white paper the polst paradigm and form: facts and … · white paper the polst paradigm and form:...
TRANSCRIPT
White Paper
The POLST paradigm and form:Facts and analysis
CHRISTIAN BRUGGER, PH.D.1, LOUIS C. BRESCHI, M.D.2,EDITH MARY HART, R.S.M., D.O.3, MARK KUMMER, M.D.4,JOHN I. LANE, M.D.5, PETER T. MORROW, M.D.6, FRANKLIN L. SMITH, M.D.7,WILLIAM L. TOFFLER, M.D.8, MARISA BEFFEL, R.N., PH.D.9,JOHN F. BREHANY, PH.D., S.T.L.10, SARA BUSCHER, J.D.11 AND
RITA L. MARKER, J.D.12
1St. John Vianney Theological Seminary Denver, CO, USA2Franklin Square Medical Center, Baltimore, MD, USA3Sacred Heart Mercy Health Care Center, Jackson, MN, USA4Nemours Children’s Clinic and Florida State University School of Medicine,
Pensacola, FL, USA5Mayo Clinic, Rochester, MN, USA6St. Cloud Regional Medical Center, St. Cloud, FL, USA7Aurora Summit Hospital, Summit, WI, USA8Oregon Health & Science University, Portland, OR, USA9Brookfield, WI10Ethicist of the Catholic Medical Association, Bala Cynwyd, PA, USA11Appleton, WI12Patients Rights Council, Steubenville, OH, USA
This white paper, prepared by a working group of the Catholic Medical Association, provides a com-mentary on a new type of end-of-life document called a POLST form (Physician Orders for Life-Sustaining Treatment) as well as on its model (or “paradigm”) for implementation across the UnitedStates. After an introductory section reviewing the origin, goals, and standard defenses of the POLSTparadigm and form, the paper offers a critical analysis of POLST, including an analysis of the risksthat POLST poses to sound clinical and ethical decision-making. The paper ends with several rec-ommendations to help Catholic healthcare professionals and institutions better address the challenges ofend-of-life care with alternatives to POLST.
Keywords: POLST, End of life care, Living will, Advance directive, Advance decision-making,In-the-moment-of-need medical decision-making, Euthanasia, Catholic health care
The Linacre Quarterly 80 (2) 2013, 103–138
© Catholic Medical Association 2013 DOI 10.1179/0024363913Z.00000000027

INTRODUCTION
The Challenge of Ethical Decision-Making at the End of Life
An attitudinal shift has taken place in thepast half-century in the culture ofend-of-life (EOL) care. The ancient andineradicable fear of death has begun to liveuncomfortably along side a waxing fear ofliving too long, of being a burden to one’scaregivers and of languishing meaning-lessly in debility, dementia, or terminaldemise. Many factors account for thisshift, but three seem most significant.First, the development of medical technol-ogies and better health measures sinceWorld War II have meant that elderlypeople are living longer, which meansmore are living into a period of dementiafrequently spending their final years ininstitutions away from their families andloved ones. Second, the loss of Christianfaith has meant that people’s thoughts onsuffering, old age, and dying are decreas-ingly characterized by a sense of divinejudgment (i.e. of a hope for heaven anddesire to avoid hell), of the Christianmeaning of suffering, and of the intrinsicvalue of human life. Finally, the weaken-ing of our bonds of community has meantthat more elderly experience lonelinessand alienation when the measurableutility of their daily activities naturallydecreases. One prominent Americanbioethicist writes: “many of us now worrythat death will come too late—long afterlife has lost its usefulness and its savor,long after we have ceased to have a ‘life,’perhaps long after we are even ourselves”(Hardwig 2009, 38). Consequently, moreand more people are feeling an urgentneed to control the conditions surround-ing their own deaths in order to avoidwhat they believe may be “a death thatcomes too slowly and too late” (Hardwig2009, 38).
This attitudinal shift has foundexpression in our practices of EOL care,in particular, the widespread use of EOLdocuments (such as living wills) directingthe limitation of life-sustaining medicalprocedures. Although decisions limitingmedical interventions can be legitimateand have been defended under certain cir-cumstances in the Catholic tradition andin papal teaching since Pope Pius XII,1 adisturbing mentality is gaining prominencein US health care. It advances the ideathat disability and dysfunction can reducethe value of a person’s life; it increases invulnerable people a fear of living too long,of being a burden, and of dying—as itsmantra goes—“without dignity”; and itpromotes EOL documents as a meansprecisely for controlling the circumstancesand timing of death.
Intent of This White Paper
This white paper considers in detail onepotentially problematic response to thisattitudinal shift in the form of a new typeof EOL document known as PhysicianOrders for Life Sustaining Treatment(POLST)2 and an organized campaign toencourage its widespread use. We acknowl-edge that the POLST form was developedto deal with real challenges in communicat-ing and respecting patients’ decisionsregarding treatment at the end of life. Weare well aware of the problem of over-aggressive medical care being delivered topatients who did not want it and whoseconditions did not warrant it. Overtreat-ment at the EOL has resulted from at leastthree factors: (1) a medical culture charac-terized by paternalism that placed morevalue on the way physicians viewed deathand dying than patients; (2) fear and uncer-tainty among patients and family memberswhen dealing with their own or a lovedone’s demise; and (3) obstacles to learning,
104 The Linacre Quarterly 80 (2) 2013

documenting, and respecting patient wishesfor their EOL care.3 However, medicalpaternalism has been replaced by a cultureof autonomy that values patient wishes inmedical decision-making sometimes to afault. Fear and uncertainty at life’s endcannot so much be avoided as its effectson decision-making minimized. Overcom-ing the range of obstacles tocommunication and implementation ofpatient wishes has been a primary objectiveof those promoting the POLST form, andof many other people as well. Like advo-cates of POLST, we are committed toovercoming obstacles to the clear com-munication of the values and wishes ofpatients. As Catholic physicians andhealthcare professionals, we are also com-mitted to upholding the values of Catholichealth care, which include providingappropriate, ordinary treatments withoutdiscrimination and always providing themost basic forms of care that all patientsneed and deserve.In contrast to advocates of POLST,
however, we believe that the use ofPOLST forms will create unacceptablerisks from both the perspective of goodmedical decision-making and good ethicaldecision-making. Although we recognizethat POLST might offer some benefits tosome patients, the benefits will be grosslyoutweighed by the harms and abuses thatwill result from use of the POLST formand the campaign to promote it.We begin with a brief introduction to the
POLST paradigm and form, and reviewarguments which favor its widespread use.We then outline the challenges that webelieve POLST poses to good clinical careand ethical decision-making. We end withrecommendations regarding POLST andpropose some alternatives to the longstand-ing focus on advance decision-makingmodels, alternatives that we think are moreconsistent with good clinical practice andCatholic moral principles.
REVIEW OF THE POLST PARADIGM AND
FORM
Introduction to the POLST Paradigmand Form
Origin, Promotion and Spread4
The “POLST Paradigm Initiative” wascreated in 1991 by a task force of health-care professionals and ethicists from theCenter for Ethics in Health Care atOregon Health & Science University(OHSU)5 with the stated goal of facilitat-ing patients’ choices regarding end-of-lifecare, in general, and life-sustainingmedical treatments, in particular. The“paradigm” was designed around a processof EOL counseling that would culminatein the completion of a “POLST form.”Although the POLST form is examined
in more detail below, it is distinctive in that,after being signed by a clinician, the form isimmediately invested with the status of anactionable medical order, without regard topatient decisional capacity.In 1991, the OHSU task force devel-
oped the approach and form thateventually would come to be known asPOLST.6 A pilot instrument, called the“Medical Treatment Coversheet” (MTC),along with a process for implementationand evaluation, was created.7 For the firsttime, medical directives formerly dispersedover multiple forms were consolidatedonto a single document.8 In 1993, theMTC’s name was changed to “PhysicianOrders for Life-Sustaining Treatment(POLST)”9 and, in 1995, a POLST docu-ment was released for use in the state ofOregon. After that, the POLST paradigmand form began to spread across theUnited States. While a high degree ofunity prevailed, given the origin of thePOLST paradigm and materials atOHSU’s Center for Ethics in HealthCare,10 some states began to use otheracronyms, including: POST (“Physician
Brugger et al. – The POLST paradigm and form: Facts and analysis 105

Orders for Scope of Treatment”) in WestVirginia; MOLST (“Medical Orders forLife-Sustaining Treatment”) in Maryland;MOST (“Medical Orders for Scope ofTreatment”) in Colorado; and COLST(“Clinical Orders for Life-SustainingTreatment”) in Vermont.In 2004, OHSU’s Center for Ethics in
Health Care assembled a task force ofrepresentatives from participating states tofurther facilitate the spread of the POLSTparadigm nationally. The new NationalPOLST Paradigm Task Force (NPPTF)established standards by which individualstates could develop “endorsed” POLSTprograms (Sabatino and Karp 2011, 3).States or regions interested in seeking
endorsement from the NPPTF mustsubmit an application that demonstratesthat they meet the program requirements.The NPPTF supplies well-developedguidelines for implementing a statewide orregional POLST paradigm programincluding advice on assembling local taskforces,11 conducting pilot programs, iden-tifying a core group of “physicianchampions” who will take leadership inprogram implementation and education,12
addressing legal issues, training non-phys-icians to act as advance care planningfacilitators,13 disseminating the programelements throughout the region, dealingwith media, and conducting self-reviews.All endorsed programs must meet a set
of requirements that include thefollowing:14
(1) state or regional healthcare facilitiesand workers must recognize properlycompleted forms as current or (insome states, standing) medical orders;
(2) training programs for POLSTimplementation must be instituted;
(3) forms should be recommended forpersons who might die in the nextyear, who suffer from “chronic pro-gressive illness and/or frailty,” or who
are elderly “with strong, specificinformed preferences” about theirEOL options;
(4) the signatures of patients or their sur-rogates on POLST forms are“strongly” recommended, but oftennot required, as “evidence that patientsor their legal representatives agreewith the orders on the form”;15
(5) POLST forms should be the preferredadvance-planning document in diversehealth care settings (“e.g., emergencymedical services, long-term care, andhospice”); their completion should beleft voluntary; shared decision-makingand patient wishes should govern theircompletion;
(6) a plan should be developed for POLSTimplementation and ongoing evaluation;
(7) “a single strong entity” should beidentified who is willing to “acceptownership for the program” and iscapable of implementing it.16
Efforts at spreading the POLST para-digm since 2004 have been remarkablyeffective. As of September 2012, fifteenstates had programs “endorsed” by theNPPTF17 and 30 additional states (orstate regions) had “developing” pro-grams.18 Compare this with the 12 statesprograms and 21 developing programs inJune 2011 (Saunders 2011, iv). POLSTadvocates are well-funded and organized,using an “incremental strategy” to get theprogram up and running throughout states(Saunders 2011, vi). Their commitment toPOLST leads them to focus upon andaccentuate its benefits. No state yet man-dates the completion of a POLST form,but two states (Tennessee and Utah)require that the forms be offered to certainpatients and residents (Sabatino and Karp2011, v.).In closing this brief historical review, we
acknowledge that the POLST paradigmand form must be evaluated mainly in
106 The Linacre Quarterly 80 (2) 2013

terms of their nature and results, ratherthan in terms of the people and organiz-ations associated with them. Still, it isworthy of note that POLST promotionwas not a grassroots effort. Four foun-dations provided substantial donations forcreating and promoting POLST—theGreenwall Foundation (Lewis-Husk andGarland 1999, 10), the Nathan Cum-mings Foundation, the Open SocietyInstitute, and the Robert Wood JohnsonFoundation.19 These same foundationsalso have provided significant funding forright-to-die organizations. To give only afew examples: the Greenwall Foundationfunded Nancy Dubler, member of theBoard of Advisors for Compassion &Choices, in 1991,20 appointed ChristineCassel, physician-assisted suicide advocateas chair of its board of directors in 1999,and awarded a total of $400,000 in grantsto Choice in Dying a New York-basedright-to-die organization, in 1994–1995.21
The Nathan Cummings Foundationawarded $185,000 to Choice in Dyingbetween 1996–1999.22 A decade later,Cummings continued right-to-die fundingby awarding Community Catalyst$135,000 to spearhead a MergerWatchcampaign to “fight religious restrictions onend-of-life care.”23 The Open SocietyInstitute granted assisted-suicide advocacygroup Compassion in Dying $100,000 peryear from 2000 through 2004.24 Finally,the Robert Wood Johnson Foundation(RWJF) funded Choice in Dying at leastas far back as 1998 with a grant for$231,920.25 Perhaps, then, it is not coinci-dental that POLST programs are stronglysupported right-to-die coalitions26 andsome palliative care organizations.Further, many hospitals, health systems
have expressed support for POLST andpromoted its use, up to and including theprovision of payment incentives for phys-icians for completion of advance directiveforms.
Goals and RationalePOLST supporters believe the paradigmrepresents a necessary advance over olderstatutory models for advance care planning.Older models offered instruments topatients to express their wishes for EOLtreatment, and immunity to doctors fromhomicide laws if they executed patients’designated wishes in good faith. The“living will” was the first document of thiskind to receive statutory support. Its orig-inators conceived it as a means for legallyspecifying the conditions for dying—forrevoking consent to treat—for patientswith severe and irreversible pathologies.27
California passed the first living will statutein 1976 (Sabatino 2010). Over the next10 years the majority of states passed sta-tutes establishing living wills as legallybinding documents. In 1990 the U.S.Congress passed the Federal Patient Self-Determination Act28 requiring health-carefacilities to provide written information topatients concerning advance healthcaredirectives upon admission to the facility.Advocates for patient autonomy began to
argue that living will statutes were insuffi-cient to ensure that patient care reflectspatient preferences, especially in cases ofadvanced stage illness when criticaldecisions need to be made. Despite thewidespread availability of living wills, thedocuments, they argued, were frequentlyunavailable when needed, lacked “clinicalspecificity with respect to the here-and-nowmedical decisions faced by seriously illpatients” (Sabatino and Karp 2011, 2–3),and did not embody the clinical normativityof a doctor’s order (Hickmen et al. 2005).These complaints were picked up by the1990 task force at OHSU which arguedthat nothing less than translating patientpreferences into actionable medical orderswould overcome the problem.The three aims of the POLST para-
digm have recently been summarized(Sabatino 2010, 229):
Brugger et al. – The POLST paradigm and form: Facts and analysis 107

• The first is advance care planning; themodel requires a discussion on careoptions between POLST representativesand patients or their surrogates.
• The second is integrating patient prefer-ences into physicians’ orders byrecording them onto POLST forms;each state adopts its own version of theform, but all forms share certain identi-cal characteristics.
• The third is ensuring that the document“travels” with patients and remains appli-cable across all care settings.
The POLST form
State of Oregon POLST FormSee figure 1.
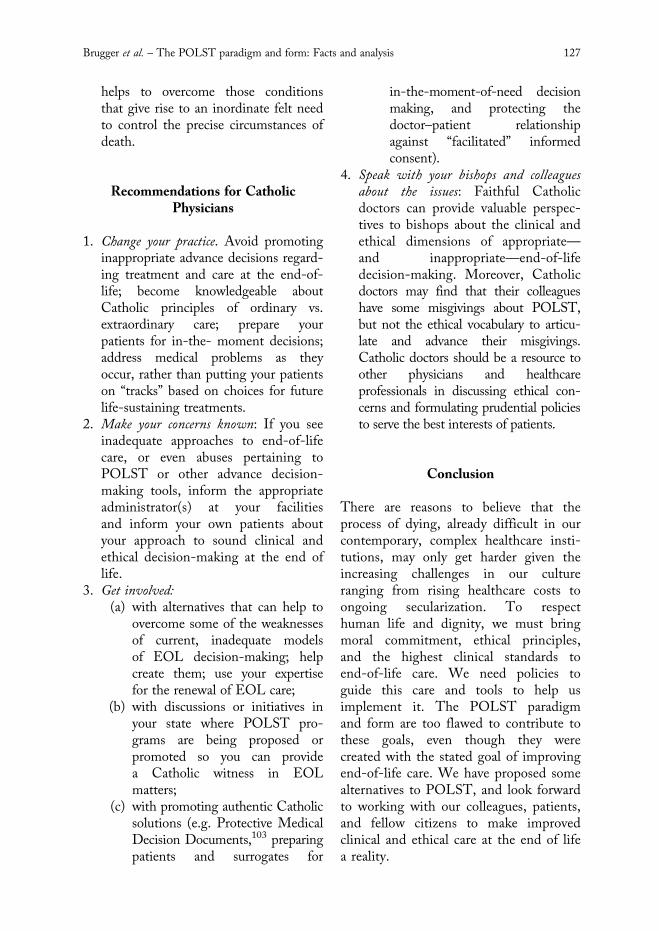
State of West Virginia POLST FormSee figure 2.
POLST forms, on which patients ortheir surrogates specify patient wishesregarding specific types of life-sustainingtreatments, are the centerpiece of thePOLST paradigm. POLST forms areusually printed on brightly colored paper(florescent pink, green, or yellow) so thatthey will stand out for ready reference inthe patient’s medical chart. The forms aresimilar to some advance directives (ADs)insofar as they employ a check-box formatto make preferences known. But thePOLST has one very important difference:traditional ADs provide discretion forclinicians to withhold or withdraw someor all life-sustaining treatments providedcertain conditions regarding patient com-petency and health status (e.g., patient hasbeen diagnosed with a terminal conditionor a state of unconsciousness from whichrecovery is judged unlikely) are met in thefuture. A completed POLST form con-tains a clinician’s signature investing itimmediately with the status of an action-able medical order, whether or not the
patient lacks decisional capacity.29 And, asa standing doctor’s order, the form remainsactive across healthcare venues, whether apatient is in the hospital, at home, oradmitted to a nursing home. It binds notonly hospital and nursing home personnelbut also emergency medical workers.POLST forms always include three sec-
tions of information: introductory topsection, specific medical directives, andbottom section containing the signaturesof a healthcare provider (MD, NP, or PAis generally required) and/or a witness orwitnesses.
Top section
The document’s name and its acronymappear at the top of the page (“POLST”or MOLST, MOST, etc.) along withpatient information and brief instructionsdirecting medical practitioners to “followthese orders.”
Medical directives
Three or four large boxes, depending on theform, contain specific medical directives. Ifpatients have no pulse and are not breathing,the form directs caregivers to follow instruc-tions in box one; if they have a pulse or arebreathing, they proceed to boxes two tofour. The wording of the following sectionsmay vary slightly on different state forms.The first directive is titled “Cardiopul-
monary Resuscitation (CPR).” Patients or“facilitators” (term explained below) aredirected to check one of two directives:“Attempt Resuscitation/CPR” or “Do NotAttempt Resuscitation/DNR.”The second directive is titled “Medical
Interventions.” One of three directivesis checked: “Comfort Measures Only,”“Limited Additional Interventions”(additional, that is, to comfort measures),including antibiotics and intravenous (IV)fluids; but it specifically directs prac-titioners not to use intubation, advanced
108 The Linacre Quarterly 80 (2) 2013
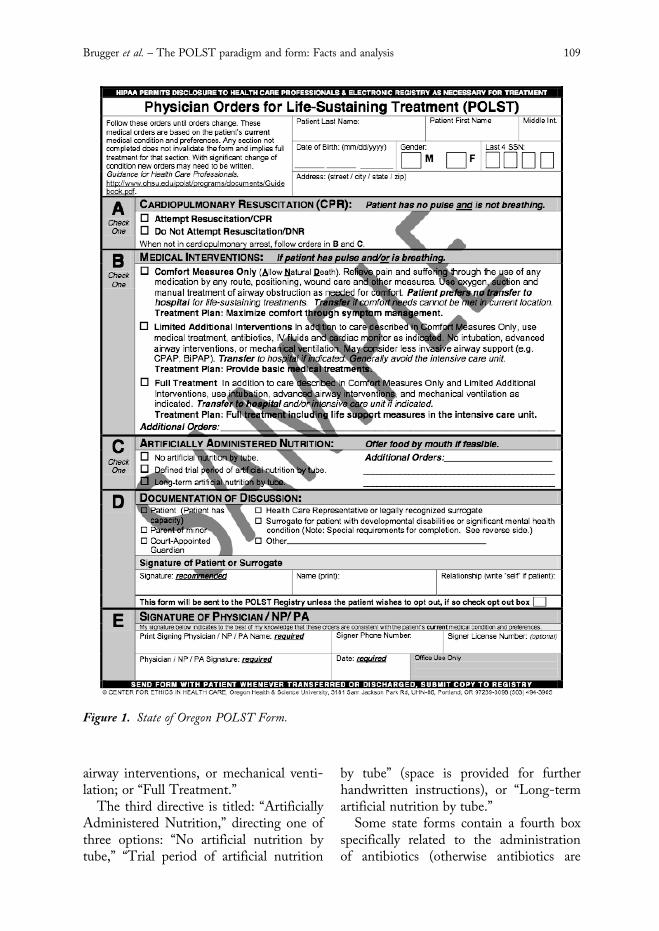
airway interventions, or mechanical venti-lation; or “Full Treatment.”The third directive is titled: “Artificially
Administered Nutrition,” directing one ofthree options: “No artificial nutrition bytube,” “Trial period of artificial nutrition
by tube” (space is provided for furtherhandwritten instructions), or “Long-termartificial nutrition by tube.”Some state forms contain a fourth box
specifically related to the administrationof antibiotics (otherwise antibiotics are
Figure 1. State of Oregon POLST Form.
Brugger et al. – The POLST paradigm and form: Facts and analysis 109

included under the “Medical Interventions”section); one of three directives can bechecked: “no antibiotics: use other measuresto relieve symptoms”; “determine use orlimitation of antibiotics when infectionoccurs, with comfort as goal”; or “use anti-biotics if life can be prolonged.”
Bottom section
At the bottom is a place to specify withwhom the document’s contents were dis-cussed: patient, legal guardian, health-carerepresentative, spouse, etc. Two signaturelines then follow, one for a physician, nursepractitioner, or physician’s assistant, which
Figure 2. State of West Virginia POST Form.
110 The Linacre Quarterly 80 (2) 2013

is always mandatory, and one for thepatient or legal guardian, which in somestates is required (Washington) and inothers only recommended (Oregon). Moststate forms include a second page whichrecords additional contact information ofpatient, caregivers, and practitioners.
Use of “Facilitators”POLST advocates insist that the preemi-nent aim of the paradigm is to honor theinformed wishes of patients. This requiresthat patients effectively be informed of theirprognosis, their options for care, and thebenefits and burdens of adopting one optionover another, and that the information istranslated into a plan of action consistentwith patients’ value systems and desires.The POLST paradigm proposes that
non-physician healthcare personnel (e.g.nurses, social workers, chaplains, admissionscoordinators, nursing home administrators)initiate advance care planning discussionswith patients or their surrogates. These“facilitators,” as they are called, act asfrontline implementers of the POLSTparadigm (Sabatino and Karp 2011, 24).Completed forms are then referred to clin-icians for signature.The Respecting Choices program30 run
by Gunderson Lutheran Medical Centerin La Crosse, Wisconsin, has become anational center for the training of POLSTfacilitators.31 Gunderson has operatedregionally since the early 1990s promotingthe use of advance care planning docu-ments.32 Non-physician candidates mustcomplete an approved training curriculumso they can serve as certified POLSTfacilitators.33
Defenses of POLST
Since its origin in the 1990s, a variety ofjustifications have been put forth for
encouraging the use of POLST formslocally, regionally, and nationally. Webriefly describe here some of these—without regard to order of importance.Promoters of POLST argue that the
form:(1) Ensures patient autonomy: This has
been an essential aim from the outset.(2) Standardizes documentation: An early
paper written by one of the architects ofthe POLST paradigm, Dr. Patrick Dunn,notes that the goal of the MTC was tostandardize documentation (Dunn et al.1996). His group felt the results of theirresearch were so positive that (even priorto the paper’s publication) the groupplanned statewide implementation of theform. This was in 1995. Today, POLSTpromoters boast that POLST has becomethe “medical standard of care” in Oregon(used by all hospices and over 95 percentof nursing homes). Now many other statesalso seeking the goal of standardizationhave adopted the POLST paradigm.(3) Optimizes communication (to diminish
anxiety and disputes among family members):A recent column in the Wall StreetJournal emphasized the importance thatpatient wishes be shared both verbally andin writing with family members (Landro2011). The author, Laura Landro, notes:“Making end-of-life decisions when aloved one’s wishes are not known can bedifficult for families.” She narrates a casein which the competing concerns of thechildren of a terminally ill woman werequelled when they found out their motherhad signed a POLST form limiting life-sustaining procedures: “the POLST madeit easier for us because my mom had madeher own healthcare decisions.”(4) Minimizes the use of unwanted inter-
ventions: Some express fear or frustrationregarding what they deem to be an exces-sive use of medical interventions at theend of life. This was graphically illus-trated by an elderly British woman, Joy
Brugger et al. – The POLST paradigm and form: Facts and analysis 111

Tompkins, who tattooed the acronym,“D.N.R.” (do not resuscitate) on herchest.34 Proponents of POLST stronglybelieve that use of the document can limitunwanted interventions.35
(5) Simplifies decision making: A singleform is simpler than longer documents;consequently, POLST is seen to be asolution to the complexity of EOLdecision-making.(6) Consistency of care across healthcare
settings: POLST advocates note the dis-tinction between POLST and other typesof ADs. POLST is valid across all health-care settings (Dominique 2009). Thisincludes pre-hospital care by EmergencyMedical Technicians, residential carefacilities, and hospitals as well as betweenhospitals. In many cases, the forms areeven honored across state lines.(7) Decreases interventions and the cost of
care at the end of life: Medical care at theend of life consumes 10–12 percent of thetotal healthcare budget, and 10 percent ofthe Medicare budget is spent during thelast 30 days of life (Kurent 2000). POLSTadvocates cite statistics regarding POLST’seffectiveness for limiting interventions:“What we found was that if peoplemarked ‘comfort measures only’ and ‘donot resuscitate’ and did not want to goback to the hospital, there was a 67percent reduction in life-sustaining treat-ments, primarily hospitalization andemergency room visits.”36 GundersenLutheran Health System in recommend-ing legal recognition of statewide POLSTsystems claims its innovative advancedirectives program saves $3,000 to $6,000per patient at the end of life.37 JohnGorman of the Gorman Health Groupbelieves the “POLST solution” is an idealway to cut costs: “There can be no hopeof long-term Medicare solvency withoutmore rational policy and assistance toseniors as they decide how they want todie—not when Medicare spends 1 in 4
dollars today on care in the last 6 monthsof life. The POLST solution … is cheap,effective, and should be encouraged byCMS and the Administration.”38
Problems with POLST
POLST, Patient Autonomy, and Good
Moral Decision-MakingPerhaps nowhere in the area of health carehas the intersection of human freedom anddignity been analyzed so extensively inCatholic teaching as in the development andapplication of the principles of “extraordi-nary” and “ordinary” treatment at the end oflife and particularly in regard to the properuse of medically assisted nutrition andhydration. The following principles havebeen consistently taught the past 50 years:
• Patients have the right and duty to makedecisions regarding the extent of themeasures they choose to conserve theirlives. They are not obligated to acceptor pursue treatments that are “extra-ordinary” or “disproportionate.” In thisregard, there is a wide scope for humanfreedom and for individual/subjectivefactors in someone coming to a con-scientious judgment about limitingmedical interventions at the end of life.
• At the same time, their choices are notethical simply in virtue of the fact thatpatients are competent and legally auth-orized to make them. Patients areobligated to respect their own lives, andto conserve them by pursuing thosemedical treatments that are “ordinary” or“proportionate,” as well as to accept themost basic forms of human care. Thesame is true for surrogates makingdecisions on behalf of patients who arenot competent to make their owndecisions. In this regard, the teachingof the Church on the use of medicallyassisted nutrition and hydration
112 The Linacre Quarterly 80 (2) 2013

illustrates that there are foundationalgoods in human embodiment that mustbe respected in the free choices ofpatients and surrogates alike.
How should claims about the accept-ability of POLST be evaluated in light ofthese principles? Although POLST is saidto be designed for use by terminally andchronically ill elderly, there is nothing inmost POLST programs or state POLSTlaws that actually limits it to this popu-lation. The POLST model introduces aparadigm shift into the statutory and pro-cedural understanding of who is entitledto direct the refusal of life-sustaining treat-ments. The state laws that introducedliving wills into common use in the 1980slimited the rightful use and execution ofrefusal orders to patients who, accordingto the judgment of two physicians, suf-fered from a “terminal condition” or werein a state of permanent unconsciousness.The pedagogical message of those lawswas clear: the refusal of life-sustainingtreatments is sanctioned for persons suffer-ing from irreversible and terminalconditions; refusal was legally contextua-lized within and on behalf of thepopulation of the dying.The POLST model legislation annuls
the requirement that a patient must be term-inally ill before he or she may directthe withholding or withdrawal of life-sustaining treatments.39 We believe that itis naïve to think that if the law makes pro-vision for the inappropriate use of refusalorders by populations who are not termin-ally ill, that some people will not takeadvantage of those provisions.Moreover, as noted, Catholic teaching
distinguishes between rightful and wrong-ful refusal decisions by using the terms“ordinary” (proportionate) and “extraordi-nary” (disproportionate) means of medicalcare. We have an obligation to acceptordinary/proportionate means of medical
treatment, and may forgo extraordinary/disproportionate means. The POLSTmodel and POLST forms make no distinc-tion between ordinary and extraordinarymeans. This sets up an obvious conflictbetween the moral obligation of Catholicinstitutions not to honor (in the words ofERD, no. 24) “an advance directive that iscontrary to Catholic teaching,” and thelegal liberties of patients in those insti-tutions to write such a directive.Finally, every POLST form has a
section dedicated to the refusal of nutri-tion and hydration. But Pope John Paul IIin 2004 clarified that the administration ofnutrition and hydration, even by artificialmeans, “should be considered, in principle,ordinary and proportionate, and as suchmorally obligatory, insofar as and until itis seen to have attained its proper final-ity.”40 In all but cases where a patient isimminently dying or rare instances wherefood and water are no longer adequate tosustain bodily life or their administrationcauses excessive suffering, the decision toforgo them would be wrongful. Butbecause the POLST functions as anactionable medical order, directives towithhold food and water, as well as otherorders to withhold morally “proportionatecare,” may be seen as legally binding andthus influence Catholic healthcare insti-tutions and providers who feel compelledto obey.
POLST and Good Clinical CareEOL decisions are among the mostimportant medical decisions people canmake. Therefore they should be made inlight of the concrete facts of a patient’smedical situation, in consultation withskilled medical practitioners, and with duerespect for the goals and desires of thepatient. The POLST design makes thisdifficult to carry out for at least fivereasons.
Brugger et al. – The POLST paradigm and form: Facts and analysis 113

First, the POLST form offers a simplecheck box list of treatment options.Complex medical decisions are reduced toover simplified scenarios that do notreflect the nuances of actual medical prac-tice. For example, Section A offers achoice between providing or withholdingCPR—specifically, when a patient has nopulse and is not breathing. The patientmust pre-determine either to consent toattempted resuscitation or to reject it. Butwhat if a patient presents with no palpablepulse but is breathing or has a pulse but isnot breathing, for example, as in achoking victim? A simple Heimlich man-euver might be all that is needed in thiscase.41 The healthcare provider is notallowed to use his clinical judgment toassist the patient, but must proceed toSection B and C. Once there, the provideris limited to the vague courses of pre-selected options that are listed there. Butevery patient and clinical presentation isunique and personal. Proper patient carerequires the aptitude and readiness torespond to situations that are complex andvaried. It cannot (and should not) bereduced to a simple predetermined check-list. Each medical decision needs to bemade in the context of a patient’s present-ing situation, which includes hispsychosocial situation especially in regardto his family members.Second, patients may make their
choices weeks, months, or even yearsbefore those choices will be carried out.Ordering future medical decisions in thisway has limitations and potentially seriousoutcomes.42 The decision to forgo anti-biotic use could be a good clinical decisionin one who is terminal and imminentlydying. But it could also be a poor decisionin an acute exacerbation of a chronic dis-ability that may be readily responsive to ashort course of antibiotics. The forms arecompleted prior to the time that manypeople know the exact nature of their
conditions or the range of reasonabletreatment options.43 In other importantareas of life (e.g. investing), people are illadvised to make consequential decisionswithout knowing all the facts. But thePOLST paradigm invites patients to makethe most consequential decision of theirlives before many facts are even possiblyknowable: What precise ailment will I besuffering from? What treatment alterna-tives will be available? What probability ofmedical benefit does each offer? Whatburdens are associated with each? Will Ihave the opportunity to receive the lastsacraments of the Church before I die?Will I have made my final peace withGod and neighbor? Will my children orother loved ones be at my bedside or will Idie alone? Will I have any measure of con-sciousness to put other affairs in order?How will my decision affect those aroundme? A POLST form is a blunt andinadequate instrument that is as likely todo damage as good for people at vulner-able moments of life.Third, as noted above, depending on the
State of origin, the POLST may notrequire a patient’s signature. This sets upa unique medical–legal situation whenspecific DNR orders or termination of careorders are expected to be followed withouta patient’s signature. All other forms ofadvanced directives such as living wills anddurable powers of attorney are signed bythe patient and witnessed. Defenders ofPOLST reply to this criticism by notingthat traditional medical orders, such as hos-pital DNRs, operate with only a clinician’ssignature.44 If this is not problematic, whyshould there be a problem with POLSTdocuments? This reply is unsatisfactory.Hospital DNR orders by a physician areinherently contextual, that is, they reflectthe actual circumstances of a patient’soverall condition at the time the order ismade. POLST orders by a physician arenot.
114 The Linacre Quarterly 80 (2) 2013

Fourth, the POLST design as a pre-signed medical order is transferable acrosscare settings. This could allow a healthcareprovider in one setting to order that EOLcare be withheld from a patient who hasbeen transferred to a different setting,without the provider having privilegeswithin the patient’s new medical facility.When a patient is transferred (admitted) toa new facility, standard medical practice isfor the admitting physician at that facilityto write new medical orders based on thepatient’s current medical condition. Itseems that POLST abrogates this practice.Moreover, the transference may lie outsidethe scope of hospital bylaws, which gener-ally require that ordering doctors must beon staff in the particular institution. Theorder is also effective immediately uponarrival in the facility’s emergency room orhospital room without the standard pro-cedure of assessing the patient’s medicalsituation, consulting the patient or patient’ssurrogate and writing new appropriateorders. This may preclude reasonable clini-cal care based on the presentation of thepatient. Again, in order to properly assessthe medical situation in view of thepatient’s goals and desires, the medicaldecision-making process needs to becontextual.Fifth, we have concerns with the verbi-
age used and the underlying psychology ofthe POLST form, which seem to carrya bias in favor of non-treatment. TheWisconsin POLST, for example, ratherthan using the term “full treatment” usesthe term “aggressive treatment.” Patientsare asked to choose between “aggressive”measures, “limited” measures,” or“comfort” measures. “Aggressive” measuresare defined as “endotracheal intubation,advanced airway, and cardioversion/automatic defibrillation.” The term“comfort” measures, however—which, ofcourse, means non-treatment—is explainedas follows: “The patient is treated with
dignity, respect and kept clean, warm anddry… offer(ed) food and fluids by mouth,and attention is paid to hygiene…measures are used to relieve pain and suf-fering,” etc. The tone of presentation ofthe two options is quite different.45 Simi-larly, the Washington State POLST,under the section dedicated to the admin-istration of antibiotics, offers as the thirdof three options: “use antibiotics if life canbe prolonged.” The term “prolonged” hasnegative implications. A “prolongedabsence” implies an unwelcomed delay; a“prolonged stay” implies overstaying one’swelcome; a “prolonged period” impliesdragging on and on. Why not use neutrallanguage such as “use antibiotics if medi-cally indicated for healing or preservationof life”? Additionally, most state forms usethe term “artificially administered nutri-tion,” rather than neutral terms such as“medically administered nutrition andfluids” or “provision of food and water.”46
Something “artificial” is opposed to whatis “natural.” The POLST gives theimpression that patients who are fed andhydrated via technical means are beingkept alive unnaturally.
POLST, the Role of Physicians and
Fundamental Ethical Values
Role of the Physician
At the heart of medicine is the individualencounter between physicians andpatients. Physicians must conscientiouslydo their best for patients including provid-ing explanations about patient conditions,a prognosis and a set of treatment alterna-tives specifying the benefits and burdensof each alternative. Truly informedconsent requires precise, truthful and clearinformation at the proper time in amanner that patients and their familiescan understand.This need for clear communication is
never more keenly felt than when
Brugger et al. – The POLST paradigm and form: Facts and analysis 115

physicians care for dying or chronically illpatients who are incapable of understand-ing the gravity of their situation. Doctorsinfluence not only with their words, but bytheir attitudes, the amount of time theyspend with patients, the frequency of theirvisits, the personal feelings they expressabout certain types of disease, and eventheir own views on death. In 1806,Chrisoph Hufeland recognized this issuewhen he wrote: “It is not up to [thedoctor] whether … life is happy orunhappy, worthwhile or not, and should heincorporate these perspectives into histrade … the doctor could well become themost dangerous person in the state” (Smith1997, 70–1). He recognized that the tre-mendous power given to physicians bysociety can be used for good when patientsare viewed as having inherently equalworth, but can be abused when doctorsimpose their own values.47
Physician–Patient RelationshipThat power for doing good is principallyexpressed in and through physicians’ diag-nostic expertise and ability and readinessto offer precise and timely treatment ofsickness. Because of the difficulty in pre-dicting all possible contingent scenarios atthe end of life, and because patients andfamilies often change their minds at criti-cal moments, the POLST may placeunreasonable restrictions on their ability toknow the real-time wishes of patients andto offer them the best care possible. Asone author wrote: ADs “promise morecontrol over future care than is possible”(Perkins 2007). Many primary care phys-icians practicing in large medical systemsdo not care for their own patients duringemergency visits or hospital admissions—the times of greatest vulnerability of death.Deprived of the security of personalrelationships with their physicians, patientsmay seek comfort through instruments
like POLST. Yet beyond the marks onthe page, these documents are mute. Theydo not know their patients, express noexpert opinions, are never poised andready to meet the complex demands of theunexpected; in every situation, they mouththe same words. They cannot possiblyembody the knowledge, readiness, andpersonalized care of a doctor who hasknown his or her patient for many years.The problem of the weakening of the
doctor–patient relationship is bigger thanthe POLST form. Because of a tight prac-tice schedule and a large impersonalcommunity, physicians may know littleabout their patients or their families.Clinic time is limited for detailed discus-sions about values, even when completingforms treating subjects as important asEOL wishes. The goal of an EOL plan-ning meeting can easily change fromhaving a thorough discussion of values,wishes, and options to merely completingthe form. Talking about the end of lifemay be left to other staff and the physicianis presented with a completed form tosign, or even at times the form is signedwithout any conversation with the patientat all. If physicians do not participate inthe discussion in a meaningful way, ortake any kind of detailed notes aboutsubtleties of their patients’ wishes, howwill they be able to provide the kind ofcare that patients think they have commu-nicated? Does this constitute informedconsent?
Marginalization of the role of physicians
and delegation of the informed consent
process to facilitators
Education and counseling about medicalinformation necessary to informed consentbelong to the physician–patient relation-ship. The American Medical Association(AMA) Code of Medical Ethics states:“The patient’s right of self-decision can be
116 The Linacre Quarterly 80 (2) 2013

effectively exercised only if the patientpossesses enough information to enable aninformed choice… The physician’s obli-gation is to present the medical factsaccurately… Informed consent is a basicpolicy in both ethics and law that phys-icians must honor.”48 The AMA alsocounsels physicians that “in the communi-cations process, you, as the physicianproviding or performing the treatmentand/or procedure (not a delegated represen-tative), should disclose and discuss withyour patient” the different treatmentoptions available and the nature, purpose,risks and benefits of each option, and therisks and benefits of forgoing particulartreatment options. “This communicationsprocess,” it continues, “or a variationthereof, is both an ethical obligation and alegal requirement spelled out in statutesand case law in all 50 states.”49
As stated above, under the POLSTparadigm, non-physician facilitators under-take this critical communications process:they approach patients, initiate POLSTconversations, “assist in making informedend-of-life decisions,”50 complete thePOLST forms, and submit the forms todoctors for their signatures. Sabatino andKarp state that facilitators “provide much ifnot most of the patient counseling andassistance in completing POLST forms”(Sabatino and Karp 2011, 24). Althoughthis may be an efficient way to increase theutilization of advance decision-makingdocuments in a given community,51 it mar-ginalizes the role of physicians from an areaof medical care that by definition—“end-of-life”—has life and death impli-cations. “More often than not the physicianrole is to verify the choices made and theprocess used and then sign off on theorders.”50 One study found that, whereasphysicians are required to sign POLSTforms, 72 percent of the POLST forms ofnursing home residents were completed byfacilitators; “in light of such data, physician
participation in POLST completionappears to be tepid” (CANHR Policy Brief2010, 3).Moreover, physicians bear primary
responsibility for patients and, as such,write orders directing care and treatmentsfor their patients. Other healthcare pro-fessionals, primarily nurses, are in frequent,direct contact with the patient and in thatrole are responsible for carrying out theseorders. It is standard care for nurses toinform physicians of the status of theirpatients and of any unexpected develop-ments or adverse reactions to treatments.This collaborative relationship, mutuallyinforming, enhances patient safety andcohesiveness of the team. In light of this, itis concerning that the POLST forms from10 states have printed at the top statementsto the effect: First Follow These Orders, ThenContact Physician [original emphasis].52
Healthcare professionals have a responsibil-ity to carry out doctors’ orders, but neverwithout question. Acting in accord withthis statement could jeopardize the safety ofpatients. Licensed healthcare professionalsare placing their professional conduct atrisk by carrying out orders that may not beappropriate for the patient.
Facilitator scripts and materials contain
negative bias regarding life-sustaining
treatment
Facilitator trainees, as nonphysicians, havelittle or no preexisting knowledge regard-ing indications for and relative benefitsand burdens of life sustaining treatments.However, facilitator training scripts and
materials have been found to have aninordinate emphasis on burdens of lifesustaining treatments53 while dismissing thedisadvantages and potential complicationsof rejection of treatments.54 For example,the likelihood of certain death without life-sustaining treatments seems to be absentfrom discussions. Having no prior
Brugger et al. – The POLST paradigm and form: Facts and analysis 117

knowledge and in light of training that maybe negatively biased, facilitators may take onnegative attitudes toward life-sustainingtreatments. In one study, for example,California Advocates for Nursing HomeReform found that materials accompanyingPOLST forms are “meant to sway patientdecisions … [and are] clearly intended toconvince patients or their representativesto forego CPR” (CANHR Policy Brief2010, 5).
Healthcare institutions, employed
facilitators, and potential conflict of
interest
Sabatino and Karp (2011, 13–16), asstated above, describe the central roleplayed by facilitators in implementing thePOLST model. Local healthcare organiz-ations, hospitals and nursing homes, maysend their non-physician staff (socialworkers, nurses, administrative staff) forfacilitator training, engaging them inPOLST form completion and submissionto physicians. We question whether suchorganizations and institutions possesslegitimate authority to delegate informedconsent and thereby alter the physician–patient relationship. It appears that mostfacilitators are employees of the insti-tutions in which they perform POLSTpatient facilitation. Thus, it seems reason-able to consider whether hospital-employed facilitators create a financialconflict of interest in their institution-appointed duties. Given that hospitalMedicare reimbursement is a fixed pricebased on admission diagnosis (diagnosis-related group) (Reinhardt 2009), whenpatients agree to fewer life sustainingtreatments upon conversations with nega-tively biased facilitators, hospital costsdecrease while profits increase. This is notto imply that administrators seriouslyponder financial trade-offs for theirclients, even in light of the cost crisis in
health care. Nonetheless significant costsavings have been achieved at the end oflife with POLST/facilitator programs andmay constitute a powerful driver for sub-scription in facilitator programs.55 Weshould not forget examples where medicalplans have unethically balanced costs oftreatment against patients’ lives, such as adisturbing case where the Oregon HealthPlan refused to cover expensive che-motherapy for a woman with lungcancer, but offered to cover drugs if shewished to consider physician-assistedsuicide.56
Lack of Evidence that POLST Orders
Reflect Patient WishesThe POLST paradigm was designed “toensure that seriously ill patients can choosethe treatments they want and that theirwishes are honored by medical provi-ders.”57 But whether POLST accuratelycaptures the treatment preferences ofpersons for whom POLST orders arewritten is an important question. Discre-pancies between patient wishes and thecontent of orders can be particularlyserious, given the irreversibility of someorders.Research summaries on the national
POLST web site report that medical careis almost always consistent with POLSTorders (i.e., that POLST orders are fol-lowed) and that such orders record a highpercentage of treatment refusals.58 Instudies involving a group of 255 deceasedpatients, the Hammes study found thatmedical caregivers followed POLST ordersover 90 percent of the time; and the ordersrefused full medical treatment 92 percent ofthe time.59 But a high percentage ofPOLST compliance and treatment refusalare not in themselves evidence thatPOLST orders reflect patient wishes.According to the national POLST web
site’s Quality/Research tools, a 2004 study
118 The Linacre Quarterly 80 (2) 2013

by Meyers et al. (2004) is “the only pub-lished evaluation of whether POLSTorders match patient preferences.”60 Butthe authors of the Meyers study state thatthe small sample size and other limitations“preclude an accurate determination of theform’s effectiveness and diminish anyinferences that can be made.” (Meyerset al. 2004, 43) Despite this, the nationalPOLST web site references the Meyersstudy to say POLST accurately conveyswishes 90 percent of the time.60 More-over, a recent major study involving over1700 nursing home residents, called for“additional data that the orders on thePOLST form are reflective of residenttreatment preferences, as has beensuggested by previous pilot research [theMeyers study]” (Hickman et al. 2010,1247).Further, even if wishes were recorded
accurately, there is evidence that the stab-ility of recorded decisions is low.Researchers have found that patient pre-ferences for life-sustaining treatmentschange up to 77 percent of the time whenquestions are asked differently (Fagerlinand Schneider 2004, 33), and patients arefrequently uncertain when their wishes areinitially recorded (up to 45 percent of thetime) (Sudore et al. 2010).Other research has examined how
patient decisions vary depending on poss-ible outcomes. A study in the NewEngland Journal of Medicine (Fried et al.2002) found the vast majority of patientswho would qualify for a POLST in factwant treatment. They enrolled 226 people(with advanced cancer, congestive heartfailure or chronic obstructive pulmonarydisease) whose primary care physicianssaid had limited life expectancies. Asked ifthey wanted medical treatment to avoiddeath and return to their current state ofhealth, 88.8 percent said yes to more thana month in the hospital, being on a venti-lator, in the ICU, having surgery or the
like. Another 9.9 percent said yes to treat-ments such as a week in the hospital andIV antibiotics. The desire for treatmentdid not drop significantly until the odds ofsurvival with recovery dropped below 10percent.61 Just over half of them diedduring the following two years, yet theirdesires for intensive treatment with only a50 percent chance of recovery stayed rela-tively stable: during the four 6-monthperiods over the two years, the desire forintensive therapy was 87, 90, 93, and76 percent (Cosgriff et al. 2007). Thisdisparity in patient preferences as com-pared with typical POLST orders (in arather large sample and well designedresearch study) is disturbing (see table 1).
Table 1. Percent of patients desiring treatment
POLSTpreferences (%)
Fried et al.(%)
Hospitalization 38 98.7
Intensive care unit 8 88.8
Mechanicalventilation
8 88.8
Intravenousantibiotics
43 98.7
Moreover, Fagerlin and Schneider(2004, 33) note that “…answers [onadvance decision making documents] areshaped by the way questions are asked.Preferences about treatments are influ-enced by factors such as whether successrates or failure rates are used, the level ofdetail employed, and whether long- orshort-term consequences are explainedfirst.” They cite an example: “201 elderlysubjects opted for the intervention 12% ofthe time when it was presented negatively,18% of the time when it was phrased asin an advance directive already in use,and 30% of the time when it was phrasedpositively. Seventy-seven percent of thesubjects changed their minds at least oncewhen given the same case scenario but adifferent description of the intervention”
Brugger et al. – The POLST paradigm and form: Facts and analysis 119

(Fagerlin and Schneider 2004, 33). Theyfurther observe that living-will type ofdocuments “have come to have two pur-poses that are in tension… to honorpatients’ autonomy by having them maketheir own decisions… [and] to preventdying patients from being over treated.The second purpose has become so centralin the mind of patients and the doctors,social workers, and lawyers who counselthem that the first purpose quite gets lost.But these are truly life-and-deathdecisions, and they deserve to be madewith greater care than we fear they cur-rently are or could be in a world wheremost of us have living wills.”62
Hickman et al. (2010), found thatnursing home residents with POLSTforms are far more likely to have orderslimiting life-sustaining treatments beyond“No CPR” than those with conventionaladvance directives (98.1% vs. 16.1%). Inaddition, fewer life-sustaining treatments,such as IV fluids, are utilized in compari-son with patients having conventionaladvance directives. The authors concludethat: “The POLST program’s associationwith less use of unwanted life-sustainingtreatments in a large, geographically dispa-rate sample is unprecedented.”The assertion that POLST lessens
“unwanted life-sustaining treatments”must be challenged. In light of innovationsof the POLST paradigm—facilitatedinformed consent, unwitnessed interviews,lack of patient signature—how canmedical professionals called upon toexecute POLST orders be confident thattreatments are truly unwanted? We findtroubling the lack of reliable research toconfirm that POLST accurately capturesthe wishes of patients about life-sustainingtreatments.We also suspect that POLST may be
fraught with a tendency for errors, givenpressures to produce real-time POLSTorders in locations where the form is
“required” for admission to hospitals andnursing homes (CANHR Policy Brief2010, 6), and at sites that make patient/surrogate signature optional. Thus theinherent problems of advance decision-making may be amplified by the immedi-acy of POLST order preparation andimplementation.The President’s Council (2005, 76)
states: “a living will that is so ‘effective’ inthis sense might well be too effective, tooeasy to act on quickly, when the familymight wish to make care decisions moredeliberately, in light of changing circum-stances and new information.” It shouldbe noted that in some jurisdictions,POLST forms override all other advancedirectives, including the agent specifiedunder a durable power of attorney.63
POLST Candidacy: The Ever-
Expanding Circle of InclusionPOLST was originally conceived forpatients clearly at the end of their lives, incontrolled healthcare settings, for whomdisabling life-threatening complicationswere anticipated (Briggs 2003). Suchrestrictive parameters for use of POLSTcan be replaced with looser limits oralmost no limits, as borne out in variouslocations throughout the country.For example, the first version of a
POLST used at Gundersen Lutheran inLaCrosse, Wisconsin, was for patients withrenal failure who could suffer a stroke orheart attack while on dialysis (Briggs 2003).As described below, POLST is now beingrecommended for people who may beexpected to live for five more years or whosimply live independently in low-incomesenior apartment complexes.Deciding that a person was near the
end of life was at first based on alife expectancy of six or fewer months ifan illness runs its course.64 Because esti-mating when someone will die is very
120 The Linacre Quarterly 80 (2) 2013

difficult, even for doctors who work withthe dying, the following question wasdeveloped initially to encourage patientreferrals for hospice services, “Would yoube surprised if this patient died in the next6 months or so?” (Lynn et al. 2008). Thequestion for POLST eligibility is usually:“Would you be surprised if this patientdied in the next year?”65 Some systems usetwo years.66 In Oregon, the question is“Would I be surprised if this patient diedor lost decision-making capacity in thenext 1–2 years?”67 Legislation recentlypassed in New Jersey not only hasexpanded POLST to patients who have alife expectancy of less than five years, butalso to patients who “otherwise wish tofurther define their preferences for healthcare, to make their preferences concerninglife-sustaining treatment or other interven-tions known in advance.” Such adescription could encompass any person inany state of health.Other examples may be given.
California Advocates for Nursing HomeReform (CANHR) reported that “someproviders have been giving out POLSTsto practically all patients, healthy or ill,with healthcare directives or not.”68 In oneWisconsin community all individuals inlow-income senior apartment complexesare considered eligible for POLST.69
Some recommend POLST for all nursinghome residents,70 even though over half ofthem live in nursing homes for more thana year (Jones et al. 2009, 4), and 25.3percent for more than three years.71
People discharged from hospitals to theirown homes with home care are anothercategory (Jones et al. 2009, 4). In WestVirginia, the form is to be “completed forany individual with a chronic illness whomay need a life-sustaining treatment inthe future to attempt to survive.”72 Thiscriterion would include a 25-year-old withasthma or diabetes; for that matter mostof us within some finite period of time
will have a chronic condition, and on anygiven day each of us could find ourselvesin an emergency situation needing treat-ment to survive.Yet another expansion is to individuals
with disabilities and children. Accordingto the Delaware MOLST Coalition,citing New York, “persons with mentalretardation or developmental disabilitiesor persons with mental illness withcapacity (capable of making their owndecisions)” can complete MOLSTs as canparents of minor children.73 In September2012, the California’s Children’s Hospice& Palliative Care Coalition offered aseminar entitled “POLST: Beginning theConversation for Pediatrics.”74 ThisCoalition claims its “success is particularlyvital to the more than 17,000 low-incomefamilies in California whose children havebeen diagnosed with life-threateningconditions such as cancer, cysticfibrosis, muscular dystrophy, and cerebralpalsy.”75
While POLST was originally designedfor patients at the end of their lives andcontinues to be described as such,76 near-ness to end of life is by no means theexclusive criteria for POLST. Beginningwith the question formulated above andextending over time and with newPOLST rollouts, the paradigm developsan ever-broadening circle of inclusion.The expanding of “eligible” populationsthrough loosened inclusion criteria is onemore factor widening the doorway formisuse, for medically inappropriate restric-tions of treatments leading to the untimelydeaths of patients, especially those who arelow-income. Recently, in Delaware, wherePOLST is called MOLST77 the StateDivision of Public Health asked all health-care workers to refrain from followingMOLST orders until new state regulationsare issued because “there have been reportsof facilities and healthcare providers com-pleting ‘MOLST’ forms on patients who
Brugger et al. – The POLST paradigm and form: Facts and analysis 121

have not been determined to be terminallyill.”77
POLST Compliance and Respect for
ConscienceA growing number of states currently havePOLST programs and many others aredeveloping them. In considering theimpact that such programs have or mayhave on conscience rights or the religiousfreedom of healthcare providers, it isimportant to recognize that differencesexist between state programs. To illustratethese variations we focus on POLST pro-grams in three states, Maryland, NewJersey, and Oregon, asking the followingthree questions: Is POLST addressed inthe law? Are healthcare providers com-pelled to execute and comply withPOLST forms? What can be done torespect conscience and religious freedom?POLST and the Law: Are NPPTF
endorsed POLST programs always intro-duced through the state legislative process?States address POLST through variousmechanisms, which may be laws, regu-lations, or guidelines. For example, inMaryland, the MOLST program is con-tained in the state code78 with regulationsin the process of being formulated by theMaryland Dept. of Health and MentalHygiene. Likewise, New Jersey lawaddresses POLST.79 However, Oregon, thestate where POLST originated, has nolegislation pertaining to POLST. It is onlyaddressed in Oregon Administrative rules.80
Freedom of conscience and religious liberty:Are healthcare providers compelled toexecute and comply with POLST forms?Proponents often imply that once aprogram is implemented POLST formsare required, recognized, and binding. Yet,state requirements and exceptions vary.In Maryland, pending regulations state
that certain facilities will be required toaccept, update, and complete a MOLST
for each patient during the admissionprocess.81 This reflects the state law,which provides that a health facility shallaccept a completed MOLST upon admis-sion for each patient or complete aMOLST order during admission for eachpatient being admitted or discharged.82
Furthermore, the law says that a facilitymust comply with all medical orders in aMOLST form regardless of whether thephysician or nurse practitioner who signedthe form has admitting privileges or isotherwise credentialed at the facility.83
However, there appears to be an exceptionto this requirement to comply since itrefers to certain instances covered inanother portion of the Maryland codeaddressing advance directives.84 Yet, eventhis limited exception seems to tilt towardrequiring compliance.The administrative rules in Oregon
state that physicians and physician assist-ants must comply with POLST, even ifthe physician, physician assistant, or nursepractitioner who executed the form doesnot have admitting privileges at the facilitywhere the patient is being treated.85
However, the rules do state that, inkeeping with the state’s advance directivelaw, unwilling providers may refuse tocomply.86 This provision includes anexception for facilities, organizations, orproviders based on religious or philosophi-cal beliefs but does require that theprovider must be willing to discharge ortransfer the patient.87
In New Jersey, POLST forms areintended to be honored by all personnelattending the patient.88 However, private,religiously affiliated healthcare institutionsare not required to participate in withhold-ing or withdrawing of specified measures89
if particular requirements are met. Thoserequirements include the formulation ofinstitutional policies and practices whichare properly communicated to the patientor the patient’s representative upon
122 The Linacre Quarterly 80 (2) 2013

admission or as soon thereafter as possibleand, if conflicts between the healthcareprovider and patient cannot be resolved,the provider takes all reasonable steps totransfer the patient.90
Protecting conscience and religious liberty:What can be done to respect conscienceand religious freedom? The above discus-sion refers to only three states but providesan illustration of ways in which healthcareprovider compliance varies. In additionto laws, regulations, and guidelines thataddress noncompliance, it is likely thatvarious programs and facilities may exertpressure on physicians to comply. Thus, itis important that facilities and providerstake steps to preempt any appearance ofcoercion. We discuss some of these stepsbelow.
Problems with AdvanceDecision-Making in General
Do advance planning documents
facilitate good moral decisions?Catholic moral principles and advancemedical decision-making:The Ethical and Religious Directives
state:
In compliance with federal law,91 aCatholic healthcare institution will makeavailable to patients information abouttheir rights, under the laws of their state,to make an advance directive for theirmedical treatment. The institution,however, will not honor an advance direc-tive that is contrary to Catholic teaching.If the advance directive conflicts withCatholic teaching, an explanation shouldbe provided as to why the directivecannot be honored (No. 24).
This directive was added after Congressin 1990 passed the federal Patient SelfDetermination Act requiring healthcarefacilities to make available to adult patients
upon admission to the facility informationabout advance healthcare directives. Itshould not be read as an endorsement bythe U.S. bishops of advance directives oradvance decision-making. It states thatsome decisions specified on advance plan-ning documents may conflict withCatholic moral teaching; if they do, theyshould not be honored. In compliancewith federal law, it is vital that patientsshould be informed of this policy byCatholic institutions upon admission.How can patients and their physicians
ensure that advance planning decisions areconsistent with moral principles? And howdo healthcare workers determine whetheran advance directive conflicts with Catholicteaching?ERDs 56 and 57 state that decisions
to refuse life-sustaining treatments arelegitimate as long as these treatments aredisproportionate/extraordinary. But in whatsituations can a Catholic determine inadvance that a life-sustaining treatment isdisproportionate, removed from the contextof the specific, future situation of medicalneed?We would like to suggest a simple test
to determine whether the risks of advancedecisions to withhold specific treatmentsare justifiable, through the satisfaction oftwo separate but simultaneous conditions.(By advance decisions, we are talkingabout decisions made well before patientsfind themselves in a compromised state ofhealth; on advance planning forms, suchdecisions are often preceded by phrasessuch as, “If I am in a condition such asterminal disease or dementia…”. However,POLST forms contain no such clarifyingconditions).The first condition we call “medical
imminence,” and addresses the question,“Which decisions to withhold treatmentmust be made in advance?” To fulfill thiscondition, the treatment is of the type thatmust be administered immediately or a
Brugger et al. – The POLST paradigm and form: Facts and analysis 123

patient will die. Why “medical immi-nence”? Because when consideringnon-imminent life-sustaining procedures(such as antibiotics or medically adminis-tered nutrition and hydration), there is nourgent need for advance decision-making,there is time to reasonably consider alloptions once the need arises. In short,decisions for or against non-imminenttreatments are best made, together withpatient and/or surrogate, at the time theneed is apparent, weighing actual medicalcircumstances rather than a “best guess” ofsome future theoretical situation that hasbeen posited.The second condition we call “sufficient
moral foresight.” It would only be justifi-able to reject in advance some treatmentthat sustains life if a patient could accu-rately judge now that receiving thattreatment in the future would be extra-ordinary or disproportionate. However,given the multiplicity of factors that mightimpact on such an analysis—factors thatcreate the setting in which a treatmentbecomes proportionate or disproportion-ate, the ability to make in advance anaccurate judgment in this regard islimited. There are exceptions—mechanicalventilation may meet both the conditionof medical imminence and sufficient moralforesight, as, for example, when an indi-vidual is diagnosed with end-stage chronicobstructive pulmonary disease when event-ual extubation is unlikely. There may beother examples, particularly as this relatesto cardiopulmonary resuscitation (meaningchest compressions) in certain individualswith advance illness.Deciding in advance to withhold life-
sustaining treatments without such dueconsideration poses unacceptable andunjustifiable risks to the good of thepatient. We believe that the paradigm ofsoliciting treatment choices in nursinghomes using checkboxes on a form, far inadvance of the actual medical events, may
pressure patients and surrogates to makeinappropriate decisions lacking due moralconsideration. We strongly recommendthat this paradigm be abandoned.
RECOMMENDATIONS
To assist physicians and healthcare facili-ties in offering an effective response to theproblems we have discussed, we offer thefollowing recommendations.
Replace the POLST Modelof End-of-life Care with “Preparationfor in-the-Moment-of-Need Medical
Decision-Making”
If the model of advance medical decision-making as formulated in POLST forms isill advised, what model then should beused in its place? We recommend a modelthat Sudore and Fried (2010) referred toas “preparation for in-the-moment-of-needmedical decision making.” Sound clinicaland ethical decisions are best made whenactual medical facts and the complexitiesof patients’ conditions, including previousresponses to treatment and burdens andbenefits of available options, are weighedand considered in the moment of medicalneed. This requires that doctors and othercaregivers have the information necessaryto make the appropriate decisions. Sincerelevant information, especially in crisissituations, cannot always be communicatedorally by patients in their moment ofneed, we recommend that patients,especially elderly and chronically illpatients, should provide authorization inadvance to surrogate decision makers, whoknow of their values and are willing towork with medical teams, to speak ontheir behalf in cases of incapacitation.Sudore and Fried recommend that surro-gates engage in open discussions about
124 The Linacre Quarterly 80 (2) 2013

patients’ values and be given leeway to workwith doctors to make the best decision theycan in light of these values. A physicianshould engage patients and surrogates inconversations ahead of time, and preparethem to be able to participate in making thebest possible medical decisions in-the-moment. Compare this to the all or nothingapproach of advance decisions where ques-tions are often posed as, “If you suffer aserious complication, do you want every-thing done or stop all efforts?”92 Real lifein-the-moment decisions can consider avariety of appropriate options centered onthe patient’s actual situation—weighingspecific benefits and burdens of each—unlike the limited choices and consider-ations offered in advance on a POLSTform.
Recommendations for Caring for“Unbefriended” Elderly Persons
(1) Raise awareness of the problem of theunbefriended: Patients who lack deci-sional capacity, have no advancedirective, and no one to serve as theirhealthcare surrogate are sometimesreferred to as “unbefriended.” Theyare at risk of overtreatment, under-treatment, or treatment inconsistentwith their values.93 Unbefriendedpeople who become problematic dis-charges are estimated to account for1–2% of patients.94 The majority ofunbefriended people are thought tolive in hospitals and nursing homes.Roughly 3–4% of nursing homeresidents are estimated to be unbe-friended (White et al. 2007).
(2) Identify alternatives to properly care forthe unbefriended: Studies indicate thatdiligent searching can locate surro-gates for close to half of those initiallythought to be unbefriended (Griggons2010). Even this leaves a significant
number of people who fall into thecategory. A 2010 Information Brief bythe National Long-Term CareOmbudsman Center, titled “Advocat-ing for the Unbefriended Elderly,”provides information about severalpromising practices.95 Most of theserevolve around finding people to serveas healthcare surrogates for theunbefriended.96
(3) Create diocesan and parish programsand ministries to better meet the needs ofthe unbefriended: Within the Catholiccommunity, some dioceses coordinateparish-based programs where parishnurses or lay volunteers (sometimesusing the Befriender Ministry model97
or the Stephen Ministries model98) visitthose who are hospitalized, living inresidential care settings, or homebound.These programs could be tapped totrain volunteers to help those at risk ofbecoming unbefriended in a healthcaresetting to name health agents. Theymight also be tapped to locate volun-teers willing to serve as agents.
In dioceses without these programs,diocesan bishops or parish pastors shouldconsider establishing ministries that makeavailable a pool of suitably trained personsto serve as surrogate decision-makerscapable of being and willing to be assignedpowers of attorney. In this way, the Catho-lic community can take responsibility for itselderly and infirmed brothers and sisterswho are often tempted by the fear of over-treatment to have recourse to simplisticalternatives such as the POLST form.
Recommendations for CatholicHealthcare Facilities
1. Do not accept POLST forms and declineto participate in the POLST paradigm.99
Given the significant flaws in the
Brugger et al. – The POLST paradigm and form: Facts and analysis 125

POLST paradigm and form and theethical hazards inherent in theirimplementation, we think the mostprudential policy for Catholic health-care facilities is to not accept POLSTforms and to decline to participate inPOLST programs. We advise insti-tutional administrators to delineate inwriting the principles necessary tomake ethically sound advance medicaldecisions (e.g. explicitly setting forththe distinction between proportionateand disproportionate means of care andintroducing the concepts of “medicalimminence” and “sufficient moralforesight”). Administrators should for-mulate specific policies based on thoseprinciples, stating that, because of theinherent risks associated with POLSTorders, their institution shall not use orrecognize POLST forms, nor will itexecute any AD that conflicts withCatholic moral teaching.100 The rightof an institution to delineate “EthicalPrinciples and Policies” regarding EOLtreatment and care is recognized inthe Patient Self-Determination Act(PSDA).101 Healthcare facilities shouldprovide such written principles andpolices to all patients on admission.Following the lead of the bishops ofMinnesota, we recommend thathealthcare facilities that already haveimplemented POLST should reviewtheir POLST forms and update themas quickly and as much as possible toensure compliance with patients’ wishesand informed consent, and withCatholic moral principles. Ideally, evenafter these improvements, suchPOLST forms would be phased outand replaced with better alternatives. Inthose few states that obligate providersto comply with POLST orders,102
doctors and staff should be appraisedof the dangers these documents poseand of their primary obligation to
follow the ERDs and institutionalprinciples and policies. In addition,they should be provided assistance onfollowing their consciences as opposedto merely following documents.
2. Avoid using forms (such as living wills)with a simplistic checkbox format forrejecting treatment options in advance.These documents may induce people tomake hasty decisions without full andinformed consent, and minimize theimportance of the considerationsnecessary for sound clinical and ethicaldecision-making.
3. Discourage advance decisions to rejectnon-medically imminent treatments.This draws attention to the difficulty ofsecuring sufficient moral foresight forpersons making these decisions.
4. Counsel patients to select a healthcareagent and offer them the opportunity tocomplete a protective durable power ofhealth attorney.103
5. Enact programs for training medicalpractitioners and other staff involved inEOL care about:(a) the principles and norms taught in
ERD nos. 24–26, 28, 56–59 and57. Medical and nursing staffshould understand the basic cri-teria for judging rightly whetherparticular treatment alternativesconstitute extraordinary (dis-proportionate) or ordinary(proportionate) care; and
(b) the benefits and risks of advancedecision-making with regard tolife-sustaining treatments; and
(c) preparing patients and surrogatesfor appropriate in-the-momentmedical decisions at the end of life.
6. Create alternatives to current inadequatemodels of end-of-life decision making.Consider how to promote an EOLculture in your institution that meetsthe relational, emotional, and spiritualneeds of the sick and dying and so
126 The Linacre Quarterly 80 (2) 2013
helps to overcome those conditionsthat give rise to an inordinate felt needto control the precise circumstances ofdeath.
Recommendations for CatholicPhysicians
1. Change your practice. Avoid promotinginappropriate advance decisions regard-ing treatment and care at the end-of-life; become knowledgeable aboutCatholic principles of ordinary vs.extraordinary care; prepare yourpatients for in-the- moment decisions;address medical problems as theyoccur, rather than putting your patientson “tracks” based on choices for futurelife-sustaining treatments.
2. Make your concerns known: If you seeinadequate approaches to end-of-lifecare, or even abuses pertaining toPOLST or other advance decision-making tools, inform the appropriateadministrator(s) at your facilitiesand inform your own patients aboutyour approach to sound clinical andethical decision-making at the end oflife.
3. Get involved:(a) with alternatives that can help to
overcome some of the weaknessesof current, inadequate modelsof EOL decision-making; helpcreate them; use your expertisefor the renewal of EOL care;
(b) with discussions or initiatives inyour state where POLST pro-grams are being proposed orpromoted so you can providea Catholic witness in EOLmatters;
(c) with promoting authentic Catholicsolutions (e.g. Protective MedicalDecision Documents,103 preparingpatients and surrogates for
in-the-moment-of-need decisionmaking, and protecting thedoctor–patient relationshipagainst “facilitated” informedconsent).
4. Speak with your bishops and colleaguesabout the issues: Faithful Catholicdoctors can provide valuable perspec-tives to bishops about the clinical andethical dimensions of appropriate—and inappropriate—end-of-lifedecision-making. Moreover, Catholicdoctors may find that their colleagueshave some misgivings about POLST,but not the ethical vocabulary to articu-late and advance their misgivings.Catholic doctors should be a resource toother physicians and healthcareprofessionals in discussing ethical con-cerns and formulating prudential policiesto serve the best interests of patients.
Conclusion
There are reasons to believe that theprocess of dying, already difficult in ourcontemporary, complex healthcare insti-tutions, may only get harder given theincreasing challenges in our cultureranging from rising healthcare costs toongoing secularization. To respecthuman life and dignity, we must bringmoral commitment, ethical principles,and the highest clinical standards toend-of-life care. We need policies toguide this care and tools to help usimplement it. The POLST paradigmand form are too flawed to contribute tothese goals, even though they werecreated with the stated goal of improvingend-of-life care. We have proposed somealternatives to POLST, and look forwardto working with our colleagues, patients,and fellow citizens to make improvedclinical and ethical care at the end of lifea reality.
Brugger et al. – The POLST paradigm and form: Facts and analysis 127

ENDNOTES
1. Pope Pius XII, in an address to anesthe-siologists in 1957, introduced the term“ordinary means” to refer to forms ofmedical care that one is morally obligedto use (see The Prolongation of Life: AnAddress to an International Congressof Anesthesiologists, 1957); the terms“ordinary” (or “proportionate”) and “extra-ordinary” (or “disproportionate”) wereelaborated in the 1980 document of theCongregation for the Doctrine of theFaith, Declaration on Euthanasia (sec. IV);the terms “ordinary” and “extraordinary”are also used in the United StatesConference of Catholic Bishops, Ethicaland Religious Directives for Catholic HealthCare Facilities (nos. 56 and 57).
2. Although POLST is similar in somerespects to traditional Advance Directives(ADs), POLST advocates specificallystate that POLST forms are not ADs(e.g., Coleman and Mclean 2012, seenote 13, p. 65). This has important legalimplications. Federal and state lawsspecifically direct that ADs cannot berequired as a condition to receive healthcare. Most POLST programs contain nosuch patient protection. Without suchprotection, programs actually removepatient choice and control since aPOLST could be required for admissionor treatment.
3. Other factors include a mindset thattreats patients as a collection of con-ditions that can be addressed withoutreference to the entire patient, and to theuncoupling of the economics of medicinewhere the payer is outside of the doctor–patient interaction.
4. We thank Ione Whitlock for much of theresearch contained in the next 30 footnotes.
5. http://www.polst.org/about-the-national-polst-paradigm/history/.
6. Lee Lewis-Husk and Michael Garland,The First Decade, ed. Susan W. Tolle andGary T. Chiodo (Portland, OR: TheCenter for Ethics in Health Care,Oregon Health Sciences University,1999), p. 10; cf. Tolle and Tilden (2002).
7. Patrick Dunn of Good SamaritanHospital in Portland, OR, and ethicistMichael Garland of OHSU and OregonHealth Decisions, convened the Health
Ethics Network of Oregon (HENO) in themid-1980s. Dunn wrote in 1992 that itwas HENO that identified “a significantproblem … at the interface between acutecare and long-term care: residents’ prefer-ences for emergent treatment.”Paramedics arriving at the long-term carefacility were unable to find “an indicationof the patient’s treatment preference,either orally from the care providers, orfrom the medical record … HENO con-vened [physicians, nurses, long-term careproviders and others] interested in thisissue.” The MTC was devised “after con-siderable effort over a period of two years”(see Dunn 1992).
8. Dunn’s (1992) article includes a copy ofthe MTC as it was in 1992: specified sig-nature of “attending physician”; care level3 stated “provide” (as opposed to “con-sider”) medical treatments; Section Ddirects “oral fluids and nutrition mustalways be offered.”
9. See “Milestones of the Oregon PolstProgram (1990-Present).” In 1996, Dunnet al. were still calling it MTC, but saysthat focus groups had determinedPOLST was a better name.
10. The Center for Ethics in Health Care atOHSU is also the publisher of “TheOregon Death with Dignity Act: AGuidebook for Health Care Professionals”;see http://www.ohsu.edu/xd/education/continuing-education/center-for-ethics/ethics-outreach/upload/Oregon-Death-with-Dignity-Act-Guidebook.pdf. Theinterconnection between POLST and theright-to-die movement is very troubling;one POLST critic, who’s undertaken con-siderable research on the links betweenthe two, has said, “if you scratch POLST,you find right-to-die.”
11. The NPPTF recommends that local taskforces include a “broad representation” ofpersons working in the field of healthcare, including representatives “fromEMS, emergency department physiciansand nurses, the state long-term careassociation, the state medical association,the state surveyors, the agency responsiblefor senior services, the state department ofhealth, the state hospital association, homehealth association, the state bar associationand the state hospice association.”Curiously, however, the national task force
128 The Linacre Quarterly 80 (2) 2013

recommends that “representatives of thedisability community or interestedright-to-life organizations can be consultedas needed and may not need to serve on thetask force” (emphases added). See http://www.ohsu.edu/polst/developing/implementation-steps.htm
12. POLST literature emphasizes the supportof physicians, especially in collaborationwith local medical societies and otherphysician-led groups. The support ofnon-physician health care workers isimportant, but physician support is “keyto the initial institutional culture change… necessary to establish the POLSTparadigm” Sabatino and Karp (2011, 13).
13. Step 6 on the implementation check liststates: “Train social workers, nurses, cha-plains, and others to be advance careplanning facilitators so that they are com-fortable and knowledgeable discussing thePOLST Paradigm form.” See http://www.ohsu.edu/polst/developing/implementation-steps.htm.
14. See “Program Requirements”; available athttp://www.polst.org/develop-a-program/program-requirements/. Endorsed pro-grams must also demonstrate that theirforms meet several requirements. Theseare summarized in a power point at http://www.polst.org/wp-content/uploads/2013/02/hammes+requiredelements-of-a-revised.ppt and include the following: (1) formconstitutes medical orders that must befollowed by health professionals acrossthe continuum of care, (2) form is stan-dardized in format, color and wording;(3) form is primarily used with patientswith advanced, progressive illness or thosewho further wish to define their prefer-ences, (4) form may be used to limittreatment or to express a desire for fulltreatment, (5) form provides clear direc-tion about the desired response if patientis pulseless and apenic, (6) form allowsfor clear directions about other life-sus-taining treatment, (7) from transfers withthe patient, (8) health professionals aretrained to use the form, and (9) measuresare made to monitor the success of theprogram and its implementation.
15. See no. 4 under “Program Requirements”;Level 3 and no. 1 under Level 4; availableat http://www.polst.org/develop-a-program/program-requirements/.
16. Sabatino and Karp identify severalexamples of effective statewide end-of-lifeorganizations: Coalition for CompassionateCare of California (http://www.coalitionccc.org), Idaho End-of-Life Coalition(http://www.idahoendoflifecoalition.org)Community-Wide End of Life/PalliativeCare Initiative of New York (formerlyA Better Way Coalition) (http://www.compassionandsupport.org), TennesseeEnd-of-Life Partnership (http://www.endoflifecaretn.org); see Sabatino and Karp(2011, 13).
17. 15 States: California, Colorado, Hawaii,Idaho, Louisiana, Montana, New York,North Carolina, Oregon, Pensylvania,Tenesee, Washington, West Virginia,Wisconsin, Utah; see http://www.polst.org/programs-in-your-state/
18. 30 States: Alaska, Alabama, Arizona,Connecticut, Delaware, Florida, Georgia,Illinois, Indiana, Iowa, Kentucky, Maine,Massachusetts, Michigan, Minnesota,Missouri/Kansas (metro region),Nebraska, Nevada, New Hampshire, NewJersey, New Mexico, North Dakota,Ohio, South Carolina, Texas, Vermont,Virginia, Washington, DC, Wyoming;see http://www.ohsu.edu/polst/programs/state+programs.htm.
19. Tolle and Tilden (2002, 316): “ThePhysician Orders for Life-SustainingTreatment (POLST) Program was devel-oped and implemented with support fromThe Greenwall Foundation. Studies ofOregon’s progress and continuing barriersto advance planning were supported bythe Meyer Memorial Trust, the Projecton Death in America and NIH NationalInstitute of Nursing Research (R01NR03526). Dissemination of our findingshas been supported in part by TheNathan Cummings Foundation and TheRobert Wood Johnson Foundation.”
20. See http://www.compassionandchoices.org/who-we-are/board-of-advisors/
21. The website for Choice appears to beextinct. To view their website as it was inthe late 1990s, visit http://web.archive.org/web/19961031150257/http://www.choices.org/.
22. See http://www.nathancummings.org/grant-programs/health-program-grants/
23. See MergerWatch Fact Sheet at http://community.compassionandchoices.org/
Brugger et al. – The POLST paradigm and form: Facts and analysis 129

document.doc?id=413, authored by ElenaCohen, who was an attorney for theSociety for the Right to Die in the 1980s,and is now with Compassion & Choices.Funding data are at http://www.nathancummings.net/Health_Grants_2005/CommCat-MergerWatch.pdf and http://www.nathancummings.net/health_grants/HPGLstNov06.pdf. It is not surprising that thePOLST model is actively promoted byCompassion and Choices; see http://www.compassionoforegon.org/services/polst/
24. United States, Department of Treasury,Internal Revenue Service. “Return ofOrganization Exempt from Income Tax(Form 990-PF): Open Society Institute,”990 Finder. Foundation Center, 2012.Web.
25. Grant #37343. Robert Wood JohnsonFoundation., “Annual Report,”(Princeton, NJ 1998, 65). Report is avail-able online at http://www.rwjf.org/en/research-publications/find-rwjf-research/1998/04/annual-report-1998-.html.
26. http://us5.campaign-archive1.com/?u=76217e6abc7f11ac3e5fd7629&id=560bbce60a&e=54cbf2cf98.
27. The first proposal for a legal document ofthe sort was advanced by the EuthanasiaSociety of America in 1967. The Society’slawyer, Luis Kutner, published an essaythat year in which he argued that theright to refuse to be treated by doctorswhen in compos mentis, including withlife-sustaining procedures, implicitly con-tained the right to designate in advancethat consent to certain types of treatmentshould be terminated. Such advancedconsent, or rather revocation of consent,would limit physicians from takingfurther action on behalf of patients’ lives“and the patient would be permitted to dieby virtue of the physician’s inaction”(Kutner 1969, quote on 551). Kutner pro-posed that the document should be called“a living will” (he also proposed the names:“a declaration determining the terminationof life,” “testament permitting death,”“declaration for bodily autonomy,” “declara-tion for ending treatment,” “body trust”).
28. 42 U.S.C. 1395 cc (a).29. “POLST differs from an advance direc-
tive (living will or health care power ofattorney) in that it is an actionablemedical order dealing with the here-and-
now needs of patients—it can build on anadvance directive but can be created forpatients without advance directives.”Charles P. Sabatino and Naomi Karp,Improving Advanced Illness Care: TheEvolution of State POLST Programs(Washington, D.C.: AARP Public PolicyInstitute, 2011), available at http://assets.aarp.org/rgcenter/ppi/cons-prot/POLST-Report-04-11.pdf
30. http://respectingchoices.org/.31. “The La Crosse, Wisconsin program,
operating regionally for several years, hasdeveloped a trained “facilitator” modelthat requires completion of an approvedtraining curriculum by nonphysicianswho then serve as facilitators for allstages of advance care planning, includ-ing POLST.” Sabatino and Karp(2011, 24).
32. In 1991 four health systems inWisconsin, Gundersen Clinic, Ltd.,Lutheran Health System-Lacrosse (nowGunderson Lutheran), Franciscan HealthSystem and Skemp Clinic, collaborated ina program called “Respecting YourChoices,” an aggressive advanced directiveeducation program that included thetraining and sending out of approximately120 local nonphysician educators. Allhealth-care organizations had access tononphysician educators. Over the courseof the program, the prevalence of advancedirective usage increased from 15 to 85%.98% of the patients opted to forgo treat-ment. See review essay by Hammes andRooney (1998).
33. http://www.polst.org/develop-a-program/implementation-steps-and-materials; http://respectingchoices.org/training_certification/what_certification_is_right_for_me.
34. http://lawmrh.wordpress.com/2011/09/09/81-year-old-woman-tattoos-do-not-resuscitate-d-n-r-on-her-chest-just-to-make-sure/
35. The POLST movement has beendescribed as the “next stage” in achievingthe intent of limiting undesired end-of-life medical care through advance decision-making; Meier and Beresford (2009); seealso Tuohey and Hodges (2011).
36. Susan Tolle, Director of the OHSUCenter for Ethics; her quote may befound at: http://blog.gormanhealthgroup.com/2012/03/14/oregon-leads-the-way-on-end-of-life-planning/
130 The Linacre Quarterly 80 (2) 2013

37. http://www.gundluth.org/?id=3016&sid=138. http://blog.gormanhealthgroup.com/2012/
03/14/oregon-leads-the-way-on-end-of-life-planning/
39. E. Christian Brugger develops this criti-cism in 2011 especially 158–161.
40. John Paul II, “Life-SustainingTreatments and the Vegetative State:Scientific Advances and EthicalDilemmas” (2004) (On the “VegetativeState”); available at http://www.vatican.va/holy_father/john_paul_ii/speeches/2004/march/documents/hf_jp-ii_spe_20040320_congress-fiamc_en.html. This teaching wasreaffirmed in 2007 by the Congregationfor the Doctrine of the Faith (see Responsesto Certain Questions of the United StatesConference of Catholic Bishops ConcerningArtificial Nutrition and Hydration, August1, 2007 and incorporated by the UnitedStates Catholic Conference of Bishops intothe Ethical and Religious Directives forCatholic Health Care Services (ERDs) in2009 (n. 58); for CDF document see http://212.77.1.247/roman_curia/congregations/cfaith/documents/rc_con_cfaith_doc_20070801_risposte-usa_en.html
41. This specific scenario was reportedrecently by a man whose father waschoking on a piece of chicken. The nursecalled frantically to determine whether tointervene: she was uncertain whether hisstatus was “Do Not Resuscitate.” He was“Full resuscitation.” Fortunately shereached the son in time to successfullyintervene. (personal contact, FLS).
42. Fagerlin and Schneider (2004, 30–42)observe that: “In pursuit of the dreamthat patients’ exercise of autonomy couldextend beyond their span of competence,living wills have passed from controversyto conventional wisdom, to widely pro-moted policy. But the policy has notproduced results… Even patients makingcontemporary decisions about contempor-ary illnesses are regularly daunted by thedecisions’ difficulty… How much harder,then, is it to conjure up preferences for anunspecifiable future confronted with uni-dentifiable maladies with unpredictabletreatments?”
43. See the insightful critique of this modelby Perkins (2007).
44. Flygt (2012, 47) misrepresents Bruggeret al. by suggesting that they argue that
“non-signature invalidates a POLSTDNR order.” The authors never statedthis nor was it their point. They ques-tioned whether designating a patient’ssignature on POLST forms as merelyoptional eliminates an important guaran-tee of fully informed consent (see Bruggeret al. (2012, 2)). Flygt goes on to saysomething revealing. If non-signatureinvalidates a POLST DNR, he says, then“why doesn’t non-signature invalidate ahospital DNR order, which is generally notformally consented?” [emphasis added]. Ishe conceding by use of this analogy thatthe orders on POLST forms need not be“formally consented” to by patients inorder to be fully valid?
45. Crafting POLST form language in thisway is required policy cited by theNational POLST Paradigm ProgramRequirements: “…Language in theforms should start with positivelanguage. For example, the comfortmeasures description might read ‘Treatwith dignity and respect. Keep clean,warm, and dry. Use medication by anyroute…’ In the comfort measuressection, the forms should avoid wordingthat starts with negative language andsuggests that care and comfort of thepatient are not paramount, for example,‘Do not intubate or transport….’ ” Seehttp://www.polst.org/develop-a-program/program-requirements/ under “FormRequirements for Endorsed Programs,”No. 12.
46. The North Carolina MOST uses themore neutral term “medically adminis-tered fluids and nutrition.”
47. Concerns about physician controlleddecision-making and loss of trust have ledto a greater demand for patient infor-mation about illnesses and for patients toshare in more decisions. This has evolvedfrom most decisions being physician-directed to include various levels ofpatient preferences. The far end of thiscontinuum is an expression of radicalautonomy in which the patient may insistupon certain tests or procedures evenwhen not medically necessary or refusecare altogether. Other steps have beendefined in a shared decision-making con-tinuum that gives more options for allinvolved (see Kon 2010).
Brugger et al. – The POLST paradigm and form: Facts and analysis 131
48. AMA Code of Ethics, Opinion 8.08(http://www.ama-assn.org/ama/pub/physician-resources/medical-ethics/code-medical-ethics/opinion808.page).
49. Emphasis added; available at http://www.ama-assn.org/ama/pub/physician-resources/legal-topics/patient-physician-relationship-topics/informed-consent.page
50. http://respectingchoices.org/training_certification/on-site_courses/last_steps_acp_%28physician_orders_for_life_sustaining_treatment_%28polst%29_paradigm%29
51. Facilitators increase utilization of advancedirectives in a given community. This wasfirst demonstrated in 1991 in Wisconsin,where advance directive completionincreased from 15 to 85% (Hammes andRooney 1998); the effect was confirmedin a randomized control trial inMelbourne, Australia in 2010, where 84%of patients who, receiving advance careplanning by “trained non-medical facilita-tors” (based upon the Respecting PatientChoices model, La Crosse, Wisconsin),completed advance directives, comparedwith 30% in the non-facilitator controlgroup (see Detering et al. 2010).
52. Wisconsin POLST, West Virginia POST,Tennessee POST, Washington POLST,Pennsylvania POLST, Minnesota POLST,Louisiana LaPOST, Hawaii POLST,California POLST, Colorado MOST.
53. Respecting Choices (2007), chapter 4.12.For example, a suggested training scriptinvolving decisions on feeding tubesstates: “To assist you in making thisdecision, I’d like to give you someexamples of the side effects that can occurbecause of receiving artificial nutritionand hydration. First, the artificial nutri-tion that is delivered through tubes oftenmoves out the stomach and slips into thelungs, causing pneumonia. This is calledaspiration. The artificial hydration that isdelivered may also increase the amount offluid the body has to absorb, causingextra fluid in the lungs, making it moredifficult to breathe. The extra fluid alsocauses congestion in other parts of thebody, causing pain and discomfort as wellas the need to urinate more frequently.”
54. Respecting Choices, “Tube Feeding:What You Should Know,” fact sheet,2011; one section reads, “You may havefears about not getting food or water.
You may think you will starve or beuncomfortable. This is not true. Whenfood and water are not given, you will diefrom your chronic illness. You will notfeel hungry, and you will receive goodcare to make you comfortable”.This script has been prepared, ofcourse, without actually knowing whatdiagnosis or illnesses the patient actuallyhas, if any.
55. “Transforming Healthcare: Advance CarePlanning”, Gunderson Lutheran HealthSystem. Available at: http://www.gundluth.org/upload/docs/TransformACP.pdf
56. “Death Drugs Cause Uproar in Oregon”,ABC News, August 6, 2008. Available athttp://abcnews.go.com/Health/story?id=5517492&page=1#.UHpgVI7Gbpg.
57. Response to What is POLST? at http://www.polst.org
58. See summaries of research studies at http://www.polst.org/?s=research and http://www.polst.org/wp-content/uploads/2013/02/POLST-Literature-Review.docx
59. In addition, they refused resuscitation98% of the time, hospitalization and anymedical interventions 62% of the time,intensive care (ICU) 92% of the time,potentially curative antibiotics 57% of thetime and feeding tubes 64% of the time(only 2% opted for long-term use offeeding tubes); see Hammes et al. (2012),see p. 83 and table 3, p. 80; cf. Hammeset al. (2010).
60. Susan Hickman, Ph.D, “POLSTResearch and Evaluation” power point,slide three citing Meyers et al. (2004),available at http://www.slidefinder.net/p/polst_research_evaluation_susan_hickman/hickman-nhpco-research-slides-rev/28067343; and a description of the Meyers et al.study at at http://www.polst.org/wp-content/uploads/2013/02/Summary-Q-Washington-POLST-Nursing-Facility-Project.docx; the study itself was nolonger listed on the updated web site’slist of research studies in 2013 athttp://www.polst.org/?s=research.
61. Although a 10% chance of recovery com-pared to certain death may seem low, inMartin v. Richards, 531 N.W.2d 70, 75,192 Wis.2d 156, 167–68 (Wis. 1994), theWisconsin Supreme Court held a phys-ician liable for failing to disclose tests thatcould have been run to check for a 1–3%
132 The Linacre Quarterly 80 (2) 2013
possibility of a brain bleed (a complicationwith serious consequences), after thepatient later suffered a disabling stroke.
62. Fagerlin and Schneider, 2004. Fagerlinand Schneider, “Response to letter to theeditor, A Viable Alternative to TraditionalLiving Wills from Hickman, SE et al.,”Hastings Center Report (Sept–Oct 2004),page 6. In 2005, the President’s Council onBioethics questioned whether living-willtype of documents really ensure thatpatient preferences are honored: “Datafrom the Robert Wood JohnsonSUPPORT study suggests that manypatients filling out living wills are con-fused about what they are being asked todecide, and vague or misinformed aboutthe purpose and effectiveness of themedical interventions they are beingasked to choose among.” The Councilargued that when people are healthy theymay “incautiously” opt for death over dis-ability. But when sickness comes and theyare forced to face death, they oftenchange their minds: “There is in fact anextensive body of research showing howpoor we are at predicting our own prefer-ences and desires, especially in regard tochoices far off in the future. This inabilityis likely to be acutely present here, sincewe have no experience deciding how andwhen to die” (President's Council onBioethics (2005). Taking care: ethical care-giving in our aging society, page 74. http://bioethics.georgetown.edu/pcbe/reports/taking_care/index.html.
63. Nelson and Tuohey 2011. From Q&Afollowing presentation: Q: “If the patientcompletes a POA for health care and alsocompletes a POLST, does the POA havethe authority to override the POLST?” A:(Fr. John Tuohey) “Here, if the POLSTis completed by a physician with thepatient, that document supersedes allothers. We would not listen to a POAregarding a POLST… As a practicalmatter, we advise that when a POLST iscompleted with the patient, the physicianrecommends to the patient that theyinform the POA that they are likely offthe hook now for any decision-making –they quite likely won’t be needed.”
64. 42 C.F.R. §418.3 defining “terminalillness” for purposes of eligibility forMedicare’s hospice benefit.
65. POLST-Developing a Program, at http://www.polst.org/develop-a-program/program-requirements/ for Level 3 Endorsed pro-grams and at #1 for Level 4 MatureEndorsed programs.
66. Fox Valley Coalition for End of Life, BasicNeeds Giving Partnership Grant ApplicationSeptember 29, 2011 at pages 9–10; and adraft of the same dated September 1, 2012at page 2; Briggs (2003). http://www.edc.org/lastacts.
67. Guidance for Oregon’s Health CareProfessionals (August 2011) at http://www.nursepractitionersoforegon.org/associations/11517/files/NPO_POLST-Guidebook2011V2FINALPOLST.pdf.
68. California Advocates for Nursing HomeReform (CANHR), Physicians Orders forLife Sustaining Treatment (“POLST”)Problems and Recommendations (2010) atpage 5, available at http://www.canhr.org/reports/2010/POLST_WhitePaper.pdf.
69. Fox Valley Coalition for End of Life, BasicNeeds Giving Partnership Grant ApplicationSeptember 29, 2011, at 9–10.
70. Respecting Choices Advance CarePlanning Facilitator Course Manual,Chapter 5.
71. The National Nursing Home Survey:2004 Current Resident Tables: Table 12at http://www.cdc.gov/nchs/nnhs/resident_tables_estimates.htm#Demographics
72. Frequently Asked Questions about thePhysician Orders for Scope of Treatment,FAQ #2 at http://www.wvendoflife.org/MediaLibraries/WVCEOLC/Media/professional/faq_post.pdf.
73. MOLST is the name for POLST inDelaware and New York. The expansionfor people with mental disabilities and forchildren is contained in FAQ at http://delawaremolst.org/?page_id=30
74. Web site of Children’s Hospice &Palliative Care Coalition (CHPCC):Events page available at http://www.chpcc.org/calendar/polst-beginning-the-coversation-for-pediatrics
75. Web site of CHCPP: About Us: Who WeRepresent at http://www.chpcc.org/about-us/
76. http://www.ohsu.edu/polst/77. “The term MOLST is generally applied to
an end-of-life document, which is intendedto be portable and can be relied upon byany health care provider.” Letter datedNovember 14, 2012, from Division of
Brugger et al. – The POLST paradigm and form: Facts and analysis 133

Public Health Director to Health CareProviders, available at http://web.archive.org/web/20130115163536/http://www.patientsrightscouncil.org/site/wp-content/uploads/2012/12/Delaware_MOLST_11_12.pdf.
78. Md. Code Ann. [Health-Gen] §5-608.79. NJ Legis 145 (2011) effective 7/1/12;
future §§26:2H – 129 – 26:2H – 140.80. OAR 847-035-0030 (6) regarding EMTs
and OAR 847-010-0110 pertaining tophysicians or physician assistants.
81. MD pending regulation Title 10 DHMH10.10.21.04. Facilities include assistedliving programs, home health agencies,hospices, kidney dialysis centers, andnursing homes. Note that although aMOLST form is required for each patient,the patient need only be offered the oppor-tunity to participate in the process and nopatient or surrogate signature is required.
82. Md. Code Ann. [Health-Gen] §5-608.1(c) (3).
83. Md. Code Ann. [Health-Gen] §5-608.1 (d).84. The law notes that a facility must
comply except as provided in §5-611 (e)or §5-613 (a). Those provisions statethat the health care provider need notcomply if aware that patient disagreeswith the action [§5-611 (e)] and thatthe provider who intends not to complyshall inform, assist in transfer andcomply pending transfer if non-compliance would likely result in death[§5-613 (a)]. Note that this does notaddress a situation in which compliancewould likely result in death.
85. OAR 847-010-0110.86. OAR 847-010-0110.87. OAR 847-010-0110, referring to ORS
§127.625 (a) (c) and ORS §127.654 (1).88. NJ Legis 145 (3f) (2011) effective 7/1/12;
future §26:2H – 131.89. NJ Legis 145 (0e) (2011) effective 7/1/
12; future §26:2H – 137.90. NJ Legis. 145 (9e (1)) (2011), effective 7/
1/12; future §26:2H – 137.91. “Federal law” would refer to the Patient
Self-Determination Act of 1991, requir-ing that health care institutions informpatients of their right to accept or rejectmedical care offered to them and providethem with an opportunity to create anadvance directive reflecting those wishes.It also requires institutions to state theirpolicies regarding advance directives.
92. An example of this “everything” or“nothing” approach is seen in the PBSTelevision Religion and Ethics Newsweeklyentitled “Advance Directives” (Oct 21,2011) featuring staff and patient fromGunderson Lutheran Hospital, LaCrosse, WI. http://www.pbs.org/wnet/religionandethics/episodes/october-21-2011/advance-directives/9748/.
93. Naomi Karp and Erica Wood,“Incapacitated and Alone: HealthcareDecision Making for Unbefriended OlderPeople ABA,” Human Rights 31, no. 2(2004), 20-24, available at http://www.americanbar.org/publications/human_rights_magazine_home/human_rights_vol31_2004/spring2004/hr_spring04_incapacitated.html.
94. Douglas Silverman, “Serving theUnbefriended Elder Population: Trends,Challenges, and Successes,” Power PointPresentation, 2011 Minnesota Age &Disabilities Odyssey, Mayo Civic Center,Rochester, MN June 21, 2011 accessed athttp://www.mnodyssey.org/2011/PowerPoint/Monday/McDonnell-B/9-30am/SilvermanOdysseyFinal.pptx at slide31. In a large study of ICU admissions atseven hospitals, attending physicianswould have considered withdrawing life-sustaining treatment for 37 unbefriendedpatients if a surrogate had been available.These 37 patients accounted for 1.2% ofadmissions during the six-monthperiod studied; twenty-five died in theICU—fifteen after life support was with-drawn, ten died while life supportcontinued. D.B. White, et al., “LifeSupport for Patients without a SurrogateDecision Maker: Who Decides?” Annalsof Internal Medicine 147 (2007): 34-40.
95. This report is available at http://www.ltcombudsman.org/sites/default/files/ombudsmen-support/training/Informational-Brief-on-Unbefriended-Elders_0.pdf
96. Three approaches are offered for con-sideration by those seeking to address thehealth care decision-making needs ofpeople thought to be unbefriended. Twoprograms address finding people beforethey become unbefriended in a medicalsetting and one links them to volunteeradvocates afterwards.(1) Next of Kin Registry. The next of kinregistry (http://www.nokr.org) provides a
134 The Linacre Quarterly 80 (2) 2013

free tool for securing next of kin infor-mation in emergency situations. Theregistry trains volunteers who visit withpeople and record their information whichis then only shared with law enforcement,emergency responders and medical person-nel. They have a faith-based sub-program,described at http://www.nokr.org/nok/restricted/faith.htm which appears torequire a local government partner. It maybe possible to link a program like this withone that would take the next step ofhelping people complete health care direc-tives and appoint an agent.(2) Minneapolis Volunteers of AmericaUnbefriended Pilot Program. This pilotproject was supported in part by grantsfrom the Minnesota Department of HealthServices (DHS) and a local foundation (Id.at 7-8). A 2011 presentation by the DHSgrantor reported this project developed pro-tocols to identify, locate and support familyor decision-makers and served nearly 100individuals in the metro area. Of thoseserved, 63% completed a health care direc-tive, 80% of which named an agent and78% had a follow-up conversation with adoctor; (see Douglas Silverman, “Servingthe Unbefriended Elder Population:Trends, Challenges, and Successes,” PowerPoint Presentation 2011 Minnesota Age &Disabilities Odyssey, Mayo Civic Center,Rochester, MN June 21, 2011, accessed athttp://www.mnodyssey.org/2011/PowerPoint/Monday/McDonnell-B/9-30am/SilvermanOdysseyFinal.pptx).(3) Indiana Volunteer Advocates forSeniors Program This program wasfounded by a Catholic healthcare system toprovide volunteer advocates for unbe-friended inpatients in hospitals, nursinghomes and hospices. A volunteer advocateserves a patient for up to 90 days so as toavoid the need for a court appointed guar-dian. Volunteers carry out all the duties of atypical guardian except for finances, includ-ing ethical health care decisions and locatingappropriate residential facilities for dischargeplanning. They are court-appointed aslimited guardians and complete monthlyreports to the court. This comprehensiveapproach requires volunteers to complete 40hours of initial training and another 12hours per year of continuing training.Limiting volunteers to health care decision-
making and ethics, including communi-cation within health care systems couldlimit training to a day or less. This programis partially funded by grants. (Informationabout the Volunteer Advocates for Seniorsprogram is available at http://www.franciscanalliance.org/hospitals/hammond/services/seniors/vas/Pages/default.aspx)
97. http://www.befrienderministry.org98. http://www.stephenministries.org99. This will also protect nursing and other staff
from being forced to conform to POLSTorders that violate their consciences.
100. United States Conference of CatholicBishops, Ethical and Religious Directives forCatholic Health Care Facilities (no. 24), 2009.
101. The PSDA requires most health careinstitutions (but not individual doctors) toprovide patients at the time of admissiona written summary of their health-caredecision-making rights and the facility’spolicies with respect to recognizingadvance directives; they must if patientshave an AD, and document the fact intheir medical record if they do; and theymay never discriminate against patientsbased on whether or not they have anadvance directive. It is against the law forthem to require either that you have or nothave an advance directive (see http://www.americanbar.org/groups/public_education/resources/law_issues_for_consumers/patient_self_determination_act.html).
102. See Stewards of the Gift of Life: APastoral Statement on Physician Orders forLife-Sustaining Treatment (POLST) fromthe Catholic Bishops of Minnesota, avail-able at http://www.mncc.org/stewards-of-the-gift-of-life/
103. Oregon, for example, requires the follow-ing: “A physician or physician assistantlicensed pursuant to ORS Chapter 677shall respect the patient’s wishes includinglife-sustaining treatments. Consistent withthe requirements of ORS Chapter 127, aphysician or physician assistant shallrespect and honor life-sustaining treatmentorders executed by a physician, physicianassistant or nurse practitioner. The factthat a physician, physician assistant ornurse practitioner who executed a life-sustaining treatment order does not haveadmitting privileges at a hospital or healthcare facility where the patient is beingtreated does not remove the obligation
Brugger et al. – The POLST paradigm and form: Facts and analysis 135

under this section to honor the order”(Oregon Administrative Rule 847-010-0110: Physicians and Physician Assistantsto Honor Life-Sustaining Treatment Orders).
104. One such document is available from thePatients Rights Council: http://www.patientsrightscouncil.org
105. See http://www.patientsrightscouncil.org/site/advance-directive-protective-medical-decisions-document/.
REFERENCES
Briggs, L. 2003. Shifting the focus of advancecare planning: using an in-depth interviewto build and strengthen relationships.Innovations in End-of-Life Care 5: http://www.edc.org/lastacts
Brugger, E. C. 2011. A Critique of theNational POLST Paradigm through ananalysis of Colorado’s new MOSTLegislation. The Linacre Quarterly 78:157–71, esp. 158–61.
Brugger, E. C. et al. 2012. POLST andCatholic Health Care. Ethics & Medics37:2.
CANHR Policy Brief. 2010. Physician Ordersfor Life Sustaining Treatment (“POLST”)– Problems and Recommendations. ASpecial Report by California Advocates forNursing Home Reform, San Francisco,CA, http://www.canhr.org/reports/2010/POLST_WhitePaper.pdf
Coleman, G. D., and M. R. Mclean 2012.POLST supports care in context ofERDs. Health Progress: Journal of theCatholic Health Association of the UnitedStates 58–65.
Cosgriff, J. A., T. R. Fried et al. 2007. Theassociation between treatment preferencesand trajectories of care at the end of life.J Gen Intern Med 22:1566–71.
Detering, K. M. et al. 2010. The impact ofadvance care planning on end of lifecare in elderly patients: randomized con-trolled trial. British Medical Journal 340:1345–53.
Dominique, K. 2009. MOLST DemonstrationProject: Care Transitions Seminar.Partners HealthCare.
Dunn, P. M. 1992. The health ethics networkof oregon: a model to enhance healthcare
ethics committee collaboration. HECForum 4:135–48.
Dunn, P. M., T. A. Schmidt, M. M. Carley,M. Donius, M. A. Weinstein, and V.T. Dull. 1996. Journal of the AmericanGeriatrics Society 44:785–91
Fagerlin, A., and C. E. Schneider. 2004.Enough – the failure of the living will.Hastings Center Report 34:30–42.
Flygt, T. R. 2012. Reflections on the use ofthe POLST paradigm. Health Care EthicsUSA: A Resource for the Catholic HealthCare Ministry 20:47.
Fried, T. R. et al. 2002. Understanding thetreatment preferences of seriously illpatients. New England Journal of Medicine346:1061–66.
Geisz, M. B. Researchers Study End-of-LifeCare in Oregon, Issue Report Card, EngageHealth Care Professionals to Improve Care.Robert Wood Johnson Foundation.
Griggons, C. 2010. Patients without oroxies:what’s happening in other states? Mid-Atlantic Ethics Committee Newsletter 7–9.
Hamel, R. 2012. POLST under fire. HealthCare Ethics USA 20:30–5, quote on 34.
Hammes, B. J., and B. L. Rooney. 1998.Death and end-of-life planning in onemidwestern community. Archives ofInternal Medicine 158:383–90.
Hammes, B. J. et al. 2010. A comparative ret-rospective, observational study of theprevalence, availability, and specificity ofadvance care plans in a county thatimplemented an advance care planningmicrosystem. Journal of the AmericanGeriatrics Society 58:1249–55.
Hammes, B. J. et al. 2012. The POLSTprogram: a retrospective review of the demo-graphics of use and outcomes in onecommunity where advance directives areprevalent. Journal of Palliative Medicine15:77–85.
Hardwig, J. 2009. Going to meet death: theart of dying in the early part of thetwenty-first century. Hastings CenterReport 39:37–45.
Hickman, S. E., S. W. Tolle, V. P. Tilden, andA. G. Rosenfeld. 1999. The Oregon ReportCard: Improving Care of the Dying.Portland, OR: The Center for Ethics inHealth Care, Oregon Health & ScienceUniversity.
Hickman, S. E. et al. 2005. Hope for thefuture: achieving the original intent of
136 The Linacre Quarterly 80 (2) 2013
advance directives. Hastings Center ReportSpecial Report 35:S26–30.
Hickman, S. E. et al. 2010. A Comparison ofmethods to communicate treatment pre-ferences in nursing facilities: traditionalpractices versus the physician orders forlife-sustaining treatment program. Journalof the American Geriatrics Society 58:1241–8.
Hill, T. P., D. A. Shirley and Choice in Dying(Organization: U.S.). 1992. A Good Death:Taking More Control at the End of YourLife. Reading, Mass.: Addison-WesleyPub. Co.
John Paul II, Pope. 2004. Life-SustainingTreatments and the Vegetative State:Scientific Advances and Ethical Dilemmas(On the “Vegetative State”), http://www.vatican.va/holy_father/john_paul_ii/speeches/2004/march/documents/hf_jp-ii_spe_20040320_congress-fiamc_en.html
Jones, A. L., L. L. Dwyer, A. R. Bercovitz,and G. W. Strahan. 2009. The nationalnursing home survey: 2004 overview.National center for health statistics. VitalHealth Stat 13:4, Available at http://www.cdc.gov/nchs/data/series/sr_13/sr13_167.pdf
Karp, N., and E. Wood. 2004. Incapacitatedand Alone: Healthcare Decision Makingfor Unbefriended Older People ABA.Human Rights 31:20–24, available at http://www.americanbar.org/publications/human_rights_magazine_home/human_rights_vol31_2004/spring2004/hr_spring04_incapacitated.html
Keating, R. F., A. H. Moss, M. Sorkin, J.J. Paris et al. 1994. Stopping dialysis of anincompetent patient over the family’sobjection: is it ever ethical and legal?J. Am. Soc. Nephrol. 4:1879–83.
Kon, A. A. 2010. The shared decision-makingcontinuum. Journal of the American MedicalAssociation 304:903–4.
Kurent, J. E. 2000. Death and dying inAmerica: the need to improve end-of-life care. Carolina Healthcare Business16–9.
Kutner, L. 1969. Due process of Euthanasia:the living will, a proposal. Indiana LawJournal 44, 539–54.
Landro, L. 2011. New efforts to simplifyend-of-life care wishes. Wall Street Journal,Mar. 15, 2011.
Lewis-Husk, L., and M. J. Garland. 1999.Pink ‘Polst’ works in Oregon: use spread-ing across U.S. In The First Decade, ed.
Susan W. Tolle, and Gary T. Chiodo,p. 10. Portland, OR: The Center forEthics in Health Care, Oregon HealthSciences University.
Lynn, J. et al. 2008. Improving Care for theEnd of Life, A Sourcebook for Health CareManagers and Clinicians, 2nd edn. OxfordUniversity Press; p. 7.
Meier, D., and L. Beresford. 2009. POLSTOffers Next Stage in Honoring PatientPreferences. Journal of Palliative Medicine12:291–5.
Meyers, J. L. et al. 2004. Use of the PhysicianOrders for Life-Sustaining Treatment(POLST) form to honor the wishes ofNursing Home Residents for End ofLife Care: Preliminary Results of aWashington State Pilot Project. Journalof Gerontological Nursing, 30:37–46.
Moss, A. H. 2000. A New ClinicalPractice Guideline on Initiation andWithdrawal of Dialysis That MakesExplicit the Role of Palliative Medicine.J Palliat Med 3:253–60.
Moss, A. H. et al. 2010. Prognostic signifi-cance of the ‘‘Surprise’’ question in cancerpatients. Journal of Palliative Medicine13:837–40.
Nelson, S. E., and J. F. Tuohey. 2011.POLST: A Dangerous Development or aUseful Tool?. Catholic Health AssociationWebinar June 28, 2011.
Otten, A. L. 1999. The Greenwall Foundation:A Story of a Work in Progress. New York,NY: The Greenwall Foundation.
Parker, S. G. 2004. Community–StatePartnerships. In Program Results (http://www.rwjf.org/en/research-publications/find-rwjf-research/2004/10/community-state-partnerships-to-improve-end-of-life-care.html: Robert Wood Johnson Foundation).
Perkins, H. S. 2007. Controlling death: Thefalse promise of advance directives. Annalsof Internal Medicine 147:51–7.
President’s Council on Bioethics. 2005.Taking care: ethical caregiving inour aging society. https://bioethics.georgetown.edu/pcbe/reports/taking_care/index.html
Project on Death in America. 1998. Project onDeath in America: Report of Activities (July1994–December 1997). New York, NY:Open Society Institute.
Project on Death in America. 2009. Project onDeath in America Grantees, 1994–2003.
Brugger et al. – The POLST paradigm and form: Facts and analysis 137
http://www.opensocietyfoundations.org/sites/default/files/pdia_20040101.pdf
Reinhardt, U. E. 2009. How do hospitals getpaid? A primer. New York Times, January23, 2009. Available at http://economix.blogs.nytimes.com/2009/01/23/how-do-hospitals-get-paid-a-primer/
Respecting Choices. 2007. Advance CarePlanning: Facilitating the Process. InAdvance Care Planning: Facilitator’s Manual,3rd ed. La Crosse, WI: GundersenLutheran Medical Foundation.
Sabatino, C. P. 2010. The evolution of healthcare advance planning law and policy.Milbank Quarterly 88:211–39.
Sabatino, C. P., and N. Karp. 2011 ImprovingAdvanced Illness Care: The Evolutionof State POLST Programs. Washington,D.C.: AARP Public Policy Institute;v:1–64.
Saunders, W. L. 2011. POLST: EthicalConsiderations for Catholic Health CareProviders and Patients, p. 4; delivered atInternational Association of CatholicBioethicists conference, July 2011, atPhiladelphia, PA; theme PalliativeSedation: Moral Distinctions and PracticalConsiderations, available at http://www.iacbweb.org/Readings/Saunders2011.pdf
Silverman, D. 2011. Serving the UnbefriendedElder Population: Trends, Challenges, andSuccesses. Power Point Presentation,Minnesota Age & Disabilities Odyssey,Mayo Civic Center, Rochester, MN, June21, 2011, accessed at http://www.mnodyssey.org/2011/PowerPoint/Monday/McDonnell-B/9-30am/SilvermanOdysseyFinal.pptx at slide 31.
Smith, W. 1997. Forced Exit: The SlipperySlope from Assisted Suicide to LegalizedMurder. New York: Times Books.
Sudore, R. L., and T. R. Fried. 2010.Redefining the ‘Planning’ in advance care
planning: preparing for end-of-lifedecision making. Annals of InternalMedicine 153:256–61.
Sudore, R. L. et al. 2010. Uncertainty aboutadvance care planning treatment prefer-ences among diverse older adults. Journalof Health Communication: InternationalPerspectives 15(S2):159–71.
Tolle, S. W., and V. P. Tilden 2002.Changing end-of-life planning: the oregonexperience. Journal of Palliative Medicine5:311–7.
Tuohey, J. F. 2010. POLST orders are notdangerous but effective devices forend-of-life care. Ethics & Medics 35:3–4.
Tuohey, J., and M. O. Hodges. 2011. POLSTreflects patient wishes, clinical reality.Health Progress: Journal of the CatholicHealth Association of the United States60–4.
White, D. B. et al. 2007. Life Support forPatients without a Surrogate DecisionMaker: Who Decides? Annals of InternalMedicine 147:34–40.
BIOGRAPHICAL NOTE
E. Christian Brugger, Ph.D., is theJ. Francis Cardinal Stafford Professor ofMoral Theology at St. John VianneyTheological Seminary in Denver, CO, anda Senior Fellow of Ethics, and Director ofthe Fellows Program, at the Culture ofLife Foundation, Washington, D.C. In2000, he received his D. Phil. in MoralTheology from Oxford University, St.Hugh’s College. His email address is:[email protected]
138 The Linacre Quarterly 80 (2) 2013