with acute coronary insufficiency
TRANSCRIPT

Natural History of Cardiac Arrhythmiasand their Prevention with Quinidine in Patients
with Acute Coronary Insufficiency
By SAUL S. BLOOMFIELD, M.D., DONALD W. ROMHILT, M.D.,
TE-CHUAN CHOU, M.D., AND NOBLE 0. FOWLER, M.D.
SUMMARYIn a prospective controlled clinical trial the natural history of cardiac arrhythmias and their
prevention with prophylactic quinidine therapy were studied in 23 patients with acute coro-
nary insufficiency without myocardial infarction. After a loading procedure, 300 mg of quini-dine sulfate or placebo was administered orally every 6 hours for up to 5 days under balanced,random, double-blind conditions. An automated arrhythmia detection system was used to quan-
tify arrhythmias from stored continuous electrocardiographic tape recordings.The frequency of ventricular and supraventricular arrhythmias tended to increase progressively
on each successive day of study in placebo-treated patients. By contrast, in quinidine-treated pa-
tients all arrhythmias were quantitatively lower on each day of therapy and did not show a ten-dency toward progressive daily increases. In the placebo group there was an average of 140premature ventricular contractions (PVC's) per day on the first day which increased to 600PVC's per day by the fifth day, whereas with quinidine there was an average of 40 PVC's per
day or less throughout the 5 days of study (P < 0.01). The daily increase in ventricular arrhyth-mias in placebo-treated patients with acute coronary insufficiency during the 5 days is in contrastto the natural history of patients with documented myocardial infarction who have a marked dailydecrease in the frequency of ventricular arrhythmias during the first 5 days. Significant arrhythmiasuppression with quinidine was present when mean blood quinidine concentration reached a steadystate above 4 mg/liter at the end of the first day of therapy. Adverse reactions to quinidine were
not observed. On the basis of these data, quinidine sulfate given prophylactically at a dosage pro-ducing modest blood concentrations appeared to be both effective and safe for the prevention ofventricular and supraventricular arrhythmias that occurred during the first 5 days after an episodeof acute coronary insufficiency without infarction.
Additional Indexing Words:Coronary heart diseasePremature ventricular contractions
Antiarrhythmic drug Coronary care unit
T HE HIGH INCIDENCE of ventricular ar-
rhythmias following acute myocardial infarc-tion has been well documented1- and has led totreatment programs, both therapeutic and prophy-lactic4-7 aimed at suppressing these arrhythmias
From the Divisions of Clinical Pharmacology andCardiology, Departments of Medicine and Pharmacologyand Therapeutics, University of Cincinnati Medical Center,Cincinnati, Ohio.
Supported by U. S. Public Health Service Grants HE-11817, HE-05776, and HE-06307. Saul S. Bloomfield wasthe recipient of a U. S. Public Health Service SpecialResearch Fellowship Award, HE-34658.
Address for reprints: Donald W. Romhilt, M.D., CardiacResearch Laboratory, Cincinnati General Hospital, Cincin-nati, Ohio 45229.
Received November 17, 1972; revision acc,epted forpublication January 22, 1973.
Circulation, Volume XLVII, May 1973
with the intent of reducing mortality. In thecoronary care unit initial emphasis was directedtoward patients with verified myocardial infarction,but more recently patients with acute coronaryinsufficiency without infarction have received con-siderable attention.8 9 In a previous communica-tion,5 we reported a clinical trial which demonstrat-ed the efficacy of prophylactic quinidine sulfate forthe prevention of arrhythmias following uncompli-cated acute myocardial infarction in 55 patients.During the same period we also studied 25 patientswhose presenting symptoms were similar, but thediagnosis of acute myocardial infarction was notsubsequently verified. The purpose of this report isto describe the incidence and natural history ofarrhythmias and their prevention with quinidinesulfate in 25 patients with acute coronary insuffi-ciency.
967
by guest on January 31, 2018http://circ.ahajournals.org/
Dow
nloaded from

BLOOMFIELD ET AL.
Methods
Patient Selection Criteria
On accession to study, the 25 patients were under 70years of age and had a history of coronarylike painduring the previous 24 hours. Twenty-two patients hadsevere substernal chest pain lasting longer than 30 minwhile three patients had multiple episodes of substernalchest pain lasting 15-20 min which were more severeand lasted longer than previous episodes of anginapectoris. The electrocardiogram of 19 patients hadeither S-T-segment elevation suggestive of an acuteinjury pattern (three patients) or marked T-waveinversion consistent with myocardial ischemia (16patients). One patient had marked S-T-segmentdepression and five patients had nonspecific abnormal-ities of the S-T segment and T wave. Two patients hadan old myocardial infarction on the electrocardiogram.The following complications were absent at the onset ofstudy: shock, atrioventricular block, bundle-branchblock, severe heart failure, uremia, coma, or an existingarrhythmia. The diagnosis of acute myocardial infarc-tion was excluded on the basis of an evaluation by twoindependent observers utilizing the following criteria:(1) daily electrocardiograms which failed to reveal thedevelopment of pathologic Q waves, and (2) dailyserum enzyme determinations (creatine phosphokinase,serum glutamic oxaloacetic transaminase, lactic dehy-drogenase) which did not demonstrate a rise.
Patients under study were admitted to either theCincinnati General, Jewish, or Veterans AdministrationHospitals. At all three hospitals, patients receiveduniform management, including routine nasal adminis-tration of oxygen for 48 hours, opiates for analgesia,barbiturates for sedation, and heparin as an anticoagu-lant. No antiarrhythmic agent except the studymedication was administered during the trial. It was
planned to remove from study any patient whodeveloped a recognized arrhythmia which requiredspecific therapy, or any patient who developed heartblock, shock, uremia, or heart failure requiring digitalistherapy. Also, any patient with evidence of quinidinetoxicity by symptomatology or by QRS prolongationgreater than 25% from the pretreatment tracing on
conventional electrocardiograms taken twice daily was
removed from the trial. Data were collected for 5 dayson 20 patients and for 2 days on five patients unless anyof the above-named complications occurred earlier. Inthe latter eventualities, data collected up to the time ofwithdrawal from study were retained for inclusion inthe analysis.
Design of TrialThe trial compared a quinidine-treated group of
patients with a control group receiving indistinguish-able placebos under double-blind conditions. Attendingphysicians and staff nurses also were unaware of whichpatients received quinidine, and the investigatorsremained blind until after the data had been analyzed.Upon entering the study patients were randomlyallocated to one of the two treatment groups accordingto a predetermined schedule. The randomizationprovided for stratification of patients according to sex
and hospital, with equal balancing of treatments within
strata. Since the trial was a between-subject comparison,each patient was studied with only one form of treat-ment.
Experimental medications consisted of quinidinesulfate, 300 mg, or placebo in identical coded capsules.Three oral doses were given fasting10 at 3-hour intervalsas a loading procedure, followed by one dose every 6hours before meals for the remainder of the studyperiod. If necessary, the drug code for any patientcould be broken without revealing the treatmentreceived by other patients. The decision to remove a
patient from study was always made before the code forthat patient was broken.
Evaluation of Response
Results of treatment with quinidine and placebowere evaluated with continuous electrocardiographictape recordings using the Holter-Avionics recorder forthe entire time the patient was being studied." Thestored tapes with the continuous electrocardiogram forthe entire study period were subsequently played backat real time and analyzed with a Hewlett-Packardautomated arrhythmia detection system. The automatedarrhythmia detection system recognized arrhythmias bytwo criteria: (1) change in R-R interval by more than20%; (2) widening of the QRS by more than 0.015 secas compared with the average of four normal QRScomplexes for that patient. The instrument was set toprintout automatically intermittent electrocardiogramswhich contained a complete record of all arrhythmias,including single ectopic beats fulfilling either of thesetwo criteria. The time of each episode of arrhythmia tothe nearest minute was recorded on the electrocardio-gram by an automated time stamp. All electrocardio-graphic print-outs by the automated arrhythmia detec-tion system were read, and each arrhythmia orpremature ventricular contraction was identified andquantified from the electrocardiographic printout on
an hour-by-hour basis by the investigators. From thisanalysis each arrhythmia or single premature ventricu-lar contraction was verified visually by the investiga-tors, and all artifacts were excluded.12The efficacy of quinidine in preventing arrhythmias
was determined by a comparison between the twotreatment groups with respect to the occurrence of thefollowini arrhythmias: premature ventricular contrac-tions (PVC's), serious ventricular arrhythmias,* andpremature sunraventricular contractions. All arrhythmiadata were statistically analyzed for treatment differ-ences by the Mann-Whitney U test (two-tailed)13 withthe ulse of a computer program specially written for thispurpose.
In all patients, blood quinidine levels were deter-mined at the sixth and ninth hours after entry intostudy, i.e., before and 3 hours after the end of theloading period, and then once or twice daily for theremaining days immediately before administration of a
dose of drug. Blood quinidine concentration was
*Serious ventricular arrhythmias were defined accordingto the criteria set by Lown;4 PVC's of more than five/min,multifocal, "R on T," consecutive in runs of two or more orbigeminy.
Circulation, Volume XLVII, May 1973
968
by guest on January 31, 2018http://circ.ahajournals.org/
Dow
nloaded from

PREVENTION OF ARRHYTHMIAS
determined in all samples by an automated adaptationof the protein precipitation spectrophotofluorometricmethod.14
Results
Patient Characteristics and Resultsof Randomization
Electrocardiographic tape recordings for 23 ofthese 25 patients were acceptable for processingand analysis and the data presented concern thisgroup of 23 patients. Electrocardiographic data forthe two excluded patients were uninterpretableowing to technical problems with the tape record-ings. Three patients in the placebo group and twoin the quinidine group were studied for only 48hours. The 23 patients included 13 men and 10women.
Twelve patients comprised the placebo group
and 11 the quinidine-treated group. Group charac-teristics of these patients on entry into study are
shown in table 1. The two treatment groups were
similar in all baseline characteristics examined atthe time of entry except for sex distribution, Q-Tinterval, and numbers of patients on maintenancedigitalis therapy. Especially noteworthy was thetime at which study drugs were started in relationto the onset of the acute episode; the mean intervalwas 16 hours in both the placebo and quinidinegroups.
After entry into the study, the numbers ofpatients in each treatment group receiving concomi-tant medications including opiates, barbiturates,and heparin were equal. An exception, however,
was diuretic therapy which was given to five place-bo-treated patients but only one quinidine-treatedpatient. The fact that more placebo-treated patientsthan those treated with quinidine received digitalis(table 1) and diuretics before and after enteringthe study was probably due to chance. Thepossibility is raised, however, that despite therandomization of patients to the two treatmentgroups, the discrepancy between the groups inadministered diuretics and digitalis might havecontributed in some way to observed differences inarrhythmia activity associated with the two treat-ments.
Effect on Arrhythmias
Data on arrhythmias for the entire duration ofstudy in all 23 patients were completely analyzedand form the basis of this report. The mean numberof PVC's per day was significantly lower (P<0.01or better) in the quinidine-treated patients than inthe placebo patients on each of the 5 days of thestudy (fig. 1). The mean number of PVC's per
day in quinidine-treated patients stayed at a ratherconstant low level throughout the 5 days of study,i.e., 40 PVC's per day or less. By contrast, inplacebo-treated patients the mean number of PVC'stended to increase progressively on each successiveday. On the first day there was an average of 140PVC's and these increased progressively during thecourse of the 5 days, until a maximum of 600 PVC'swas reached on the fifth day. A parallel pattern was
observed with respect to the mean number of
able 1
Characteristics of Treatment Groups on Entry into Study
Placebo QuinidineCharacteristics group group
Total no. of patients 12 11
Sex (no.):Men 5 8Women 7 3
Age (mean yr SEM) 55 2 53 2Weight (mean kg sEM) 74.3 3.8 73.9 2.3Interval between acute episode and entry (mean hr SEM) 16 1.7 16 2.2History of previous infarction (no. of pt) 2 1Maintenance digitalis therapy (no. of pt) 4 1
Serum enzymes (mean SEM):Maximum SGOT (U/ml) 43 7 45 6Maximum LDH (U/ml) 519 - 40 464 44Maximum CPK (U/ml) 29 -12 43 10
Blood chemical findings (mean SEM):Blood urea nitrogen (mg/100 ml) 17 1 15 2Serum potassium (mEq/liter) 4.2 0.2 4.3 0.1Serum sodium (mEq/liter) 137 1 138 1
Circulation, Volume XLVII, May 1973
969
by guest on January 31, 2018http://circ.ahajournals.org/
Dow
nloaded from
BLOOMFIELD ET AL.
PVC
20 r
P ' .001
DAYS AFTER ENTRY
SERIOUS VENTRICULAR ARRHYTHMIASP < .001
15
10
P <.001
<. 02 3 4DAYS AFTER ENTRY
I
5
PREMATURE SUPRAVENTRICULAR CONTRACTIONS
2 3 4
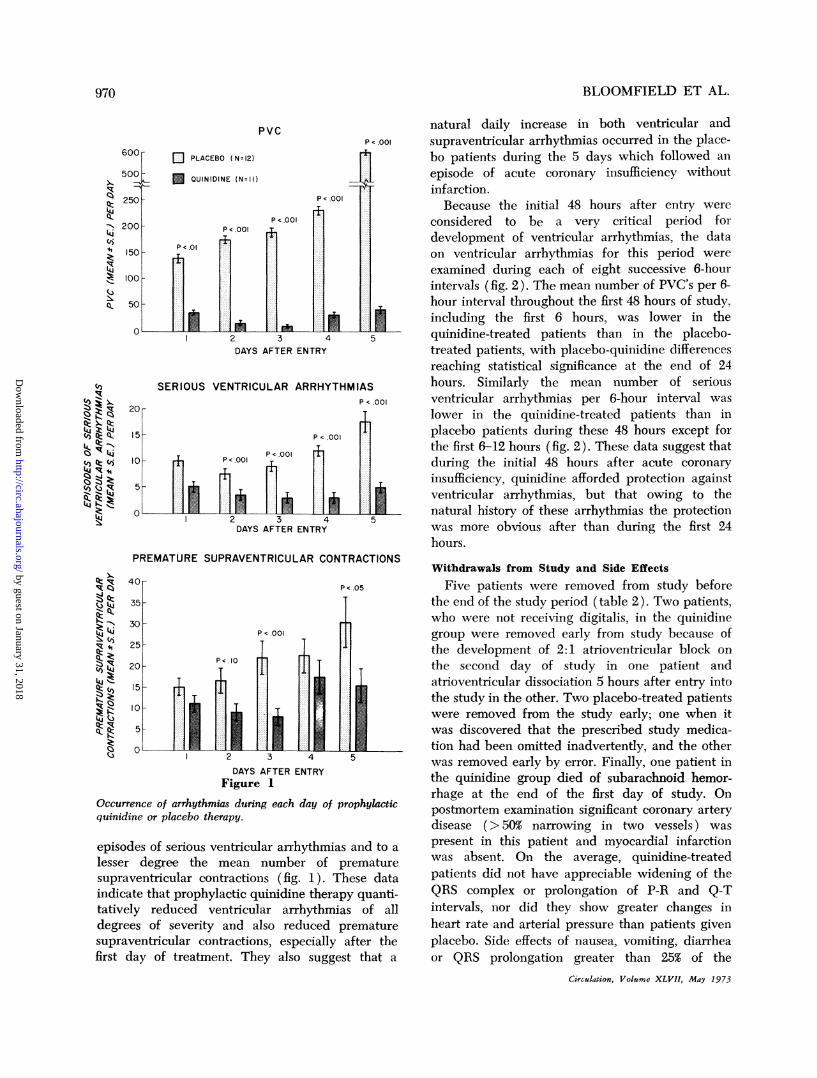
DAYS AFTER ENTRYFigure 1
Occurrence of arrhythmias during each day of prophylacticquinidine or placebo therapy.
episodes of serious ventricular arrhythmias and to a
lesser degree the mean number of prematuresupraventricular contractions (fig. 1). These dataindicate that prophylactic quinidine therapy quanti-tatively reduced ventricular arrhythmias of alldegrees of severity and also reduced prematuresupraventricular contractions, especially after thefirst day of treatment. They also suggest that a
natural daily increase in both ventricular andsupraventricular arrhythmias occurred in the place-bo patients during the 5 days which followed anepisode of acute coronary insufficiency withoutinfaretion.Because the initial 48 hours after entry were
considered to be a very critical period fordevelopment of ventricular arrhythmias, the dataon ventricular arrhythmias for this period wereexamined during each of eight successive 6-hourintervals (fig. 2). The mean number of PVC's per 6-hour interval throughout the first 48 hours of study,including the first 6 hours, was lower in thequinidine-treated patients than in the placebo-treated patients, with placebo-quinidine differencesreaching statistical significance at the end of 24hours. Similarly the mean number of seriousventricular arrhythmias per 6-hour interval waslower in the quinidine-treated patients than inplacebo patients during these 48 hours except forthe first 6-12 hours (fig. 2). These data suggest thatduring the initial 48 hours after acute coronaryinsufficiency, quinidine afforded protection againstventricular arrhythmias, but that owing to thenatural history of these arrhythmias the protectionwas more obvious after than during the first 24hours.
Withdrawals from Study and Side Effects
Five patients were removed from study beforethe end of the study period (table 2). Two patients,who were not receiving digitalis, in the quinidinegroup were removed early from study because ofthe development of 2:1 atrioventricular block onthe second day of study in one patient andatrioventricular dissociation 5 hours after entry intothe study in the other. Two placebo-treated patientswere removed from the study early; one when itwas discovered that the prescribed study medica-tion had been omitted inadvertently, and the otherwas removed early by error. Finally, one patient inthe quinidine group died of subarachnoid hemor-rhage at the end of the first day of study. Onpostmortem examination significant coronary arterydisease (>50% narrowing in two vessels) waspresent in this patient and myocardial infarctionwas absent. On the average, quinidine-treatedpatients did not have appreciable widening of theQRS complex or prolongation of P-R and Q-Tintervals, nor did they show greater changes inheart rate and arterial pressure than patients givenplacebo. Side effects of nausea, vomiting, diarrheaor QRS prolongation greater than 25% of the
Circulation, Volume XLVII, May 1973
RC.QZL44-k
t4jco.41kllq
itk-1
.j11k
lq:h,
'Clii >,. k4.j k_ -11.,R (4j
(0) Q: tdR m
.d kikzt
W,.
'I
kJb,
,R.d oz1c.oz
-11%.c.l, (,.R it
1,111qR
tAi(0)k
RciRkkk
U -- E - - 9: aW10A V:
w.:
970
11
by guest on January 31, 2018http://circ.ahajournals.org/
Dow
nloaded from

PREVENTION OF ARRHYTHMIAS
PVC
cl PLACEBO (N=12)
n~ QUINIDINE ( N=11
6-12 2-18
i...:....:................
1t .- 1t
P<.05
1i
18 -24 24-30 30-36 36-42 42-48
HOURS AFTER ENTRY
SERIOUS VENTRICULAR ARRHYTHMIAS
||;4 ~~~~~~~~P<.10
2
0~~~ ~ ~ ~ ~~~~..
0-6 6-12 12-18 18-24 24-30 30-36
HOURS AFTER ENTRYFigure 2
36-42 42-48
Occurrence of ventricular arrhythmias during initial 48 hours of prophylactic quinidine or placebo therapy.
pretreatment tracing did not occur in any placeboor quinidine-treated patient.
Blood Quinidine Concentration
Mean blood quinidine concentrations at varioustimes after entry into study are shown in figure 3.At the sixth hour, the blood quinidine level was
Table 2
Number of Patients Removed beforePeriod
End of Study
No. of Heart Drug notGroup pt block received Other Totals
Placebo 12 0 1 1* 2Quiinidine 11 2 0 it 3Totals 23 2 1 2 5
*By error.tDied of subarachnoid hemorrhage.
Circulation, Volume XLVII, May 1973
3.3 + 0.5 (mean + SEM) mg/liter. A maximummean concentration of 5.2 + 0.5 mg/liter was
reached by the ninth hour after which a steady statewas in effect. From the arrhythmia data, it wouldappear that significant arrhythmia suppression withquinidine was present when steady state bloodlevels had been achieved.On the basis of these data, quinidine sulfate
given prophylactically at a dosage producingmodest blood concentrations appeared to be botheffective and safe for the prevention of ventricularand supraventricular arrhythmias that occurredduring the first 5 days after an episode of acutecoronary insufficiency without infarction.
DiscussionIn an earlier report5 on the efficacy of prophylac-
tic quinidine against cardiac arrhythmias after
50 F
40 h1*
P<.05P<.OI
A E~0LQ'
Q..
il~t) 4...i
P<.01
.1'.-.-. ...............
.....
30 k
20
1OF
,., W
0-6I IL
971
,. ..........
i......-
........
by guest on January 31, 2018http://circ.ahajournals.org/
Dow
nloaded from

BLOOMFIELD ET AL.
600
500
Xll6-
M 0 6 9 24 48 72 96
HOURS AFTER ENTRYFigure 3
Blood quinidine concentrations at various intervals during5 days of prophylactic quinidine therapy in 11 patients withacute coronary insufficiency.
rJ::R4C~
0)
14L4
0ti
Q PLACEBO- NON-INFARCT (N=12)
E PLACEBO-MYOCARDIAL INFARCT (N=26)
DAYS AFTER ENTRY
acute myocardial infarction, the present authorsobserved that over the course of the first 5 daysfollowing acute myocardial infarction there was anatural daily decline in numbers of supraventricularand ventricular arrhythmias of all degrees ofseverity. This progressive decrease in arrhythmiaswas present in both untreated (placebo) andquinidine-treated patients, such that the highestfrequency of arrhythmias occurred on the first dayafter acute myocardial infarction, and by the fifthday arrhythmias were virtually absent. By contrast,the data reported in the present paper show that incoronary heart disease patients with acute coronaryinsufficiency without infarction there is a reversal inthe natural history of arrhythmias (fig. 4). Inuntreated (placebo) patients with acute coronaryinsufficiency the lowest frequency of all arrhythmiasoccurred on the first day of study with progressivedaily increments such that by the fifth day thefrequency of cardiac arrhythmias was still increas-ing. Although this increase in PVC's is rathermarked in figure 4, it still represents only one PVCevery 2-3 min on day 5 and could represent abaseline level of PVC's for this group of patients.This difference in natural history of arrhythmias inpatients with acute coronary insufficiency withoutinfarction compared with patients having acuteinfarction is difficult to explain and certainly wasnot anticipated. These data suggest that there isincreasing excitability of myocardial tissue inpatients with acute coronary insufficiency, anddecreasing excitability of the myocardium inpatients with acute infarction. However, it ispossible that PVC's actually decreased during theinitial period of observation in the patients withacute coronary insufficiency because of treatment
.jc.z
.L1J
0)41
0)',-14.0)
LJ.jc.z
.4Q-
K0)
0)',-.14j0)
20
18
16
DAYS AFTER ENTRY
100 _
90 _
80
70
60
50
40
30 _
20
10 _
0 _2 3 4 5
DAYS AFTER ENTRY
Figure 4
Comparison of arrhythmias during each day of placebotherapy in 12 patients with acute coronary insufficiency and26 patients with acute myocardial infarction.
Circulation, Volume XLVII, May 1973
-
972
.....1........1......
by guest on January 31, 2018http://circ.ahajournals.org/
Dow
nloaded from

PREVENTION OF ARRHYTHMIAS
with oxygen, analgesics, and sedatives, and laterreturned to their baseline level.The protection afforded by quinidine in prevent-
ing the development of arrhythmias, althoughpresent in the early hours after an acute episode,did not reach statistical significance until the end of24 hours. This contrasts with the findings in patientswith acute myocardial infarction5 where the samedosage regimen of quinidine was found to affordsignificant protection as early as the sixth hour afterinitiation of therapy. One possible explanation forthis difference could be a need for higher bloodlevels of quinidine in patients with acute coronaryinsufficiency without infarction. This is supportedby the observation that arrhythmia suppression inthe latter patients occurred only when mean bloodquinidine concentrations reached a steady state inexcess of 4 mg/liter whereas in patients with acuteinfarction, arrhythmia suppression was present withmean concentration as low as 2.5 mg/liter. Thisfinding raises the possibility that arrhythmiasfollowing acute myocardial infarction are moreeasily suppressed by quinidine than arrhythmias incoronary heart disease without acute myocardialinfarction. However, other factors could also ac-count for the difference in arrhythmia protectionwith quinidine between coronary insufficiency andinfarct patients. These factors include differences inthe natural history of arrhythmias in these twoclinical conditions which, as already mentioned,would tend to show significant differences betweentreated and untreated patients as early as the firstday in patients with acute infarction but only laterin patients with acute coronary insufficiency.Furthermore, the number of coronary insufficiencypatients studied was less than half that of themyocardial infarction patients (N = 55) so thatsignificant differences between treated and untreat-ed coronary insufficiency patients might be difficultto demonstrate in the early hours when arrhythmiaswere quantitatively at a lower level of frequency.The effectiveness of quinidine in protecting
patients with acute coronary insufficiency againstarrhythmias was matched by its apparent lack ofsignificant toxicity. In view of the efficacy andsafety of prophylactic quinidine in suppressingarrhythmias in patients with acute coronary heart
disease it seems reasonable to suggest that prophy-lactic quinidine should be evaluated in a clinicaltrial to determine its effect on morbidity andmortality in ambulatory patients with coronaryartery disease, who are at high risk of suddendeath.
References1. SPANN JF, MOELLERING RC, HABER E, WHEELER EO:
Arrhythmias in acute myocardial infarction. New EngJ Med 271: 427, 1964
2. JULIAN DC, VALENTINE PA, MILLER GG: Distur-bances of rate, rhythm and conduction in acutemyocardial infarction. Amer J Med 37: 915, 1964
3. STOCK E, GOBLE A, SLOMAN G: Assessment ofarrhythmias in myocardial infarction. Brit Med J 2:719, 1967
4. LOWN B, FAKHRO AM, HOOD WB, THORN GW: Thecoronary care unit: New perspectives and directions.JAMA 199: 188, 1967
5. BLOOMFIELD SS, ROMmLT DW, CHOU TC, FOWLERNO: Quinidine for prophylaxis of arrhythmias inacute myocardial infarction. New Eng J Med 285:979, 1971
6. KOCH-WESER J, KLEIN SW, FOO-CANTO LL, KASTORJA, DESANCTIS RW: Antiarrhythmic prophylaxiswith procainamide in acute myocardial infarction.New Eng J Med 281: 1253, 1969
7. MOGENSON L: Ventricular tachyarrhythmias and ligno-caine prophylaxis in acute myocardial infarction. ActaMed Scand (suppl) 513: 39, 1970
8. KRAUSS KR, HUTTER AM, DESANCTIS RW: Acutecoronary insufficiency: Clinical course and follow-up.Circulation 44 (suppl II): II-102, 1971
9. AUER JE, JOHNSON VWD, FLEMMA RJ, TECTOR AJ,LEPLEY D: Direct coronary artery surgery forimpending myocardial infarction. Circulation 44(suppl II): II-102, 1971
10. DITLEFSEN E-ML: Concentrations of quinidine inblood following oral, parenteral and rectal adminis-tration. Acta Med Scand 146: 81, 1953
1 1. HINKLE LE JR, MEYER J, STEVENS M, CARVER ST:Tape recordings of the ECG of active men.Circulation 36: 752, 1967
12. ROMHILT DW, BLOOMFIELD SS, LIPICKY RJ, WELCHRM, FOWLER, NO: Evaluation of bretylium tosylatefor the treatment of premature ventricular contrac-tions. Circulation 45: 800, 1972
13. SIEGEL S: Nonparametric Statistics for the BehavioralSciences. New York, McCraw-Hhll Book Co, 1956
14. BRODIE BB, UDENFRIEND S: The estimation of quininein human plasma with a note on the estimation ofquinidine. J Pharmacol Exp Ther 78: 154, 1943
Circulation, Volume XLVII, May 1973
973
by guest on January 31, 2018http://circ.ahajournals.org/
Dow
nloaded from

SAUL S. BLOOMFIELD, DONALD W. ROMHILT, TE-CHUAN CHOU and NOBLE O. FOWLERAcute Coronary Insufficiency
Natural History of Cardiac Arrhythmias and their Prevention with Quinidine in Patients with
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1973 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.47.5.967
1973;47:967-973Circulation.
http://circ.ahajournals.org/content/47/5/967Wide Web at:
The online version of this article, along with updated information and services, is located on the World
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer in the
Permissions in the middle column of the Web page under Services. Further information about this process is availableOnce the online version of the published article for which permission is being requested is located, click Request
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Circulation Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on January 31, 2018http://circ.ahajournals.org/
Dow
nloaded from