week 3 jan 27, 2011. word finding difficulty is one of the striking feature of aphasia (t/f) ...
TRANSCRIPT
ADULT LANGUAGE DISORDERS
Week 3Jan 27, 2011

Review
Word finding difficulty is one of the striking feature of aphasia (T/F)
Aphasia is a language impairment affecting all four modalities of language (T/F)
Writing is typically least impaired area in an individual with aphasia (T/F)
Aphasic individuals are good at using ________ forms of speech
Aphasia is an impairment of intellectual functioning such as reasoning, problem solving, etc. (T/F)

Objectives
Understand the explanations for Aphasia Learn about the etiology of Aphasia Understand the Aphasia classification
systems Discuss the symptomatology of different
forms of fluent Aphasias Wernicke’s Aphasia Conduction Aphasia Anomic Aphasia Transcortical sensory aphasia
Explanations for Aphasia
Two orientations: Neurological and cognitive 1. Neural processes
(i.e., neurons, cerebral areas)
2. Psychological or
mental processes (i.e., ideas or memories, comprehension)
• Relationship between ideas and words

Neurological Explanation for Aphasia
Features and severity of neurogenic communication disorders depend on location and magnitude of the damage… (Brookshire, 1997)
Neurological Explanation for Aphasia
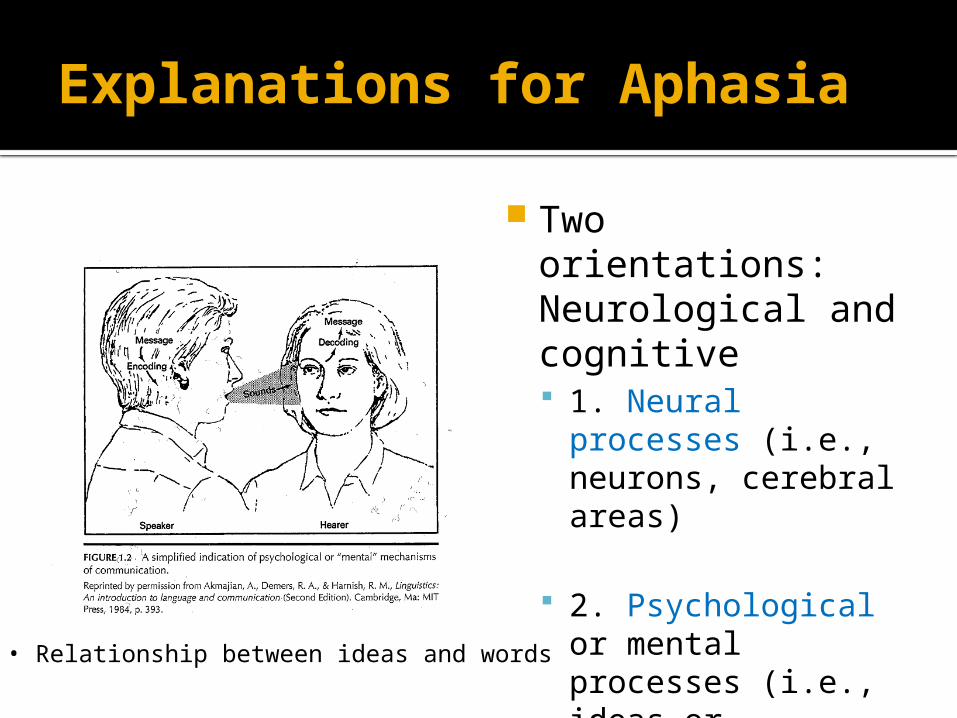
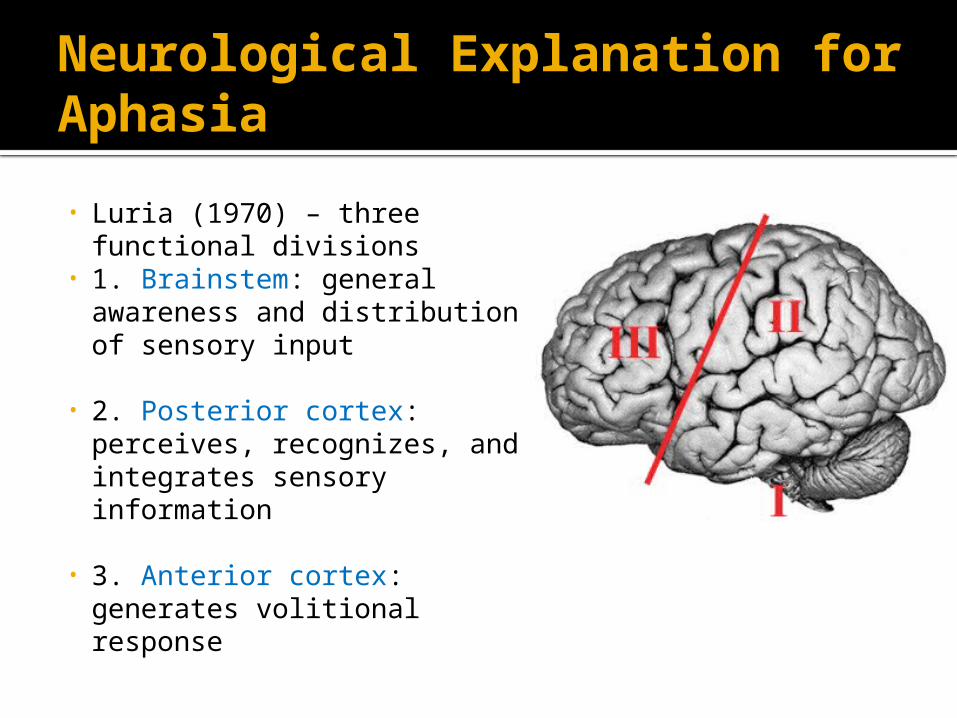
• Luria (1970) – three functional divisions
• 1. Brainstem: general awareness and distribution of sensory input
• 2. Posterior cortex: perceives, recognizes, and integrates sensory information
• 3. Anterior cortex: generates volitional response
Luria
Neurological Explanation for Aphasia
Focal lesions (e.g., stroke) multifocal lesions (e.g., little strokes
through the year) diffuse lesions (spread evenly
throughout the brain)
Neurological Explanation for Aphasia
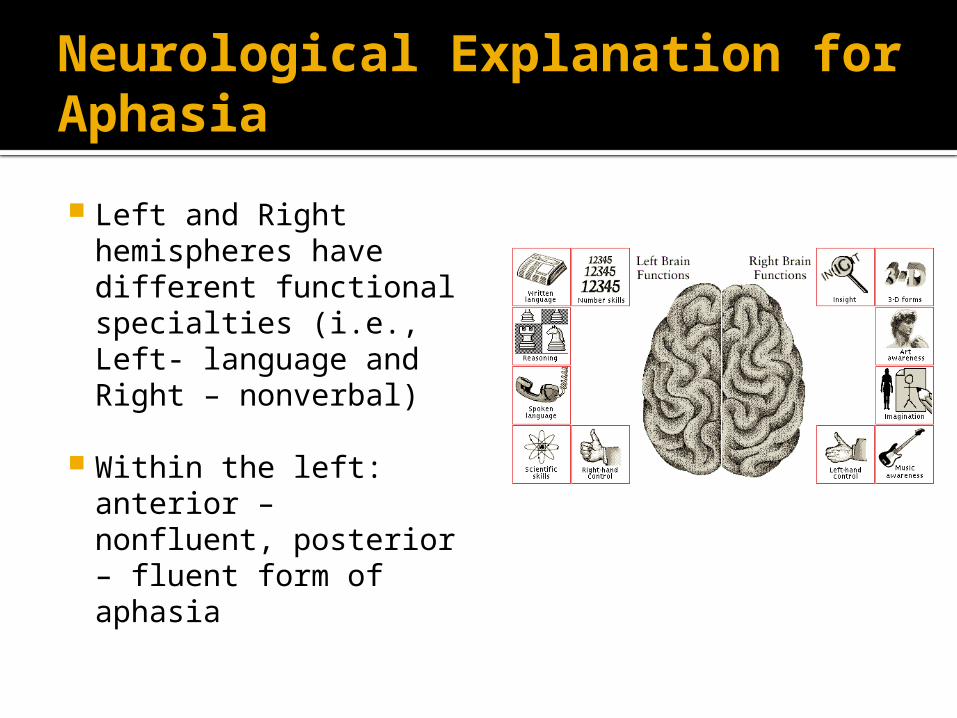
Left and Right hemispheres have different functional specialties (i.e., Left- language and Right – nonverbal)
Within the left: anterior – nonfluent, posterior – fluent form of aphasia
Cognitive Explanation for Aphasia
Encoding and decoding messages – relationship between ideas and words stored in our memory
Two features of cognition Knowledge (stable storage) – about the world and
language we speak Process – transient activity of mind, a response to
stimulus
Memory is the key to carryout all cognitive functions

Memory
Long-term memory (LTM) Different types of knowledge
Episodic memory Semantic memory- common knowledge Procedural memory Lexical memory- words and knowledge
about words
Memory
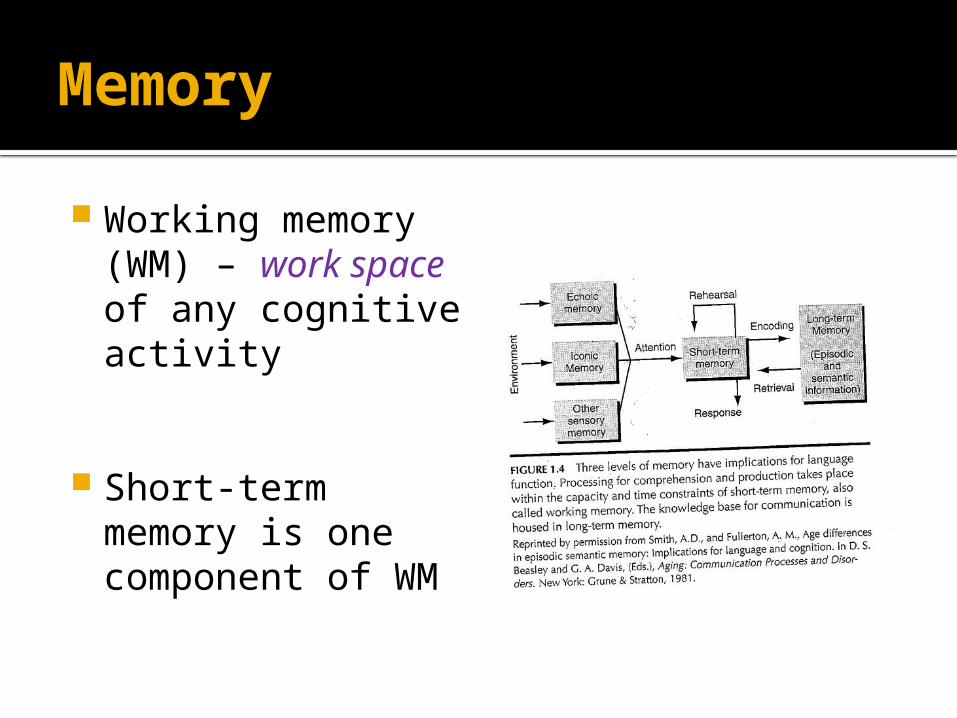
Working memory (WM) – work space of any cognitive activity
Short-term memory is one component of WM

Aphasia
Cognitive processing including language processing Constrained by the capacity of WM Draws knowledge from LT storage Operates at automatic and controlled levels
In aphasia language storage system is relatively intact Impairment of processing

Aphasia- Take Home
Aphasia is a selective impairment of the cognitive system specialized for comprehending and formulating language, leaving other cognitive capacities relatively intact. (Davis, 2007, p.15)
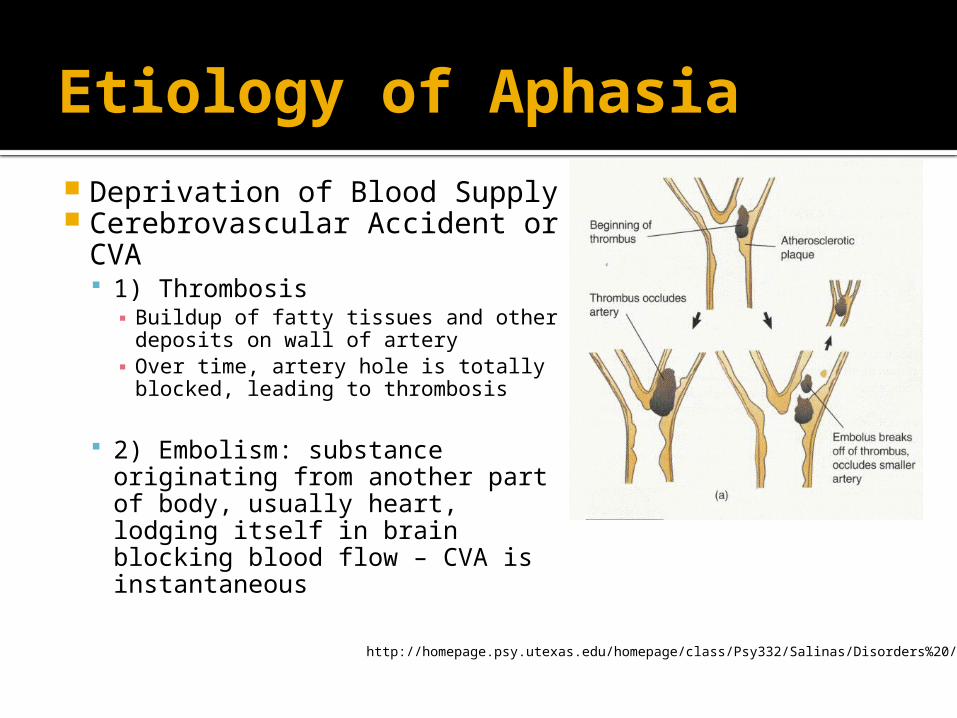
Etiology of Aphasia Deprivation of Blood Supply Cerebrovascular Accident
or CVA 1) Thrombosis
▪ Buildup of fatty tissues and other deposits on wall of artery
▪ Over time, artery hole is totally blocked, leading to thrombosis
2) Embolism: substance originating from another part of body, usually heart, lodging itself in brain blocking blood flow – CVA is instantaneous
http://homepage.psy.utexas.edu/homepage/class/Psy332/Salinas/Disorders%20/stroke1.gif
Etiology of Aphasia
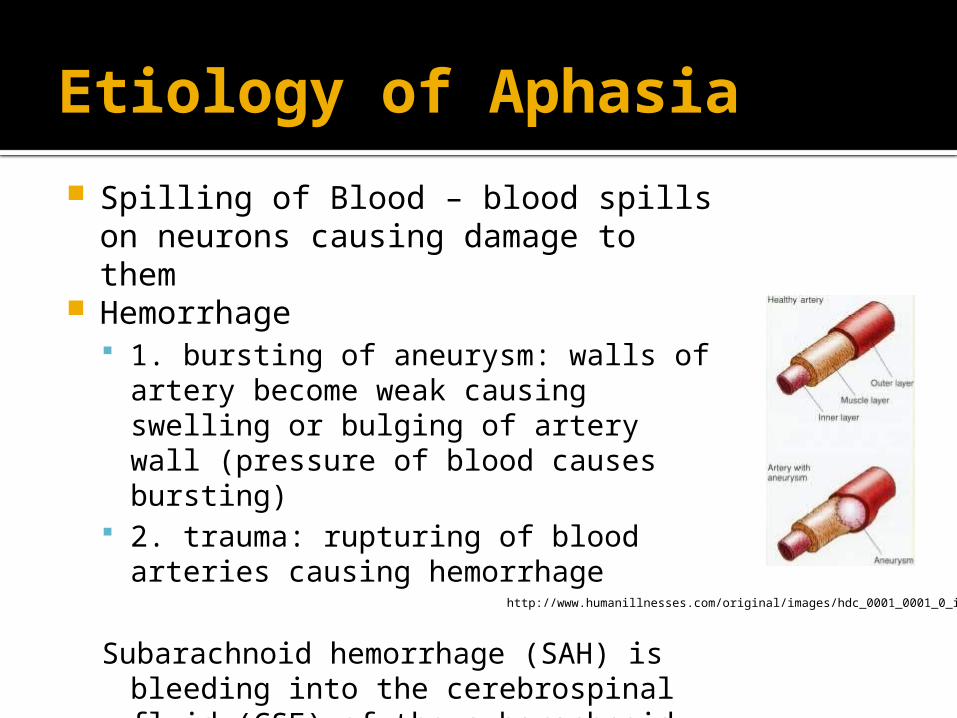
Spilling of Blood – blood spills on neurons causing damage to them
Hemorrhage 1. bursting of aneurysm: walls of artery
become weak causing swelling or bulging of artery wall (pressure of blood causes bursting)
2. trauma: rupturing of blood arteries causing hemorrhage
Subarachnoid hemorrhage (SAH) is bleeding into the cerebrospinal fluid (CSF) of the subarachnoid space surrounding the brain.
http://www.humanillnesses.com/original/images/hdc_0001_0001_0_img0020.jpg

Aphasia Classification
A. Receptive versus expressive aphasia▪ 1. based on predominance of one set of
abilities over another▪ 2. major difficulties related to language
reception or expression
Aphasia Classification
B. Anterior versus posterior aphasia : anatomically-based
C. Fluent versus nonfluent aphasia▪ 1. divides patients based on verbal output▪ 2. using this dichotomy, patients can be
additionally classified

Aphasia Classification
Fluent a. patients who
produce longer phrases
b. five or more connected words
c. speak more than 75 words per minute
Nonfluent a. those who
produce only single word utterances or short phrases
b. four or fewer connected words
c. speak 50 or fewer words per minute
Fluent Aphasias
• Posterior lesions
• Discharged early – may not be referred to speech-pathologist
• They are not controllable (stimulus-response model) – agitated, suspicious
• They are fewer than fluent aphasics
• Mixed up with confused patients (misdiagnosed)
• Older than most aphasic patients (mean age -63 Vs 52 in Broca’s)
Fluent Aphasias
• Three syndromes based on speech features: • Wernicke’s, conduction, anomic • (dysproportionality features, it is not all or nothing) –
Long-standing classification
▪ Melodic line – intonational pattern encompasses entire sentence
▪ Phrase length- length of uninterrupted word groups
▪ Articulatory agility – ease with which patient articulates phonemic sequence
▪ Grammatical forms – variety of grammatical construction
Wernicke’s aphasia
• Set of behaviors associated with a generally similar lesion.
• Wernicke postulated that traces of words would be stored at or near the Sylvian fissure (first temporal gyrus)
• Defective auditory comprehension
Wernicke’s aphasia
• Poor self-monitoring
• Fluent but paraphasic speech (due to loss of the internal correction of the motor process)
• Paraphasic speech pattern is unnoticed by the speaker (due to impaired auditory monitoring)
• Defective repetition skills (due to impaired auditory comprehension)
• Both reading and writing usually disrupted including reading comprehension
• Verbal expression consists of • a) word finding problems• b) verbal paraphasias (semantic and unrelated)• c) some phonemic paraphasias• d) neologisms• e) jargon• g) paragrammatism
▪ Press for speech: irrepressible intention of the speaker to continue in his monologue (possible due to lack of correction over output)
▪ increase in awareness of errors usually demonstrates an improvement in comprehension
Wernicke’s aphasia
▪ Because posterior lesion, usually show no paralysis (hemiplegia) or weakness (hemiparesis) in extremities
▪ http://www.youtube.com/watch?v=B-LD5jzXpLE&feature=related
▪ Lesion site:▪ Posterior portion of STG▪ The auditory association area or Wernicke’s area▪ Kertesz et al. (1993) found that persisting Wernicke’s
aphasia usually involves the supramarginal and angular gyri in addition to the superior temporal area
Wernicke’s aphasia

• Functional reorganization of language after stroke
• Recovery of function in Wernicke’s aphasia may be accompanied by a redistribution of activity within both cerebral hemispheres.
• fMRI data suggests that clinical recovery is associated with a redistribution of function to the right hemisphere (Thurlborn et al., 1999; Cherney & Robey, 2001)
Wernicke’s aphasia
Comprehension deficit
Fluent but paraphasic speech
Reading comprehension deficits: Aphasic Alexia Oral reading versus reading
comprehension
Writing deficits
Wernicke’s aphasia:Differentiating features

Ancillary behaviors: Depression: 37% (cumulative)
▪ Major post stroke depression▪ Reactive post stroke depression
▪ Sadness, dependency and indecisiveness
Lesion causing Wernicke’s symptomatology may go unnoticed.
Wernicke’s Aphasia
1. Locus of lesion is parietal operculum or arcuate fasciculus although controversy exists over lesion site• Left hemisphere supramarginal gyrus and arcuate
fasciculus• The insula, and underlying white matter of left
hemisphere• Small lesions of Wernicke’s area• More anterior and inferior lesions (anterior
supramarginal gyrus, underlying white matter, angular gyrus, and insular cortex) are deemed responsible for phonologic output problems
Conduction Aphasia
▪ 2. breakdown in transmission of information from posterior to anterior regions
▪ 3. relatively good auditory comprehension
▪ 4. verbal expression consists of ▪ Fluent, preserved melody, variety and complexity of syntactic structures▪ word finding problems, ▪ paraphasias with much higher incidence of phonemic than verbal paraphasias; ▪ hallmark feature of disorder is severe repetition deficit, especially for functions
and numbers
▪ 5. much more aware of errors and more interested in correcting errors than Wernicke’s patients probably due to better comprehension
▪ 6. visual comprehension is relatively intact and writing skills mirror verbal output
Conduction Aphasia
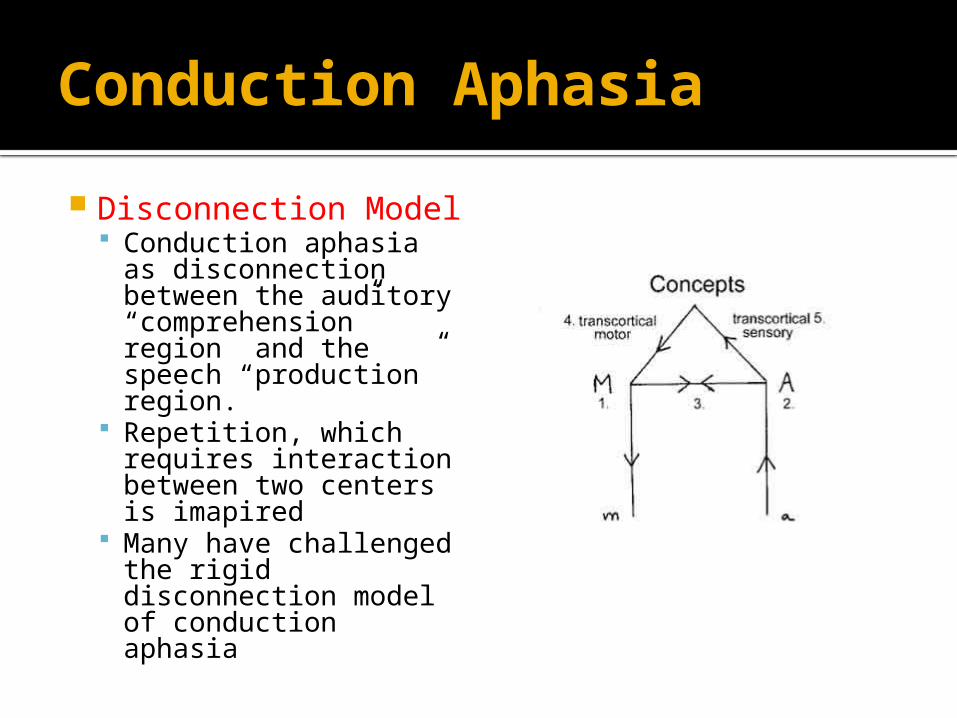
Disconnection Model Conduction aphasia
as disconnection between the auditory “comprehension” region and the speech “production” region.
Repetition, which requires interaction between two centers is imapired
Many have challenged the rigid disconnection model of conduction aphasia
Conduction Aphasia
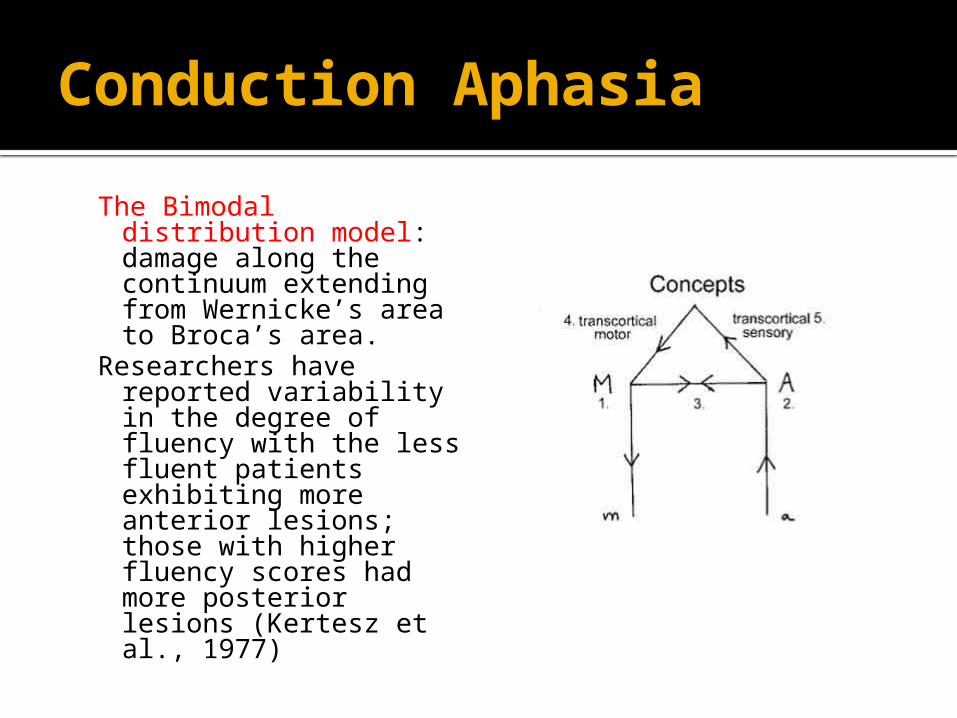
The Bimodal distribution model: damage along the continuum extending from Wernicke’s area to Broca’s area.
Researchers have reported variability in the degree of fluency with the less fluent patients exhibiting more anterior lesions; those with higher fluency scores had more posterior lesions (Kertesz et al., 1977)
Conduction Aphasia

The “Two” Conduction Aphasias Two disorders with distinct pathophysiologic
mechanism (Nadeau, 2001)▪ Repetition conduction aphasia: deficit in auditory
short-term memory, disturbance only of verbal repetition tasks
▪ Reproduction conduction aphasia: more general language impairment affecting phonologic output process▪ Deficits in word production across verbal tasks including
conversation, naming, and oral reading as well as repetition.
▪ These two types of difficulties arise from lesions in functionally distinct but anatomically adjacent areas in temporoparietal region
Conduction Aphasia

Primary criteria for diagnosis Fluent, paraphasic conversational speech
No significant difficulty in comprehension of normal conversation
Significant verbal repetition disturbance
A preponderance of phonemic paraphasias
Conduction Aphasia
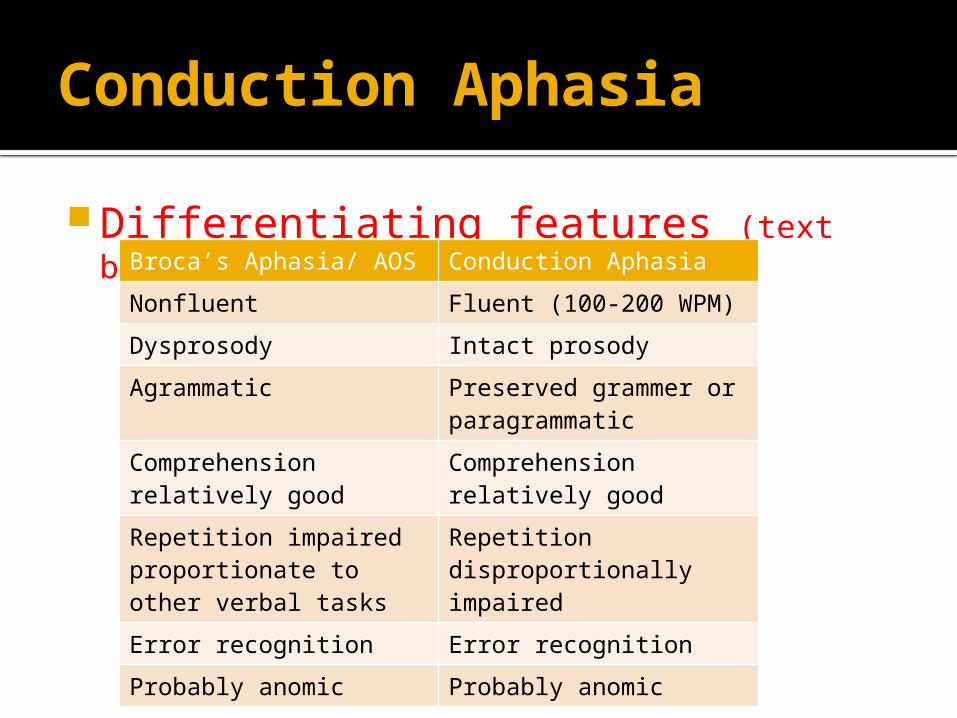
Differentiating features (text book, pg 156)
Conduction Aphasia
Broca’s Aphasia/ AOS Conduction Aphasia
Nonfluent Fluent (100-200 WPM)
Dysprosody Intact prosody
Agrammatic Preserved grammer or paragrammatic
Comprehension relatively good
Comprehension relatively good
Repetition impaired proportionate to other verbal tasks
Repetition disproportionally impaired
Error recognition Error recognition
Probably anomic Probably anomic
More description of salient features:• Fluency
▪ Fluent but not as fluent as Wernicke’s aphasics
• Word finding (content words): Some variability • Paraphasias: phonemic paraphasias
▪ produce more errors on a forced choice of specific target words
• Error recognition• Repetition
▪ Difficulties appear more on phrases, short sentences, poly syllabic words
• Auditory comprehension• Reading
Conduction apahsia

Favorable spontaneous recovery pattern
Conduction aphasics show significant or even complete recovery
Sometimes they “evolve” from classifications such as “jargon or Wernicke’s aphasia
They perform well in situations that do not require single-word accuracy or specific responses.
Conduction Aphasia

▪ Poorly localized: angular gyrus lesion and/or posterior middle gyrus
▪ Many Wernicke’s evolve into Anomic
▪ 1. Empty speech: lot of words like, thing, it, you know what I mean.. Frustrated
▪ 2. relatively good auditory comprehension
Anomic aphasia
▪ 3. verbal expression consists of predominance of word finding problems with the more salient the word, the more difficulty finding it and an absence of paraphasic errors (emptiness of substantive words in speech)
▪ 4. reading and writing skills vary from patient
to patient due to how extensive the lesion posteriorly – the more posterior the lesion, the more involved are reading and graphic impairments
Anomic aphasia

▪ 1. like severe Wernicke’s aphasia in verbal output with verbal paraphasias (both unrelated and semantic), phonemic paraphasias, neologisms, word retrieval deficits – more jargon
▪ 2. very poor auditory comprehension
Transcortical sensory aphasia

▪ 3. unlike Wernicke’s aphasia, repetition is intact as well as a preservation of memorized material
▪ 4. lesion is in posterior part of parietal lobe with sparing of Wernicke’s area and arcuate fasciculus fibers (referred to as watershed lesion)
▪ 5. written language is impaired for both reading and writing
Transcortical sensory aphasia

Fluent Aphasias
Wernicke’s Conduction Transcortical sensory
Auditory comprehension Severely impaired Slightly impaired Severely impairedReception Impaired Impaired IntactSpeech Fluent, paraphasic Paraphasic Fluent, ParaphasicReading Impaired Intact ImpairedWriting Impaired Impaired Impaired
Behavioral Patterns of Types of Aphasia