when to care – when to refer acute eye problems in …library.nhsggc.org.uk/mediaassets/chp...
TRANSCRIPT
When to Care When to Care –– When to ReferWhen to Refer
Acute Eye Problems in the Acute Eye Problems in the CommunityCommunity
Frank MunroFrank Munro

TodayToday’’s Talks Talk
nn Acute Eye ProblemsAcute Eye Problems
nn Burden of Disease Burden of Disease –– Making a DifferenceMaking a Difference
nn Shifting the Balance of Care?Shifting the Balance of Care?
nn What do I do now What do I do now –– Could I do more?Could I do more?
nn Clinical Decisions MakingClinical Decisions Making-- When to Care When to Care –– When to ReferWhen to Refer

Clinical decision MakingClinical decision Making
nn DiagnosisDiagnosis
nn ManagementManagement
nn Demonstrate CompetenceDemonstrate Competence
nn Working within scope of practiceWorking within scope of practice
nn DO NO HARM!DO NO HARM!

BirthBirth
DeathDeath
The Challenge!The Challenge!

Scope of PracticeScope of Practice
Where am I?Where am I?Ant / Post BlepharitisAnt / Post Blepharitis
Bacterial Bacterial conjunctivitisconjunctivitis
Microbial KeratitisMicrobial Keratitis
Retinal Retinal DetachmentDetachment
Anterior Anterior UveitisUveitis
Dry EyeDry Eye
CataractCataract
RetinoschissisRetinoschissis
‘‘WetWet’’ ARMDARMD
Dry ARMDDry ARMD
GlaucomaGlaucoma
Allergic/Toxic ConjunctivitisAllergic/Toxic Conjunctivitis
Ischaemic Optic Ischaemic Optic NeuropathyNeuropathy
Corneal FBCorneal FB
Marginal Marginal KeratitisKeratitis
EpiscleritisEpiscleritis
ScleritisScleritis
EndophthalmitisEndophthalmitis
Conjunctival HgeConjunctival Hge
Corneal AbrasionCorneal Abrasion
InclusionInclusion
Chemical BurnsChemical BurnsNeoplasiaNeoplasia
CellulitisCellulitis
ENTRYENTRY HESHESADVANCEDADVANCED
Viral Viral CorneaCornea
PVDPVD
Ping / PterygiumPing / Pterygium
Trichiasis /EpilationTrichiasis /Epilation
Keratitis/ KeratopathyKeratitis/ Keratopathy
ChalaziaChalazia
KerataconusKerataconus
UV BurnUV Burn Penetrating Penetrating InjuryInjury
UveitisUveitisint/postint/post
CornealCornealDystrophyDystrophy
Corneal ErosionCorneal Erosion
Sub tarsal fbSub tarsal fb Viral ConjunctivitisViral Conjunctivitis
EXPERTEXPERT

GIES Patient CategoriesGIES Patient Categories
CategoryCategory NoNo %% CategoryCategory NoNo %% CategoryCategory NoNo %%
NADNAD 112112 9.69.6 BlepharitisBlepharitis 3939 3.43.4 OcularOcular 1616 1.41.4
Dry EyeDry Eye 111111 9.69.6 GlaucomaGlaucoma 3737 3.23.2Anterior Anterior uveitisuveitis 1515 1.31.3
ConjunctivitisConjunctivitis 9090 7.87.8 RetinalRetinal 3535 3.03.0 FloatersFloaters 1414 1.21.2
DiabetesDiabetes 7272 6.26.2 Tear duct etcTear duct etc 3131 2.72.7 CystCyst 1212 1.01.0
CataractCataract 6868 5.95.9 EpiscleritisEpiscleritis 2929 2.52.5 EyelashesEyelashes 99 0.80.8
VitreoVitreo--retret 5252 4.54.5 KeratitisKeratitis 2222 1.91.9 OthersOthers 225225 19.419.4
Corneal/UlcerCorneal/Ulcer 4848 4.14.1 Visual disturbanceVisual disturbance 2020 1.71.7
PVDPVD 4444 3.83.8 MacularMacular 1717 1.51.5
Headache/migraineHeadache/migraine 4343 3.73.7 OcularOcular 1616 1.41.4 TotalTotal 11611161 100100
1
2
17
1
15
1
3
12
2
6
13
6
38
45
1109152
221185
1
181
1
9
6
152
9
1
1
216
4
4
1
220
1
156
110 21 6 5 11 5
11
2 21
462
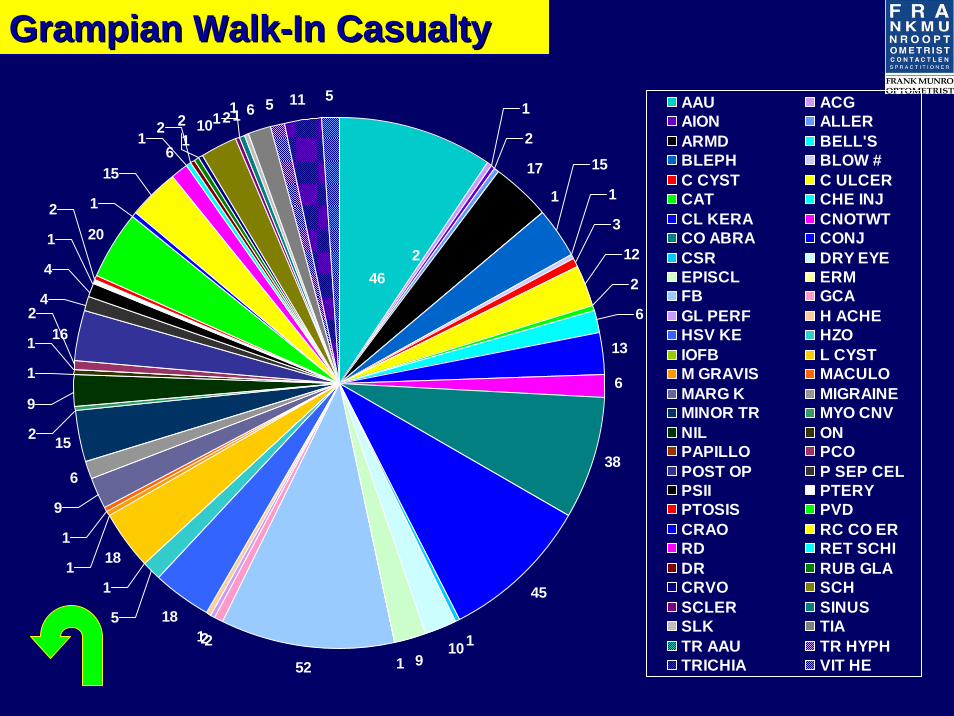
AAU ACGAION ALLERARMD BELL'SBLEPH BLOW #C CYST C ULCERCAT CHE INJCL KERA CNOTWTCO ABRA CONJCSR DRY EYEEPISCL ERMFB GCAGL PERF H ACHEHSV KE HZOIOFB L CYSTM GRAVIS MACULOMARG K MIGRAINEMINOR TR MYO CNVNIL ONPAPILLO PCOPOST OP P SEP CELPSII PTERYPTOSIS PVDCRAO RC CO ERRD RET SCHIDR RUB GLACRVO SCHSCLER SINUSSLK TIATR AAU TR HYPHTRICHIA VIT HE
Grampian WalkGrampian Walk--In CasualtyIn Casualty
Top 10 Top 10 –– Eye Casualty!Eye Casualty!
1.1. Seasonal allergic conjunctivitisSeasonal allergic conjunctivitis2.2. Anterior UveitisAnterior Uveitis3.3. Infective ConjunctivitisInfective Conjunctivitis4.4. Corneal AbrasionCorneal Abrasion5.5. Dry EyeDry Eye6.6. EpiscleritisEpiscleritis7.7. Corneal FBCorneal FB8.8. HSKHSK9.9. Marginal KeratitisMarginal Keratitis10.10. PVDPVD11.11. TrichiasisTrichiasis

Contact Lens WorkContact Lens Work

CURRENT PRACTICECURRENT PRACTICE
THYGESONSTHYGESONS TRICHIASISTRICHIASIS
Meibomian

Dry Eye Allergy Infection Auto Immune
TraumaMechanical
Toxic Other
EvaporativeEvaporative NonEvaporative
NonEvaporative ChronicChronic AcuteAcute
VernalVernal
AtopicAtopic
GPCGPC
SeasonalSeasonal
PerennialPerennial
ViralViral
BacterialBacterial
InclusionInclusion
ParasiticParasitic
FungalFungal
EpiscleritisEpiscleritis
PemphigoidPemphigoid
UveitisUveitis
VasculitisVasculitis
ScleritisScleritis
Foreign Body
Foreign Body
InjuryInjury
TrichiasisTrichiasis
ChemicalChemical
MicrobialToxins
MicrobialToxins
AngleClosure
Glaucoma
AngleClosure
Glaucoma
RosaceaRosacea
EXTERNAL EYEEXTERNAL EYE
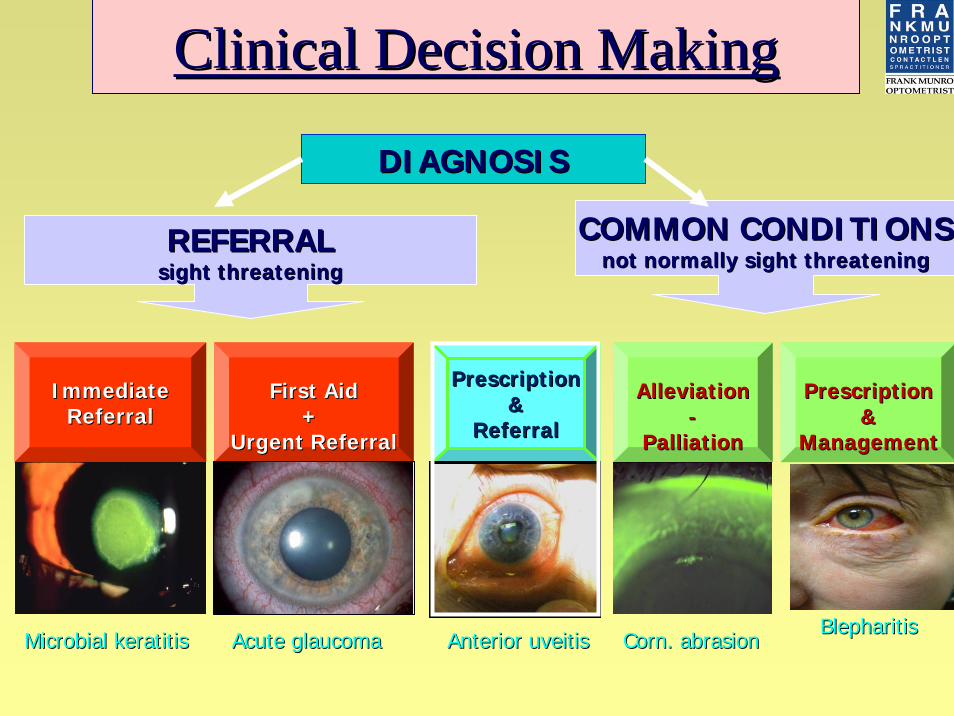
Clinical Decision MakingClinical Decision Making
COMMON CONDITIONSCOMMON CONDITIONSnot normally sight threateningnot normally sight threatening
REFERRALREFERRALsight threateningsight threatening
First AidFirst Aid+ +
Urgent ReferralUrgent Referral
ImmediateImmediateReferralReferral
PrescriptionPrescription&&
ReferralReferral
AlleviationAlleviation--
PalliationPalliation
PrescriptionPrescription&&
ManagementManagement
DIAGNOSISDIAGNOSIS
Acute glaucomaAcute glaucomaMicrobial keratitisMicrobial keratitis Anterior uveitisAnterior uveitis Corn. abrasionCorn. abrasionBlepharitisBlepharitis

External Eye Disease Patient Pathway
Patient PresentationSuspected external
eye disease
Self Care Primary Care Secondary Care
Hospital Eye ServiceRefer to Hospital Eye Service for diagnosis and appropriate management
Condition not normally sight threatening
Optometrist/GPManagement
AdvicePrescription
Diagnosis uncertain
Optometrist/GP
If no response or there is concern
Optometrist / GPSuspected external eye
disease
Optometrist
Diagnosis
If sight threatening condition is identified
Common conditions that are not normally sight threatening (can therefore be managed in the community) for example:
Dry EyeCorneal AbrasionForeign bodiesBlepharitisEpiscleritisBacterial conjunctivitisConjunctival haemorrhageHordeolaAllergic, Toxic or Viral external eye conditions
Conditions that are normally sight threatening (should therefore be managed in secondary care) for example:
Anterior UveitisInclusionScleritisEndophthalmitisCellulitisMicrobial KeratitisAngle Closure GlaucomaChemical BurnsMarginal KeratitisNeoplasia
URGENT REFERRAL
Follow up & discharge

HistoryHistory
nn Age / SexAge / Sexnn General HealthGeneral Healthnn POHPOHnn Family HistoryFamily Historynn Recent HistoryRecent Historynn Onset / Duration / Symptoms stable or varying or Onset / Duration / Symptoms stable or varying or
regressingregressingnn Pain / redness /vision /photophobiaPain / redness /vision /photophobiann Presentation Presentation –– recurring/ / Intermittent?recurring/ / Intermittent?

What is the problem?What is the problem?
nn Pain v No Pain Pain v No Pain -- ? severity? severity
nn Red v WhiteRed v White
nn Visual Loss v Normal VisionVisual Loss v Normal Vision
nn ? Floaters / Photopsia? Floaters / Photopsia
nn Duration: Recent v Long Term Duration: Recent v Long Term

ExaminationExamination
nn VA /PinholeVA /Pinholenn PupilsPupilsnn Ocular MotilityOcular Motilitynn Anterior Segment Anterior Segment –– lids/lashes/red?/conj/cornea/anterior lids/lashes/red?/conj/cornea/anterior
chamberchambernn Internal Internal –– Lens/vitreous/retina/macula/optic nerveLens/vitreous/retina/macula/optic nervenn Applanation tonometryApplanation tonometrynn Slit LampSlit Lampnn Volk Volk –– DILATE!DILATE!nn GonioGonionn Visual Fields / confrontationVisual Fields / confrontation

Points to PonderPoints to Ponder
AdnexaLid Margin
Lashes
LimbusFornices
Upper Lower Tarsal
Plica

Follicles v PapillaeFollicles v Papillae
Follicles consist of hyperplastic lymphoid tissue & appear as elevated lesions encircled by blood vessels. Typically seen in reaction to topical agents, adenoviral & chlamydial disease
Papillae consist of hyperplastic conjunctival tissue full of inflammatory cells, normally seen in the palpebral conjunctiva. Associated with bacterial, and allergic conjunctivitis

External Eye ProblemsExternal Eye Problems

Dry EyeDry Eye
EvaporativeEvaporativeEvaporative TearDeficient
TearTearDeficientDeficient
Exposure
Meibomian Gland Disease
Other
CL
Lid ProblemSjogren’s
Primary
Secondary
Non-Sjogren’s
Lacrimal Disease
Abnormal Blink
Abnormal Aperture
Incongruous Surface
Glands Missing
(Distichiasis)
Ant / Post Blepharitis
Ocular Surface (Xerophthalmia)
Lacrimal Gland Obstruction
Primary
Secondary
Auto Immune Disease
Loss of Reflex Tearing

TestsTests
nn SchirmersSchirmers type1 with anaesthesiatype1 with anaesthesiatype 2 as 1 with nasal irritationtype 2 as 1 with nasal irritation
whatman no 41 filter paperwhatman no 41 filter paper< 10mm abnormal. < 3mm conculsive< 10mm abnormal. < 3mm conculsive
nn Tear Break Up timeTear Break Up timefluorscein stain tearfilmfluorscein stain tearfilm< 10 sec abnormal (average of 3 tests)< 10 sec abnormal (average of 3 tests)

Treatment overviewTreatment overviewTear secretorsTear secretors
Castor oilCastor oil
Meibomium lid diseaseMeibomium lid disease
Plugs or occlusionPlugs or occlusionWarm compressesWarm compresses
Moisture chambersMoisture chambers
Androgen dropsAndrogen drops
Artificial tearsArtificial tears
ImmunosuppressiveImmunosuppressive
Omega 3 fatty acidsOmega 3 fatty acids
Mucin secretorsMucin secretors

Mechanical StimulationMechanical StimulationHot CompressesHot Compresses
Lid MassageLid Massage
Lid ScrubsLid Scrubs

Lubricants Promote Healing!Lubricants Promote Healing!
Normal goblet cell density
They’re decreased in Dry Eye
Treated with preservative free lubricants Lubricant
preserved with Benzalkonium Chloride
Goblet Cell Density & Preservatives

Choices? Choices? Choices?Choices? Choices? Choices?
Avoid Avoid Benzalkonium Benzalkonium
Chloride!Chloride!

TreatmentTreatment retention retention –– Punctum PlugsPunctum Plugs
Plastic or silicone plugs Plastic or silicone plugs or Collagenor Collagen
Removable?Removable?
Can fall outCan fall outCan irritateCan irritateInfection?Infection?Can convert a dry eye to Can convert a dry eye to
a wet onea wet one
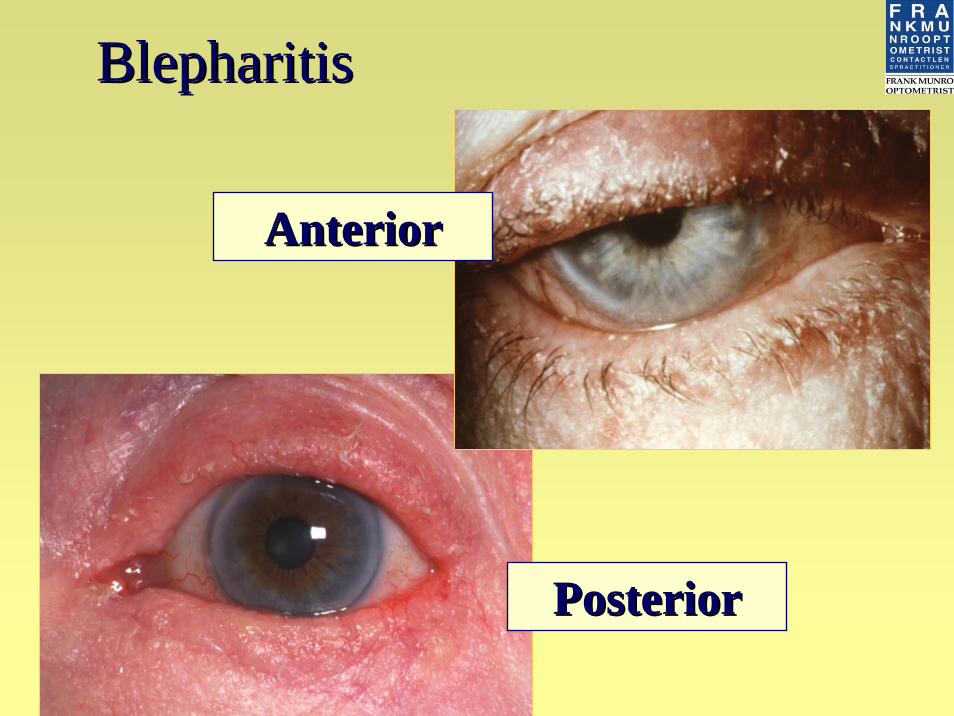
BlepharitisBlepharitis
AnteriorAnterior
PosteriorPosterior

BLEPHARITIS
1. Anterior• Staphylococcal• Seborrhoeic
• Meibomianitis• Meibomian seborrhoea
2. Posterior
3. Treatment

Staphylococcal blepharitis
•• Hyperaemia and telangiectasia of anteriorHyperaemia and telangiectasia of anteriorlid marginlid margin
•• Scarring and hypertrophy if longstandingScarring and hypertrophy if longstanding•• Scales around base of lashes Scales around base of lashes (collarettes)(collarettes)
•• Chronic irritation worse in morningsChronic irritation worse in mornings

Complications of blepharitis
Recurrent styes
Marginal keratitis Tear film instability
Trichiasis,madarosis,poliosis

Seborrhoeic blepharitis
•• Shiny anterior lid marginShiny anterior lid margin •• Greasy scales Greasy scales •• Lashes stuck togetherLashes stuck together•• Hyperaemia of lid marginHyperaemia of lid margin

Treatment of Blepharitis
1. Lid hygiene / Lid Scrubs1. Lid hygiene / Lid Scrubswith 50% baby shampoo / Suprannettes / Lid Carewith 50% baby shampoo / Suprannettes / Lid Care
2. Tear substitutes 2. Tear substitutes -- for associated tear film instabilityfor associated tear film instability
5. Systemic tetracyclines / Topical Steroids5. Systemic tetracyclines / Topical Steroids-- for severe blepharitisfor severe blepharitis
3. Warm compresses 3. Warm compresses -- to melt solidified sebum to melt solidified sebum in posterior blepharitis / ? Eyebagin posterior blepharitis / ? Eyebag
4. Topical antibiotics (Fucidic Acid) & steroids

HordeolaHordeola
Internal Internal
ExternalExternal

Chalazion (meibomian cyst)
Painless, roundish, firm lesion Painless, roundish, firm lesion within tarsal platewithin tarsal plate
May rupture through conjunctiva May rupture through conjunctiva and cause granulomaand cause granuloma

Acute hordeola
• Staph. abscess of meibomian glands
• Tender swelling within tarsal plate
• May discharge through skin or conjunctiva
• Staph. abscess of lash follicle and associated gland of Zeis or Moll
• Tender swelling at lid margin
• May discharge through skin
Internal hordeolum ( acute chalazion )
External hordeolum (stye)
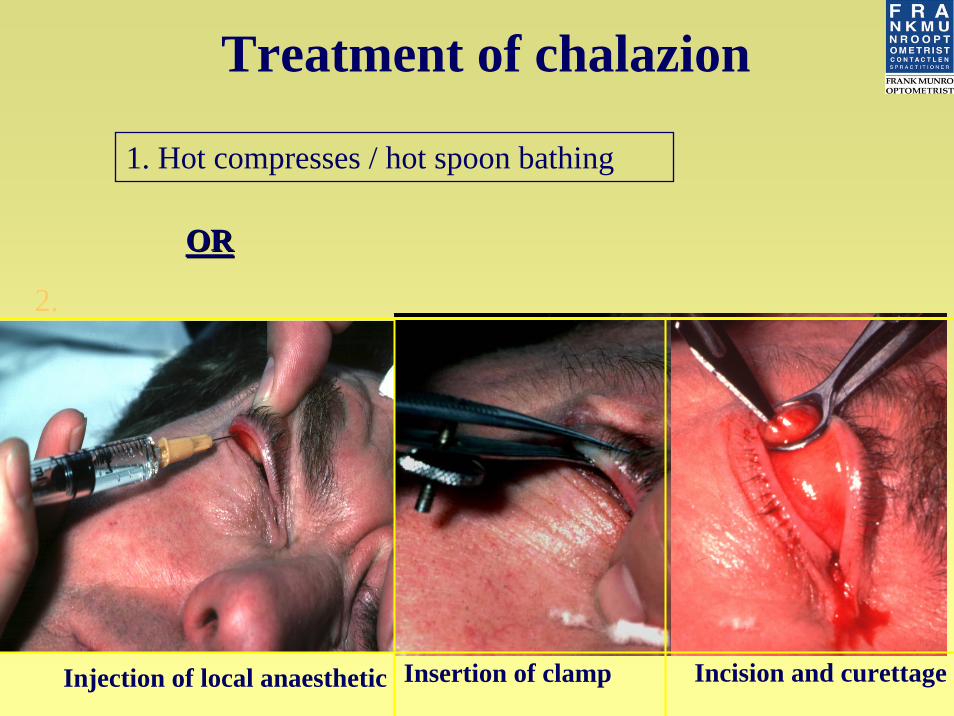
Treatment of chalazion
Injection of local anaesthetic Insertion of clamp Incision and curettage
1. Hot compresses / hot spoon bathing
OROR
2.

Trichiasis
•• Posterior misdirection of normal lashesPosterior misdirection of normal lashes
•• Most frequently affects lower lidMost frequently affects lower lid
Complications
•• Inferior punctate epitheliopathyInferior punctate epitheliopathy
•• Corneal ulceration and pannusCorneal ulceration and pannus
Signs

Treatment Options for Trichiasis
1. Epilation - but recurrence within few weeks
2. Electrolysis - but frequently repeated treatments required
3. Cryotherapy - for many lashes
4. Laser ablation - for few scattered lashes
5. Surgery - for localized crop resistant to other methods
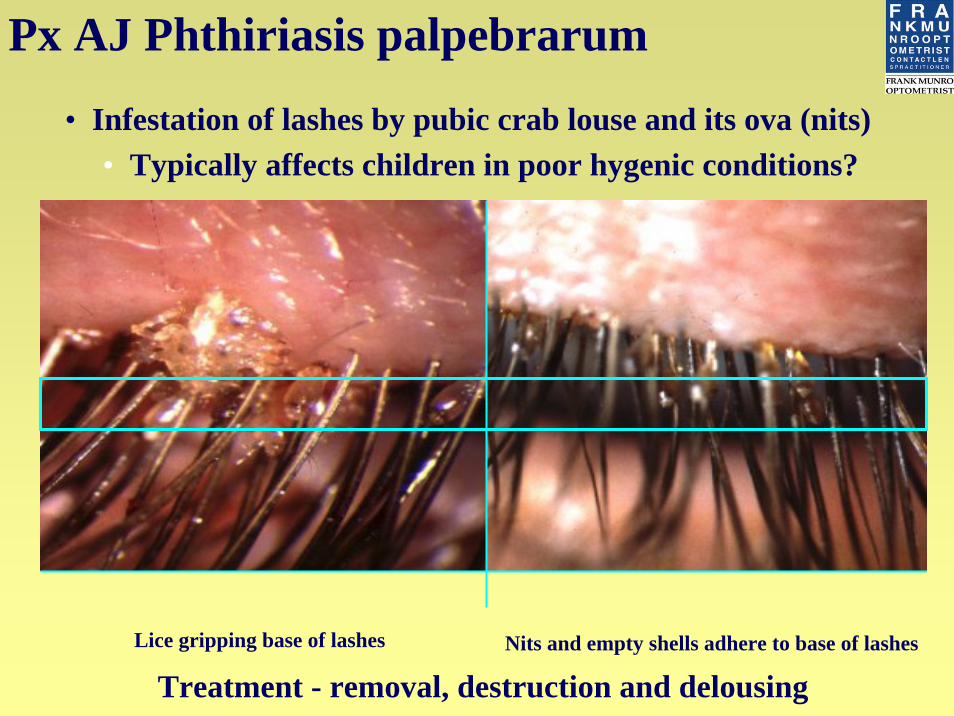
Px AJ Phthiriasis palpebrarum
• Infestation of lashes by pubic crab louse and its ova (nits)• Typically affects children in poor hygenic conditions?
Treatment - removal, destruction and delousingLice gripping base of lashes Nits and empty shells adhere to base of lashes

ConjunctivitisConjunctivitisBacterialBacterial
ViralViralAllergyAllergyToxicToxic

Simple bacterial conjunctivitis
Crusted eyelids and conjunctival injection
Subacute onset of mucopurulent discharge
Treatment - broad-spectrum topical antibiotics eg Chloramphenicol
Signs

Adenoviral KeratoconjunctivitisAdenoviral Keratoconjunctivitis
Pharyngoconjunctival fever • Adenovirus types 3 and 7• Typically affects children• Upper respiratory tract infection• Keratitis in 30% - usually mild
Epidemic keratoconjunctivitis • Adenovirus types 8 and 19• Very contageous• No systemic symptoms• Keratitis in 80% of cases - may be severe

Adenoviral conjunctivitis
Usually bilateral, acute waterydischarge and follicles
Subconjunctival haemorrhages andpseudomembranes if severe
Treatment - Symptomatic / lubricants / NSAIDS eg Acular/? Steroids?

Signs of Adenoviral keratitis
•• Focal, epithelial keratitisFocal, epithelial keratitis •• Focal, subepithelial keratitis Focal, subepithelial keratitis •• May persist for monthsMay persist for months
Treatment - topical steroids if visual acuitydiminished by subepithelial keratitis
•• TransientTransient

Adult chlamydial keratoconjunctivitis• Infection with Chlamydia trachomatis serotypes D to K• Concomitant genital infection is common
Treatment - topical tetracycline and oral tetracycline or erythromycin
Subacute, mucopurulent follicular conjunctivitis
Variable peripheral keratitis

Allergic rhinoconjunctivitis• Hypersensitivity reaction to specific airborn antigens
Transient conjunctival oedema
• Frequently associated nasal symptoms
Transient eyelid oedema
• May be seasonal or perennial
Treat. H1 blocker (topical/systemic) / Mast Cell Stabiliser / Topical Steroids

Recurrent Corneal Erosion Recurrent Corneal Erosion

Recurrent Corneal Erosion Recurrent Corneal Erosion SyndromeSyndrome
Corneal defect might look Corneal defect might look like thislike this

Corneal epithelium basement Corneal epithelium basement membranemembrane
Basal cells Basal cells secretesecrete basement basement membrane, and have membrane, and have hemidesmosome attachments hemidesmosome attachments through the basement through the basement membrane to the underlying membrane to the underlying stromastroma

Corneal epithelium basement Corneal epithelium basement membranemembrane
Spontaneous
~ Anterior Basement Membrane Dystrophy (map-dot-fingerprint dystrophy)Traumatic
~ Branch/ twig in eye, childs fingernail
Ass
ympt
omat
ic

Recurrent Corneal Erosion Recurrent Corneal Erosion SyndromeSyndrome
Typical therapy once correctly Typical therapy once correctly diagnosed is often something diagnosed is often something
like:like:---- Lacrilube before going to sleepLacrilube before going to sleep-- Artificial tears eg Viscotears or Artificial tears eg Viscotears or
Systane as required through the Systane as required through the day day -- (For up to 3 (For up to 3 –– 6 months)6 months)
-- Silicone Hydrogel Bandage CLSilicone Hydrogel Bandage CL

Recurrent Corneal Erosion SyndromeRecurrent Corneal Erosion Syndrome
Alternative therapies for those who fail with Alternative therapies for those who fail with ““basic therapybasic therapy””::--
-- Mechanical Debridement/ Diamond Burr (to Mechanical Debridement/ Diamond Burr (to ““polishpolish”” Bownams Membrane)Bownams Membrane)
-- Anterior Stromal MicroAnterior Stromal Micro--PuncturePuncture-- Excimer laser phototherapeutic Excimer laser phototherapeutic ––
keratectomykeratectomy-- Nd:YAG laser treatmentNd:YAG laser treatment-- Superficial phototherapeutic keratectomySuperficial phototherapeutic keratectomy

Marginal keratitis • Hypersensitivity reaction to Staph. exotoxins• Often associated with Staph. blepharitis• Normally unilateral, transient but recurrent
Subepithelial infiltrate separated by clear zone
Circumferential spread Bridging vascularization followed by resolution
Progression
Treatment -- short course of topical steroids / topical antibiotic eg Fucidic Acid

Acne rosaceaAcne rosacea

Rosacea keratitis
Peripheral inferiorvascularization
Subepithelial infiltration Thinning and perforationif severe
• Affects 5% of patients with acne rosaeca• Bilateral and chronic
Progression
Treatment - topical steroids and systemic/topical tetracycline or doxycyline
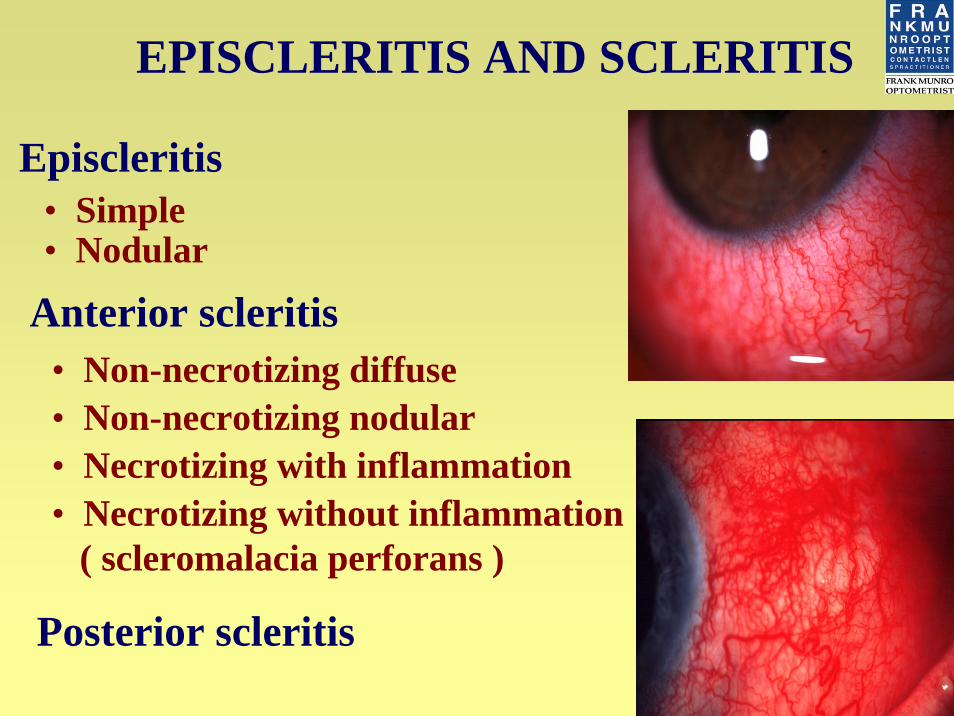
EPISCLERITIS AND SCLERITIS
Episcleritis• Simple• Nodular
Anterior scleritis• Non-necrotizing diffuse • Non-necrotizing nodular• Necrotizing with inflammation• Necrotizing without inflammation
( scleromalacia perforans )
Posterior scleritis

Applied anatomy of vascular coats
Scleritis
•• Maximal congestion of Maximal congestion of deep vascular plexusdeep vascular plexus
•• Slight congestion of Slight congestion of episcleral vesselsepiscleral vessels
•• Maximal congestion Maximal congestion of episcleral vesselsof episcleral vessels
EpiscleritisNormal
•• Radial superficial episcleralRadial superficial episcleralvesselsvessels
•• Deep vascular plexus Deep vascular plexus adjacent to scleraadjacent to sclera

Simple episcleritis• Common, benign, self-limiting but frequently recurrent• Typically affects young adults• Seldom associated with a systemic disorder
Treatment • Lubricants• Topical steroids • Systemic flurbiprofen if unresponsive)
Simple sectorial episcleritis Simple diffuse episcleritis

Nodular episcleritis• Less common than simple episcleritis• May take longer to resolve• Treatment - similar to simple episcleritis
Localized nodule which can be moved over scleraLocalized nodule which can be moved over sclera Deep scleral part of slitDeep scleral part of slit--beam beam not displacednot displaced

Phenylephrine TestPhenylephrine Test

Diffuse anterior non-necrotizing scleritis
• Widespread scleral and episcleral injection• Relatively benign - does not progress to necrosis
• Oral steroids if unresponsiveTreatment • Oral NSAIDs

Nodular anterior non-necrotizing scleritis
Scleral nodule cannot be moved over underlying tissue
More serious than diffuse scleritis
On cursory examination resembles nodular episcleritis
Treatment - similar to diffuse non-necrotizing scleritis

Case SL Case SL -- History History
nn Age 56, femaleAge 56, femalenn Referred to GIESReferred to GIESnn Presented with painful red eyePresented with painful red eyenn Hx recurring red eyeHx recurring red eyenn Vision down R 6/7.5, L 6/5Vision down R 6/7.5, L 6/5nn Good General HealthGood General Healthnn Early cataractEarly cataractnn Health fundiHealth fundinn IOP 10mmHg, L 14 mmHgIOP 10mmHg, L 14 mmHgnn PresbyopicPresbyopic

Slit LampSlit Lamp
nn Perilimbal rednessPerilimbal rednessnn Mild painMild painnn BlurringBlurringnn Flare anterior chamber Flare anterior chamber
–– finefinenn Irreg pupilIrreg pupilnn GP for checks GP for checks ––
autoimmune diseaseautoimmune disease(idiopathic)(idiopathic)

TreatmentTreatment
nn Cyclopentolate 1%Cyclopentolate 1%nn Pred Forte 1%Pred Forte 1%nn Review 1 week (check Review 1 week (check
IOP IOP –– ? steroid responder)? steroid responder)nn After 2 weeks eyes quietAfter 2 weeks eyes quietnn Wean off steroidWean off steroid
for one week (Rebound for one week (Rebound effect)effect)

UVEITISUVEITIS
Anterior UveitisAnterior Uveitis
Int. UveitisInt. Uveitis
Posterior UveitisPosterior Uveitis
Systemic Association / Infectious / Idiopathic
71%71%
1%1%
5%5%

Causes of Anterior UveitisCauses of Anterior Uveitis
50% 50% HLAHLA--B27 B27 positivepositive
Ankylosing Ankylosing spondylitisspondylitis
Psoriatic Psoriatic arthropathyarthropathy
Reiters Reiters SyndSynd
ACUTE v CHRONICACUTE v CHRONIC
Juvenile Juvenile Idiopathic Idiopathic ArthritisArthritis
Fuchs Fuchs Heterochromic Heterochromic
CyclitisCyclitis
Secondary to Secondary to trauma or trauma or infection infection
Behcets Behcets diseasedisease
SarcoidosisSarcoidosis
Herpes Herpes Zoster Zoster Ophth.Ophth.
SyphilisSyphilis
Ulcerative Ulcerative colitiscolitis
Crohn Crohn diseasedisease
IdiopathicIdiopathic

SIGNSSIGNS

Treatment of Anterior UveitisTreatment of Anterior Uveitisnn Pupil dilationPupil dilation
-- CyclopentolateCyclopentolate-- PhenylephrinePhenylephrine
nn Relieve painRelieve painnn Avoid post synAvoid post synnn Break post synBreak post synnn Reduce risk pupil blockReduce risk pupil block
nn Topical SteroidsTopical Steroids-- Pain reliefPain relief-- Inhibit migration of neutrophilsInhibit migration of neutrophils-- inhibit macrophage accessinhibit macrophage access-- decrease number of B & T lymphocytesdecrease number of B & T lymphocytes-- reduce histamine releasereduce histamine release-- reduce fibroblast proliferation & reduce fibroblast proliferation & collagen depositioncollagen deposition-- inhibit inflammatory activityinhibit inflammatory activity-- inhibit tissue scarring & regeneratoininhibit tissue scarring & regeneratoin
Steroids Derivatives Steroids Derivatives
nn Alcohol, acetate and phosphate baseAlcohol, acetate and phosphate base
nn Needs to be biphasic (to penetrate intact Needs to be biphasic (to penetrate intact hydrophobic and hydrophylic corneal hydrophobic and hydrophylic corneal layers)layers)
nn Alcohol & acetate base Alcohol & acetate base –– better penetration better penetration of the intact corneaof the intact cornea

Available Topical steroidsAvailable Topical steroids
nn Betamethasone sodium phosphate 0.1% Betamethasone sodium phosphate 0.1% –– Betnesol (Celltech)Betnesol (Celltech)nn Dexamethasone Alcohol 0.1% Dexamethasone Alcohol 0.1% -- Maxidex (Alcon)Maxidex (Alcon)nn Dexamethasone sodium phosphate 0.1% Dexamethasone sodium phosphate 0.1% -- Minims (Chauvin)Minims (Chauvin)nn Fluorametholone alcohol 0.1% Fluorametholone alcohol 0.1% -- FML (Allergan)FML (Allergan)nn Hydrocortisone acetate 0.5% Hydrocortisone acetate 0.5% -- non proprietrynon proprietrynn Prednisolone acetate 0.1% Prednisolone acetate 0.1% -- Pred Forte (Allergan)Pred Forte (Allergan)nn Prednisolone sodium phosphate 0.5% Prednisolone sodium phosphate 0.5% -- Predsol (Celltech)Predsol (Celltech)nn Rimexolone ? Acetate 1% Rimexolone ? Acetate 1% -- Vexol (Alcon)Vexol (Alcon)

Risk Effects Risk Effects -- Topical SteroidsTopical Steroids
nn Cataract formationCataract formationnn OHT OHT –– Glaucoma (steroid responder Glaucoma (steroid responder –– 70% of 170% of 1stst
degree F/H of glaucoma sufferers)degree F/H of glaucoma sufferers)nn Retardation of corneal healingRetardation of corneal healingnn Keratitis + aggravate HSKKeratitis + aggravate HSKnn Corneal thinningCorneal thinningnn PtosisPtosisnn Infection Infection –– fungalfungalnn Uveitis!Uveitis!

Px KM Px KM –– 45 year female45 year female
nn Pain / Red RE / Agony!Pain / Red RE / Agony!nn Arrived 10 hour plane journey AsiaArrived 10 hour plane journey Asiann Tender to touch Tender to touch --nn Nausea / blurred / needs to close eyeNausea / blurred / needs to close eyenn Gradual increase in pain past 10 hoursGradual increase in pain past 10 hoursnn Mild similar events in the recent pastMild similar events in the recent pastnn ? Infection? Infectionnn Good General HealthGood General Health

Clinical PresentationClinical Presentationnn VA poor 6/10VA poor 6/10nn SL gross bulbar rednessSL gross bulbar rednessnn Significant corneal oedemaSignificant corneal oedemann Pupil partially dilated & fixedPupil partially dilated & fixednn IOP R 48mmHg L 18Hg (Goldman)IOP R 48mmHg L 18Hg (Goldman)nn Narrow angle Narrow angle –– Shafer grade 0 Shafer grade 0

Angle Closure Glaucoma Angle Closure Glaucoma = Ocular Emergency= Ocular Emergency
First Aid First Aid –– PilocarpinePilocarpine
Same Day Same Day -- Rapid ReferralRapid Referral
Systemic Systemic –– oral & intravenous oral & intravenous DiamoxDiamox
YAG laser PI / ? TrabeculectomyYAG laser PI / ? Trabeculectomy
Beta Blockers / Steroids / Beta Blockers / Steroids / Hyperosmotic agentsHyperosmotic agents
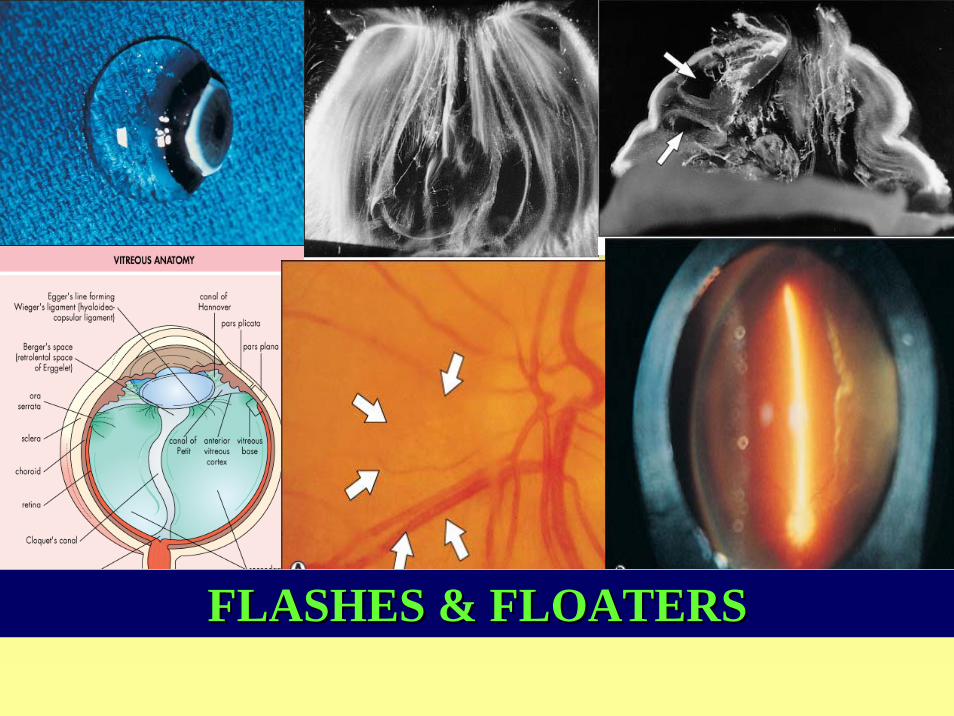
FLASHES & FLOATERSFLASHES & FLOATERS

Examine the patient on the slit Examine the patient on the slit lamplamp

Look at the anterior vitreousLook at the anterior vitreous
uu Dilate the pupilDilate the pupiluu Reduce Reduce ¼¼ width, width,
slit height<pupil, slit height<pupil, use maximum use maximum brightnessbrightness
uu Stir the vitreous: Stir the vitreous: ask the patient to ask the patient to look up, down and look up, down and straight aheadstraight ahead

Look for Vitreous HaemorrhageLook for Vitreous Haemorrhage
nn Numerous opacitiesNumerous opacitiesnn Can happen without Can happen without
retinal tearsretinal tearsnn Compare with other Compare with other
eyeeye

Posterior Vitreous DetachmentPosterior Vitreous Detachment
uu Detached Detached posterior hyaloid posterior hyaloid face behind lens, face behind lens, rippled mobile rippled mobile undulating net undulating net curtaincurtain

‘‘Tobacco dustTobacco dust’’ or Shafer signor Shafer sign
nn pigment clumps, pigment clumps, usually larger, darker usually larger, darker and more irregular and more irregular
nn Can be caused by Can be caused by ocular surgeryocular surgery

Acute posterior vitreous detachment: the Acute posterior vitreous detachment: the predictive value of vitreous pigment and predictive value of vitreous pigment and symptomatologysymptomatology
nn ‘‘presence of pigment in the vitreous gel to be a presence of pigment in the vitreous gel to be a reliable indicator of the presence of a retinal break reliable indicator of the presence of a retinal break in association with an acute PVD occurring in in association with an acute PVD occurring in 23/25 (92%) patients23/25 (92%) patients’’
nn V. Tanner, D. Harle, J. Tan, B. Foote, T. Williamson, and A. ChiV. Tanner, D. Harle, J. Tan, B. Foote, T. Williamson, and A. Chignellgnell Br J Ophthalmol. Br J Ophthalmol. 2000 November; 2000 November; 84(11): 126484(11): 1264––1268. 1268.

Look at Posterior vitreousLook at Posterior vitreous
nn Weiss ringWeiss ring

Look at Posterior PoleLook at Posterior Pole
nn Preretinal Preretinal haemorrhagehaemorrhage

Look at Peripheral RetinaLook at Peripheral Retina
uu Retinal tearsRetinal tearsFF 10% of PVD10% of PVDFF UU--shaped or shaped or
horseshoehorseshoeFF red red
discontinuitiesdiscontinuitiesFF Upper retina Upper retina
75%75%

Look at Peripheral RetinaLook at Peripheral Retina
uu Volk or 3 mirrorVolk or 3 mirroruu Retinal hole or lattice Retinal hole or lattice
degenerationdegeneration

Look at Peripheral RetinaLook at Peripheral Retinauu Retinal Retinal
detachmentdetachmentFF Convex Convex
configuration, configuration, corrugated corrugated appearance, appearance, undulatesundulates

Urgent Referral if Urgent Referral if symptomatic PVD symptomatic PVD with any of the following:with any of the following:
uu ‘‘Tobacco dustTobacco dust’’
uu Vitreous haemorrhageVitreous haemorrhage
uu Retinal tear Retinal tear
uu Retinal hole or lattice degenerationRetinal hole or lattice degeneration
uu Retinal detachmentRetinal detachment

ItIt’’s All About Decision Makings All About Decision Making
nn Accept responsibilityAccept responsibilitynn Work within your scope of practice : Do no harmWork within your scope of practice : Do no harmnn Develop GOS ? Grampian?Develop GOS ? Grampian?nn Develop your skill setDevelop your skill setnn Make GOS workMake GOS worknn Demonstrate all optometric competenciesDemonstrate all optometric competenciesnn Shift the balance of care!Shift the balance of care!nn Develop Level 2 / Independent PrescribingDevelop Level 2 / Independent Prescribing

Conclusion Conclusion –– Can we do More?Can we do More?
nn Professional AspirationProfessional Aspirationnn Fully Utilise Skill SetFully Utilise Skill Setnn Practice Development Practice Development –– Niche Opportunity?Niche Opportunity?
-- additional revenueadditional revenuenn Patient LoyaltyPatient Loyaltynn Practice DiversityPractice Diversity
-- Can we see beyond specs?Can we see beyond specs?nn Public BenefitPublic Benefit

Thanks for your kind attention!Thanks for your kind attention!