who prequalification of in-vitro diagnostics, medicines ... · “pqtm’s mission is to work in...
TRANSCRIPT

WHO PREQUALIFICATION TEAM
01 - 05 October 2018
WHO Prequalification of in-vitro diagnostics,
medicines, vaccines and vector control products
WHO Prequalification – contributing to access to
quality assured products and regulatory
harmonization
Deus Mubangizi
PQT Coordinator
WHO Technical Briefing Seminar Essential
Medicines and Health Products
Geneva, Switzerland

WHO PREQUALIFICATION TEAM
Outline of the presentation – PQ and its contribution to MDGs, SDG and 13th GPW – Organisation structure & procedures of PQT – PQ Transparency: Website and guidance documents Key numbers, product pipeline
– Updates on: New SRA definition New funding model and KPIs New PQT IT solution Collaborative registration procedure and harmonization
activities – WHO-PQT: Looking to the future – Take home messages

WHO PREQUALIFICATION PROGRAMME
3 • WHO-PQ contributed to the Millennium Development Goals (MDGs):
• Eight international development goals that 192 United Nations member states and at least 23 international organizations have agreed to achieve by the year 2015
4. Reduce child mortality
5. Improve maternal Health
6. Combat HIV/AIDs, Malaria and other diseases
WHO PREQUALIFICATION PROGRAMME
4
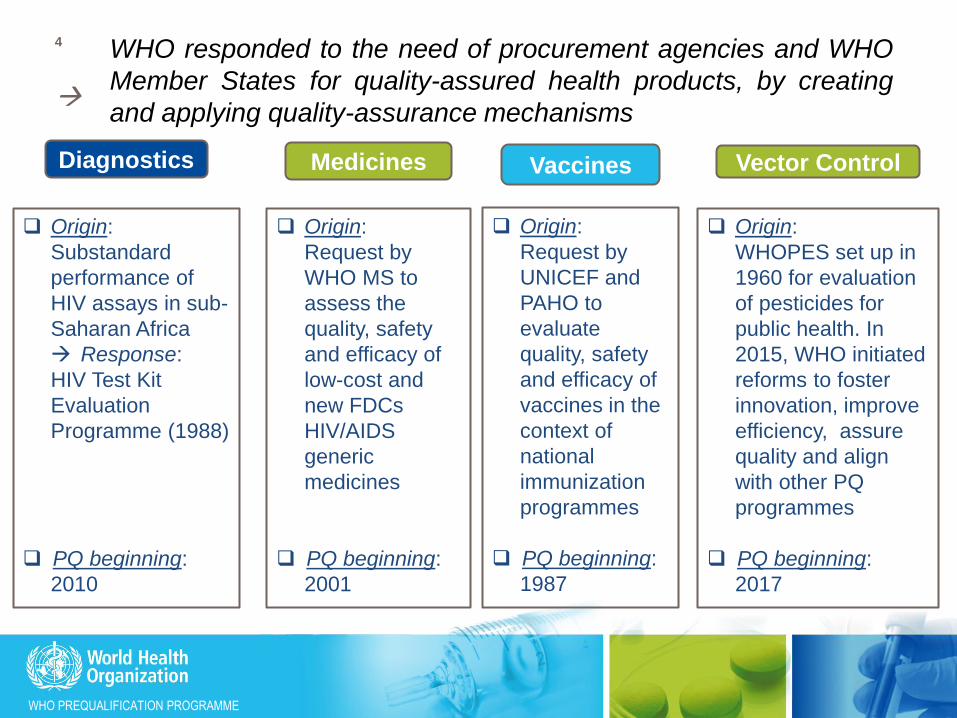
WHO responded to the need of procurement agencies and WHO
Member States for quality-assured health products, by creating
and applying quality-assurance mechanisms
Diagnostics Vaccines Medicines
Origin:
Substandard
performance of
HIV assays in sub-
Saharan Africa
Response:
HIV Test Kit
Evaluation
Programme (1988)
PQ beginning:
2010
Origin:
Request by
UNICEF and
PAHO to
evaluate
quality, safety
and efficacy of
vaccines in the
context of
national
immunization
programmes
PQ beginning:
1987
Origin:
Request by
WHO MS to
assess the
quality, safety
and efficacy of
low-cost and
new FDCs
HIV/AIDS
generic
medicines
PQ beginning:
2001
Vector Control
Origin:
WHOPES set up in
1960 for evaluation
of pesticides for
public health. In
2015, WHO initiated
reforms to foster
innovation, improve
efficiency, assure
quality and align
with other PQ
programmes
PQ beginning:
2017

WHO PREQUALIFICATION PROGRAMME
WHO-PQ contributes to the achievement of
Sustainable Development Goals (SDGs) http://www.un.org/sustainabledevelopment/sustainable-development-goals/

WHO PREQUALIFICATION TEAM
6
WHO-PQ by making safe quality priority health products available
through efficient and scientifically solid assessment contributes to
achieving SDGs and UHC. SDG 3 targets by 2030 include:
reduce the global maternal mortality
end preventable deaths of newborns and children under 5 years of
age,
end the epidemics of AIDS, tuberculosis, malaria and neglected
tropical diseases and combat hepatitis, water-borne diseases and
other communicable diseases
ensure universal access to sexual and reproductive health-care
services, including for family planning
Achieve universal health coverage, including access to quality
essential health-care services and access to safe, effective, quality
and affordable essential medicines and vaccines for all
Support the research and development of vaccines and medicines for
the communicable and noncommunicable diseases that primarily
affect developing countries and provide access to medicines for all
Background

WHO PREQUALIFICATION TEAM 7
Key Themes of WHO’s 13th
General Programme of Work
2019-2023 Mission Promote Health - Keep the World Safe - Serve the Vulnerable
Strategic Priorities
Health Coverage: 1 billion more people with health coverage
Health Emergencies: 1 billion more people made safer
Health Priorities: 1 billion lives improved
Strategic Shifts
Set up
global
leadership
Focus
global
public
goods
on
impact
Drive impact in every country
Policy dialogue Strategic support
Technical assistance
Service delivery
Fragile health system Mature health system

WHO PREQUALIFICATION TEAM
8
PQ will contribute to the 13th General Programme of Work
(GPW 2019-2023) “The Organization will continue to support the availability of quality-assured
generic products for procurement by global agencies and countries through
the WHO prequalification Programme, which will evolve to meet the
changing health needs of countries.”
PQ through the EUAL will contribute to:
“ensure that populations affected by emergencies have rapid access to essential
life-saving health services.”
“Ensure that populations affected by health emergencies have access to
essential life-saving health services and public health interventions;”
PQ will contribute to the Heath priorities:
Women, children and adolescent health
Reduce maternal deaths (maternal mortality ratio) by 50% (RH)
Reduce the rate of under-five child deaths by 30% (D, Vx, Dx)
Increase degree to which contraceptive demand is satisfied through modern
methods by 10% (RH)
Increase coverage of cervical cancer vaccine by 40 percentage points (SBP)

WHO PREQUALIFICATION TEAM
9
PQ will contribute to the 13thGPW Heath priorities…
HIV, Tuberculosis, malaria, hepatitis, neglected tropical
diseases, antimicrobial resistance and polio At least 1 million fewer new HIV infections per year
Reduce deaths from tuberculosis by 50%
Reduce malaria deaths by 50%
Prevent half a million deaths per year from hepatitis B and C virus related
liver disease
Eliminate at least one neglected tropical disease in 35 countries
Eradicate polio: zero cases of poliomyelitis caused by wild poliovirus or
circulating vaccine-derived poliovirus
Increase coverage of treatment for multidrug- and rifampicin-resistant
tuberculosis to 80% of estimated incidence
Noncommunicable diseases (NCDs), mental health, substance use, road
traffic injuries
Reduce prevalence of raised blood pressure by 20%

WHO PREQUALIFICATION TEAM
10
PQ already designed to fit in the 13th GPW strategic shifts
Step global leadership:
PQ has been recognised as a stamp of quality and a point of reference
for QA for UN, International, regional and national procurement
Drive impact in every country:
Programmatic suitability built in Vx PQ
Focus on EID and RDTs for use in resource limited settings
Collaborative procedure, harmonization and capacity building
Placing countries at the centre:
“PQTm’s mission is to work in close cooperation with national regulatory
agencies and partner organizations to make quality priority medicines available for
those who urgently need them. This is achieved through assessment and inspection
activities, building national capacity for manufacture, regulation and monitoring
of medicines, and working with regulators to register those medicines
quickly.” https://extranet.who.int/prequal/content/overview-history-mission
Each bimonthly assessment session in CPH attracts ≥50 experts from
across the globe, ≥35 from LMICs and ≥15 from well resourced NRMAs –
best impact on capacity building and promoting convergence
WHO PREQUALIFICATION TEAM
Outline of the presentation – PQ and its contribution to MDGs, SDG and 13th GPW – Organisation structure & procedures of PQT – Transparency: Website and guidance documents Key numbers, product pipeline
– Updates on: New SRA definition New funding model and KPIs New PQT IT solution Collaborative registration procedure and harmonization
activities – WHO-PQT: Looking to the future – Take home messages

WHO PREQUALIFICATION TEAM
Structure of the Prequalification Team
Prequalification Team
Vaccines Assessment
Medicines Assessment
Diagnostics Assessment
Inspections Vector control
Coordinator’s office

WHO PREQUALIFICATION TEAM
Product eligibility: Based on WHO Member States needs, WHO disease programmes set eligibility
criteria and determine priorities for prequalification
Diagnostics
In vitro diagnostics (IVD) & male
circumcision device (MCD)
Medicines Finished pharmaceutical
product (FPP), active pharm ingredient (API), quality control lab (QCL)
Vaccines
Vaccines (Vx), Immunization device
(ImD) & cold chain equipment (CCE)
Vector Control
VC Products (VCP) (VCPs: FPPs & APIs)
Larvicides Long-lasting
insecticidal nets Indoor residual
spraying products Space spraying
products
24 priority diseases, covering vaccines required for routine immunization
Eligibility criteria for evaluation includes NRA functionality & programmatic suitability
HIV/AIDS Malaria Tuberculosis Diarrhoea Influenza Reproductive
Health Neglected tropical
diseases (NTDs)
HIV/AIDS Hep B Hep C HPV Malaria G6PD Cholera Syphilis
80 IVD 2 MCD 312FPP 129 API
44 QCL
148 Vx (327 Vx*)
400 ImDs/CCE
71 VCP
(Cumulative numbers of PQed products: August 2018)
Hep B Hep C
NEW: as of Jan 2017
Vx*: covering all dosage forms 13

WHO PREQUALIFICATION TEAM
14
For each type of product, prequalification includes a comprehensive dossier
assessment and a manufacturing site inspection, as well as other product-
specific elements of evaluation
Prequalification workflow
NRA functionality
Programmatic suitability
Lab
evaluation
Dossier
submission
Screening
Assessment Inspection
CAPA
Follow-up
inspection
CAPA
Prequalification decision
Pre-submission
form
Maintenance and monitoring Collaborative registration
Routine inspections Special inspections Handling complaints
Variations Annual reports Requalification
Inspection closing letter Letter of prequalification Web listing Public reports (WHOPAR, WHOPIR)
Follow-up NOC
WHO PREQUALIFICATION PROGRAMME
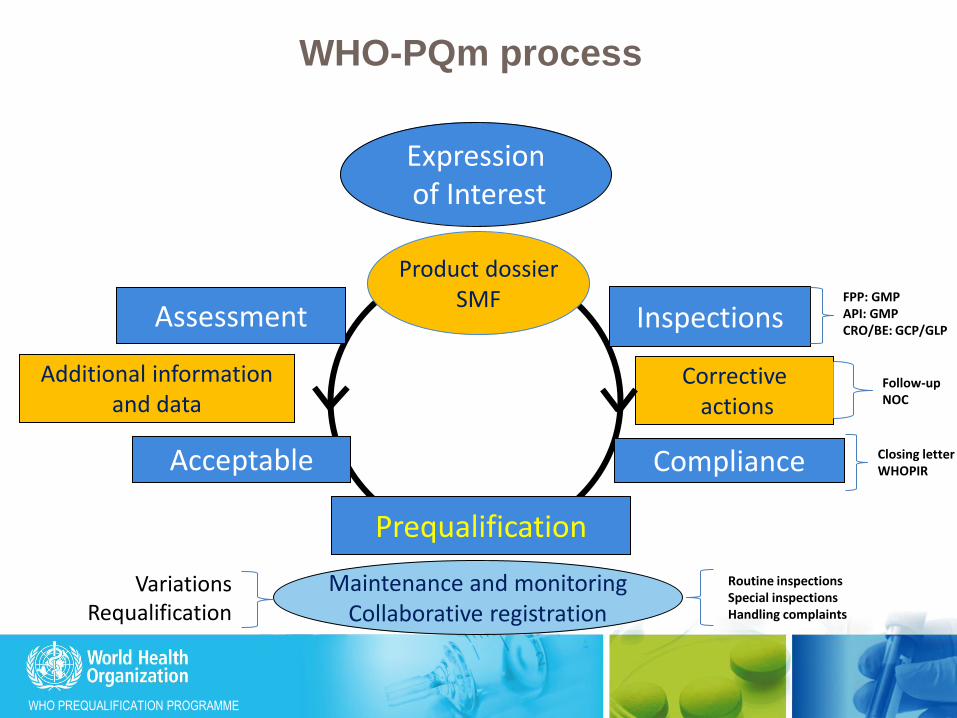
WHO-PQm process
Expression of Interest
Acceptable
Additional information and data
Corrective actions
Compliance
Assessment Inspections
Prequalification
Maintenance and monitoring Collaborative registration
Product dossier SMF FPP: GMP
API: GMP CRO/BE: GCP/GLP
Closing letter WHOPIR
Routine inspections Special inspections Handling complaints
Follow-up NOC
Variations Requalification

WHO PREQUALIFICATION PROGRAMME
WHO-PQT-Rx: Inspection Timelines
• First inspection: 6 months from dossier acceptance for assessment or from site confirming it is ready for inspection.
• Notification: 1 – 2 months before inspection.
• Onsite days: 3 – 5 days based on scope and complexity.
• Report: 30 days from last date of inspection.
• CAPAs: 30 days from receipt of report (max 2 rounds, comprehensive, soft and not hard copies)
• Closing of inspection: 6 months from inspection.
• Follow-up inspection: 6 months from inspection
• Routine inspection: – Due date 1 – 3 years from the previous inspection (risk based) – Actual ± 3 months from due date.

WHO PREQUALIFICATION TEAM
17
Inspections – Team and scope
• Team: qualified and experienced inspectors
• WHO representative (qualified inspector)
• Inspector from well-established inspectorate (Pharmaceutical
Inspection Cooperation Scheme countries – PIC/S)
• National inspector/s invited to be part and observe the inspection
• Observer from recipient/developing countries (nominated by
NMRA of the country)
• Scope
• Compliance with guidelines: GMP for API and FPP sites, GCP
for CROs, GLP for FPP/API factory QCL, CRO-BAL, NQCL,
IQCL
• Data integrity verification – data manipulation, falsification,
(validation, stability, clinical, bioanalytical)
2. Prequalification process
WHO PREQUALIFICATION PROGRAMME
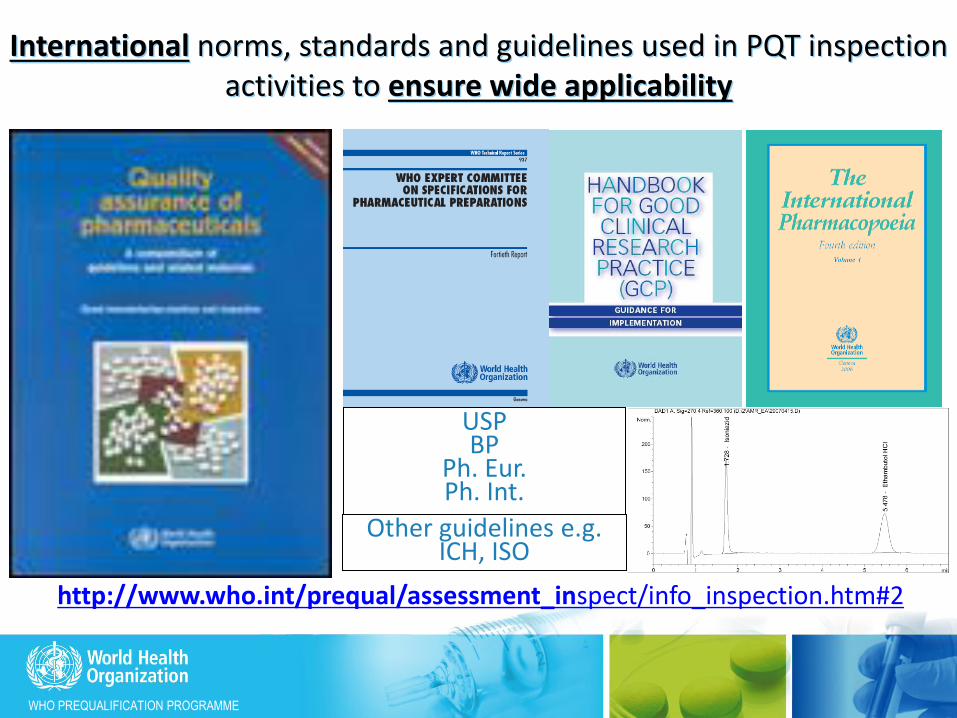
USP BP
Ph. Eur. Ph. Int.
International norms, standards and guidelines used in PQT inspection activities to ensure wide applicability
Other guidelines e.g. ICH, ISO
http://www.who.int/prequal/assessment_inspect/info_inspection.htm#2
WHO PREQUALIFICATION PROGRAMME
Prequalification Programme: Use of Inspection
reports from other NMRAs
Inspectorates whose reports are recognized:
√ PICS member inspectorates
√ EU (EDQM + EMA)
√ USFDA – now also member of PICS
What GMP evidence to submit:
– SMF – Up-to-date
– Inspection report - conducted NMT 2 years
• + CAPAs to deficiencies + final conclusion
– Product Quality Review – not more than 1 year old
Review of the report:
scope covered the specific FPP or API
Is comprehensive and supports the final outcome.
PQP reserves the right to inspect the FPP/API manufacturer – as long as product is active in WHO-PQP.
on-going GMP compliance will be confirmed by WHO

WHO PREQUALIFICATION PROGRAMME
Risk-based approach in:
definition and classification of deficiencies
• Deficiencies are descriptions of non-compliance with GMP requirements.
• A distinction is made between deficiencies as a result of: - – a defective system or,
– failure to comply with the system.
• Deficiencies may be classified as: – Critical Observation – potential risk harm to the user
– Major Observation – major deviation from GMP/GCP
– Minor or Other Observation – minor deviation from GMP

WHO PREQUALIFICATION PROGRAMME
21 Risk-based approach in:
Conclusion following an inspection
• When there are "other" observations only: – considered to be operating at an acceptable level of compliance with
WHO GMP.
– The manufacturer is expected to provide CAPAs.
– CAPAs are evaluation and followed up during the next routine inspection.
• When the are "other" and a few "major" observations: – compliance with WHO GMP is made after the CAPAs have been
assessed.
– CAPAs for majors to include documented evidence of completion.
– CAPAs paper evaluated ± an on-site follow up inspection.
• When there are "critical" or several "major" observations:
– considered to be operating at an unacceptable level of compliance with WHO GMP guidelines.
– Another inspection will be required

WHO PREQUALIFICATION TEAM
Outline of the presentation – PQ and its contribution to MDGs, SDG and 13th GPW – Organisation structure & procedures of PQT – Transparency: Website and guidance documents Key numbers, product pipeline
– Updates on: New SRA definition New funding model and KPIs New PQT IT solution Collaborative registration procedure and harmonization
activities – WHO-PQT: Looking to the future – Take home messages

WHO PREQUALIFICATION PROGRAMME
• Website: https://extranet.who.int/prequal/
• Email: [email protected]
| WHO Prequalification of Medicines 23 Further information

WHO PREQUALIFICATION TEAM
24

WHO PREQUALIFICATION TEAM
25
Through the prequalification process, WHO has made available
numerous quality-assured products to WHO Member State markets
At the close of August 2018, PQT’s list of prequalified products included:
Key numbers
Medicines
412 FPPs 129 APIs
44 QCLs
Diagnostics
81 IVDs 2 MCDs
Vaccines
148 Vx 400 ImDs
Vector control
71

WHO PREQUALIFICATION TEAM
1. Oral hormonal contraceptives #FPPs PQ’d #FPPs under assessment
Ethinylestradiol + desogestrel, tablet 30 micrograms +150 micrograms
4 2
Ethinylestradiol + levonorgestrel, tablet 30 micrograms + 150 micrograms
8 2
Levonorgestrel, tablet 30 micrograms 2 -
Levonorgestrel, tablet 750 micrograms (pack of two) 3 1
Levonorgestrel, tablet 1.5 mg (pack of one) 3 2
Norethisterone, tablet 350 micrograms 2 -
Norgestrel, tablet 75 micrograms - -
Lynestrenol, tablet 500mcg 1 -
https://extranet.who.int/prequal/key-resources/documents/summary-fpps-and-apis-invited-prequalification

WHO PREQUALIFICATION TEAM
http://www.who.int/diagnostics_laboratory/pq_status/en/
WHO PREQUALIFICATION TEAM
Expert Review Panel (ERP)
• ERP established in April 2009 by GF and WHO.
• Objective: To review the potential risk/benefit for FPPs not yet WHO-prequalified or SRA-authorized, for the purpose of providing information to aid procurement decisions
• ERP risk categories developed by WHO/RHT.
• ERP is coordinated by the WHO/RHT as a service to interested procurers
• ERP reviews are done by experienced regulatory professionals
• Procurer responsible for all communications with manufacturers and procurement decision.
WHO PREQUALIFICATION TEAM
29
WHO prequalification serves as a guarantee of good quality for
health products, is a reference in terms of internal technical
expertise and has the power to convene external expertise
Benefits for stakeholders
Access to quality-assured products, adapted to their specific needs
Accurate prevention, diagnosis, and treatment
Patients
List of prequalified products
Increased availability of quality-assured products
Monitoring quality of prequalified products
Healthy market: diversity and affordability of products
Donors, procurers and UN agencies
Reduced burden for regulatory approval
Increased regulatory capacity & harmonization of regulatory practices in WHO MS
Implementation of specifically developed and road-tested international guidelines
Access to quality-assured products
WHO Member States & NRAs

WHO PREQUALIFICATION TEAM
30
WHO prequalification serves as a guarantee of good quality for
health products, is a reference in terms of internal technical
expertise and has the power to convene external expertise
Benefits for stakeholders
Access to donor-sponsored tenders
Faster regulatory approval
Timely assessment of variations and changes
International quality-assured product status (improved image)
Recognition of GMP status, beyond prequalified products
Increased capacity in quality management systems
Target Product Profiles
Harmonization of regulatory practices within WHO Member States
Reduced operating and manufacturing costs
Manufacturers
International recognition of prequalified QCLs
Technical assistance and scientific advice
QC labs

WHO PREQUALIFICATION TEAM
Outline of the presentation – PQ and its contribution to MDGs, SDG and 13th GPW – Organisation structure & procedures of PQT – Transparency: Website and guidance documents Key numbers, product pipeline
– Updates on: New SRA definition New funding model and KPIs New PQT IT solution Collaborative registration procedure and harmonization
activities – WHO-PQT: Looking to the future – Take home messages
WHO PREQUALIFICATION TEAM
New SRA definition
Recommendations from the 52nd ECSPP
• That the term “stringent regulatory authority (SRA)” be replaced by
“WHO-Listed Authority”.
• That those NRAs currently identified as “SRAs” in accordance with the
current interim definition be regarded as WHO-Listed Authorities.
• That the designation of additional NRAs as WHO-Listed Authorities
should be based on an assessment against the Global Benchmarking
Tool (GBT), as well as successful completion of an agreed and
transparent confidence-building process.
• That a procedure for listing be developed accordingly through the usual
public consultation process.”
-Draft WHO Global Benchmarking Tool (GBT) version VI was published
comments in January 2018 to end of February. The comments are currently
under consideration

WHO PREQUALIFICATION TEAM
New Funding Structure for PQ • Objectives:
– ensure the financial sustainability of WHO’s PQ
– to make PQ better equipped to address current global quality challenges,
– to lay the ground for strengthening and expanding services provided, and
– to improve financial predictability and transparency
• Fees structure:
– Designed to ensure equity among manufacturers
– modelled on the practice of NRAs around the world,
• Fees principles and structure:
– product nature: active pharmaceutical ingredient (API) or finished pharmaceutical product (FPP);
– type of assessment: full or abridged assessment of new application, or assessment of major variation;
– an annual maintenance fee tailored to whether the initial assessment was full or abridged.
Diagnostics Model went live on 1 August 2018
New application
full assessment
New application
abridged assessment
Annual fee Change
assessment fee
5,000 + 12,000 8,000 4,000 3,000

WHO PREQUALIFICATION TEAM

WHO PREQUALIFICATION TEAM
PQT – revised fee model - When are fees payable?
• Screening, application/evaluation fee, inspection fee:
– Payment should be made within 15 days of receipt of the invoice from WHO
– Application/evaluation (including variation) fee for medicines invoiced after the application has been successfully screened and accepted for assessment
– Screening, application and inspection fees for vaccines are invoiced before start of activity
• The annual fee:
– for medicines and APIs is fixed, whereas for vaccines the annual levy is linked to sales from PQ’d vaccines (PQ enabled sales).
– The annual fee is invoiced by the 1 October each year for all products that have been present on the list of prequalified APIs, FPPs or vaccines for 12 months or greater as of the 1 September of that year. Payment of the annual fee should be made before 30 November of the calendar year in which the invoice was issued.

WHO PREQUALIFICATION TEAM
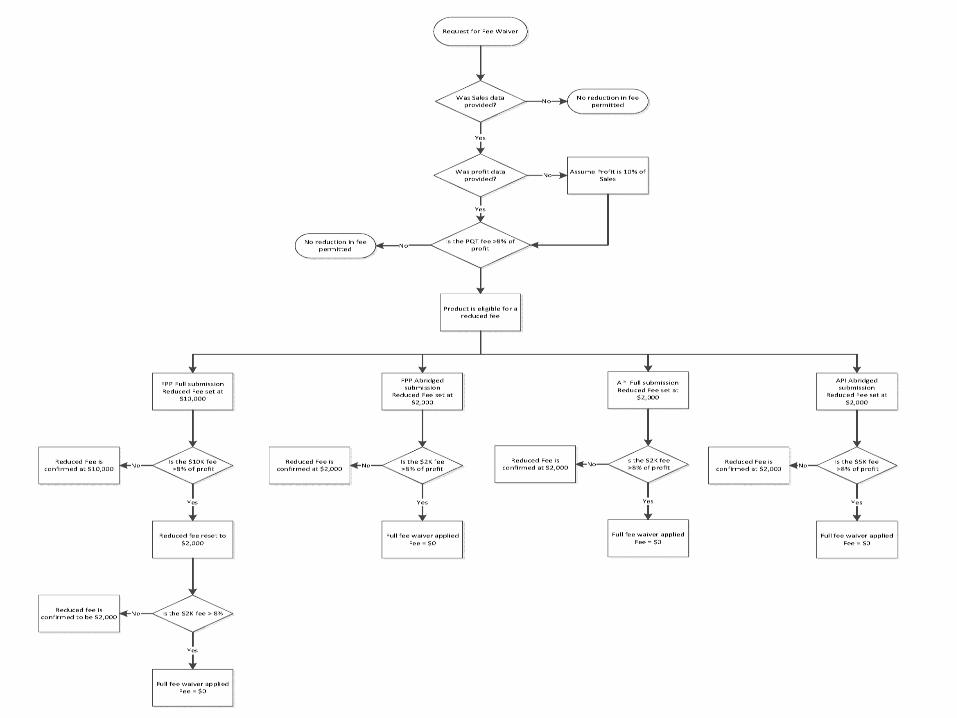
• Certain products with low commercial value will be eligible for reduced fees or a waiver of the fees*.
– This is to ensure that fees to do not become an impediment
to access.
– Equally, waiver should not compromise the objectives of
equity (based on actual sales and profits) and contribution
to the financial sustainability of related PQ activities.
• A reduced annual fee or waiver of the annual fee will be
granted following an application.
*https://extranet.who.int/prequal/sites/default/files/documents/PQ_Fees_Annex_092017.pdf
Principles for reduced and waivers of annual fees for
medicines manufacturers

WHO PREQUALIFICATION TEAM
1. A reduced annual fee or waiver of the annual
fee will be granted following an application.
2. This information will be reviewed to inform the decision on the reduction/waiver request, putting into consideration:
• supply security (need plus availability of alternative sources)
plus
• equity and fairness to all players – based on actual sales and profit.
37
Criteria for granting reduced fees and waivers
WHO PREQUALIFICATION TEAM
WHO PREQUALIFICATION TEAM
New PQ funding model: Updates
• There has been good response to the new
funding model and fee structure
• There is no apparent impact on the number of
applications received.
• There were some products withdrawn but these
were mainly related to changes in the treatment
guideline and EOI and hence reduced demand.
• Reduction or waiver of annual fees have been
granted where this was deemed justified.

WHO PREQUALIFICATION TEAM
40
2014 2015 2016 2017
FPP Received* 66 56 65 52
FPP accepted for assessment 65 49 63 50
APIs Received* 23 26 24 22
APIs accepted for assessment 23 24 23 22
0
10
20
30
40
50
60
70
No
of
app
licat
ion
s
Trends in application submitted to PQ

WHO PREQUALIFICATION TEAM
Reasons for introducing new performance metrics
Increased transparency for manufacturers and other
stakeholders following the introduction of the new fee model
Advantages of those new performance indicators
Following up the progress of applications throughout the PQ
pipeline (as opposed to only measuring timeline at the end of the
PQ assessment)
Monitoring performance of the different components of the PQ
assessment
Measuring performance of processes controlled by WHO PQ
(limited external influence on performance)
- Reasons & Advantages -
41
* https://extranet.who.int/prequal/content/key-performance-indicators-who-prequalification
Key performance Indicators (KPIs)*

WHO PREQUALIFICATION TEAM
Key performance Indicators (KPIs)
42
Time to prequalification (from acceptance for assessment to prequalification) for applications accepted after 1 January 2015, 2016 for APIs
100 Number of products PQed - -
110 Median WHO PQ time - N/A
111 Median manufacturer PQ time - N/A
112 Median total PQ time - N/A
KPI 1% of products prequalified at or below target WHO
PQ time
70%
(30% for
APIs)
Full assessment:
270 calendar days, 350 calendar days for IVDs PQed
without the alternative laboratory mechanism
Abridged assessment:
100 calendar days, 180 calendar days for IVDs PQed
without the alternative laboratory mechanism
Annual PQ cohort (products prequalified in a calendar year)
Time to ‘screening first action’
200 Number of PQ applications submitted - -
210 Number of ‘screening first actions’ - -
KPI 2% of 'screening first actions' taken at or below
target time80% 30 calendar days
Submission cohort (PQ applications submitted for PQ assessment in a calendar year)

WHO PREQUALIFICATION TEAM
Key performance Indicators (KPIs)
43
Time to 'first action’
300 Number of PQ applications accepted - -
310 Number of ‘dossier first actions’ - -
KPI 3.1% of ‘dossier first actions’ taken at or below target
time80%
90 calendar days, 120 calendar days for FPPs & APIs
(due to fixed assessment sessions)
320 Number of ‘inspection first actions’ - -
KPI 3.2% of ‘inspection first actions’ taken at or below
target time80% 210 calendar days
330 Number of 'laboratory first actions’ - -
KPI 3.3% of 'laboratory first actions’ taken at or below
target time80% 180 calendar days
Assessment cohort (PQ applications accepted for PQ assessment in a calendar year)
Time to ‘post-PQ change first action’
400 Number of post-PQ change applications assessed - -
410 Number of ‘post-PQ change first actions’ - -
KPI 4% of 'post-PQ change first actions' taken at or
below target time80%
APIMF|major (minor) amendment: 90 (60) calendar days
APIMF|immediate notification: 45 calendar days
FPP|major (minor) variation: 90 (60) calendar days
FPP|immediate notification: 45 calendar days
IVD|reportable change: 90 calendar days
Vx|major variation, type A: 90 calendar days
Change cohort (post-PQ change applications accepted for change assessment in a calendar year)

WHO PREQUALIFICATION TEAM
Time to prequalification of medicines (FPPs, median,
full assessment) 2010-2017
0
100
200
300
400
500
600
700
800
900
1000
2010 2011 2012 2013 2014 2015 2016 2017
WHO time Company time Total time to PQ
270 days

WHO PREQUALIFICATION TEAM
285
147
203
131 122
162
238
194
544
289
488
246
307
263
467
276
0
100
200
300
400
500
2010 2011 2012 2013 2014 2015 2016 2017
DA
YS
YEARS
Time to Vaccines Prequalification
WHO average time Total time to PQ
270 days

WHO PREQUALIFICATION TEAM
PQ measures to reduce manufacturer time, and total
time to prequalification - PQ provides advice at any stage before, or after submission (F2F-meetings,
TC, e-mails, specific pre-submission meetings) – PQ is accessible.
- Pre-submission meetings now mandatory for all new applicants
- Strict response timelines for manufacturers introduced – 30, 60 or 90 days
depending on the deficiencies
- Common Deficiencies in FPP Dossiers – additional guidance to manufacturers
- Feb 2018
- 1st PQ Quality workshop for manufacturers held in July 2018
- PQ develops product-specific guidance, on an ongoing basis, e.g. BE study
design, Q&As (ZnSO4, MgSO4, RH products, HVAC, TSS, TGS, etc.).
- PQ reviews final draft BE study protocols, before study start.
- PQ does an in-depth screening of dossiers, to ensure that dossiers are
complete before start of full assessment. This feedback is provided to the
applicant. The screening checklist is on the PQ website.
- Model dossier in CTD format to guide applicants (2016) and for IVDs
- Alternative lab performance evaluation
- Expansion of the expert pool – annual clearance

WHO PREQUALIFICATION TEAM
• Fast track to prequalification = Good quality dossier
at submission + prompt, complete, good-quality
responses to PQ’s questions, throughout the
process.

WHO PREQUALIFICATION TEAM
Universally accepted comparator:
enables one BE study to be conducted for use across countries
enables such generic products to be interchangeable.
Lists for comparator products for each treatment area
available on PQTm website which is updated regularly https://extranet.who.int/prequal/key-resources/documents/application-reference-scaled-criteria-auc-bioequivalence-studies-conducted
Not all products listed in PQ Expressions of Interest
(EOIs) will have comparators indicated on these lists
For example, some dispersible products do not have
comparable references so conventional product may have
to be used as comparator
If a comparator is not listed, consult PQTm
Comparator products

WHO PREQUALIFICATION TEAM
A regulatory authority that is
a member of ICH prior to 23 October 2015, namely: the US
Food and Drug Administration, the European Commission
and the Ministry of Health, Labour and Welfare of Japan also
represented by the Pharmaceuticals and Medical Devices
Agency; or
an ICH observer prior to 23 October 2015, namely: the
European Free Trade Association, as represented by
Swissmedic and Health Canada; or
a regulatory authority associated with an ICH member
through a legally-binding, mutual recognition agreement prior
to 23 October 2015, namely: Australia, Iceland, Liechtenstein
and Norway.
Comparator products:
Where can they be purchased?

WHO PREQUALIFICATION TEAM
Biowaivers In vitro approaches for demonstrating safety and
efficacy of products in lieu of conducting in vivo bioequivalence studies
Biopharmaceutics Classification System (BCS) –
based biowaivers Suitable for products containing eligible APIs Abbreviated submission if API is on the eligibility list
Additional strengths biowaivers Suitable for additional strengths in a product line when
one of the strengths has shown in vivo bioequivalence
to the comparator

WHO PREQUALIFICATION TEAM
BCS-based Biowaivers
eligible APIs
Medicines for HIV/AIDS and
related diseases Abacavir sulfate (Class III)
Emtricitabine (Class I)
Fluconazole Polymorphs II & III (Class I)
Lamivudine (Class III)
Stavudine (Class I)
Zidovudine (Class I)
Neglected Tropical Disease
medicines
Diethylcarbamazine (Class III)*
Anti-tuberculosis medicines Ethambutol (Class III)
Isoniazid (Class III)
Levofloxacin (Class I)
Linezolid (Class I)
Moxifloxacin HCl (Class I)
Ofloxacin (Class I)
Pyrazinamide (Class III)

WHO PREQUALIFICATION TEAM
BCS-based Biowaivers Do not use classifications provided in 2006 WHO
TRS 937, Annex 8 ECSPP overseeing the development of a new
biowaiver classification list Living document
Information on equilibrium solubility experiments Appendix 2 of WHO TRS 1003, Annex 6 (2017)
Document with more technical detail under
development by ECSPP

WHO PREQUALIFICATION TEAM 53

WHO PREQUALIFICATION TEAM 54
WHO PREQUALIFICATION TEAM 55

WHO PREQUALIFICATION TEAM
PQ of Vector Control Products: Progress
56
PQT-VC Prequalification
Established Single Point of Entry to WHO Data requirements determined and under review 125+ manufacturers meetings Operations manual developed 89 product applications for conversion received in PQ 71 products prequalified 7 new products applications under review 1 active ingredient under re-evaluation Website developed and information posted, e.g.: guidance, process, meetings Communication strategy under development, including Website re-design
PQT-VC Stakeholders Meeting with procurement
agencies Manufacturers meetings Conferences and WHO
organised meetings
PQT-VC Assessors Group SOPs for evaluation process,
documentation development and decision making
2nd Assessors Group meeting held in Arusha, Tanzania
3rd Assessors meeting planned for 26-30 November
WHO PREQUALIFICATION TEAM
• New PQT IT solution for all PQT streams is under
development
• Medicines platform will be launched Q1/Q2 2019
• Applicants will upload all their submissions to the IT
platform
• Applicants will need to create accounts to be verified
before submission
• Communication will be done using system communicator.
• System will allow applicant to monitor progress of their
applications.
• eCTD software under investigation
57
New IT platform

WHO PREQUALIFICATION TEAM
Regional harmonization initiatives
ASEAN SIAHR Project
PANDRH African Vaccine Regulators Forum (AVAREF)
African Medicines Regulatory Harmonization Project (AMRH)

WHO PREQUALIFICATION TEAM
59
The collaborative procedure enables NRAs to accelerate the
registration of prequalified products so that they can enter local
markets more quickly
Collaborative procedure
Procedure in
development
Ongoing discussions
with NRAs
Diagnostics
WHO PQ shares the reports that served as the basis for the prequalification
decision, so that NRAs do not conduct assessment and inspections
National registration based on PQT evaluation
Started in 2012
As of February 2018:
31 countries
participating
299 registrations in
more than 20
countries for over73
different products
Medicines
Procedure published
in 2007, harmonized
for medicines and
vaccines as of 2014
In 2015:
Adopted by expert
committee (ECBS)
Vaccines
Pri
ncip
les

WHO PREQUALIFICATION TEAM
Participating NMRAs
1. Armenia 2. Botswana 3. Burkina Faso 4. Burundi 5. Cameroon 6. *Caribbean Community (CARICOM) 7. Cameroon 8. Cote d'Ivoire 9. Dem. Rep. Congo 10. Eritrea 11. Ethiopia 12. Georgia 13. Ghana 14. Kenya 15. Kyrgyzstan 16. Lao PDR * CARICOM Member States: Antigua and Barbuda, Bahamas, Belize, Dominica, Grenada, Haiti, Jamaica, Montserrat, Saint Lucia, St. Kitts and Nevis, St Vincent and the Grenadines, Suriname and Trinidad and Tobago Associate Member States: Anguilla, Bermuda, British Virgin Islands, Cayman Islands and Turks and Caicos Islands
17. Madagascar 18. Malawi 19. Mali 20. Mozambique 21. Namibia 22. Nigeria 23. Pakistan 24. Philippines 25. Senegal 26. Sierra Leone 27. South Africa 28. Sri Lanka 29. Tanzania 30. Thailand 31. Uganda 32. Ukraine 33. Zambia 34. Zanzibar 35. Zimbabwe
As at 16 May 2018

WHO PREQUALIFICATION TEAM
• Voluntary
• Product and registration dossier
in countries are 'the same' as
prequalified by WHO.
• Shared confidential information
to support NRA decision making
in exchange for accelerated
registration process
• 'Harmonized product status' is
monitored and maintained
KEY Principles of WHO PQ Collaborative Registration Procedure

WHO PREQUALIFICATION PROGRAMME 62
Manufacturer informs PQP about national submission
and
gives consent with information sharing
Participating NMRA confirms its interest to
participate in procedure for specific product
PQP shares with participating NMRA
outcomes of assessment and inspections
Participating NMRA reviews WHO PQP outcomes,
decides within 90 days decides upon the national
registration and informs PQP about its decision
Steps of the procedure: registration
PQ product is submitted for national registration
to NMRA participating in the procedure
NMRA is informed about the interest to follow PQP

WHO PREQUALIFICATION TEAM
WHO PQ CRP: Documents shared
Assessment reports (All reports generated through the review process)
Inspections reports (API, FPP and CROs)
WHO Quality Information Summary (QIS)
NB: This information is useful for NRA for marketing authorisations

WHO PREQUALIFICATION TEAM 64
What has been achieved through CRP: as of February 2018
299 registrations
Median = 85 days
35 plus countries
manufacturer
WHO
NRA
Before CRP – 2 months to 10 years
Days
Target

WHO PREQUALIFICATION TEAM
Outline of the presentation – PQ and its contribution to MDGs, SDG and 13th GPW – Organisation structure & procedures of PQT – Transparency: Website and guidance documents Key numbers, product pipeline
– Updates on: New SRA definition New funding model and KPIs New PQT IT solution Collaborative registration procedure and harmonization
activities – WHO-PQT: Looking to the future – Take home messages

WHO PREQUALIFICATION TEAM
WHO-PQT: Looking to the future
– Continue the assessment of current scope of products by PQT at HQ – Rx,
VCP, Vx and Dx.
– Complete the transition from WHOPES to PQ-VCP and streamline
procedures
– Gradually expand scope of PQ to cover products, e.g. on the EML through: • setting up criteria for prioritisation and gradual scope expansion
• NCDs: BTP/SBP pilot launched, under discussion (Diabetes/Insulin, Hypertension, other cancer medical products)
• IVDs for Cholera, TB, NCDs, NTDs/Dengue, measles, Rubella, etc. Consultation scheduled for Q42018
– Gradually expand the mechanisms for PQ through:
• Expanding the abridged assessment of products approved by WHO Listed
Authorities as defined from time to time. • Reliance on regional-network-joint-assessments that have been quality assured by PQ with cooperation from RSS -
medicines.
– Strengthen mechanisms to evaluate new products developed with special focus on LMICs and emergencies – including cooperation with EU Art58, Swiss medic MAPGHP.
– Expand risk based approaches like ERP, ERPD, EUAL and other mechanisms for Snake anti-venoms, Rabies vaccine, RSV, DAT, other products on the EML.

WHO PREQUALIFICATION PROGRAMME
To summarise, WHO Prequalification:
• Current scope: IVDs, MCDs, FPPs, APIs, QCLs, vaccines, immunization devices, VCPs and VCIs
• Contributes to achieving SDGs and UHC
facilitates access to quality assured priority health products
• Role recognized by WHO 13th General Programme of Work (2019 – 2013):
The Organization will continue to support the availability of quality-assured generic products for procurement by global agencies and countries through the WHO prequalification programme, which will evolve to meet the changing health needs of countries.
• Already designed to fit in the WHO 13th GPW strategic shifts:
Step up global leadership - recognized as a stamp of quality
Drive impact in every country and placing countries at the centre:
Doing it with NMRAs – best impact on capacity building and promoting convergence
Programmatic suitability of vaccines
Focus on IVDs - POC, EID and RDTs - for use in resource limited settings

WHO PREQUALIFICATION TEAM
Take home messages
PQ responded to needs of members states and contributed to
objectives and targets of MDGs and SDGs
The WHO 13th GPW (2019 – 2013) recognises continued
need for PQ which will evolve
PQ has been recognized as a stamp of quality and a point of
reference for QA for UN, International, regional and national
procurement
PQ has been instrumental in building national capacity for the
manufacture, regulation and monitoring of medicines –
promoting harmonization and convergence
PQ has put in place measures to improve sustainability and
transparency
PQ is evolving and adapting to the needs of the time and
future
WHO PREQUALIFICATION TEAM
Contacts 69
Diagnostics
Irena Prat
Medicines
Matthias Stahl
Vaccines
Carmen
Rodriguez Hernandez
Inspections
Johanna Gouws
Technical assistance &
laboratories
Rutendo Kuwana
Prequalification team
Deus Mubangizi
PQT Coordinator
Vector control
Marion Law