who europe initiative on the health of children and young people with intellectual disabilities and...
TRANSCRIPT

WHO Europe Initiative on theWHO Europe Initiative on theHealth of Children and Young People Health of Children and Young People
with Intellectual Disabilities with Intellectual Disabilities and their Familiesand their Families
Dr Roger BanksConsultant in the Psychiatry of Learning Disability
Betsi Cadwaladr University Health Board
Wales UK
Mental Health Programme
• Declaration• Action plan
evidence based interventions.
• Background Paperkey issues / challenges
• Expert Papersresource bank for developing national action plans. Evidence, recommendations and resources for each priority
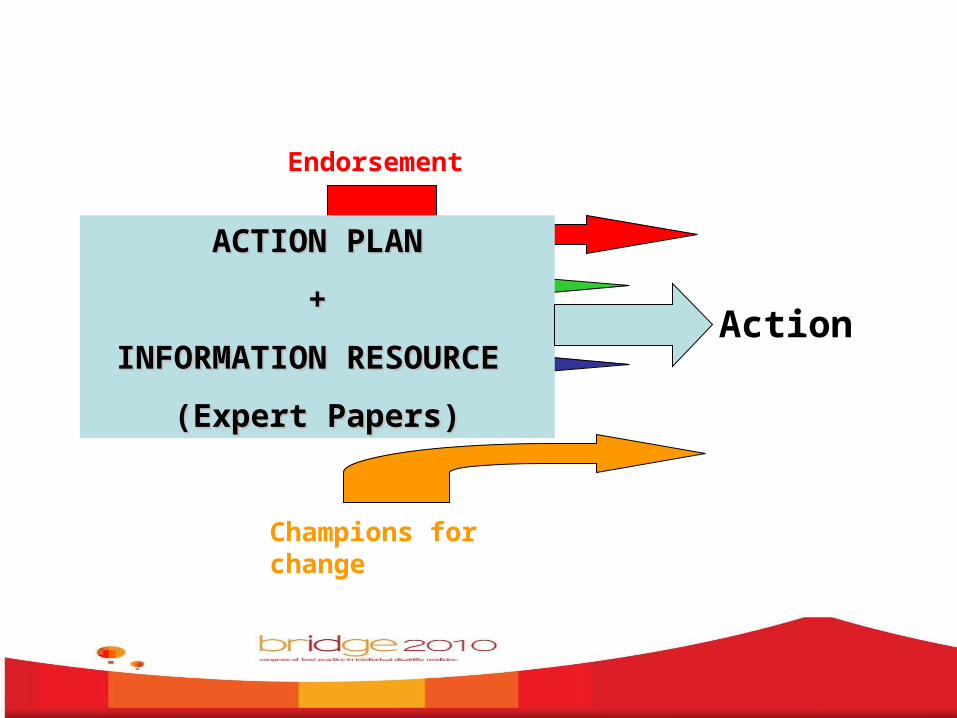
Declarationto ActionFrom
Endorsement
Dissemination
Levers
Champions for change
ACTION PLANACTION PLAN
++
INFORMATION RESOURCE INFORMATION RESOURCE
(Expert Papers)(Expert Papers)

10 PRIORITIES
1: Protect children and young people with intellectual disabilities from harm and abuse.
• All children and young people with intellectual disabilities, wherever they live, must be guaranteed lives free from bullying, harm or abuse and should not live in fear or neglect.
2: Enable children and young people to grow up in a family environment.
• Promoting secure attachments and improving family functioning limits the impact of intellectual disability. Ongoing support to families is essential.

3: Transfer care from institutions to the community
• Residential institutions that have a negative impact on the health and development of children and young people should be replaced by high quality community support. New admissions to such institutions should be stopped through the development of community services.

4: Identify the needs of each child and young person.
• Early identification and early intervention improve long-term outcomes. Children and young people require repeated assessment of their needs and planned support to make seamless transitions at each life stage.

5: Ensure that good quality mental and physical health care is coordinated and sustained.
• Children and young people with intellectual disabilities need the same access to health care as other children but may also need access to specialist treatment and care.

6: Safeguard the health and well-being of family carers.
• In order for a child with intellectual disabilities to grow up and develop within a family, the health and well-being of the family as a whole should be supported. Enabling families to care for their child from the time of identification of intellectual disability through to adulthood can prevent harmful family strain or rejection of the disabled child.

7: Empower children and young people with intellectual disabilities to contribute to decision-making about their lives.
• Children and young people with intellectual disabilities can and will make their needs and wishes known and contribute to their community, given appropriate support and a receptive environment. Family members and advocates also need encouragement and support to make themselves heard.

8: Build workforce capacity and commitment.
• The well-being of children and young people with intellectual disabilities is strongly reliant on the knowledge, skills, attitudes and commitment of staff in all settings and sectors.

9: Collect essential information about needs and services and assure service quality.
• Quality standards and adequate information systems are needed to monitor quality of care, with transparent responsibilities for all stakeholders.

10: Invest to provide equal opportunities and achieve the best outcomes.
• Ensure fair and, if necessary, preferential spending on services from which intellectually disabled children and young people and their families benefit.

ACTIONS & EXPERT PAPERS

1: Protect children and young people with intellectual disabilities from harm and abuse
• Children need safe and stable environments in which they can grow, develop, play and learn. Children with intellectual disabilities are disproportionately at risk of neglect and abuse. They face additional risks, and require additional protection, in times of social or economic instability and conflict.
• All children and young people with intellectual disabilities, wherever they live, must be guaranteed lives free from harm or abuse and should not live in fear or neglect as a consequence of discrimination, poverty, or a failure of the responsible agencies to provide appropriate protection and support.

Background evidence:
• Socio-economic adversity– Long term effects on physical and mental
health
• Environmental toxicity– Poverty, violence, family disruption, despair,
alienation
• Resilience– How to develop

Background evidence:
risk of abuse:– Physical, emotional and sexual
• More likely to be care for away from home• ‘Institutional care’ associated with:
– Vulnerability to abuse– Poor diet / feeding– Poor and inadequate personal care / toileting– Lack of stimulation, attention, emotional support– Aversive, punitive interventions to control behaviour

Background evidence: vulnerability factors
• Lack of awareness of vulnerability• Lack of awareness of signs and
symptoms of abuse• Denial and under-reporting• General devaluing of disability and
disempowerment• Stigma and exclusion leading to less
participation in society and less access to preventive or protective services

Background evidence: vulnerability factors
• Lack of choice and control
• Poor or absent support for children and their families in the community
• Lack of effective child protection systems
• Poor systems for assessment of children’s development leading to a failure to recognise indicators of neglect and abuse
• Diagnostic overshadowing

Background evidence: contributory characteristics of child
• Chronic behaviour / mental health problems
• Sensory impairments (visual / hearing impairment)
• Need for intimate personal care
• Physical disability
• Medical problems

Background evidence: contributory characteristics of child
• Communication difficulties
• Lack of knowledge of relationships and sexuality
• Previous history of abuse
• Lack of peer support or presence of another person to confide in
• Dependency on others, over compliance and fear of “speaking out”

Recommended actions:Nationally• Establishing a priority
• Determining the size and scope of the issue
• Creating a plan of action and implementation
• Establishing systems for evaluation of processes and outcomes
Recommended actions:
• Safeguarding
• Investigation
• Therapeutic
• Policy

Recommended actions:Safeguarding• Education
• Listening and empowering
• Selection, training and supervision of staff
• Greater integration in communities
• Involving communities in the opening up and decommissioning of institutions

Recommended actions:Investigation• Research, develop & implement measures of health,
wellbeing and social conditions for children & their families outcomes of interventions in social protection, poverty reduction, child protection and fostering of resilience can be effectively evaluated.
• Enable access and adaptation of existing child protection systems
• Audit professional practice in health and social care should be regularly audited against standards of safety and quality of assessment, record keeping, inter-professional and inter-agency communication.
• Develop clear reporting and investigation protocols

Recommended actions:Therapeutic• Develop therapeutic skills of workforce
(health and social)• Education and awareness of professionals
about consequences of neglect / abuse / social deprivation
• Extension and adaptation of established routine therapeutic models and interventions for working with children and families

Recommended actions:Policy• Clear national child protection policies that guarantee
equality of opportunity and specific provision for children with intellectual disabilities
• Address vulnerability of children placed outside of family settings and in segregated, communal care + inter-agency working, information sharing and adherence to common care standards, inspection and monitoring frameworks
• Standards have to state the kind of practices that are unacceptable:– restrictive practices that limit the freedom of movement and
participation – staff competence and training– need for mandatory training in child protection
Recommended actions:Policy• More effective communication and collaboration
between social care, education and health agencies, and justice systems, in the identification of children at risk and of potential perpetrators of abuse
• National and local policy level:– anti-stigma programmes and activities– promote a more inclusive society– reduce negative stereotyping and low expectations

Examples of good practice
• ‘Keeping Children Safe – Toolkit’ for Child Protection. This was developed by a number of aid and development agencies based in UK and Switzerland, along with the NSPCC, which make up the Keeping Children Safe Coalition. It contains standards which should ensure that through awareness, good practice and robust systems and procedures, staff and other representatives are able to keep children safe from harm. Based on these standards, Save the Children Norway developed Codes of Conduct which are an obligatory part of the contracts with their partners implementing the projects in South East Europe supported by SCN.

Examples of good practice
• The Ministry of Social Policy of Serbia created and adopted in 2005 a “Special protocol on protecting children in social care institutions from abuse and neglect”; the majority of children in institutions in Serbia are children with disabilities. The staff of the institutions have been trained for the implementation of the protocol and as a result there appear to be more reported cases of abuse and neglect.

Examples of good practice
• McGrath and colleagues in the South of Ireland have developed a 10-week anti bullying intervention program drawing upon elements from established programs for the general population and adapted to meet the needs of adults with an intellectual disability18.

Examples of good practice
• The Books Beyond Words series (RCPsych, UK) provide a resource to support children and young people with intellectual disabilities who cannot read or who have difficulty reading. These books, in which people with intellectual disabilities are involved in the design and trialling, address the emotional aspects of difficult events and in particular cover issues of sexual abuse and its disclosure, being a victim of mugging and the use of counselling23,24.
So ………
How could you see yourself using, promoting, developing the action plan, expert papers ?