why measure cardiac output in critically ill children?
TRANSCRIPT

Radboud University NijmegenMedical Centre
J. LemsonAnesthesiologist/(pediatric)intensivist
Why measure cardiac output incritically ill children?
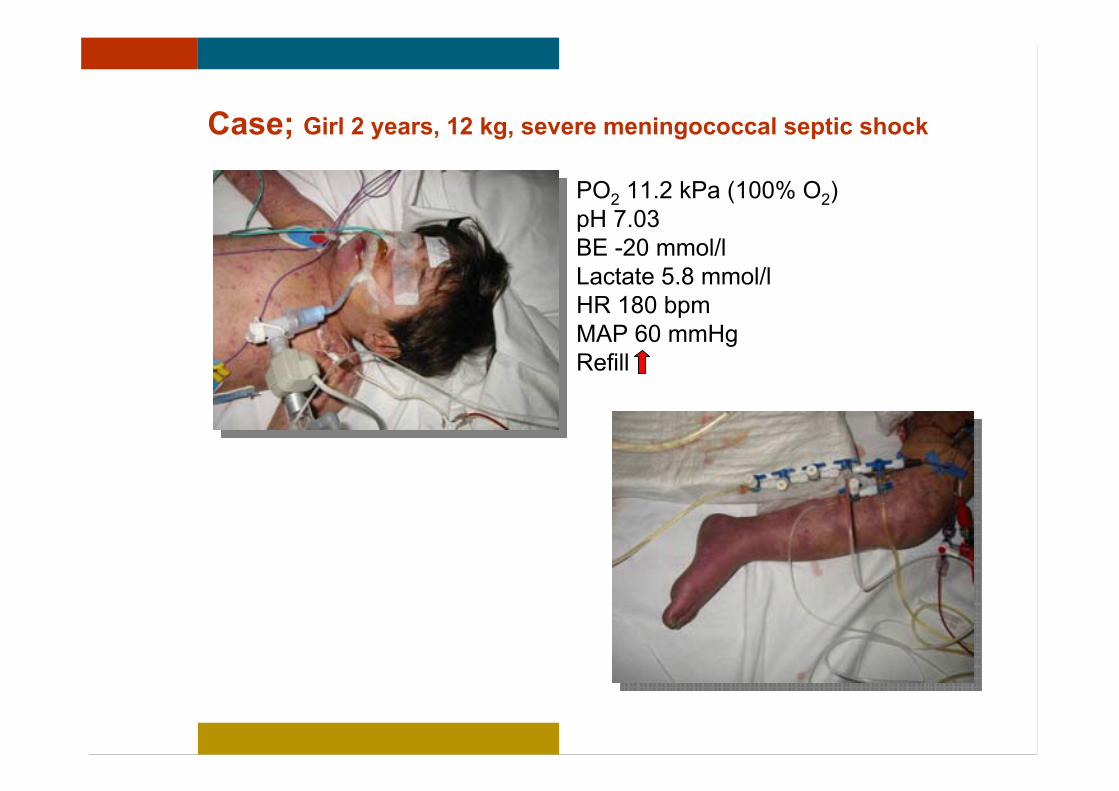
Case; Girl 2 years, 12 kg, severe meningococcal septic shock
PO2 11.2 kPa (100% O2)pH 7.03BE -20 mmol/lLactate 5.8 mmol/lHR 180 bpmMAP 60 mmHgRefill

CI 6.5 l/min/m2
Case; Girl 2 years, 12 kg, severe meningococcal septic shock
PO2 11.2 kPa (100% O2)pH 7.03BE -20 mmol/lLactate 5.8 mmol/lHR 180 bpmMAP 60 mmHgRefill

Hemodynamic monitoring in Brussels 2007 (adults)

Hemodynamic monitoring Geneva 2007

Lancet 2005; 366: 472–77
The Pulmonary Artery Catheter (PAC)
“…. our trial was never sufficiently powered to compare managementwith a PAC against no cardiac output monitoring”
=> Not all PAC trials concern cardiac output measurement itself!

PAC in children
Courtesy of dr. Jeroen Verwiel
The use of the PAC is not advised in (small) children
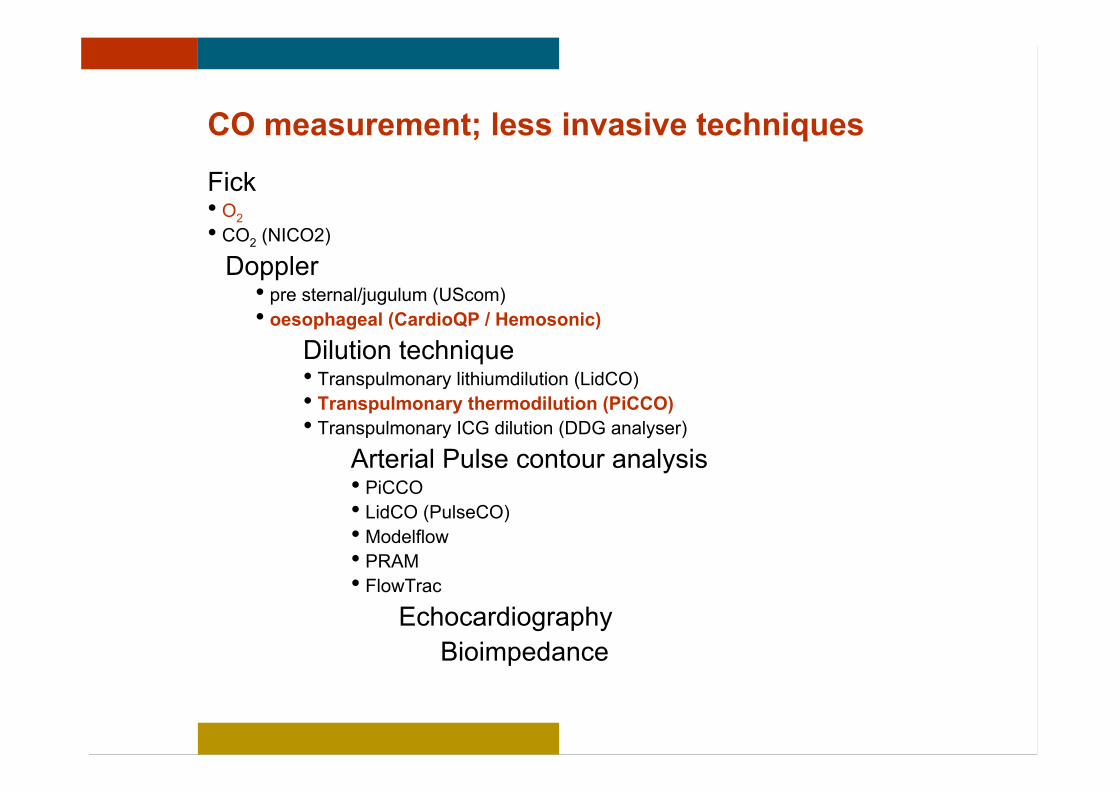
CO measurement; less invasive techniques
Fick• O2• CO2 (NICO2)Doppler• pre sternal/jugulum (UScom)• oesophageal (CardioQP / Hemosonic)
Dilution technique• Transpulmonary lithiumdilution (LidCO)• Transpulmonary thermodilution (PiCCO)• Transpulmonary ICG dilution (DDG analyser)
Arterial Pulse contour analysis• PiCCO• LidCO (PulseCO)• Modelflow• PRAM• FlowTrac
EchocardiographyBioimpedance

Controlled variable (baroreflex) PreloadAfterloadContractility
Basic haemodynamics

preload
SV
Basic haemodynamics
Normal contractility
Decreased contractility
Decreased myocardial contractility => decreased “margin of preload”

Crit Care Med 2002; 30:2191–2198
Septic cardiomyopathy
Effects of normal and meningococcal serum on rat myocyte contraction amplitude.

Inflammation
Pediatr Crit Care Med 2003; 4:299 –304
Neonates and infants undergoing congenital cardiac surgery usingcardiopulmonary bypass.

Patients undergoing CPB with neonate or infants group.
Eur J of Cardio-thoracic Surg 1997; 12: 862–868
Inflammation

Crit Care Med 2007; 35:1599 – 1608
Inflammation
Inflammation
Sepsis
Surgery / Trauma
Myocardial dysfunctionIncreased capillary permeabilityVasodilation
Autonomic dysregulation
Cardiovascular Research 2007;73:26–36
(Younger children more susceptible ?)

Arch Dis Child 1997;77:516–518
Clinical estimation of cardiac output

Heart rate and cardiac output
N = 11; Newborn animal modelFluid resuscitation (10 ml/kg) from hypovolemic shock
R2 = 0,0213
-100
-50
0
50
100
150
200
250
-30 -20 -10 0 10 20 30
HR (%)
cardiacoutput(%)
J. Lemson et al; accepted Ped Crit Care Med 2007

J. Lemson et al. Europediatrics 2006
R2 = 0,2446
-3
-2
-1
0
1
2
3
-60 -40 -20 0 20 40
HR (bpm)
cardiacindex(l/min/m
2 )
N = 13; critically ill children (2 months - 8 years)
Heart rate and cardiac output

-120
-100
-80
-60
-40
-20
0
20
40
60
-40 -30 -20 -10 0 10 20 30 40
delta CO (%)
deltaMAP(%)
-120
-100
-80
-60
-40
-20
0
20
40
60
-40 -30 -20 -10 0 10 20 30 40
delta CO (%)
deltaMAP(%)
MAP and cardiac output
J. Lemson et al. Europediatrics 2006
N = 13; critically ill children (2 months - 8 years)

n = 15; age 3 – 264 hoursEffect of 20 ml/kg fluid loading
Before After p-value
HR (bpm) 140 (125–164) 139 (119–187) NS
MAP (mmHg) 33 (22–40) 37 (31–60) < 0.005
CI (ml/min/kg) 295 (134–376) 323 (182–382) < 0.01
FS (%) 33 (23–40) 32 (23–44) NS
Int Care Med 1997;23:982-986
Stroke volume and cardiac output

-50
0
50
100
150
200
-100 -50 0 50 100 150 200 250
delta CO (%)
delta
SV(%)
-50
0
50
100
150
200
-100 -50 0 50 100 150 200 250
delta CO (%)
delta
SV(%)
J. Lemson et al; accepted Ped Crit Care Med 2007
Stroke volume and cardiac output
N = 11; Newborn animal modelFluid resuscitation (10 ml/kg) from hypovolemic shock

JAMA 1991;266:1242-1245
• 34 patients (median age 13.5 months) with septic shock.• Rapid fluid resuscitation in excess of 40 mL/kg in the first hour followingemergency department presentation was associated with improvedsurvival…..
Give enough fluids….
N Engl J Med 2001;345:1368-1377
Early goal directed therapy (“Rivers study”)

Chest 2005;128;3098-3108
Variables Odds Ratio (95% Confidence Interval)Cancer 4.4 (1.6–12.1)High tidal volume 2.3 (1.2–4.4)Mean SOFA score 1.4 (1.3–1.6)Mean fluid balance 1.5 (1.1–1.9)
3147 adult patients with acute lung injury
Sepsis Occurrence in Acutely Ill Patients (SOAP) network in 24 European countriesduring a 14-day period from May 1, 2002, to May 15, 2002.
But not to much! …..

Kidney International, 2005;67:653–658
Higher fluid balance => higher mortality
Variable Survivors Non-survivors p value
Patient age (years) 8.49 ± 6.74 8.51 ± 7.19 NS
PRISM 2 at PICU admit 14.3 ± 8.2 16.2 ± 9.7 NS
Fluid overload (%) 14.2 ± 15.9 25.4 ± 32.9 <0.03
116 children with MODS requiring renal replacement therapy

Fluid resuscitation
increase preload cardiac output
“fluid responsive”

Fluid resuscitation
increase preload cardiac output =
risk of fluid “overloading”
Neth J Med 2000;57:82-93Acta Anaesthesiol Scand 2004;8:69-73

Fluid resuscitation
increase preload cardiac output
“fluid responsive”Fluid responsiveness adults• Arterial pressure variation• Global end diastolic volume (GEDV)• Passive leg raising• etc

Fluid resuscitation
increase preload cardiac output
“fluid responsive”Fluid responsiveness children?????????
?

1. Clinical parameters, heart rate and blood pressure do notreflect changes in cardiac output
2. Cardiac output measurement is the cornerstone inhaemodynamic management of children
3. Advanced hemodynamic monitoring could be beneficial
Conclusion
Radboud University NijmegenMedical Centre

PiCCOplus
Calorimeter(Fick)
NICO2
USCom
COLD
CCO (PAC)
BoMed
CardioQP
PiCCO
What’s it all about?

What’s it all about?
“No monitoring device, no matter how simple or sophisticated, willimprove patient-centered outcomes unless coupled with a treatment that,itself, improves outcome……”
Pinsky & Vincent
Crit Care Med 2005;33:1119-1122

The author has no financial or other relationship that might leadto a conflict of interest
Statement
