why are the blind and severely visually impaired children with mental retardation much more retarded...
TRANSCRIPT

S Y M P O S I U M E A R L Y V I S U A L D E V E L O P M E N T March 1982, Solna, Sweden
Acta Ophthalmol (Copenh). Suppll57: 72-81
B$rnehospatulet i Vungede, Gentofte, Denmark
WHY ARE THE BLIND AND SEVERELY VISUALLY IMPAIRED CHILDREN WITH
MENTAL RETARDATION MUCH MORE RETARDED THAN THE SIGHTED CHILDREN?
BY
M E T E WARBURG
Five per cent of mentally retarded children in Denmark have a visual acuity below 6/60 as compared to 0.02% in the normal child population. Profound mental retardation was more prevalent among the visually impaired than among the sighted patients. An analysis was performed concerning the correlation between the degree of retardation and the severity of visual impairment, chronological age, number of complicating signs, and degree of motor impairment. The degree of mental retardation was also compared with the aetiology of visual impairment. Severe motor impairment was dosely correlated with profound mental retardation.
K P ~ words: causes of blindness - education - child development - brain damage - motor function.
When Lilli Nielsen, teacher for the blind, and I began our cooperation in the beginning of the 1970’s, we felt that the prevalence of profound mental retardation was much higher among the blind than among the sighted mentally retarded children. A screening for blindness and severe visual impairment in 1976 (Warburg et al. 1979) confirmed this opinion (Table 1).
72
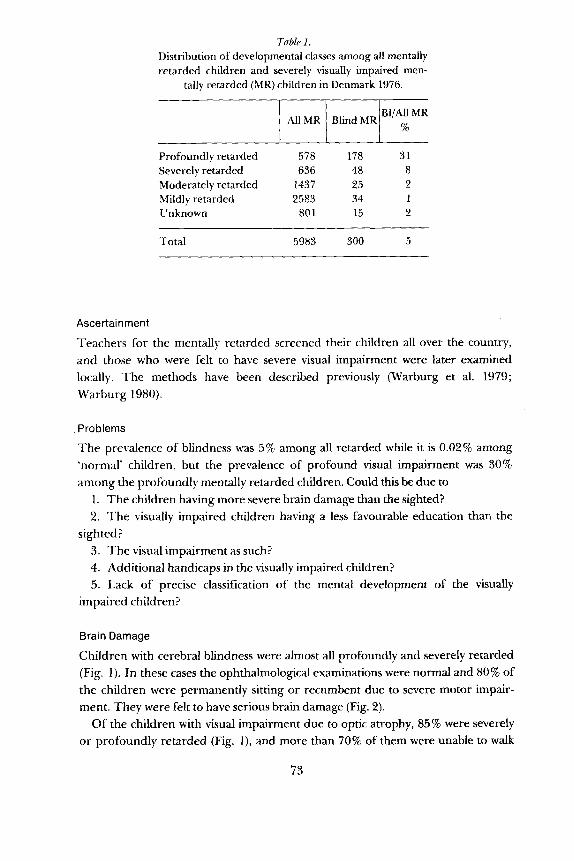
Table I . Distribution of developmental classes among all mentally retarded children and severely visually impaired men-
tally retarded (MR) children in Denmark 1976.
AllMR BlindMR % I I I B ” A 1 l M R I
Profoundly retarded 578 178 31 Severely retarded 636 48 8 Moderately retarded 1437 25 2 Mildly retarded 2583 34 1 Unknown 80 1 15 2
Total 5983 300 5
Ascertainment
Teachers for the mentally retarded screened their children all over the country, and those who were felt to have severe visual impairment were later examined locally. The methods have been described previously (Warburg et al. 1979; Warburg 1980).
Problems
The prevalence of blindness was 5% among all retarded while it is 0.02% among ‘normal’ children, but the prevalence of profound visual impairment was 30% among the profoundly mentally retarded children. Could this be due to
1. The children having more severe brain damage than the sighted? 2. The visually impaired children having a less favourable education than the
3. The visual impairment as such? 4. Additional handicaps in the visually impaired children? 5. Lack of precise classification of the mental development of the visually
sighted?
impaired children?
Brain Damage
Children with cerebral blindness were almost all profoundly and severely retarded (Fig. 1). In these cases the ophthalmological examinations were normal and 80% of the children were permanently sitting or recumbent due to severe motor impair- ment. They were felt to have serious brain damage (Fig. 2).
Of the children with visual impairment due to optic atrophy, 85 % were severely or profoundly retarded (Fig. 1) . and more than 70% of them were unable to walk
73

DIAGNOSES AND PRESENTING MENTAL FUNCTION
100
80
$ 6o
$ 4 0
c,
20
0
PROFOUNDLY AND SEVERELY R E T A R D E D U MILDLY AND MODERATELY RETARDED
Fzg I Diagnoses and presenting mental functlon among 300 severely and profoundly visually impaired children with mental retardation and among all mentally retarded children in
Denmark 1976.
(Fig. 2). The optic atrophy was caused by the brain disorder giving rise to mental retardation.
There were 121 children whose visual impairment was due to ordinary ocular disorders (Table 2). Even among these, the prevalence of severe and profound
GROSS MOTOR FUNCTION AND DIAGNOSES
Fig. 2. Gross motor function and diagnoses among 300 severely and profoundly visually impaired
children with mental retardation. L: lying down, S: citting, W: walking.
74

Table 2. Ocular causes of visual impairment and class of
development.
Diagnosis 1 Function I Function High IUnXnown/Total
Congenital cataract 14 5 1 20
9 4 4 17 Retinopathy of prematurity
6 18 3 27 Tapeto-retinal degeneration
Other causes 41 13 3 57
Total 70 40 11 121
mental retardation was conspicuous, and only 60% of them were able to walk (Fig. 2). Complications such as epilepsy, spasticity or hearing impairment were less pronounced among children with ocular causes of visual impairment than among the others (Fig. 3).
THUS; Although severe brain damage was an important cause of severe mental retardation, visually impaired children with less severe brain damage showed astonishing severe psychomotor retardation.
Education
In 1976 only very few of the visually and mentally impaired children had special education by teachers for the blind. If some child was thought to benefit from special education he would be transferred to the school for the blind or to local classes with special education, Very few children had such opportunity, we had contact with the school for the blind and were told that no mentally retarded pupil was living there at the time of the study.
THUS: The visually handicapped children who were mentally retarded had a less favourable education than the sighted retarded and than other visually retarded children. This has been changed to-day.
Visual Impairment
The distribution between the developmental classes observed among the children is seen from Fig. 4. There is no significant difference between children without
75
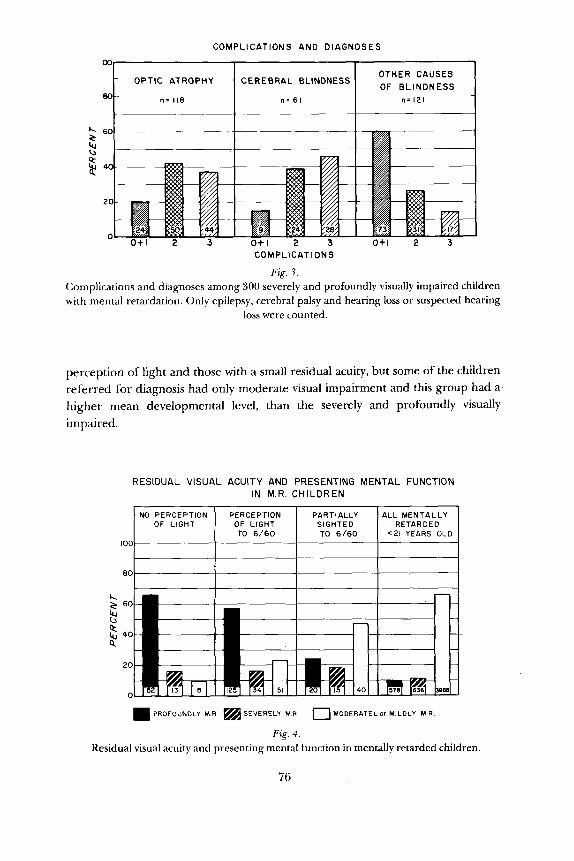
COMPLICATIONS AND DIAGNOSES
80-
OTHER CAUSES OPTIC ATROPHY CEREBRAL BLINDNESS
n = 118 n = 61 n = 121
COMPLICATIONS
Fig. 3. Complications and diagnoses among 300 severely and profoundly visually impaired children with mental retardation. Only epilepsy, cerebral palsy and hearing loss or suspected hearing
loss were counted.
perception of light and those with a small residual acuity, but some of the children referred for diagnosis had only moderate visual impairment and this group had a higher mean developmental level, than the severely and profoundly visually impaired.
RESIDUAL VISUAL ACUITY AND PRESENTING MENTAL FUNCTION IN M.R. CHILDREN
OF LIGHT OF LIGHT SIGHTED RETARDED
80
PROFOUNDLY M R SEVERELY M R
Fig. 4 . Residual visual acuity and presenting mental function in mentally retarded children.
76
0 MOOERATEL or MILDLY M R
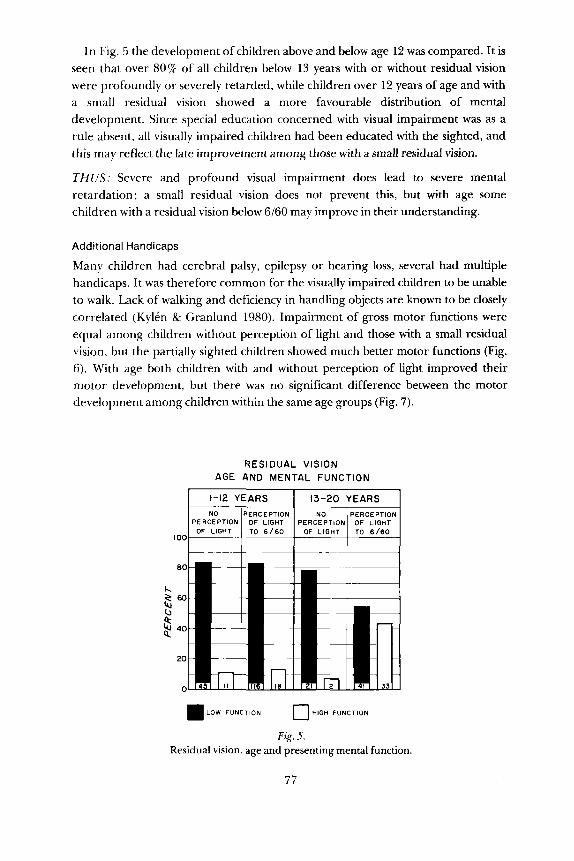
In Fig. 5 the development of children above and below age 12 was compared. It is seen that over 80% of all children below 13 years with or without residual vision were profoundly or severely retarded, while children over 12 years of age and with a small residual vision showed a more favourable distribution of mental development. Since special education concerned with visual impairment was as a rule absent, all visually impaired children had been educated with the sighted, and this may reflect the late improvement among those with a small residual vision.
THUS: Severe and profound visual impairment does lead to severe mental retardation; a small residual vision does not prevent this, but with age some children with a residual vision below 6/60 may improve in their understanding.
Additional Handicaps
Manv children had cerebral palsy, epilepsy or hearing loss, several had multiple handicaps. It was therefore common for the visually impaired children to be unable to walk. Lack of walking and deficiency in handling objects are known to be closely correlated (Kylen & Granlund 1980). Impairment of gross motor functions were equal among children without perception of light and those with a small residual vision, but the partially sighted children showed much better motor functions (Fig. 6). With age both children with and without perception of light improved their motor development, but there was no significant difference between the motor development among children within the same age groups (Fig. 7).
RESl DUAL VISION AGE AND MENTAL FUNCTION
I00
LOW FUNCTION 0 HIGH FUNCTION
Fig. 5. Residual vision, age and presenting mental function.
77

R E S I D U A L VISUAL ACUITY AND GROSS MOTOR S K I L L
100
80
c, 2 6o
2 $ 4o
20
0
SITTING WITH SUPPORT AND 4 L O N E 4 N D 4 L O N E
0 W4LKlNG WITH SUPPORT
Fig. 6. Residual visual acuity and gross motor skills among mentally retarded children with visual
impairment.
RESIDUAL V I S I O N AGE AND GROSS MOTOR FUNCTION
8
6
4
2
h
~ ~~
1-12 Y E A R S 1 13-20 YEARS
60
40
20
0
L Y I N G or S I T T I N G 0 W 4 L K l N G
Fig. 7. Residual visual acuity, age and gross motor function among mentally retarded children.
78
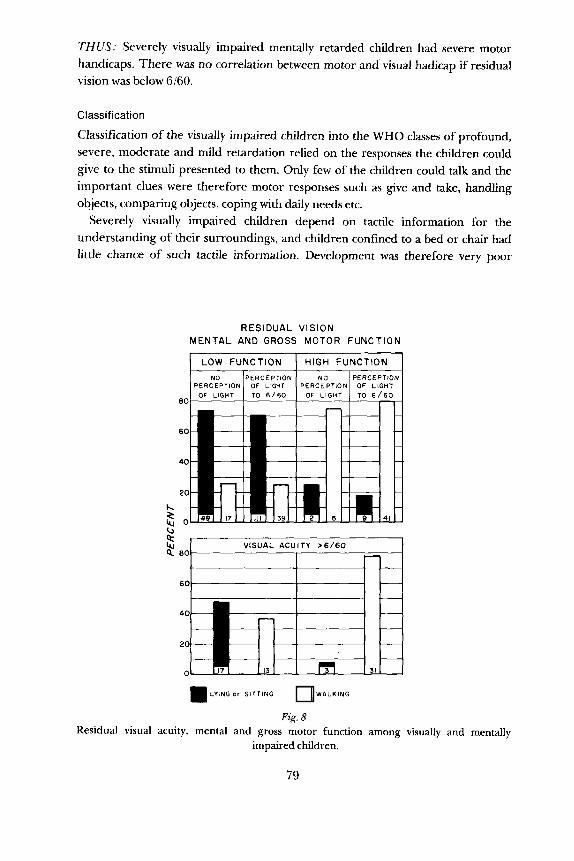
THUS; Severely visually impaired mentally retarded children had severe motor handicaps. There was no correlation between motor and visual hadicap if residual vision was below 6160.
L O W FUNCTION
NO PERCEPrlON PERCEPTION OF LIGHT
Classification
Classification of the visually impaired children into the WHO classes of profound, severe, moderate and mild retardation relied on the responses the children could give to the stimuli presented to them. Only few of the children could talk and the important clues were therefore motor responses such as give and take, handling objects, comparing objects, coping with daily needs etc.
Severely visually impaired children depend on tactile information for the understanding of their surroundings, and children confined to a bed or chair had little chance of such tactile information. Development was therefore very poor
HIGH FUNCTION NO PERCEPTION
PERCEPTION OF LIGHT
RESIDUAL VISION MENTAL AND GROSS MOTOR FUNCTION
u VISUAL ACUITY >6 /60
n
20 40E! 0 31 - =LYING or SITTING WALKING
Fig. 8. Residual visual acuity, mental and gross motor function among visually and mentally
impaired children.
79
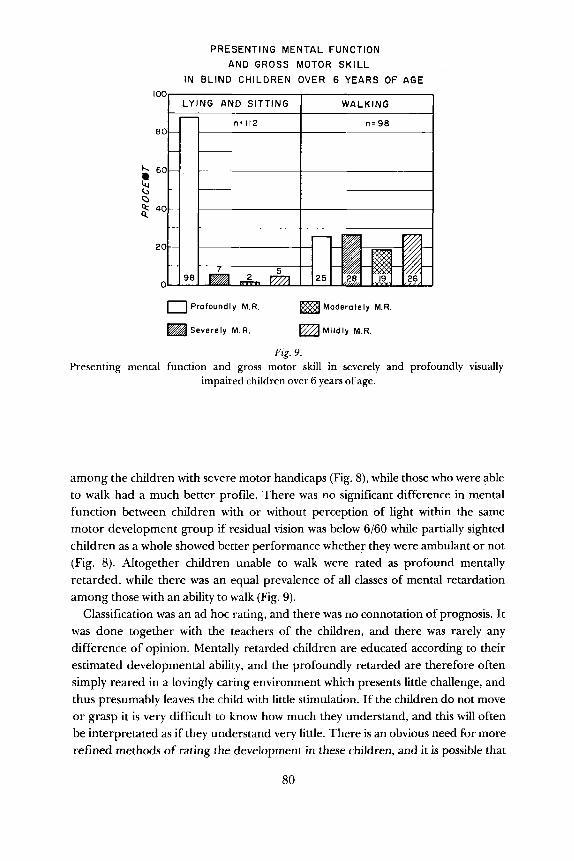
PRESENTING MENTAL FUNCTION AND GROSS MOTOR SKILL
IN BLIND CHILDREN OVER 6 YEARS OF AGE
80
60
0 2 40 t
20
Presenting mental
0 Profoundly M.R. Moderately M.R.
Severely M.R. Mildly M.R.
Fig. 9.
impaired children over 6 years of age. function and gross motor skill in severely and profoundly visually
among the children with severe motor handicaps (Fig. 8), while those who were able to walk had a much better profile. There was no significant difference in mental function between children with or without perception of light within the same motor development group if residual vision was below 6/60 while partially sighted children as a whole showed better performance whether they were ambulant or not (Fig. 8). Altogether children unable to walk were rated as profound mentally retarded, while there was an equal prevalence of all classes of mental retardation among those with an ability to walk (Fig. 9).
Classification was an ad hoc rating, and there was no connotation of prognosis. It was done together with the teachers of the children, and there was rarely any difference of opinion. Mentally retarded children are educated according to their estimated developmental ability, and the profoundly retarded are therefore often simply reared in a lovingly caring environment which presents little challenge, and thus presumably leaves the child with little stimulation. If the children do not move or grasp it is very difficult to know how much they understand, and this will often be interpretated as if they understand very little. There is an obvious need for more refined methods of rating the development in these children, and it is possible that
80

assessment of profound mental retardation in severely visually impaired children is to some extent influenced by deficiency of communication.
The distribution of developmental classes among the ambulatory children showed that it was possible to assess development among visually impaired retarded children and also that it needs more than the ability to walk for a visually impaired child to be rated among those with a fairly high mental function.
THC’S: There is a need of precise assessment of development among visually impaired children with deficient gross motor function, but those who can walk (and grasp) can be differentially rated.
Conclusion
Visual impairment among mentally retarded children is sometimes due to severe brain damage, but some children without serious brain damage and reared among sighted retarded children show a remarkable low development. This may be due to lack of special education but lack of motor development is probably the most important single cause. The difficulty in assessing development in visually impaired children with deficient gross motor function may lead to lack of assessment of their ‘signals’ and thereby give rise to a viscious circle, so that a child is given education as if he was profoundly retarded.
References
Warburg M, Frederiksen P & Rattleff J (1979): Blindness among 7700 mentally retarded children. In: Smith V & Keen J (eds). Visual Handicap in Children. Clin Dev Med 73: 56-69. Spastics International Med Pub1 with Heinemann Med. London, Philadelphia.
Warburg M (1980): Blindhed blandt mentalt retarderede b0rn. Bib1 f Lzg 172: 133- 152. Kylkn G & Granlund M (1980): Forstindshandikappade vuxna p i A-stadiet. ALA Liber
Forlag, Stockholm
Author’s address: Mette Warburg, M.D., B0rnehospitalet i Vangede, Sognevej 40, DK-2820 Gentofte, Denmark
81 Supplemenium 157 6