week 3 adaptations and accumulations dr.İ.taci cangül bursa-2008
TRANSCRIPT
Week 3Adaptations and Accumulations
Dr.İ.Taci Cangül
Bursa-2008
Adaptations
• Hyperplasia: Increase in number of cells
• Hypertrophy: Increase in size of cells
• Atrophy: Decrease in size
• Metaplasia: Cellular differentiation
• Dysplasia: Disordered growth patterns

Hyperplasia
• Physiologic hyperplasia: – Hormonal stimulation (breast and uterus)– Extra workloads
• Pathologic hyperplasia:– Excessive hormonal stimulation (endometrial
hyperplasia)

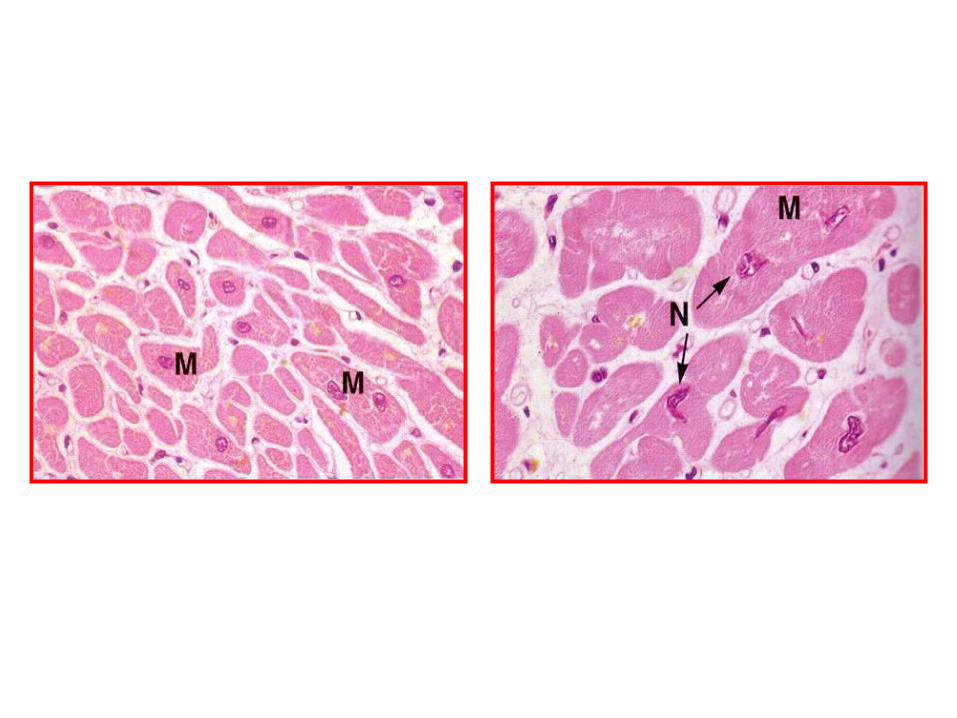
Hypertrophy
• Increase in size of an organ as a result of an increase in the size of individual cells
• Physiologic: When muscles are worked
• Pathologic: Hypertension causes hypertrophy of the heart, specifically of the left ventricle



Atrophy• A shrinkage in the size of the cell by loss of cell
substance• Physiologic atrophy: Loss of the ductus
arteriosus in utero• Pathologic atrophy: Shrinkage of our brains as
we age• Local atrophy: Most often the result of
decreased blood flow to that area• Disuse atrophy: Essentially when an organ is
underused, it undergoes atrophy. Another example of this is an immobilized limb, which undergoes muscle wasting upon casting.


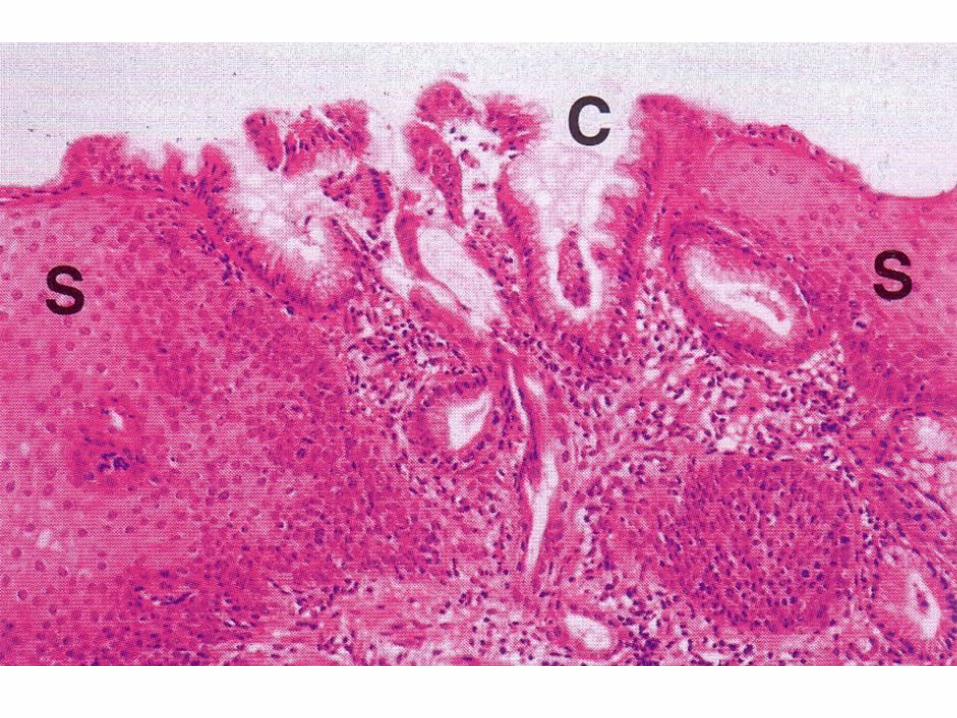
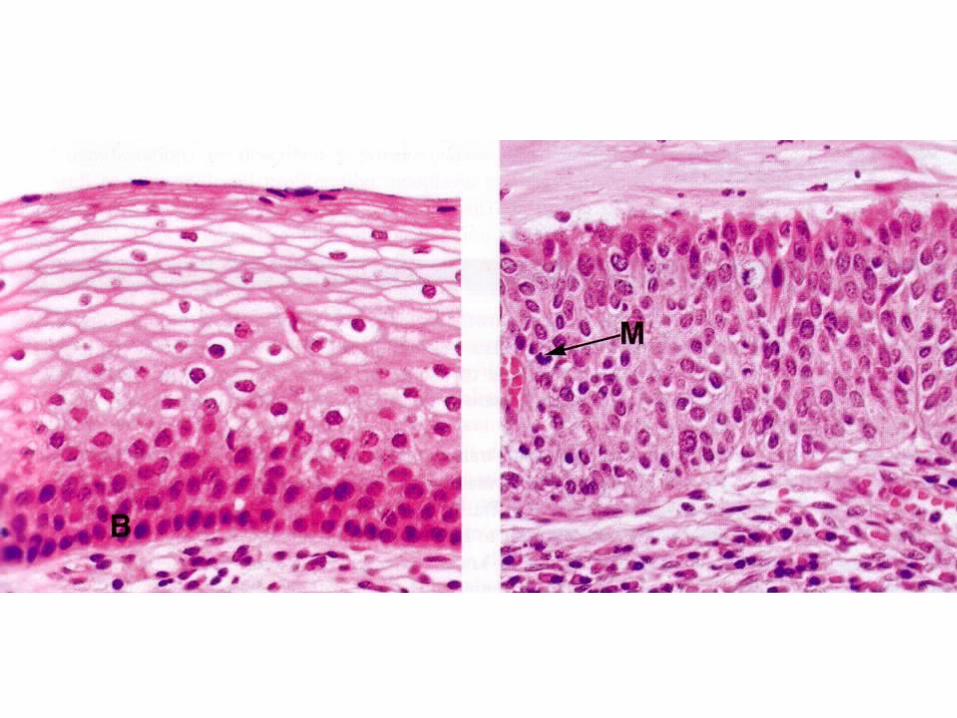
Metaplasia
• One mature adult tissue is replaced by another.• Smoking: Replacement of pseudo‑stratified
columnar epithelium of the lungs by stratified squamous epithelium
• Metaplasia may also be seen within mesenchymal tissue. Soft tissues that undergo trauma may be replaced by mature bone.

Dysplasia
• Abnormal epithelial maturation which is characterized by alterations in cell size, shape and organization
Accumulations and Pigmentations

Intracellular Accumulations
• Under certain circumstances, in normal or injured cells
• Most often occurs in the cytoplasm and usually contained within lysosomes
• Mostly, substances that are produced by the cell – Either their rate of production is increased or their rate
of utilization and/or elimination is reduced
• In other instances, substances that originate in other organs or tissues accumulate in cells because of an inability on the part of that cell to eliminate or metabolize the substance at a rate exceeding its acquisition

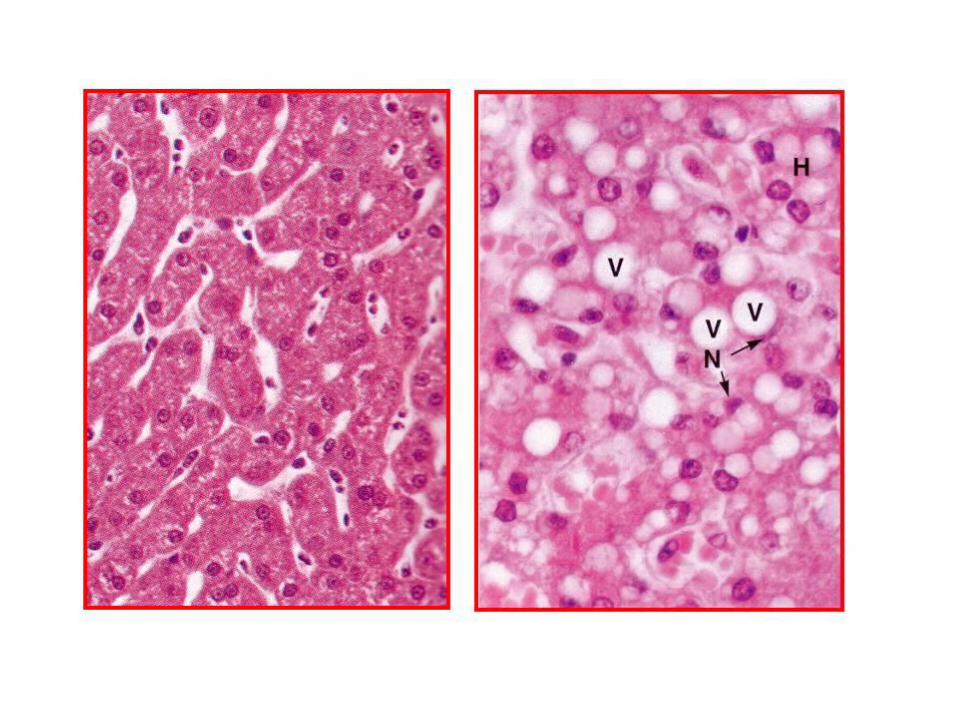
Fatty Change
• Abnormal accumulation of fat within parenchymal cells
• Fatty degeneration, fatty infiltration• Most notedly in hepatocytes• The liver plays a pivotal role in the
metabolism of fat because it is largely responsible for the conversion of free fatty acids into a lipoprotein which is more readily utilizable by other cells

Causes of Fatty Change
1. Excessive entry of lipids into the liver 2. Enhanced fatty acid synthesis by
hepatocytes3. Decreased oxidation of fatty acids by
mitochondria4. Increased esterification of fatty acids to
triglycerides5. Decreased apoprotein synthesis6. Impaired lipoprotein excretion


Other Lipid Accumulations
• Cholesterol and cholesterol esters
• In atherosclerosis, cholesterol accumulates in smooth muscle cells and macrophages in the intima of arteries
• In hereditary hyperlipemia, cholesterol accumulates in macrophages, usually under the skin, forming tumor-like structures known as xanthomas

Intracellular Accumulation of Proteins
• Primarily in epithelial cells of the proximal convoluted tubules of the kidney and in plasma cells
• In the kidney, this excessive accumulation occurs subsequent to leakage of proteins from glomeruli into the glomerular filtrate
• Plasma cells actively engaged in the production of immunoglobulins sometimes become overloaded with these immunoglobulins and large eosinophilic inclusions, called Russell Bodies, appear in their cytoplasm

Intracellular Accumulation of Glycogen
• Glycogen Infiltration and Glycogen Storage • Glycogen appears as clear vacuoles in the
cytoplasm of cells• Hyperglycemia
• Epithelial cells of the distal portion of the proximal convoluted tubule and in the loop of Henle in the kidney
• Leukocytes within inflamed or necrotic tissue• Liver • Cardiac muscle fibers

Intracellular Accumulations of Complex Lipids and Carbohydrates• Lysosomal storage diseases• Mainly in reticuloendothelial cells,
neurons, myocardial fibers and the parenchymal cells of the liver and kidneys
• Sphingolipids, mucopolysaccharides, mucolipases, complex carbohydrates, cholesterol esters and triglycerides.
• Tay-Sachs disease, Niemann-Pick disease, Gaucher's disease, etc.

Inclusion Bodies
• Intracellular or intracytoplasmic
• Eosinophilic or basophilic
• Major significance in making an etiologic diagnosis
• Aggregates of virions which tend to have characteristic stain affinities
Inclusion Bodies
• Lead poisoning: Acid fast intranuclear inclusions in renal tubular epithelial cells
• Chediak-Higashi syndrome: Autosomal recessive genetic disorder, large intracytoplasmic granules (abnormally fused versions of normal granule subpopulations)

Extracellular Accumulations
• Calcification
• Hyaline change
• Amyloid and amyloidosis
• Gout
• Fibrinoid
Calcification
• “Deposition of calcium salts in vital or dying/dead tissues”
• Dystrophic and metastatic
Dystrophic Calcification
• “Deposition of calcium salts in dead or dying tissues”
• Principally in areas of coagulative, liquefactive, caseous and/or fat necrosis that persist for rather long periods of time.
• Normal levels of serum calcium (around 10 mg/100 ml) and in the absence of derangement in calcium metabolism


Metastatic Calcification
Deposition of calcium salts in vital tissues in association with a defect in calcium metabolism that is characterized by hypercalcemia
Usual causes:(1) Hyperparathyroidism, either primary or secondary(2) Vitamin-D intoxication(3) Deficiency of magnesium(4) Hypercalcemia of malignancy
Metastatic Calcification
• Principally in interstitial tissue of blood vessels, kidneys, lungs and gastric mucosa
• The fundamental abnormality is the pathologic entry of large amounts of ionic calcium into cell organelles, chiefly the mitochondria (it is suggested that mitochondria are the organelles first involved in the pathogenesis of metastatic calcification)

Hyaline Change
• “A homogeneous, glassy, pink appearance in tissues or cells stained with H&E”
• Widely used descriptive histologic term rather than a specific marker for cell injury
• Connective tissue hyaline
• Epithelial hyaline
• Kerato-hyaline
Amyloid and Amyloidosis
• Deposition of amyloid protein fibrils in tissue
• Chronic antigenic stimulation and plasmacytosis reticuloendothelial and immune system dysfunction
• Abnormal processing of components of immunoglobulins, insulin, growth hormone and an acute-phase reactant of inflammation called the serum amyloid associated protein (SAA)
Detection of Amyloid
• Small amounts: Virtually undetectable
• Large amounts: Organ enlargement and a yellowish to greyish discoloration
• Rubbery consistency
• Painting the cut surface organs with iodine: A brownish to yellow-red color
• Application of dilute sulfuric acid: Colour changes to blue or violet

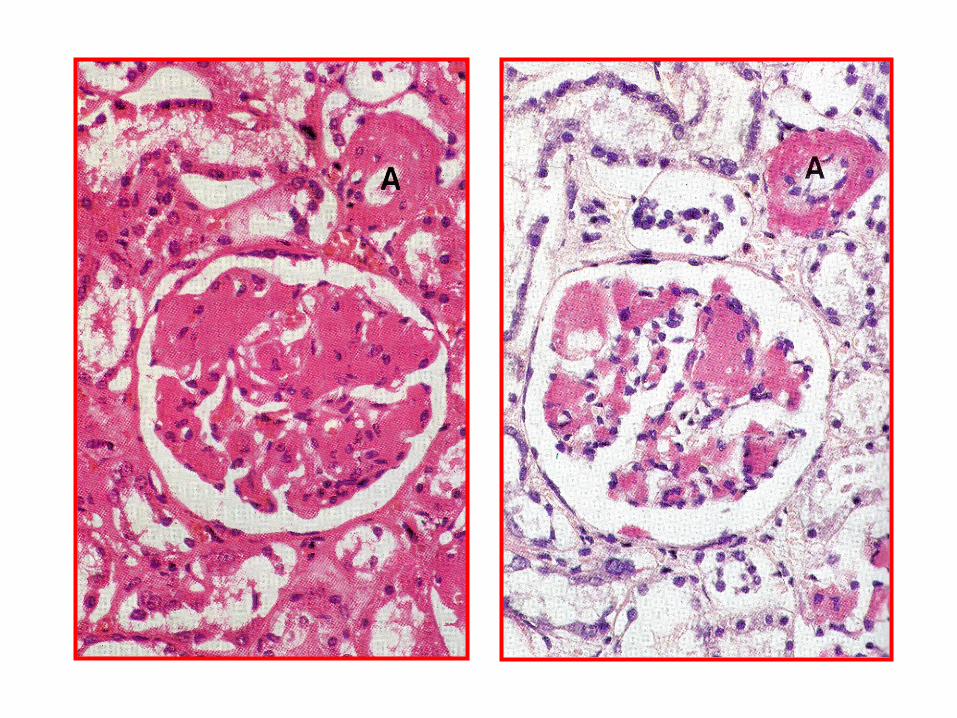
Histologically Amyloid
• Homogeneous, eosinophilic material that stains reddish pink with the Congo red stain. Under polarized light, the Congo red-stained amyloid has a green birefringence
• Compression atrophy

Ultrastructurally Amyloid
• Amyloid fibrils are 7.5-10 nm in diameter
• Rigid, nonbranching, hollow-cored tubules of indeterminate length
• Beta-pleated sheet configuration: Responsible for the previously described birefringence. Probably also responsible for its resistance to proteolytic digestion
Gout
• “Deposition of uric acid and urate crystals in tissues subsequent to defective purine metabolism”
• The condition occurs primarily in humans and in birds. In birds, articular and visceral forms of gout are recognized

Articular Gout
• Uric acid and urate crystals are deposited in joint spaces over the serous membranes
• Affected joints are enlarged, and white, chalky masses (“tophil”) may be observed when opened. The condition may result in severe pain


Visceral Gout
• Uric and urate crystals are deposited over the serous surfaces within the body cavity (pleural, pericardium, etc.)
• Deposits are also found in the renal tubules
• Grossly, serous membranes are encrusted by a thin grayish layer having a metallic sheen



Fibrinoid
• Amorphous, eosinophilic, sometimes granular deposit that resembles fibrin. It is typically seen in a focus of tissue injury (especially in vessel walls or in connective tissue)
• With H&E stains, fibrinoid appears as a deeply eosinophilic, amorphous material which sometimes entraps leukocytes or other necrotic cells. It is most often located in the intima and media of vessel walls