what’s new in dermatopathology melanocytic proliferationswhat’s new in dermatopathology...
TRANSCRIPT

3/27/2017
1
What’s New in DermatopathologyMelanocytic proliferations
Aleodor (Doru) Andea, MD, MBAAssociate Professor of Pathology and DermatologyDirector of Dermatopathology Molecular Diagnostic LaboratoryUniversity of MichiganAnn Arbor, [email protected]@DoruAndea
Disclosure of Relevant Financial Relationships
USCAP requires that all planners (Education Committee) in a position to
influence or control the content of CME disclose any relevant financial
relationship WITH COMMERCIAL INTERESTS which they or their
spouse/partner have, or have had, within the past 12 months, which relates to
the content of this educational activity and creates a conflict of interest.
Disclosure of Relevant Financial Relationships
USCAP requires that all faculty in a position to
influence or control the content of CME disclose any relevant financial
relationship WITH COMMERCIAL INTERESTS which they or their
spouse/partner have, or have had, within the past 12 months, which relates to
the content of this educational activity and creates a conflict of interest.
Dr. Aleodor Andea declares he has no conflict(s) of interest
to disclose.
Overview1. Case based presentation
2. Updates in molecular ancillary studies for thediagnosis of difficult melanocytic tumors (SNPmicroarrays)
3. Updates in diagnosis and prognosis of fewmelanocytic entities
• Why do we need more stuff?
MelanomaCommon nevus

3/27/2017
2
• A small proportion have ambiguous histology
Nevoid melanomaCommon nevus
?
• 40-year old woman with a papule on the right shoulder
• Clinical R/O BCC
8
• Melanocytic neoplasm with borderline features between nevus and melanoma• Suspicious for nevoid melanoma

3/27/2017
3
What else we can do?
Molecular studies
Molecular studies
• Genomic instability in melanoma
Molecular studies
• Genomic instability in melanoma
• Detection of numerical abnormalities in the tumor genome (CGH/SNP and FISH)
Molecular studies
• Detection of numerical abnormalities in the tumor genome
• Mass spectrometry
• Gene expression profile
• Identification of mutations (TERT gene promoter)
Comparative Genomic Hybridization (CGH)/ Single Nucleotide Polymorphism (SNP) arrays
• Screens the entire genome for gains and losses in DNA material in one experiment
• Variants:• Array based CGH –Gains and Losses• Array based SNP –Gains, Losses and Loss of
Heterozygosity

3/27/2017
4
SNP arrays SNP arrays• Copy number changes
SNP arrays• Copy number changes
11p gain
SNP arrays• Copy number changes
• Allele peak
SNP arrays• Copy number changes
• Allele peak
SNP arrays• Copy number changes
• Allele peak
• Mutation data• BRAF• NRAS• PTEN• TP53

3/27/2017
5
Univ of Michigan Cohort
Melanoma
Nevus
Univ of Michigan Cohort
Melanoma
Nevus
Univ of Michigan Cohort
Melanoma
Nevus
Univ of Michigan Cohort
Melanoma
Nevus
Compound nevus
• No gains or losses
• BRAF V600E
Primary melanoma
• 19 CNA
• 13 losses
• 6 gains
• BRAF V600E

3/27/2017
6
Metastatic melanoma
• 30 CNA• 25 gains• 2 losses• 3 CN-LOH
• BRAF V600K
• Chr 22 CN-LOH
• Chr 9p21 homozygous loss (CDKN2A)
• Chr 1p gain (NRAS)
• NRAS Q61R
• Chr 13q loss (BRCA2) • Chr 9p 21 homozygous loss• Chr 22 CN-LOH• Chr 1p gain (NRAS)• Chr 13q loss (BRCA2)
• NRAS Q61R

3/27/2017
7
Nevoid melanomaThis seems easy enough…
• No abnormalities – GOOD• Abnormalities – BAD
• Not that simple
Not all abnormalities are bad
• Some can be used to classify nevi
39
28 y/o F, Lt Temple
3p loss (BAP-1 locus)
BRAF V600E
BAP-1 negative nevus (BAP-oma)

3/27/2017
8
BAP1 IHC10 days old AA newbornGiant congenital nevus with several nodules
CGHOncoScanTM
Affymetrix
Cop
y nu
mbe
r
• Result: Losses of whole chromosomes 3, 4, 5, 10, 11, 13, 14, 16, 17, 18, 21
10 days old AA newborn
Proliferative nodule in a congenital nevus
1 year old
More problems
• How many abnormalities do we require for a melanoma diagnosis

3/27/2017
9
Histologicalclassification
# of cases with at least one significant copy
number variation
Average # CNV
Nevi 0/6 (0%) 0
Atypical nevi 3/15 (20%) 1.6 (1-2)
Ambiguous 15/25 (60%) 6.3 (1-25)
Melanoma 35/39 (90%) 21.7 (1-69)
Alomari et al. Platform at USCAP meeting, Seattle WA, 2016
Sensitivity: 90%
Specificity: 87%
• >=3 abnormalities significant (but with exceptions)
• Whole chromosomal abnormalities in proliferative nodules
• Isolated homozygous deletion of 9p21 favors melanoma
• Others to come….
• >=3 abnormalities significant (but with exceptions)
• Whole chromosomal abnormalities in proliferative nodules
• Isolated homozygous deletion of 9p21 favors melanoma
• Others to come….
• Molecular pathologist job: Provide a comprehensive
interpretation
• Your job: Understand the report and communicate with
your molecular pathologist
Ultimate question
• Can CNV number and/or pattern predict adverse outcome in borderline lesions?
• Unfortunately not too many studies
Ambiguous cases with clinical follow up
65
3
0
1
2
3
4
5
6
7
8
9
10
Positive CNV Negative CNV
No adverse events Adverse events
N =14
0% Adverse events
33% Adverse events
Alomari et al. Platform at USCAP meeting, Seattle WA, 2016
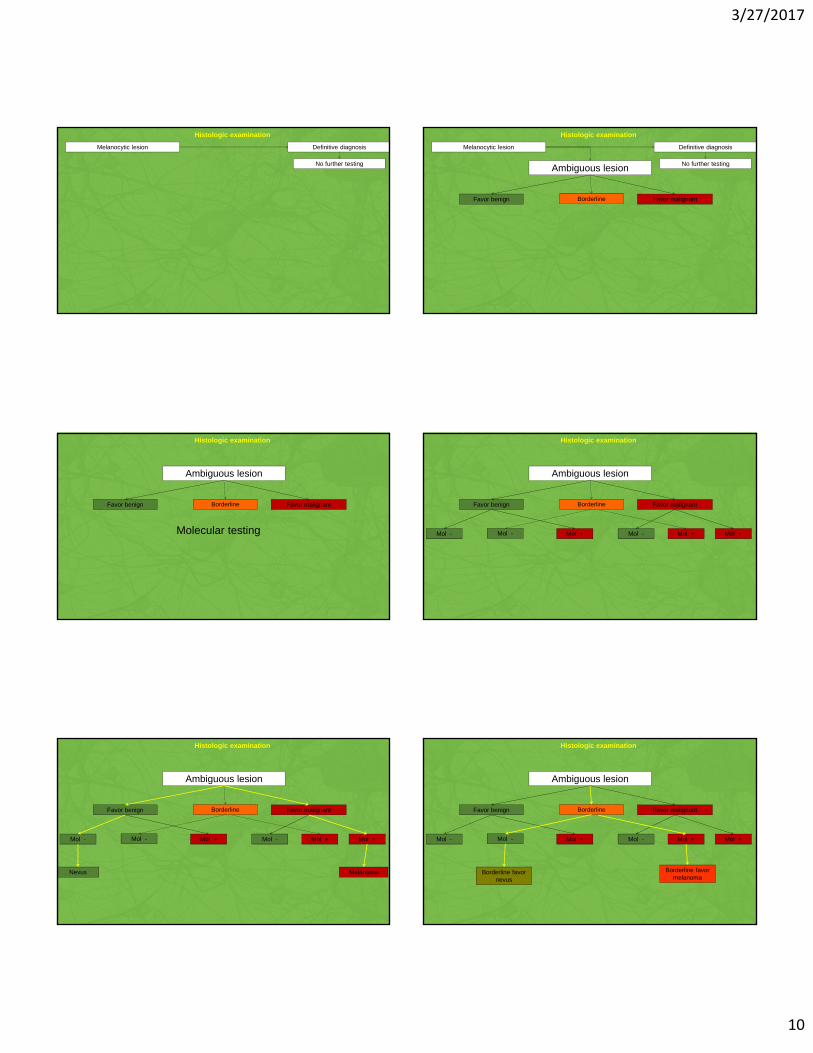
Practical algorithm for use of molecular studies
3/27/2017
10
Melanocytic lesion
Histologic examination
Definitive diagnosis
No further testing Ambiguous lesion
Favor benign Favor malignant
Melanocytic lesion
Histologic examination
Definitive diagnosis
No further testing
Borderline
Ambiguous lesion
Favor benign Favor malignant
Histologic examination
Borderline
Molecular testing
Ambiguous lesion
Favor benign Favor malignant
Mol - Mol + Mol - Mol +
Histologic examination
Borderline
Mol +Mol -
Ambiguous lesion
Favor benign Favor malignant
Melanoma
Mol -
Nevus
Mol + Mol - Mol +
Histologic examination
Borderline
Mol +Mol -
Ambiguous lesion
Favor benign Favor malignant
Mol - Mol + Mol - Mol +
Histologic examination
Borderline
Mol +Mol -
Borderline favor nevus
Borderline favor melanoma

3/27/2017
11
Ambiguous lesion
Favor benign Favor malignant
Mol -
Borderline
Mol +
Borderline
Mol - Mol +
Histologic examination
Borderline
Mol +Mol -
Ambiguous lesion
Favor benign Favor malignant
Melanoma
Mol -
Nevus Borderline
Mol +
Borderline
Mol - Mol +
Melanocytic lesion
Histologic examination
Definitive diagnosis
No further testing
Borderline
Mol +Mol -
Borderline favor nevus
Borderline favor melanoma
Risk assessment
Ambiguous lesion
Favor benign Favor malignant
Melanoma
Mol -
Nevus Borderline
Mol +
Borderline
Mol - Mol +
Melanocytic lesion
Histologic examination
Definitive diagnosis
No further testing
Borderline
Mol +Mol -
Borderline favor nevus
Borderline favor melanoma
Excision with limited margins• Excision with margins appropriate
for depth• SLN
• Excision with margins appropriate for depth if possible
• +/- SLN
Cost and TAT
Cost and TAT
Test Range TAT
SNP/CGH array $1,800-$2,400 14-21 days
FISH $800-$1,200 3-7 days
Microarray vs. FISH
• Order Microarray if • Order FISH if

3/27/2017
12
Microarray vs. FISH
• Order Microarray if• Can afford
• Order FISH if
Microarray vs. FISH
• Order Microarray if• Can afford• Have enough material
• > 1mm2• >30%tumor purity• 10 unst @ 10microns
• Order FISH if
Microarray vs. FISH
• Order Microarray if• Can afford• Have enough material
• > 1mm2• >30%tumor purity• 10 unst @ 10microns
• Can wait 2-3 weeks
• Order FISH if
Microarray vs. FISH
• Order Microarray if• Can afford• Have enough material
• > 1mm2• >30%tumor purity• 10 unst @ 10microns
• Can wait 2-3 weeks
Advantage: higher sensitivity
• Order FISH if
Microarray vs. FISH
• Order Microarray if• Can afford• Have enough material
• > 1mm2• >30%tumor purity• 10 unst @ 10microns
• Can wait 2-3 weeks
Advantage: higher sensitivity
• Order FISH if• Microarray not covered
Microarray vs. FISH
• Order Microarray if• Can afford• Have enough material
• > 1mm2• >30%tumor purity• 10 unst @ 10microns
• Can wait 2-3 weeks
Advantage: higher sensitivity
• Order FISH if• Microarray not covered• Not enough material
• Only few slides• Superficial lesions• Tumor infiltrated by benign cells/
inflammation
3/27/2017
13
Microarray vs. FISH
• Order Microarray if• Can afford• Have enough material
• > 1mm2• >30%tumor purity• 10 unst @ 10microns
• Can wait 2-3 weeks
Advantage: higher sensitivity
• Order FISH if• Microarray not covered• Not enough material
• Only few slides• Superficial lesions• Tumor infiltrated by benign cells/
inflammation
• Need faster TAT
Microarray vs. FISH
• Order Microarray if• Can afford• Have enough material
• > 1mm2• >30%tumor purity• 10 unst @ 10microns
• Can wait 2-3 weeks
Advantage: higher sensitivity
• Order FISH if• Microarray not covered• Not enough material
• Only few slides• Superficial lesions• Tumor infiltrated by benign cells/
inflammation• Need faster TAT
Disadvantage: lower sensitivity, higher false positive (lower specificity)
Key points
• CNVs can assist in the diagnosis of melanocytic lesions
• Should be used only in ambiguous lesion
• Molecular data should not overturn histologic impression
• >=3 abnormalities – significant for melanoma
• Understand the molecular report
30 y/o male blue-colored plaque on the scalp with subcutaneous nodules Bx from the plaque

3/27/2017
14
Bx from the nodules
Large plaque-type blue nevus with subcutaneous cellular nodules
6 years later

3/27/2017
15
Melanoma ex cellular blue nevus
• Aka Malignant blue nevus
Common blue nevus
Cellular blue nevus
Common blue nevus
Cellular blue nevus Atypical cellular blue nevus
3/27/2017
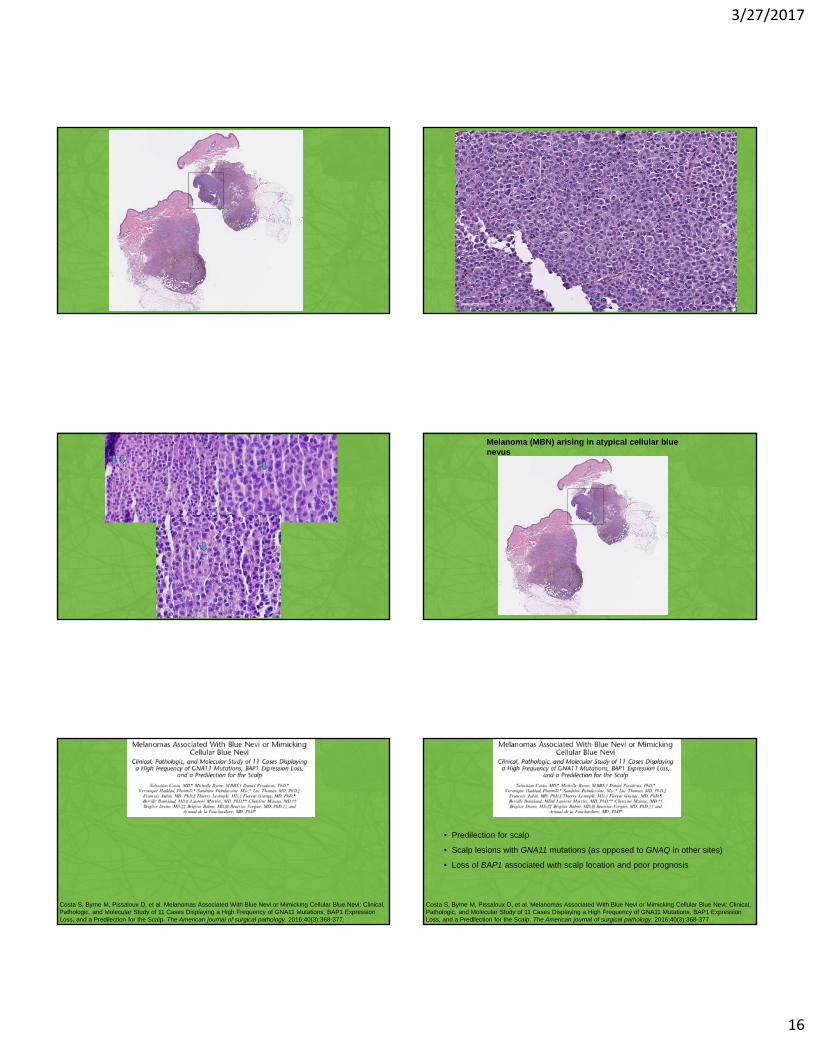
16
Melanoma (MBN) arising in atypical cellular blue nevus
Costa S, Byrne M, Pissaloux D, et al. Melanomas Associated With Blue Nevi or Mimicking Cellular Blue Nevi: Clinical, Pathologic, and Molecular Study of 11 Cases Displaying a High Frequency of GNA11 Mutations, BAP1 Expression Loss, and a Predilection for the Scalp. The American journal of surgical pathology. 2016;40(3):368-377.
Costa S, Byrne M, Pissaloux D, et al. Melanomas Associated With Blue Nevi or Mimicking Cellular Blue Nevi: Clinical, Pathologic, and Molecular Study of 11 Cases Displaying a High Frequency of GNA11 Mutations, BAP1 Expression Loss, and a Predilection for the Scalp. The American journal of surgical pathology. 2016;40(3):368-377.
• Predilection for scalp
• Scalp lesions with GNA11 mutations (as opposed to GNAQ in other sites)
• Loss of BAP1 associated with scalp location and poor prognosis

3/27/2017
17
Blue nevi: 5Atypical blue nevi: 10Melanoma ex blue nevus: 9
Blue nevus/ Cellular Blue Nevus
Blue nevus/ Cellular Blue Nevus
Atypical Cellular Blue Nevus
Atypical blue nevi may show few aberrations
Blue nevus/ Cellular Blue Nevus
Atypical Cellular Blue Nevus
Blue nevus/ Cellular Blue Nevus
Atypical Cellular Blue Nevus
Melanoma
MBN without adverse outcome
MBN with adverse outcome
3p loss may have prognostic implications in MBN
3/27/2017
18
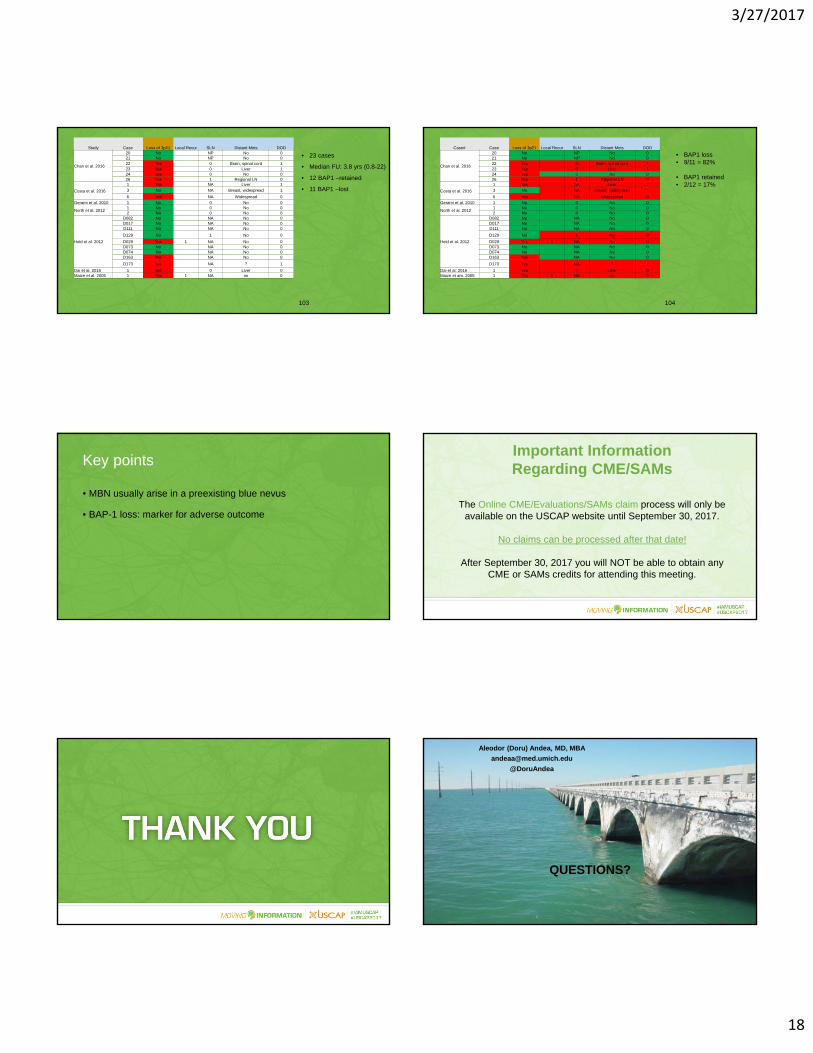
103
Study Case Loss of 3p21 Local Recur SLN Distant Mets DOD
Chan et al. 2016
20 No NP No 021 No NP No 022 Yes 0 Brain, spinal cord 123 Yes 0 Liver 124 Yes 0 No 026 Yes 1 Regional LN 0
Costa et al. 2016
1 Yes NA Liver 1
3 No NA Breast, widespread 1
6 Yes NA Widespread 0
Gerami et al. 2010 1 No 0 No 0
North et al. 20121 No 0 No 02 No 0 No 0
Held et al. 2012
D082 No NA No 0D017 No NA No 0D111 No NA No 0
D129 No 1 No 0
D029 Yes 1 NA No 0D073 No NA No 0D074 No NA No 0D163 Yes NA No 0
D173 Yes NA ? 1
Dai et al. 2016 1 Yes 0 Liver 0Maize et al. 2005 1 Yes 1 NA no 0
• 23 cases
• Median FU: 3.8 yrs (0.8-22)
• 12 BAP1 –retained
• 11 BAP1 –lost
104
Case# Case Loss of 3p21 Local Recur SLN Distant Mets DOD
Chan et al. 2016
20 No NP No 021 No NP No 022 Yes 0 Brain, spinal cord 123 Yes 0 Liver 124 Yes 0 No 026 Yes 1 Regional LN 0
Costa et al. 2016
1 Yes NA Liver 1
3 No NA Breast, widespread 1
6 Yes NA Widespread 0
Gerami et al. 2010 1 No 0 No 0
North et al. 20121 No 0 No 02 No 0 No 0
Held et al. 2012
D082 No NA No 0D017 No NA No 0D111 No NA No 0
D129 No 1 No 0
D029 Yes 1 NA No 0D073 No NA No 0D074 No NA No 0D163 Yes NA No 0
D173 Yes NA ? 1
Dai et al. 2016 1 Yes 0 Liver 0Maize et am. 2005 1 Yes 1 NA no 0
• BAP1 loss• 9/11 = 82%
• BAP1 retained• 2/12 = 17%
Key points
• MBN usually arise in a preexisting blue nevus
• BAP-1 loss: marker for adverse outcome
Important Information Regarding CME/SAMs
The Online CME/Evaluations/SAMs claim process will only be available on the USCAP website until September 30, 2017.
No claims can be processed after that date!
After September 30, 2017 you will NOT be able to obtain any CME or SAMs credits for attending this meeting.
PRESENTATION TITLE
QUESTIONS?
Aleodor (Doru) Andea, MD, MBA
@DoruAndea

3/27/2017
19
• 79 y/o man
• Pigmented lesion on left medial finger for 6 years
• Slowly growing
MELAN-A

3/27/2017
20
MITF
Current case Acral lentiginous MIS
Lentigo
• Recurrence after 4 years

3/27/2017
21
Acral lentiginous melanoma
Am J Dermatopathol 36 (2) February 2014
Kim JY, Choi M, Jo SJ, Min HS, Cho KH. Acral lentiginous melanoma: indolent subtype with long radial growth phase. Am J Dermatopathol. 2014;36(2):142-147.
• 13 patients• Bland proliferation of
melanocytes• Not sufficient for MIS
Kim JY, Choi M, Jo SJ, Min HS, Cho KH. Acral lentiginous melanoma: indolent subtype with long radial growth phase. Am J Dermatopathol. 2014;36(2):142-147.
What else we could have done? Fluorescence in situ hybridization

3/27/2017
22
FISH for melanocytic tumors
• Evaluate for copy number alterations
• Original panel:• 6p25 (RREB1) -gains• 6q23 (MYB) -losses• 11q13 (CCND1) -gains
• Expanded panel• 8q24 (MYC) -gains• 9p21 (CDKN2A) -homozygous loss
Fluorescence in situ hybridization
11q13 (CCND1) amplification
Key points
• When faced with acral pigmented lesions with histologically
subtle atypical ALWAYS ask for the clinical impression
Important Information Regarding CME/SAMs
The Online CME/Evaluations/SAMs claim process will only be available on the USCAP website until September 30, 2017.
No claims can be processed after that date!
After September 30, 2017 you will NOT be able to obtain any CME or SAMs credits for attending this meeting.

3/27/2017
23
PRESENTATION TITLE
QUESTIONS?
Aleodor (Doru) Andea, MD, MBA
@DoruAndea