when rational men fall sick: an inquiry into some assumptions made by medical anthropologists
TRANSCRIPT

ALLAN YOUNG
W H E N R A T I O N A L MEN F A L L SICK: AN I N Q U I R Y I N T O
SOME A S S U M P T I O N S M A D E BY M E D I C A L
A N T H R O P O L O G I S T S
ABSTRACT. Medical anthropologists spend most of their time eliciting and interpreting people's statements about sickness and health. For this task, they make certain assumptions about the importance of language and reason. In this paper I argue that their assumptions are tailored to fit an hypothetical Rational Man rather than real people. The concept of 'explanatory models of sickness' is used to illustrate this point.
My critique begins by drawing attention to two non-cognitive determinants of people's statements: their degree of emotional arousal and their capacities for discoursing on medical subjects. These determinants are briefly discussed and then set aside, to make room for the paper's argument proper. This starts with the observation that medical anthropologists tend to overlook the fact that they have established a cognitive no man's land stretching between their informants' statements and the cognitive structures which are supposed to generate these statements.
I survey this void, using a five-fold model of medical knowledge. People use one kind of knowledge to organize their medical experiences and perceptions. In Rational Man writing, this form of knowledge is considered equivalent to cognitive structures (e.g., causal models, classificatory schemes), but I argue that it also includes knowledge of prototypical sickness events and knowledge that is embedded in actions, social relations, and material equipment. The theoretical implications of the five-fold model are outlined.
This is followed by an analysis of the reasoning processes in which people use medical knowledge to produce the statements whose meaning we wish to learn. I demonstrate the importance of being able to distinguish operational and monothetiC forms of rea- soning from pre-operational and polythetic ones. Rational Man writers are described as ignoring the latter pair. The concept of 'prototypes' is reintroduced to illustrate these points.
RATIONAL MAN AND THE ANTHROPOLOGISTS
Medical anthropologists study many kinds of facts, but most of their time is spent
studying people's statements about sickness and healing. This paper is about
how anthropologists interpret these statements. I shall argue that the relation
between what a person says and what he thinks, knows, and feels is usually
problematic, but most medical anthropologists ignore this problematic nature
by assuming that informants can be treated as if they were rational men. Their
assumption is unwarranted and leads them to bracket out the non-cognitive
and non-rational determinants of the statements they study.
Their unwarranted assumption is summarized in the following set of pro-
positions about language, knowledge, reasoning, and causality:
Culture, Medicine and Psychiatry 5 (1981) 317-335. 0165-005X/81/0054-0317 $01.90. Copyright © 1981 by D. Reidel Publishing Co., Dordrecht, Holland, and Boston, U.S.A.
318 ALLAN YOUNG
Language. It is through language that people are able to produce new knowl- edge, accommodate existing knowledge to new circumstances, and store knowl- edge. Cognition and language share underlying structures which organize thinking and thinkers' statements. Each verbal concept denotes a distinctive set of prop- erties which differentiates it from other terms along logical and often hierarchical divisions. Language gives people access to their knowledge ('beliefs'), and it is a satisfactory instrument for communicating this information to others. Thus, it is usually unnecessary to make a distinction between someone's 'volition' and his verbalizable 'intentions' (found embedded in his statements), in order to explain his behavior.
Knowledge. A person's knowledge about a given object, event, etc., is assumed to be more or less non-contradictory. Further, what he knows about the physical effects of his or some other agent's actions is broadly consistent with the effects he has actually observed. Contradictions occasionally occur in his knowledge or between his knowledge and observations, but under conditions which limit their importance. The thinker has 'reasons' for discounting them: he ignores some contradictions because they are irrelevant to the matter at hand, he defers the meaning of other contradictions to the attention of experts, and so on.
Reasoning. This is conscious mental processes by which people respond to internal and external demands for information by organizing knowledge. People tend to reason deductively or inductively, but not necessarily in logically rigorous ways. Deductive reasoning moves from a general principle to explain a particular instance. Someone says, for example, "Anxiety can produce sexual dysfunction. Because I am suffering a sexual dysfunction, a psychotropic medicine may end my symptoms." Inductive reasoning moves from a set of particular instances to a general principle. Someone says, for example, "I know many people who have been heavy smokers for years, and none of them developed heart disease. So, I don't think smoking is an important determinant of whether or not you'll have
a heart attack." Other forms of reasoning (e.g., 'symbolism') also occur, but they are generally
outside commonplace activities. They are usually found in dreams, rituals, magic, and expressive culture.
Causality. When people feel threatened by sickness, they are inclined to behave pragmatically. It is because they are able to conceive sickness events in causal terms, that they can attempt to predict and control what is going to happen.
These four propositions describe the human subject of most medical an- thropologists. I shall call him 'Rational Man'. 1 Although the universality of Rational Man has been questioned by various anthropologists - by Freudians, sociobiologists, proponents of prelogics and paralogies, for example - he is today a widely accepted paradigm. To be fair, Rational Man may be satisfactory
WHEN RATIONAL MEN FALL SICK 319
for understanding certain domains, such as commodity production and exchange. Further, it would be impossible to understand what people say and do if we did not take into account their strong rational and pragmatic tendencies. My aim is to put these tendencies in their place, not to deny their existence.
AN EXAMPLE OF HOW RATIONAL MAN THINKS
Medical anthropology cannot claim a distinctive and unified theory of sickness and healing. As a field, it depends on applying established anthropological concepts and methods to medical subjects. Within the medical anthropology literature, a central notion is the familiar idea that what people say and do needs to be understood in terms of the 'explanatory models' they carry in their minds. Explanatory models of sickness are sets of generalizations which enable the thinker to produce information about particular sickness episodes and events. More specifically, they are Rational Man's way to explain why and how a sickness episode occurred, ran its specific course, and produced its particular outcome. Explanatory models provide him with the information he needs for choosing and evaluating medical strategies, communicating with other people about sickness, and making his own distress recognizable to them (e.g., Kleinman
1980: 71-72 , 105). Because of their instrumental importance, explanatory models are strongly oriented to making statements about causality. For example, in a recent monograph Kleinman suggests a set of open-ended questions as a means for eliciting patients' explanatory models in clinical settings. An initial question asks the informant to label his complaint; the seven remaining questions ask him information about causality, i.e., about the causes of onset, the causes of specific symptoms, personal problems sickness has caused or can cause, and the treatment that can cause desirable results (Kleinman 1980:106).
I want to reiterate that none of these anthropologists is supposing that Rational Man is either a rigorous logician or necessarily a systematic thinker. Kleinman and others call attention to the fact that explanatory models are frequently fragmentary and not fully worked out, that they need to be under- stood contextually (for a particular individual, a particular complaint, and a particular time), that they often change and are influenced by the individual's experiences, and that they do not determine medical behavior in a mechanical way (e.g., Kleinman 1980: 107,109).
NON-COGNITIVE DETERMINANTS OF STATEMENTS
Students of Rational Man concentrate on the cognitive determinants of his statements. In my critical comments, I shall want to focus on cognitive issues,

320 ALLAN YOUNG
also. But first I need to say something about two non-cognitive determinants, i.e., emotional arousal and the ability to discourse on medical subjects.
STATEMENTS AND EMOTION
It is not news to read that a person's thoughts about sickness can arouse in him intense emotional states (particularly in the clinical environment), or that prolonged and intense emotions can affect a person's cognition and the form and content of his statements. In spite of this obvious connection between sickness, affect, and cognition, anthropologists have tended to take a narrow view of emotions, thinking of them either as socially disruptive forces that need to be controlled, or as energies that sometimes can be harnassed in rituals.
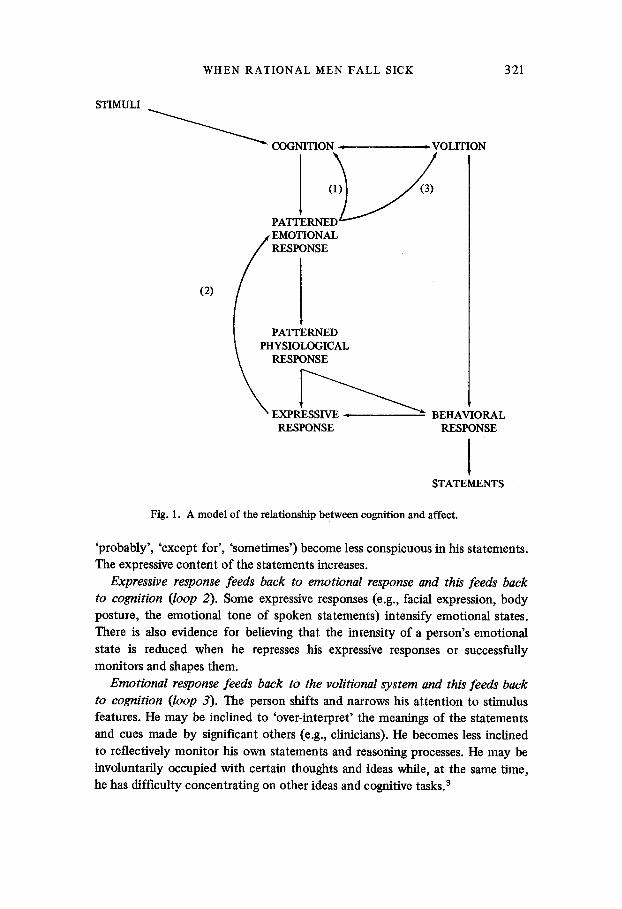
There is not yet a fully worked out social psychological theory about the relationship between emotion and thinking. The beginnings of a cognitive theory of affect can be found in the recent writings of Richard Lazarus and his associates (1979, 1980), Howard Leventhal (1980), Aaron Beck and his associates (1979), and Aruthur Kleinman (1980). Figure One schematizes this emerging framework. The theory articulates three psychological systems - cognitive, volitional, and affective. 2 In it, the quality and intensity of someone's emotional arousal (e.g., anger, dysphoria) depend on his cognitive appraisal of threatening or challenging stimuli, and his evaluation of his options and resources for coping with them. In addition, the intensity of his arousal may be affected by the verbalizable concepts (terms) he uses to identify, monitor, and explain his emotional states. For example, some writers have suggested that when a person intellectualizes his emotional experiences, by conceptualizing them in abstract and consciously analytical terms, he also disassociates the cognitive, volitional, and affective systems from one another. Somatization of affect, where a person thinks of his emotional state as a physical consequence of non-psychological causes, is described in similar terms. In each case, writers suggest, disassociation may reduce the intensity of the individual's arousal.
I make these points in order to call attention to the three feed back loops in Figure 1. Because they mark the ways in which emotional arousal may affect cognition, the loops are reasons for asking questions about the meaning of Rational Man's statements about sickness. It seems to me that it is too early to give a detailed account to the cognitive effects of particular emotional exper- iences. They will have to be worked out in future research. Even so, it is possible to speculate, at a very abstract level, about some of the cognitive shifts and changes that appear to occur under these conditions:
Emotional response feeds back to cognition (loop 1). The speaker shifts away from abstract deductive and inductive reasoning and talks about objects and events in terms of their concrete meanings for him. 'Hedges' (e.g., 'nearly',
WHEN RATIONAL MEN FALL SICK 321
STIMULI
(2)
COGNITION ~,
P A T T E R N E ( ~
'
ESPONSE
E X P R E ~ RESPONSE
, VOLITION
BEHAVIORAL RESPONSE
1 STATEMENTS
Fig. 1. A model of the relationship between cognition and affect.
'probably', 'except for', 'sometimes') become less conspicuous in his statements. The expressive content of the statements increases.
Expressive response feeds back to emotional response and this feeds back to cognition (loop 2). Some expressive responses (e.g., facial expression, body posture, the emotional tone of spoken statements) intensify emotional states. There is also evidence for believing that the intensity of a person's emotional state is reduced when he represses his expressive responses or successfully monitors and shapes them.
Emotional response feeds back to the volitional system and this feeds back to cognition (loop 3). The person shifts and narrows his attention to stimulus features. He may be inclined to 'over-interpret' the meanings of the statements and cues made by significant others (e.g., clinicians). He becomes less inclined to reflectively monitor his own statements and reasoning processes. He may be involuntarily occupied with certain thoughts and ideas while, at the same time, he has difficulty concentrating on other ideas and cognitive tasks, a
322 ALLAN YOUNG
Having made a case for studying cognitive, volitional, and emotional systems in association, I want to make an exception for myself. In the interests of simpli- fying my argument in the following section, I shall write about the cognitive system more or less in isolation from the others.
THE ABILITY TO DISCOURSE
Let me briefly mention something which is perhaps obvious already. The state- ments which anthropologists overhear and elicit are influenced by extrinsic determinants. People differ widely in their abilities and willingness to discourse on a given subject: one person can generate statements effortlessly, a second cannot. Common explanations for this include differences in people's verbal abilities (e.g., access to elaborated codes), technical knowledge of the subject, previous experiences at discoursing or thinking about the subject, notions about what are socially permitted statements on this subject or to this kind of person, beliefs about what the speaker can reasonbly expect the listener to understand, hidden agendas (e.g., the intentions of avoiding a protracted session or pleasing the listener), self-assurance, and intelligence. For many of the same reasons, the freedom or fluency with which a person discourses on a subject may change from occasion to occasion.
In order to leave my following argument as uncluttered as possible, I shall also bracket out these extrinsic influences and ask the reader to suppose that I am referring only to the statements of knowledgeable and freely discoursing people.
A COGNITIVE NO MAN'S LAND
A statement about sickness is a moment in a process in which the speaker is producing knowledge for himself and others. To learn the meaning of his statement, we must be able to re-insert it into this complicated process and articulate it with the forms of knowledge and modes of reasoning which deter- mined it. Medical anthropologists tend to over-simplify the process by reducing it to two elements: statement and the cognitive structures (e.g., explanatory models, conceptual categories) which are supposed to generate the statements. The distance between cognitive structures and spoken statements is left as a kind of mental no man's land.
Why have they neglected this issue? Once again, it is because most medical anthropologists have been studying Rational Man. In their writing, they have tended to assume that either (1) an informant can be coached to reproduce in speech the ostensible internal, mental statements that are equivalent to his 'thinking' and the cognitive determinants of his actions, or (2) an anthropologist

WHEN RATIONAL MEN FALL SICK 323
can, by studying his informant's spoken statements, identify cognitive structures with which he (the anthropologist) can reconstruct facsimiles of the informant's mental statements. This is the reason that these anthropologists are satisfied with a void between cognitive structure and spoken statements. It is also the reason why they tend to see what is in reality a central theoretical problem (i.e., how statements are connected to thinking and behavior) as if it were a methodological one (e.g., the problem of framing questions for eliciting statements).
The following sections are about this neglected subject. In them, I outline a way of conceptualizing the process through which people produce their state- ments about sickness and healing.
THEORETICAL KNOWLEDGE AND COGNITIVE STRUCTURES
Although each person knows a variety of medical facts, he does not know all of his facts in the same way. When we study these different kinds of facts and how they are related to one another within a process producing knowledge and statements, we are mapping the cognitive void left behind by Rational Man theorists. In a later section, I shall conceptualize these relations in terms of five kinds of knowledge. In the next few pages, however, I am interested in only one kind, a form I shall call 'theoretical knowledge'.
A person uses his theoretical knowledge of sickness and healing to organize discrete events and experiences into classes or families. Sometimes, his theoret- ical knowledge is in the form of explicit verbal schemes, such as standardized etiologies, ethnophysiological models, and formal nosologies. Other verbal schemes take the form of analogies, e.g., physiological processes are described in terms of the workings of machines, classifications implicit in everyday lan- guage, e.g., the chronic/transient contrast between 'a nervous person' and 'a person suffering a case of nerves'; and functional notions implicit in the layman's use of terms such as 'hypertension' and 'nervous breakdown'.
These examples of theoretical knowledge are ~cognitive structures', in the sense in which Rational Man theorists use this term. In the next two sections, I am going to argue that there are schemes which are theoretical knowledge but not 'cognitive structures', as that term is ordinarily used. These schemes include instanCes where an organizing principle is embedded in the behavior, social relations, and material equipment that people use in order to produce their knowledge of sickness and to shape sickness in socially recognizable and acceptable ways. They also include instances in which a person uses a particular sickness episode (e.g., an episode he has lived) as a prototype for organizing and understanding subsequent episodes. My point will be that these two instances of theoretical knowledge are generally beyond the reach, and interest, of Rational Man writers.

324 ALLAN YOUNG
EMBEDDED PRINCIPLES AS THEORETICAL KNOWLEDGE
Rational Man assumptions concentrate on the verbal determinants of statements, perceptions, and behavior. These assumptions are adequate for analyzing many sickness episodes, of course. We know that when sickness creates a disturbing flux of events, language sometimes restores a sense of order.
Only sometimes, however. Language often orders events which have been ordered already through schemes embedded in the actions, social relations, and equipment needed to produce these events - e.g., embedded in taken-for- granted clinical procedures and apparatuses.
Latour and Woolgar (1979) use the term 'reified statements' to describe the theoretical knowledge they found embedded in the skills and equipment of medical scientists. In a recent paper (Young 1980), I made a similar point, describing how complex theoretical knowledge is embedded in the division of labor and interlocutory instruments that researchers use for producing their facts and statements about stressful life events. My argument was that these arrangements always produce facts and statements about de-socialized people.
Both studies make the point that people (patients, clinicians, researchers, etc.) are generally unable or unwilling to scrutinize their embedded theoretical knowledge. One reason is that a person's language does not always give him access to his non-verbal schemes. Second, these schemes often take the form of common sense knowledge and customary behavior for which there seem to be no reasonable alternatives. Third, the clinician's professional and intellectual authority are generally effective barriers against his patients' critical interests in such matters (e.g., in the trajectory of questions during a diagnostic interview). Finally, from the clinician's point of view, embedded knowledge is a form of pro- fessional investment (absorbing money and professional time), and is integral to his reputation and capacity for continued productive work. His tendency is to continue investing in this knowledge rather than to self-consciously examine it.
I want to mention one more study. But in this instance I want to draw attention to the embedded knowledge of medical anthropologists. In The Domestication of the Savage Mind (1977), Jack Goody makes the point that printed and written texts are saturated with reified statements, embedded in the architecture of sentences, clauses, and paragraphs, in the use of markers such as quotation marks, in the suspension and reversibility of time, and so on. One implication of Goody's book is that as people become habituated to interpreting and producing texts, they acquire a tendency to 'textualize' utterances. That is, they expect utterances to conform to the character o f written statements. The tendency is reinforced by the high value that these people, among whom we include medical anthropologists of course, come to place on textualizing their own utterances.
WHEN RATIONAL MEN FALL SICK 325
By 'textualizing', I mean tendencies towards (1) interpreting statements abstractly, as simultaneously objects in themselves and elements in a system of statements (the text), (2) evaluating and interpreting statements in terms of the technical procedures used to produce them, and (3) treating a corpus of statements, the text, as an object about which other statements (i.e., com- mentaries) can be produced. When we textualize oral statements, these three tendencies are carried over as a set of expectations, i.e., expectations that speakers can discourse abstractly, produce utterances that mirror prior internal statements ('thinking'), and self-consciously monitor the trajectory of their oral statements.
These are reasons for arguing that textualization, rather than putatively universal cognitive tendencies, accounts for some key properties attributed to Rational Man. Let me add quickly that there are other traditions - e.g.,juridical, rhetorical, and narrative - which may have similar effects in non-literate com- munities. My point in introducing this argument is that features such as abstrac- tion, deliberation, and commentary must not be assumed a priori.
PROTOTYPES AS THEORETICAL KNOWLEDGE
Rational Man theorists assume that interpretive schemes are more or less stable from occasion to occasion and can be translated into a propositional language (e.g., " I f X occurs in the presence of Y, then Z is likely to follow because . . . " ) . It is this translatability that is supposed to enable an empathetic physician to 'reason together' with his patients about the causes and implications of their sicknesses. Once more, the Rational Man assumption is only sometimes justified.
Two objections can be raised in this connection. The first is that Rational Man uses his terms monotheticaUy, in the sense that each of his terms denotes a constant and distinctive set of properties that differentiates it from other terms along logical and often hierarchical divisions. But Rodney Needham has argued persuasively that real speakers often use key terms polythetically, so that a verbal concept - e.g., 'pain', 'health', 'therapeutic' - refers to a range of experiences,
actions, and utterances, linked to one another on the basis of heterogeneous features and qualities (Needham 1975: 352). I shall elaborate on the notion of polythetic usages in a later section.
Second, Rational Man's belief-statements about medical events are organized mainly in terms of causes and effects embedded in explanatory models. The statements made by real speakers, on the other hand, are often determined by their knowledge of prototypical sickness events.
At first glance, the prototypical sickness event seems similar to what physi- cians call a 'classic case', since in both instances an individual is using a sickness
326 ALLAN YOUNG
episode which occurred in the past as an instrument for organizing subsequent events and episodes. But there is a fundamental difference: while a classic case is a representation of general principles (causal and functional), a prototypical episode consists of a congeries of elements rather than a system of elements. In the latter, symptoms, behavior patterns, psychological states, sensations, outcomes, etc., are juxtaposed. They seem grouped into an episode on the basis of continguity - the speaker has observed that they co-occur or follow after one another - rather than on causal or functional grounds. Because these elements are not organized into functional systems or locked into nesting hierachies of verbal classifications, the individual has considerable freedom to disassociate, recombine, invoke, or ignore particular elements from occasion to occasion, even from moment to moment. This fact helps to explain why even empathetic clinicians sometimes have difficulty identifying the implications of their patients' statements or the limits of their symptomatic complaints.
KINDS OF MEDICAL KNOWLEDGE
Earlier, I remarked that people do not know all of their medical facts in the same way. I want to elaborate this remark now, showing that people produce different forms of knowledge for different ends. Before I begin, I want to emphasize that the following division of knowledge is n o t a typology. It is simply a way of conceptualizing how a speaker's knowledge, modes of reasoning and expectations determine the contents and form of his statements.
I think it is useful to talk about five kinds of knowledge: (1) There is a person's theoretical knowledge. (2) There is his empirical knowledge of objects, events, and experiences that
he has observed or that have been related to him. While theoretical knowledge refers to reality by means of an 'all things being equal' clause (e.g., 'X follows Y, all things being equal'), empirical knowledge takes account, albeit selectively, of the particularities of things and experiences.
(3) There is his rationalized knowledge, in which he conceptualizes objects, events, and experiences in psychologically satisfying ways (e.g., by organizing medical events into coherent narratives), making them ontologicaUy consistent with his beliefs about the nature of the material world and existentially coherent with his beliefs and feelings about his and other people's essential nature, pre- vious life experiences, fate, etc.
(4) There is his intersubjective knowledge, in which he conceptualizes objects, events, and experiences in ways and words which he believes will make them intelligible to the people with whom he wants to communicate.
(5) Finally, there is the knowledge which he produces by negotiating the meaning of objects, events, and experiences, in interaction with other people.
WHEN RATIONAL MEN FALL SICK 327
For example, negotiated knowledge is produced in diagnostic sessions when a patient and clinician collaborate to establish the character and importance of a 'subjectively' experienced symptomatic state (e.g., the intensity of the patient's discomfort, the extent to which the discomfort interferes with his daily activities).
In the course of a sickness episode, a person is likely to produce several kinds of knowledge. This is one reason it is incorrect to assume that every statement
he makes about a set o f medical events can be properly worked into a single
account o f those events. (Another reason has already been discussed in con- nection with the tendency of some writers to 'textualize' their informants' utterances.)
Why then have Rational Man writers singled out the importance of theoretical knowledge (i.e., 'cognitive structures')? Partly, it is because this knowledge seems to be more permanent and more a social fact than do the other forms. That is, a person's theoretical knowledge is less context dependent, versions of it are often stabilized in written texts and as professional knowledge, and a modicum of shared (and, therefore, conserved) theoretical knowledge is required for successful interaction during sickness episodes and on other social occasions. Theoretical knowledge also seems more fundamental than do other forms, because actors use it to decide the relevance and utility of making certain observations or holding certain interests. (For example, it is the physician's allopathic theoretical knowledge that makes clincial observations about hot/cold imbalances in his patients' diets irrelevant and meaningless.) Thus, it increases or decreases the likelihood that certain instances of empirical knowledge will be produced and, in this way, affects the content of intersubjective and negotiated knowledge.
Nevertheless, there is no a priori reason to suppose that one kind of knowl- edge is more authentic than the others. After all, each form is connected to specific intentions and acts, and the adequacy of each is evaluated against its particular effects, e.g., how well it identifies an appropriate therapeutic inter- vention, reduces or controls anxiety, or meets the demands of an interlocutor for information. For instance, informants sometimes report that the knowledge they have negotiated in clinical sessions is less valid than their own empirical knowledge. They reason that the former was determined by the social authority of the physician while the latter reflects, however imperfectly, the objective facts. Put into other words, they claim that the clinician has coerced them into misrepresenting their symptoms. Clearly this is not always the case. The same people, on other occasions, report that their empirical knowledge is unreliable, while knowledge negotiated with an expert diagnostician is credible. (Is this more likely when an acute self-limited ailment is being presented?)
Also, the relation between kinds of knowledge is often dialectical. For
328 ALLAN YOUNG
instance, a person's negotiated knowledge of a particular event is made possible by his theoretical knowledge of the class of events into which it fits. But there are also occasions when newly negotiated knowledge becomes theoretical knowl- edge. This occurs when a patient uses negotiated (diagnosed) knowledge of his or her ailment to construct a prototype for interpreting future instances - when, for example, a woman's experiences with depression become for her and her family an instrument for interpreting the other cases of depression they learn
about.
SOME QUESTIONS ABOUT MEANING
Now we can see how the establishment of a cognitive no man's land, bounded on one side by utterances (i.e., negotiated knowledge, and the only kind of state- ments to which we have direct access) and on the other by cognitive structures (one form of theoretical knowledge), imposes two serious limitations on the sorts of questions we can ask and the sorts of analyses we can undertake.
First, it obscures the question of how people's utterances are related to intemal states, such as 'healing' and 'satisfaction', to which medical anthropolo- gists allude. Needham, following Wittgenstein, writes that "when a man utters a belief-statement he is not reporting an inner experience of a discriminable kind . . . . " The meaning the speaker expresses "is the effect that he intends to procure, and this is an expectation that he has learned by his familiarity with the linguistic and other conventions of the culture" (Needham 1972: 242). Whether or not Needham is correct is of less immediate importance than the question he calls attention to: What do we have to know before we can give a meaning to terms like 'healing' and 'satisfaction'? Given their prominence in the medical anthropolgy discourse, these terms would seem to be too impor- tant to abandon on a no man's land. And yet we have no clear idea of precisely what they mean outside the domain of acute self-limited diseases. Do they properly refer to certain states of rationalized knowledge, e.g., what R. D. Laing describes as 'ontological security'? Or should they be equivalent to the speaker's empirical knowledge of certain psychophysiological states? Once again, the immediate point is not to choose an answer, but to be able to ask such questions at all.
Second, the existence of a cognitive no man's land makes it difficult to conceptualize the production of medical knowledge in terms of anything ex- cept universal and abstract cognitive operations. (In the case of Rational Man theory, these operations are assumed to take the form of pervasive deductive and inductive modes of reasoning.) But, as I shall argue in the next section, there are good grounds for supposing that these cognitive operations are really highly variegated.

WHEN RATIONAL MEN FALL SICK 329
REASONING
My final task is, then, to identify the cognitive operations in which different forms of knowledge are used and produced. These operations are mental pro- cesses through which a person (1) accomodates his thinking to reality, so that his knowledge of objects, events, and experiences transcends the variabilities and fluctuations of his environment, and (2) assimilates new, or newly reflected upon, experiences and observations to his existing knowledge.
Jean Piaget introduced the terms 'operational' and 'pre-operational' to identify developmental stages in an individual's ability to perform cognitive operations. 4 C. R. Hallpike (1979) has recently adapted Piaget's distinction to characterize types of cognitive orientations, without limiting them to ontogenetic issues. I follow Hallpike's practice here. 5
Operational thought can be defined inexactly as what is meant in everyday language by 'logical reasoning'. Rational Man is an operational thinker. Pre- operational thought is not consistent with syllogistic reasoning. In the sense in which I have adapted this term from Piaget and Hallpike, it is typified by two features: (1) in practice, the individual blurs the distinction between theoretical and rationalized knowledge in a way that centers his interpretive schemes on his own experiences, and (2) his movement between theoretical and empirical knowledge is dominated by transductive rather than inductive or deductive reasoning, and polythetic rather than monothetic terms. I shall have more to say about these points in a moment.
There are people whose thinking is habitually pre-operational. These are children according to Piaget, but Hallpike also includes tribal peoples in this category. There are also those people whose cognitive operations generally lie somewhere between the operational and pre-operational poles. I conjecture that a large proportion of people living in industrial societies fall into this category. Finally, there are people who revert to pre-operational thinking when they are drawn into difficult and emotion-arousing situations. I alluded to this point at the end of the section on affect and cognition.
The distinction between operational and pre-operational reasoning is impor- tant because each mode produces distinctive statements and understandings of medical events. In pre-operational thought, reality is bound up with phenomenal reality, and statements emphasize concrete imagery rather than abstract prop- erties and relationships that transcend experiences. The thinker does not reason on the basis of propositions: he cannot consider statements merely as statements separate from action and his own experiences, and he has no notion of mind as mediating and encoding experience by means of conceptual structures. For example, he cannot understand words and names in terms of their conventional origins.
330 ALLAN YOUNG
The pre-operational thinker has a propensity to detach objects and events from the constellation of factors and relationships which affect them, and often attributes to them an inner dynamism or essence which is believed to account for what happens. For example, the thinker ascribes someone's repeated sick- nesses to his 'sickliness', or explains someone's recurrent misfortunes to his 'bad
luck'. He has a second propensity to assimilate his current experiences to prototypes
- an issue raised in an earlier section. It is through his use of prototypes that the thinker reasons transductively (Hallpike's term), i.e., moving from particular (prototype) to particular (experiential referent), rather than from particular to general (inductively) or from general to particular (deductively). By extrapolating from the work of L. S. Vygotsky (1962, orig. 1934; see also Olver and Hornsby 1966), we can anticipate that subsequent research will show that transductive reasoning takes various forms. In one form, a thinker associates elements (symp- toms, organs, emotions, patterns of behavior, etc.) into a 'complex' on the basis of their contiguity. In a more complicated form, called a 'chain-complex', meaning is carried from link to link but the decisive attribute keeps changing during the process.
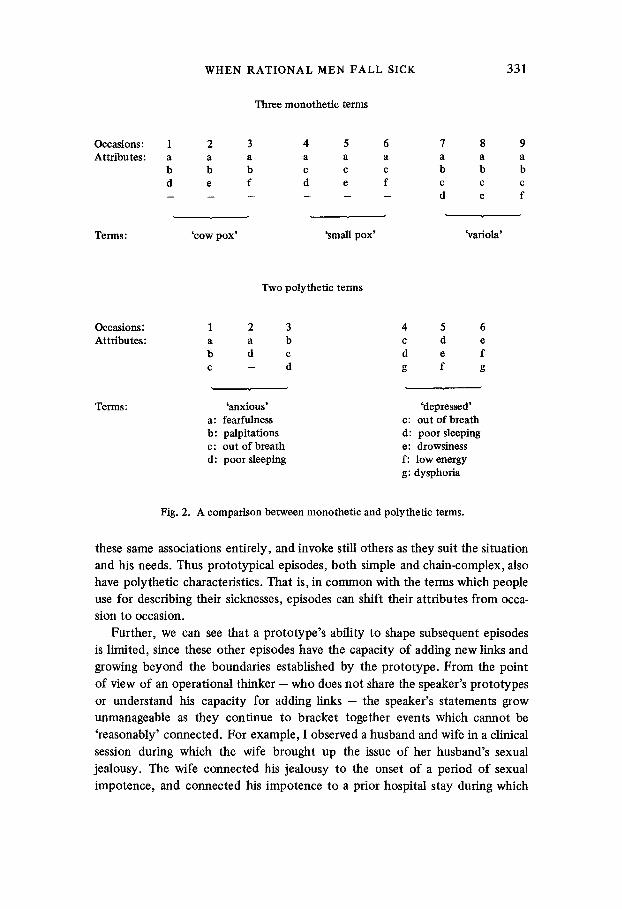
In order to understand this last point, it is necessary to return to the notions of monothetic and polythetic terms. You will recall that a monothetic term denotes a constant and distinctive set of attributes which differentiates it from other terms along logical and often hierarchical divisions. The statements made by Rational Man consist of monothetic terms. Figure 2 schematizes three monothetic terms: 'cow pox', 'small pox', and 'variola' (a term which subsumes the other two). 6 Figure Two also contains two examples of polythetic terms. By their nature, polythetic terms are often difficult to describe succinctly, and I have illustrated this notion by referring to how one informant used the terms 'anxious' and 'depressed' to describe himself on different occasions.
Now let us come back to the observation that in a chin-complex prototype J
elements or attributes are joined together by heterogeneous links (e.g., in the case of 'anxiety' the links between a, b, c on occasion 1). Some elements can be connected as causes and effects, others by their propinquity within the body, still others through linguistic conventions and imagery, or through shared emotive qualities. Because these complexes consist only of relations between single elements and no more ( a -b , a -c , b - c , rather than a - b - c ) , all elements seem functionally equal. Finally, since each element enters such a complex concretely and in its entirety, complexes have a capacity for continually ex- panding, adding link after link.
Depending on the particular occasion for which he uses a prototypic event, the pre-operational thinker invokes only some of the possible concrete associa- tions between the prototype and its referent. On other occasions, he may ignore
WHEN RATIONAL MEN FALL SICK
Three monothetic terms
331
Occasions: Attributes:
1 2 3 4 5 6 7 a a a a a a a b b b c c c b d e f d e f c . . . . . . d
Terms: 'cow pox' 'small pox'
8 a
b e
e
'variola'
Two polythetic terms
Occasions: Attributes:
1 2 3 4 5 a a b c d b d c d e c - d g f
Terms: 'anxious' 'depressed' a: fearfulness c: out of breath b: palpitations d: poor sleeping c: out of breath e: drowsiness d: poor sleeping f: low energy
g: dysphoria
Fig. 2. A comparison between monothetic and polythetic terms.
these same associations entirely, and invoke still others as they suit the situation
and his needs. Thus prototypical episodes, both simple and chain-complex, also
have polythetic characteristics. That is, in common with the terms which people
use for describing their sicknesses, episodes can shift their attributes from occa-
sion to occasion.
Further, we can see that a prototype's ability to shape subsequent episodes
is limited, since these other episodes have the capacity of adding new links and
growing beyond the boundaries established by the prototype. From the point
of view of an operational thinker - who does not share the speaker's prototypes
or understand his capacity for adding links - the speaker's statements grow
unmanageable as they continue to bracket together events which cannot be
'reasonably' connected. For example, I observed a husband and wife in a clinical
session during which the wife brought up the issue of her husband's sexual
jealousy. The wife connected his jealousy to the onset of a period of sexual
impotence, and connected his impotence to a prior hospital stay during which
332 ALLAN YOUNG
he had been treated for undiagnosed (her view) back pain. The hospital stay and the onset of impotence were separated by many months. In the course of this session and in response to the clinician's questions, the wife went on to describe (what seemed to me) a wide variety of behavioral changes and symptomatic complaints which she attributed to her husband and seemed to connect to his
stay in the hospital. For the sake of argument, we can suppose that in this case the speaker used
a prototypic episode to associate unwarranted accusations of sexual misconduct with sexual impotence, and that her other comments Oinking impotence to hospitalization, linking her husband's back trouble to some of his current phys- ical complaints, etc.) were added in response to the clinician's demand for more information. In the absence of more data, however, it is just as plausible for us to suppose that her statements were determined by more than a single prototype or, alternatively, that all of the links have been forged in the absence of any prototype. Once again, it is the questions rather than particular answers I want to call attention to.
Prototypes and complexes are weakly accomodated to reality, their associa- tions are continually shifting per occasion, and the pre-operational thinker cannot achieve a critical understanding of how they operate or affect his conclu- sions. His theoretical knowledge (actually, his theoretical-rationalized knowledge) is non-propositional. Instead, it is characterized by congeries of prototypes and, so, his generalizations about sickness, support systems, etc., tend to have the form of conglomerated wholes. For these reasons, the conclusions which he arrives at by means of transductive reasoning and polythetic classifications
cannot be shown to be self-contradictory. The relationship between knowledge and action is particularly interesting
in this context. The operational thinker's theoretical knowledge reflects and
determines his acts, and this is one reason why it is strongly accommodated to reality. In the case of the pre-operational thinker, theoretical knowledge is sometimes inserted into action. That is to say, not only is he a conceptual realist who fails to distinguish between his concepts and mental operations and the objects and events which they organize, but he also tends to project into the real world the impact made on his mind by the symbolic associations through which he orders the world and assimilates experience.
CONCLUSIONS BEARING ON WESTERN CLINICAL PRACTICE
(1) In episodes involving acute self-limited sicknesses, where the connections between statements, action, and events seem clear cut, there is probably no reason to bother with the arguments I have raised on the preceeding pages. It is only when one moves away from episodes in which the meanings of 'efficacy'
WHEN RATIONAL MAN FALL SICK 333
and 'healing' are reasonably unambiguous that it becomes necessary to distinguish varieties of medical knowledge and reasoning.
(2) The standards of science demand operational thinking; the exigencies of clinical practice mean that physicians must sometimes reason, discourse, and act in less than operational ways. What makes a physician's clinical think- ing special are (1) the content of his theoretical knowledge, (2) the relative importance of his operational thinking, and (3) his capacity for keeping up the boundaries between his theoretical, rationalized, and negotiated knowledge of his client's sickness.
(3) Operational, boundary.maintaining thinkers and pre-operational, bound- ary-collapsing thinkers negotiate medical knowledge in different ways, i.e., by means of abstraction and syllogistic argument on the one hand, and by concretizing and emotional arousal on the other. If this is true, then research should be able to distinguish different types of clinical negotiations, including the following interactions: (1) between operational thinkers and pre-operational thinkers, (2) between operational thinkers, although not necessarily ones sharing agendas, theoretical knowledge, or equal boundary-keeping capacities, (3) between pre-operational thinkers who share prototypes and reason about them in mutually resonant ways (e.g., interactions within a family), and (4) between pre-operational thinkers who share neither prototypes nor sets of concrete associations (e.g., interactions between people of different primary groups).
ACKNOWLEDGEMENTS
I want to thank Drs. Robert Like and David Schmidt of the Case Western Reserve University Medical School for making it possible for me to observe outpatient consultations in a Family Practice clinic. I owe Dr. Like a special debt for our many discussions of these clinical sessions. Earlier versions of this paper were presented to the Dept. of Psychiatry and Behavioral Sciences of the University of Washington Medical School and the Dept. of Anthropology of Michigan State University. I am grateful to these listeners for their many helpful comments. The research leading up to this paper was partly supported by a grant from the National Science Foundation.
Case Western Reserve University Cleveland, Ohio
NOTES
1. I have tried to keep my argument concise. One of my shortcuts is a blanket reference to "medical anthropologists who study Rational Man". My reference brackets together a

334 A L L A N Y O U N G
wide variety of opinions and approaches, and I apologize for failing to distinguish the important differences among these views and their authors.
2. I tried to keep this model simple. One could reasonably add a physiological system (linked to the patterned physiological response) and sensorimotor schemes or programs (to which arrows would come from physiological and emotional systems and behavioral and expressive responses, and from which an arrow could be drawn to volition).
3. The cognitive theory of emotions is different from theories which dispense with the role of the cognitive apparatus and connect undifferentiated stimuli di:ectiy to emotional arousal and general physiological response via neuroendocrinological pathways (e.g., a general arousal theory). It is also different from theories which connect stimuli to emotional responses via unconscious drives (e.g., a psychoanalytic theory).
4. Piaget's developmental stages are more complicated than this, of course, In his scheme, the pre-operational stage is preceeded by a sensorimotor stage, and the operational stage is divided into a period during which concrete reasoning dominates, followed by a final period characterized by abstract thinking.
5. Hallpike has been criticized by several reviewers for characterizing tribal peoples as pre-operational thinkers, and for forcing the contingent, multiform, and heterogeneous path of human cognitive growth into a simplistic stage theory (see, e.g., Willis 1981). Questions can be raised about the appositeness of some of these criticisms. In any event, I am using the notions 'operational' and 'pre-operational' in a very general way, as a means of talking about cognitive proclivities, and outside the developmental and evolutionary issues on which Hallpike's critics have settled.
6. I have adapted these diagrams from Needham 1975.
B I B L I O G R A P H Y
Beck, Aaron T., A John Rush, Brian F. Shaw, and Gary Emery 1979 Cognitive Therapy of Depression. New York: Guilford Press.
Goody, Jack 1977 The Domestication of the Savage Mind. Cambridge: Cambridge Univ. Press.
Hallpike, C. R. 1979 The Foundations of Primitive Thought. Oxford: Clarendon Press.
Kleinman, Arthur 1980 Patients and Healers in the Context of Culture: An Exploration of the Borderland
Between Anthropology, Medicine, and Psychiatry. Univ. of California Press. Latour, Bruno and Steven Woolgar
1979 Laboratory Life: The Social Construction of Scientific Facts, Bererly Hills, California: Sage.
Lazarus, Richard S., Susan Folkman, and Alien Kanner 1979 Congition, Motivation, and Emotion: Putting Humpty Dumpty Together Again.
Manuscript. Lazarus, Richard S., Susan Folkman, and Allen Kanner
1980 Emotions: A Cognitive Phenomenological Analysis. In Theories of Emotions. R. Plutchnik and H. Kellerman (ed.), New York: Wiley. Pp. 66-85.
Leventhal, Howard 1980 Toward a Comprehensive Theory of Emotion. In Advances in Experimental Social
Psychology, Volume 13. L. Berkowirz, (ed.), New York: Academic Press. Needham, Rodney
1972 Belief, Language, and Experience, Chicago: Univ. of Chicago Press. Needham, Rodney
1975 Polythetic Classification: Convergence and Consequences. Man 10 (new series): 349-369.

WHEN R A T I O N A L MEN F A L L SICK 335
Olver, R. and J. Homsby 1966 On Equivalence. In Studies in Cognitive Growth. J. S. Bruner, R. Olver, and N.
Greenfield et al. (eds.), New York: Wiley. Pp. 66-85. Vygotsky, L.S.
1962 (orig. 1934) Thought and Language. Cambridge, Mass.: MIT Press. Willis, Roy
1981 Review of The Foundations of Primitive Thought, by C. R. Hallpike. Royal Anthropological Institute News number 43: 13-14.
Young, Allan 1980 The Discourse on Stress and the Reproduction of Conventional Knowledge.
Social Science and Medicine 14B: 133-146.