why worry about the opioid prescribing crisis? · prescribing crisis? faculty/presenter disclosure...
TRANSCRIPT

Dr. Sharon Koivu Physician Consultant - Palliative Care; Supportive Team Addiction
Recovery, London Health Sciences Centre,
Associate Professor
Department of Family Medicine,
Western University
Why Worry About the Opioid
Prescribing Crisis?

Faculty/Presenter Disclosure
Faculty: Dr. Sharon Koivu Relationships with commercial interests: None • Grants/Research Support: None • Speakers Bureau/Honoraria: None • Consulting Fees: None • Other: None
Learning Objectives
1. Describe the concerns about the opioid prescribing crisis
2. Examine opioid issues in Palliative Care
3. Develop a rational approach to prescribing opioids in Palliative Care

Why Worry About the Opioid about the Prescribing Crisis?
1. We contributed to the crisis, we need to be part of the solution
2. We are a caring and compassionate cohort of health care professionals
3. OUD can be a palliative condition-HydroMorph Contin is killing people
4. Breaking bad….news; people with bad diagnoses may divert (or family members, care providers)
5. As cancer becomes a chronic illness we need to think about chronic problem
6. People suffering from OUD can get other life-limiting illnesses
7. We all need to prescribe opioids wisely

Deaths due to Prescription Opioids
• 1/8 young adult (age 25-34) deaths in Canada is from prescription opioid use
• Approximately 1 of every 170 deaths in Ontario is now related to opioid use.
• Opioid-related deaths result in ~ 22,000 years of potential life lost annually,
• Death by drug overdose is 3xs higher than deaths due to motor vehicle crashes as a cause of unintentional deaths, (2012,London,ON:MLHU)
• Most deaths occur in people who were prescribed opioids

Sherry C.
• Dr. Joanne Woods attended a prestigious medical school (HOTN)
• Her Palliative Care teaching promoted pain management, addiction risk low-people in pain cannot get addicted, no ceiling on opioids
• Books and lectures and conferences funded by P. Pharma, • Dr. Woods was very compassionate, she became a chronic
pain physician and opened a clinic funded by P. Pharma • Dr. Woods had patients sign contracts • OOC was OxyContin • Dose prescribed 2000 MME daily,200 MME as a prn • Some patients did not attend follow-ups

Sherry C.
• 2007 Sherry referred for Chronic abdominal pain related to Crohn’s Disease
• Started on OxyContin • 2010 Switched to Hydromorph Contin • 2012, 2013 and 2014 Admitted with TV endocarditis, Dr. Woods states she
would never inject • 2014 Sherry discloses OUD and Injection drug use • Dr. Woods fires her as a patient • Sherry experiences severe suffering, stigma, pain, SOB, • Denied TV surgery, • One Palliative Care physician refuses to see her as he does not see people
with addiction • Another PC physician consulted good pain and symptom management,
psycho-social and spiritual support • Sherry dies of complications of her OUD TV endocarditis

Opioid Use Disorder
A predictable complication of prescribing opioids
Occurs in 2-14% of all patients treated with opioids for chronic non-cancer pain
Highest in patients on doses greater than 90 MME per day
Comparable to nausea in frequency of side effects
Being in pain does not prevent opioid use disorder

• Estimated
Hospital cost
7.51 million
$/year
9
0
500
1000
1500
2000
2500
2007 2008 2009 2010 2011 2012 2013 2014 2015
Co
un
t (#
)
PWID-IE Hospital Days

10

Deaths due to Prescription Opioids has Surpassed Illicit Street Drugs!
• Deaths from infections related to IV drug use are not captured in most statistics
• May be greater 1/4 young adult deaths are related to opioid use

Complications of HydroMorph Contin Injection Drug Use
• HC Contain Carbohydrate and protein which promote the growth of bacteria and virus
• The particle in long-acting hydromorphone cause physical damage to blood vessels and heart vales
• The Tricuspid valve is particularly vulnerable to this bombardment
• The horded cookers and/or filters are likely to become contaminated
• This amounts to injecting fiberglass with a bacterial chaser!

Role of Palliative Care Provider
• Provide impeccable pain and symptom management throughout the duration of the illness
• Provide physical, psychosocial and spiritual for the patient and their family and friends.
• Recognize and advocate that addiction be treated as an illness requiring a health response and not a crime requiring a legal response
• Enhance screening • Facilitate viable treatment • Hope for cure • Always provide care

Case: Susan
• 2009 Breast Cancer
• Had Mastectomy, radiation
• Seen by PC physician
• Fentanyl 300 mmg q 72 hours.
• Always polite and thankful at appointments
• Oct 2016 states developed allergy to adhesive
• Switched to HydroMorph Contin 48 mg q 12h
• May 2017 resident does a urine drug screen, negative for opiates and hydromorphone

Opioid Selection, Dosage, Duration, Follow-Up, and Discontinuation
When opioids are started, clinicians should prescribe the lowest effective dosage.
Clinicians should use caution when prescribing opioids at any dosage, should carefully reassess evidence of individual benefits and risks when increasing dosage to ≥50 morphine milligram equivalents (MME)/day,
and should avoid increasing dosage to ≥90 MME/day or carefully justify a decision to titrate dosage to ≥90 MME/day.
Case: Cathy
Ovarian Cancer with brain metastases Admitted to hospital after a fall, Has a sudden decrease LOC CT scan of head negative, Noticed to have pin-point pupils, decreased respirations Patient had been reconciled to home medication Hydromorph Contin 24 mg q 12 h Improved at HydroMorph Contin 12 mg q 12 h • Daughter diverting

Misguided Physician Prescribing Habits has Contributed to the Problem • Almost all prescription opioids on the street
are prescribed drugs that have been diverted,
• The age group most likely to divert their drugs is:
60-75
People with bad diagnoses can have socio-economic problem or SUD which promote diversion

Misguided Physician Prescribing habits has Contributed to the Problem
• 14 % of adolescents say they have used prescription opioids recreationally
• 75% got them from the medicine cupboard in their own home
(OSDUHS 2011)
Tell all your patients to lock up their opioids
Opioids kill more people than loaded guns
Avoiding Diversion
Use of urine drug screening:
• prior to initiating opioid therapy
• Randomly as long as the opioid is being prescribe
• Do it universally like HIV testing in pregnancy
• To improve treatment strategies not punish.
Dispensing opioids:
• small volumes at a time eg 2 weeks worth,
• Consider life expectancy

Case: Don Smith
57 year old single male staying at Salvation Army Centre for Hope Problem list: • Locally advanced Squamous Cell Carcinoma • Post- obstructive pneumonia • Thoracotomy with lung decortication and debridement for
lung abscess (Jan., 2011) • Rt 3000 cGy in 10 fractions to the left lower lobe • Post thoracotomy pain syndrome • History of IV drug abuse including OxyContin and cocaine • Hep. C • Attends MMT x 4 years

Case: Don Smith
Medications:
1) Methadone 70mg/ day ( has been unable to get x 5 days due to weakness)
2) Fentanyl 100mcg q 72 hours (from LRCP)
3) Dexamethasone 4 mg. po bid
4) Gabapentin 300 mg tid
5) Lorazepam 1 mg tid prn

Case: Don Smith
• Don presents with weakness, nausea, chills, myalgia, diaphoresis
• Unable to get to MMT x 3 days due to illness
• He is afebrile
• Chest X-ray: Extensive left lower lobe related parenchymal and pleural changes in keeping with an empyema and possible lung abscesses.
(not much change from previous x-ray)

Case: Don Smith
Treatment:
• Metronidazole 500 mg po q8h
• Levofloxin 500 mg po q 48 h
• Fentanyl decrease to 75mcg q72h d/t fear weakness was opioid related
• Consideration given to discontinuing fentanyl and switching to Acetaminophen

Case: Don Smith
• Over next 24 hours: • Remains afebrile • Lkcs remain stable at20.5 • Increase in nausea, vomiting, chills, rhinorrhea, myalgia Issue? • He may or may not have an infection but he definitely has
withdrawal • Consider restarting Methadone in conjunction with his
provider Started on: • Hydromorphone 2 mg s/c q4h ATC and 1 mg s/c q1h prn • Titrated up to Hydromorphone 8 mg s/c q4h ATC and 2-4
mg s/c q1h prn

Marion L
• Breast cancer 2010 • Post chemo – dramatic increase in diffuse body pain Medication • OxyNeo 80mg TID • Metadol 25mg TID • Oxycodone 10mg up to 10/ day for BTP • Metadol 5mg up to 6/day for BTP • Non opioids:
– Gabapentin 900 tid – Duloxetine 90mg od – Meloxicam 7.5mg bid
Marion L
• Continued to complain of severe total body pain 9-10/10
• Opioid induced Hyperalgesia considered
• Instead of escalating, terminal sedation decision to rotate to Suboxone
• Buprenorphine 24mg sl/ day
• At least “40% better”
• Able to ‘be a mother’ to the kids
• Pain on average 5/10
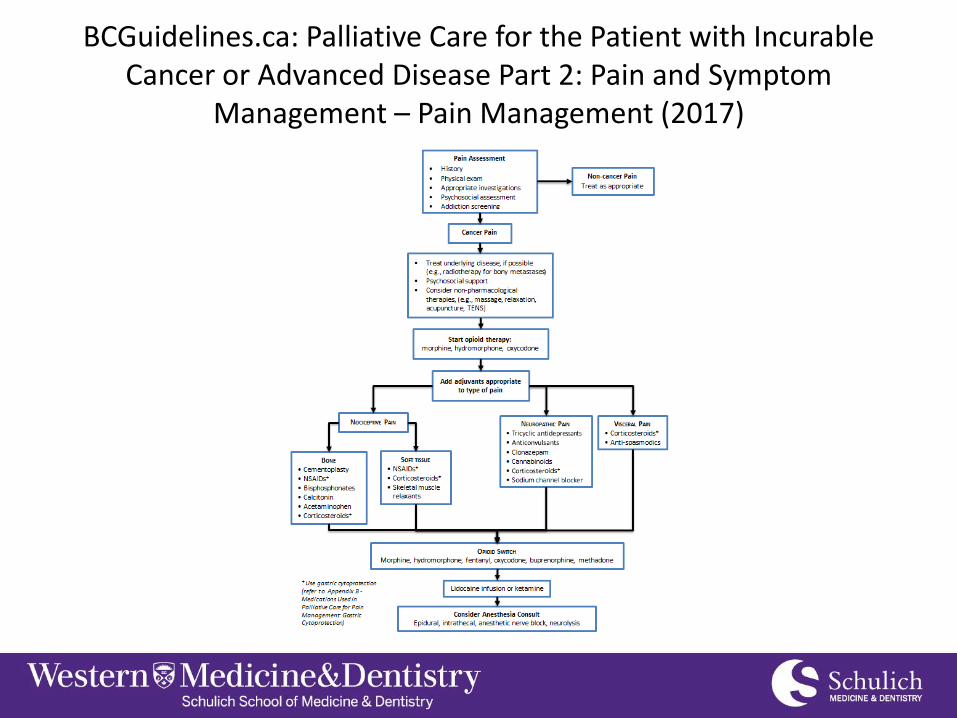
BCGuidelines.ca: Palliative Care for the Patient with Incurable Cancer or Advanced Disease Part 2: Pain and Symptom
Management – Pain Management (2017)

Prescribing opioids
• Manage pain compassionately • Consider OUD • Contemplate tapering if illness is chronic • Anticipate OIH • Consider OAT • Prevent diversion • Use universal precautions
– UDS – Small dispensing

Thank You