when delhi’s invisible citizens were noticed - manushi cholera epidemic.pdf · when delhi’s...
TRANSCRIPT
2 MANUSHI
When Delhi’s Invisible Citizens Were Noticed-The Cholera Epidemic
by Madhu KishwarPhotos by Sue Darlow
Following three years of successivedrought, we at last had a good monsoonthis year. Even before people could heavea sigh of relief, they were confronted with anew set of problems. Cholera, which in largeparts of the world is considered a diseaseof bygone centuries, appeared in epidemicform in many cities. This report is on Delhialone, but hundreds have died in other citiestoo.
For weeks, while hundreds were dyingand thousands more lay grievously ill inhospitals and homes, governmentauthorities kept denying that this was acholera epidemic. They sought to give theimpression that this was nothing more thanthe usual seasonal outbreak of hepatitis andgastroenteritis, slightly accentuatedbecause of the heavy monsoon.
Up to August 25, the governmentadmitted that 304 deaths had occurred inthe epidemic in Delhi; 1,257 people had beenconfirmed as having cholera; 8,525 peoplehad been hospitalised in Delhi; and thenumber of gastroenteritis cases was 32,646.The actual figures are likely to be muchhigher. All these deaths could easily havebeen prevented, had the administration’sresponse to the situation been less inept.
The slums and resettlement colonieswere the worst hit by the cholera epidemicthis year, as they are by most other disasters,natural or manmade. Delhi has about 45resettlement colonies, including slums. Inaddition, there are several small clusters ofhutments which do not enter into officialstatistics. Of the city’s total population ofabout 8,100,000, more than half live in thesevarious residential settlements.
Most of the inhabitants of slums and
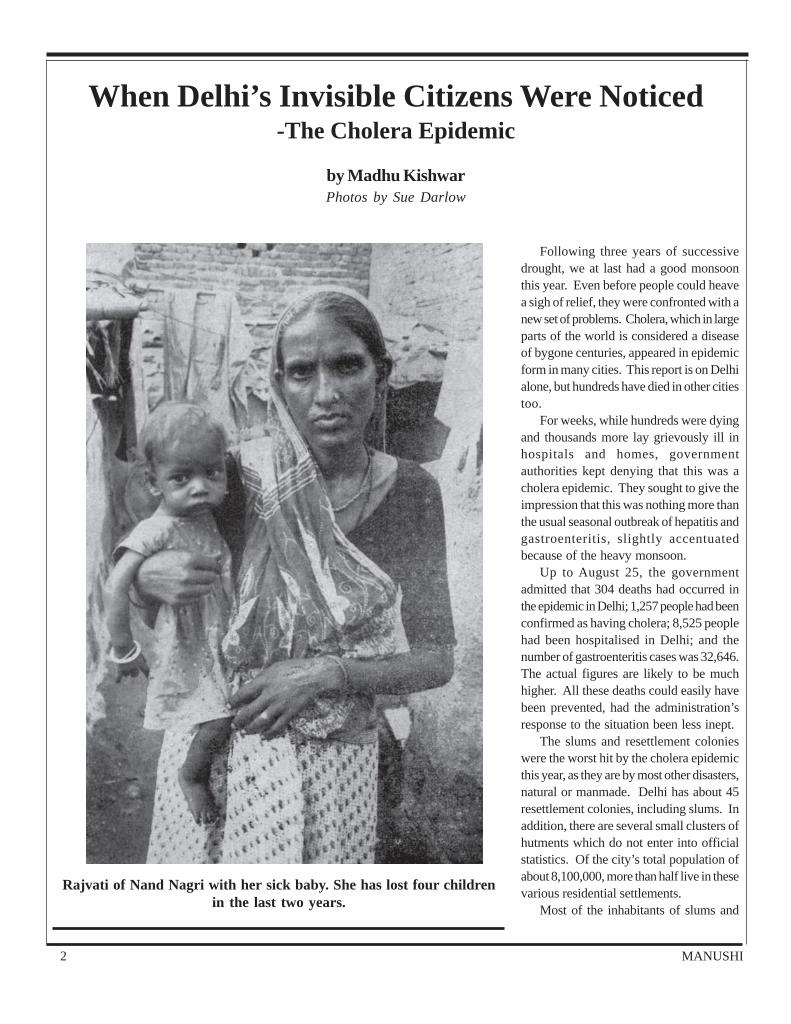
Rajvati of Nand Nagri with her sick baby. She has lost four childrenin the last two years.

No.47July-August 1988
resettlement colonies are relatively recentmigrants to the city, who came here in searchof employment. The poorer migrants haveno option but to construct little huts onneglected pieces of land, on the edges ofthe big storm-water drains and railwaytracks, near swamps, and even onpavements in the heart of the city. Mostmigrants come from their villages in groupsfrom one community, and tend to settle insmall community based clusters. Every nowand then, the city administration, in itsattempt to “beautify” the city, usesbulldozers and police force to demolish thesettlements. The migrants either return andrebuild their huts at the same site or moveon to another miserable site, where theyhope to escape attention for a while.
At times, it pleases the administrationto allot alternative pieces of land on theoutskirts of the city to those whom ituproots. These are known as resettlementcolonies. The biggest slum clearance andresettlement operations were undertakenduring the Emergency, 1975-1977. Theprocess had started earlier and continuestoday, as thousands continue to seekshelter in the islands of affluence andemployment that cities like Delhi represent.
The government disowns responsibilityfor providing services to the unauthorisedor unregularised parts of Delhi, and blamesthe inhabitants for the unsanitaryconditions prevailing there. However, livingconditions in the official resettlementcolonies are not much better.
On July 22, the prime minister made avisit, high profile even by his standards, tosome of the affected colonies in Delhi.Perhaps this was his first exposure to thecapital’s slums, for he appeared to be
was forced to resign and was replaced byanother bird of the same feather.
A Manushi team visited some of theaffected areas in Delhi at the end of Julyand in early August. We began withcolonies which had received publicity dueto the prime minister’s visit, and then wenton to some of those that lay totally forgottenbecause no VIP had cared to visit them.
The Living NightmareConditions in most areas were still
nightmarish. In “normal” times, the roadsand lanes in these areas are in an unsanitarycondition, full of potholes and puddles.Since these areas do not have sanitationfacilities, open gutters run on both sides ofeach lane and are usually full of stagnantwater, excrement and household rubbish,solid and liquid. Due to the heavy rains, allthe drains had overflowed and most areaswere ankle-deep in slush and water. Theresidents’ homes open strait on to theselanes, with no open courtyard and oftennot even a couple of stairs in between.
The houses are constructed in solidblocks with no space in between them.Therefore, the only ventilation available isthrough a small ventilator cum window inthe front of each house which opens ontothe filthy streets. Most plots in resettlementcolonies are 22 to 25 square yards in area.This allows for the construction of no morethan one and a half very small rooms -- thefront portion used as a kitchen cum entrancecum work space, and the back room themain living and sleeping space. No matter
shocked. In characteristic style, he scoldeda few officials and ordered “urgent”measures to check the spread of thedisease.. To prove that the prime ministermeant business, the lieutenant governor
A typical water source—ahandpump on the edge of a
sewage filled gutter
Living on the BrinkDelhi slums (that is, hutment clusters) are divided into the “regularised” and the “unregularised.” Slums get regularised only
when powerful political bosses, whom the slumdwellers treat as godfathers, decide to intervene. Unregularised colonies can bedemolished at any time. The bosses tend to delay and obstruct the regularisation process because they are afraid that once a colonyis regularised they cannot continue to use the threat of demolition to keep the residents as a captive vote bank. Also, the residentsmight begin to demand amenities as a right rather than as a favour.
Delhi colonies (where the houses are concrete structures) are divided into the “authorised” and the “unauthorised.” DelhiAdministration has a virtual monopoly over the purchase and sale of land in Delhi, and also over the right to acquire land in adjoiningvillages for absorption into the city. This monopoly has created an artificial scarcity of land and pushed prices artificially high -- wellbeyond the reach of even the middle classes. However, land dealers, in collusion with bureaucrats and politicians, continue to sellland in areas where urban construction is not authorised. After construction takes place, the colonies are considered “unauthorised.”“Authorisation” cannot be obtained by following any set procedures. It can be attained only if residents are able to purchase thefavour of powerful politicians.
4 MANUSHI
how neatly maintained, the back roomremains dark and dingy because it has noinlet for light or air.
None of these houses have any spacefor the construction of a bathroom or latrine.In officially authorised resettlementcolonies, public latrines have been at leastnominally provided. They cannot be usedby children and most adults find themunusable because of the lack ofmaintenance, and consequentaccumulation of filth. Children relievethemselves in the open gutters that borderthe houses. Sometimes, even adults mayuse the gutters. These gutters stink andbreed vermin, and are rarely given athorough cleaning. In the “unauthorised”colonies, there is not even a pretence ofpublic facilities.
In resettlement colonies each block ofhouses is supposed to have a block oflatrines for its use. But their number ishopelessly inadequate, given the numberof families whom they are supposed toserve. For instance, D and E blocks of NandNagri have 56 latrines between them. E blockhas 444 plots and 256 unauthorisedhutments. D block has 343 plots, that is, aminimum of 1,043 families or 5,215 peopleusing them every day -- if one were tocalculate at the rate of five persons a family,there would be one latrine per 93 users.
The lieutenant governor recentlyannounced that the government would
provide one latrine for every 45 families. Ofcourse, they would not include the adjacenthutment dwellers in this calculation sincethe latter are not “authorised” to exist. Butgiven that they end up using the latrineanyway, the “one latrine per 45 families”formula will not be any improvement.
These latrines have no flush system,not even a water tap, in them. The residentsare supposed to carry their own pitcher ofwater both for cleaning themselves as well
as for flushing the excrement down. Acouple of handpumps are installed outsidethe latrine complex. The latrines aresupposed to be fitted with septic tankswhereby the liquid part of the excrement issupposed to seep down into the earth afterautomatic bacterial action -- and only thesolid part remain in the tank which issupposed to be cleaned periodically. Aseptic tank in a private house catering toone or two families might not need morethan an annual cleaning, maybe even less.However, given that these public latrineshave to cater to a disproportionately largenumber of families, they need far moreregular cleaning. In addition, like mostgovernment buildings, they are very poorlyconstructed -- not just in matters of designbut also in the quality of material used.
The pots are in a broken down conditionand full of cracks. Most of them do noteven have footrests. Since the latrines donot have any water supply, the pots areusually filled to the top with excrement.Residents complained of, and we acuallysaw, worms crawling in and out of the cracksin the pots and gutters underneath -- thisnearly a fortnight after a massive cleaningcampaign had been ordered.
The latrines are usually enclosed bybrick walls. As the latrines get dirtier,people, especially children, start using thearea around as well, so that one has to steerone’s way though piles of excrement in
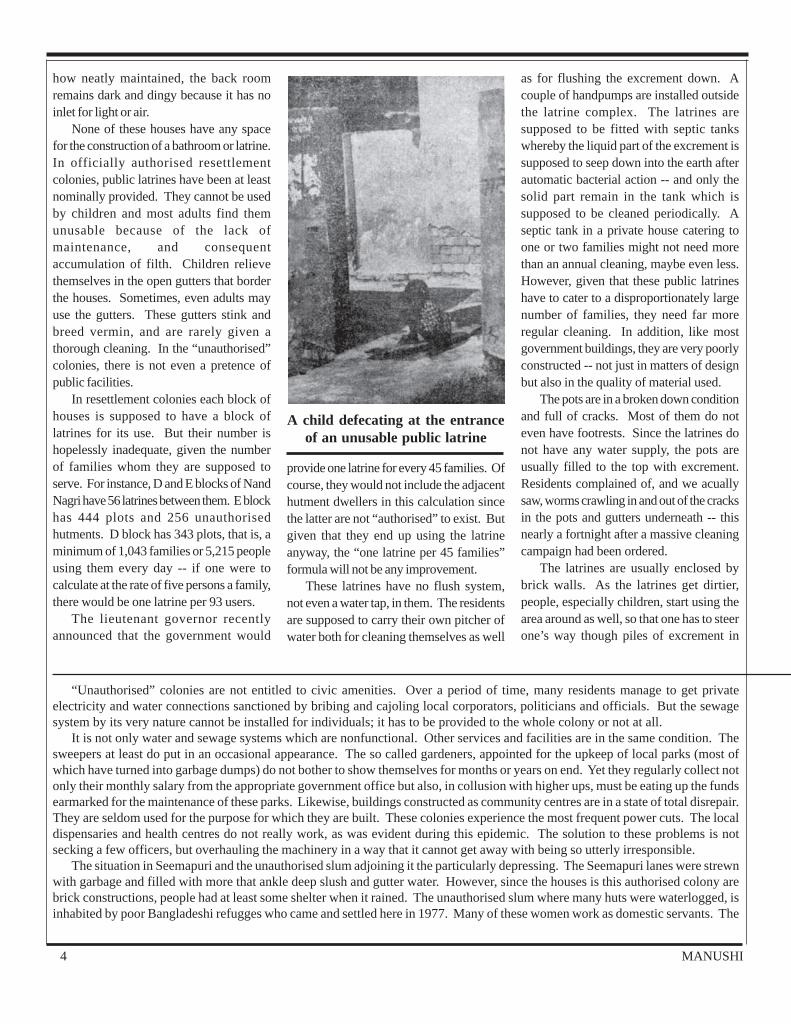
A child defecating at the entranceof an unusable public latrine
“Unauthorised” colonies are not entitled to civic amenities. Over a period of time, many residents manage to get privateelectricity and water connections sanctioned by bribing and cajoling local corporators, politicians and officials. But the sewagesystem by its very nature cannot be installed for individuals; it has to be provided to the whole colony or not at all.
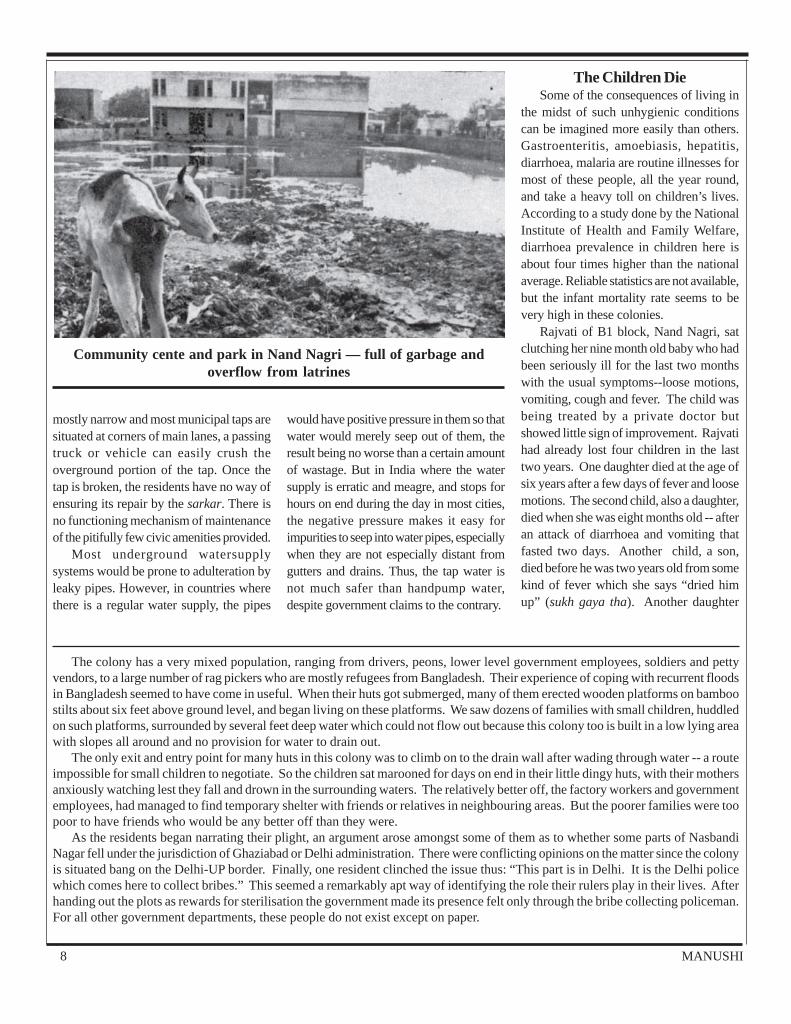
It is not only water and sewage systems which are nonfunctional. Other services and facilities are in the same condition. Thesweepers at least do put in an occasional appearance. The so called gardeners, appointed for the upkeep of local parks (most ofwhich have turned into garbage dumps) do not bother to show themselves for months or years on end. Yet they regularly collect notonly their monthly salary from the appropriate government office but also, in collusion with higher ups, must be eating up the fundsearmarked for the maintenance of these parks. Likewise, buildings constructed as community centres are in a state of total disrepair.They are seldom used for the purpose for which they are built. These colonies experience the most frequent power cuts. The localdispensaries and health centres do not really work, as was evident during this epidemic. The solution to these problems is notsecking a few officers, but overhauling the machinery in a way that it cannot get away with being so utterly irresponsible.
The situation in Seemapuri and the unauthorised slum adjoining it the particularly depressing. The Seemapuri lanes were strewnwith garbage and filled with more that ankle deep slush and gutter water. However, since the houses is this authorised colony arebrick constructions, people had at least some shelter when it rained. The unauthorised slum where many huts were waterlogged, isinhabited by poor Bangladeshi refugges who came and settled here in 1977. Many of these women work as domestic servants. The
No.47July-August 1988
order to reach the latrine. The stench fromthe latrine blocks is overpowering.
How did they manage to use the latrineswhich were overflowing with excrementmost of the time, we asked again and again.The answer people gave was simple. “Ifwe were in villages we could have gone tothe fields. Where is the place here? Andeven if there is, men might use it. It isimpossible for women to do so becausethere are no secluded spots available.” Acommon refrain: “We feel so sick after avisit to the latrines that we cannot eat ordrink a long while after that.”
The government appointed sweepersare supposed to clean the latrines once ortwice a day -- nobody seems to be sure ofthe frequency, probably because it variesaccording to the mood of sweepers. Thesweepers usually carry nothing more thana bucket of mashk and a broom for the dailycleaning operation. The residents uniformlycomplained that the sweepers did no morethan throw a little water down the potsleaving the latrines wet and messy after theso called cleaning operation.
Most latrines are constructed right inthe centre of the colonies, with very littledistance separating them from the houses,and from public places. Since the septictanks are overloaded and poorlyconstructed, excremental water consistentlyflows out of them into the open spacesaround the latrines. In Nand Nagri one set
of latrines emptied its filth out into what issupposed to be a public park with adilapidated building in its midst which issupposedly the community centre. Whenwe visited this area we found the park andall the open space around the latrines filledwith ankle-deep excrement filled water sothat the building was totally inaccessible.
In another block of Nand Nagri, thelatrine complex wall was a mere seven feetaway from a facing row of houses so that
the excrement flowed right at theirdoorsteps.
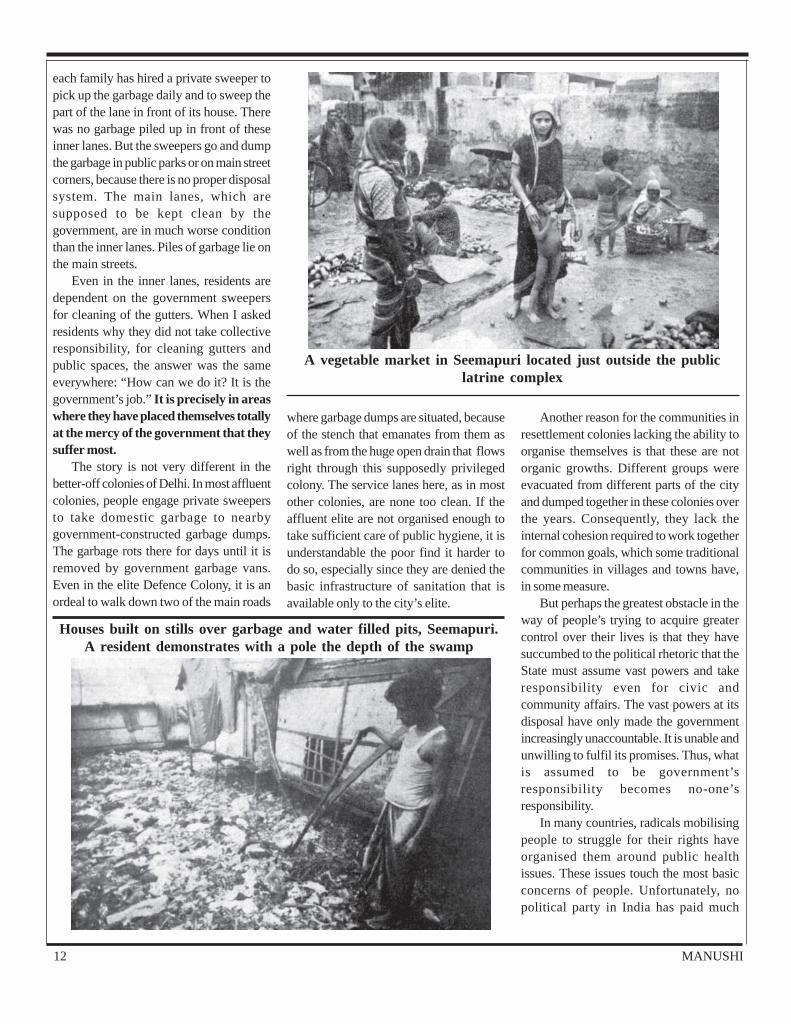
In Seemapuri, the mucky water flowedinto an open space which serves as avegetable market for local residents. Thevendors had no platforms or carts. Theydisplayed their vegetables on the ground.The open gutters outside people’s homesare also full of the overflow of water fromlatrines. The situation is particularlypathetic during the rainy season when, due
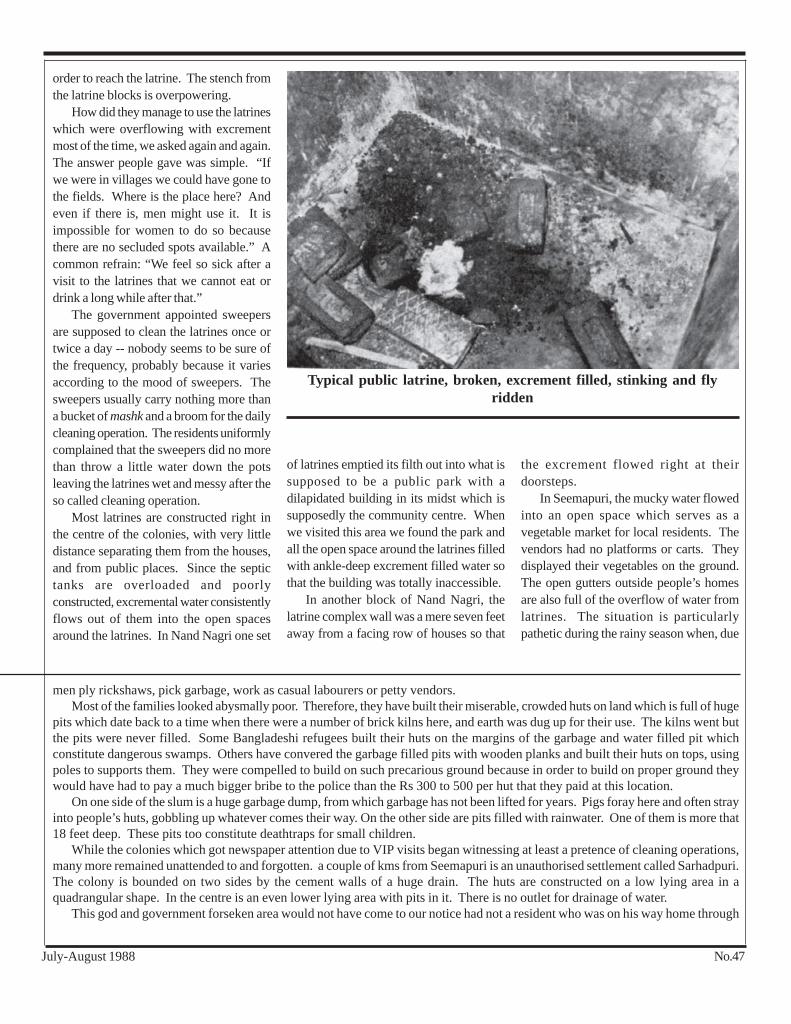
Typical public latrine, broken, excrement filled, stinking and flyridden
men ply rickshaws, pick garbage, work as casual labourers or petty vendors.Most of the families looked abysmally poor. Therefore, they have built their miserable, crowded huts on land which is full of huge
pits which date back to a time when there were a number of brick kilns here, and earth was dug up for their use. The kilns went butthe pits were never filled. Some Bangladeshi refugees built their huts on the margins of the garbage and water filled pit whichconstitute dangerous swamps. Others have convered the garbage filled pits with wooden planks and built their huts on tops, usingpoles to supports them. They were compelled to build on such precarious ground because in order to build on proper ground theywould have had to pay a much bigger bribe to the police than the Rs 300 to 500 per hut that they paid at this location.
On one side of the slum is a huge garbage dump, from which garbage has not been lifted for years. Pigs foray here and often strayinto people’s huts, gobbling up whatever comes their way. On the other side are pits filled with rainwater. One of them is more that18 feet deep. These pits too constitute deathtraps for small children.
While the colonies which got newspaper attention due to VIP visits began witnessing at least a pretence of cleaning operations,many more remained unattended to and forgotten. a couple of kms from Seemapuri is an unauthorised settlement called Sarhadpuri.The colony is bounded on two sides by the cement walls of a huge drain. The huts are constructed on a low lying area in aquadrangular shape. In the centre is an even lower lying area with pits in it. There is no outlet for drainage of water.
This god and government forseken area would not have come to our notice had not a resident who was on his way home through
6 MANUSHI
to absence of proper drainage, the lanesand open spaces get filled with ankle-deepor even knee deep water. At such times thegutter water gets mixed with rain water andoverflows into the houses.
At all events, adults and children haveto wade through this filthy water wheneverthey step out of their houses. The residentsalleged that even though some money wasallotted in 1976 for construction of propersewers, none of this was used for thispurpose. In many colonies, sewers weredug before the last elections. There aremany open manholes as evidence of thework abandoned halfway as soon as theelections were over. Many of the opengutters are more than five feet deep andabout four feet wide. Residents call these“Bacha doob nale” (gutters for drowningchildren). Quite a few instances were citedof small children falling into these gutters.While some were lucky enough to berescued, deaths of children by drowning inthese gutters and big pools of dirty, stagnantwater are not an uncommon occurrence inthese colonies.
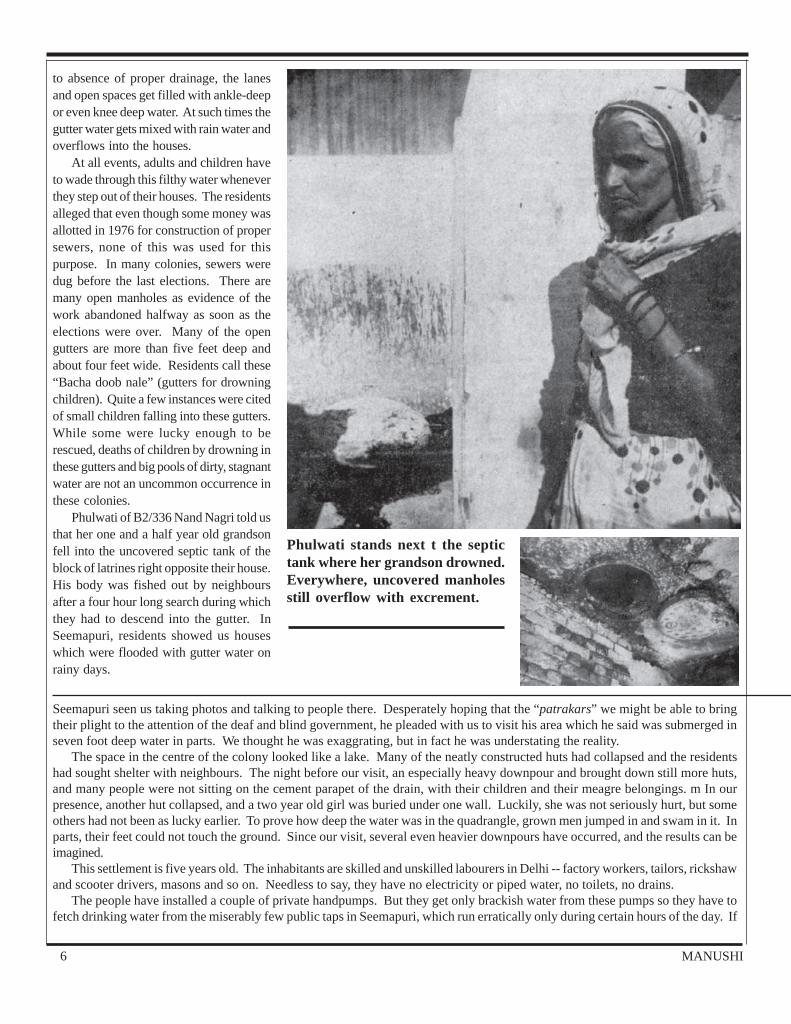
Phulwati of B2/336 Nand Nagri told usthat her one and a half year old grandsonfell into the uncovered septic tank of theblock of latrines right opposite their house.His body was fished out by neighboursafter a four hour long search during whichthey had to descend into the gutter. InSeemapuri, residents showed us houseswhich were flooded with gutter water onrainy days.
Phulwati stands next t the septictank where her grandson drowned.Everywhere, uncovered manholesstill overflow with excrement.
Seemapuri seen us taking photos and talking to people there. Desperately hoping that the “patrakars” we might be able to bringtheir plight to the attention of the deaf and blind government, he pleaded with us to visit his area which he said was submerged inseven foot deep water in parts. We thought he was exaggrating, but in fact he was understating the reality.
The space in the centre of the colony looked like a lake. Many of the neatly constructed huts had collapsed and the residentshad sought shelter with neighbours. The night before our visit, an especially heavy downpour and brought down still more huts,and many people were not sitting on the cement parapet of the drain, with their children and their meagre belongings. m In ourpresence, another hut collapsed, and a two year old girl was buried under one wall. Luckily, she was not seriously hurt, but someothers had not been as lucky earlier. To prove how deep the water was in the quadrangle, grown men jumped in and swam in it. Inparts, their feet could not touch the ground. Since our visit, several even heavier downpours have occurred, and the results can beimagined.
This settlement is five years old. The inhabitants are skilled and unskilled labourers in Delhi -- factory workers, tailors, rickshawand scooter drivers, masons and so on. Needless to say, they have no electricity or piped water, no toilets, no drains.
The people have installed a couple of private handpumps. But they get only brackish water from these pumps so they have tofetch drinking water from the miserably few public taps in Seemapuri, which run erratically only during certain hours of the day. If

No.47July-August 1988
Waters of DeathAccording to one estimate, over one
third of Delhi’s population has to use publicplaces and roadside gutters to easethemselves. More than half of Delhi’spopulation has no sewage facility. Thesewage treatment capacity of the plants inDelhi is about half of what is required. Theremaining half of the sewage is left to flowthrough open drains which empty into theYamuna. This river is a major source ofwater supply to many parts of Delhi and toother cities downstream. Its water has, thus,become a major health hazard. No wonderthat cholera deaths have been reported fromseveral north Indian cities this summer.
These slums and colonies do not havepiped water supply in the houses. Theauthorised colonies have a few public tapswhich bring piped water supplied by themunicipal corporation during certain hoursof the day. Most of the water needs of theresidents are met from handpumps - mostlyprivately dug and some dug by thegovernment. The latter were installed in agreat hurry in the pre-election period.Almost all of them are extremely shallow.
What makes the water sources lethal isthat the handpumps are situated bang nextto the open gutters. Even under normalconditions, some amount of sewage wateris bound to seep into these drinking watersources. But during the rainy season,especially after a heavy monsoon, it isimpossible to separate the one from theother. The excremental water flows on to
the sides and the top of the handpumpswhich are no more than three feet high.When the lanes fill with several feet of rainwater mixed with sewage, the handpumpsare partially submerged. The residentsshowed us worms coming out as they drewwater from these pumps.
The administration tried to make outthat these handpumps were the real culprits
for the severe outbreak of disease and thatpeople would be safe if they drank watersupplied by the municipal taps. Theadvertisements inserted in newspapers bythe municipal corporation of Delhi as partof its whitewash exercise loudlywarned:”Water drawn from sources otherthan municipal water supply should beboiled before drinking.” This is quitemisleading. The municipal taps are not muchsafer, given the way they are installed.
In all the colonies we visited, we foundthat the water taps, like the handpumps, areusually no more than a foot above groundlevel and often are placed in a small cementenclosure which opens into the gutter.When these gutters overflow, the water fillsup the cement enclosure around the tap.All the taps we saw had their faucetsmissing. In some cases, even the one-foot-high overground pipe was missing. In suchsituations, the tap was no more than a feeblefountain coming from a few inches belowroad level - surrounded by gutter water.Residents had fixed small plastic pipes todraw out the water. Women using these tapsshowed how they first had to drain out thegutter water with mugs from theseenclosures and then draw out what theycan from the tap.
How and why did the faucets of thetaps break? The residents told us that somebroke because they were made of poorquality material, and others were stolen bymiscreants. A number of them were crushedby passing vehicles. Since these lanes are
Broken watertap, faucet belowsewage water level, situated nextto latrine and gutter. Dinking wa-ter is obtained through a hose con-nected to the faucet.
they manage to get to the tap on time they get some water, but if they are too far back in the queue, they have to return emptyhanded.Shahadat Ali, who works as a tailor in a shop in Delhi, said he had been running around for the last one week from one government
office to another, requesting that they drin out the water with a motor pump, since there is no outlet for the water the flow away. Withgreat difficulty, after pleading for days on end, he managed to persuade them to send a pump. The man who came to operate it workedfor an hour, and then disappeared, saying the pump needed repair.
Shahhadat Ali, who earns Rs 20 to 25 a day as a daily wage worker, had not been able to go to work for the last six days. He, hiswife and four children may soon starve, for they have no other source of income. The children were sitting huddled on a pile ofbroken bricks in the midst of water, as though on an island. Their hut had collapsed a couple of days ago. Their mother sat on theparapet of the drain, grinding spices for the evening meal. At the very least, it will cost each family about Rs 2,000 to 3,000 to rebuilda hut, pushing many a family into debt.
The neighbouring Rajiv Colony, better known as Nasbandi Nagar, was in even worse shape, even though it is an officiallysponsored and authorised colony. Most of the houses lay submerged in water. The brick houses of the relatively better off familieswere less in danger of collapse than the mud and bamboo huts.
8 MANUSHI
mostly narrow and most municipal taps aresituated at corners of main lanes, a passingtruck or vehicle can easily crush theoverground portion of the tap. Once thetap is broken, the residents have no way ofensuring its repair by the sarkar. There isno functioning mechanism of maintenanceof the pitifully few civic amenities provided.
Most underground watersupplysystems would be prone to adulteration byleaky pipes. However, in countries wherethere is a regular water supply, the pipes
would have positive pressure in them so thatwater would merely seep out of them, theresult being no worse than a certain amountof wastage. But in India where the watersupply is erratic and meagre, and stops forhours on end during the day in most cities,the negative pressure makes it easy forimpurities to seep into water pipes, especiallywhen they are not especially distant fromgutters and drains. Thus, the tap water isnot much safer than handpump water,despite government claims to the contrary.
The Children DieSome of the consequences of living in
the midst of such unhygienic conditionscan be imagined more easily than others.Gastroenteritis, amoebiasis, hepatitis,diarrhoea, malaria are routine illnesses formost of these people, all the year round,and take a heavy toll on children’s lives.According to a study done by the NationalInstitute of Health and Family Welfare,diarrhoea prevalence in children here isabout four times higher than the nationalaverage. Reliable statistics are not available,but the infant mortality rate seems to bevery high in these colonies.
Rajvati of B1 block, Nand Nagri, satclutching her nine month old baby who hadbeen seriously ill for the last two monthswith the usual symptoms--loose motions,vomiting, cough and fever. The child wasbeing treated by a private doctor butshowed little sign of improvement. Rajvatihad already lost four children in the lasttwo years. One daughter died at the age ofsix years after a few days of fever and loosemotions. The second child, also a daughter,died when she was eight months old -- afteran attack of diarrhoea and vomiting thatfasted two days. Another child, a son,died before he was two years old from somekind of fever which she says “dried himup” (sukh gaya tha). Another daughter
Community cente and park in Nand Nagri — full of garbage andoverflow from latrines
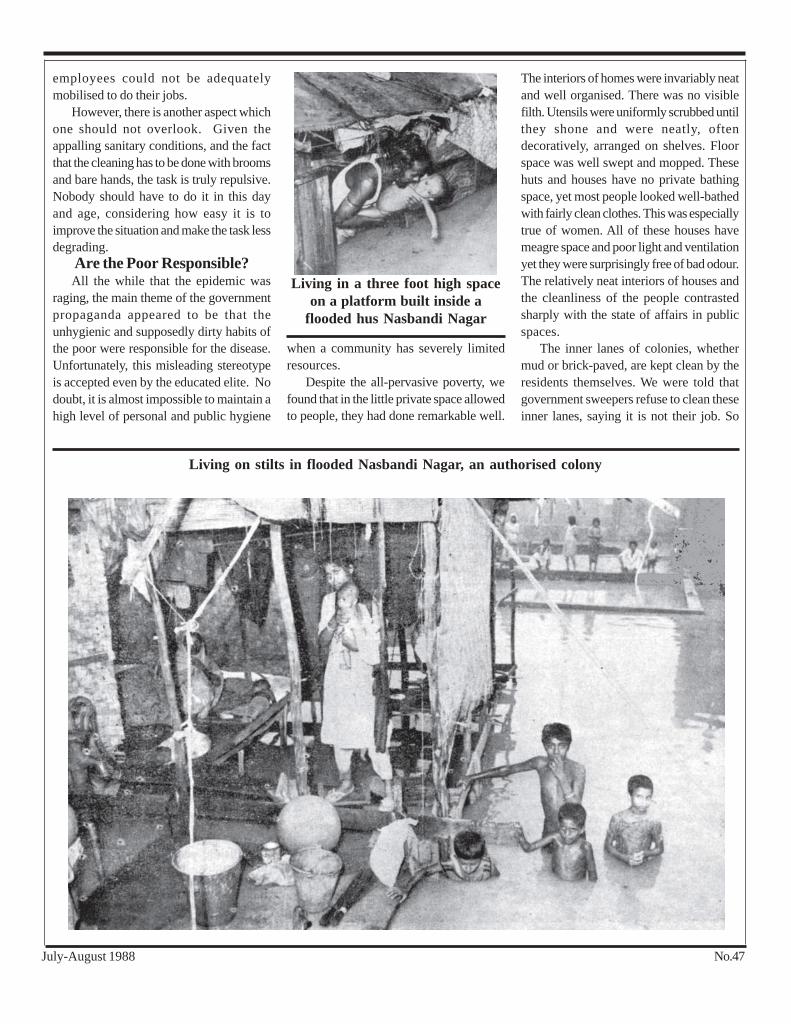
The colony has a very mixed population, ranging from drivers, peons, lower level government employees, soldiers and pettyvendors, to a large number of rag pickers who are mostly refugees from Bangladesh. Their experience of coping with recurrent floodsin Bangladesh seemed to have come in useful. When their huts got submerged, many of them erected wooden platforms on bamboostilts about six feet above ground level, and began living on these platforms. We saw dozens of families with small children, huddledon such platforms, surrounded by several feet deep water which could not flow out because this colony too is built in a low lying areawith slopes all around and no provision for water to drain out.
The only exit and entry point for many huts in this colony was to climb on to the drain wall after wading through water -- a routeimpossible for small children to negotiate. So the children sat marooned for days on end in their little dingy huts, with their mothersanxiously watching lest they fall and drown in the surrounding waters. The relatively better off, the factory workers and governmentemployees, had managed to find temporary shelter with friends or relatives in neighbouring areas. But the poorer families were toopoor to have friends who would be any better off than they were.
As the residents began narrating their plight, an argument arose amongst some of them as to whether some parts of NasbandiNagar fell under the jurisdiction of Ghaziabad or Delhi administration. There were conflicting opinions on the matter since the colonyis situated bang on the Delhi-UP border. Finally, one resident clinched the issue thus: “This part is in Delhi. It is the Delhi policewhich comes here to collect bribes.” This seemed a remarkably apt way of identifying the role their rulers play in their lives. Afterhanding out the plots as rewards for sterilisation the government made its presence felt only through the bribe collecting policeman.For all other government departments, these people do not exist except on paper.
No.47July-August 1988
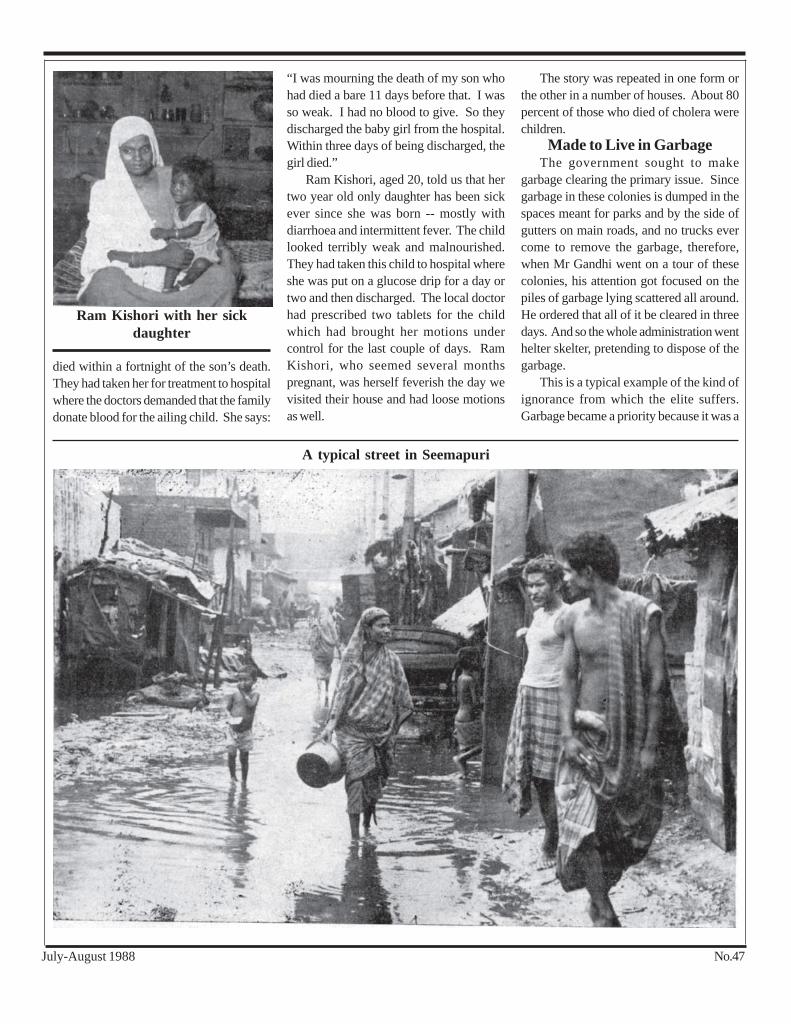
died within a fortnight of the son’s death.They had taken her for treatment to hospitalwhere the doctors demanded that the familydonate blood for the ailing child. She says:
“I was mourning the death of my son whohad died a bare 11 days before that. I wasso weak. I had no blood to give. So theydischarged the baby girl from the hospital.Within three days of being discharged, thegirl died.”
Ram Kishori, aged 20, told us that hertwo year old only daughter has been sickever since she was born -- mostly withdiarrhoea and intermittent fever. The childlooked terribly weak and malnourished.They had taken this child to hospital whereshe was put on a glucose drip for a day ortwo and then discharged. The local doctorhad prescribed two tablets for the childwhich had brought her motions undercontrol for the last couple of days. RamKishori, who seemed several monthspregnant, was herself feverish the day wevisited their house and had loose motionsas well.
The story was repeated in one form orthe other in a number of houses. About 80percent of those who died of cholera werechildren.
Made to Live in GarbageThe government sought to make
garbage clearing the primary issue. Sincegarbage in these colonies is dumped in thespaces meant for parks and by the side ofgutters on main roads, and no trucks evercome to remove the garbage, therefore,when Mr Gandhi went on a tour of thesecolonies, his attention got focused on thepiles of garbage lying scattered all around.He ordered that all of it be cleared in threedays. And so the whole administration wenthelter skelter, pretending to dispose of thegarbage.
This is a typical example of the kind ofignorance from which the elite suffers.Garbage became a priority because it was a
A typical street in Seemapuri
Ram Kishori with her sickdaughter

10 MANUSHI
visible eyesore. And the elite do not wanttheir cities to have visible eyesores. Certainmore important measures that would havehelped combat the spread of cholera werebypassed in favour of cosmetic cleaning.
to have been hired to lift it out of coloniesand dump it elsewhere. The residents werecynical about this too. A common response:“This gives the corrupt bosses anopportunity to make some more money.Hundreds of trucks are being hired to makeso many trips per day. Most of these tripswill be on paper. A few trucks will make afew trips, and the rest of the money will bepocketed by the bosses.” This may not bean exaggerated allegation, given that 10 to15 days after the launching of an intensivegarbage removal drive, we found piles ofgarbage lying around, just as before, inevery affected colony we visited.
The attempts to clean the gutters wereequally farcical in most places we visited.Since the gutters are not cleaned regularly,they tend to get stagnant due toaccumulation of silt and other solid matter.This prevents water from flowing easily.When the cleaning drive began, thegovernment sweepers took out the filth andpiled it up at intervals of a few feet, at theedge of the gutters, even right next to thetaps. We were shown a number of suchheaps which had not been cleared for thelast few weeks, thus posing a greater healthhazard than had it stayed in the gutter,because now the rain water just carried itout over the streets and lanes.
Nobody asked and nobody explainedwhy the administration had to hire so manycasual workers to carry out the cleaningoperations. Why could the regular staffnot have been deployed for it? Theyresidents, of course, had their ownexplanation. They alleged that the
Government “cleaning—takinggarbage out of gutters and
leaving it on the streets
Given that cholera spreads from humanexcrement rather than garbage, it wascrucial to disinfect and dispose of theexcrement of cholera victims in particularand of the population in general. All theadministration needed to do was to dig pitsin which the excrement could be depositedand covered with lime or bleaching powder.If they had invested all the available humanpower in this job, the epidemic could havebeen controlled much sooner. Instead, theywent around pretending they were clearingthe accumulated garbage.
And how was this garbage disposedof? In some cases, we saw it just beingspread out more evenly in parks and thenflattened out by road rollers, or depositedin an open ground a little distance away. Ofcourse, hundreds of trucks were supposed
“Bacha doob nalas” run at thedoorstep in Seemapur—death
traps for tiny children
Interior of a house in Nand Nagri—typically neat and clean
government- employed sweepers and otherstaff are able to get away with not doingtheir routine work, by giving regular bribesto the supervisory staff. The bribes seemedto have more power than the primeminister’s directive. Even during thisemergency, we were told, the regular
No.47July-August 1988
employees could not be adequatelymobilised to do their jobs.
However, there is another aspect whichone should not overlook. Given theappalling sanitary conditions, and the factthat the cleaning has to be done with broomsand bare hands, the task is truly repulsive.Nobody should have to do it in this dayand age, considering how easy it is toimprove the situation and make the task lessdegrading.
Are the Poor Responsible?All the while that the epidemic was
raging, the main theme of the governmentpropaganda appeared to be that theunhygienic and supposedly dirty habits ofthe poor were responsible for the disease.Unfortunately, this misleading stereotypeis accepted even by the educated elite. Nodoubt, it is almost impossible to maintain ahigh level of personal and public hygiene
when a community has severely limitedresources.
Despite the all-pervasive poverty, wefound that in the little private space allowedto people, they had done remarkable well.
The interiors of homes were invariably neatand well organised. There was no visiblefilth. Utensils were uniformly scrubbed untilthey shone and were neatly, oftendecoratively, arranged on shelves. Floorspace was well swept and mopped. Thesehuts and houses have no private bathingspace, yet most people looked well-bathedwith fairly clean clothes. This was especiallytrue of women. All of these houses havemeagre space and poor light and ventilationyet they were surprisingly free of bad odour.The relatively neat interiors of houses andthe cleanliness of the people contrastedsharply with the state of affairs in publicspaces.
The inner lanes of colonies, whethermud or brick-paved, are kept clean by theresidents themselves. We were told thatgovernment sweepers refuse to clean theseinner lanes, saying it is not their job. So
Living in a three foot high spaceon a platform built inside a
flooded hus Nasbandi Nagar
Living on stilts in flooded Nasbandi Nagar, an authorised colony
12 MANUSHI
each family has hired a private sweeper topick up the garbage daily and to sweep thepart of the lane in front of its house. Therewas no garbage piled up in front of theseinner lanes. But the sweepers go and dumpthe garbage in public parks or on main streetcorners, because there is no proper disposalsystem. The main lanes, which aresupposed to be kept clean by thegovernment, are in much worse conditionthan the inner lanes. Piles of garbage lie onthe main streets.
Even in the inner lanes, residents aredependent on the government sweepersfor cleaning of the gutters. When I askedresidents why they did not take collectiveresponsibility, for cleaning gutters andpublic spaces, the answer was the sameeverywhere: “How can we do it? It is thegovernment’s job.” It is precisely in areaswhere they have placed themselves totallyat the mercy of the government that theysuffer most.
The story is not very different in thebetter-off colonies of Delhi. In most affluentcolonies, people engage private sweepersto take domestic garbage to nearbygovernment-constructed garbage dumps.The garbage rots there for days until it isremoved by government garbage vans.Even in the elite Defence Colony, it is anordeal to walk down two of the main roads
where garbage dumps are situated, becauseof the stench that emanates from them aswell as from the huge open drain that flowsright through this supposedly privilegedcolony. The service lanes here, as in mostother colonies, are none too clean. If theaffluent elite are not organised enough totake sufficient care of public hygiene, it isunderstandable the poor find it harder todo so, especially since they are denied thebasic infrastructure of sanitation that isavailable only to the city’s elite.
Another reason for the communities inresettlement colonies lacking the ability toorganise themselves is that these are notorganic growths. Different groups wereevacuated from different parts of the cityand dumped together in these colonies overthe years. Consequently, they lack theinternal cohesion required to work togetherfor common goals, which some traditionalcommunities in villages and towns have,in some measure.
But perhaps the greatest obstacle in theway of people’s trying to acquire greatercontrol over their lives is that they havesuccumbed to the political rhetoric that theState must assume vast powers and takeresponsibility even for civic andcommunity affairs. The vast powers at itsdisposal have only made the governmentincreasingly unaccountable. It is unable andunwilling to fulfil its promises. Thus, whatis assumed to be government’sresponsibility becomes no-one’sresponsibility.
In many countries, radicals mobilisingpeople to struggle for their rights haveorganised them around public healthissues. These issues touch the most basicconcerns of people. Unfortunately, nopolitical party in India has paid much
A vegetable market in Seemapuri located just outside the publiclatrine complex
Houses built on stills over garbage and water filled pits, Seemapuri.A resident demonstrates with a pole the depth of the swamp
No.47July-August 1988
attention to this issue. This was evidentduring this epidemic too. Every partydutifully passes resolutions and issuedpress statements condemning thegovernment. Some even went through theritual of organising protest demonstrations.These actions only served to strengthenthe foundations of our “Petition Raj”, asthey all ended in the presentation ofmemoranda to government officials.
The Bharatiya Janata Party, which hasa solid mass base in Delhi, organised somehealth camps but clearly more for publicitythan as a serious attempt to control theepidemic. The camps functioned on thelines of government dispensaries - injectinganti-cholera vaccine and distributingmedicines. No attempt was made to launchan awareness campaign. Nor did anyone,not even those who swear by mass politics,think of mobilizing the affected communitiesto shake off some of their cripplingdependence on a callous governmentmachinery, and make a beginning incommunity-based sanitation drives.
The Medical AspectIt is shameful that cholera occurred at
all. Even more shameful is the fact that aneasily preventable and controllable diseasewas allowed to assume epidemicproportions. This happened primarilybecause the administration ignored all priorwarnings by health institution that such anoutbreak was imminent. No preventivemeasures were taken. Doctors in certainhospitals have alleged that even when theybegan to report the first cholera cases, thegovernment paid no heed. If, at that earlystage, the first cases had been isolated andurgent action taken to ensure that thebacteria did not spread, the situation couldhave been brought under control.
Instead, the government indulged in acynical debating match, trying to convincethe public that this was no more than the“outburst of a seasonal disease, now wellunder control.” This is a quotation fromthe statement of the honourable municipalcommissioner on July 20. It is hard tounderstand why the government found itnecessary to start a controversy about
A couple in Guru Tegh Bahadur hospital with their dangerously illbaby
whether or not the disease was cholera. Thediagnosis is simple and inexpensive -- thecausative organism vibriocholeraeserogroup 01 ogava, is isolated from rectalswabs or fresh stools and grown in cultures.This technique, known for decades, isconsidered reliable for diagnosis.
Having lost the bebate, the machinerykept manipulating and distorting statistics.Many people, and even some doctors,allege that cholera cases were oftenregistered as hepatitis or gastronteritiscases, and cases of the latter two oftendismissed as simple cases of diarrhoea.
After being hauled up by the primeminister, the administration launched acampaign for administering anticholeravaccine to lakhs of people. The vaccine,once considered the standard method ofpreventing cholera, is now considered thestandard method of preventing cholera, isnow considered an inadequate method ofdealing with the disease. No more that 30to 40 percent of the vaccinated populationdevelops immunity.
During the rainy season, the probabilityof polio virus being present in the bodydue to contaminated water is higher thanusual and any injection, including the
cholera vaccine, can precipitate paralyticpolio, particularly in children. Therefore,no injection should be given in the rainyseason, unless absolutely unavoidable.Already, an unusually large number of poliocases are being reported.
The anticholera vaccine begins to workonly after a gestation period of 10 days soit offers virtually no protection in a situationof rapid spread of disease. It is alleged thatin some cases vaccine from stocks whoseefficacy had expired was injected. Anothercommon complaint was that the needlesused for vaccination were not properly
sterlised. In any case, the vaccine has noeffect in reducing the incidence of carrierswho play the most vital role in the spread ofthe disease. Nor does it reduce the severityof attack in people previously innoculated.The protection endures for the limitedperiod, ranging from three to six months.
The World Health Organisation hasacknowledged the ineffectiveness of thevaccine. Yet, the government pursued theinjection campaign with a vengeance,determined to complete a target of 900,000.There were several reports of childrenhaving registered immediate adversereactions to the anticholera vaccime. In

14 MANUSHI
Saleema of Seemapuri
some cases, when the stocks of anticholeravaccine were exhausted, antityphoidvaccine was administered. All this so thatquantitative targets could be attained anda pretence of doing something maintained.
Most hospitals were not equipped tohandle the rush of patients. In some, therewere two or three patients per bed and manymore on the floors. In many colonies peoplecomplained that local governmentdispensaries refused to handle even simplecases, and referred them to the overcrowdedhospitals.
Hospitalisation is not crucial or evennecessary for control of cholera,gastroenteritis or hepatitis. Glucose drip isnecessary only in very severe cases. Themajority of cases could have beenadequetely dealt with by the primary helthcentres and dispensaries, had these beeneven reasonably functional. The treatmentfor cholera is fairly simple -- tetracycline, orfurazolidine for tetracycline resistantstrains. Tetracycline should beaccompanied by B complex and by largequantities of water.
Since most deaths occur due todehydration the most important combatmeasure would have been to communicateeffectively to people the fact that oralrehydration solution -- a water solutionmade with sugar and salt, if given in largequantities to affected patients, would havesaved almost all lives. This was not done.Hospitals and private clinics who putpatients on glucose drip did not explain withcare that after the patient was taken off thedrip and sent home, he or she shouldcontinue to be given oral rehydration.
Government and private agenciesdistributed a couple of oral rehydrationpackets per family but did not explain whatthe family should do after the packets wereused up. Most women we net were underthe impression that the packet constituteda one time dose like the vaccination. Theyused one packet and kept the other for somesort of emergency. We did not see manyfamilies using oral rehydration solution.
At the Mercy of QuacksA number of people preferred to go to
private doctors, many of whom were not
even qualified. Even though it is hard to becertain about the proportion of the sick whowent to private doctors, my impression, fromtalking to people, is that the ration might bearound 50 percent. So the governmentstatistics are misleadingly low. They donot take into account the cases that wentto private doctors, and those that got notreatment whatsoever.
Most patients we met told us thatprivate doctors put patients on a glucosedrip for a while; gave them an injection orpills (no one knew the contents of these)and prescribed tonics, vitamin tablets andpainkillers. In house after house, we sawbottles of tonics, iron tablets and irrelevantmedicines bought at exorbitant prices.Most private doctors in these colonies notonly prescribe but also dispensed were notin wrappers hence there was no way ofknowing what they were. The tonics soldby the doctors seemed to be of spuriousquality, manufactured by small unknowncompanies in and around Delhi.
Kohinoor, a pitiably poor woman, whoworks as a domestic servant nearSeemapuri, said that the doctor charged herRs 200 in one day. She had borrowed the
money from her brother, a vegetable vendor.She had fever, diarrhoea and vomiting, andfainted on her way back from work. Theprivate doctor put her on glucose drip, gaveher an injection and sold her a large bottleof B Complex syrup manufactured by aspurious sounding company in Ghaziabad,and an equally spurious looking iron tonic.She was still so weak that she found it hardto stand.
Saleema’s one and a half year old sonhad died two days before we met her. Hehad been sick for about for months withthe usual symptoms of diarrhoea andvomiting. She took him to the localgovernment hospital where he was givensome tablets but did not improve.
She then took him to a private doctorwho gave some tablets, handed her aCerelac Baby Care Book and recommendedthat she feed the child with this baby foodmanufactured by Nestles. One tin costher Rs 21.50. She bought two tins. Thechild continued to deteriorate and died onJuly 30.
Kamla, aged 25, wife of a rickshawpuller, lost her five month old son who hadbeen ailing for about a month with

No.47July-August 1988
diarrhoea, vomiting and fever. The localgovernment dispensary refused to treathim and told her to go to the main hospital.The local quack said: “Don’t worry, havalag gayi hai” and gave some medicine.The child kept getting worse and wastaken to the OPD of the local hospital.Despite the medicines given there, hiscondition continued to deteriorate, so theparents discontinued the treatment. Bythe time they took him to hospital a secondtime, he was probably beyond help anddied soon after admission.
One important reason why so manypoor people prefer to go to expensive butdubious private doctors rather than to thefree government hospitals is that at thelatter, they have to stand in various queuesfor hours before they get to see a doctor.A long wait could be fatal for a very sickchild. Also, many of these poor men andwomen work as casual labourers earning adaily wage, and cannot afford to lose aday’s wage each time they visit thehospital. The quality of care and attentionat the hospital is rather poor and often thehospitals do not dispense the freemedicines they are supposed to, so themedicines have to be paid for, anyway. In
these circumstances, paying the privatedoctor often seems more convenient.
Unauthorised Lives?One of the government’s of repeated
excuses for its inability to control theepidemic was that in parts of Delhi,especially in trans Yamuna areas, a largenumber of unauthorised colonies havemushroomed over the years, for theprovision of civic amenities to which thegovernment is not responsible since theyhave come into being “illegally.”
The deputy commissioner (water) MrRai, admitted at a press conference onAugust 18 that even according togovernment’s own (mostly misleading)estimates, about 3,000,000 people in thecapital are still dependent for drinkingwater on handpumps which have beenidentified as the main source of cholerainfection Expressing his inability to doanything in the matter, he explained thatthese 3,000,000 people live inunauthorised, the Delhi Water Supply andSewage Disposal Undertaking cannotprovide them with potable water (TheHindu, August 19).
While the deputy commissioner, with
his limited vision and mandate, may betechnically correct in making such astatement, the government should not beallowed to get away with so irresponsiblean attitude. Health is indivisible, and theuncleanliness in the farflung hutments andcolonies is bound to affect, has indeedalready affected, the hygiene level of theentire city.
It should be remembered thathundreds of thousands throng to Delhiand other big cities, not for the pleasure ofliving in slums, but because they find thebarest survival impossible in the villagesfrom which they are forced to migrate. TheState, claiming as it does to be omnipotentin economic development, cannot disownresponsibility for the destitution which isthe direct consequence of its ownplanning. The problem cannot be wishedaway by an ostrichlike posture.
What Could be Done1. If the influx of population into
cities continues at the current rate,life in the cities will becomeincreasingly unviable. However,this migration cannot be stoppedby legislativeflat or by force. Itcan only stop if life outside bigcities is made at least liveable forthe poort.
2. The emergence of sprawlingslums containing more than halfof city’s population, people withprecarious rights, has facilitatedthe rise of hoodlums as politicalgodfathers. The unholy power ofthese fuffians can be checked onlyif institutions of local selfgovernment are allowed to existand are given powers workeffectively. The local communityin each area should have the powerto hire and fire and manage thelocal administration.
3. The health policies of thegovernment, with their emphasison elephantine hospitals andsophisticated equipmentconcentrated at a few centres, aretotally unfitted to cope with thepeople’s everday health careneeds, let alone large scale
Shahadat Ali’s, family, huddled on a pile of bricks in the flooded slum,Sarhadpuri

16 MANUSHI
“Ladies First” -- The Story of Nasbandi NagarMen consider themselves the braver of the two sexes, but time and again, we find
that when it comes to shouldering some unpleasant responsibility, or undertaking arisky job, they gallantly put women forward, saying “ladies first.” Here is an interestingexample of this gallantry.
As one always associates nasbandi with Sanjay, I was intrigued as to how NasbandiNagar came to be officially named Rajiv Colony. I was told that the colony was foundedin 1985. The patwari of the local village had to meet sterilisation quotas to qualify fora government award. Therefore, he announced that a 100 square yard plot would begiven to anyone who got sterilised. A number of volunteers were given plots on wasteland on the edge of a huge stormwater drain. Plots were similarly allotted in 1986, 1987and 1988, but the size of the plots kept shrinking. It shrank from 100 to 60 to 50 and to25 square yards. The residents chuckled: “The latest of the sterilised people have havegot papers, no land yet. Abhi woh chakkar hi kaat rahe hain.” The 100 square yardplot is now valued at about Rs 16,000 even though the area is totally undeveloped,without water, sanitation or electricity, and is surrounded by drains, hutments andwaste lard.
I asked whether both husband and wife were sterilised in return for the plot, andwas told that either spouse could volunteer to be sterilised. “How many allottees weremen and how many women?” was my next question. One many evisively said thenumbers were equal, at which others laughed sheepishly. When I persisted in equiringabout the ratio, a 45 year old woman burst out: “The majority were women -- more than75 percent were most men had told their wives to get sterilised because they felt “admikamzor ho jayenge.” (men would get weak). After this, as we went through the colony,I asked about 20 people at random as to who in their family was sterilised. The ratio wasabout eight women to every two men. Of these men, I asked one, 28 year old AmarSingh of Delhi Home Guards, why he had gotten sterilised and not his wife. He repliedwithout embarrassment: “At that time my wife was in the village. I would have missedgetting the plot if I had waited for her to return.”
The most spinechilling response came from the 40 year old wife of a cobbler whosaid with a rare ferocity: “I did not want my husband to go in for it because I was afraidhe would get weak. What if anything had happened to him, the bread earner? So Ipreferred to get operated.” When I asked: “What if something had happened to you?”she replied with even greater ferocity: “Auraton ka kya hai? Paanv hai to juta aa hijayega, paanv nahin to koi juta rakh ke kya karega? Mein to manti hun ki aurat kohar hal mein admi se pehle marna chahiye” (What does a woman’s life matter? If youhave a food, you can always get a shoe for it. If you don’t have a foot, what will you dowith a shoe? I believe that a woman should always die before her husband).
The plots were allotted in the women’s names when it was they who got sterilised.It would be interesting to keep track of how long the ownership papers remain in thewomen’s names. Already, many families have sold their plots and moved away. I doubtvery much that the women would have had any control over the sale money even whenthe plots were allotted in their names.
We are told a major reason for the defeat of Mras Gandhi in the post emergencygeneral election of 1977 was the issue of forced sterilisations. Apart from the use offorce in those sterilisation campaigns, a major cause of the outburst of anger was thatfor once, men became the prime targets. About 80 percent of sterilisations at that timewere performed on men. After the emergency, apart from abandoning the use of blatantforce, the authorities also abandoned their focus on men, and women came to be theprimary targets. As in the pre emergency days, about 85 percent of all sterilisationsnow performed are on women.
disasters. The health policyshould be redesigned to focus oncommunity based preventivemedicine and a delivery systemthat can reach those who needhealth care most. We need moreprimary health workers whoshould work under the directsupervision of local selfgovernment institutions.
The cholera epidemic is now subsidingand will soon be forgotten as newerdisasters occur. However, it has broughtinto sharp focus the problems, economicand political, inherent in ourovercentralised system of governance. Ifevery drain in the country must wait for aprime ministerial visit before a pretence ismade of cleaning it, then, clearly, thesystem of governance has been reducedto a farce.
Cholera -- Not Confined to DelhiAlone
Cholera deaths occurred in severalnorth Indian cities but were lessdocumented and reported than those inthe capital city. This picture, taken onAugust 13, shows mourners in a home in aHarijan colony in Rewa, a Madhya Pradeshtown. This family had lost two memberswithin 24 hours -- Chotibai, aged 60, andOm Prakash, aged 15 months. Both hadthe usual symptoms -- acute diarrhoea andvomiting.
Conditions in slums like this one arenot very different from those in Delhislums. Residents complained that no onecomes to clean the area. Latrines are filthyand dilapidated. the only drinking watersource is the open well seen in the picture.
P.S. As this goes to press, conjunc-tivitis, also spread by u n h y g i e n i cconditions, is sweeping through Delhi andother cities.