenic levels
are much higher than in the U.S.- by making assumptions about the shape of the dose-response curve.
Bangladesh has a large number of people exposed to arsenic at levels lower than those recorded in Taiwan.
Findings on the dose-response curve in Bangladesh will be of use in setting standards throughout the world.
The question can best be answered by following cohorts as described in (c). Typical doses are not known,
so the work must include evaluation of the amount of arsenic usually drunk by men, women, and children,
accounting for season of the year, pregnancy status, et cetera. Because the results will be of interest around
the world, it may be possible to involve significant foreign investment in the work. It should also be noted
that some dose-response work is presently being carried out in India.
Some dose-response estimates can be made from the cross-sectional survey described in (a). However, these
estimates will suffer from the relatively short time (compared to expected health outcome latent periods)
between tube well installation and the present date.
(f) How do the risks of water contaminated with arsenic compare with the risks of drinking surface
water contaminated with pathogenic bacteria?
This question has been raised by some who wish to provide sound advice in the interim before arsenic
mitigation technologies become widely available. As with any risk trade-off, the answer will depend on
how the question is parameterized. Presumably, people would be advised to boil surface water whenever
possible; and the time period of exposure to both imperfect water sources would be several years at most.
The answer might be different for children and adults, because the risks of using surface water are much
greater for children. There may or may not be sufficient information available regarding the risks of
drinking water with arsenic, the prevalence of arsenical and bacterial contamination, and the ability of
householders to disinfect surface water before use. In any case, it is widely thought that people will be
unwilling to use surface water due to previous education campaigns advocating against its use. This work
is therefore of relatively low priority.
1.2 Susceptibility
Importance:
Anecdotal evidence indicates that within a single household using a common water supply, some
may show effects (skin lesions) while others do not. There are limited data from other countries suggesting
that nutritional, health status, and/or genetic factors might place individuals at greater or lesser risk of
toxicity from arsenic. Findings regarding susceptibility factors could generate hypotheses leading to
effective treatment.
Specific questions addressed in this section and Specific recommendations:
(g) How is susceptibility modified by factors such as nutritional status, general health status, infections,
et cetera, which have a potential for intervention?

Appendix 6Public Health Research Needs
Thls question is of obvious interest because some risk factors for arsenicosis, such as nutritional deficiencies
or infections, are potentially remediable. Observational studies have suggested that underweight persons
and those with diets low in green vegetables are at increased risk. The question could be partially addressed
by a case-control study bemg performed by Harvard University with DCH and a similar study proposed by
the U.S. Centers for Disease Control and Prevention (CDC). Both studies are to examine various nutritional
parameters as risk factors for arsenicosis. Harvard University has received funding from NIH and CDC has
received funding from UNICEF. However, the proposed CDC study does not include adequate data
collecfion on general health status or infections (e.g. with helminths, which could affect intestinal absorption
of arsenic), to answer questions about these factors). Additional studies will be needed to answer these
questions. These could be performed either by identifying patients through clinical rolls of institutions
treating arsenic cases (as is happening at DCH) or by nesting the studies in larger cohorts (see c). If
susceptibility factors are found, further studies of those factors could take place through clinical trials of
nutritional supplementation, treatment of infections, et cetera. Such studies must include experienced
epidemiologists and clinicians in order to be properly performed and interpreted. ICDDR,B plans to
examine the relationship of nutritional factors and skin lesions in Matlab. DCH is planning some additional
work with researchers at the London School of Hygiene and Tropical Medicine with funding from DFID, but
details have not been finalized or made available. There also exists a nutritional database on individuals
from Jessore, Saturia, and Mymensingh from a 1996-1997 longitudinal study by the International Food
Policy Research Institute; databases such as this one could be supplemented by current measures of water
arsenic and health effects to shed light on the issues.
(h) How is susceptibility modiLfied by factors such as age and sex, which don't have a potential for
intervention?
This question is important for two reasons: it affects projections of current and future cases, and it can affect
choices of who is given priority access to safe water in village situations where quantities are limited. For
example, children appear to be more sensitive to arsenic, presumably because their smaller size leads to a
relatively higher body burden. Age and sex are fairly straightforward to measure (and the studies described
in (a), (c), and (d) will all address this issue. (For those who were born before birth certificates were routinely
kept, interview probes must be used to estimate time of birth.)
Genetic factors may affect susceptibility, and there is a Harvard University-DCH study ongoing to examine
potentially relevant genetic polymorphisms and markers in a molecular epidemiology study. Because this
study is under-funded, full analysis of the biological samples collected is unlikely to be completed for
several years (until more funding is obtained). However, genetic testing is unlikely to become a feasible
means of prioritizing interventions, and if arsenicosis-resistant populations are found, it would still be many
years before this discovery could possibly be translated into effective treatments. Therefore, genetic factors
are not a priority area for study.

Appendix 6Public Health Research Needs
1.3 Treatment
Importance:
At present, efforts are being made by some agencies to treat individuals with hyper- and hypo-melanosis
and hyperkeratosis. These lesions, by themselves, are not usually of health concern, but may be painful and
have highly undesirable social consequences. Treatment is not being offered to those with known arsenic
exposure who do not show skin lesions. All who are known to be using water contaminated with arsenic
are advised to switch to arsenic-free water, and some organizations give arsenic-filtration kits to those with
skin lesions.
The effectiveness of the treatments being used for skin conditions is unknown. More important, the
effectiveness of these treatments against progression to more severe conditions is unknown. The
reversibility of health effects upon institution of arsenic-free water is unknown. Treatments currently in use
as well as potential treatments not yet in use should be evaluated through clinical trials. Priority should be
given to treatments already being used. In no case should arsenic-free drinking water be withheld from any
individual.
Specific questions addressed in this section and Specific recommendations:
(i) What is the effectiveness of treatment with anti-oxidant vitamins (A, E, & C) in reversing skin
lesions?
This question deserves the highest priority because several agencies (such as BRAC and DCH) are already
treating patients with vitamins in combination with recommending arsenic-free water, and all seem to accept
that vitamins are a useful treatment. However, whether they actually do help, as well as the mechanism by
which vitamins might affect skin lesions or other arsenic-related health outcomes is unclear. BRAC and
DCH staff both report that the treatment is useful; however, they base their findings solely on anecdotal
reports that their patients feel better and because all patients are advised to use arsenic-free water as well, it
is difficult to quantify any improvement or confidently attribute it to vitamins versus safe water.
Two approaches should be taken. First, existing medical records should be utilized to the extent possible.
Both BRAC and DCH report keeping records of each encounter for patients who are seen multiple times for
arsenical lesions. The records are said to include objective ratings of the severity of skin lesions. To be useful
for this purpose, the records should also keep account of whether vitamins have actually been taken and
whether and when the patient's water source was changed. However, inspection of a DCH record form
revealed that it did not include spaces for recording size of lesions, compliance with water
recommendations, and treatment prescriptions or compliance. Any records that do contain such
information can be reviewed to attempt to quantify the amount of improvement seen by the treating
physician and the time until improvement, depending on whether the patient switched water or took
vitamins or both. Presumably, some patients will have switched water sources, some will have used
vitamins, and some will have done both, so it should be possible to examine the effects of each "treatment"
as well as the two combined. Compliance with the prescribed water and vitamin regimens must be assessed,

Appendix 6Public Health Research Needs
and this information may be useful in future program planning. If the records prove inadequate to answer
the questions - i.e., because lesions are not objectively rated at each visit or because insufficient information
is collected on patients' use of arsenic-free water and vitamins - the record format should be changed so that
this analysis can be performed in the future, and the relevant clinicians should be trained to interview
patients and fill in the records properly. (NIPSOM performed an analysis along this line, but with very few
patients. Among 9 patients who used vitamins but unsafe water, 2 improved. Among 22 patients who used
vitamins and drank safe water, 20 improved. There was no comparison group of patients who did not use
vitamins and drank safe water.)
The second approach is a controlled, double-blinded, clinical trial. Vitamins should be tested alone and in
each combination. There are no ethical concerns about doing such a trial because there is no evidence that
vitamins are beneficial. The vitamins (and placebos) must be provided free of charge to allow full
compliance. All ages and both sexes should be included, although high doses of vitamin A should not be
tested on women who are or may become pregnant because of potential teratogenicity, and patients should
be monitored to avoid overdoses of vitamins A and E. All subjects should receive arsenic-free drinking
water. The trial must be conducted at an institution that sees sufficient numbers of arsenicosis patients and
has trained research and medical staff. BRAC, DCH, and ICDDR,B are possible institutions.
(j) What is the effectiveness of selenium (and other micronutrients) in reversing skin lesions?
&
(k) What is the effectiveness of increased protein intake in reversing skin lesions?
The responses to these questions have been combined because the approach is similar for both.
Selenium and arsenic reduce each others' effects in the body, and so selenium supplementation might be
useful. Protein is involved in methylating inorgamc arsenic to organic arsenic. While fluctuations in protein
intake and methylation cofactors do not affect methylation capacity in individuals with normal dietary
intakes, it is plausible that severely malnourished individuals may have decreased methylation capacity that
could be affected by changing the diet. Similarly, deficiencies of methyl donors such as choline or
methionine could be important. Other chemicals that play a role in the methylation process, such as
glutathione, could affect toxicity. Folate has also been mentioned as possibly playing an important role.
Spirulina, a locally-available, purportedly high-protein, high-carotene food denved from algae, has been
recommended to some patients as an anti-arsenicosis treatment. Because arsenic is rapidly cleared from the
body, it is unclear whether any of these factors would be effective after exposure is stopped, even if they are
effective during exposure.
A study is now planned that will examine arsenic health effects according to a number of nutritional
parameters, including selenium and protein status (see g). If this study shows important differences, then
controlled, blinded, clinical trials may be indicated as a next step. These trials would require free provision
of the supplements, as above. The trials must be conducted at institutions that see sufficient numbers of9

Appendix 6Public Health Research Needs
arsenicosis patients and have trained research staff. Trials involving manipulation of micronutrients,
including selenium, would require intensive monitoring of patients under study to avoid untoward health
effects. Over-supplementation with selenium is a potential hazard. Therefore, this trial should be attempted
only if qualified investigators and a site can be identified where patients can be carefully monitored for
selenium status, health status, et cetera.
Spirulina should be studied as described in (i) because it is already being recommended.
(1) Is chelation therapy useful in long-term exposure?
This question has been raised by some. Although chelation therapy may have some utility in acute
exposures when initiated within a few hours after exposure, it seems unlikely to be of value in long-term
exposure because the half-life of arsenic in the body is only 4 days and arsenic is not stored in metabolically
active body tissues. In addition, chelation therapy is usually done an inpatient basis and requires careful
medical monitoring because of serious side effects including pain, fever, hypotension, and nephrotoxicity.
This treatment is therefore unlikely to be of great value in Bangladesh, and researching it is not
recommended at this time.
(m) What is the effectiveness of salicylic and other skin lotions in reversing skin lesions?
Some organizations are providing ointments to those with keratoses. These ointments are thought to soothe
painful lesions and perhaps reverse them. These assumptions could be tested as described in (i); they could
be tested very simply by applying them to one hand only, if patient compliance is good.
(n) What is the impact of providing arsenic-free water in reversing skin lesions?
This question can only be answered by observation because it would be unethical to withhold safe water
from any affected individuals. As discussed in (i), there is one limited report from NIPSOM on this point.
Extant medical records should be reviewed to answer the question to the extent possible now, and record
formats should be improved if necessary. In the middle term, as various NGO and government programs
are implemented to institute safe water systems, those programs that have access to trained professionals
could take objective baseline measures of the skin status of individuals who will be using the new water
system, and re-visit them for follow-up measures at regular intervals to re-assess status and determine if any
changes have occurred. Objective follow-up of lesions would be an important feature of the longitudinal
cohorts described in (c). Finally, the surveillance system recommended in (a) might provide information on
national impacts in the long term.
(o) What is the impact of treating skin lesion patients on the longer-term incidence of other health
outcomes?
As mentioned above, the long term impact of treating those with lesions is unknown, but it is possible that
a given treatment will affect some, but not all, potential health outcomes. Some skin lesions may develop

Appendix 6Public Health Research Needs
into cancers, and successful treatment of the lesion may reduce the skm cancer risk. It is also possible that
the same mechanism that diminishes skin lesions might also interfere with development of other health
outcomes. Once again, this question can best be answered by an observational cohort study that follows
patients in time, as discussed in (c).
I

Appendix 6Public Health Research Needs
Table 6. Summary of Research Recommendations.
Near Term (within next year):
Activity Relevant ResearchQuestions
national, population-based health survey a, b, h
case-control studies to determine risk factors for susceptibility g, h
clinical trial of vitamins A, E, & C i
development of qualified reference laboratories for assaying arsenic in water e
review of BINP and Matlab data on pregnancy outcomes / quantitatively d
test water supplies in those areas
review of DCH and BRAC medical records for arsenic patients / revise i
forms as necessary
cohort studies in Matlab and Araihazar / baseline measurements and b, c, d, e, g, h
nested case-control studies
Middle Term (next 2 to 6 years):
Activity Relevant Research
Questions
add arsenic items to the DHS a, b, e, h
other clinical trials as indicated i, j, k, m
training and active case finding by outreach organizations a
continue cohort studies / calculate middle-term incidence rates and n, o
treatment effectiveness
Long Term (next 7 and more years):
Activity Relevant Research
Questions
ongoing surveillance of skin lesions a, o
continue cohort studies / complete projections of case numbers of skin n, o
cancer, et cetera

Appendix 7Public Health Research Needs
ISSUES RELEVANT TO TESTING OF WATER SAMPLES FORARSENIC
It is estimated that Bangladesh has 8 - 12 million tube wells which will need to be tested. At least in the short
term, a large proportion of these will need to be tested regularly as the levels of arsenic may change over
time. Table 7 shows the current capacity in Bangladesh for laboratory testing of water samples for arsenic.
Three points are noteworthy:
* the lowest detectable level is 10 ppb, which suggests that a reduction the officially prescribed national
safety level from 50 ppb to 10 ppb is feasible.
* the cost is still very high for the resource situation of Bangladesh
* Nearly all the testing centers are in Dhaka, the capital. There is clearly a need to establish more regional
testing centers around the country.
Table 7. Analytical methods for arsenic testing and capacity in Bangladesh.
Method Lowest Availability Commentdetectable level and cost
Flow injection hydride 10 ppb BCSIR*, BARC**, Widely accepted for water,generation atomic absorption TK 600/per urine, soil, hair and nailspectrometry sample analysis. Inexpensive.
Graphite fluorescence atomic 10 ppb BUET Widely used for water, urine,absorption spectrometry TK 1000/per soil, hair and nail analysis
sample
Anodic stripping voltmeter 10 ppb Chemistry Used for water, hair, and nailwith gold electrode Department, analysis
DU***Not commerciallyavailable
Total reflection X-ray 10 ppb Atomic Energy Used for water, hair and nailfluorescence Commission analysis
TK 1500/persample
Neutron Activation Analysis 10 ppb Atomic Energy Used for water andCommission biological samples
Molecular absorption -100 ppb NGO Forum Waterspectroholometry (TK300),
DPHE (TK500)
* Bangladesh Councilfor Scientific and Industrial Research** Bangladesh Agricultural Research Council*** Dhaka University

Appendix 7Public Health Research Needs
The need for suitable test kits: The amount of testing required, the capacity and price of laboratory testing,
and the need for feedback to those using the tube well water strongly suggest the use of field kits for
nationwide testing. Several kits exist, but are none as yet is found to be ideal in terms of price, ease of use,
and accuracy simultaneously; and none is readily available throughout Bangladesh (see Table 8).
Table 8. Basic data onfield-test kits
Field Test Kit Cost Commercially Manufactured Time Lowest Level(approx. and locally taken of Arsenic
US$) available per test Detectable(minutes (ppb)
Merck 50 Yes Germany 30 100
GPL 45 Yes Bangladesh 20
NIPSOM 40 No Bangladesh 10
HACH 160 Yes USA 30 10
PeCo75 800 Yes Austria 15 30
Spectrochemicals 50 In the near future India 10
NCL 100 In the near future India 10
Source: WaterAid, 200119.
Reliable test kits must be available at an affordable price at the village level. This will likely require multiple
distribution systems managed by one or more government agencies, NGOs and the private sector. The
private sector should be encouraged to start production and distribution of field test kits. A pricing policy
will have to be developed and safeguards put in place to ensure that the poor have access to testing of their
water. A key issue to be addressed is capacity requirements for water testing and considerations as to how
and where such capacity may be developed.
Also, reliable laboratories must be in place to provide backup testing to confirm field testing, e.g. to verify
performance of field kits and testers.
Research. Finally, some research is needed to determine how frequently wells need to be re-tested. It is
currently unknown whether there are seasonal fluctuations in arsenic content and whether there are secular
trends (either increasing or decreasing). In theory, arsenic content could vary by season (related to flooding)
and / or by amount of water used from the aquifer in question. It is also unknown whether deep tube wells,
currently considered safe in almost all circumstances, may become contaminated with arsenic over time.
Incorrectly assuming that arsenic content does not fluctuate could result in significant wastage of safe water
as well as continued consumption of unsafe water. The question must be addressed by repeated,
quantitative testing of both shallow and deep tube wells with a variety of depths and arsenic concentrations. q

REFERENCES
Agency for Toxic Substances and Disease Registry. Toxicological Profile for Arsenic (Update). United
States Department of Health and Human Services, 2000.
Ahmad SA et al. Arsenic contamination in ground water and arsenicosis in Bangladesh. International
Journal of Environmental Health Research, 1997, 7:271-276.
Biswas BK et al. Detailed study report of Samta, one of the arsenic-affected villages of Jessore District,
Bangladesh. Current Science, 1998, 74:134-145.
Biswas BK et al. Groundwater arsenic contamination and sufferings of people in Bangladesh, a report up to
January, 1999. Paper presented at the International Conference, Arsemc in Bangladesh Ground Water:
World's Greatest Arsenic Calamity, Staten Island, New York, USA, 27-28 February, 1999.
BRAC. Combating a deadly menace: early experiences with a community based arsenic mitigation project
in Bangladesh, 2000.
British Geological Survey and Department of Public Health Engineering. Arsenc contamination of
groundwater in Bangladesh. Kinniburgh, D G and Smedley, P L (Editors). Volume 2: Final report. British
Geological Survey Report WC/00/19, British Geological Survey, Keyworth, 2001
British Geological Survey and Mott MacDonald (UK): Executive Summary of the main report of Phase I,
groundwater studies of arsenic contamination in Bangladesh. For the Government of Bangladesh, Ministry of
Local Government, Rural Development, and Cooperatives, Department of Public Health Engineering, and
Department for International Development (UK), 1999.
Chen CJ et al. Arsenic and cancer (letter). Lancet, 1988, 1:414-415.
Chen CJ et al. Cancer potential in liver, lung, bladder and kidney due to ingested inorganic arsenic in
drinking water. British Journal of Cancer, 1992, 66:888-892.
Chen CJ et al. Malignant neoplasms among residents of a Black-Foot Disease-endemic area in Taiwan: high-
arsenic artesian well water and cancers. Cancer Research, 1985, 45:5895-5899.
Chen CJ, Wang CJ. Ecological correlation between arsenic levels in well water and age adjusted mortality
from malignant neoplasms. Cancer Research, 1990, 50:5470-5475.
Ch'i IC, Blackwell RQ. A controlled retrospective study of blackfoot disease, an endemic peripheral
gangrene disease in Taiwan. American Journal of Epidemiology, 1968, 88:7-24.
Chowdhury TR et al. Arsenic poisoning in the Ganges delta. Nature, 1999, 401:545-546.
Dhaka Community Hospital. Report on action research on community based arsenic mitigation project,
DCH-DPHE-UNICEF Project, 2000.
Dhar RK et al. Groundwater arsenic calamity in Bangladesh. Current Science, 1997, 73:48-59.
Grameen Bank. Completion report of community based arsenic mitigation project (GB-DPHE-UNICEF
Project), 2000.

Guha Mazumder DN et al. Arsenic levels in drinking water and the prevalence of skin lesions in West
Bengal, India. International Journal of Epidemiology, 1998, 27:871-877.
Guha Mazumder DN et al. Non-cancer effects of chronic arsenicosis with special reference to liver damage.
In: Abernathy CO, Calderon RL, Chappel WR, editors. Arsenic: exposure and health effects, pages 112-123.
London: Capman and Hall, 1997.
Hopenhayn-Rich C et al. Bladder cancer mortality associated with arsenic in drinking water in Argentina.
Epidemiology, 1996, 7:117-124.
Hopenhayn-Rich C et al. Lung and kidney cancer mortality associated with arsenic in drinking water in
Cordoba, Argentina. International Journal of Epidemiology, 1998, 27:561-569.
Hutchinson J. Arsenic cancer. British Medical journal, 1887, 2:1280-1281.
Hutchinson J. On some examples of arsenic-keratosis of the skin and of arsenic-cancer. Transactions of the
Pathological Society of London, 1887, 39:352-363.
Integrated Services for Development of Children and Mothers, Community Based Arsenic Mitigation
Project in Manikgong Sadar Upazila, 2000.
Kao TM et al. Spontaneous gangrene and chronic potassium poisoning. Presented at the 46th Annual
Meeting of the Formosan Medical Association, Taipei, Taiwan, 1954.
Khan AW, Ahmad SA. Arsenic in drinking water. Health effects and management. A training manual.
Dhaka: Department of Occupational and Environmental Health. NIPSOM, 1997.
Khan AW et al. Arsenic contamination in groundwater and its effect on human health with particular
reference to Bangladesh. Journal of Preventive and Social Medicine, 1997, 16:65-73.
Mandal BK et al. Arsenic in groundwater in seven districts of West Bengal, India - the biggest arsenic
calamity in the world. Current Science, 1996, 70:976-986.
National Research Council. Arsenic in drinking water. Washington, DC: National Academy Press, 1999.
Pershagen G, Vahter M. Arsenic: a toxicological and epiderniological appraisal. SNV PM 1128. The
national Swedish Environment Protection Board, Stockholm, 1979.
Quamruzzaman Q et al. Rapid action programme: emergency arsenic mitigation programme in two
hundred villages in Bangladesh. In: Arsenic Exposure and Health Effects: Proceedings of the Third International
Conference on Arsenic Exposure and Health Effects, 12-15 July 1998, San Diego, pages 363-366. Oxford, Elsevier
Science, 1999.
Rahman M. Nonmalignant Health Effects of Arsenic Exposure. Linkbping University Medical Dissertation.
No 612, Linkoping, Sweden: 1999.
Rahman M et al. Diabetes mellitus associated with arsenic exposure in Bangladesh. American Journal of
Epidemiology, 1998, 148:198-203.
Rahman M et al. Hypertension and arsenic exposure in Bangladesh. Hypertension, 1999, 33:74-78.
Rahman M et al. Relations between exposure to arsenic, skin lesions, and glucosuria. Occupational and
Environmental Medicine, 1999, 56:277-281.

Saha KC. Chronic arsenical dermatoses from tube-well water in West Bengal during 1983-87. Indian Journal
of Dermatology, 1995, 40:1-12.
Smith AH et al. Cancer risks from arsenic in drinking water. Environmental Health Perspectives, 1992, 97:259-
257.
Smith AH et al. Cancer risks from arsenic in drinking water: implications for drinking water standards. In:
Proceedings of the Third International Conference on Arsenic Exposure and Health Effects, 12-15 July 1998,
San Diego, pp 191-200. Oxford: Elsevier Science, 1999.
Smith AH et al. Contamination of drinking-water by arsenic in Bangladesh: a public health emergency.
Bulletin of the World Health Organization 2000;78:1093-1103.
Smith AH et al. Marked increase in bladder and lung cancer mortality in a region of Northern Chile due to
arsenic in drinking water. American Journal of Epidemiology, 1998, 147:660-669.
Smith AH, Rahman M. Arsenic in drinking water: a public health point of view. Medicine Digest, 2001; Jan-
Mar:5-6.
Tondel M et al. The relationship of arsenic levels in drinking water and the prevalence of skin lesions in
Bangladesh. Environmental Health Perspectives, 1999, 107:727-729.
Tseng WP. Blackfoot disease in Taiwan: a 30-year follow-up study. Angiology 1989, 40:547-558.
Tseng WP. Effects and dose-response relationships of skin cancer and blackfoot disease with arsenic.
Environmental Health Perspectives, 1977, 19:109-119.
Tseng WP et al. A clinical study of blackfoot disease in Taiwan, an epidemic peripheral vascular disease.
Memoirs of the College of Medicine National Taiwan University, 1961, 7:1-17.
Tseng WP et al. Prevalence of skin cancer in an endemic area of chronic arsenicism in Taiwan. Journal of the
National Cancer Institute, 1968, 40:453-463.
UNICEF. Progotir pathey, on the road to progress; achieving the goals for children in Bangladesh, October
1998. Dhaka. Bangladesh Bureau of Statistics, Ministry of Planning, Government of the People's Republic
of Bangladesh with UNICEF, 1999.
United States Environmental Protection Agency. Special report on ingested inorganic arsenic: skin cancer;
nutritional essentiality. Washington, DC: EPA 625/3-87/013, 1988.
WaterAid. Arsenic, 2000: An Overview of Arsenic Issues in Bangladesh, 2000.
WaterAid. Rapid Assessment of Household Level Arsenic Removal Technologies, Phase II Executive
Summary, 2001. Available at http://www.wateraid.org.uk/research/BangladeshA.html
World Bank. Project Appraisal Document, Bangladesh Arsenic Mitigation and Water Supply Project, 1998.
World Health Organization. Arsenic in Drinking Water Fact Sheet No. 210, Revised May, 2001. (Available
at http: / / www.who.int / mf-fs / en / fact2l0.html.)
World Health Organization. Environmental health criteria 18: Arsenic. Geneva: WHO, 1981.
World Health Organization. WHO guidelines for drinking-water quality. Vol. 2, second edition, Health
criteria and other supporting information. Geneva: WHO, 1996.

