weaknesses of major randomized trials: they are cleverly designed against coronary surgery. they are...
TRANSCRIPT
Weaknesses of major randomized trials: they are cleverly designed
against coronary surgery. They are not representative of the daily
practice (highly selected patient population), but their results are
generalized for the whole population with CAD.
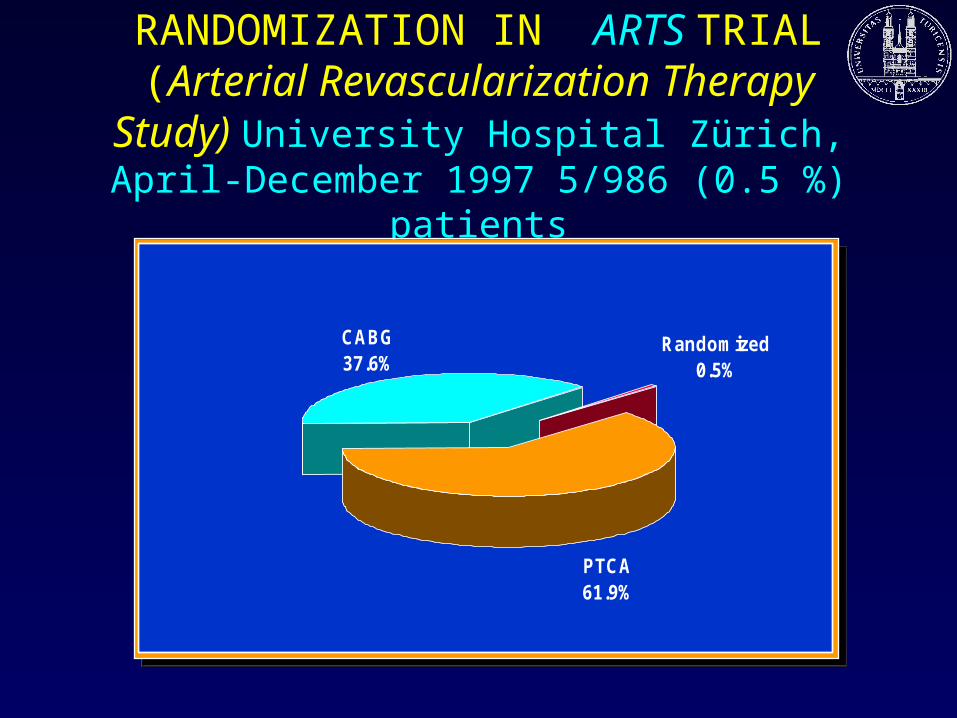
RANDOMIZATION IN ARTS TRIAL(Arterial Revascularization Therapy Study) University Hospital Zürich, April-December 1997 5/986 (0.5 %) patients
PTCA61.9%
CABG37.6%
Randomized0.5%
PTCA61.9%
CABG37.6%
Randomized0.5%
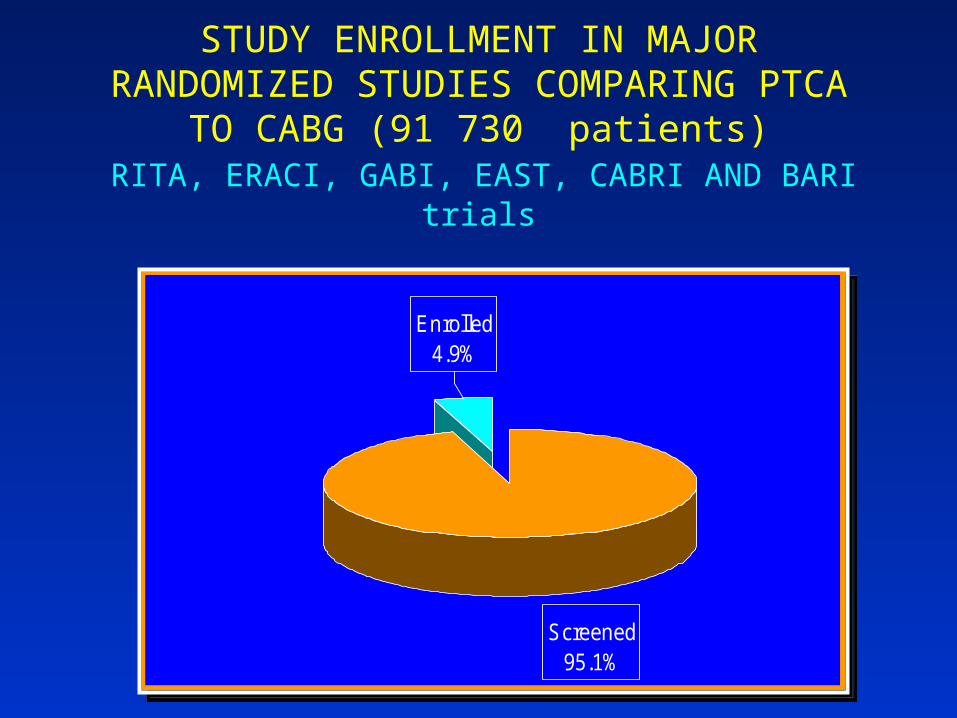
STUDY ENROLLMENT IN MAJOR RANDOMIZED STUDIES COMPARING PTCA
TO CABG (91 730 patients) RITA, ERACI, GABI, EAST, CABRI AND BARI trials
Screened95.1%
Enrolled4.9%
Screened95.1%
Enrolled4.9%
It is a well-known fact that patients recruited for trial have better survival
and better results than those eliminated from the trial because of some
exclusion criteria.
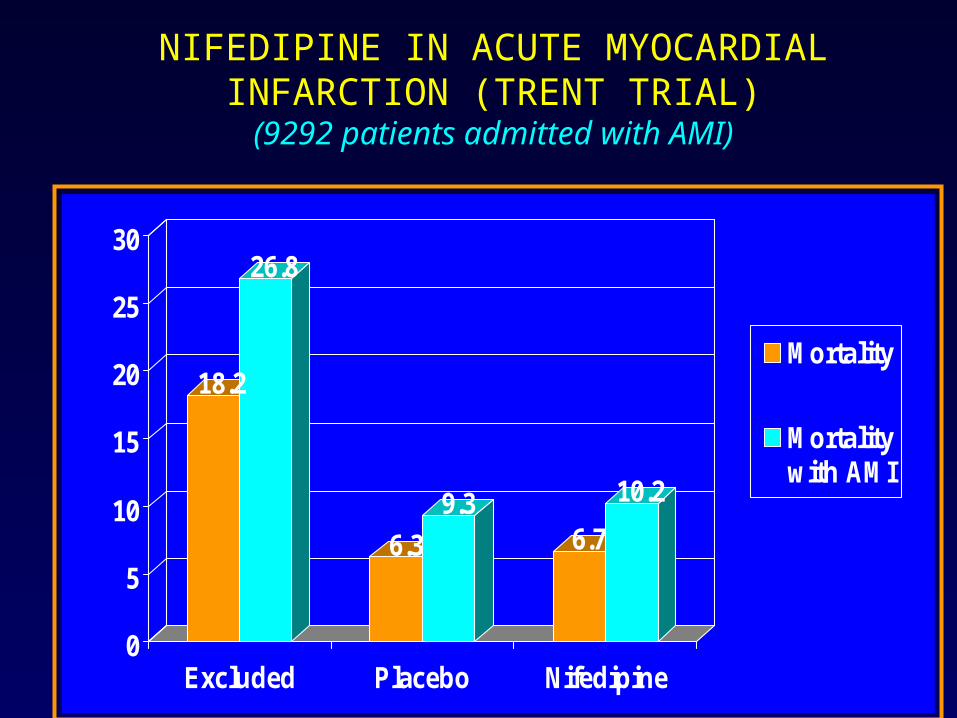
NIFEDIPINE IN ACUTE MYOCARDIAL INFARCTION (TRENT TRIAL)
(9292 patients admitted with AMI)
18.2
26.8
6.3
9.36.7
10.2
0
5
10
15
20
25
30
Excluded Placebo Nifedipine
Mortality
Mortalitywith AMI
When analyzing a trial, look carefully at “Material and Methods” section: crucial information explaining the
results might be found there.


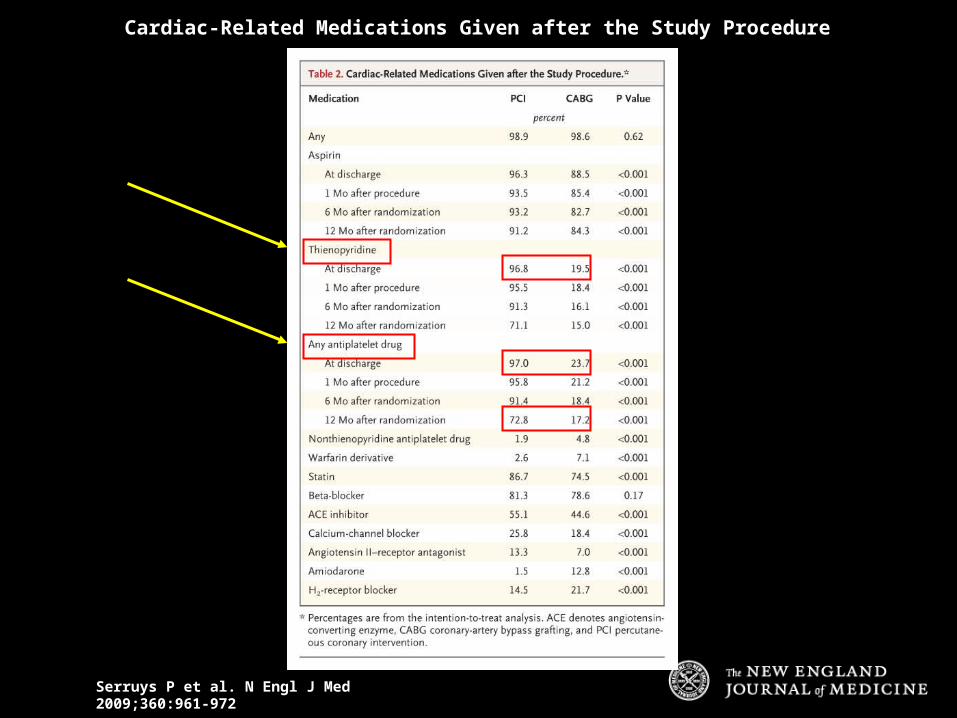
Serruys P et al. N Engl J Med 2009;360:961-972
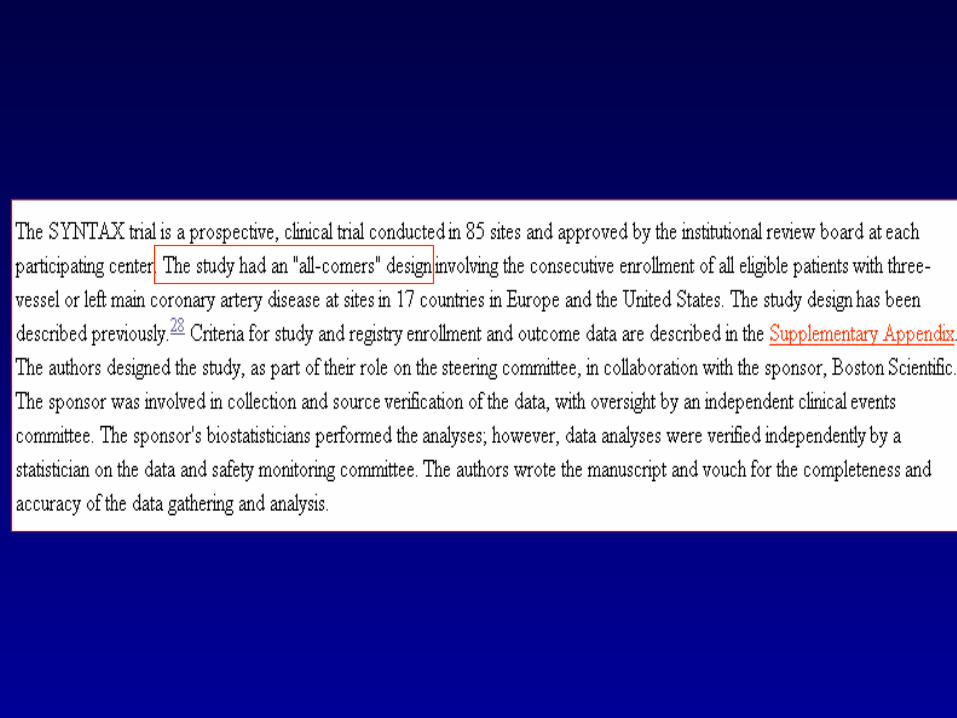
Enrollment and Randomization of Patients with Previously Untreated Three-Vessel or Left Main Coronary Artery Disease in the SYNTAX Trial
2 years, 85 centres:10.6 patients/year

Average number of patients seen by centres in Syntax trial is less than 11 patients/year!
If we accept the fact that “all comers” entered the trial, these centres should have been closed long ago, according to present
standard of PCI and CABG practice.
Serruys P et al. N Engl J Med 2009;360:961-972
Cardiac-Related Medications Given after the Study Procedure

A study with a radically different drug treatment protocols in the two analyzed groups is statistically
invalid.
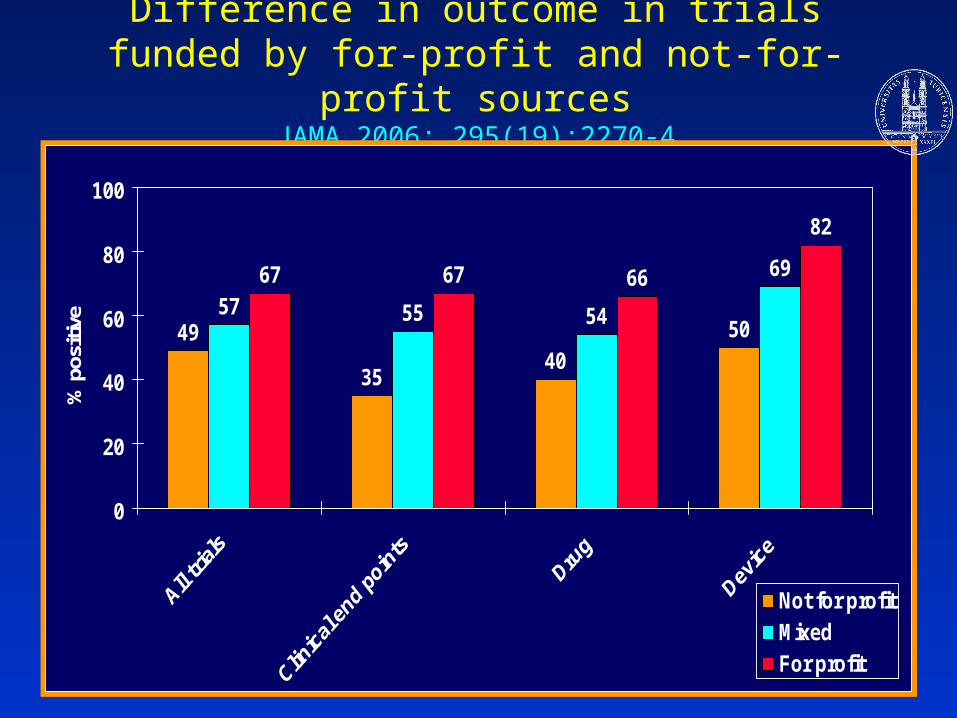
Difference in outcome in trials funded by for-profit and not-for-profit sources
JAMA 2006; 295(19):2270-4
49
3540
5057 55 54
6967 67 66
82
0
20
40
60
80
100
% p
ositi
ve
Not for profitMixedFor profit
p for trend < o.oo5


Beware of industry sponsored trials! Results very often meet the
sponsor’s expectations!

CABG MORTALITY RATES AMONG DIFFERENT SURGEONS: A PROSPECTIVE STUDY
JAMA 1991;266:803-809


There is a major difference between swallowing a pill and performing a complex operation; this fact is not
appreciated by statisticians.
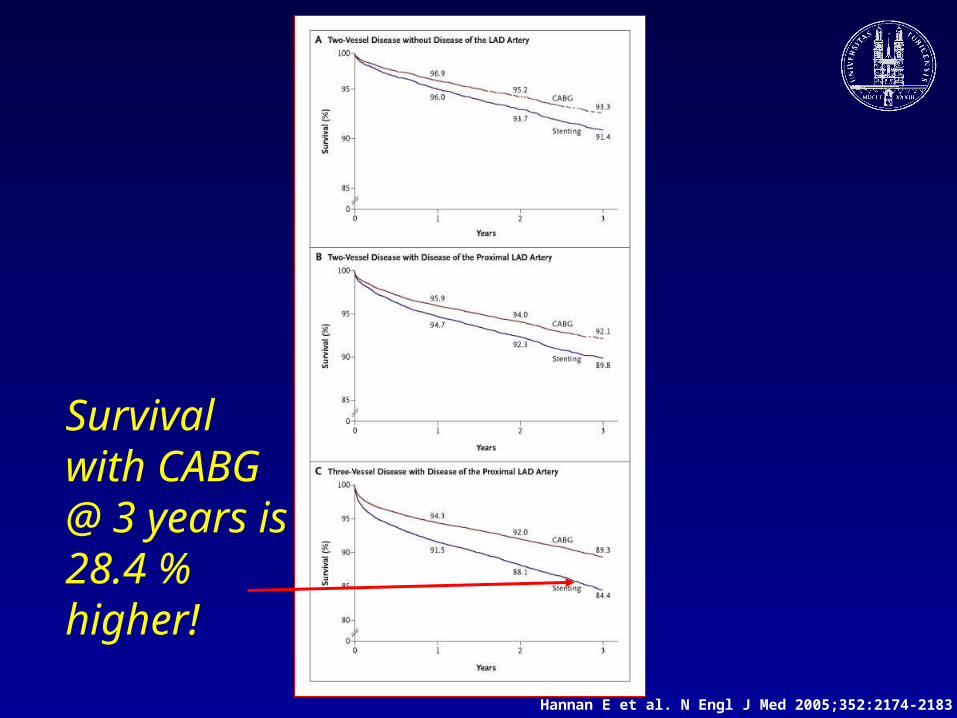
Survival with CABG @ 3 years is 28.4 % higher!
Hannan E et al. N Engl J Med 2005;352:2174-2183

Non-randomized observational trials can reach very important results, which are
presently ignored by the academia schooled in conventional statistics