wella afriani (1111012041) vancomycin
TRANSCRIPT
Clinical Pharmacokinetics of VANCOMYCIN
WELLA AFRIANIWELLA AFRIANI11110120411111012041
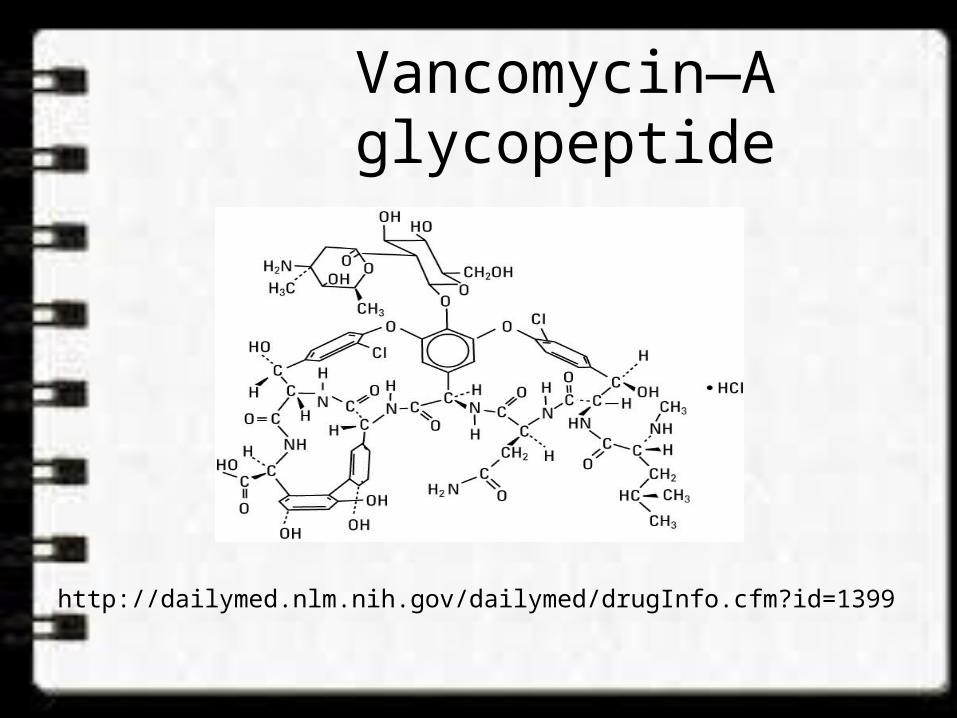
Vancomycin—A glycopeptide
http://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?id=1399
INTRODUCTION• Inhibits bacterial cell wall synthesis• Time-dependent effect • Gram positive bacteria• Indications :– Documented infections:
• Methicillin/Cephalosporin-Resistant Staphycoccal infection.• Penicillin/Cephalosporin-Resistant Streptococcal infection.• Staphy./Strep. infection in patient allergic to penicillin.• Staphy. infection in patient with renal disease undergoing
hemodialysis. • Penicillin-Resistant Diphtheroid infection.• Severe antibiotic-associated enterocolitis.
• Indications (cont’) :
– Empiric Therapy:• Suspected MRSA nosocomial infection.• Meningitis in patient who had neurosurgery.• Neutropenic febrile patient not responding or allergic to
penicillin.• Suspected Staphy. infection in patient with renal disease
undergoing hemodialysis.
– Prophylaxis:• Endocarditis in patient allergic to penicillin.• Prosthetic valve placement in patient allergic to
penicillin.
Vancomycin• Volume of distribution: • An average value of 0.7 L/kg or • For patient older than 18 years:
V (L) = 0.17 (age in yr) + 0.22 (TBW in kg) + 15• Eliminated primarily by the renal route;
approximately 5% of the dose is metabolized (Vancomycin Cl ~ Clcr)
Winter ME. Basic Clinical Pharmacokinetics. 5th ed. Philadelphia: Lippincott Williams and Wilkins, 2010.
Vancomycin• t1/2 elimination• Newborns: 6-10 hours• Infants & Children 3 months to 4 years: 4 hours• Children > 3 years: 2.2 – 3 hours• Adults: 5 – 11 hours; significantly prolonged with renal
impairment
Lexicomp Online, June 2012
ADVERSE DRUG REACTION• Ototoxicity (tinnitus, fullness in the ear)• Nephrotoxicity
• An increase in SrCr of 0.5mg/dL or greater, or as 50% increase from baseline.
• Occurs at a rate of 5% with Vancomycin alone and increase to 22% with addition of Aminoglycosides.
• Red-Man Syndrome (hypotension, upper body maculopapular rash)
• Cutaneous reaction (urticaria, angioedema, erythema)
• Neutropenia (within 15 – 30 days of drug initiation)• Fever
PHARMACOKINETIC CHARACTERISTICS
• Two- or three-compartment model.• Bioavailability– Per oral < 5%– Intravenous 100%
• Protein binding 30 – 55%• Excretion– Renal: >90% unchanged in urine
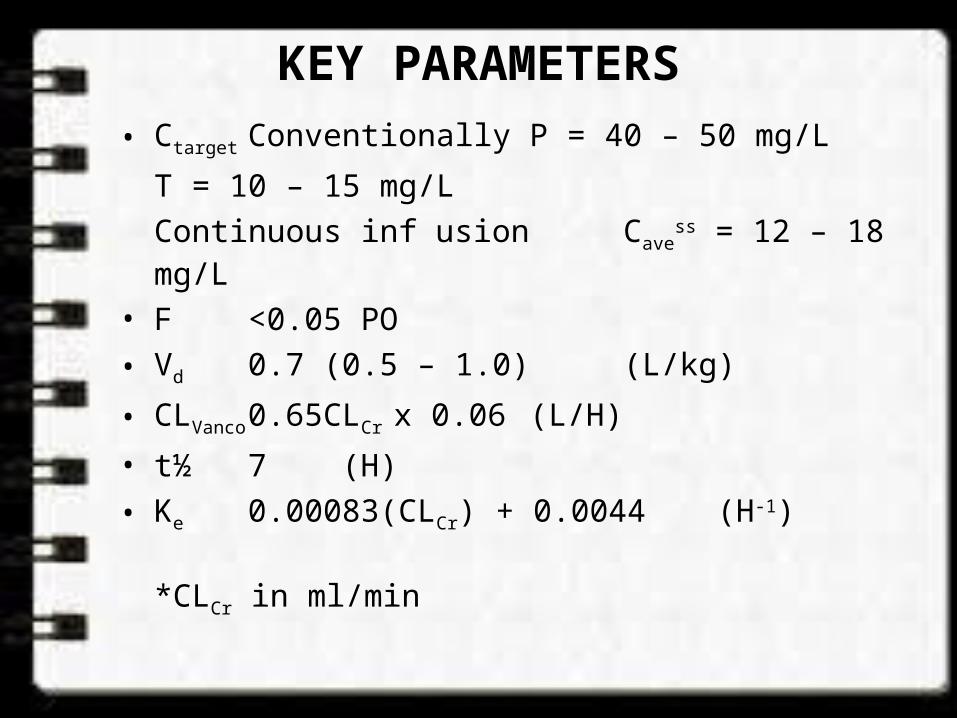
KEY PARAMETERS• Ctarget Conventionally P = 40 – 50 mg/L
T = 10 – 15 mg/LContinuous infusion Cave
ss = 12 – 18 mg/L• F <0.05 PO• Vd 0.7 (0.5 – 1.0) (L/kg)
• CLVanco 0.65CLCr x 0.06 (L/H)• t½ 7 (H)• Ke 0.00083(CLCr) + 0.0044 (H-1)
*CLCr in ml/min
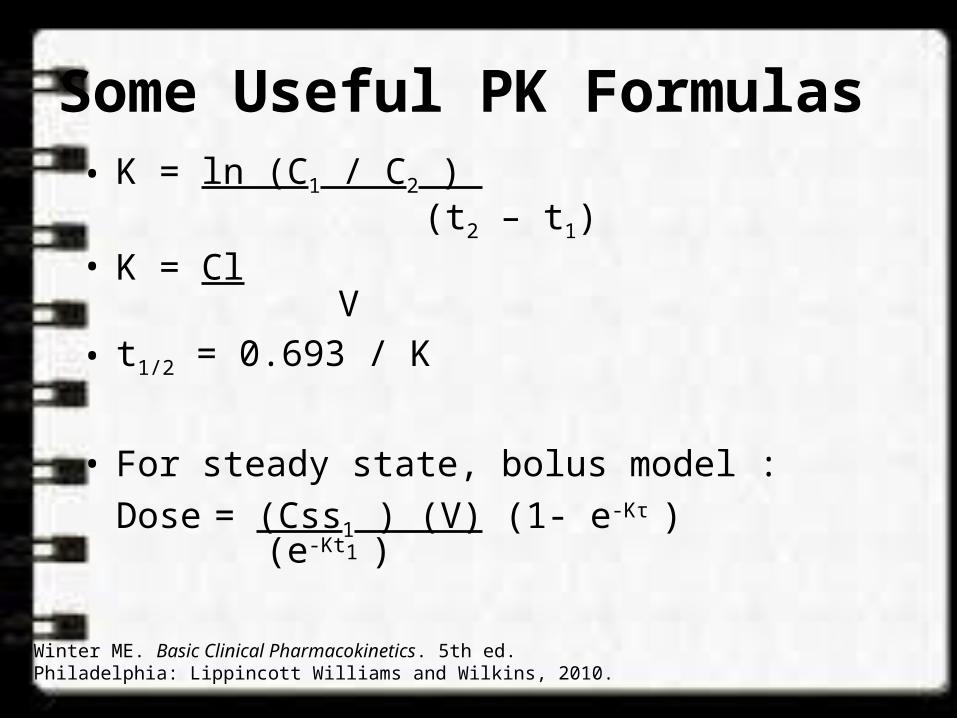
Some Useful PK Formulas• K = ln (C1 / C2 ) (t2 – t1)• K = Cl V• t1/2 = 0.693 / K
• For steady state, bolus model :Dose = (Css1 ) (V) (1- e-Kτ )
(e-Kt1 )
Winter ME. Basic Clinical Pharmacokinetics. 5th ed. Philadelphia: Lippincott Williams and Wilkins, 2010.
Some Useful PK Formulas
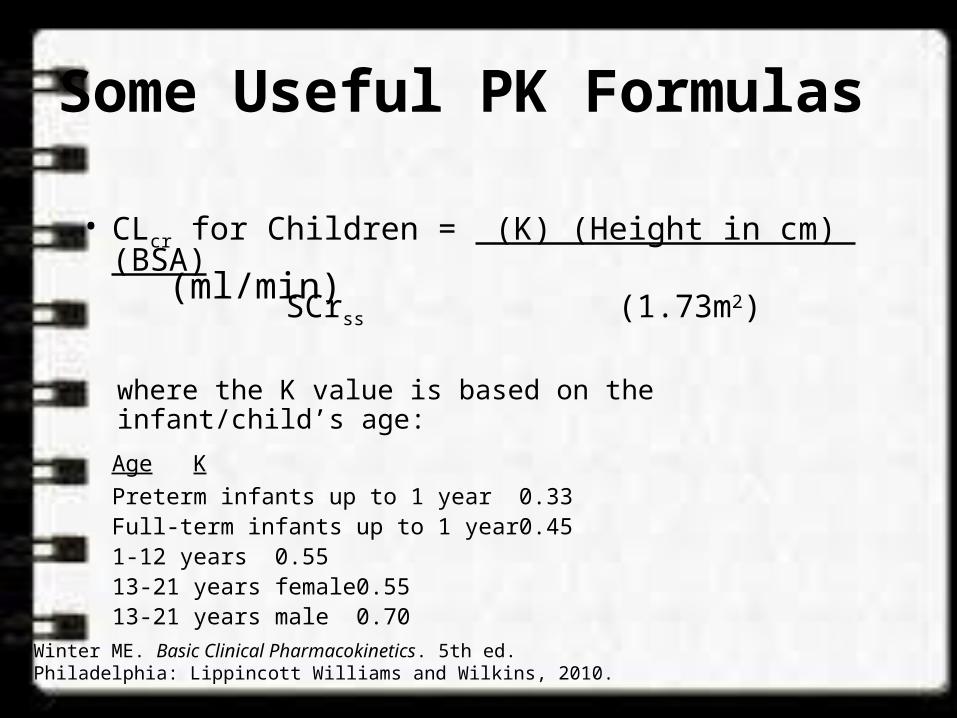
• CLcr for Children = (K) (Height in cm) (BSA) (ml/min) SCrss (1.73m2)
where the K value is based on the infant/child’s age:Age KPreterm infants up to 1 year 0.33Full-term infants up to 1 year 0.451-12 years 0.5513-21 years female 0.5513-21 years male 0.70
Winter ME. Basic Clinical Pharmacokinetics. 5th ed. Philadelphia: Lippincott Williams and Wilkins, 2010.
Some Useful PK Formulas
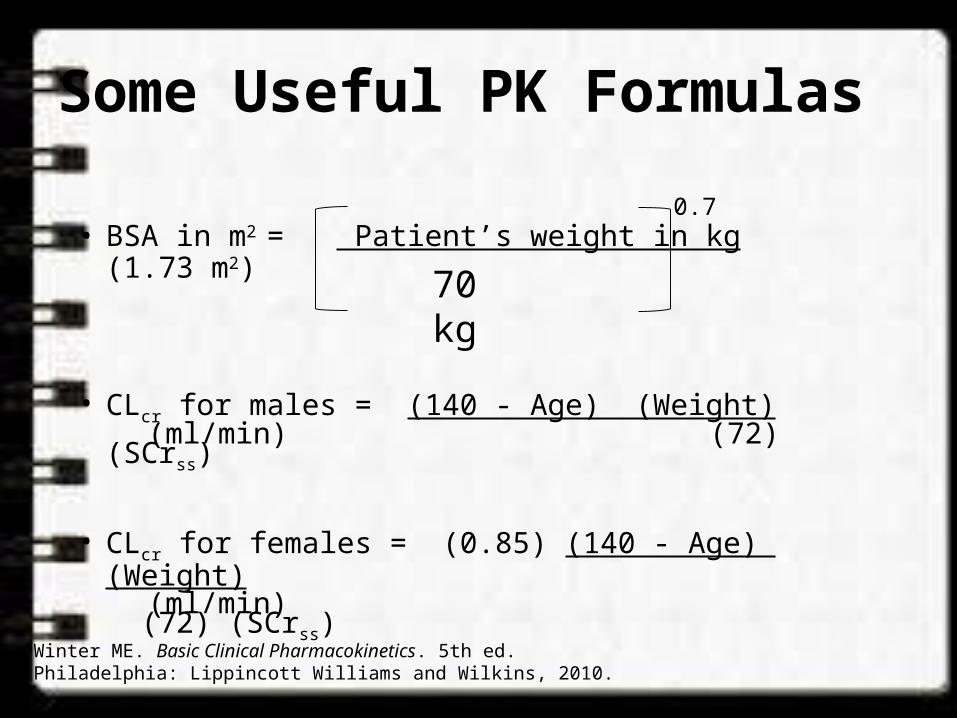
• BSA in m2 = Patient’s weight in kg (1.73 m2)
• CLcr for males = (140 - Age) (Weight) (ml/min) (72) (SCrss)
• CLcr for females = (0.85) (140 - Age) (Weight) (ml/min) (72) (SCrss)
Winter ME. Basic Clinical Pharmacokinetics. 5th ed. Philadelphia: Lippincott Williams and Wilkins, 2010.
70 kg
0.7
Clinical Calculators• Clinical calculator available at LPCH Intranet:
Lane Library Specialty Portals Pharmacy-Calculators Drug Levels-Vancomycin & Aminoglycoside Pharmacokinetics•http://medcalc.com.laneproxy.stanford.edu/pk/•Other calculators available at Pharmacy Network: Pharmacy Network Pharmacokinetic Monitoring• CF Kinetics - by Dr. Carlos Milla• NICU Drug Kinetics - by Dr. William Benitz
Additional Information
• Area Under the Curve (AUC) = area under the plasma drug concentration vs. time curve• AUC = dose administered/drug clearance• AUC (mg.hr/L)= C0 = initial concentration (mg/L)
k elimination rate constant (hr-1)
• Gentamicin and Tobramycin:• AUC24 = 70 – 100 mg.hr/L
• Cystic fibrosis patients: tobramycin AUC24 ~ 100 to 125
Prescott WA Jr, Nagel JL. Extended-interval once-daily dosing of aminoglycosides in adult and pediatric patients with cystic fibrosis. Pharmacotherapy 2010 Jan;30(1):95-108.
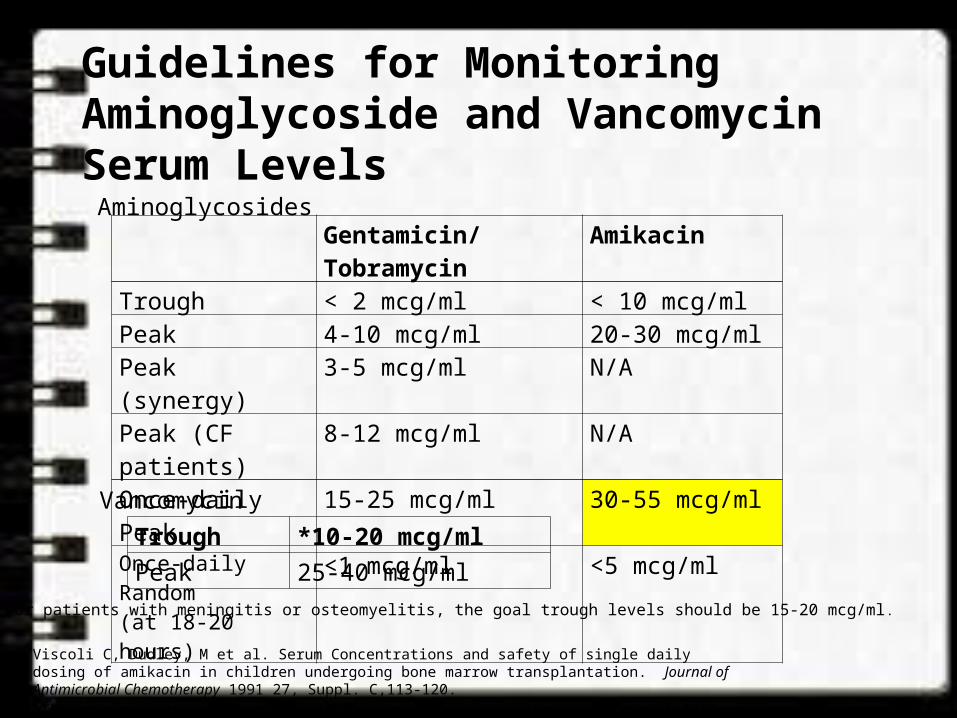
Guidelines for Monitoring Aminoglycoside and Vancomycin Serum Levels
Gentamicin/Tobramycin
Amikacin
Trough < 2 mcg/ml < 10 mcg/mlPeak 4-10 mcg/ml 20-30 mcg/mlPeak (synergy) 3-5 mcg/ml N/APeak (CF patients) 8-12 mcg/ml N/AOnce-daily Peak 15-25 mcg/ml 30-55 mcg/mlOnce-daily Random(at 18-20 hours)
<1 mcg/ml <5 mcg/ml
Trough *10-20 mcg/mlPeak 25-40 mcg/ml
Aminoglycosides
Vancomycin
*For patients with meningitis or osteomyelitis, the goal trough levels should be 15-20 mcg/ml.
Viscoli C, Dudley, M et al. Serum Concentrations and safety of single daily dosing of amikacin in children undergoing bone marrow transplantation. Journal of Antimicrobial Chemotherapy 1991 27, Suppl. C,113-120.Trujillo H, Robledo J et al. Single daily dose amikacin in paediatric patients with severe Gram-negative infections. Journal of Antimicrobial Chemotherapy 1991 27, Suppl. C, 141-147.
INITIATING VANCOMYCIN
• Cultures– Appropriate C&S obtain within 48hrs before
starting therapy.– Antibiotic therapy modified (if necessary) within
24hrs of the C&S results.• Renal Function– Estimated CLCr within 24hrs of initiating therapy.
– Monitoring CLCr every 3 – 5 days during therapy.
INITIATING VANCOMYCIN (CONT’)
• Dosage Regimen & Monitoring Needs– Conventional dosing• Peak & Trough concentration method
– Continuous infusion• Trough concentration method
INITIATING VANCOMYCIN (CONT’)
• Conventional Dosage Regimen– Initial per dose is between 10 – 15 mg/kg body wt– Dosage interval based on estimated CLCr.– Rate of infusion not more than 20 mg/min.– Adjustment based on measured levels.
• Serum Drug Concentration– Levels taken at steady-state.– If stable renal function, repeat trough levels once a
week.– Trough levels obtained if with other nephrotoxic drugs.– Trough and peak levels obtained if:
» Not responding to therapy.» Altered physiologic parameters
INITIATING VANCOMYCIN (CONT’)
• Continuous Infusion Regimen– Infusion rate is based on estimated CLCr and
targeted Cavess (15 mg/L).
– Rate of infusion, Ro (mg/H)
Ro = CLvancoCavess
= VdKeCavess
– Adjustment based on measured Cavess
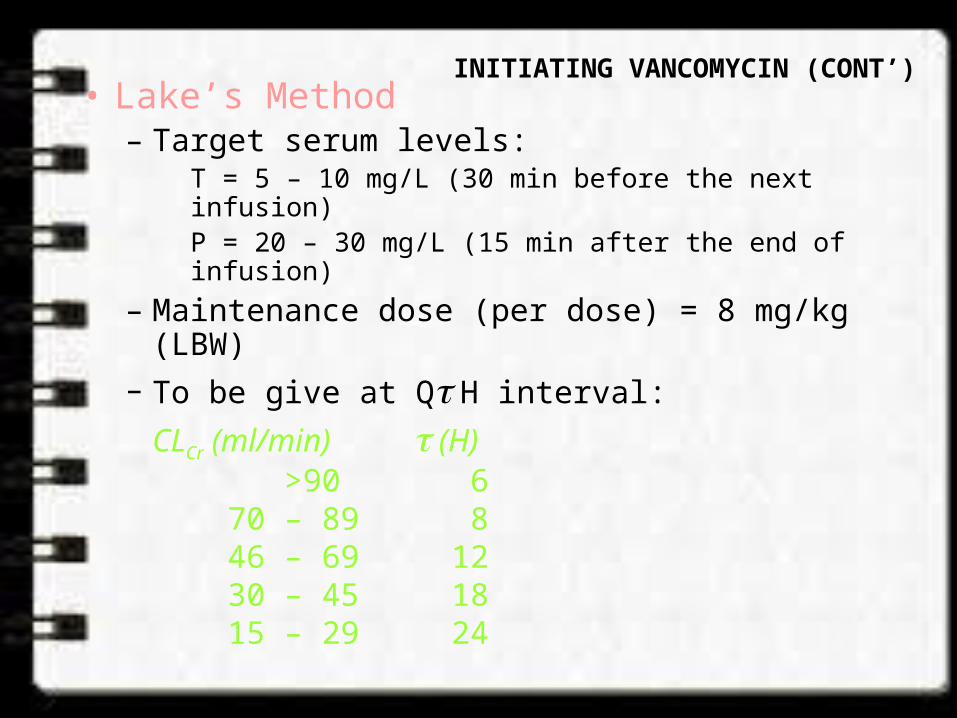
INITIATING VANCOMYCIN (CONT’)• Lake’s Method– Target serum levels:
T = 5 – 10 mg/L (30 min before the next infusion)P = 20 – 30 mg/L (15 min after the end of infusion)
– Maintenance dose (per dose) = 8 mg/kg (LBW)– To be give at Q H interval:
CLCr (ml/min) (H) >90 6 70 – 89 8 46 – 69 12 30 – 45 18 15 – 29 24
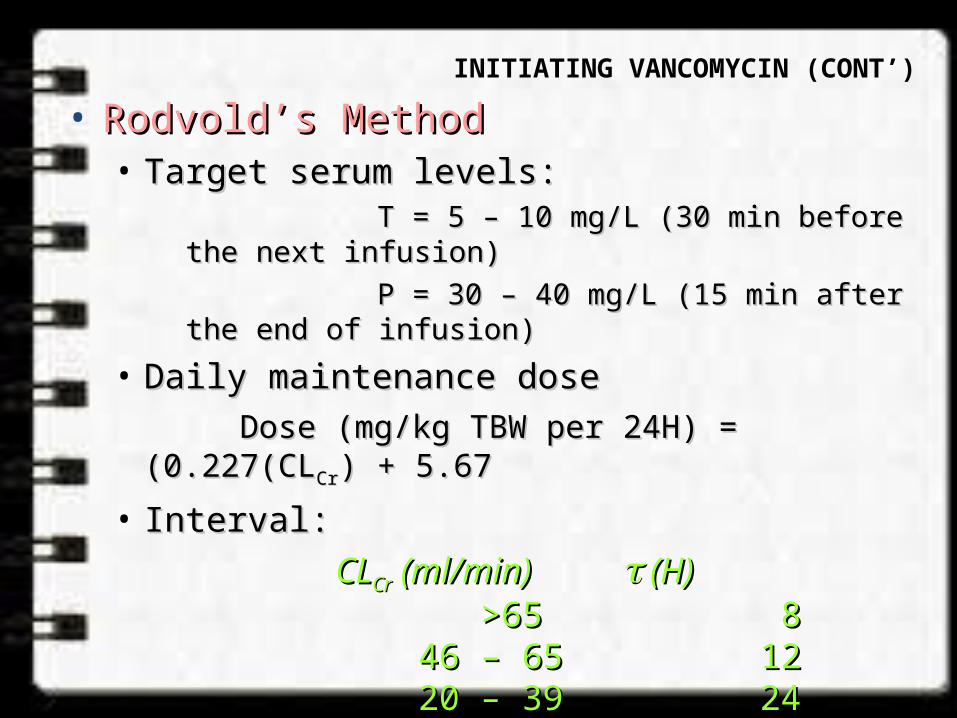
• Rodvold’s MethodRodvold’s Method• Target serum levels:Target serum levels:
T = 5 – 10 mg/L (30 min before the next T = 5 – 10 mg/L (30 min before the next infusion)infusion)
P = 30 – 40 mg/L (15 min after the end of P = 30 – 40 mg/L (15 min after the end of infusion)infusion)
• Daily maintenance dose Daily maintenance dose Dose (mg/kg TBW per 24H) = (0.227(CLDose (mg/kg TBW per 24H) = (0.227(CLCrCr) + 5.67) + 5.67
• Interval:Interval:CLCLCrCr (ml/min) (ml/min) (H) (H) >65>65 8 8 46 – 65 46 – 65 12 12 20 – 39 20 – 39 24 24 10 – 19 10 – 19 48 48
INITIATING VANCOMYCIN (CONT’)
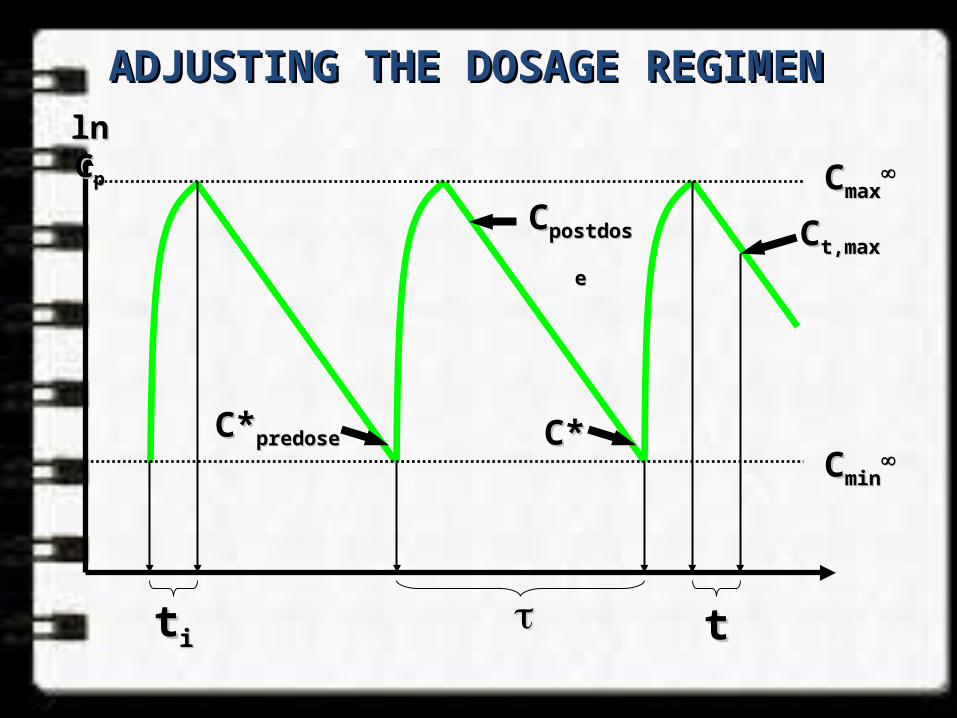
ADJUSTING THE DOSAGE REGIMEN ADJUSTING THE DOSAGE REGIMEN ln Cln Cpp
ttii tt
CCminmin
CCmaxmax
C*C*predosepredose C*C*
CCpostdosepostdose CCt,maxt,max
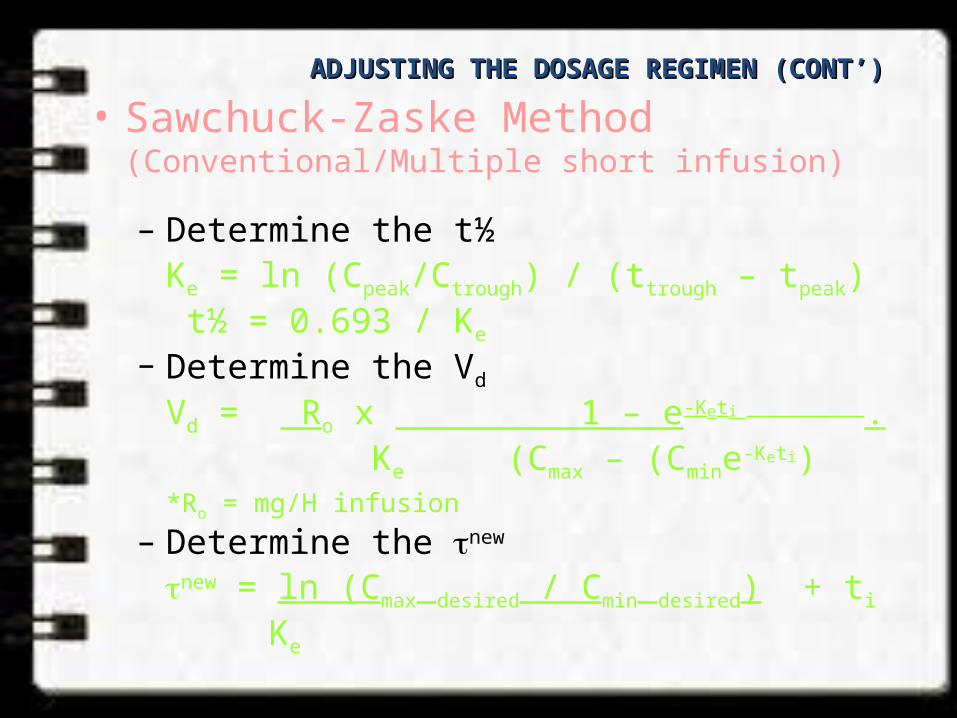
• Sawchuck-Zaske Method (Conventional/Multiple short infusion)
– Determine the t½Ke = ln (Cpeak/Ctrough) / (ttrough – tpeak) t½ = 0.693 / Ke
– Determine the Vd
Vd = Ro x 1 – e-Keti . Ke (Cmax – (Cmine-Keti)
*Ro = mg/H infusion– Determine the new
new = ln (Cmax desired / Cmin desired) + ti
Ke
ADJUSTING THE DOSAGE REGIMEN (CONT’) ADJUSTING THE DOSAGE REGIMEN (CONT’)
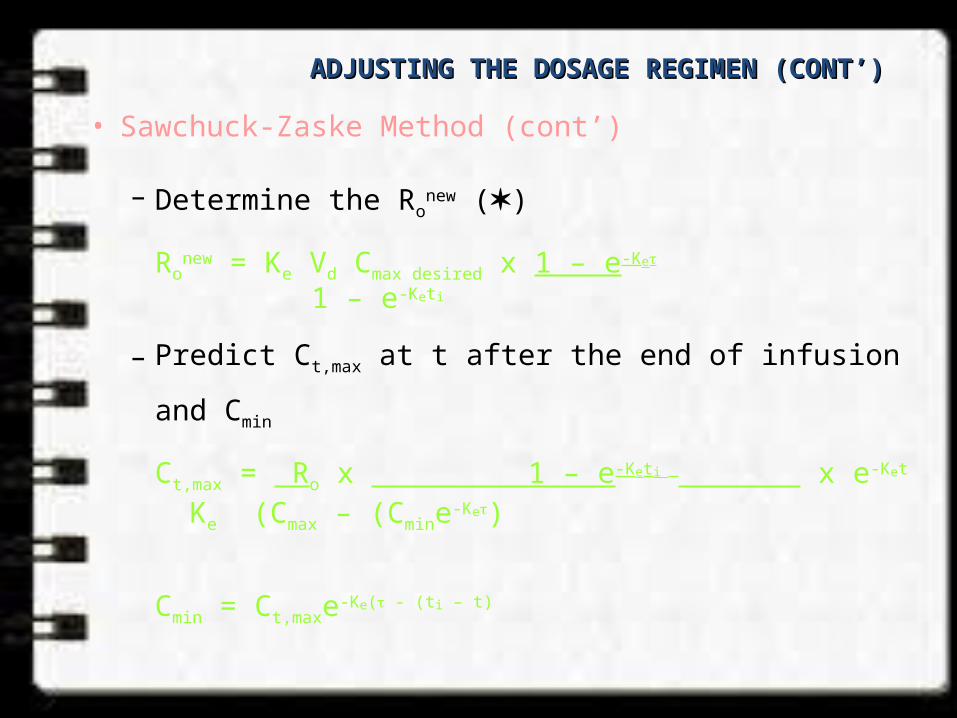
• Sawchuck-Zaske Method (cont’)
– Determine the Ronew ()
Ronew = Ke Vd Cmax desired x 1 – e-Ke
1 – e-Keti
– Predict Ct,max at t after the end of infusion and Cmin
Ct,max = Ro x 1 – e-Keti x e-Ket
Ke (Cmax – (Cmine-Ke)
Cmin = Ct,maxe-Ke( - (ti – t)
ADJUSTING THE DOSAGE REGIMEN (CONT’) ADJUSTING THE DOSAGE REGIMEN (CONT’)
• Continuous Infusion Method
– Determine the CLvanco
CLvanco* = Ro / achieved Cave
ss
– Determine the new Ro (mg/H)
Ro = CLvanco* x targeted Cave
ss
ADJUSTING THE DOSAGE REGIMEN (CONT’) ADJUSTING THE DOSAGE REGIMEN (CONT’)
THANK YOU